select plan basic kids - dominion national · pdf filed2980 crown repair, by report ... select...
TRANSCRIPT

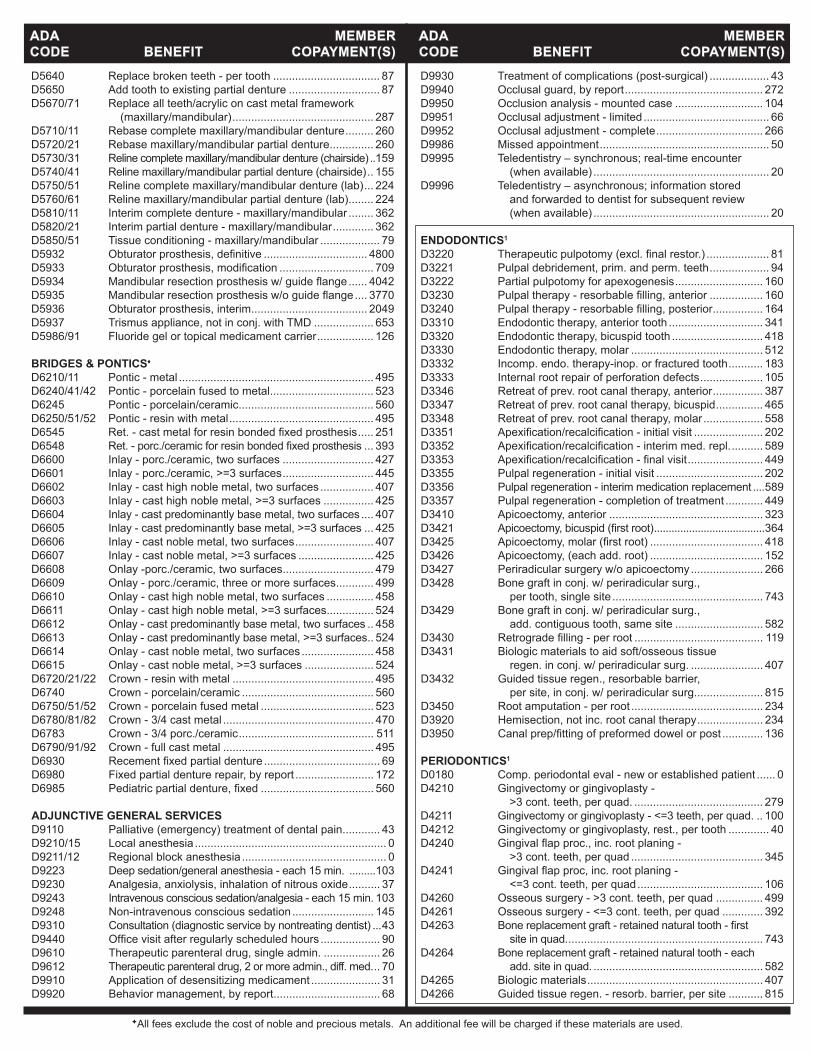
DMNDC18DBLINDPEDEHB All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.
D2951 Pin retention - per tooth, in addition to restoration ........22D3110/20 Pulpcap-direct/indirect(excl.finalrestoration) ...........32
CROWNS & BRIDGES♦
D2510/20 Inlay- metallic - 1 -2 surfaces .....................................407D2530 Inlay - metallic - three or more surfaces ......................425D2542 Onlay - metallic-two surfaces ......................................458D2543/44 Onlay - metallic - >=4 surfaces ....................................524D2610/20 Inlay - porcelain/ceramic - 1 - 2 surfaces ....................427D2630 Inlay - porcelain/ceramic - >=3 surfaces .....................445D2642 Onlay - porcelain/ceramic - two surfaces ....................479D2643/44 Onlay - porcelain/ceramic - >=3 surfaces ....................499D2650/51/52 Inlay-resin-basedcomposite->=1surface(s) ...........440D2662/63/64 Onlay - resin-based composite - >=2 surfaces ............444D2710 Crown-resinbasedcomposite(indirect) ....................272D2712 Crown-3/4resin-basedcomposite(indirect) ..............485D2720/21/22 Crown - resin with metal ..............................................495D2740 Crown - porcelain/ceramic substrate ...........................560D2750/51/52 Crown - porcelain fused metal .....................................523D2780/81/82 Crown - 3/4 cast with metal .........................................478D2783 Crown - 3/4 porcelain/ceramic .....................................511D2790-94 Crown - full cast metal .................................................495D2910/20 Recement inlay, onlay/crown or partial coverage rest. ......43D2929 Procelain/cermaic crown - prim. tooth .........................560D2930 Prefab. stainless steel crown - prim. tooth ..................110D2931 Prefab. stainless steel crown - perm. tooth .................121D2932 Prefabricated resin crown ............................................140D2941 Interim therapeutic restoration, primary dentition ..........31D2952 Cast post and core in addition to crown ......................186D2954 Prefab. post and core in addition to crown ..................154D2955 Postremoval(notinconj.withendo.therapy) ............105D2970 Temporarycrown(fracturedtooth) ..................................0D2980 Crown repair, by report ................................................102D2981/82/83 Inlay, onlay or veneer repair ........................................102D2990 Resininfitrationlesion ...................................................41 PROSTHETICS (DENTURES)D5110/20 Complete denture - maxillary/mandibular ....................697D5130/40 Immediate denture - maxillary/mandibular ..................722D5211/12 Maxillary/mandibular partial denture - resin base ........649D5213/14 Maxillary/mandibular partial denture - cast metal ........750D5221/22 Immediate maxillary/mandibular partial denture - resin base .............................................................649D5223/24 Immediate maxillary/mandibular partial denture - cast metal .............................................................750D5225/26 Maxillary/mandibularpartialdenture-flexiblebase ....750D5281 Rem. unilateral partial denture - one piece cast metal ....419D5410/11 Adjust complete denture - maxillary/mandibular ...........38D5421/22 Adjust partial denture - maxillary/mandibular ................38D5510/5610 Repairbrokencompletedenturebase(complete/resin) ... 87D5520 Replace missing or broken teeth - complete denture ....87D5620 Repair cast framework ..................................................87D5630/60 Clasp repaired, replaced or added ..............................115D5640 Replace broken teeth - per tooth ...................................87D5650 Add tooth to existing partial denture ..............................87D5670/71 Replace all teeth/acrylic on cast metal framework (maxillary/mandibular) ............................................287D5710/11 Rebase complete maxillary/mandibular denture .........260D5720/21 Rebase maxillary/mandibular partial denture ..............260
D9439 Officevisit ......................................................................10 DIAGNOSTIC/PREVENTIVED0120 Periodic oral eval - established patient ............................0D0140 Limited oral eval - problem focused ................................0D0145 Oral eval for a patient under 3 years of age ....................0D0150 Comprehensive oral eval - new or established patient ....0D0160 Detailed and extensive oral eval - problem focused ........0D0170 Re-evaluation - limited, problem focused ........................0D0210 Intraoral-completeseries(includingbitewings) ...........26D0220/30 Intraoral-periapicalfirstfilmandeachadditional ...........0D0240 Intraoral-occlusalfilm ....................................................0D0250 Extraoralfilm ...................................................................0D0270-74 Bitewingx-rays-1-4films ...............................................0D0277 Verticalbitewings-7to8films ........................................0D0330 Panoramicfilm ...............................................................30D0340 2D cephalometric radiographic image .............................0D0350 2Doral/facialphotographicimages(intraoral/extraoral) ..0D0351 3D photographic image ...................................................0D0391 Interpretation of diagnostic image only ............................0D0460 Pulp vitality tests ..............................................................0D0470 Diagnostic casts ..............................................................0D1110 Prophylaxis(cleaning)-adult ........................................13D1120 Prophylaxis(cleaning)-child ........................................10D1206 Topicalfluoridevarnishformod/highriskcariespatients ....0D1208 Topicalapplicationoffluoride ..........................................0D1310 Nutritional counseling for control of dental disease .........0D1320 Tobacco counseling for control of prev. oral disease .......0D1330 Oral hygiene instructions .................................................0D1351 Sealant - per tooth .........................................................21D1352 Prev resin rest. mod/high caries risk – perm. tooth .......21 SPACE MAINTAINERSD1510/20 Spacemaintainer-fixed/removable-unilateral ..........143D1515/25 Spacemaintainer-fixed/removable-bilateral ............198D1550 Re-cementation of space maintainer .............................34 D1575 Distalshoespacemaintainer-fixed-unilateral ..........143 RESTORATIVE DENTISTRY (FILLINGS) AMALGAMRESTORATIONS(SILVER)D2140 Amalgam - one surface, prim. or perm. .........................41D2150 Amalgam - two surfaces, prim. or perm. .......................51D2160 Amalgam - three surfaces, prim. or perm. .....................64D2161 Amalgam - >=4 surfaces, prim. or perm. .......................78 RESIN/COMPOSITERESTORATIONS(TOOTHCOLORED)D2330 Resin-based composite - one surface, anterior .............69D2331 Resin-based composite - two surfaces, anterior ...........83D2332 Resin-based composite - three surfaces, anterior .........99D2335 Resin-based composite - >=4 surfaces, anterior .........119D2390 Resin-based composite crown, anterior ......................192D2391 Resin-based composite - one surface, posterior ...........73D2392 Resin-based composite - two surfaces, posterior .........87D2393 Resin-based composite - three surfaces, posterior .....102D2394 Resin-based composite - >=4 surfaces, posterior .......123 D2940 Protective restoration ....................................................39D2949 Restorative foundation for an indirect restoration ............0D2950 Core buildup, including any pins .................................125
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
Annual Out-of-Pocket Maximum: $350 per child per calendar year for medically necessary treatment (maximum of $700 for policy covering two or more children)
Select Plan Basic Kids 702xs (DC)Description of Benefits & Member Copayments for Pediatric Services (under age 19)
Coverage continues through end of month in which the Member turns 19.
The dental plan is underwritten by Dominion Dental Services, Inc. d/b/a Dominion National.

D5730/31 Relinecompletemaxillary/mandibulardenture(chairside) ..159D5740/41 Relinemaxillary/mandibularpartialdenture(chairside) ..155D5750/51 Relinecompletemaxillary/mandibulardenture(lab) ...224D5760/61 Relinemaxillary/mandibularpartialdenture(lab) ........224D5810/11 Interim complete denture - maxillary/mandibular ........362D5820/21 Interim partial denture - maxillary/mandibular .............362D5850/51 Tissue conditioning - maxillary/mandibular....................79 BRIDGES & PONTICS♦
D6010 Surgical placement of implant body, endosteal .........1716D6011 Second stage implant surgery .....................................200D6012 Surgical placement of interim implant body ...............1782D6013 Surgical placement of mini implant ..............................572D6040 Surgical placement, eposteal implant ........................3564D6050 Surgical placement, transosteal implant ....................4455D6055 Dental implant supported connecting bar ..................1611D6056 Prefabricated abutment ...............................................456D6058 Abutment supported porcelain/ceramic crown ............560D6059/60/61 Abutment supported porcelain fused to metal crown - metal ..523D6062/63/64 Abutment supported cast metal crown - metal ............495D6065 Implant supported porcelain/ceramic crown ................560D6066 Implant supported porcelain fused to metal crown - titanium, titanium allow, high noble metal ...............523D6067 Implant supported metal crown - titanium, titanium alloy, high noble metal ............................................523D6068 Abutment supported retainer for porc/ceramic ............788D6069 Abutment supp. retainer for porc/high noble ...............843D6070 Abutment supp. retainer for porc/pred. base ...............695D6071 Abutment supp. retainer for porc/noble .......................704D6072 Abutment supp retainer for cast high noble .................788D6073 Abutment supp. retainer for cast high noble ................749D6074 Abutment supp. retainer for cast noble metal ..............758D6075 Implant supported retainer for ceramic FPD ...............874D6076 Implant supported retainer for porc/metal FPD ...........823D6077 Implant supported retainer for cast metal FPD ............872D6080 Implant maintenance procedures ..................................61D6081 Scalinganddebridementinthepresenceofinflammation or mucositis of a single implant, including cleaning of theimplantsurfaces,withoutflapentryandclosure .... 63 D6090 Repair implant supported prosthesis ...........................362D6091 Replacement of Precision Attachment ..........................34D6095 Repair implant abutment, by report .............................391D6100 Implant removal, by report ...........................................241D6101 Debribement periimplant defect ....................................90D6102 Deridement and osseous contouring periimplant defect ...180D6103 Bone graft repair perrimplant defect ............................600D6104 Bone graft at time of implant placement ......................600D6190 Radiographic surgical implant index, by report ...............0D6210-14 Pontic - metal ..............................................................495D6240/41/42 Pontic - porcelain fused to metal .................................523D6245 Pontic - porcelain/ceramic ...........................................560D6250/51/52 Pontic - resin with metal ..............................................495D6545 Ret.-castmetalforresinbondedfixedprosthesis .....251D6548 Ret.-porc./ceramicforresinbondedfixedprosthesis ....393D6549 Resinretainer-forresinbondedfixedprosthesis .......251D6600 Inlay - porc./ceramic, two surfaces ..............................427D6601 Inlay - porc./ceramic, >=3 surfaces .............................445D6602 Inlay - cast high noble metal, two surfaces .................407D6603 Inlay - cast high noble metal, >=3 surfaces .................425D6604 Inlay - cast predominantly base metal, two surfaces ....407D6605 Inlay - cast predominantly base metal, >=3 surfaces ....425D6606 Inlay - cast noble metal, two surfaces .........................407D6607 Inlay - cast noble metal, >=3 surfaces .........................425D6608 Onlay -porc./ceramic, two surfaces .............................479D6609 Onlay - porc./ceramic, three or more surfaces ............499D6610 Onlay - cast high noble metal, two surfaces ................458D6611 Onlay - cast high noble metal, >=3 surfaces ...............524D6612 Onlay - cast predominantly base metal, two surfaces ...458
D6613 Onlay - cast predominantly base metal, >=3 surfaces ..524D6614 Onlay - cast noble metal, two surfaces .......................458D6615 Onlay - cast noble metal, >=3 surfaces .......................524D6720/21/22 Crown - resin with metal ..............................................495D6740 Crown - porcelain/ceramic ...........................................560D6750/51/52 Crown - porcelain fused metal .....................................523D6780 Crown - 3/4 cast high noble metal ...............................470D6781 Crown - 3/4 cast predominantly base metal ................470D6782 Crown - 3/4 cast noble metal .......................................470D6783 Crown - 3/4 porc./ceramic ...........................................511D6790/91/92 Crown - full cast metal .................................................495D6930 Recementfixedpartialdenture .....................................69D6980 Fixed partial denture repair, by report .........................172 ADJUNCTIVE GENERAL SERVICESD9110 Palliative(emergency)treatmentofdentalpain ............43D9210/15 Local anesthesia .............................................................0D9211/12 Regional block anesthesia ..............................................0D9223 Deep sedation/general anesthesia - each 15 min. ......... 103D9230 Analgesia, anxiolysis, inhalation of nitrous oxide ..........37D9243 Intravenous conscious sedation/analgesia - each 15 min. 103D9310 Consultation(diagnosticservicebynontreatingdentist) ... 43D9910 Application of desensitizing medicament ......................31D9930 Treatmentofcomplications(post-surgical)....................43D9940 Occlusal guard, by report ............................................272D9950 Occlusion analysis - mounted case .............................104D9951 Occlusal adjustment - limited ........................................66D9952 Occlusal adjustment - complete ..................................266D9986 Missed appointment ......................................................50D9995 Teledentistry – synchronous; real-time encounter (whenavailable)........................................................20 D9996 Teledentistry – asynchronous; information stored and forwarded to dentist for subsequent review (whenavailable)........................................................20 ENDODONTICS1
D3220 Therapeuticpulpotomy(excl.finalrestor.) ....................81D3221 Pulpal debridement, prim. and perm. teeth ...................94D3222 Partial pulpotomy for apexogenesis ............................160D3230 Pulpaltherapy-resorbablefilling,anterior ..................160D3240 Pulpaltherapy-resorbablefilling,posterior ................164D3310 Endodontic therapy, anterior tooth ..............................341D3320 Endodontic therapy, bicuspid tooth .............................418D3330 Endodontic therapy, molar ...........................................512D3333 Internal root repair of perforation defects ....................105D3346 Retreat of prev. root canal therapy, anterior ................387D3347 Retreat of prev. root canal therapy, bicuspid ...............465D3348 Retreat of prev. root canal therapy, molar ...................558D3351 Apexification/recalcification-initialvisit .......................202D3352 Apexification/recalcification-interimmed.repl. ..........589D3353 Apexification/recalcification-finalvisit ........................449D3355 Pulpal regeneration - initial visit ...................................202D3356 Pulpal regeneration - interim medication replacement ....589D3357 Pulpal regeneration - completion of treatment ............449D3410 Apicoectomy - anterior ................................................323D3421 Apicoectomy-bicuspid(firstroot) .................................... 364D3425 Apicoectomy-molar(firstroot) ...................................418D3426 Apicoectomy(eachadd.root) .....................................152D3427 Periradicular surgery w/o apicoectomy .......................266D3430 Retrogradefilling-perroot ..........................................119D3450 Root amputation - per root ..........................................234D3920 Hemisection, not inc. root canal therapy .....................234D3950 Canalprep/fittingofpreformeddowelorpost .............136 PERIODONTICS1 D0180 Comp. periodontal eval - new or established patient ......0D4210 Gingivectomy or gingivoplasty - >3 cont. teeth, per quad. ..279D4211 Gingivectomy or gingivoplasty - <=3 teeth, per quad. .100
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.

