sedation practices in icu
TRANSCRIPT
SEDATION PRACTICES IN ICU
Dr. Abhijit S. NairConsultant Anesthesiologist
CITIZENS HOSPITALSHyderabad
Scope of the class:
Sedation scores Problems of sedation To evolve a sedation protocol Emphasize on documentation
What I won’t discuss?
Pharmacology of drugs Dosing Preparation/ storage etc
Why sedate?

Why sedate?
Tube tolerance Ventilator synchronization Reduce agitation ( withdrawal etc) Pain relief Facilitate interventions
Problems of inadequate sedation
Sleep deprivation Increased stress Increased inflammatory mediators
Over-sedation
Vs Under-sedation
Oversedation
Prolongs ICU stay Prolongs weaning Risk factor for delirium ( BZDs ) ?CIPN Hemodynamic disturbances
Undersedation:
hyper-catabolism immunosuppression Hyper-coagulability increased sympathetic activity Accidental extubation Hyperglycemia PTSD
Consales G, Chelazzi C, Rinaldi S, De Gaudio A R. Bispectral index compared to Ramsay score for sedation monitoring in intensive care units. Minerva Anestesiol 2006; 72: 329–36
Non-pharmacological sedation
Counselling ( family, primary, nursing staff )
Psychologist Psychiatrist Music Feeding Adequate hydration
NOT FOR VENTILATED PATIENTS
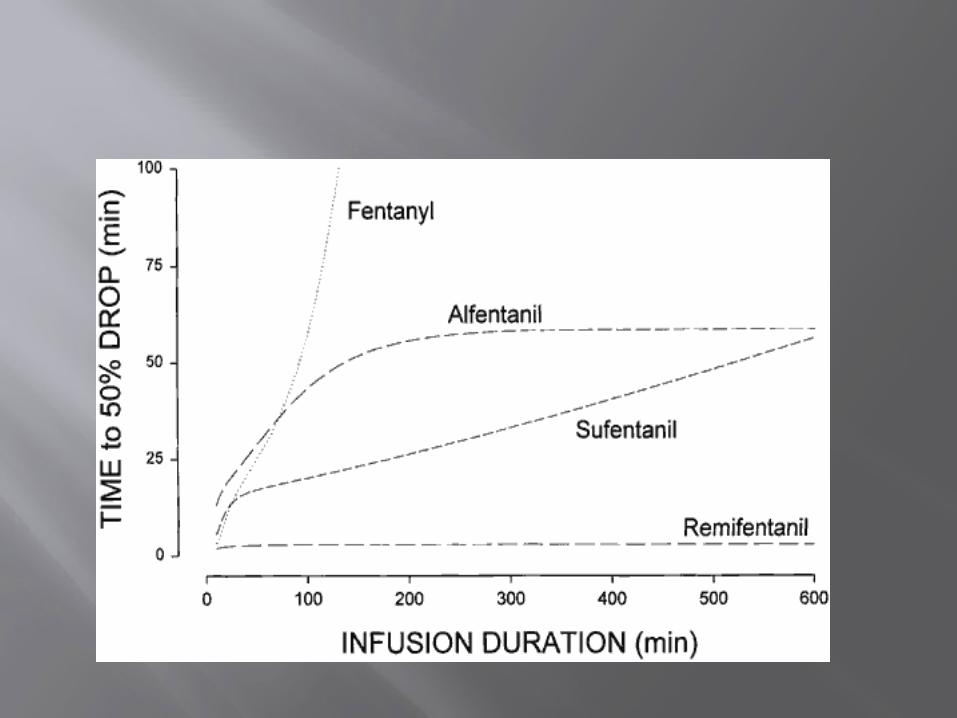
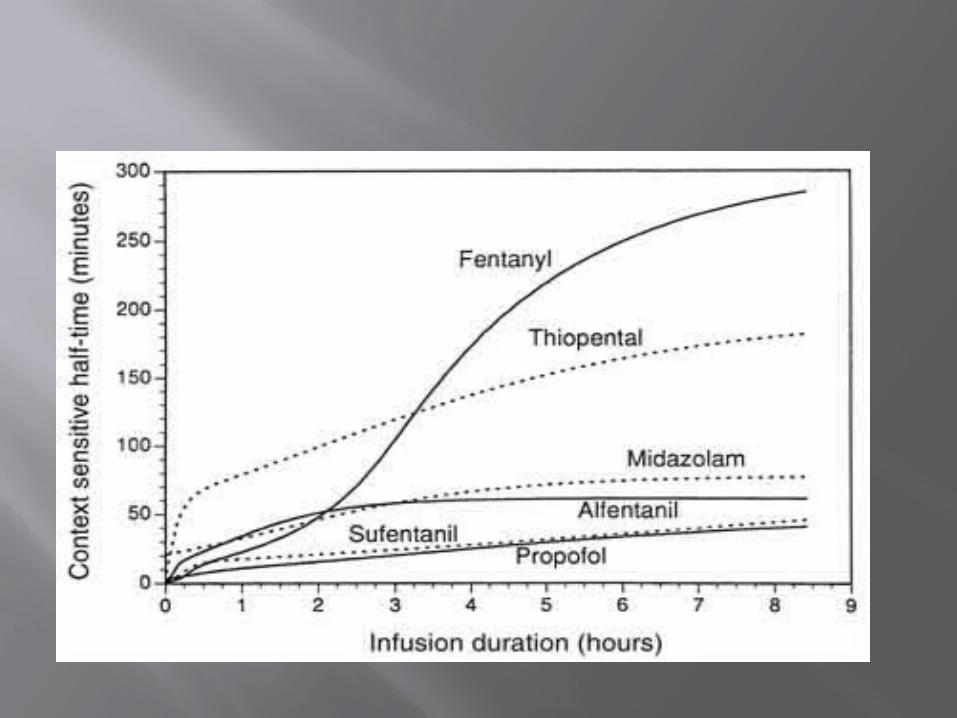
