searching for joy and meaning at work: supporting staff satisfaction and engagement ·...
TRANSCRIPT

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
Searching for Joy and Meaning at Work:
Supporting Staff Satisfaction and
Engagement
Ann Scott Blouin, RN, PhD, FACHE Joanne Watson, MD, MPH
Executive Vice President, Customer Relations Deputy Medical Director
The Joint Commission Torbay & South Devon
NHS Foundation Trust
5th Annual Middle East Forum on Quality and Safety in Healthcare
May 5, 2017
2
Objectives
Explore the concepts of joy and meaning within one’s professional work
Understand the issues around staff engagement, clinical leadership
behaviors, and how these directly relate to high quality clinical outcomes
Discuss specific strategies for developing joy and meaning in one’s work

3
To provide caring, competent care
When nurses feel powerless, they become disillusioned and
may leave their job or even the profession
Why Do People Choose Nursing?

4
Practicing from inner core beliefs
Understanding others from within (a sense of empathy
and connection to patients as persons)
Making a difference
Evolving as a professional nurse, willing to learn and
open to others
What Keeps Nurses in Nursing?
Adapted from Dunn, D. What Keeps Nurses in Nursing?
International Journal for Human Caring. 2012, Vol. 16, No. 3.

5
An intensely positive, vivid, and expansive emotion that
arises from an internal state or results form an external
event or situation.
What is Joy at Work?
Manion, 2003.
6
Gratitude
Intentional listening
Mindfulness with each interaction
Personal health & well-being
Willingness to help
Positivity
Personal Attributes Underlying Joy & Meaning

7
Loving your work
Being recognized
Achieving something meaningful
Feeling connected
Leads to satisfaction and engagement
What Creates Joy and Meaning?
Manion, 2003.

8
USA physicians: 60% respondents considering leaving
practice; 70% knew at least one colleague who left due to
poor morale
British physicians: 44% respondents had low or very low
morale
USA nurses: 35% felt like resigning from their current job
European surveys report nurse dissatisfaction ranging from
11% to 56%
Current State of Joy and Meaning
Sikka R, et al. BMJ Qual Saf 2015;0:1-3. doi:10.1136/bmjqs-2015-004160.

9
Lack of organizational/unit support
Inability to provide quality care
Being overwhelmed with workload, exhaustion
Lack of challenge, boredom
What Prevents or Diminishes Joy & Meaning?

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
10
What Really Is Fatigue?
Fatigue: “the body’s response to sleep loss or to
prolonged physical or mental exertion” (Am Coll
Occup Envir Med, 2012)
– Not the same as “sleepiness” which is the tendency to
fall asleep (e.g., boredom, post-prandial, night time)
Affected by both the quantity and quality of sleep
– Sufficient hours, individual variation
– Uninterrupted
– Consistency with natural day/night Circadian rhythms
Acute or chronic

11
Contributing Factors
Organization & Management
• Overtime requirements
• Inadequate staffing
• Excessive workload
• Lack of safety culture, trust
• Lack of support systems, provisions (places to rest, etc.)
Nature of the Work
• Shift work (around the clock)
• Shift rotation
• Shift length
• Patient / resident acuity, needs
• Mental and physical demands of activities
Personal
• “Moonlighting”
• Extra work, education
• Habits, choices
• Family (new baby, multiple care-giving roles)
• Sleep disorders
• Overconfidence

12
Contributing Factor: Staff Shortages
Staff Shortages
Difficulty in Recruiting &
Retaining Staff
Changing Work
Patterns (OT) & Physical demands
Impact on Quality of
Care

13
Costly and Dangerous Cycle When Workload-Staffing
Imbalance Exists
Understaffing
Increasing Overtime
FatigueStaff
Burnout
Increased Turnover
Source: Lerman et al, 2012, ACOEM Fatigue Risk Management

14
Consequences of Fatigue
Lapses in attention Inability to stay focused Memory lapses
Confusion
Irritability
Diminished reaction time Slowed or faulty information processing and judgment
Compromised problem solving
Impaired communication
Reduced motivation
Indifference and loss of empathy*
Adverse effects on worker nervous, cardiovascular, metabolic, and immune functioning **
Sources: Sentinel Event Alert 48, Dec 14, 2011; *Hughes 2004; **NIOSH 2009