ADA MEMBERCODE BENEFIT COPAYMENT(S)
1 Specialty care is provided at the listed copayment whether performed by a Participating General Dentist or a Participating Specialist. Referrals to a specialist must be made by a member’s Participating General Dentist. See Plan Exclusion #13.
2 See exclusion #15 and limitation #28 for additional coverage information.
Only current ADA CDT codes are considered valid by Dominion NationalCurrent Dental Terminology © American Dental Association.
D4212 Gingivectomy or gingivoplasty, rest., per tooth ..............40D4240 Gingivalflapproc.,inc.rootplaning- >3 cont. teeth, per quad ..........................................345D4241 Gingivalflapproc,inc.rootplaning- <=3 cont. teeth, per quad........................................106D4249 Clinical crown lengthening - hard tissue ......................576D4260 Osseous surgery - >3 cont. teeth, per quad ................499D4261 Osseous surgery - <=3 cont. teeth, per quad ..............392D4268 Surgical revision proc., per tooth .................................358D4270 Pedicle soft tissue graft procedure ..............................643D4273 Subepithelial connective tissue graft proc. ..................800D4274 Mesial/distal wedge procedure, single tooth ...............308D4277 Free soft tissue graft, per tooth ...................................654D4278 Free soft tissue graft, each add. tooth .........................100D4341 Perio scaling and root planing - >3 cont teeth, per quad. ..109D4342 Perio scaling and root planing - <= 3 teeth, per quad ...63D4346 Scaling in presence of generalized moderate or severegingivalinflammation-fullmouth, after oral evaluation .....................................................45 D4355 Full mouth debridement .................................................89D4381 Localized delivery of chemotherapeutic agents ............98D4910 Periodontal maintenance ...............................................74D4921 Gingival irrigation, per quadrant ......................................0 ORAL SURGERY1
D7111 Extraction, coronal remnants - deciduous tooth ............56D7140 Extraction, erupted tooth or exposed root .....................69D7210 Extraction, erupted tooth req elev, etc ........................133D7220 Removal of impacted tooth - soft tissue ......................151D7230 Removal of impacted tooth - partially bony .................196D7240 Removal of impacted tooth - completely bony ............241D7241 Removal of imp. tooth - completely bony, with unusual surg. complications ............................217D7250 Removal of residual tooth roots ...................................141D7251 Coronectomy-intentional partial tooth removal ............217D7270 Tooth reimplant./stabiliz. of acc. evulsed/displaced tooth ....226D7280 Exposure of an unerupted tooth ..................................153D7291 Transseptalfiberotomy/supracrestalfiberotomy,byreport ....60D7310/20 Alveoloplasty, >=4 per quad. .......................................141D7321 Alveoloplasty in conj. with extractions, 1-3 per quad.....141D7471 Removal of lateral exostosis .......................................351D7510 Incision and drainage of abscess - intraoral soft tissue ...96D7910 Suture of recent small wounds up to 5 cm ....................59D7921 Collection application of blood concentrate ...................40D7960 Frenulectomy(frenectomy/frenotomy)-separateproc. ..263D7971 Excision of pericoronal gingiva ....................................131 ORTHODONTICS2 - PRE-AUTHORIZATION REQUIREDD8010 Limited ortho. treatment of the primary dentition .......3304D8020 Limited ortho. treatment of the transitional dentition ...3304D8030 Limited ortho treatment - adolescent dentition ..........3422D8050 Interceptive ortho. treatment of the primary dentition ....3304D8060 Interceptive ortho. treatment of the transitional dentition ...3304D8070 Comp. ortho. treatment - transitional dentition ..........3304D8080 Comp. ortho. treatment - adolescent dentition ..........3422D8090 Comp. ortho. treatment - adult dentition ....................3658D8210 Removable appliance therapy .....................................770D8220 Fixed appliance therapy ..............................................783D8660 Pre-orthodontic treatment visit ....................................413D8670 Periodicortho.treatmentvisit(aspartofcontract) ......118D8680 Ortho.ret.(rem.ofappl./placementofretainer(s)) ......413

Plan Exclusions1. Services which are covered under worker’s compensation or employer’s liability laws.2. Services which are not necessary for the patient’s dental health as determined by the Plan.3. Cosmetic, elective or aesthetic dentistry except as required due to accidental bodily injury to sound natural teeth as determined by the Plan.4. Oral surgery requiring the setting of fractures or dislocations.5. Services with respect to malignancies, cysts or neoplasms, hereditary, congenital, mandibular prognathism or development malformations where,intheopinionofthePlan,suchservicesshouldnotbeperformedinadentaloffice.6. Dispensing of drugs.7. Hospitalization for any dental procedure.8. Treatment required for conditions resulting from major disaster, epidemic, war, acts of war, whether declared or undeclared, or while on active duty as a member of the armed forces of any nation.9. Replacement due to loss or theft of prosthetic appliance.10. ProceduresnotlistedascoveredbenefitsunderthisPlan.11. ServicesobtainedoutsideofthedentalofficeinwhichenrolledandthatarenotpreauthorizedbysuchofficeorthePlan(withtheexception ofout-of-areaemergencydentalservices).12. ServicesrelatedtothetreatmentofTMD(TemporomandibularDisorder)exceptifTMDiscausedbysevere,dysfunctional,handicapping malocclusion that requires medically necessary orthodontia services.13. ServicesperformedbyaParticipatingSpecialistwithoutareferralfromaParticipatingGeneralDentist(withtheexceptionofOrthodontics). Participating dentists should refer to Specialty Care Referral Guidelines.14. Elective surgery including, but not limited to, extraction of non-pathologic, asymptomatic impacted teeth as determined by the Plan. The prophylactic removal of these teeth for medically necessary orthodontia services may be covered subject to review.15. Non-medicallynecessaryorthodontiaisnotacoveredbenefitunderthispolicy.AdiscountisprovidedtomembersthroughthePlan’s agreements with its participating orthodontists. The provider agreements create no liability for payment by the Plan, and payments by the member for these services do not contribute to the Out-of-Pocket Maximum. The Invisalign system and similar specialized braces are not acoveredbenefit.Seelimitation#28concerningmedicallynecessaryorthodontia.
Plan Limitations1. Oneevaluation(D0120,D0140,D0145,D0150,D0160,D0180)iscoveredoncepersixmonths,perpatient.D0150limitedtooncein12 months.2. One(1)teethcleaning(D1110orD1120)per6months,perpatient.3. One(1)fluorideapplicationevery6months,perpatient.4. One(1)setofbitewingx-raysarecoveredpersix(6)months,perpatientstartingatagetwo.5. One(1)setoffullmouthx-raysorpanoramicfilmiscoveredeveryfive(5)years.Panoramicx-raysarelimitedtoages6-18.Nomorethan one set of x-rays are covered per visit. 6. One(1)sealantpertoothiscoveredper36months,perpatientuptoage18(limitedtoocclusalsurfacesofposteriorpermanentteeth withoutrestorationsordecay).7. One(1)spacemaintainer(D1510,D1520,D1515orD1525)iscoveredper24monthsperpatient,perarch.D1575limitedtoonceperlifetime.8. Replacementofafillingiscoveredifitismorethanthree(3)yearsfromthedateoforiginalplacement.9. Replacementofaprimarystainlesssteelcrown(underage15),crown,denture,orotherprosthodonticapplianceiscoveredifitismore thanfive(5)yearsfromthedateoforiginalplacement.10. Crownandbridgefeesapplytotreatmentinvolvingfiveorfewerunitswhenpresentedinasingletreatmentplan.Additionalcrownor bridgeunits,beginningwiththesixthunit,areavailableattheprovider’sUsual,Customary,andReasonable(UCR)fee,minus25%.11. Relining and rebasing of dentures is covered once per 24 months, per patient.12. Root canal treatment is covered once per lifetime.13. Periodontalscalingandrootplaning(D4341orD4342),limitedtoone(1)per24months,perpatient,perquadrant.14. Scalinginpresenceofgeneralizedmoderateorseveregingivalinflammation-fullmouth,afteroralevaluationandinlieuofacovered D1110, limited to once per two years.15. Osseoussurgery(D4260orD4261),gingivalflapprocedure(D4240),andgingivectomyorgingivoplasy(D4210-D4212)arelimitedtoone (1)per36months.16. Full mouth debridement is covered once per lifetime, per patient.17. ProcedureCodeD4381islimitedtoone(1)benefitpertoothforthreeteethperquadrant;oratotalof12teethforallfourquadrantsper twelve(12)months.Musthavepocketdepthsoffive(5)millimetersorgreater.18. Periodontal surgery of any type, including any associated material, is covered once every 24 months, per quadrant or surgical site.19. Periodontalmaintenanceiscoveredtwicepercalendaryearinadditiontoadultprophylaxis,within24monthsafterdefinitiveperiodontal therapy.20. Denture rebase and denture reline is limited to 1 in a 36 month period 6 months after initial placement.21. One(1)scalinganddebridementinthepresenceofinflammationormucositisofasingleimplant,includingcleaningoftheimplant surfaces,withoutflapentryandclosure,pertwo(2)years. 22. Coronectomy,intentionalpartialtoothremoval,one(1)perlifetime. 23. Anesthesia requires a narrative of medical necessity be maintained in patient records. A maximum of 60 minutes of services are allowed for general anesthesia and intravenous or non-intravenous conscious sedation. General anesthesia is not covered with procedure codes D9230 or D9243. Intravenous conscious sedation is not covered with procedure codes D9223 or D9230. Nonintravenous conscious sedationisnotcoveredwithprocedurecodeD9223orD9230.Analgesia(nitrousoxide)isnotcoveredwithprocedurecodesD9223or D9243. 24. Occlusal guards are covered by report for patients 13 years of age or older when the purpose of the occlusal guard is for the treatment of bruxismordiagnosesotherthantemporomandibulardysfunction(TMD).Occlusalguardsarelimitedtooneper12consecutive month period. 25. Deepsedation/generalanesthesiaandintravenousconscioussedationarecovered(byreport)onlywhenprovidedinconnectionwith acoveredprocedure(s)whendeterminedtobemedicallyordentallynecessaryfordocumentedhandicappedoruncontrollablepatientsor justifiablemedicalordentalconditions.26. Fixed partial dentures, buildups, and posts and cores for members under 16 years of age are only covered if deemed necessary by the Plan.27. Onlays, crowns, and posts and cores for members 12 years of age or younger are only covered if deemed necessary by the Plan. Cast postsandcores(D2952)areprocessedasanalternatebenefitofaprefabricatedpostandcore.Postsareeligibleonlywhenprovidedas part of a crown buildup or implant and are considered integral to the buildup or implant. 28. Orthodontics is only covered if medically necessary as determined by the Plan. Patient copayments will apply to the routine orthodontic appliance portion of services only. Additional costs incurred will become the patient’s responsibility. 29. Teledentistry,synchronous(D9995)orasynchronous(D9996),limitedtotwopercalendaryear(whenavailable).
