seidel chap9
DESCRIPTION
How to examine the chest and lungs. Assess health of the patient by inspecting, auscultating, palpating, and observing.TRANSCRIPT

K1
98
CHAPTER
9 Chest and Lungs
EQUIPMENT
◆ Drape◆ Skin-markingpencil◆ Rulerandtapemeasure◆ Stethoscopewithbellanddiaphragm
EXAMINATION
Havepatientsit,disrobedtowaist.
TECHN IQUE F IND INGS
CHEST AND LUNGS
Inspect front and back of chest
Seethoraciclandmarks.■ Size/shape/symmetry■ Landmarks EXPECTED: Supernumerary
nipplespossible(canbecluetoothercongenitalabnormalities,particularlyinwhites).
■ Compare anteroposterior diameter with transverse diameter
EXPECTED: Ribsprominent,claviclesprominentsuperiorly,sternumusuallyflatandfreeofabundanceofoverlyingtissue.Chestsomewhatasymmetric.Anteroposteriordiameteroftenhalfoftransversediameter.UNEXPECTED: Barrelchest,posteriororlateraldeviation,pigeonchest,orfunnelchest.
Seidel_5405_Chapter 9_main.indd 98 12/1/2009 10:34:49 AM

K1
CHAPTER 9 ChestandLungs 99
Thoracic landmarks. A, Anterior thorax. B, Right lateral thorax. C, Posterior thorax.
Rightupper lobe
Right middlelobe
Rightlowerlobe
Thyroid cartilage
Trachea
Suprasternal notch
Rightmidclavicularline
Right anterioraxillary line
A
C
BMidsternalline
First rib
Angle ofLouis
Leftupper lobe
Leftlowerlobe
Posterioraxillaryline
Anterior axillary line
Mid-axillaryline
Vertebralline
Scapularline
Rightupper lobe
Scapula
Rightmiddlelobe
Rightlowerlobe
Leftlowerlobe
Leftupperlobe
Spinalprocesses
TECHN IQUE F IND INGS
■ Assess nails, lips, nares UNEXPECTED: Clubbedfingernails(usuallysymmetricandpainless;mayindicatedisease,maybehereditary),pursedlips,flaredalaenasi.
Seidel_5405_Chapter 9_main.indd 99 12/1/2009 10:34:52 AM

K1
100 CHAPTER 9 ChestandLungs
TECHN IQUE F IND INGS
■ ColorAssessskin,lips,andnails.
UNEXPECTED: Superficialvenouspatterns.Cyanosisorpalloroflipsornails.
■ Breath UNEXPECTED: Malodorous.
Evaluate respirations
■ Rhythm or pattern and rateSeepatternsofrespirationinfigurebelow.
EXPECTED: Breathingeasy,regular,withoutdistress.Patterneven.Rate12to20respirationsperminute.Ratioofrespirationstoheartbeatsabout1:4.UNEXPECTED: Dyspnea,orthopnea,paroxysmalnocturnaldyspnea,platypnea,tachypnea,hypopnea.Useofaccessorymuscles,retractions.
Patterns of respiration. The horizontal axis indicates the relative rates of these patterns. The vertical swings of the lines indicate the relative depth of
respiration.
Normal
Bradypnea
Slower than 12 breathsper minute
Regular and comfortable ata rate of 12-20 per minute
Faster than 20 breathsper minute
Faster than 20 breathsper minute, deep breathing
Frequently intersperseddeeper breath
Varying periods ofincreasing depthinterspersed with apnea
Increasing difficulty ingetting breath out
Rapid, deep, labored
Irregularly interspersedperiods of apnea in a disorganized sequenceof breaths
Significant disorganizationwith irregular and varyingdepths of respiration
Tachypnea
Hyperventilation(hyperpnea)
Sighing
Airtrapping
Cheyne-Stokes
Kussmaul
Biot
Ataxic
Seidel_5405_Chapter 9_main.indd 100 12/1/2009 10:34:52 AM

