sebaceous carcinoma of the scalp with rare involvement of ... carcinoma of the scalp with rare...
TRANSCRIPT
Poster Design & Printing by Genigraphics® - 800.790.4001
Sebaceous Carcinoma of the Scalp with Rare Involvement of Nodal Metastasis Brian Lawton, MD1; Songlin Zhang, MD²; Amol Takalkar, MD³; Cherie-Ann Nathan, MD1
1Department of Otolaryngology – Head & Neck Surgery2Department of Pathology ³Department of Radiology
Louisiana State University Health Sciences Center-Shreveport, LA
INTRODUCTION DISCUSSION
PATHOLOGY
Image 2 Image 3
ABSTRACT
Sebaceous Carcinoma of the Scalp with Rare Involvement of Nodal Metastasis
Educational Objective: At the conclusion of this presentation, the participants should be able to:
1) Understand the risk factors of sebaceous carcinoma of the scalp presenting with lymphatic metastasis. 2) Understand the role of PET imaging in these rare tumors.
Objectives: 1) To understand the risk factors of sebaceous carcinoma of the scalp presenting with lymphatic metastasis. 2) To understand the role of PET imaging in these rare tumors.
Study Design: Case Report
Methods: An 83 year old white male presented with a rapidly enlarging 8 cm scalp mass and lymphadenopathy. Biopsy revealed sebaceous carcinoma. CT and PET scans revealed the mass and nodal metastasis. Excision of the lesion with rotational flap closure and postero-lateral neck dissection was performed.
Results: Following excision of the lesion, pathology revealed perineural and lymphovascular invasion and a single occipital lymph node was positive. The patient declined postoperative radiation because of his debilitated condition, but subsequent follow up has not revealed any evidence of disease.
Conclusions: Most sebaceous carcinomas occur in the ocular area, but extraocular sebaceous carcinomas are even rarer. Only seven case studies of sebaceous carcinoma of the scalp have been reported with metastasis to lymphatics noted in one other patient. According to the SEER database for the reported cases of sebaceous carcinoma of the scalp and neck, only 1.7% presented with known regional LN involvement. Of the 7 case reports the only other definite LN met was from a 1cm lesion, suggesting that nodal metastasis is not predictive of size of the primary and PET scans may play a role in this disease.
The tumor measured 4.5 x 3.5 x 1.7cm. Tumor cells were positive for high-molecular weight cytokeratin, negative for S-100, CEA, P63, and BEREPP4. Immunohistochemical stains were positive for EMA and BEREP4, focally positive for CK7, and negative for CK20, TTF-1, CEA and S100 on the original incisional biopsy.
H&E staining at 40x revealed nests and sheets of tumor cells with infiltrative growth pattern and focal necrosis (image 4). At 200x the tumor cells have abundant cytoplasm and cytoplasmic lipid vacuoles, prominent nucleoli and visible mitoses (image 5).
Sebaceous carcinomas are rare malignant neoplasms which develop from sebaceous glands and may occur wherever these glands are found. The most common clinical presentation is a painless subcutaneous nodule, but other presentations may include diffuse skin thickening, pedunculated lesions, or an irregular mass. Its’ clinical appearance may mimic common benign lesions and misdiagnosis is common. Histologically four patterns have been reported: lobular, comedocarcinoma, papillary, and mixed. Treatment typically involves wide local excision (1cm margins) with lymphadenectomy for treatment of regional metastasis. Radiation therapy is controversial but should be considered in cases of aggressive disease, but data is limited advocating its use as adjuvant or primary treatment. The SEER database indicates that patients with sebaceous carcinoma have an age-matched overall survival of 91.9% at five years and 79.2% at 10 years. The median age at diagnosis was 73 years.