15
Potential Impact of Fatigue
Increased Rate of Errors
Patient Adverse Events
• Medication errors
• Charting errors
• Transcription
• Medical errors
Worker Adverse Events
• Sharps injuries
• Musculoskeletal injuries
• Decreased physical/emotional well-being
• Decreased personal safety (e.g., motor vehicle accidents)
Organi-zationalEffects
Sources: Rogers et al. 2004; Landrigan et al. 2007; Lockley et al 2007; DHHS (NIOSH) 2009
• Legal issues, injury claims
• Satisfaction
• Staff turnover

16
Alarming Statistics
Risk of error (especially medication errors) increases after 8
hours and is more significant after 12.5 hours
Employee accident rates increase after 9 hours of work and
double after 12 hours of consecutive work
3 Mile Island, Chernobyl, Exxon Valdez: accidents occurred at
night – contributing factor was sleep deprivation

17
Alarming Statistics
Extended work hours per day (>8hrs) = 37% increase in injury
rate
Extended work hours per week (>48hrs)= 23% increase in injury
rate
OT = 61% increase in injury rate
Time of day night nurses struggle to stay awake:
2 a.m. to 4 a.m. and 12 p.m. to 4 p.m.

18
Recommendations for Staff
Eat balanced diet
Exercise to decrease work-dependent fatigue
Report unsafe work conditions
Recognize symptoms of own fatigue
Collaborate with other staff on taking breaks
Practice good sleep hygiene (schedule 7-8 hours of sleep)

19
©2016 Advisory Board • All Rights Reserved •33975D
Source: “The AONE Nurse Executive Competencies,” AONE,
http://www.aone.org/resources/leadership%20tools/nursecomp.shtm;Nursing
Executive Center interviews and analysis.
19

20
Nobility (n.)
The state of being in one’s character, mind,
birthright, rank.
Associated with dignity, goodness and courage.
Adams, JH. The Joy of Nursing. Reclaiming Our Nobility. SteamboatSprings Publishing. 2011.

21
If one is lucky, one solitary fantasy
can totally transform one million
realities.
MAYA ANGELOU
Adams, JH. The Joy of Nursing. Reclaiming Our Nobility. SteamboatSprings Publishing. 2011.

22
Maslow’s Hierarchy of Needs
Maslow, Abraham H. Oxford, England: Viking The farther reaches of human
nature.(1971). xxi 423 pp.

23
Deeply understand work environment challenges for the staff
Be an active listener and problem-solver
Develop initiatives to stimulate sense of meaning and
achievement
Use peer role models to help
Stop “fantasy thinking” about work-life balance
Money alone won’t provide joy & meaning
What Can Leaders Do to Help?

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
24
3 Waves of Innovation in Patient Safety
Technical and procedural improvements have made surgery safer, but future innovations will
focus on reliably organizing the work of patient care.
Ghaferi AA, et al. The Next Wave of Hospital Innovation to Make
Patients Safer. Harvard Business Review. Aug. 8, 2016

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
25
Leadership RPI
Commitment to
Zero Patient
Harm
Safety
Culture
Empowering staff to
speak up
about patient risks
Systematic data-driven
approach to solving
complex problems
High Reliability in Health Care Requires

26
Eight Recommendations for Achieving Total
Systems Safety

27
Eight Recommendations for Achieving Total
Systems Safety

28
ECRI Institute
New Safety Concern 2016
Failure to Embrace a
Culture of Safety
Healthcare organizations must have a culture of
safety that both spans the entire organization and
permeates each department.
Source: Top 10 Patient Safety Concerns for Healthcare
Organizations 2016. ECRI Institute Executive Brief. April 2016.

29
Why Culture Is Important
Culture
The shared values and beliefs of individuals
in a group or organization
CultureShared Values
& Beliefs
Shared Values& Beliefs Our Behaviors
Our Behaviors Outcomes
=

30
11 Tenets of a Safety Culture
Definition of a Safety Culture: Safety Culture is the sum of what an organization is and does in the
pursuit of safety. The Patient Safety Systems (PS) chapter of The Joint Commission accreditation
manuals defines safety culture as the product of individual and group beliefs, values, attitudes,
perceptions, competencies, and patters of behavior that determine the organization’s commitment to
quality and patient safety.
Source: “The essential role of leadership in developing a safety culture,”
The Joint Commission Sentinel Event Alert, Issue 57, March 1, 2017.