K1
CHAPTER 9 ChestandLungs 101
TECHN IQUE F IND INGS
■ Inspiration/expiration ratio UNEXPECTED: Airtrapping,prolongedexpiration.
Inspect chest movement with breathing
■ Symmetry EXPECTED: Chestexpansionbilaterallysymmetric.UNEXPECTED: Asymmetry.Unilateralorbilateralbulging.Bulgingonexpiration.
Listen to respiration sounds audible without stethoscope
EXPECTED: Generallybronchovesicular.UNEXPECTED: Crepitus,stridor,wheezes.
Palpate thoracic muscles and skeleton
■ Symmetry/condition EXPECTED: Bilateralsymmetry.Someelasticityofribcage,butsternumandxiphoidrelativelyinflexibleandthoracicspinerigid.UNEXPECTED: Pulsations,tenderness,bulges,depressions,unusualmovement,unusualpositions.
■ Thoracic expansionStandbehindpatient.Placepalmsinlightcontactwithposterolateralsurfacesandthumbsalongspinalprocessesattenthrib,asshowninfigureatright.Watchthumbdivergenceduringquietanddeepbreathing.Facepatient;placethumbsalongcostalmarginandxiphoidprocesswithpalmstouchinganterolateralchest.Watchthumbdivergenceduringquietanddeepbreathing.
EXPECTED: Symmetricexpansion.UNEXPECTED: Asymmetricexpansion.
Palpating thoracic expansion. The thumbs are at the level of the
tenth rib.
Seidel_5405_Chapter 9_main.indd 101 12/1/2009 10:34:53 AM
K1
102 CHAPTER 9 ChestandLungs
TECHN IQUE F IND INGS
■ Sensations EXPECTED: Nontendersensations.UNEXPECTED: Crepitusorgratingvibration.
■ Tactile fremitusAskpatienttorecitenumbersorwordswhilesystematicallypalpatingchestwithpalmarsurfacesoffingersorulnaraspectofclenchedfist,usingfirm,lighttouch.Assesseacharea,fronttoback,sidetoside,lungapices.Comparesides.
EXPECTED: Greatvariability;generally,fremitusismoreintensewithmales(lower-pitchedvoice).UNEXPECTED: Decreasedorabsentfremitus;increasedfremitus(coarser,rougher);orgentle,moretremulousfremitus.Variationbetweensimilarpositionsonrightandleftthorax.
Note position of trachea
Usingindexfingerorthumbs,palpategentlyfromsuprasternalnotchalongupperedgesofeachclavicleandinspacesabove,toinnerbordersofsternocleidomastoidmuscles.
EXPECTED: Spacesequalsidetoside.Tracheamidlinedirectlyabovesuprasternalnotch.Possibleslightdeviationtoright.UNEXPECTED: Significantdeviationortug.Pulsations.
Perform percussion on chest