Exclusions & Limitations

D2950 Core buildup, including any pins ................................. 125D2951 Pin retention - per tooth, in addition to restoration ........ 22D3110/20 Pulpcap-direct/indirect(excl.finalrestoration) ........... 32 CROWNS & BRIDGES♦
D2510 Inlay- metallic - one surface ........................................ 407D2520 Inlay- metallic - two surfaces ....................................... 407D2530 Inlay - metallic - three or more surfaces ...................... 425D2542 Onlay - metallic-two surfaces ...................................... 458D2543 Onlay - metallic - three surfaces ................................. 524D2544 Onlay - metallic - four or more surfaces ...................... 524D2610 Inlay - porcelain/ceramic - one surface ....................... 427D2620 Inlay - porcelain/ceramic - two surfaces ...................... 427D2630 Inlay - porcelain/ceramic - >=3 surfaces ..................... 445D2642 Onlay - porcelain/ceramic - two surfaces .................... 479D2643/44 Onlay - porcelain/ceramic - >=3 surfaces ................... 499D2650/51/52 Inlay-resin-basedcomposite->=1surface(s) ........... 440D2662/63/64 Onlay - resin-based composite - >=2 surfaces ........... 444D2710 Crown-resinbasedcomposite(indirect) ................... 272D2712 Crown-3/4resin-basedcomposite(indirect) ............. 485D2720/21/22 Crown - resin with metal ............................................. 495D2740 Crown - porcelain/ceramic substrate .......................... 560D2750/51/52 Crown - porcelain fused metal .................................... 523D2780/81/82 Crown - 3/4 cast with metal ......................................... 478D2783 Crown - 3/4 porcelain/ceramic .................................... 511D2790/91/92 Crown - full cast metal ................................................ 495D2799 Provisional crown ............................................................ 0D2910/20 Recement inlay, onlay/crown or partial coverage rest. .... 43D2915 Recement cast or prefab. post and core ....................... 82D2930 Prefab. stainless steel crown - prim. tooth .................. 110D2931 Prefab. stainless steel crown - perm. tooth ................. 121D2932 Prefabricated resin crown ........................................... 140D2933 Prefab. stainless steel crown w/ resin window ............ 271D2952 Cast post and core in addition to crown ...................... 186D2953 Each add. indirectly fabricated post - same tooth ......... 50D2954 Prefab. post and core in addition to crown .................. 154D2955 Postremoval(notinconj.withendo.therapy) ............ 105D2957 Each add. prefab post - same tooth .............................. 40D2970 Temporarycrown(fracturedtooth) .................................. 0D2980 Crown repair, by report ............................................... 102 PROSTHETICS (DENTURES)D5110/20 Complete denture - maxillary/mandibular ................... 697D5130/40 Immediate denture - maxillary/mandibular .................. 722D5211/12 Maxillary/mandibular partial denture - resin base ....... 649D5213/14 Maxillary/mandibular partial denture - cast metal ....... 750D5221/22 Immediate maxillary/mandibular partial denture - resin base ............................................................. 649D5223/24 Immediate maxillary/mandibular partial denture - cast metal .............................................................. 750 D5225/26 Maxillary/mandibularpartialdenture-flexiblebase .... 750D5281 Rem. unilateral partial denture - one piece cast metal ....419D5410/11 Adjust complete denture - maxillary/mandibular ........... 38D5421/22 Adjust partial denture - maxillary/mandibular ................ 38D5510/5610 Repairbrokencompletedenturebase(complete/resin) ...87D5520 Replace missing or broken teeth - complete denture ... 87D5620 Repair cast framework .................................................. 87D5630/60 Clasp repaired, replaced or added .............................. 115
D9439 Officevisit ..................................................................... 20 DIAGNOSTIC/PREVENTIVED0120 Periodic oral eval - established patient ........................... 0D0140 Limited oral eval - problem focused ................................ 0D0145 Oral eval for a patient under 3 years of age .................... 0D0150 Comprehensive oral eval - new or established patient ... 0D0160 Detailed and extensive oral eval - problem focused ....... 0D0170 Re-evaluation - limited, problem focused ........................ 0D0210 Intraoral-completeseries(includingbitewings) ........... 26D0220/30 Intraoral-periapicalfirstradiographicimage/eachadd. . 0D0240 Intraoral - occlusal radiographic image ........................... 0D0250 Extraoral - 2D projection radiographic image .................. 0D0270-74 Bitewing - 1-4 radiographic images ................................. 0D0277 Vertical bitewings - 7 to 8 radiographic images ............... 0D0322 Tomographic survey ........................................................ 0D0330 Panoramic radiographic image ..................................... 30D0340 2D cephalometric radiographic image ............................ 0D0350 2Doral/facialphotographicimages(intraoral/extraoral) . 0D0460 Pulp vitality tests ............................................................. 0D0470 Diagnostic casts .............................................................. 0D0999 Unspecifieddiagnosticprocedure,byreport ................... 0D1110 Prophylaxis(cleaning)-adult ........................................ 13D1120 Prophylaxis(cleaning)-child ........................................ 10D1206 Topicalfluoridevarnishformod/highriskcariespatients .... 0D1208 Topicalapplicationoffluoride .......................................... 0D1310 Nutritional counseling for control of dental disease ........ 0D1320/30 Oral hygiene instructions ................................................ 0D1351 Sealant - per tooth ........................................................ 21D1352 Prev resin rest. mod/high caries risk – perm. tooth ....... 21 SPACE MAINTAINERSD1510/20 Spacemaintainer-fixed/removable-unilateral .......... 143D1515/25 Spacemaintainer-fixed/removable-bilateral ............ 198D1550 Re-cementation of space maintainer ............................ 34D1555 Removaloffixedspacemaintainer, by non-originating dentist ......................................... 44 D1575 Distalshoespacemaintainer-fixed-unilateral ......... 143 RESTORATIVE DENTISTRY (FILLINGS) AMALGAMRESTORATIONS(SILVER)D2140 Amalgam - one surface, prim. or perm. ........................ 41D2150 Amalgam - two surfaces, prim. or perm. ....................... 51D2160 Amalgam - three surfaces, prim. or perm. .................... 64D2161 Amalgam - >=4 surfaces, prim. or perm. ...................... 78 RESIN/COMPOSITERESTORATIONS(TOOTHCOLORED)D2330 Resin-based composite - one surface, anterior ............ 69D2331 Resin-based composite - two surfaces, anterior ........... 83D2332 Resin-based composite - three surfaces, anterior ........ 99D2335 Resin-based composite - >=4 surfaces, anterior ........ 119D2390 Resin-based composite crown, anterior ...................... 192D2391 Resin-based composite - one surface, posterior .......... 73D2392 Resin-based composite - two surfaces, posterior ......... 87D2393 Resin-based composite - three surfaces, posterior .... 102D2394 Resin-based composite - >=4 surfaces, posterior ...... 123D2940 Protective restoration .................................................... 39D2941 Interim therapeutic restoration, primary dentition .......... 31
DMNDE18DBLINDPEDEHB All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.
Annual Out-of-Pocket Maximum: $350 per child per calendar year for medically necessary treatment (maximum of $700 for policy covering two or more children)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
Select Plan Basic Kids 702xs (DE)Description of Benefits & Member Copayments for Pediatric Services (under age 19)
Coverage continues through end of month in which the Member turns 19.
The dental plan is underwritten by Dominion Dental Services, Inc. d/b/a Dominion National.
D5640 Replace broken teeth - per tooth .................................. 87D5650 Add tooth to existing partial denture ............................. 87D5670/71 Replace all teeth/acrylic on cast metal framework (maxillary/mandibular) ............................................. 287D5710/11 Rebase complete maxillary/mandibular denture ......... 260D5720/21 Rebase maxillary/mandibular partial denture .............. 260D5730/31 Relinecompletemaxillary/mandibulardenture(chairside) ..159D5740/41 Relinemaxillary/mandibularpartialdenture(chairside) .. 155D5750/51 Relinecompletemaxillary/mandibulardenture(lab) ... 224D5760/61 Relinemaxillary/mandibularpartialdenture(lab) ........ 224D5810/11 Interim complete denture - maxillary/mandibular ........ 362D5820/21 Interim partial denture - maxillary/mandibular ............. 362D5850/51 Tissue conditioning - maxillary/mandibular ................... 79D5932 Obturatorprosthesis,definitive ................................. 4800D5933 Obturatorprosthesis,modification .............................. 709D5934 Mandibularresectionprosthesisw/guideflange ...... 4042D5935 Mandibularresectionprosthesisw/oguideflange .... 3770D5936 Obturator prosthesis, interim ..................................... 2049D5937 Trismus appliance, not in conj. with TMD ................... 653D5986/91 Fluoride gel or topical medicament carrier .................. 126 BRIDGES & PONTICS♦
D6210/11 Pontic - metal .............................................................. 495D6240/41/42 Pontic - porcelain fused to metal ................................. 523D6245 Pontic - porcelain/ceramic ........................................... 560D6250/51/52 Pontic - resin with metal .............................................. 495D6545 Ret.-castmetalforresinbondedfixedprosthesis ..... 251D6548 Ret.-porc./ceramicforresinbondedfixedprosthesis ... 393D6600 Inlay - porc./ceramic, two surfaces ............................. 427D6601 Inlay - porc./ceramic, >=3 surfaces ............................. 445D6602 Inlay - cast high noble metal, two surfaces ................. 407D6603 Inlay - cast high noble metal, >=3 surfaces ................ 425D6604 Inlay - cast predominantly base metal, two surfaces .... 407D6605 Inlay - cast predominantly base metal, >=3 surfaces ... 425D6606 Inlay - cast noble metal, two surfaces ......................... 407D6607 Inlay - cast noble metal, >=3 surfaces ........................ 425D6608 Onlay -porc./ceramic, two surfaces ............................. 479D6609 Onlay - porc./ceramic, three or more surfaces ............ 499D6610 Onlay - cast high noble metal, two surfaces ............... 458D6611 Onlay - cast high noble metal, >=3 surfaces ............... 524D6612 Onlay - cast predominantly base metal, two surfaces .. 458D6613 Onlay - cast predominantly base metal, >=3 surfaces .. 524D6614 Onlay - cast noble metal, two surfaces ....................... 458D6615 Onlay - cast noble metal, >=3 surfaces ...................... 524D6720/21/22 Crown - resin with metal ............................................. 495D6740 Crown - porcelain/ceramic .......................................... 560D6750/51/52 Crown - porcelain fused metal .................................... 523D6780/81/82 Crown - 3/4 cast metal ................................................ 470D6783 Crown - 3/4 porc./ceramic ........................................... 511D6790/91/92 Crown - full cast metal ................................................ 495D6930 Recementfixedpartialdenture ..................................... 69D6980 Fixed partial denture repair, by report ......................... 172D6985 Pediatricpartialdenture,fixed .................................... 560 ADJUNCTIVE GENERAL SERVICESD9110 Palliative(emergency)treatmentofdentalpain ............ 43D9210/15 Local anesthesia ............................................................. 0D9211/12 Regional block anesthesia .............................................. 0D9223 Deep sedation/general anesthesia - each 15 min. .........103D9230 Analgesia, anxiolysis, inhalation of nitrous oxide .......... 37D9243 Intravenous conscious sedation/analgesia - each 15 min. 103D9248 Non-intravenous conscious sedation .......................... 145D9310 Consultation(diagnosticservicebynontreatingdentist) ...43D9440 Officevisitafterregularlyscheduledhours ................... 90D9610 Therapeutic parenteral drug, single admin. .................. 26D9612 Therapeutic parenteral drug, 2 or more admin., diff. med. .. 70D9910 Application of desensitizing medicament ...................... 31D9920 Behavior management, by report .................................. 68
D9930 Treatmentofcomplications(post-surgical) ................... 43D9940 Occlusal guard, by report ............................................ 272D9950 Occlusion analysis - mounted case ............................ 104D9951 Occlusal adjustment - limited ........................................ 66D9952 Occlusal adjustment - complete .................................. 266D9986 Missed appointment ...................................................... 50D9995 Teledentistry – synchronous; real-time encounter (whenavailable) ........................................................ 20 D9996 Teledentistry – asynchronous; information stored and forwarded to dentist for subsequent review (whenavailable) ........................................................ 20 ENDODONTICS1 D3220 Therapeuticpulpotomy(excl.finalrestor.) .................... 81D3221 Pulpal debridement, prim. and perm. teeth ................... 94D3222 Partial pulpotomy for apexogenesis ............................ 160D3230 Pulpaltherapy-resorbablefilling,anterior ................. 160D3240 Pulpaltherapy-resorbablefilling,posterior ................ 164D3310 Endodontic therapy, anterior tooth .............................. 341D3320 Endodontic therapy, bicuspid tooth ............................. 418D3330 Endodontic therapy, molar .......................................... 512D3332 Incomp. endo. therapy-inop. or fractured tooth ........... 183D3333 Internal root repair of perforation defects .................... 105D3346 Retreat of prev. root canal therapy, anterior ................ 387D3347 Retreat of prev. root canal therapy, bicuspid ............... 465D3348 Retreat of prev. root canal therapy, molar ................... 558D3351 Apexification/recalcification-initialvisit ...................... 202D3352 Apexification/recalcification-interimmed.repl. .......... 589D3353 Apexification/recalcification-finalvisit ........................ 449D3355 Pulpal regeneration - initial visit .................................. 202D3356 Pulpal regeneration - interim medication replacement ....589D3357 Pulpal regeneration - completion of treatment ............ 449D3410 Apicoectomy, anterior ................................................. 323D3421 Apicoectomy,bicuspid(firstroot) ......................................364D3425 Apicoectomy,molar(firstroot) .................................... 418D3426 Apicoectomy,(eachadd.root) .................................... 152D3427 Periradicular surgery w/o apicoectomy ....................... 266D3428 Bone graft in conj. w/ periradicular surg., per tooth, single site ................................................ 743D3429 Bone graft in conj. w/ periradicular surg., add. contiguous tooth, same site ............................ 582D3430 Retrogradefilling-perroot ......................................... 119D3431 Biologic materials to aid soft/osseous tissue regen. in conj. w/ periradicular surg. ....................... 407D3432 Guided tissue regen., resorbable barrier, per site, in conj. w/ periradicular surg. ..................... 815D3450 Root amputation - per root .......................................... 234D3920 Hemisection, not inc. root canal therapy ..................... 234D3950 Canalprep/fittingofpreformeddowelorpost ............. 136
PERIODONTICS1
D0180 Comp. periodontal eval - new or established patient ...... 0D4210 Gingivectomy or gingivoplasty - >3 cont. teeth, per quad. ......................................... 279D4211 Gingivectomy or gingivoplasty - <=3 teeth, per quad. .. 100D4212 Gingivectomy or gingivoplasty, rest., per tooth ............. 40D4240 Gingivalflapproc.,inc.rootplaning- >3 cont. teeth, per quad .......................................... 345D4241 Gingivalflapproc,inc.rootplaning- <=3 cont. teeth, per quad ........................................ 106D4260 Osseous surgery - >3 cont. teeth, per quad ............... 499D4261 Osseous surgery - <=3 cont. teeth, per quad ............. 392D4263 Bonereplacementgraft-retainednaturaltooth-first site in quad. .............................................................. 743D4264 Bone replacement graft - retained natural tooth - each add. site in quad. ...................................................... 582D4265 Biologic materials ........................................................ 407D4266 Guided tissue regen. - resorb. barrier, per site ........... 815
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.

ADA MEMBERCODE BENEFIT COPAYMENT(S)
1 Specialty care is provided at the listed copayment whether performed by a Participating General Dentist or a Participating Specialist. Referrals to a specialist must be made by a member’s Participating General Dentist. See Plan Exclusion #13.2 Phase I Treatment (D8010 - D8050) is provided at a 15% reduction from the orthodontist’s UCR fees. See exclusion #15 and limitation #24 for additional coverage information.
Only current ADA CDT codes are considered valid by Dominion NationalCurrent Dental Terminology © American Dental Association.