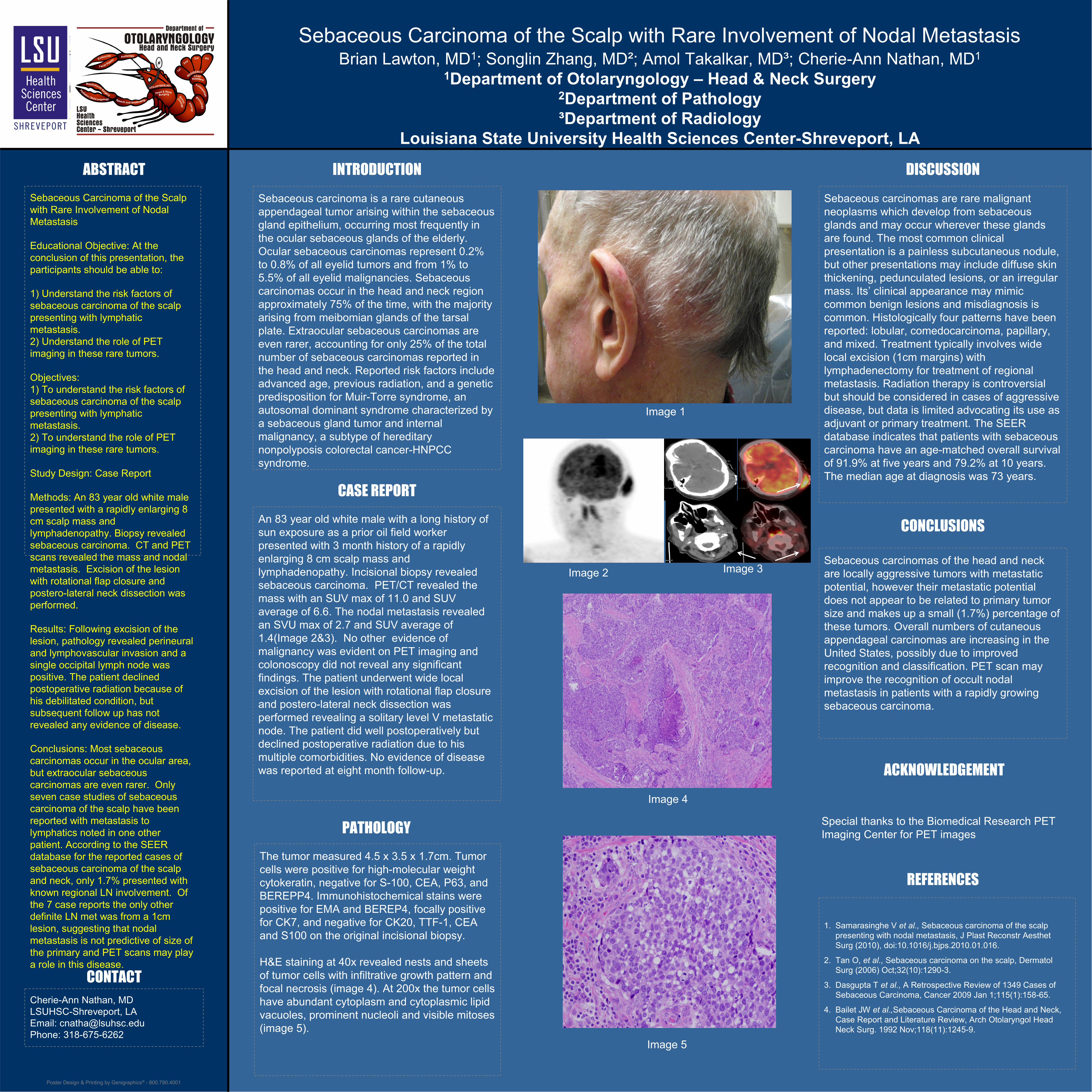
An 83 year old white male with a long history of sun exposure as a prior oil field worker presented with 3 month history of a rapidly enlarging 8 cm scalp mass and lymphadenopathy. Incisional biopsy revealed sebaceous carcinoma. PET/CT revealed the mass with an SUV max of 11.0 and SUV average of 6.6. The nodal metastasis revealed an SVU max of 2.7 and SUV average of 1.4(Image 2&3). No other evidence of malignancy was evident on PET imaging and colonoscopy did not reveal any significant findings. The patient underwent wide local excision of the lesion with rotational flap closure and postero-lateral neck dissection was performed revealing a solitary level V metastatic node. The patient did well postoperatively but declined postoperative radiation due to his multiple comorbidities. No evidence of disease was reported at eight month follow-up.
Sebaceous carcinomas of the head and neck are locally aggressive tumors with metastatic potential, however their metastatic potential does not appear to be related to primary tumor size and makes up a small (1.7%) percentage of these tumors. Overall numbers of cutaneous appendageal carcinomas are increasing in the United States, possibly due to improved recognition and classification. PET scan may improve the recognition of occult nodal metastasis in patients with a rapidly growing sebaceous carcinoma.
Sebaceous carcinoma is a rare cutaneous appendageal tumor arising within the sebaceous gland epithelium, occurring most frequently in the ocular sebaceous glands of the elderly. Ocular sebaceous carcinomas represent 0.2% to 0.8% of all eyelid tumors and from 1% to 5.5% of all eyelid malignancies. Sebaceous carcinomas occur in the head and neck region approximately 75% of the time, with the majority arising from meibomian glands of the tarsal plate. Extraocular sebaceous carcinomas are even rarer, accounting for only 25% of the total number of sebaceous carcinomas reported in the head and neck. Reported risk factors include advanced age, previous radiation, and a genetic predisposition for Muir-Torre syndrome, an autosomal dominant syndrome characterized by a sebaceous gland tumor and internal malignancy, a subtype of hereditary nonpolyposis colorectal cancer-HNPCC syndrome.
CASE REPORT
1. Samarasinghe V et al., Sebaceous carcinoma of the scalp presenting with nodal metastasis, J Plast Reconstr Aesthet Surg (2010), doi:10.1016/j.bjps.2010.01.016.
2. Tan O, et al., Sebaceous carcinoma on the scalp, Dermatol Surg (2006) Oct;32(10):1290-3.
3. Dasgupta T et al., A Retrospective Review of 1349 Cases of Sebaceous Carcinoma, Cancer 2009 Jan 1;115(1):158-65.
4. Bailet JW et al.,Sebaceous Carcinoma of the Head and Neck, Case Report and Literature Review, Arch Otolaryngol Head Neck Surg. 1992 Nov;118(11):1245-9.
CONCLUSIONS
REFERENCES
Cherie-Ann Nathan, MDLSUHSC-Shreveport, LAEmail: [email protected]: 318-675-6262
CONTACT
REPLACE THIS BOX WITH YOUR
ORGANIZATION’SHIGH RESOLUTION
LOGO
Image 4
Image 5
Image 1
Special thanks to the Biomedical Research PET Imaging Center for PET images
ACKNOWLEDGEMENT