Percussasshowninfigurebelow.Compareallareasbilaterally,followingasequencesuchasshowninfiguresonp.103Seetableonp.103forcommontones,intensity,pitch,duration,quality.
Method for percussion.
Seidel_5405_Chapter 9_main.indd 102 12/1/2009 10:34:53 AM
K1
CHAPTER 9 ChestandLungs 103
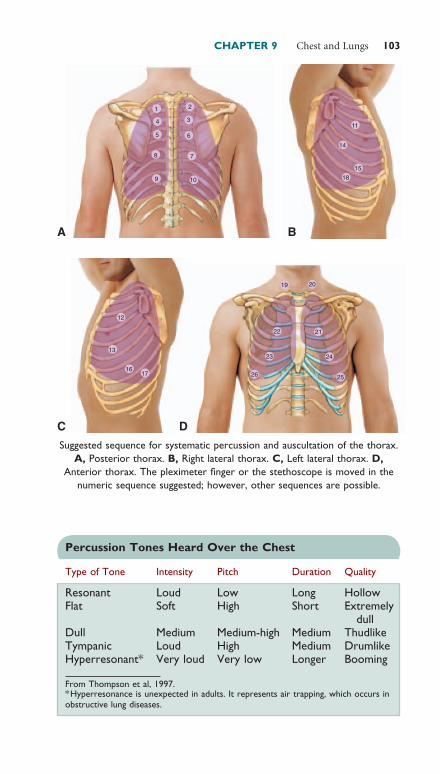
Suggested sequence for systematic percussion and auscultation of the thorax. A, Posterior thorax. B, Right lateral thorax. C, Left lateral thorax. D,
Anterior thorax. The pleximeter finger or the stethoscope is moved in the numeric sequence suggested; however, other sequences are possible.
13
16
1 2
4 3
5 6
8 7
9 10
11
14
15
18
17
12
19
22
23
26 25
24
21
20
A B
C D
Percussion Tones Heard Over the Chest
Type of Tone Intensity Pitch Duration Quality
Resonant Loud Low Long HollowFlat Soft High Short Extremely
dullDull Medium Medium-high Medium ThudlikeTympanic Loud High Medium DrumlikeHyperresonant* Very loud Very low Longer Booming
* Hyperresonance is unexpected in adults. It represents air trapping, which occurs in obstructive lung diseases.
From Thompson et al, 1997.
Seidel_5405_Chapter 9_main.indd 103 12/1/2009 10:34:57 AM
K1
104 CHAPTER 9 ChestandLungs
TECHN IQUE F IND INGS
■ ThoraxHavepatientsitwithheadbentandarmsfoldedinfrontwhilepercussingposteriorthorax,thenwitharmsraisedoverheadwhilepercussinglateralandanteriorchest.Percussat4-to5-cmintervalsoverintercostalspaces,movingsuperiortoinferior,medialtolateral.Thefemalebreastmayobscurefindings.Youorthepatientmayneedtoshiftthebreast,butpaycarefulattentiontomodesty.
EXPECTED: Resonanceoverallareasoflungs,dulloverheartandliver,spleen,areasofthorax.UNEXPECTED:Hyperresonance,dullness,orflatness.
■ Diaphragmatic excursionAskpatienttobreathedeeplyandholdbreath.Percussalongscapularlineononesideuntiltonechangesfromresonanttodull.Markskin.Allowpatienttobreathenormally,thenrepeatonotherside.Havepatienttakeseveralbreaths,thenexhaleasmuchaspossibleandhold.Oneachside,percussupfrommarktochangefromdulltoresonant.Tellpatienttoresumebreathingcomfortably.Measureexcursiondistance.
EXPECTED: 3to5cm(higheronrightthanleft).UNEXPECTED: Limiteddescent.
Measuring diaphragmatic excursion. Excursion distance is usually 3 to 5 cm.
Seidel_5405_Chapter 9_main.indd 104 12/1/2009 10:34:58 AM