D4267 Guided tissue regen. - non-resorb. barrier, per site .... 797D4268 Surgical revision proc., per tooth ................................ 358D4270 Pedicle soft tissue graft procedure .............................. 643D4273 Subepithelial connective tissue graft proc. .................. 800D4274 Mesial/distal wedge procedure, single tooth ............... 308D4275 Soft tissue allograft ..................................................... 854D4276 Comb. connec. tissue/double pedicle graft, per tooth .. 1019D4320 Provisional splinting - intracoronal .............................. 427D4321 Provisional splinting - extracoronal ............................. 377D4341 Perio scaling and root planing - >3 cont teeth, per quad. .. 109D4342 Perio scaling and root planing - <= 3 teeth, per quad ... 63D4346 Scaling in presence of generalized moderate or severe gingivalinflammation-fullmouth,afteroralevaluation ..45 D4355 Full mouth debridement ................................................ 89D4381 Localized delivery of chemotherapeutic agents ............ 98D4910 Periodontal maintenance .............................................. 74D4920 Unscheduled dressing change by non-treating dentist ... 84 ORAL SURGERY1
D7111 Extraction, coronal remnants - deciduous tooth ............ 56D7140 Extraction, erupted tooth or exposed root ..................... 69D7210 Extraction, erupted tooth req elev, etc ........................... 133D7220 Removal of impacted tooth - soft tissue ...................... 151D7230 Removal of impacted tooth - partially bony ................. 196D7240 Removal of impacted tooth - completely bony ............ 241D7241 Removal of imp. tooth - completely bony, with unusual surg. complications ............................ 217D7250 Removal of residual tooth roots .................................. 141D7251 Coronectomy-intentional partial tooth removal ........... 217 D7270 Tooth reimplant./stabiliz. of acc. evulsed/displaced tooth .. 226D7272 Tooth transplantation ................................................... 615D7280 Exposure of an unerupted tooth .................................. 153D7282 Mobil. of erupted/malpositioned tooth to aid eruption ... 231D7283 Place. of device to facilitate erupt. of impacted tooth.... 144D7291 Transseptalfiberotomy/supracrestalfiberotomy,byreport ... 60D7310/20 Alveoloplasty in conj. with/out extractions, per quad. . 141D7340 Vestibuloplasty - ridge ext. sec. epithel. ...................... 923D7350 Vestibuloplasty - ridge ext. inc. grafts, etc ................. 1776D7510 Incision and drainage of abscess - intraoral soft tissue ..... 96D7511 Incision/drainage of abscess - intra. soft tissue, comp. . 112D7520 Incision/drainage of abscess - extra. soft tissue ......... 116D7521 Incision/drainage of abscess - extra. soft tissue, comp. ..120D7910 Suture of recent small wounds up to 5 cm .................... 59D7911 Complicated suture, <= 5 cm ........................................ 69D7912 Complicated suture, > 5 cm .......................................... 79D7960 Frenulectomy(frenectomy/frenotomy)-separateproc... 263D7963 Frenuloplasty .............................................................. 293D7970 Excision of hyperplastic tissue - per arch .................... 233D7971 Excision of pericoronal gingiva ................................... 131 ORTHODONTICS2 - PRE-AUTHORIZATION REQUIREDD8060 Interceptive ortho. treatment - transitional dentition .... 3304D8070 Comp. ortho. treatment - transitional dentition .......... 3304D8080 Comp. ortho. treatment - adolescent dentition .......... 3422D8090 Comp. ortho. treatment - adult dentition ................... 3658D8660 Pre-orthodontic treatment visit .................................... 413D8670 Periodicortho.treatmentvisit(aspartofcontract) ..... 118D8680 Ortho.ret.(rem.ofappl./placementofretainer(s)) ..... 413D8692 Replacement of lost or broken retainer ....................... 179

Plan Exclusions1. Services which are covered under worker’s compensation or employer’s liability laws.2. Services which are not necessary for the patient’s dental health as determined by the Plan.3. Cosmetic, elective or aesthetic dentistry except as required due to accidental bodily injury to sound natural teeth as determined by the Plan.4. Oral surgery requiring the setting of fractures or dislocations.5. Services with respect to malignancies, cysts or neoplasms, hereditary, congenital, mandibular prognathism or development malformations where,intheopinionofthePlan,suchservicesshouldnotbeperformedinadentaloffice.6. Dispensing of drugs.7. Hospitalization for any dental procedure.8. Treatment required for conditions resulting from major disaster, epidemic, war, acts of war, whether declared or undeclared, or while on active duty as a member of the armed forces of any nation.9. Replacement due to loss or theft of prosthetic appliance.10. ProceduresnotlistedascoveredbenefitsunderthisPlan.11. ServicesobtainedoutsideofthedentalofficeinwhichenrolledandthatarenotpreauthorizedbysuchofficeorthePlan(withtheexception ofout-of-areaemergencydentalservices).12. ServicesrelatedtothetreatmentofTMD(TemporomandibularDisorder)exceptifTMDiscausedbysevere,dysfunctional,handicapping malocclusion that requires medically necessary orthodontia services.13. ServicesperformedbyaParticipatingSpecialistwithoutareferralfromaParticipatingGeneralDentist(withtheexceptionofOrthodontics). Participating dentists should refer to Specialty Care Referral Guidelines.14. Elective surgery including, but not limited to, extraction of non-pathologic, asymptomatic impacted teeth as determined by the Plan. The prophylactic removal of these teeth for medically necessary orthodontia services may be covered subject to review.15. Non-medicallynecessaryorthodontiaandPhaseITreatmentformedicallynecessaryorthodontiaarenotcoveredbenefitsunderthis policy. Discounts are provided to members through the Plan’s agreements with its participating orthodontists. The provider agreements create no liability for payment by the Plan, and payments by the member for these services do not contribute to the Out-of-Pocket Maximum.TheInvisalignsystemandsimilarspecializedbracesarenotacoveredbenefit.Seelimitation#24concerningmedically necessary orthodontia.
Plan Limitations1. One(1)evaluation(D0120,D0145,D0150orD0160)persix(6)months,perpatient.2. One(1)teethcleaning(D1110orD1120)persix(6)months,perpatient.3. Onefluoridetreatmentpersix(6)months,perpatient.4. Fourbitewingx-rayfilmspersix(6)months,perpatient.5. One(1)setoffullmouthx-raysorpanoramicfilmiscoveredeverythree(3)years.6. Onesealantpertooth,perpatientuptoage19(limitedtoocclusalsurfacesofposteriorpermanentteethwithoutrestorationsordecay).7. Onefixedspacemaintainer(D1510,D1515)per5years,perarch,perpatientuptoage14,topreservespacebetweenteethfor prematurelossofaprimarytooth(doesnotincludeusefororthodontictreatment).D1575limitedtoonceperlifetime.8. Replacementofafillingiscoveredifitismorethantwo(2)yearsfromthedateoforiginalplacement.9. Replacementofacrown(forteethwithextensivecariesorfracturethatisunabletoberestoredwithanamalgamorcompositefilling), bridge(thatcannotberepaired)ordentureiscoveredifitismorethanfive(5)yearsfromthedateoforiginalplacementandcannotbe restored.10. Crownandbridgefeesapplytotreatmentinvolvingfive(5)orfewerunitswhenpresentedinasingletreatmentplan.Additionalcrownor bridgeunits,beginningwiththesixthunit,areavailableattheprovider’sUsual,Customary,andReasonable(UCR)fee,minus25%.11. Reliningandrebasingofdenturesiscoveredonceper24months,perpatient,onlyaftersix(6)monthsofinitialplacement.12. Periodontalscalingandrootplaning(D4341orD4342),osseoussurgery(D4260orD4261)andgingivectomyorgingivoplasy(D4210or D4211)arelimitedtoone(1)perpatient,perquadrant.13. Scalinginpresenceofgeneralizedmoderateorseveregingivalinflammation-fullmouth,afteroralevaluationandinlieuofacovered D1120/D1110, limited to once per two years.14. Full mouth debridement is covered once per 36 months, per patient.15. ProcedureCodeD4381islimitedtoone(1)benefitpertoothforthreeteethperquadrant;oratotalof12teethforallfourquadrantsper twelve(12)months.Musthavepocketdepthsoffive(5)millimetersorgreater.16. Periodontal surgery of any type, including any associated material, is covered once every 24 months, per quadrant or surgical site.17. Periodontalmaintenancefollowingsurgery(D4341isnotconsideredsurgery)iscoveredonceperthree(3)months.18. All dental services that are to be rendered in a hospital setting require coordination and approval from both the dental insurer and the medical insurer before services can be rendered. Services delivered to the patient on the date of service are documented separately using applicable procedure codes.19. Coronectomy,intentionalpartialtoothremoval,one(1)perlifetime. 20. Anesthesia requires a narrative of medical necessity be maintained in patient records. A maximum of 60 minutes of services are allowed for general anesthesia and intravenous or non-intravenous conscious sedation. General anesthesia is not covered with procedure codes D9230 or D9243. Intravenous conscious sedation is not covered with procedure codes D9223 or D9230. Nonintravenous conscious sedation is not coveredwithprocedurecodesD9223orD9230.Analgesia(nitrousoxide)isnotcoveredwithprocedurecodesD9223orD9243.21. Occlusal guard with covered surgery, by report.22. Gingivectomy, once per quadrant.23. One pedicle, free soft tissue, subepithelial connective tissue or double pedicle graft per site.24. Orthodontics is only covered if medically necessary as determined by the Plan. Patient copayments will apply to the routine orthodontic appliance portion of services only. Additional costs incurred will become the patient’s responsibility.
Exclusions & Limitations

DMNMD18DBLINDPEDEHB All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.
Annual Out-of-Pocket Maximum: $350 per child per calendar year for medically necessary treatment (maximum of $700 for policy covering two or more children)For any medically necessary treatments in which the member copayment listed below is over the annual out-of-pocket maximum, the member shall only be responsible up to the maximum and the Plan would be responsible for the remainder.
D2335 Resin-based composite - >=4 surfaces, anterior .......... 119D2390 Resin-based composite crown, anterior ........................192D2391 Resin-based composite - one surface, posterior .............73D2392 Resin-based composite - two surfaces, posterior ...........87D2393 Resin-based composite - three surfaces, posterior .......102D2394 Resin-based composite - >=4 surfaces, posterior .........123 D2940 Protective restoration ......................................................39D2950 Core buildup, including any pins ...................................125D2951 Pin retention - per tooth, in addition to restoration ..........22D3110/20 Pulpcap-direct/indirect(excl.finalrestoration) .............32 CROWNS & BRIDGES♦
D2510 Inlay- metallic - one surface ..........................................407D2520 Inlay- metallic - two surfaces .........................................407D2530 Inlay - metallic - three or more surfaces ........................425D2542 Onlay - metallic-two surfaces ........................................458D2543 Onlay - metallic - three surfaces ...................................524D2544 Onlay - metallic - four or more surfaces ........................524D2610 Inlay - porcelain/ceramic - one surface .........................427D2620 Inlay - porcelain/ceramic - two surfaces ........................427D2630 Inlay - porcelain/ceramic - >=3 surfaces .......................445D2642 Onlay - porcelain/ceramic - two surfaces ......................479D2643/44 Onlay - porcelain/ceramic - >=3 surfaces .....................499D2650/51/52 Inlay-resin-basedcomposite->=1surface(s) .............440D2662/63/64 Onlay - resin-based composite - >=2 surfaces .............444D2710 Crown-resinbasedcomposite(indirect) ......................272D2712 Crown-3/4resin-basedcomposite(indirect) ...............485D2720/21/22 Crown - resin with metal ................................................495D2740 Crown - porcelain/ceramic substrate .............................560D2750/51/52 Crown - porcelain fused to metal ..................................523D2780/81/82 Crown - 3/4 cast with metal ...........................................478D2783 Crown - 3/4 porcelain/ceramic ...................................... 511D2790-94 Crown - full cast metal ...................................................495D2910/20 Recement inlay, onlay/crown or partial coverage rest. ......43D2930 Prefab. stainless steel crown - prim. tooth .................... 110D2931 Prefab. stainless steel crown - perm. tooth ...................121D2932 Prefabricated resin crown .............................................140D2933 Prefab. stainless steel crown w/ resin window ..............271D2934 Prefab. esthetic coated primary tooth ...........................296D2941 Interim therapeutic restoration, primary dentition ............31D2952 Cast post and core in addition to crown ........................186D2954 Prefab. post and core in addition to crown ....................154D2955 Postremoval(notinconj.withendo.therapy) ..............105D2960 Labialveneer(resinlaminate)-chairside .....................434D2961 Labialveneer(resinlaminate)-laboratory ....................601D2962 Labialveneer(porcelainlaminate)-laboratory .............449D2970 Temporarycrown(fracturedtooth) ....................................0D2980 Crown repair, by report ..................................................102 PROSTHETICS (DENTURES)D5110/20 Complete denture - maxillary/mandibular .....................697D5130/40 Immediate denture - maxillary/mandibular ....................722D5211/12 Maxillary/mandibular partial denture - resin base .........649D5213/14 Maxillary/mandibular partial denture - cast metal ..........750D5221/22 Immediate maxillary/mandibular partial denture - resin base ..............................................................649D5223/24 Immediate maxillary/mandibular partial denture - cast metal ...............................................................750
D9439 Officevisit ........................................................................10 DIAGNOSTIC/PREVENTIVED0120 Periodic oral eval - established patient .............................0D0140 Limited oral eval - problem focused ..................................0D0145 Oral eval for a patient under 3 years of age ......................0D0150 Comprehensive oral eval - new or established patient .....0D0160 Detailed and extensive oral eval - problem focused .........0D0170 Re-evaluation - limited, problem focused ..........................0D0210 Intraoral-completeseries(includingbitewings) .............26D0220/30 Intraoral-periapicalfirstradiographicimage/eachadd. ...0D0240 Intraoral - occlusal radiographic image .............................0D0250 Extraoral - 2D projection radiographic image ....................0D0270 Bitewing - 1 radiographic image ........................................0D0272 Bitewing - 2 radiographic images ......................................0D0273 Bitewing - 3 radiographic images ......................................0D0274 Bitewing - 4 radiographic images ......................................0D0277 Vertical bitewings - 7 to 8 radiographic images .................0D0290 Posterior/anterior or lateral skull bone radiographic image .........................................................................83D0310 Sialography ...................................................................370D0320 Temporomandibular joint arthrogram, incl. injection ......562D0321 Other temporomandibular joint radiographic images, by report ...................................................................120D0330 Panoramic radiographic image .......................................30D0340 2D cephalometric radiographic image ...............................0D0350 2Doral/facialphotographicimages(intraoral/extraoral) ...0D0351 3D photographic image .....................................................0D0460 Pulp vitality tests ...............................................................0D0470 Diagnostic casts ................................................................0D0486 Accession of Brush Biopsy Sample ..................................0D1110 Prophylaxis(cleaning)-adult ............................................0D1120 Prophylaxis(cleaning)-child ............................................0D1206 Topicalfluoridevarnishformod/highriskcariespatients ......0D1208 Topicalapplicationoffluoride ............................................0D1310 Nutritional counseling for control of dental disease ...........0D1320/30 Oral hygiene instructions ...................................................0D1351 Sealant - per tooth ...........................................................21D1352 Prev resin rest. mod/high caries risk – perm. tooth .........21 SPACE MAINTAINERSD1510/20 Spacemaintainer-fixed/removable-unilateral ............143D1515/25 Spacemaintainer-fixed/removable-bilateral ..............198D1550 Re-cementation of space maintainer ..............................34D1555 Removaloffixedspacemaintainer, by non-originating dentist ..........................................44D1575 Distalshoespacemaintainer-fixed-unilateral ...........143 RESTORATIVE DENTISTRY (FILLINGS) AMALGAMRESTORATIONS(SILVER)D2140 Amalgam - one surface, prim. or perm. ...........................41D2150 Amalgam - two surfaces, prim. or perm. .........................51D2160 Amalgam - three surfaces, prim. or perm. .......................64D2161 Amalgam - >=4 surfaces, prim. or perm. .........................78 RESIN/COMPOSITERESTORATIONS(TOOTHCOLORED) ...D2330 Resin-based composite - one surface, anterior ..............69D2331 Resin-based composite - two surfaces, anterior .............83D2332 Resin-based composite - three surfaces, anterior ..........99
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
Select Plan Basic Kids 702xs (MD)Description of Benefits & Member Copayments for Pediatric Services (under age 19)
Coverage continues through end of month in which the Member turns 19.
The dental plan is underwritten by Dominion Dental Services, Inc. d/b/a Dominion National.

ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
D5225/26 Maxillary/mandibularpartialdenture-flexiblebase ......750D5281 Rem. unilateral partial denture - one piece cast metal ..... 419D5410/11 Adjust complete denture - maxillary/mandibular .............38D5421/22 Adjust partial denture - maxillary/mandibular ..................38D5510/5610 Repairbrokencompletedenturebase(complete/resin) ......87D5520 Replace missing or broken teeth - complete denture ......87D5620 Repair cast framework ....................................................87D5630/60 Clasp repaired, replaced or added ................................ 115D5640 Replace broken teeth - per tooth .....................................87D5650 Add tooth to existing partial denture ................................87D5670/71 Replace all teeth/acrylic on cast metal framework (maxillary/mandibular) ..............................................287D5710/11 Rebase complete maxillary/mandibular denture ...........260D5720/21 Rebase maxillary/mandibular partial denture ................260D5730/31 Relinecompletemaxillary/mandibulardenture(chairside) .....159D5740/41 Relinemaxillary/mandibularpartialdenture(chairside) .... 155D5750/51 Relinecompletemaxillary/mandibulardenture(lab) .....224D5760/61 Relinemaxillary/mandibularpartialdenture(lab) ..........224D5810/11 Interim complete denture - maxillary/mandibular ..........362D5820/21 Interim partial denture - maxillary/mandibular ...............362D5850/51 Tissue conditioning - maxillary/mandibular .....................79D5863/65 Overdenture - complete maxillary/mandibular ............1694D5864/66 Overdenture - partial maxillary/mandibular .................1668D5992 Adjustment of prosthetic appliance, by report .................24D5993 Cleaning and maintenance prosthetic appliance ............18 BRIDGES & PONTICS♦
D6058 Abutment supported porcelain/ceramic crown ..............560D6059/60/61 Abutment supported porcelain fused to metal crown .....523D6066 Implant supported porcelain fused to metal crown - titanium, titanium allow, high noble metal .................523D6081 Scaling and debridement in the presence of inflammationormucositisofasingleimplant, including cleaning of the implant surfaces, without flapentryandclosure .................................................63D6210/11/12 Pontic - cast high noble metal .......................................495D6240/41/42 Pontic - porcelain fused metal .......................................523D6245 Pontic - porcelain/ceramic .............................................560D6250/51/52 Pontic - resin with metal ................................................495D6545 Ret.-castmetalforresinbondedfixedprosthesis .......251D6548 Ret.-porc./ceramicforresinbondedfixedprosthesis ......393D6549 Resinretainer-forresinbondedfixedprosthesis .........251D6600 Inlay - porc./ceramic, two surfaces ................................427D6601 Inlay - porc./ceramic, >=3 surfaces ...............................445D6602 Inlay - cast high noble metal, two surfaces ...................407D6603 Inlay - cast high noble metal, >=3 surfaces ...................425D6604 Inlay - cast predominantly base metal, two surfaces ......407D6605 Inlay - cast predominantly base metal, >=3 surfaces ......425D6606 Inlay - cast noble metal, two surfaces ...........................407D6607 Inlay - cast noble metal, >=3 surfaces ..........................425D6608 Onlay -porc./ceramic, two surfaces ...............................479D6609 Onlay - porc./ceramic, three or more surfaces ..............499D6610 Onlay - cast high noble metal, two surfaces .................458D6611 Onlay - cast high noble metal, >=3 surfaces .................524D6612 Onlay - cast predominantly base metal, two surfaces .....458D6613 Onlay - cast predominantly base metal, >=3 surfaces ......524D6614 Onlay - cast noble metal, two surfaces .........................458D6615 Onlay - cast noble metal, >=3 surfaces .........................524D6720/21/22 Crown - resin with metal ................................................495D6740 Crown - porcelain/ceramic ............................................560D6750/51/52 Crown - porcelain fused metal ......................................523D6780 Crown - 3/4 cast high noble metal .................................470D6781 Crown - 3/4 cast predominantly base metal ..................470D6782 Crown - 3/4 cast noble metal ........................................470D6783 Crown - 3/4 porc./ceramic ............................................. 511D6790/91/92 Crown - full cast metal ...................................................495D6930 Recementfixedpartialdenture .......................................69D6980 Fixed partial denture repair, by report ...........................172
ADJUNCTIVE GENERAL SERVICESD9110 Palliative(emergency)treatmentofdentalpain ..............43D9210/15 Local anesthesia ...............................................................0D9211/12 Regional block anesthesia ................................................0D9223 Deep sedation/general anesthesia - each 15 min. ............103D9230 Analgesia, anxiolysis, inhalation of nitrous oxide ............37D9243 Intravenous conscious sedation/analgesia - each 15 min. ..103D9248 Non-intravenous conscious sedation ............................145D9310 Consultation(diagnosticservicebynontreatingdentist) ......43D9410 House/extended care facility call ...................................200D9420 Hospital call ...................................................................350D9910 Application of desensitizing medicament ........................31D9930 Treatmentofcomplications(post-surgical) .....................43D9940 Occlusal guard, by report ..............................................272D9941 Fabrication of athletic mouthguard ................................102D9950 Occlusion analysis - mounted case ...............................104D9951 Occlusal adjustment - limited ..........................................66D9952 Occlusal adjustment - complete ....................................266D9986 Missed appointment ........................................................50 D9995 Teledentistry – synchronous; real-time encounter (whenavailable) ..........................................................20 D9996 Teledentistry – asynchronous; information stored and forwarded to dentist for subsequent review (whenavailable) ...............................................................20 ENDODONTICS1
D3220 Therapeuticpulpotomy(excl.finalrestor.) ......................81D3221 Pulpal debridement, prim. and perm. teeth .....................94D3230 Pulpaltherapy-resorbablefilling,anterior ....................160D3240 Pulpaltherapy-resorbablefilling,posterior ..................164D3310 Endodontic therapy, anterior tooth ................................341D3320 Endodontic therapy, bicuspid tooth ...............................418D3330 Endodontic therapy, molar.............................................512D3332 Incomp. endo. Therapy-inop. or fractured tooth ............183D3333 Internal root repair of perforation defects ......................105D3346 Retreat of prev. root canal therapy, anterior ..................387D3347 Retreat of prev. root canal therapy, bicuspid .................465D3348 Retreat of prev. root canal therapy, molar .....................558D3351 Apexification/recalcification-initialvisit ........................202D3352 Apexification/recalcification-interimmed.repl. ............589D3353 Apexification/recalcification-finalvisit ..........................449D3355 Pulpal regeneration - initial visit ....................................202D3356 Pulpal regeneration - interim medication replacement ......589D3357 Pulpal regeneration - completion of treatment ..............449D3410 Apicoectomy, anterior ....................................................323D3421 Apicoectomy,bicuspid(firstroot) .....................................364D3425 Apicoectomy,molar(firstroot).......................................418D3426 Apicoectomy(eachadditionalroot) ...............................152D3427 Periradicular surgery w/o apicoectomy .........................266D3430 Retrogradefilling-perroot ........................................... 119D3450 Rootamputation(resection)-perroot ..........................234D3470 Intentional reimplantation ..............................................718D3920 Hemisection, not inc. root canal therapy .......................234D3950 Canalprep/fittingofpreformeddowelorpost ...............136 PERIODONTICS1
D0180 Comp. periodontal eval - new or established patient ........0D4210 Gingivectomy or gingivoplasty - >3 cont. teeth, per quad. ..........................................279D4211 Gingivectomy or gingivoplasty - <=3 teeth, per quad. .....100D4230 Anatomical crown exposure, >=4 teeth per quad. .........454D4231 Anatomical crown exposure, 1-3 teeth per quad. ..........424D4240 Gingivalflapproc.,inc.rootplaning- >3 cont. teeth, per quad ...........................................345D4241 Gingivalflapproc,inc.rootplaning- <=3 cont. teeth, per quad .........................................106D4249 Clinical crown lengthening - hard tissue ........................576D4260 Osseous surgery - >3 cont. teeth, per quad ..................499D4261 Osseous surgery - <=3 cont. teeth, per quad ................392
All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.

ADA MEMBERCODE BENEFIT COPAYMENT(S)
1 Specialty care is provided at the listed copayment whether performed by a Participating General Dentist or a Participating Specialist. Referrals to a specialist must be made by a member’s Participating General Dentist. See Plan Exclusion #12.
2 See exclusion #15 and limitation #24 for additional coverage information.
Only current ADA CDT codes are considered valid by Dominion NationalCurrent Dental Terminology © American Dental Association.
D4268 Surgical revision proc., per tooth ...................................358D4274 Mesial/distal wedge procedure, single tooth .................308D4320 Provisional splinting - intracoronal ................................427D4321 Provisional splinting - extracoronal ...............................377D4341 Perio scaling and root planing - >3 cont teeth, per quad. ....109D4342 Perio scaling and root planing - <= 3 teeth, per quad .....63 D4346 Scaling in presence of generalized moderate or severe gingivalinflammation-fullmouth,after oral evaluation ............................................................45D4355 Full mouth debridement ..................................................89D4381 Localized delivery of chemotherapeutic agents ..............98D4910 Periodontal maintenance ................................................74D4920 Unscheduled dressing change by non-treating dentist ..... 84 ORAL SURGERY1
D7111 Extraction, coronal remnants - deciduous tooth ..............56D7140 Extraction, erupted tooth or exposed root .......................69D7210 Extraction, erupted tooth req. bone cut .........................133D7220 Removal of impacted tooth - soft tissue ........................151D7230 Removal of impacted tooth - partially bony ...................196D7240 Removal of impacted tooth - completely bony ..............241D7241 Removal of imp. tooth - completely bony, with unusual surg. complications .............................217D7250 Removal of residual tooth roots ....................................141D7251 Coronectomy-intentional partial tooth removal ..............217D7260 Oroantralfistulaclosure ................................................578D7270 Tooth reimplant./stabiliz. of acc. evulsed/displaced tooth ......226D7272 Tooth transplantation .....................................................615D7280 Exposure of an unerupted tooth ....................................153D7285 Biopsyoforaltissue-hard(bone,tooth) ......................387D7286 Biopsyoforaltissue-soft(allothers) ...........................295D7290 Surgical repositioning of teeth .......................................407D7291 Transseptalfiberotomy/supracrestalfiberotomy,byreport......60D7310/20 Alveoloplasty, per quadrant ...........................................141D7311/21 Alveoloplasty in conj. with/out extractions .....................141D7340 Vestibuloplasty - ridge ext. sec. epithel. ........................923D7350 Vestibuloplasty - ridge ext. inc. grafts, etc ...................1776D7410 Excision of benign lesion up to 1.25 cm ........................278D7440 Exc. of malignant tumor- lesion diam. <=1.25cm ..........608D7450 Removal of benign odon cyst/tumor - diam <=1.25cm .....354D7451 Removal of benign odon cyst/tumor - diam >1.25cm ....543D7460 Removal of benign nonodon cyst/tumor-diam <=1.25cm .....516D7461 Removal of benign nonodon cyst/tumor-diam >1.25cm ....718D7471 Removal of lateral exostosis .........................................351D7472/73 Removal of torus palatinus/mandibularis ......................480D7510 Incision and drainage of abscess - intraoral soft tissue .....96D7520 Incision/drainage of abscess - extra. soft tissue ........... 116D7550 Partial ostect/sequestrect non-vital bone rem. ..............336D7960 Frenulectomy(frenectomy/frenotomy)-separateproc. ....263D7970 Excision of hyperplastic tissue - per arch ......................233D7971 Excision of pericoronal gingiva ......................................131 ORTHODONTICS2 - PRE-AUTHORIZATION REQUIREDD8070 Comp. ortho. treatment - transitional dentition ............3304D8080 Comp. ortho. treatment - adolescent dentition ............3422D8090 Comp. ortho. treatment - adult dentition ......................3658D8660 Pre-orthodontic treatment visit ......................................413D8670 Periodicortho.treatmentvisit(aspartofcontract) ....... 118D8680 Orthodonticret.(rem.ofappl./placementofretainer(s)) ....413D8692 Replacement of lost or broken retainer .........................179D8693 Rebondingorrecementingfixeddentures ....................174D8694 Repairoffixedretainers,includesreattachment ...........174
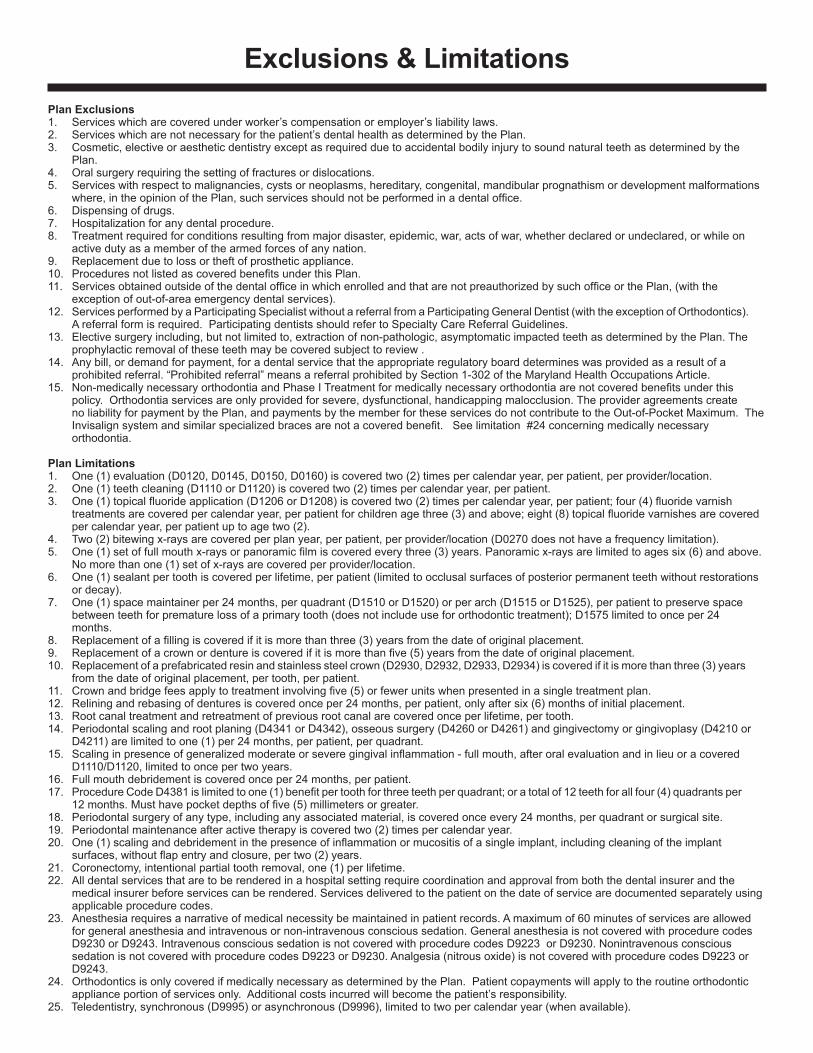
Plan Exclusions1. Services which are covered under worker’s compensation or employer’s liability laws.2. Services which are not necessary for the patient’s dental health as determined by the Plan.3. Cosmetic, elective or aesthetic dentistry except as required due to accidental bodily injury to sound natural teeth as determined by the Plan.4. Oral surgery requiring the setting of fractures or dislocations.5. Services with respect to malignancies, cysts or neoplasms, hereditary, congenital, mandibular prognathism or development malformations where,intheopinionofthePlan,suchservicesshouldnotbeperformedinadentaloffice.6. Dispensing of drugs.7. Hospitalization for any dental procedure.8. Treatment required for conditions resulting from major disaster, epidemic, war, acts of war, whether declared or undeclared, or while on active duty as a member of the armed forces of any nation.9. Replacement due to loss or theft of prosthetic appliance.10. ProceduresnotlistedascoveredbenefitsunderthisPlan.11. ServicesobtainedoutsideofthedentalofficeinwhichenrolledandthatarenotpreauthorizedbysuchofficeorthePlan,(withthe exceptionofout-of-areaemergencydentalservices).12. ServicesperformedbyaParticipatingSpecialistwithoutareferralfromaParticipatingGeneralDentist(withtheexceptionofOrthodontics). A referral form is required. Participating dentists should refer to Specialty Care Referral Guidelines.13. Elective surgery including, but not limited to, extraction of non-pathologic, asymptomatic impacted teeth as determined by the Plan. The prophylactic removal of these teeth may be covered subject to review .14. Any bill, or demand for payment, for a dental service that the appropriate regulatory board determines was provided as a result of a prohibited referral. “Prohibited referral” means a referral prohibited by Section 1-302 of the Maryland Health Occupations Article.15. Non-medicallynecessaryorthodontiaandPhaseITreatmentformedicallynecessaryorthodontiaarenotcoveredbenefitsunderthis policy. Orthodontia services are only provided for severe, dysfunctional, handicapping malocclusion. The provider agreements create no liability for payment by the Plan, and payments by the member for these services do not contribute to the Out-of-Pocket Maximum. The Invisalignsystemandsimilarspecializedbracesarenotacoveredbenefit.Seelimitation#24concerningmedicallynecessary orthodontia.
