segmental absence of intestinal musculature concerning a ... · segmental absence of intestinal...
TRANSCRIPT
Contents lists available at ScienceDirect
J Ped Surg Case Reports 3 (2015) 207e210
Journal of Pediatric Surgery CASE REPORTS
journal homepage: www.jpscasereports .com
Segmental absence of intestinal musculature concerning a child withacute appendicitis
Stéfanie Pereira a,*, Francisco Tortosa b, Miroslava Gonçalves a
a Pediatric Surgery, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Avenida Professor Egas Moniz, 1649-035 Lisboa, Portugalb Pathology, Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, Avenida Professor Egas Moniz, 1649-035 Lisboa, Portugal
a r t i c l e i n f o
Article history:Received 11 December 2014Received in revised form19 February 2015Accepted 20 February 2015
Key words:Segmental absence of intestinal musculatureAcute appendicitisIntestinal perforationIntestinal obstruction
* Corresponding author. Tel.: þ351968135062.E-mail address: [email protected] (S. Pereira)
2213-5766/� 2015 The Authors. Published by Elsevier Inhttp://dx.doi.org/10.1016/j.epsc.2015.02.009
a b s t r a c t
Segmental absence of intestinal musculature (SAIM) is a rare histopathologic entity with few describedcases, most of which in neonates. Rare reports of pediatric cases have been made. Pathogenesis is stilluncertain. This report aims to highlight a pathologic condition that substantially affects the clinicalevolution of an abdominal post-operative state as well as the therapeutic approach. We present the caseof a 4-year old child, previously healthy, with a 4-day long intestinal obstruction. The exploratory lap-arotomy demonstrated peritonitis from a necrosed and perforated acute appendicitis. Post-operatoryintestinal perforation led to a second laparotomy, with resection of a perforated ileal segment and onewith vascular compromise. Pathologic analysis showed segmental absence of intestinal musculature ofthe small bowel. On a third operative time, resection of the macroscopically injured bowel segments andhigh protective enterostomy were made. A three years follow-up shows a healthy, well-developed child,who has already undergone enterostomy closure with no intercurrences. Etiology remains to be defined,possibly related to congenital or ischemic acquired defects. It usually manifests in neonates, but wepresent a case of a 4-year old child. Treatment consists of resection of the injured bowel segments.� 2015 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND
license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
The segmental absence of intestinal musculature (SAIM) is ahistopathological entity, underdiagnosed, most often only recog-nized through a strong clinical suspicion.
Although the first case was described in 1943 by Herbut [1], theetiology remains unclear.
Usually, this entity manifests in the neonatal period, through anocclusion or intestinal perforation.
The purpose of this article is to highlight the histological ex-amination which made the diagnosis in a child with no relevantpersonal history to the pathogenesis of segmental absence of in-testinal muscularis propria.
1. Case report
Male child, 4 years old, 16 kg, with no known relevantpast personal or familiar history (neonatal period with nointercurrences).
.
c. This is an open access article unde
The patient was brought to the pediatric emergency room (ER)following a 48-h period characterized by abdominal pain andvomiting. He was discharged with a diagnosis of acute gastroen-teritis. The persistence and exacerbation of the clinical picture, withthe onset of fever and presence of liquid stool, led the child back tothe ER 48 h later.
Upon arrival the patient was prostrated and was found to have adistended, timpanized and tender abdomen with no signs of peri-toneal irritation. He was hospitalized for symptomatic treatment fora suspected bowel sub-occlusion. Standing abdominal x-rayrevealed a distended bowel with presence of fluid levels, abdominalultrasound showed a small amount of free fluid and marked intes-tinal distension, blood analysis revealed leukocitosis (10.090 U/L;80% neutrophils) and an elevated c-reactive protein of 25.9 mg/dL.