Ideal sedative: Short acting ( plasma t 1/2 & context
sensitivity ) Amnesia Analgesia Less accumulation in peripheral tissues Hemodynamically stable No withdrawal effects No respiratory depression Bronchodilator CHEAP
SEDATIVES
Narcotics Benzodiazepines Miscellaneous
Unwanted side-effects of opioids
Respiratorydepression
ConfusionVasodilation
Gut motilitydepression
Opioids
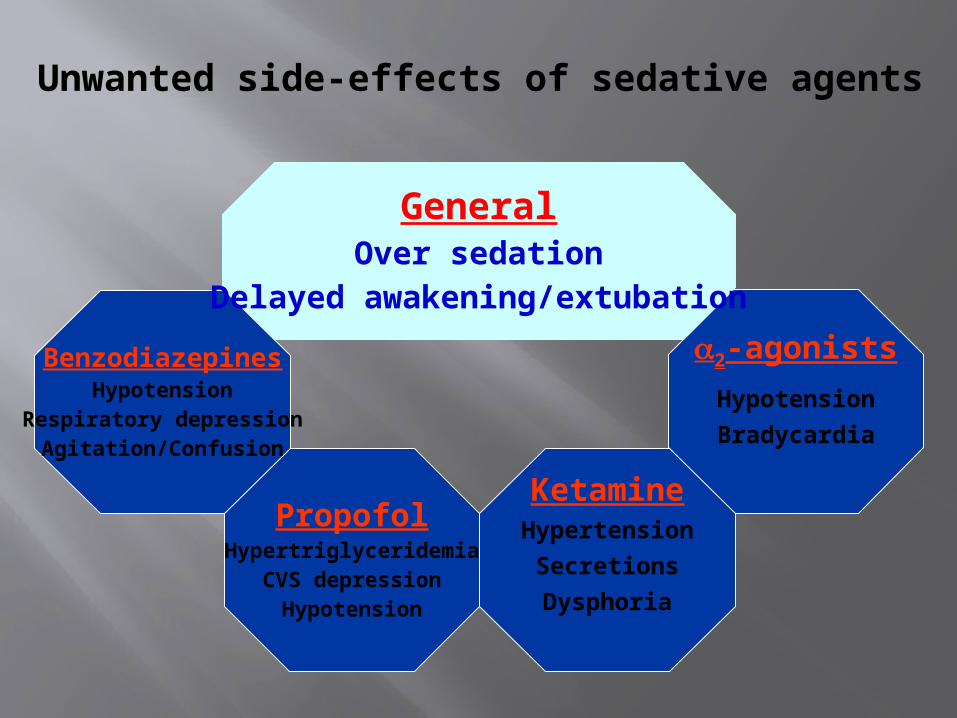
Unwanted side-effects of sedative agents
PropofolHypertriglyceridemia
CVS depressionHypotension
2-agonists
Hypotension
Bradycardia
BenzodiazepinesHypotension
Respiratory depressionAgitation/Confusion
KetamineHypertension
Secretions
Dysphoria