31
11 Tenets of a Safety Culture(continued)
Source: “The essential role of leadership in developing a safety culture,”
The Joint Commission Sentinel Event Alert, Issue 57, March 1, 2017.

32
Getting to Zero Harm
“The single greatest impediment to error prevention in the medical
industry is that we punish people for making mistakes.”
- Lucian Leape MD, member of the Quality of Health Care in America Committee
at the Institute of Medicine and adjunct professor of the Harvard School of Public Health

33
A Psychologically Safe Culture:
Interlocking Elements
Learning
culture
Just
culture
Reporting
culture
Source: James Reason

34
Essential Elements:
Culture of “Mindfulness” for Psychological
Safety
An atmosphere of trust in which errors and “near misses” are valuable
lessons
A “just” response to human errors, differentiating intentional from
unintentional
A system that provides for easy, de-identified reporting of unexpected
events and errors, and that gives feedback and learning to those who
report
A learning system that not only shares feedback, but uses the learning to
redesign the operations and challenge the assumptions that underlie the
system itself

35
Safety Culture Maturation
Trust and intimidating
behavior are not assessed
Emphasis is on blame;
inequitable application of
discipline
Root cause analysis is
limited to adverse events
Limited or no efforts to
assess system defenses
against quality failures and
remedy weaknesses
No measures of safety
culture exist
Beginning Approaching
High levels of (measured) trust exist in
all clinical areas
All staff recognize/act on personal
accountability; equitable disciplinary
procedures
System defenses proactively
assessed; weaknesses proactively
repaired
Close calls/unsafe conditions routinely
reported with early problem resolution
Safety culture measures results
routinely reported to the board; system
improvement initiatives under way

36
What Behaviors Are Intimidating?
Wide range: from hanging up the phone instead of answering a
question to verbal abuse (cursing, yelling) or physical abuse
Most common?
Refusal to answer questions or to return phone calls or pages;
condescending tone or language; impatience with questions
Have we improved?
37
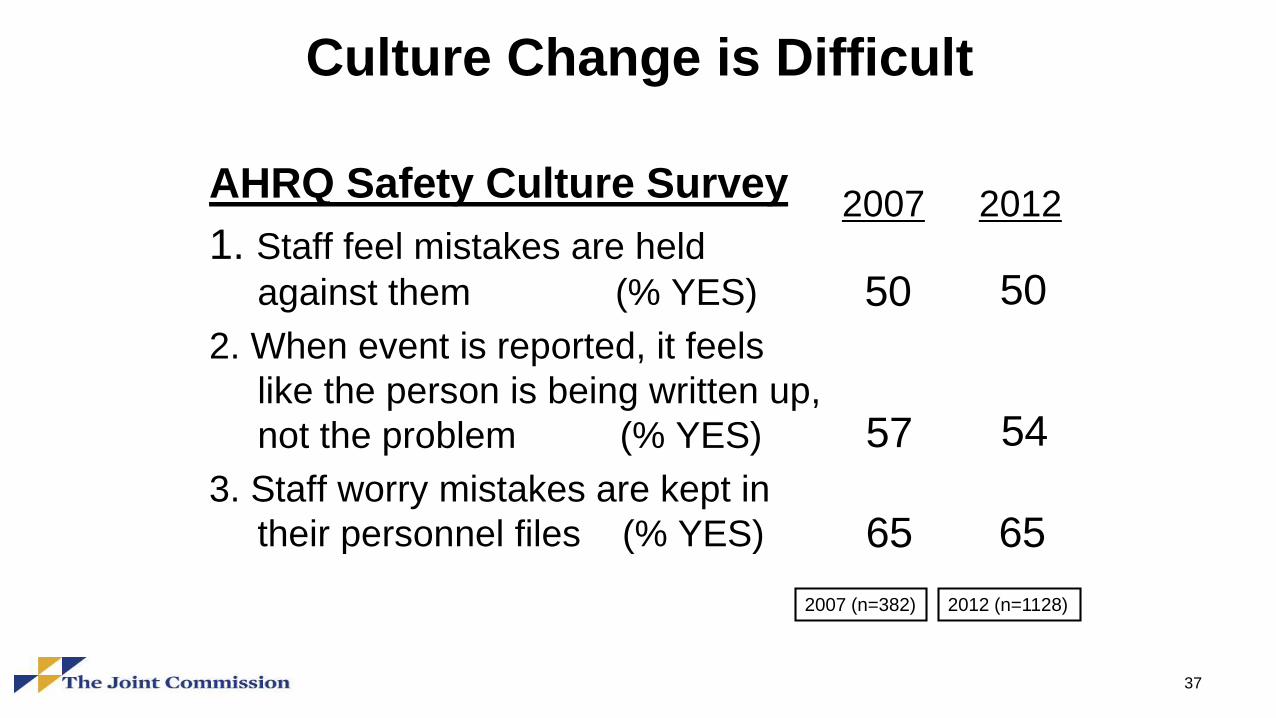
Culture Change is Difficult
AHRQ Safety Culture Survey
1. Staff feel mistakes are held
against them (% YES)
2. When event is reported, it feels
like the person is being written up,
not the problem (% YES)
3. Staff worry mistakes are kept in
their personnel files (% YES)
2007 (n=382) 2012 (n=1128)
2007 2012
50
54
65
50
57
65