The poor clinical evolution, in spite of the treatment, led to thediagnostic suspicion of acute appendicitis. As such, the patient wastaken to the operating room for an exploratory laparotomy. Intra-operatively, abundant intra-peritoneal non-clear liquid was found,as well as a clearly necrotized appendix, with apparently normalsmall intestine and colon. Pathology confirmed the diagnosis ofacute and necrotic appendicitis.
r the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
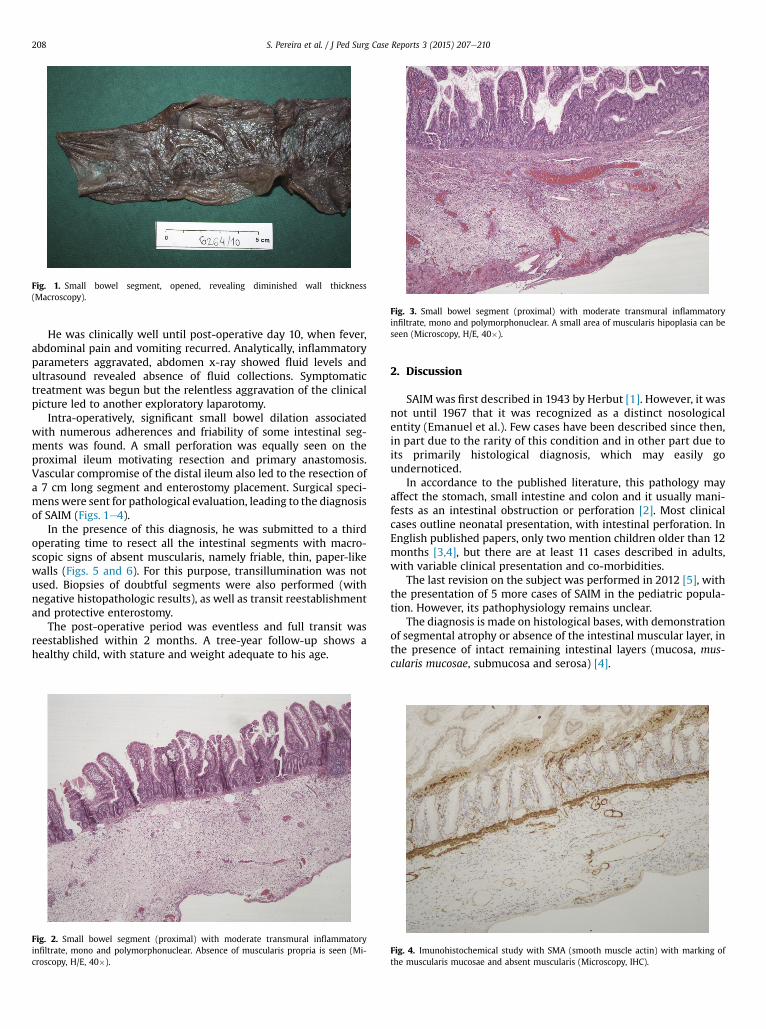
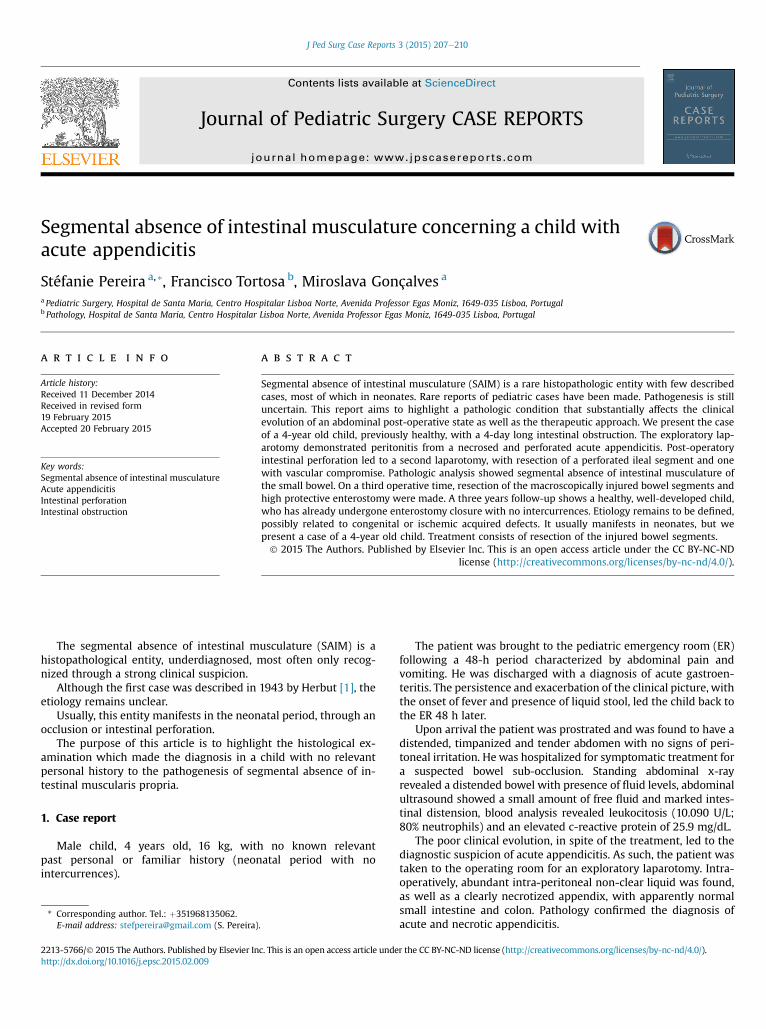
Fig. 1. Small bowel segment, opened, revealing diminished wall thickness(Macroscopy).