GeneralOver sedation
Delayed awakening/extubation
“the inability to communicate verbally does not negate the possibility that an individual is experiencing pain and is in need of appropriate pain-relieving treatment”
Painful situations:
Suctioning Positioning/ bed making Procedures ( including removals )
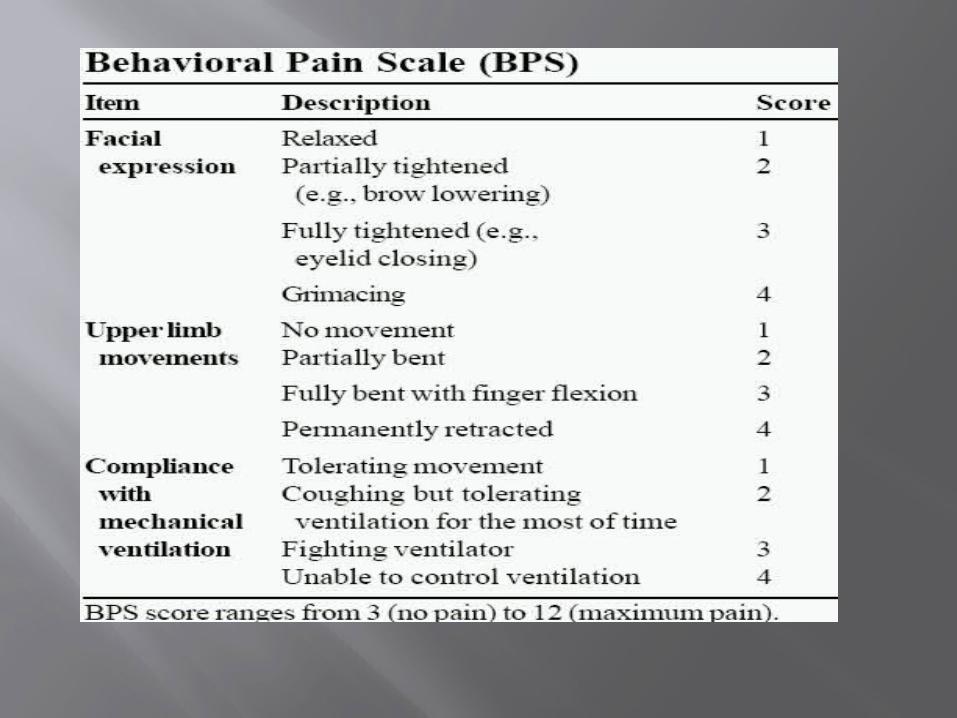
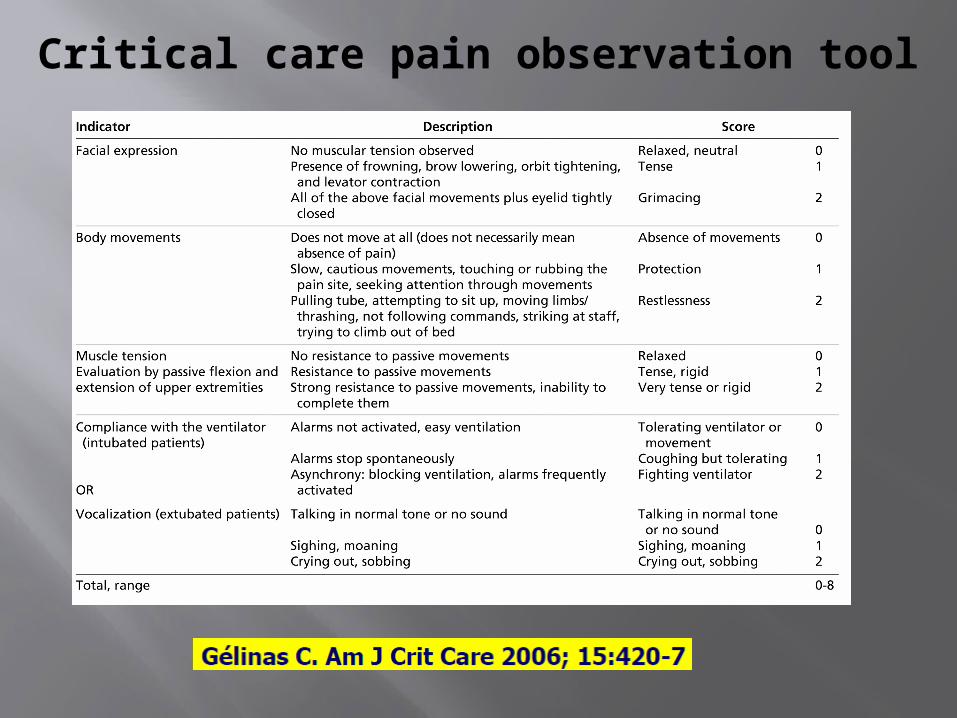
Critical care pain observation tool

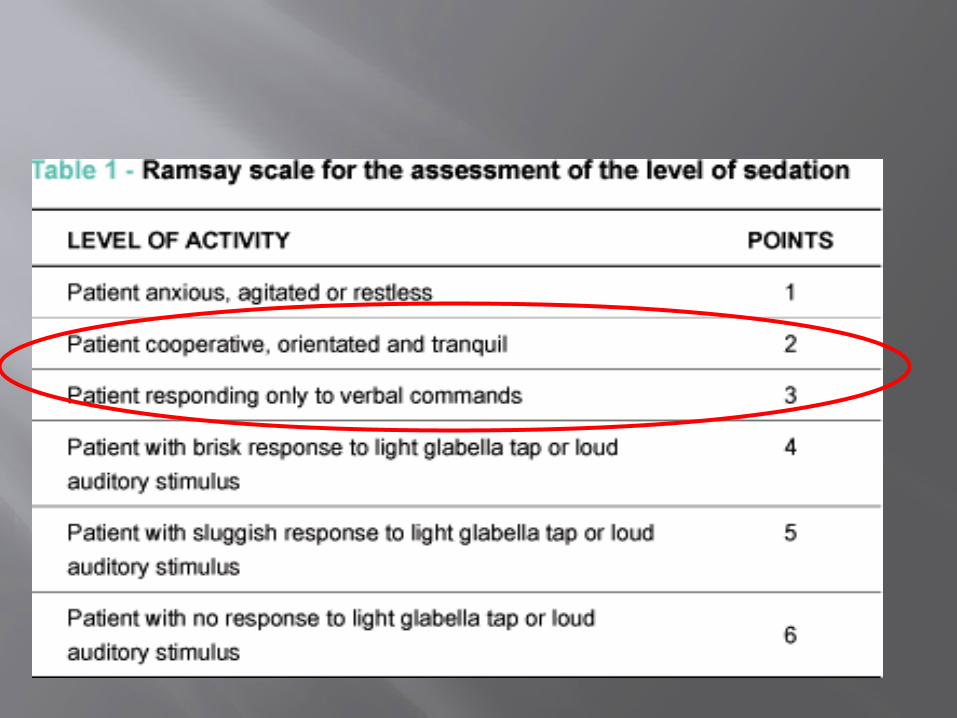
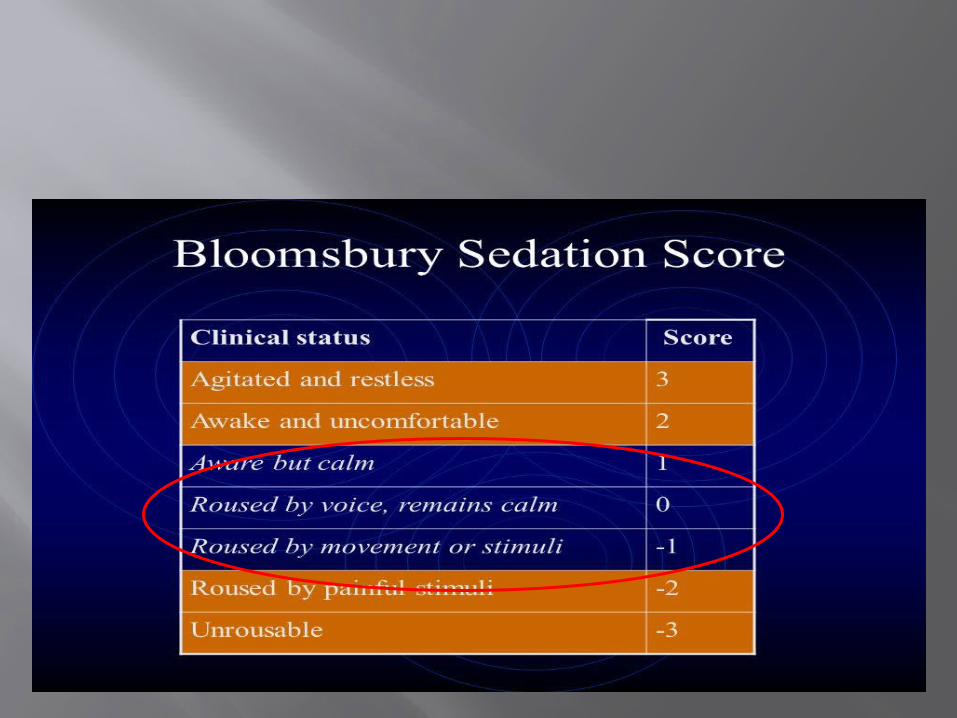
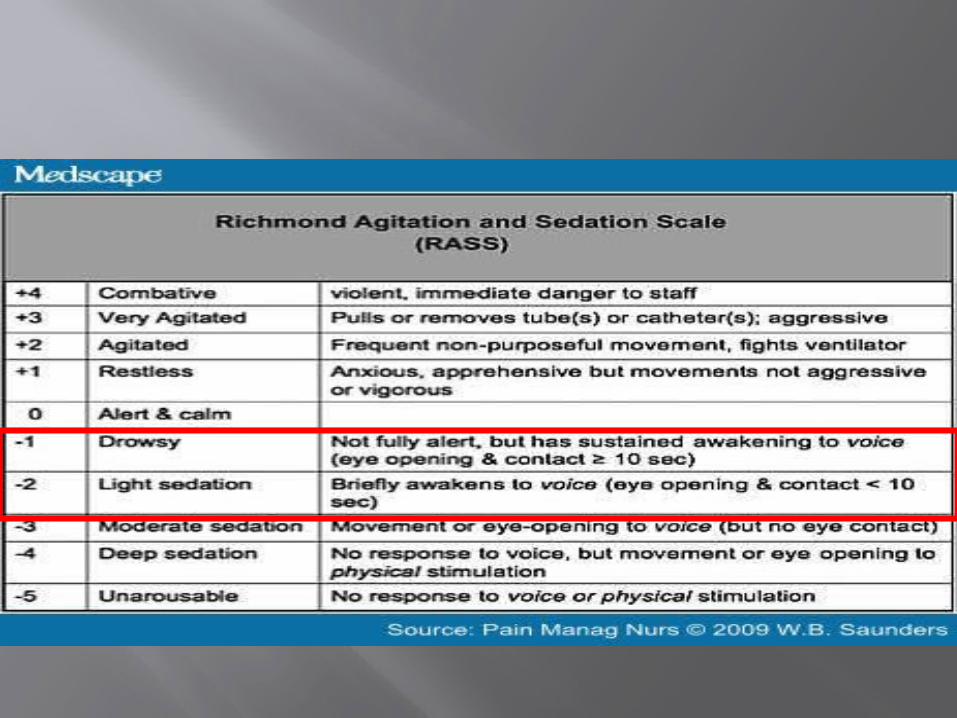
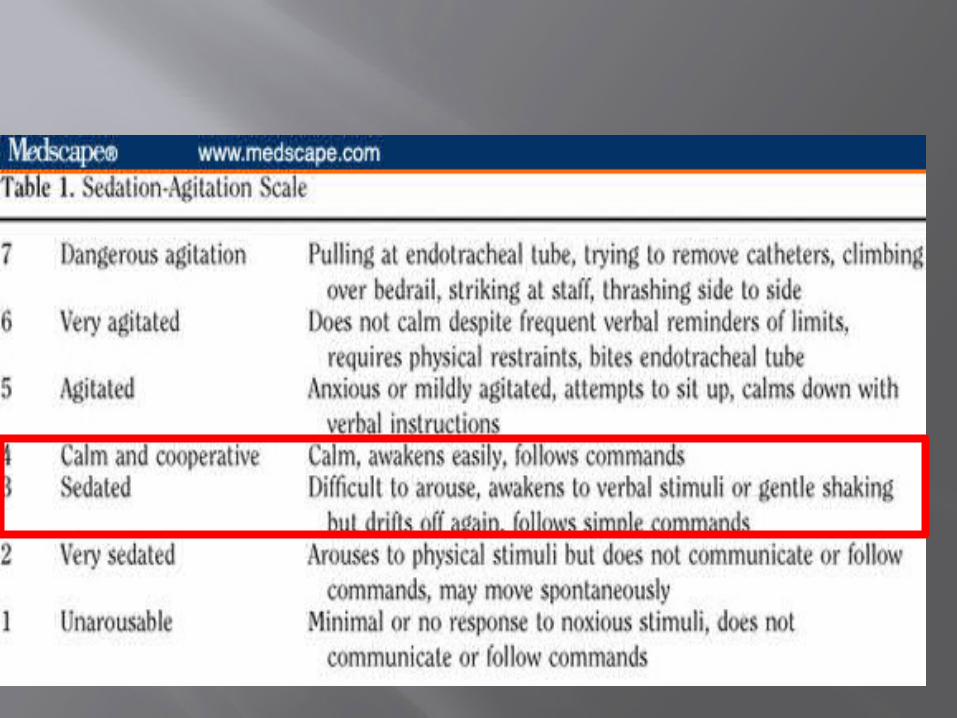
Sedation scores
Ramsay sedation score Bloomsbury sedation score RASS Sedation Agitation Scale