Plan Limitations1. One(1)evaluation(D0120,D0145,D0150,D0160)iscoveredtwo(2)timespercalendaryear,perpatient,perprovider/location.2. One(1)teethcleaning(D1110orD1120)iscoveredtwo(2)timespercalendaryear,perpatient.3. One(1)topicalfluorideapplication(D1206orD1208)iscoveredtwo(2)timespercalendaryear,perpatient;four(4)fluoridevarnish treatmentsarecoveredpercalendaryear,perpatientforchildrenagethree(3)andabove;eight(8)topicalfluoridevarnishesarecovered percalendaryear,perpatientuptoagetwo(2).4. Two(2)bitewingx-raysarecoveredperplanyear,perpatient,perprovider/location(D0270doesnothaveafrequencylimitation).5. One(1)setoffullmouthx-raysorpanoramicfilmiscoveredeverythree(3)years.Panoramicx-raysarelimitedtoagessix(6)andabove. Nomorethanone(1)setofx-raysarecoveredperprovider/location.6. One(1)sealantpertoothiscoveredperlifetime,perpatient(limitedtoocclusalsurfacesofposteriorpermanentteethwithoutrestorations ordecay).7. One(1)spacemaintainerper24months,perquadrant(D1510orD1520)orperarch(D1515orD1525),perpatienttopreservespace betweenteethforprematurelossofaprimarytooth(doesnotincludeusefororthodontictreatment);D1575limitedtoonceper24 months. 8. Replacementofafillingiscoveredifitismorethanthree(3)yearsfromthedateoforiginalplacement.9. Replacementofacrownordentureiscoveredifitismorethanfive(5)yearsfromthedateoforiginalplacement.10. Replacementofaprefabricatedresinandstainlesssteelcrown(D2930,D2932,D2933,D2934)iscoveredifitismorethanthree(3)years from the date of original placement, per tooth, per patient.11. Crownandbridgefeesapplytotreatmentinvolvingfive(5)orfewerunitswhenpresentedinasingletreatmentplan.12. Reliningandrebasingofdenturesiscoveredonceper24months,perpatient,onlyaftersix(6)monthsofinitialplacement.13. Root canal treatment and retreatment of previous root canal are covered once per lifetime, per tooth.14. Periodontalscalingandrootplaning(D4341orD4342),osseoussurgery(D4260orD4261)andgingivectomyorgingivoplasy(D4210or D4211)arelimitedtoone(1)per24months,perpatient,perquadrant.15. Scalinginpresenceofgeneralizedmoderateorseveregingivalinflammation-fullmouth,afteroralevaluationandinlieuoracovered D1110/D1120, limited to once per two years. 16. Full mouth debridement is covered once per 24 months, per patient.17. ProcedureCodeD4381islimitedtoone(1)benefitpertoothforthreeteethperquadrant;oratotalof12teethforallfour(4)quadrantsper 12months.Musthavepocketdepthsoffive(5)millimetersorgreater.18. Periodontal surgery of any type, including any associated material, is covered once every 24 months, per quadrant or surgical site.19. Periodontalmaintenanceafteractivetherapyiscoveredtwo(2)timespercalendaryear.20. One(1)scalinganddebridementinthepresenceofinflammationormucositisofasingleimplant,includingcleaningoftheimplant surfaces,withoutflapentryandclosure,pertwo(2)years.21. Coronectomy,intentionalpartialtoothremoval,one(1)perlifetime.22. All dental services that are to be rendered in a hospital setting require coordination and approval from both the dental insurer and the medical insurer before services can be rendered. Services delivered to the patient on the date of service are documented separately using applicable procedure codes.23. Anesthesia requires a narrative of medical necessity be maintained in patient records. A maximum of 60 minutes of services are allowed for general anesthesia and intravenous or non-intravenous conscious sedation. General anesthesia is not covered with procedure codes D9230 or D9243. Intravenous conscious sedation is not covered with procedure codes D9223 or D9230. Nonintravenous conscious sedationisnotcoveredwithprocedurecodesD9223orD9230.Analgesia(nitrousoxide)isnotcoveredwithprocedurecodesD9223or D9243.24. Orthodontics is only covered if medically necessary as determined by the Plan. Patient copayments will apply to the routine orthodontic appliance portion of services only. Additional costs incurred will become the patient’s responsibility. 25.Teledentistry,synchronous(D9995)orasynchronous(D9996),limitedtotwopercalendaryear(whenavailable).
Exclusions & Limitations

D9439 Officevisit ...............................................................................................................10 ............................................................ 10 DIAGNOSTIC/PREVENTIVED0120 Periodicoraleval-establishedpatient ...................................................................0 .............................................................. 0D0140 Limitedoraleval-problemfocused ........................................................................0 .............................................................. 0D0145 Oralevalforapatientunder3yearsofage ............................................................0 .............................................................. 0D0150 Comprehensiveoraleval-neworestablishedpatient ...........................................0 .............................................................. 0D0160 Detailedandextensiveoraleval-problemfocused ...............................................0 .............................................................. 0D0170 Re-evaluation-limited,problemfocused ................................................................0 .............................................................. 0D0171 Re-evaluation-post-operativeofficevisit ..............................................................41 ............................................................ 41D0180 Comp.periodontaleval-neworestablishedpatient ..............................................0 .............................................................. 0D0210 Intraoral-completeseries(includingbitewings) ....................................................26 ............................................................ 26D0220 Intraoral-periapicalfirstradiographicimage ..........................................................0 .............................................................. 0D0230 Intraoral-periapicaleachadd.radiographicimage ................................................0 .............................................................. 0D0240 Intraoral-occlusalradiographicimage ...................................................................0 .............................................................. 0D0250 Extra-oral-2Dprojectionradiographicimage........................................................0 .............................................................. 0D0251 Extra-oralposteriordentalradiographicimage ......................................................44 ............................................................ 44D0270 Bitewing-singleradiographicimage ......................................................................0 .............................................................. 0D0272 Bitewings-tworadiographicimages.......................................................................0 .............................................................. 0D0273 Bitewings-threeradiographicimages ....................................................................0 .............................................................. 0D0274 Bitewings-fourradiographicimages ......................................................................0 .............................................................. 0D0277 Verticalbitewings-7to8radiographicimages .......................................................0 .............................................................. 0D0310 Sialography ...........................................................................................................350 .......................................................... 370D0320 Temporomandibularjointarthrogram,incl.injection..............................................350 .......................................................... 562D0321 Othertemporomandibularjointradiographicimages,byreport ............................120 .......................................................... 120D0322 Tomographicsurvey ................................................................................................0 .............................................................. 0D0330 Panoramicradiographicimage ..............................................................................30 ............................................................ 30D0340 2Dcephalometricradiographicimage.....................................................................0 .............................................................. 0D0350 2Doral/facialphotographicimages(intraoral/extraoral) .........................................0 .............................................................. 0D0351 3Dphotographicimage ...........................................................................................0 .............................................................. 0D0364 ConeBeamCTlimitedview-lessthanonejaw ......................................................98 ............................................................ 98D0365 ConeBeamCTonefulldentalarch(mandibular/maxillary) ..................................164 .......................................................... 164D0366 ConeBeamCTonefulldentalarch(mandibular/maxillary) ..................................164 .......................................................... 164D0367 ConeBeamCTbothjaws .....................................................................................164 .......................................................... 164D0368 ConeBeamCT-TMJ .............................................................................................96 ............................................................ 96D0369 MaxillofacialMRI/ultrasound .................................................................................164 .......................................................... 164D0370 MaxillofacialMRI/ultrasound .................................................................................164 .......................................................... 164D0380 ConebeamCTimagecapture-lessthanonejaw ..................................................98 ............................................................ 98D0381 ConebeanCTimagecaptureonearch(mandibular/maxillary) .............................98 ............................................................ 98D0382 ConebeanCTimagecaptureonearch(mandibular/maxillary) .............................98 ............................................................ 98D0383 ConebeamCTimagecapturebothjaws ..............................................................156 .......................................................... 156D0384 ConebeamCTimagecapture-TMJ ......................................................................97 ............................................................ 97D0385 MaxillofacialMRI/ultrasoundimagecapture .........................................................164 .......................................................... 164D0386 MaxillofacialMRI/ultrasoundimagecapture .........................................................164 .......................................................... 164D0414 Labprocessingofmicrobialspecimentoincludeculture&sensitivitystudies ......29 ............................................................ 29D0415 Collectionofmicroorganismsforcultureandsensitivity ........................................29 ............................................................ 29D0416 Viralculture ............................................................................................................35 ............................................................ 35D0417 Collection/Prepofsalivasampleforlab .................................................................26 ............................................................ 26D0418 Analysisofsalivasample .......................................................................................32 ............................................................ 32D0422 Collectionandpreparationofgeneticsamplematerialforlabanalysisandreport ......50 ............................................................ 50D0423 Genetictestforsusceptibilitytodiseases .............................................................75 ............................................................ 75D0425 Cariessusceptibilitytests .......................................................................................27 ............................................................ 27D0431 Adjunctivepre-diagonostic .....................................................................................49 ............................................................ 49D0460 Pulpvitalitytests .....................................................................................................0 .............................................................. 0D0470 Diagnosticcasts ......................................................................................................0 .............................................................. 0D0472 Accessionoftissue,grossexam,prep,transm.....................................................114 .......................................................... 114D0473 Accessionoftissue,grossandmicro.exam.,prep,transm ..................................156 .......................................................... 156D0474 Accessionoftissue,grossandmicro.exam.,prep,transm ...................................53 ............................................................ 53D0480 Accessionofexfoliativecytologicsmears,micro.exam.,prep,transm .................52 ............................................................ 52D0486 Labaccessiontranscytologicsample,micro.exam.,prep,transm ........................0 .............................................................. 0D0502 Otheroralpathologyprocedures,byreport ............................................................0 .............................................................. 0D0600 Non-ionizingdiagnosticprocedurecapableofquantifying,monitoring abnormalitiesinclpremalignantandmalignantlesions .......................................0 .............................................................. 0D0601 Cariesriskassessment&documentation,withafindingoflowrisk .......................0 .............................................................. 0
DMNNJ18DBLINDPEDEHB
Annual Out-of-Pocket Maximum: $350 per child per calendar year for medically necessary treatment (maximum of $700 for policy covering two or more children). The member shall only be responsible for the copayment listed in Member Copayment column. Any procedure listed that has a Member Copayment above the annual out-of-pocket maximum may apply as these procedures are not considered medically necessary and are included as additional benefits. The Plan is responsible for the difference between the Actual Copayment and the Member Copayment for all medically necessary treatment.
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)
Select Plan Basic Pediatric 702xs (NJ) Description of Covered Services, Member Copayments, Exclusions and Limitations
for Pediatric Services (under age 19)\.
Dominion National Insurance Company

ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)
D0602 Cariesriskassessment&documentation,withafindingofmoderaterisk .............0 .............................................................. 0D0603 Cariesriskassessment&documentation,withafindingofhighrisk......................0 .............................................................. 0D1110 Prophylaxis(cleaning)-adult ..................................................................................0 .............................................................. 0D1120 Prophylaxis(cleaning)-child ..................................................................................0 .............................................................. 0D1206 Topicalfluoridevarnishformod/highriskcariespatients ........................................0 .............................................................. 0D1208 Topicalapplicationoffluoride ..................................................................................0 .............................................................. 0D1310 Nutritionalcounselingforcontrolofdentaldisease.................................................0 .............................................................. 0D1320 Tobaccocounselingforcontrolofprev.oraldisease ..............................................0 .............................................................. 0D1330 Oralhygieneinstructions.........................................................................................0 .............................................................. 0D1351 Sealant-pertooth..................................................................................................21 ............................................................ 21D1352 Prevresinrest.mod/highcariesrisk–perm.tooth ................................................21 ............................................................ 21 SPACEMAINTAINERS D1510 Spacemaintainer-fixed-unilateral......................................................................143 .......................................................... 143D1515 Spacemaintainer-fixed-bilateral........................................................................198 .......................................................... 198D1520 Spacemaintainer-removable-unilateral ............................................................143 .......................................................... 143D1525 Spacemaintainer-removable-bilateral ..............................................................198 .......................................................... 198D1550 Re-cementationofspacemaintainer .....................................................................34 ............................................................ 34D1555 Removaloffixedspacemaintainer,bynon-originatingdentist .............................44 ............................................................ 44D1575 Distalshoespacemaintainer-fixed-unilateral ...................................................143 .......................................................... 143 RESTORATIVE DENTISTRY (FILLINGS) D2140 Amalgam-onesurface,prim.orperm...................................................................41 ............................................................ 41D2150 Amalgam-twosurfaces,prim.orperm. ................................................................51 ............................................................ 51D2160 Amalgam-threesurfaces,prim.orperm...............................................................64 ............................................................ 64D2161 Amalgam->=4surfaces,prim.orperm.................................................................78 ............................................................ 78D2330 Resin-basedcomposite-onesurface,anterior .....................................................69 ............................................................ 69D2331 Resin-basedcomposite-twosurfaces,anterior ....................................................83 ............................................................ 83D2332 Resin-basedcomposite-threesurfaces,anterior .................................................99 ............................................................ 99D2335 Resin-basedcomposite->=4surfaces,anterior ..................................................119 .......................................................... 119D2390 Resin-basedcompositecrown,anterior ................................................................192 .......................................................... 192D2391 Resin-basedcomposite-onesurface,posterior....................................................73 ............................................................ 73D2392 Resin-basedcomposite-twosurfaces,posterior ..................................................87 ............................................................ 87D2393 Resin-basedcomposite-threesurfaces,posterior...............................................102 .......................................................... 102D2394 Resin-basedcomposite->=4surfaces,posterior.................................................123 .......................................................... 123D2410 Goldfoil-onesurface ...........................................................................................168 .......................................................... 168D2420 Goldfoil-twosurfaces..........................................................................................198 .......................................................... 198D2430 Goldfoil-threesurfaces .......................................................................................268 .......................................................... 268 CROWNS & BRIDGES D2510 Inlay-metallic-onesurface ..................................................................................350 .......................................................... 407D2520 Inlay-metallic-twosurfaces .................................................................................350 .......................................................... 407D2530 Inlay-metallic-threeormoresurfaces ................................................................350 .......................................................... 425D2542 Onlay-metallic-twosurfaces ................................................................................350 .......................................................... 458D2543 Onlay-metallic-threesurfaces ...........................................................................350 .......................................................... 524D2544 Onlay-metallic-fourormoresurfaces ................................................................350 .......................................................... 524D2610 Inlay-porcelain/ceramic-onesurface .................................................................350 .......................................................... 427D2620 Inlay-porcelain/ceramic-twosurfaces ................................................................350 .......................................................... 427D2630 Inlay-porcelain/ceramic->=3surfaces ...............................................................350 .......................................................... 445D2642 Onlay-porcelain/ceramic-twosurfaces ..............................................................350 .......................................................... 479D2643 Onlay-porcelain/ceramic-threesurfaces ...........................................................350 .......................................................... 499D2644 Onlay-porcelain/ceramic->=4surfaces .............................................................350 .......................................................... 499D2650 Inlay-resin-basedcomposite-onesurface .........................................................350 .......................................................... 440D2651 Inlay-resin-basedcomposite-twosurfaces ........................................................350 .......................................................... 440D2652 Inlay-resin-basedcomposite->=3surfaces .......................................................350 .......................................................... 440D2662 Onlay-resin-basedcomposite-twosurfaces ......................................................350 .......................................................... 444D2663 Onlay-resin-basedcomposite-threesurfaces ...................................................350 .......................................................... 444D2664 Onlay-resin-basedcomposite->=4surfaces .....................................................350 .......................................................... 444D2710 Crown-resinbasedcomposite(indirect)..............................................................272 .......................................................... 272D2712 Crown-3/4resin-basedcomposite(indirect) .......................................................350 .......................................................... 485D2720 Crown-resinwithhighnoblemetal ......................................................................350 .......................................................... 495D2721 Crown-resinwithpredominantlybasemetal .......................................................350 .......................................................... 495D2722 Crown-resinwithnoblemetal ..............................................................................350 .......................................................... 495D2740 Crown-porcelain/ceramicsubstrate.....................................................................350 .......................................................... 560D2750 Crown-porcelainfusedtohighnoblemetal .........................................................350 .......................................................... 523D2751 Crown-porcelainfusedtopredominantlybasemetal ..........................................350 .......................................................... 523D2752 Crown-porcelainfusedtonoblemetal.................................................................350 .......................................................... 523D2780 Crown-3/4casthighnoblemetal.........................................................................350 .......................................................... 478D2781 Crown-3/4castpredominantlybasemetal ..........................................................350 .......................................................... 478D2782 Crown-3/4castnoblemetal ................................................................................350 .......................................................... 478D2783 Crown-3/4porcelain/ceramic ..............................................................................350 .......................................................... 511D2790 Crown-fullcasthighnoblemetal .........................................................................350 .......................................................... 495D2791 Crown-fullcastpredominatelybasemetal ..........................................................350 .......................................................... 495D2792 Crown-fullcastnoblemetal .................................................................................350 .......................................................... 495D2910 Recementinlay ......................................................................................................43 ............................................................ 43D2915 Recementcastorprefab.postandcore ................................................................82 ............................................................ 82D2920 Recementcrown ....................................................................................................43 ............................................................ 43D2929 Porcelain/ceramiccrown-prim.tooth ...................................................................350 .......................................................... 560
♦Allfeesexcludethecostofnobleandpreciousmetals.Anadditionalfeewillbechargedifthesematerialsareused.