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
38
https://www.jointcommission.org/issues/article.aspx?Article=rFhOFvmOhideyaeaXWHwd
F7iIsdGP%2bTcEobEhA7d2RU%3d accessed via internet June 24, 2016

39
Some Barriers To Safety Culture
Blaming
Denial
Silence
Temporary fixes
Trade-offs

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
40
Sometimes the silence gets
so loud, the only thing left
to do is hope your heart is
strong enough to beat it out
Author: Rachel Wolchin
Culture of Silence

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
Drive out fear and create trust
- W. Edward Deming41

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
42
TrustCredibility Reliability Authenticity
Self-Interest
“The Trust Equation”

43
Trust
ReportImprove
Adapted from Reason J., and Hobbs A. 2003. Managing Maintenance Error: A
Practical Guide. Burlington, VT: Ashgate.
Safety Culture

44
What gets rewarded gets repeated
“Recognition”
It’s not a natural skill . . .
It must be taught!
“65% of Americans reported that they received no recognition
for good work in the past year …”
Source: Rath T, Clifton D. How Full Is Your Bucket, 2004.

45
Safety Culture
Principles and Traits
Principle Trait
Everyone is personally - Personal Accountability
responsible for safety
Leaders demonstrate a - Leadership safety values
commitment to safety
Trust permeates the - Effective safety communications
organization - Respectful work environment
- Environment for raising concerns
Decision-making reflects - Decision-making
safety first
Adapted from: Traits of a Healthy Nuclear Safety Culture. INPO 12–012, April 2013.
Copyright © 2012, 2013 by the Institute of Nuclear Power Operations

46
Safety Culture
Principles and Traits(continued)
Principle Trait
Health care technology is - Work processes automated
recognized as special and
unique
A questioning attitude is - Questioning attitude applauded
cultivated
Organizational learning is - Continuous learning
embraced - Problem identification & resolution
Patient Safety undergoes - Continuous learning and fixes
constant evaluation - Problem identification
Adapted from: Traits of a Healthy Nuclear Safety Culture. INPO 12–012, April 2013.
Copyright © 2012, 2013 by the Institute of Nuclear Power Operations

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
47
What Do Healthcare Staff Need for
Psychological Safety?
Respect and engagement
Freedom from harm
– physical
– psychological
Meaningful work
Opportunities to learn
and develop
Source: Lucian Leape Institute Roundtable, National Patient Safety Foundation 2013.
http://www.patientcarelink.org/uploadDocs/1/Through-Eyes-of-the-Workforce_online.pdf

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
48

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
4949
© 2015 Press Ganey Associates, Inc.
Compassionate Connected Care ™ for the CareGiver
An approach to reduce CareGiver suffering…
We should acknowledge the complexity and gravity of the work provided by caregivers
It is the responsibility of management to provide support in the form of material, human, and emotional resources
Teamwork is a vital component for success
Empathy and trust must be fostered and modeled
Caregivers' perception of a positive work/life balance reduces compassion fatigue
Communication at all levels is foundational

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
50
Elements of Psychological Safety in Teams
Trust teammates to support and help each other
Respectful communications
Assume good intentions – no “hidden agendas”
Believe everyone’s goals are aligned
Able to challenge others’ ideas in positive manner
Hold each individual accountable for own actions
Open to learning from mistakes
Fear is absent

51
Role of Hospital Leaders in Building a Culture of
Psychological Safety
Motivate care teams to uphold a fair and just safety culture
Provide a transparent environment in which patient safety
events are honestly reported
Model professional behavior
Remove intimidating behavior that might inhibit a culture of
safety
Provide the resources and training necessary to take on
improvement initiatives

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
52
Where to Start: A Simple Test
Can your staff answer yes to the following three questions?
1. Am I treated with dignity and respect everyday by everyone I work with?
2. Do I have the knowledge, skills, and tools to do my job?
3. Am I recognized and thanked for my contributions?