Which scoring system to use?
RAAS & SAS >>> Most valid and reliable sedation assessment tool in adult ICU
Monitoring of brain function( Non-comatose patients )
Auditory evoked potential BIS Narcotrend Index Patient State index State Entropy Scoring scales
Not recommended by SCCM
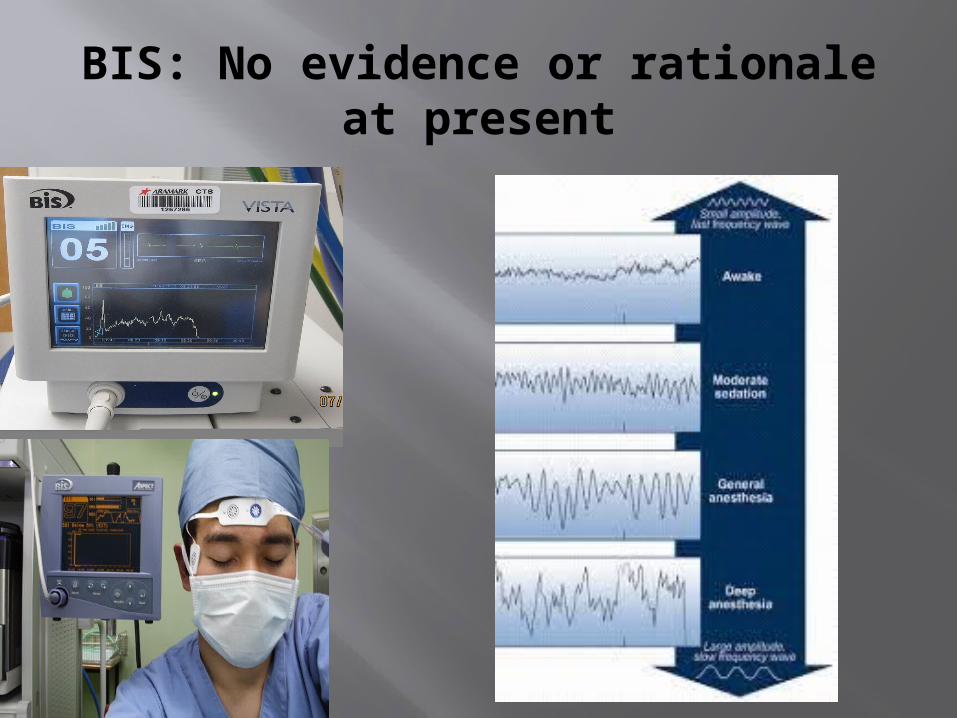
BIS: No evidence or rationale at present
Brain function monitoring not recommended for non- comatose, non-paralysed patients
Brain function monitoring recommended along with sedation scores in patients who are paralysed in ICU
EEG monitoring recommended in patients with non-convulsive seizure activity, suspected seizure activity