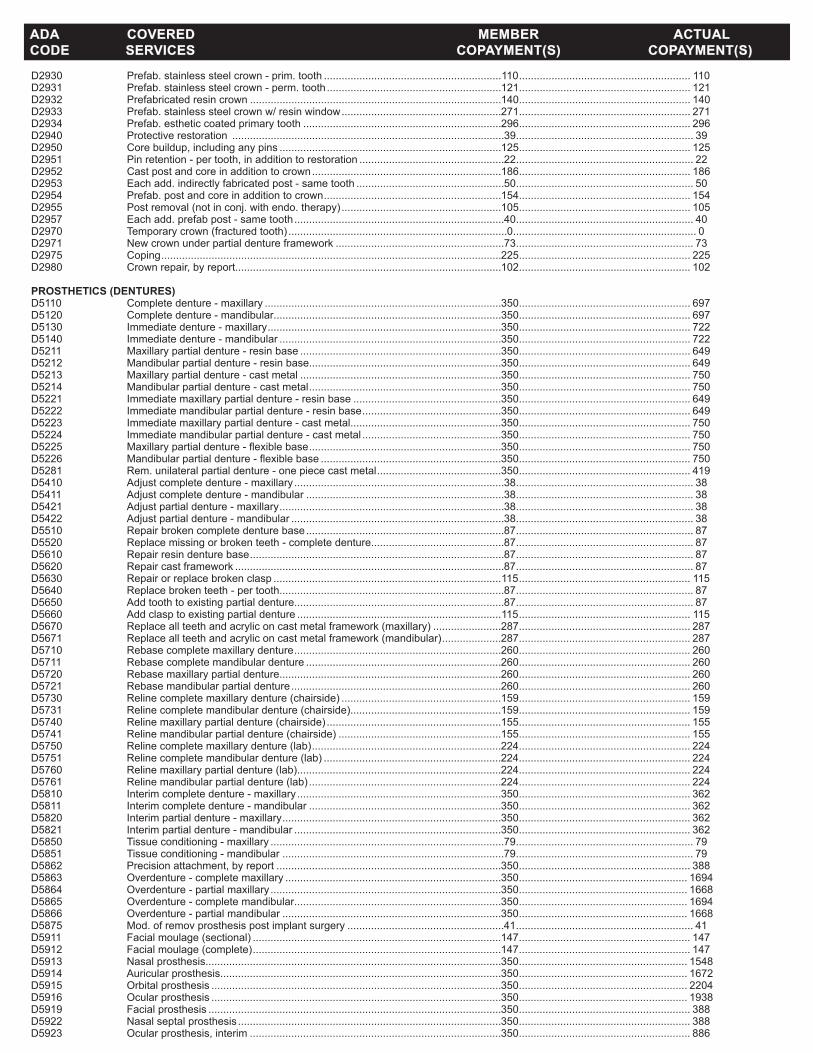
D2930 Prefab.stainlesssteelcrown-prim.tooth ............................................................110 .......................................................... 110D2931 Prefab.stainlesssteelcrown-perm.tooth ...........................................................121 .......................................................... 121D2932 Prefabricatedresincrown .....................................................................................140 .......................................................... 140D2933 Prefab.stainlesssteelcrownw/resinwindow ......................................................271 .......................................................... 271D2934 Prefab.estheticcoatedprimarytooth ...................................................................296 .......................................................... 296D2940 Protectiverestoration ............................................................................................39 ............................................................ 39D2950 Corebuildup,includinganypins ...........................................................................125 .......................................................... 125D2951 Pinretention-pertooth,inadditiontorestoration .................................................22 ............................................................ 22D2952 Castpostandcoreinadditiontocrown ................................................................186 .......................................................... 186D2953 Eachadd.indirectlyfabricatedpost-sametooth ..................................................50 ............................................................ 50D2954 Prefab.postandcoreinadditiontocrown ............................................................154 .......................................................... 154D2955 Postremoval(notinconj.withendo.therapy) ......................................................105 .......................................................... 105D2957 Eachadd.prefabpost-sametooth .......................................................................40 ............................................................ 40D2970 Temporarycrown(fracturedtooth) ..........................................................................0 .............................................................. 0D2971 Newcrownunderpartialdentureframework .........................................................73 ............................................................ 73D2975 Coping ...................................................................................................................225 .......................................................... 225D2980 Crownrepair,byreport..........................................................................................102 .......................................................... 102 PROSTHETICS (DENTURES) D5110 Completedenture-maxillary ................................................................................350 .......................................................... 697D5120 Completedenture-mandibular.............................................................................350 .......................................................... 697D5130 Immediatedenture-maxillary ...............................................................................350 .......................................................... 722D5140 Immediatedenture-mandibular ...........................................................................350 .......................................................... 722D5211 Maxillarypartialdenture-resinbase ....................................................................350 .......................................................... 649D5212 Mandibularpartialdenture-resinbase.................................................................350 .......................................................... 649D5213 Maxillarypartialdenture-castmetal ....................................................................350 .......................................................... 750D5214 Mandibularpartialdenture-castmetal .................................................................350 .......................................................... 750D5221 Immediatemaxillarypartialdenture-resinbase ..................................................350 .......................................................... 649D5222 Immediatemandibularpartialdenture-resinbase ...............................................350 .......................................................... 649D5223 Immediatemaxillarypartialdenture-castmetal...................................................350 .......................................................... 750D5224 Immediatemandibularpartialdenture-castmetal ...............................................350 .......................................................... 750D5225 Maxillarypartialdenture-flexiblebase .................................................................350 .......................................................... 750D5226 Mandibularpartialdenture-flexiblebase .............................................................350 .......................................................... 750D5281 Rem.unilateralpartialdenture-onepiececastmetal ..........................................350 .......................................................... 419D5410 Adjustcompletedenture-maxillary .......................................................................38 ............................................................ 38D5411 Adjustcompletedenture-mandibular ...................................................................38 ............................................................ 38D5421 Adjustpartialdenture-maxillary ............................................................................38 ............................................................ 38D5422 Adjustpartialdenture-mandibular ........................................................................38 ............................................................ 38D5510 Repairbrokencompletedenturebase ...................................................................87 ............................................................ 87D5520 Replacemissingorbrokenteeth-completedenture.............................................87 ............................................................ 87D5610 Repairresindenturebase ......................................................................................87 ............................................................ 87D5620 Repaircastframework ...........................................................................................87 ............................................................ 87D5630 Repairorreplacebrokenclasp .............................................................................115 .......................................................... 115D5640 Replacebrokenteeth-pertooth............................................................................87 ............................................................ 87D5650 Addtoothtoexistingpartialdenture.......................................................................87 ............................................................ 87D5660 Addclasptoexistingpartialdenture .....................................................................115 .......................................................... 115D5670 Replaceallteethandacryliconcastmetalframework(maxillary) .......................287 .......................................................... 287D5671 Replaceallteethandacryliconcastmetalframework(mandibular) ....................287 .......................................................... 287D5710 Rebasecompletemaxillarydenture ......................................................................260 .......................................................... 260D5711 Rebasecompletemandibulardenture ..................................................................260 .......................................................... 260D5720 Rebasemaxillarypartialdenture...........................................................................260 .......................................................... 260D5721 Rebasemandibularpartialdenture .......................................................................260 .......................................................... 260D5730 Relinecompletemaxillarydenture(chairside) ......................................................159 .......................................................... 159D5731 Relinecompletemandibulardenture(chairside)...................................................159 .......................................................... 159D5740 Relinemaxillarypartialdenture(chairside) ...........................................................155 .......................................................... 155D5741 Relinemandibularpartialdenture(chairside) .......................................................155 .......................................................... 155D5750 Relinecompletemaxillarydenture(lab) ................................................................224 .......................................................... 224D5751 Relinecompletemandibulardenture(lab) ............................................................224 .......................................................... 224D5760 Relinemaxillarypartialdenture(lab).....................................................................224 .......................................................... 224D5761 Relinemandibularpartialdenture(lab) .................................................................224 .......................................................... 224D5810 Interimcompletedenture-maxillary .....................................................................350 .......................................................... 362D5811 Interimcompletedenture-mandibular .................................................................350 .......................................................... 362D5820 Interimpartialdenture-maxillary ..........................................................................350 .......................................................... 362D5821 Interimpartialdenture-mandibular ......................................................................350 .......................................................... 362D5850 Tissueconditioning-maxillary ...............................................................................79 ............................................................ 79D5851 Tissueconditioning-mandibular ...........................................................................79 ............................................................ 79D5862 Precisionattachment,byreport ............................................................................350 .......................................................... 388D5863 Overdenture-completemaxillary .........................................................................350 ......................................................... 1694D5864 Overdenture-partialmaxillary ..............................................................................350 ......................................................... 1668D5865 Overdenture-completemandibular......................................................................350 ......................................................... 1694D5866 Overdenture-partialmandibular ..........................................................................350 ......................................................... 1668D5875 Mod.ofremovprosthesispostimplantsurgery .....................................................41 ............................................................ 41D5911 Facialmoulage(sectional) ....................................................................................147 .......................................................... 147D5912 Facialmoulage(complete) ....................................................................................147 .......................................................... 147D5913 Nasalprosthesis....................................................................................................350 ......................................................... 1548D5914 Auricularprosthesis...............................................................................................350 ......................................................... 1672D5915 Orbitalprosthesis ..................................................................................................350 ......................................................... 2204D5916 Ocularprosthesis ..................................................................................................350 ......................................................... 1938D5919 Facialprosthesis ...................................................................................................350 .......................................................... 388D5922 Nasalseptalprosthesis .........................................................................................350 .......................................................... 388D5923 Ocularprosthesis,interim .....................................................................................350 .......................................................... 886
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)

D5924 Cranialprosthesis .................................................................................................350 ......................................................... 4408D5925 Facialaugmentationimplantprosthesis ................................................................350 .......................................................... 500D5926 Nasalprosthesis,replacement ..............................................................................169 .......................................................... 169D5927 Auricularprosthesis,replacement .........................................................................350 ......................................................... 1948D5928 Orbitalprosthesis,replacement ............................................................................350 ......................................................... 2632D5929 Facialprosthesis,replacement .............................................................................255 .......................................................... 255D5931 Obturatorprosthesis,surgical ...............................................................................350 .......................................................... 803D5932 Obturatorprosthesis,definitive .............................................................................350 ......................................................... 4800D5933 Obturatorprosthesis,modification ........................................................................350 .......................................................... 709D5934 Mandibularresectionprosthesisw/guideflange ..................................................350 ......................................................... 4042D5935 Mandibularresectionprosthesisw/oguideflange ................................................350 ......................................................... 3770D5936 Obturatorprosthesis,interim .................................................................................350 ......................................................... 2049D5951 Feedingaid ...........................................................................................................350 ......................................................... 1395D5952 Speechaidprosthesis ...........................................................................................350 ......................................................... 1154D5953 Speechaidprosthesis,adult .................................................................................350 .......................................................... 928D5954 Palatalaugmentationprosthesis ...........................................................................350 ......................................................... 1734D5955 Palatalliftprosthesis,definitive .............................................................................350 ......................................................... 1668D5958 Palatalliftprosthesis,interim ................................................................................350 ......................................................... 1668D5959 Palatalliftprosthesis,modification ........................................................................350 ......................................................... 1668D5960 Speechaidprosthesis,modification......................................................................278 .......................................................... 278D5982 Surgicalstent .........................................................................................................87 ............................................................ 87D5983 Radiationcarrier ....................................................................................................350 .......................................................... 736D5984 Radiationshield.....................................................................................................350 .......................................................... 400D5985 Radiationconelocator ..........................................................................................350 .......................................................... 400D5986 Fluoridegelcarrier ................................................................................................126 .......................................................... 126D5987 Commissuresplint .................................................................................................350 .......................................................... 899D5988 Surgicalsplint ........................................................................................................125 .......................................................... 125D5991 Topicalmedicamentcarrier ...................................................................................126 .......................................................... 126D5992 Adjustmentofprostheticappliance,byreport ........................................................24 ............................................................ 24D5993 Cleaningandmaintenanceprostheticappliance ...................................................18 ............................................................ 18D5994 Periodontalmedicamentcarrier ............................................................................150 .......................................................... 150 BRIDGES & PONTICS D6010 Surgicalplacementofimplantbody,endosteal .....................................................350 ......................................................... 1716D6011 Secondstageimplantsurgery...............................................................................200 .......................................................... 200D6012 Surgicalplacementofinterimimplantbody ..........................................................350 ......................................................... 1782D6013 Surgicalplacementofminiimplant .......................................................................350 .......................................................... 572D6040 Surgicalplacement,epostealimplant ...................................................................350 ......................................................... 3564D6050 Surgicalplacement,transostealimplant ...............................................................350 ......................................................... 4455D6051 Interimabutment ...................................................................................................197 .......................................................... 197D6055 Dentalimplantsupportedconnectingbar..............................................................350 ......................................................... 1611D6056 Prefabricatedabutment .........................................................................................350 .......................................................... 456D6057 Customfabricatedabutment .................................................................................350 .......................................................... 563D6058 Abutmentsupportedporcelain/ceramiccrown ......................................................350 .......................................................... 560D6059 Abutmentsupportedporcelainfusedtometalcrown-highnoblemetal ..............350 .......................................................... 523D6060 Abutmentsupportedporcelainfusedtometalcrown-predominantlybasedmetal ...350 .......................................................... 523D6061 Abutmentsupportedporcelainfusedtometalcrown-noblemetal ......................350 .......................................................... 523D6062 Abutmentsupportedcastmetalcrown-highnoblemetal ....................................350 .......................................................... 495D6063 Abutmentsupportedcastmetalcrown-predominantlybasedmetal ...................350 .......................................................... 495D6064 Abutmentsupportedcastmetalcrown-noblemetal ............................................350 .......................................................... 495D6065 Implantsupportedporcelain/ceramiccrown..........................................................350 .......................................................... 560D6066 Implantsupportedporcelainfusedtometalcrown-titanium,titanium allow,highnoblemetal ......................................................................................350 .......................................................... 523D6067 Implantsupportedmetalcrown-titanium,titaniumalloy,highnoblemetal ..........350 .......................................................... 523D6068 Abutmentsupportedretainerforporc/ceramic ......................................................350 .......................................................... 788D6069 Abutmentsupp.retainerforporc/highnoble .........................................................350 .......................................................... 843D6070 Abutmentsupp.retainerforporc/pred.base.........................................................350 .......................................................... 695D6071 Abutmentsupp.retainerforporc/noble .................................................................350 .......................................................... 704D6072 Abutmentsuppretainerforcasthighnoble ..........................................................350 .......................................................... 788D6073 Abutmentsupp.retainerforcasthighnoble .........................................................350 .......................................................... 749D6074 Abutmentsupp.retainerforcastnoblemetal .......................................................350 .......................................................... 758D6080 Implantmaintenanceprocedures ...........................................................................61 ............................................................ 61D6081 Scalinganddebridementinthepresenceofinflammationormucositisofa singleimplant,includingcleaningoftheimplantsurfaces,withoutflap entryandclosure .................................................................................................63 ............................................................ 63D6090 Repairimplantsupportedprosthesis.....................................................................350 .......................................................... 362D6091 ReplacementofPrecisionAttachment ...................................................................34 ............................................................ 34D6092 Re-cementimplant/abutmentsupp.crown.............................................................56 ............................................................ 56D6093 Re-cementimpl/abutmentsupp.fixedpar .............................................................86 ............................................................ 86D6095 Repairimplantabutment,byreport .......................................................................391 .......................................................... 391D6110 Implant/abutsuppremdentforedentulousarch-maxillary ...............................350 ......................................................... 1517D6111 Implant/abutsuppremdentforedentulousarch-mandibular............................350 ......................................................... 1517D6112 Implant/abutsuppremdentforpartiallyedentulousarch-maxillary ..................350 ......................................................... 1517D6113 Implant/abutsuppremdentforpartiallyedentulousarch-mandibular ..............350 ......................................................... 1517D6114 Implant/abutsuppfixeddentforedentulousarch-maxillary ..............................350 ......................................................... 2606D6115 Implant/abutsuppfixeddentforedentulousarch-mandibular ..........................350 ......................................................... 2606D6116 Implant/abutsuppfixeddentforpartiallyedentulousarch-maxillary ................350 ......................................................... 1610D6117 Implant/abutsuppfixeddentforpartiallyedentulousarch-mandibular .............350 ......................................................... 1610
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)
♦Allfeesexcludethecostofnobleandpreciousmetals.Anadditionalfeewillbechargedifthesematerialsareused.