K1
CHAPTER 9 ChestandLungs 105
TECHN IQUE F IND INGS
Auscultate chest with stethoscope diaphragm, apex to base■ Intensity, pitch, duration, and
quality of breath soundsHavepatientbreatheslowlyanddeeplythroughmouth.Followsetauscultationsequence,holdingstethoscopeasshowninfigurebelow.Askpatienttositupright(1) withheadbentandarms
foldedinfrontwhileauscultatingposteriorthorax,
(2) witharmsraisedoverheadwhileauscultatinglateralchest,
(3) witharmsdownandshouldersbackwhileauscultatinganteriorchest.
Listenduringinspirationandexpiration.Auscultatedownwardfromapextobaseatintervalsofseveralcentimeters,makingside-to-sidecomparisons.
EXPECTED: Seeexpectedbreathsoundsintableonp.106.UNEXPECTED: Amphoricorcavernousbreathing.Soundsdifficulttohearorabsent.Crackles,rhonchi,wheezes,orpleuralfrictionrub,asdescribedinboxonp.107.
Auscultation with a stethoscope.
Seidel_5405_Chapter 9_main.indd 105 12/1/2009 10:34:59 AM

K1
106 CHAPTER 9 ChestandLungs
TECHN IQUE F IND INGS
■ Vocal resonanceAskpatienttorecitenumbersorwords.
EXPECTED: Muffledandindistinctsounds.UNEXPECTED:Bronchophony,whisperedpectoriloquy,oregophony.
Characteristics of Expected Breath Sounds
Sound Characteristics Findings
Vesicular Heard over most of lung fields; low pitch; soft and short expirations; will be accentuated in a thin person or a child and diminished in overweight or very muscular patient
Bronchovesicular Heard over main bronchus area and over upper right posterior lung field; medium pitch; expiration equals inspiration
Bronchotracheal (tubular)
Heard only over trachea; high pitch; loud and long expirations, often somewhat longer than inspiration
Modified from Thompson et al, 1997.
Seidel_5405_Chapter 9_main.indd 106 12/1/2009 10:34:59 AM

K1
CHAPTER 9 ChestandLungs 107
Adventitious Breath Sounds
Fine crackles: High-pitched, discrete, discontinuous crackling sounds heard during end of inspiration; not cleared by cough
Medium crackles: Lower, more moist sound heard during midstage of inspiration; not cleared by cough
Coarse crackles: Loud, bubbly noise heard during inspiration; not cleared by cough
Rhonchi (sonorous wheeze): Loud, low, coarse sounds, like a snore, most often heard continuously during inspiration or expiration; coughing may clear sound (usually means mucus accumulation in trachea or large bronchi)
Wheeze (sibilant wheeze): Musical noise sounding like a squeak; most often heard continuously during inspiration or expiration; usually louder during expiration
Pleural friction rub: Dry rubbing or grating sound, usually caused by inflammation of pleural surfaces; heard during inspiration or expiration; loudest over lower lateral anterior surface
Modified from Thompson et al, 1997.
Seidel_5405_Chapter 9_main.indd 107 12/1/2009 10:35:01 AM

K1
108 CHAPTER 9 ChestandLungs
AIDS TO DIFFERENTIAL DIAGNOSIS
ABNORMAL I T Y DE SCR I P T ION
Pleuraleffusion Subjective Data: Coughwithprogressivedyspneaisthetypicalpresentingconcern.Pleuriticchestpainoccurswithaninflammatoryeffusion.Objective Data: Findingsonauscultationandpercussionvarywiththeamountoffluidpresentandwiththepositionofthepatient.Theseincludedullnesstopercussionandtactilefremitus,whicharethemostusefulfindingsforpleuraleffusion.Whenthefluidismobileitwillgravitatetothemostdependentposition.Theaffectedareas,thebreathsoundsaremutedandthepercussionnoteisoftenhyperresonantintheareaabovetheperfusion.
Lungcancer Subjective Data: Cough,wheezing,avarietyofpatternsofemphysemaandatelectasis,pneumonitis,andhemoptysis.Peripheraltumorswithoutairwayobstructionmaybeasymptomatic.Objective Data: Findingsarebasedontheextentofthetumorandthepatternsofitsinvasionandmetastasis.Withairwayobstructionapostobstructivepneumoniacandevelopwithconsolidation.Amalignantpleuraleffusionmaydevelopwithcorrespondingfindings.
Seidel_5405_Chapter 9_main.indd 108 12/1/2009 10:35:02 AM

K1
CHAPTER 9 ChestandLungs 109
ABNORMAL I T Y DE SCR I P T ION
Pneumonia Subjective Data: Rapidonset(hourstodays)ofcough,pleuriticchestpainanddyspnea.Sputumproductioniscommonwithbacterialinfection(seetableonp.110).Chills,fever,rigors,andnonspecificabdominalsymptomsofnauseaandvomitingmaybepresent.Involvementoftherightlowerlobecanstimulatethetenthandelevenththoracicnervestocauserightlowerquadrantpainandsimulateanabdominalprocess.Objective Data: Febrile,tachypneic,andtachycardic.Cracklesandrhonchiarecommonwithdiminishedbreathsounds.Egophony,bronchophony,andwhisperpectoriloquy.Dullnesstopercussionoccursovertheareaofconsolidation.
Asthma Subjective Data: Episodesofparoxysmaldyspneaandcough.Chestpainiscommonand,withit,afeelingoftightness.Episodesmaylastforminutes,hours,ordays.Maybeasymptomaticbetweenepisodes.Objective Data: Tachypneawithwheezingonexpirationandinspiration.Expirationbecomesmoreprolongedwithlaboredbreathing,fatigue,andanxiousexpressionasairwayresistanceincreases.Hypoxemiabypulseoximetry.
Seidel_5405_Chapter 9_main.indd 109 12/1/2009 10:35:02 AM