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
53
Triple Aim: Better Care. Better Health. Lower Cost.
Triple Aim
Consider Quadruple Aim: Meaningful Work

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
54
Quadruple Aim

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
55
Pre-Condition: Joy and Meaning
Respect and engagement
Freedom from harm
– physical
– psychological
Meaningful work
Opportunities to learn
and develop
Source: Lucian Leape Institute Roundtable, National Patient Safety Foundation 2013.
http://www.patientcarelink.org/uploadDocs/1/Through-Eyes-of-the-Workforce_online.pdf

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
56
Strategy 1: Develop and embody shared core values of mutual respect and
civility; transparency and truth telling; safety of all workers and patients; and
alignment and accountability from the boardroom through the front lines
Strategy 2: Adopt the explicit aim to eliminate harm to the workforce and to
patients
Strategy 3: Commit to creating a high-reliability organization (HRO) and
demonstrate the discipline to achieve highly reliable performance. This will
require adopting evidence-based management skills for reliability
What Are the Seven Things
That an Organization Must Do?
“Through the Eyes of the Workforce: Creating Joy, Meaning and Safer
Health Care.” Lucian Leape Institute, National Patient Safety Foundation,
2013; pp. 27-29

© C
opyr
ight, T
he J
oin
t C
om
mis
sio
n
57
Strategy 4: Create a learning and improvement system
Strategy 5: Establish data capture, database, and performance metrics for
accountability and improvement
Strategy 6: Recognize and celebrate the work and accomplishments of
the workforce, regularly and with high visibility
Strategy 7: Support industry-wide research to design and conduct studies
that will explore issues and conditions in health care that are harming our
workforce and our patients
What Are the Seven Things
That an Organization Must Do?
“Through the Eyes of the Workforce: Creating Joy, Meaning and Safer
Health Care.” Lucian Leape Institute, National Patient Safety Foundation,
2013; pp. 27-29

58
References
Adams, JH. The Joy of Nursing. Reclaiming Our Nobility. SteamboatSprings Publishing. 2011.
Albaugh, JA. Resolving the Nursing Shortage: Finding Passion and Joy in Nursing. Urologic Nursing. February 2005, Vol. 25, No. 1.
American Nurses Association. Shiftwork Sleep Disorder: The Role of the Nurse Understanding the Consequences of SWSD For Your and
Your Patients. Toolkit Online, accessed 1/2/13.
Blouin AS, McDonagh KJ. Framework for patient safety, part 1: culture as an imperative. Journal of Nursing Administration. 2011 Oct
1;41(10):397-400.
Blouin AS, McDonagh KJ. A framework for patient safety, part 2: resilience, the next frontier. Journal of Nursing Administration. 2011 Nov
1;41(11):450-2.
Caruso, CC, Hitchcock, EM. Strategies for Nurses to Prevent Sleep Related Injuries and Errors. Rehabilitation Nursing 2010 Sept./Oct.;
35(5):192-197.
Consensus Statement of the Health Enhancement Research Organization, American College of Occupational and Environmental Cancer
Action Network, American Diabetes Association, and American Heart Association. Guidance for a Reasonably Designed, Employer-
Sponsored Wellness Program Using Outcomes-Based Incentives. Journal of Occupational & Environmental Medicine. 54(7):889-896, July
2012.
Dunn, D. What Keeps Nurses in Nursing? International Journal for Human Caring. 2012, Vol. 16, No. 3.
Ellis, JR. Quality of Care, Nurses’ Work Schedule, and Fatigue. Washington State Nurses Association White Paper, 2008.
Horstman, S. When Nurses Bond With Their Patients. The New York Times. September 13, 2013.
https://well.blogs.nytimes.com/2013/09/13/when-nurses-bond-with-their-patients/?_r=0
Hughes RG, Rogers, AE: Are you tired? Sleep deprivation compromises nurses’ health – and jeopardizes patients. American Journal ofNursing, March 2004;104(3)