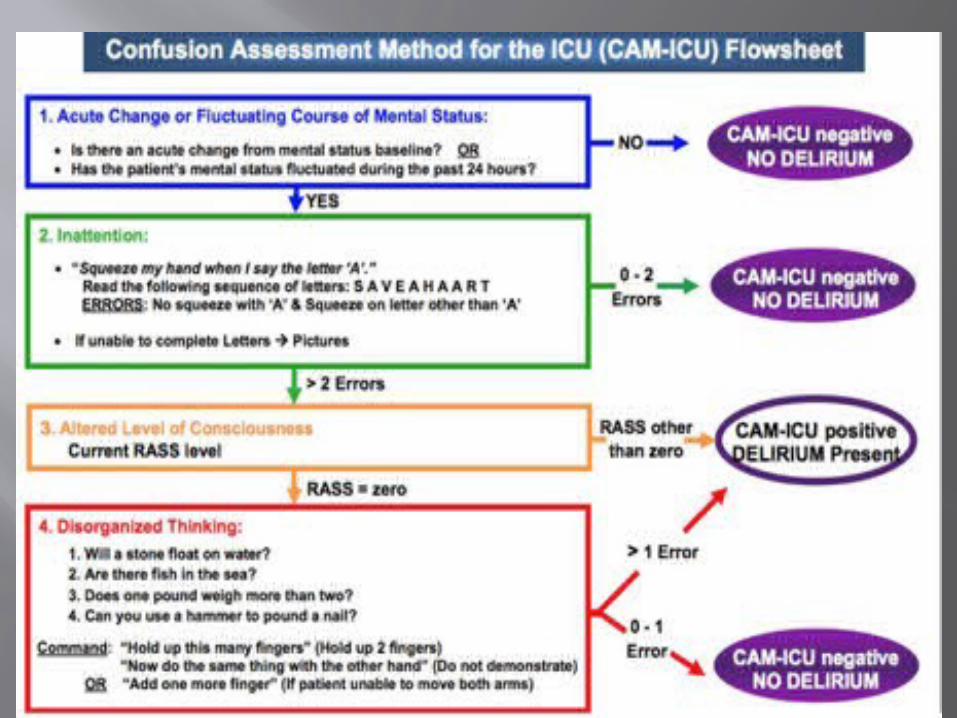
ICU delirium
Syndrome characterized by the acute onset of cerebral dysfunction with a change or fluctuation in baseline mental status, inattention, and either disorganized thinking or an altered level of consciousness
Up to 80 % adults on ventilator experience delirium
Costly affair
Gupta N, de Jonghe J, Schieveld J, et al: Delirium phenomenology: What can we learn from the symptoms of delirium? J Psychosom Res 2008; 65:215–222
Delirium
Prolonged ICU stay Prolonged sedation Benzodiazepines Alcoholics, Chronic smokers Elderly Organ dysfunction
Delirium ct.