K1
110 CHAPTER 9 ChestandLungs
ABNORMAL I T Y DE SCR I P T ION
Chronicbronchitis Subjective Data: Dyspneamaybepresentalthoughnotsevere.Coughandsputumproductionareimpressive.Objective Data: Wheezingandcrackles.Hyperinflationwithdecreasedbreathsoundsandaflatteneddiaphragm.Severechronicbronchitismayresultinrightventricularfailurewithdependentedema.
Emphysema Subjective Data: Dyspneaiscommonevenatrest.Coughisinfrequentwithoutmuchproductionofsputum.Objective Data: Chestmaybebarrelshaped,andscatteredcracklesorwheezesmaybeheard.Overinflatedlungsarehyperresonantonpercussion.Inspirationislimitedwithaprolongedexpiratoryeffort(i.e.,longerthan4or5seconds)toexpelair.
Assessing Sputum
Cause Possible Sputum Characteristics
Bacterial infection Yellow, green, rust-colored (blood mixed with yellow sputum), clear, or transparent; purulent; blood streaked; mucoid, viscid
Viral infection Mucoid, viscid; blood streaked (not common)
Chronic infectious disease
All of the above; particularly abundant in early morning; slight, intermittent blood streaking; occasionally large amounts of blood
Carcinoma Slight, persistent blood streakingInfarction Blood clotted; large amounts of bloodTuberculous cavity Large amounts of blood
Seidel_5405_Chapter 9_main.indd 110 12/1/2009 10:35:02 AM

K1
CHAPTER 9 ChestandLungs 111
Pediatric Variations
EXAMINATION
TECHN IQUE F IND INGS
CHEST AND LUNGS
Inspect front and back of chest■ Compare anteroposterior
diameter with transverse diameter
EXPECTED: Infant’schestisexpectedtomeasure2to3cmlessthanheadcircumference.
Evaluate respirations
■ Rhythm or pattern and rate EXPECTED:Age Respirations per Minute
Newborn 30-801year 20-403years 20-306years 16-2210years 16-2017years 12-20
Perform direct or indirect percussion on chest
■ Thorax EXPECTED: Hyperresonancemaybeheardinchildren.
Auscultate chest with stethoscope diaphragm, apex to base
■ Intensity, pitch, duration, and quality of breath sounds
EXPECTED: Ininfantsandchildren,expecttransmittedbreathsoundsthroughoutchest.Vesicularsoundisaccentuatedinachild.Absentordiminishedbreathsoundsarehardertodetect.
Seidel_5405_Chapter 9_main.indd 111 12/1/2009 10:35:04 AM

K1
112 CHAPTER 9 ChestandLungs
SAMPLE DOCUMENTATION
Subjective. A45-year-oldwomancomplainingofcoughandfeverfor4days.Coughisnonproductive,persistent,andworsewhensheliesdown.Shefeelsillandshortofbreath.Herchestfeels“heavy.”Feverupto38.3°C(101°F).Takingacetaminophenandnonprescriptioncoughsyrupwithoutrelief.Objective. Pulse104perminute,temperature38.2°C,bloodpressure122/82,respirations32perminuteandsomewhatlabored;noretractionsorstridor.Minimalincreaseinanteroposteriordiameterofchest,withoutkyphosisorotherdefect.Tracheainmidlinewithouttug.Thoracicexpansionsymmetric.Nofrictionrubsortendernessoverribsorotherbonyprominences.Overposteriorleftbase,diminishedtactilefremitus,dullpercussionnote,andonauscultation,cracklesthatdonotclearwithcough,diminishedbreathsounds.Remaininglungfieldsareclearandfreeofadventitioussounds,withresonantpercussiontones.Diaphragmaticexcursion3cmbilaterally.
Seidel_5405_Chapter 9_main.indd 112 12/1/2009 10:35:05 AM