59
References(continued)
Institute of Medicine: Keeping Patients Safe: Transforming the Work Environment of Nurses. Washington, DC: National Academy Press,2004.
Joint Commission Resources. Strategies for Addressing Health Care Worker Fatigue. Oak Brook IL. 2008
Landrigan CP, et al: Effect of reducing interns’ work hours on serious medical errors in intensive care units. New England Journal ofMedicine, October 28, 2004;351:1838-1848
Landrigan C.P., et al.: Effective implementation of work hour limits and systemic improvements. Jt Comm J Qual Patient Saf. 33(suppl.):19–
29, Nov. 2007.
Lerman SE, Eskin E, Flower DJ, George EC, Gerson B, Hartenbaum N, Hursh SR, Moore-Ede M, ACOEM Presidential Task Force on
Fatigue Risk Management: Fatigue Risk Management in the Workplace Journal of Occupational & Environmental Medicine. 54(2):231-258,
Feb 2012.
Lockley SW, et al: Effect of reducing interns’ weekly work hours on sleep and attentional failures. NEJM October 28, 2004;351:1829-1837
Lockley SW, et al: Effects of health care provider work hours and sleep deprivation on safety and performance. Jt Comm J Qual Patient Saf
November 2007;33(11)7-18, http://www.jointcommission.org/JQPS_11_07/
Lorenz, SG. 12-Hour Shifts: An Ethical Dilemma for One Nurse Executive. JONA 2008: 38(6)297-301.
McVay S, Kautz DD. Finding Joy, Gratitude, and Meaning in Routine PACU Tasks. Journal of PeriAnesthesia Nursing, Vol. 30, No. 2
(April), 2015: pp 160-163.
Middaugh DJ. Can There Really Be Joy at Work? MedSurg Nursing, Vol. 23, No. 2, March-April 2014.
NIOSH [2009]. State of the Sector | Health care and Social Assistance: Identification of Research Opportunities for the Next Decade of
NORA, Cincinnati, OH: US DHHS, Public Health Service, DHHS (NIOSH) Publication Number 2009-139
[http://www.cdc.gov/niosh/docs/2009-139/]
NPSF Lucian Leape Institute. Through the Eyes of the Workforce – Creating Joy, Meaning, and Safer Health Care. 2013.

60
References(continued)
Olds, DM, Clarke, SP. The Effect of Work Hours on Adverse Events and Errors in Health Care. J Safety Res 2010 April; 41(2);153-162.
Reason, J. Human Errors: Models and Management. BMJ 2000; 320:768-770.
Rogers AE, et al: The working hours of hospital staff nurses and patient safety. Health Affairs, 2004; 23(4):202-212
Rothschild JM, et al: Risks of complications by attending physicians after performing nighttime procedures. JAMA October 14,
2009;302:1565-1572
Scott, LD, Arslanian-Engoren, C, Engoren, M. “Association of Sleep and Fatigue With Decision Regret Among Critical Care Nurses.” AJCC
2014 January; 23(1):13-23.
Sikka R, et al. BMJ Qual Saf 2015;0:1-3. doi:10.1136/bmjqs-2015-004160.
Stimpfed, AW, Sloane, DM, Aiken, LH. The Longer the Shifts for Hospital Nurses, the Higher the Levels of Burnout and Patient
Dissatisfaction. Health Affairs 2012 November; 31(11):2501-2509.
The Joint Commission. Improving Patient and Worker Safety: Opportunities for Synergy, Conversation and Innovation. Oakbrook Terrace,
IL: The Joint Commission, November 2012.
The Joint Commission. Sentinel Event Alert. Health care worker fatigue and patient safety. Issue 48, Dec.14, 2011
http://www.jointcommission.org/assets/1/18/SEA_48.pdf
The Joint Commission. Strategies for Addressing Health Care Worker Fatigue. 2008. The Joint Commission: Oakbrook Terrace, IL.
Volpp, KG, et al. Effect of Protected Sleep Period on Hours Slept During Extended Overnight In-Hospital Duty Hours Among Medical Interns.
JAMA 2012; 308(21):2208-2217.
Wojciechowski M. Blog, Health & Wellness, May 9, 2016. http://dailynurse.com/why-i-love-being-a-nurse/. Accessed 1/31/2017.