Fig. 3. Small bowel segment (proximal) with moderate transmural inflammatoryinfiltrate, mono and polymorphonuclear. A small area of muscularis hipoplasia can beseen (Microscopy, H/E, 40�).
S. Pereira et al. / J Ped Surg Case Reports 3 (2015) 207e210208
He was clinically well until post-operative day 10, when fever,abdominal pain and vomiting recurred. Analytically, inflammatoryparameters aggravated, abdomen x-ray showed fluid levels andultrasound revealed absence of fluid collections. Symptomatictreatment was begun but the relentless aggravation of the clinicalpicture led to another exploratory laparotomy.
Intra-operatively, significant small bowel dilation associatedwith numerous adherences and friability of some intestinal seg-ments was found. A small perforation was equally seen on theproximal ileum motivating resection and primary anastomosis.Vascular compromise of the distal ileum also led to the resection ofa 7 cm long segment and enterostomy placement. Surgical speci-menswere sent for pathological evaluation, leading to the diagnosisof SAIM (Figs. 1e4).
In the presence of this diagnosis, he was submitted to a thirdoperating time to resect all the intestinal segments with macro-scopic signs of absent muscularis, namely friable, thin, paper-likewalls (Figs. 5 and 6). For this purpose, transillumination was notused. Biopsies of doubtful segments were also performed (withnegative histopathologic results), as well as transit reestablishmentand protective enterostomy.
The post-operative period was eventless and full transit wasreestablished within 2 months. A tree-year follow-up shows ahealthy child, with stature and weight adequate to his age.
Fig. 2. Small bowel segment (proximal) with moderate transmural inflammatoryinfiltrate, mono and polymorphonuclear. Absence of muscularis propria is seen (Mi-croscopy, H/E, 40�).
2. Discussion
SAIMwas first described in 1943 by Herbut [1]. However, it wasnot until 1967 that it was recognized as a distinct nosologicalentity (Emanuel et al.). Few cases have been described since then,in part due to the rarity of this condition and in other part due toits primarily histological diagnosis, which may easily goundernoticed.
In accordance to the published literature, this pathology mayaffect the stomach, small intestine and colon and it usually mani-fests as an intestinal obstruction or perforation [2]. Most clinicalcases outline neonatal presentation, with intestinal perforation. InEnglish published papers, only two mention children older than 12months [3,4], but there are at least 11 cases described in adults,with variable clinical presentation and co-morbidities.
The last revision on the subject was performed in 2012 [5], withthe presentation of 5 more cases of SAIM in the pediatric popula-tion. However, its pathophysiology remains unclear.
The diagnosis is made on histological bases, with demonstrationof segmental atrophy or absence of the intestinal muscular layer, inthe presence of intact remaining intestinal layers (mucosa, mus-cularis mucosae, submucosa and serosa) [4].