Acutely fluctuating mental status Inattention Disorganized thinking Altered mentation With/ without agitation
DELIRIUM Hyperactive
Hypoactive
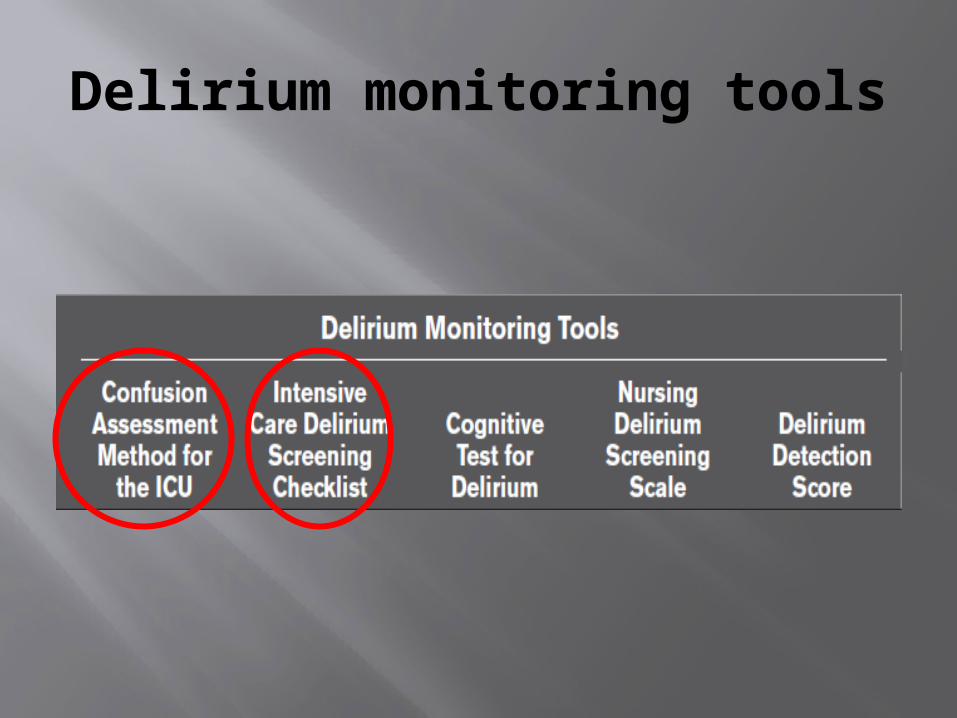
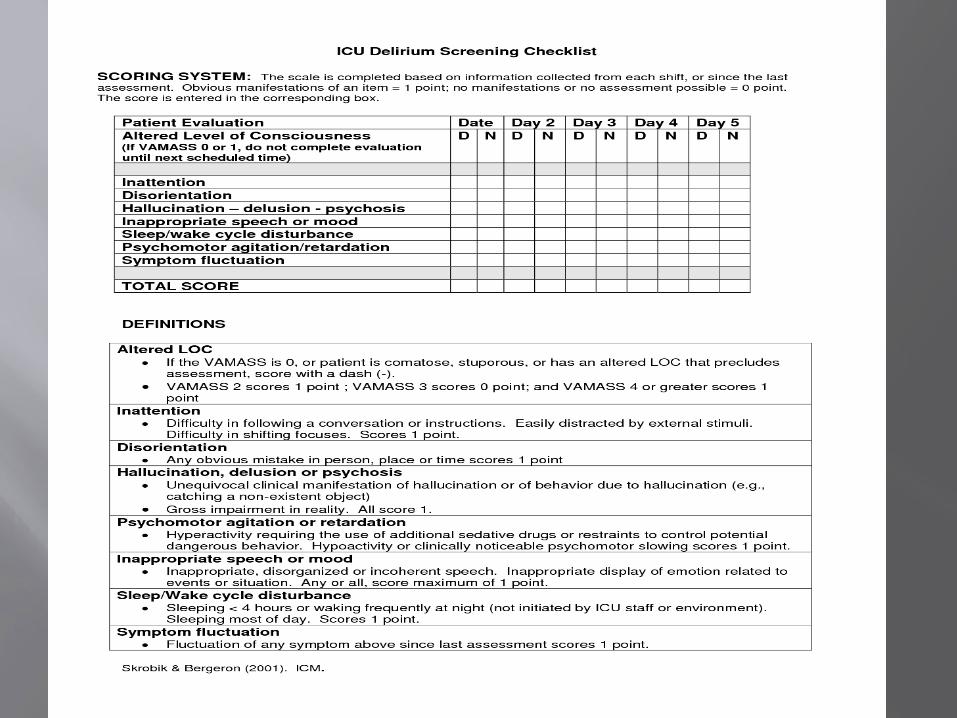
Delirium monitoring tools
Management
Neuroleptic agents ( No evidence ) α 2 agonists ( limited evidence ) Treat the cause SCCM doesn’t support or recommend
use of prophylactic methods to prevent ICU delirium ( No evidence )
Early mobilization is the only proven way to prevent ICU delirium
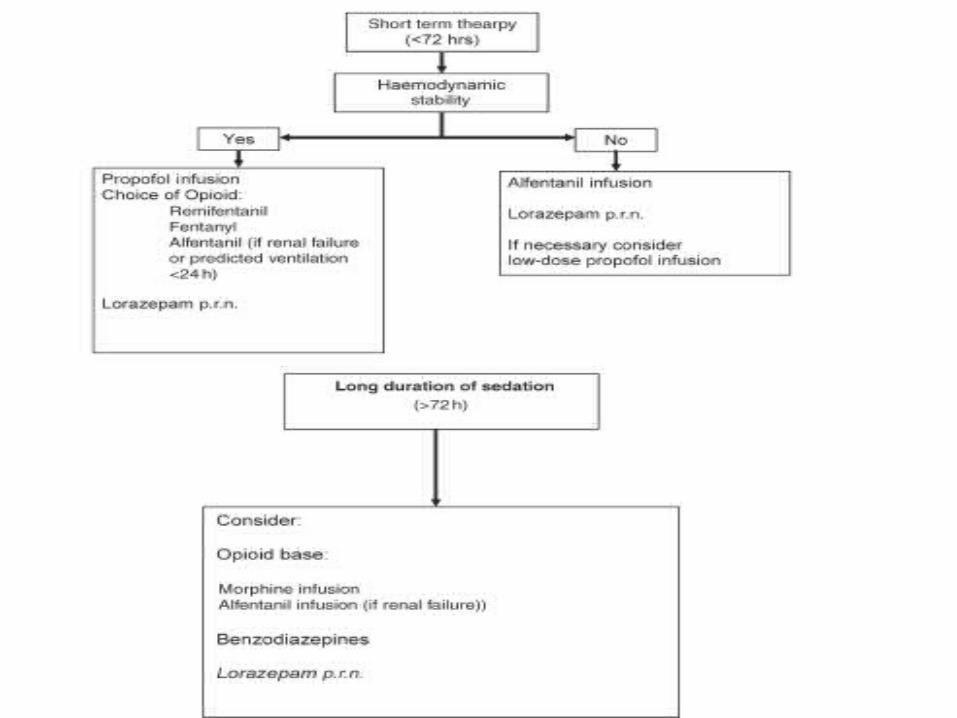
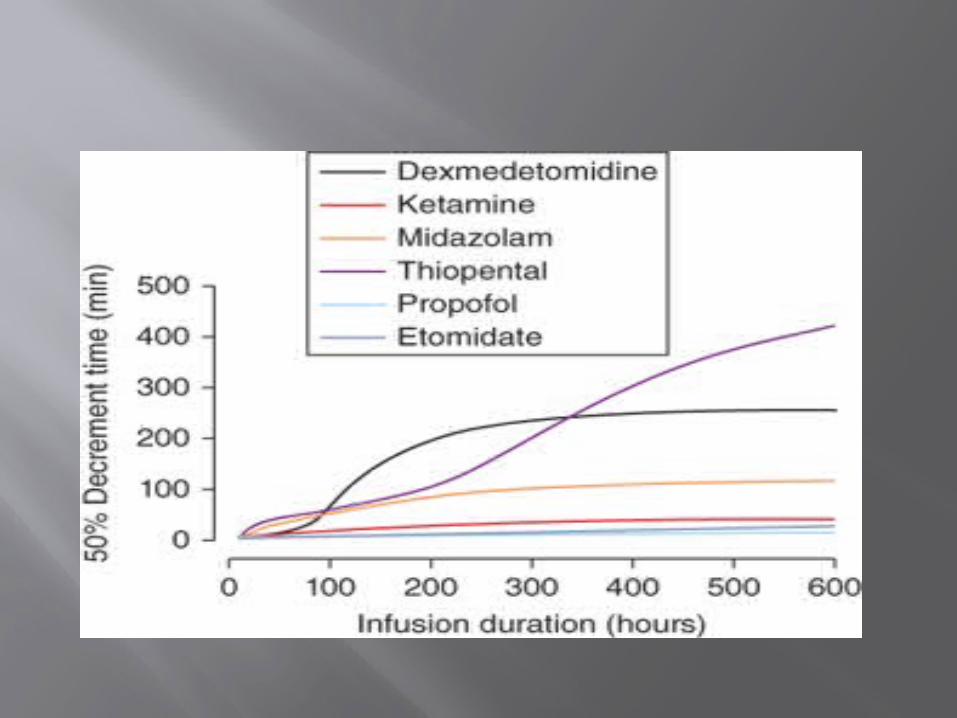
What to use? Propofol / Dexmedetomidine : Short duration
sedation( 24-48 hours ) Fentanyl ( long duration, > 48 hours ) Avoid BZD infusion SEDATION HOLIDAY

Sedation holiday
Interruption of sedation ( preferably daily )
Assess neurological status Restart after assessment or if
agitation increased Shown to reduce duration of
ventilation & ICU stay
Kress JP, Pohlman AS, O’Conner MF, et al. Daily interruption of sedation infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med 2000; 342: 1471–7
PIS
> 48 hours ? High dose metabolic acidosis, rhabdomyolysis Arrhythmias myocardial & renal failure hepatomegaly Death
What usually happens?
Pain/ sedation assessment infrequently done
Implementation of recommendations not possible ( although discussed )
No documentation of scores Scores not addressed?? Sedation Holiday is practiced most of
the times
Take home message
Protocol for addressing Pain, Agitation, Delirium in ICU
Monitor Pain, Agitation & Delirium ( Scoring systems )
Document SCORES
Ct.
Use non-benzodiazepine sedative Light level of sedation is associated with
improved clinical outcomes Adequate analgesia for procedures Review medications daily
Ct.
Sedation Holiday Early mobilization Brain function monitoring recommended
if NDMR used Brain function monitoring not
recommended in non-comatose patients CONDUCIVE ENVIRONMENT IN ICU