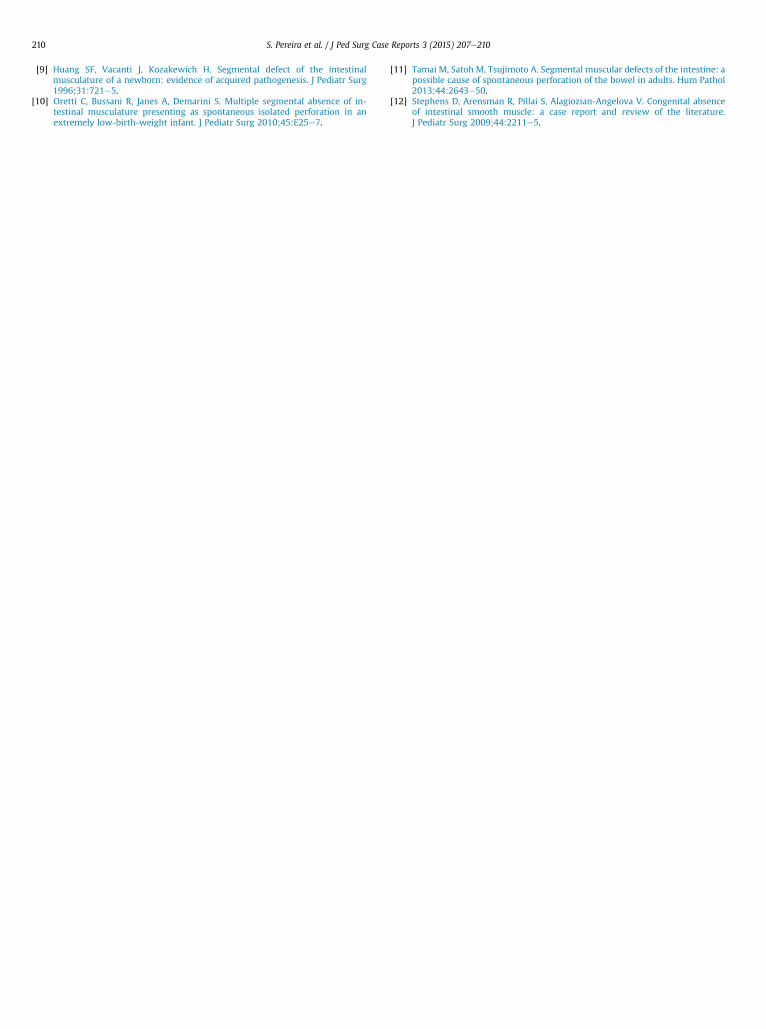
Fig. 4. Imunohistochemical study with SMA (smooth muscle actin) with marking ofthe muscularis mucosae and absent muscularis (Microscopy, IHC).

Fig. 5. Small bowel segment with thin/paper-like walls (Macroscopy).
S. Pereira et al. / J Ped Surg Case Reports 3 (2015) 207e210 209
Other less frequent histopathologic features have beendescribed and are today believed to be part of a larger histopath-ologic spectrum, which may in turn contribute to clarify the etio-pathology of SAIM. Those range from absence of fibrosis [6,7], toconstant presence [7,8] or absence of mioenteric plexuses [9e11];and absence of hemosiderin deposits [9]. Less frequently, thepresence of inflammatory infiltrate adjacent to the areas ofmuscular absence can be observed [9,12], as well as fibrosis in theareas with no muscle [9,10]; and underdeveloped vascular network[10]. Another particularity is the pathology’s primary restriction tothe medial circular muscular layer.
The treatment of this controversial entity gathers moreconsensus between the medical community than its etiopathology,and consists in segmental resection of the affected areas [7,8], withgood prognosis if the resection is performed in a timely manner.
Fig. 6. Small bowel segment with thin/paper-like walls (Macroscopy).
In our patient the macroscopic study of the resected intestinalsegments showedwall atrophy, with paper-like consistence, similarto the findings of other published cases [10,11]. Based on suchfindings, some authors defend close verification of every intestinalsegment presenting with less consistence and almost translucentcolor. Intra-operative use of transillumination is therefore recom-mended [5]. Microscopic analysis demonstrated transmural mod-erate to intense inflammatory infiltrate, with mono andpolymorphonuclear prominence, along with segmental absence ofintestinal musculature. An area of muscular hypoplasia was alsoidentified. Immunochemical study with smooth muscle actinrevealed positive staining in the muscularis mucosae with nostaining in the muscular layer, which is consistent to findings inpublished literature. No mioenteric plexuses or hemosiderin de-posits were identified in the affected intestinal segments.
Those histological findings can follow a recent ischemic insultfrom a long lasting, complicated appendicitis or a congenital defectwith delayed manifestation triggered by an acute illness. A similarcase has been described in an adult with acute appendicitis, exceptthat it had less than 24 h of evolution and the patient had a precioushistory of rectum tumor. At the microscopic analysis, areas of nointestinal musculature (replaced by adipose tissue), no mioentericplexuses and cellular degeneration were found [11].
Current advocated treatment was effective in our patient. Theresection of macroscopically suspect intestinal segments wasessential to our patient’s recovery.
The aim of this paper is to contribute to the acknowledgment ofthis disease, particularly at the histological level, because most ofthe theories about the etiology were concluded from neonatalcases. It may still be insufficient to fully clarify SAIM’s etiopathol-ogy, but its findings reinforce the possibility that two clinical formsexist e one congenital (primary SAIM) and another acquired (sec-ondary SAIM).
Considering that this disease is being discovered through theintegration of clinical and histopathological data from the fewpublished cases, it would be interesting to determine which are themain histological parameters of this condition, in order to harmo-nize concepts and facilitate comparative studies. This attempt to ahomogenous classification would also be an important tool to un-derstand and clarify SAIM’s etiopathology.
Disclosure of interest
None declared.
References
[1] Herbut PA. Congenital defect in a musculature of the stomach with rupture.Arch Pathol 1943;36:91e4.
[2] Alawadhi A, Chou S, Carpenter B. Segmental agenesis of intestinal muscularis:a case report. J Pediatr Surg 1989;24:1089e90.
[3] Humphry A, Mancer K, Stephens CA. Obstructive circular e muscle defect inthe small bowel in a one year old child. J Pediatr Surg 1980;15:197e8.
[4] McCarthy DW, Qualman S, Besner GE. Absent intestinal musculature:anatomic evidence of an embryonic origin of the lesion. J Pediatr Surg 1994;29:1476e8.
[5] Davis JS, Ryan ML, Shields JM, Sola JE, Perez EA, Neville HL, et al. Segmentalabsence of intestinal musculature: an increasingly reported pathology.J Pediatr Surg 2012;47:1566e71.
[6] Skov BG, Kofoed PE, Nielsen B. Gastrointestinal perforation due to congenitalabsence of intestinal musculature e a case report. Acta Chir Scand 1986;152:779e80.
[7] Souza CAF, Priolli DG, Martinez CAR, Fernandes Filho CLP, Nonose R, Valim A.Agenesia segmentar da camada muscular própria do intestino delgado comocausa de abdome agudo obstrutivo em recém-nascido: relato de caso. Rev BrasColoproct 2005;25:67e71.
[8] Tawfik O, Newell B, Lee KR. Segmental absence of intestinal musculature in anadult. Dig Dis Sci 1998;43:397e9.
S. Pereira et al. / J Ped Surg Case Reports 3 (2015) 207e210210
[9] Huang SF, Vacanti J, Kozakewich H. Segmental defect of the intestinalmusculature of a newborn: evidence of acquired pathogenesis. J Pediatr Surg1996;31:721e5.
[10] Oretti C, Bussani R, Janes A, Demarini S. Multiple segmental absence of in-testinal musculature presenting as spontaneous isolated perforation in anextremely low-birth-weight infant. J Pediatr Surg 2010;45:E25e7.
[11] Tamai M, Satoh M, Tsujimoto A. Segmental muscular defects of the intestine: apossible cause of spontaneous perforation of the bowel in adults. Hum Pathol2013;44:2643e50.
[12] Stephens D, Arensman R, Pillai S, Alagiozian-Angelova V. Congenital absenceof intestinal smooth muscle: a case report and review of the literature.J Pediatr Surg 2009;44:2211e5.