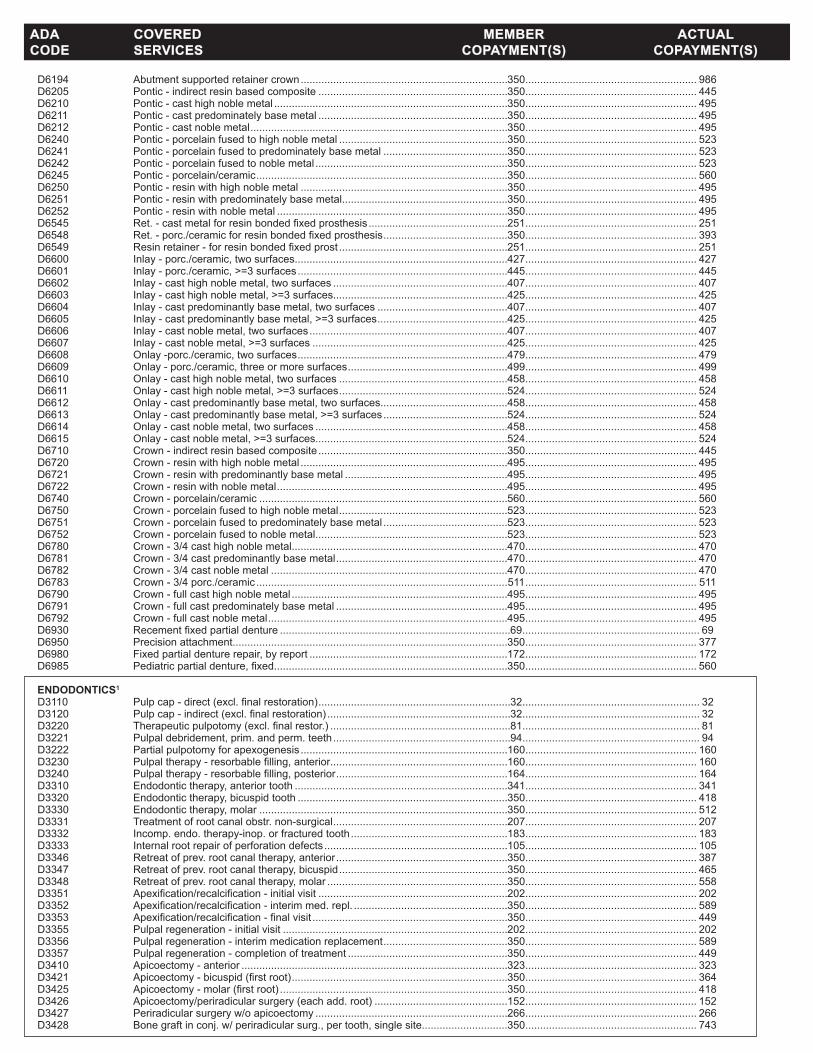
D6194 Abutmentsupportedretainercrown ......................................................................350 .......................................................... 986D6205 Pontic-indirectresinbasedcomposite ................................................................350 .......................................................... 445D6210 Pontic-casthighnoblemetal ...............................................................................350 .......................................................... 495D6211 Pontic-castpredominatelybasemetal ................................................................350 .......................................................... 495D6212 Pontic-castnoblemetal .......................................................................................350 .......................................................... 495D6240 Pontic-porcelainfusedtohighnoblemetal .........................................................350 .......................................................... 523D6241 Pontic-porcelainfusedtopredominatelybasemetal ..........................................350 .......................................................... 523D6242 Pontic-porcelainfusedtonoblemetal .................................................................350 .......................................................... 523D6245 Pontic-porcelain/ceramic .....................................................................................350 .......................................................... 560D6250 Pontic-resinwithhighnoblemetal ......................................................................350 .......................................................... 495D6251 Pontic-resinwithpredominatelybasemetal........................................................350 .......................................................... 495D6252 Pontic-resinwithnoblemetal ..............................................................................350 .......................................................... 495D6545 Ret.-castmetalforresinbondedfixedprosthesis ...............................................251 .......................................................... 251D6548 Ret.-porc./ceramicforresinbondedfixedprosthesis ..........................................350 .......................................................... 393D6549 Resinretainer-forresinbondedfixedprost .........................................................251 .......................................................... 251D6600 Inlay-porc./ceramic,twosurfaces........................................................................427 .......................................................... 427D6601 Inlay-porc./ceramic,>=3surfaces .......................................................................445 .......................................................... 445D6602 Inlay-casthighnoblemetal,twosurfaces ...........................................................407 .......................................................... 407D6603 Inlay-casthighnoblemetal,>=3surfaces...........................................................425 .......................................................... 425D6604 Inlay-castpredominantlybasemetal,twosurfaces ............................................407 .......................................................... 407D6605 Inlay-castpredominantlybasemetal,>=3surfaces ............................................425 .......................................................... 425D6606 Inlay-castnoblemetal,twosurfaces ...................................................................407 .......................................................... 407D6607 Inlay-castnoblemetal,>=3surfaces ..................................................................425 .......................................................... 425D6608 Onlay-porc./ceramic,twosurfaces .......................................................................479 .......................................................... 479D6609 Onlay-porc./ceramic,threeormoresurfaces ......................................................499 .......................................................... 499D6610 Onlay-casthighnoblemetal,twosurfaces .........................................................458 .......................................................... 458D6611 Onlay-casthighnoblemetal,>=3surfaces .........................................................524 .......................................................... 524D6612 Onlay-castpredominantlybasemetal,twosurfaces...........................................458 .......................................................... 458D6613 Onlay-castpredominantlybasemetal,>=3surfaces ..........................................524 .......................................................... 524D6614 Onlay-castnoblemetal,twosurfaces .................................................................458 .......................................................... 458D6615 Onlay-castnoblemetal,>=3surfaces.................................................................524 .......................................................... 524D6710 Crown-indirectresinbasedcomposite ................................................................350 .......................................................... 445D6720 Crown-resinwithhighnoblemetal ......................................................................495 .......................................................... 495D6721 Crown-resinwithpredominantlybasemetal .......................................................495 .......................................................... 495D6722 Crown-resinwithnoblemetal ..............................................................................495 .......................................................... 495D6740 Crown-porcelain/ceramic ....................................................................................560 .......................................................... 560D6750 Crown-porcelainfusedtohighnoblemetal .........................................................523 .......................................................... 523D6751 Crown-porcelainfusedtopredominatelybasemetal ..........................................523 .......................................................... 523D6752 Crown-porcelainfusedtonoblemetal.................................................................523 .......................................................... 523D6780 Crown-3/4casthighnoblemetal.........................................................................470 .......................................................... 470D6781 Crown-3/4castpredominantlybasemetal ..........................................................470 .......................................................... 470D6782 Crown-3/4castnoblemetal ................................................................................470 .......................................................... 470D6783 Crown-3/4porc./ceramic .....................................................................................511 .......................................................... 511D6790 Crown-fullcasthighnoblemetal .........................................................................495 .......................................................... 495D6791 Crown-fullcastpredominatelybasemetal ..........................................................495 .......................................................... 495D6792 Crown-fullcastnoblemetal .................................................................................495 .......................................................... 495D6930 Recementfixedpartialdenture ..............................................................................69 ............................................................ 69D6950 Precisionattachment.............................................................................................350 .......................................................... 377D6980 Fixedpartialdenturerepair,byreport ...................................................................172 .......................................................... 172D6985 Pediatricpartialdenture,fixed...............................................................................350 .......................................................... 560 ENDODONTICS1 D3110 Pulpcap-direct(excl.finalrestoration) .................................................................32 ............................................................ 32D3120 Pulpcap-indirect(excl.finalrestoration) ..............................................................32 ............................................................ 32D3220 Therapeuticpulpotomy(excl.finalrestor.) .............................................................81 ............................................................ 81D3221 Pulpaldebridement,prim.andperm.teeth ............................................................94 ............................................................ 94D3222 Partialpulpotomyforapexogenesis ......................................................................160 .......................................................... 160D3230 Pulpaltherapy-resorbablefilling,anterior............................................................160 .......................................................... 160D3240 Pulpaltherapy-resorbablefilling,posterior ..........................................................164 .......................................................... 164D3310 Endodontictherapy,anteriortooth ........................................................................341 .......................................................... 341D3320 Endodontictherapy,bicuspidtooth .......................................................................350 .......................................................... 418D3330 Endodontictherapy,molar ....................................................................................350 .......................................................... 512D3331 Treatmentofrootcanalobstr.non-surgical ...........................................................207 .......................................................... 207D3332 Incomp.endo.therapy-inop.orfracturedtooth .....................................................183 .......................................................... 183D3333 Internalrootrepairofperforationdefects ..............................................................105 .......................................................... 105D3346 Retreatofprev.rootcanaltherapy,anterior ..........................................................350 .......................................................... 387D3347 Retreatofprev.rootcanaltherapy,bicuspid .........................................................350 .......................................................... 465D3348 Retreatofprev.rootcanaltherapy,molar .............................................................350 .......................................................... 558D3351 Apexification/recalcification-initialvisit ................................................................202 .......................................................... 202D3352 Apexification/recalcification-interimmed.repl. ....................................................350 .......................................................... 589D3353 Apexification/recalcification-finalvisit ..................................................................350 .......................................................... 449D3355 Pulpalregeneration-initialvisit ............................................................................202 .......................................................... 202D3356 Pulpalregeneration-interimmedicationreplacement ..........................................350 .......................................................... 589D3357 Pulpalregeneration-completionoftreatment ......................................................350 .......................................................... 449D3410 Apicoectomy-anterior ..........................................................................................323 .......................................................... 323D3421 Apicoectomy-bicuspid(firstroot) .........................................................................350 .......................................................... 364D3425 Apicoectomy-molar(firstroot) .............................................................................350 .......................................................... 418D3426 Apicoectomy/periradicularsurgery(eachadd.root) .............................................152 .......................................................... 152D3427 Periradicularsurgeryw/oapicoectomy .................................................................266 .......................................................... 266D3428 Bonegraftinconj.w/periradicularsurg.,pertooth,singlesite.............................350 .......................................................... 743
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)

D3429 Bonegraftinconj.w/periradicularsurg.,add.contiguoustooth,samesite .........350 .......................................................... 582D3430 Retrogradefilling-perroot ...................................................................................119 .......................................................... 119D3431 Biologicmaterialstoaidsoft/osseoustissueregen.inconj.w/periradicularsurg...350 .......................................................... 407D3432 Guidedtissueregen.,resorbablebarrier,persite,inconj.w/periradicularsurg. ....350 .......................................................... 815D3450 Rootamputation-perroot ....................................................................................234 .......................................................... 234D3910 Surg.proc.forisol.oftoothw/rubberdam ............................................................57 ............................................................ 57D3920 Hemisection,notinc.rootcanaltherapy ...............................................................234 .......................................................... 234D3950 Canalprep/fittingofpreformeddowelorpost .......................................................136 .......................................................... 136 PERIODONTICS1 D4210 Gingivectomyorgingivoplasty->3cont.teeth,perquad. ....................................279 .......................................................... 279D4211 Gingivectomyorgingivoplasty-<=3teeth,perquad. ...........................................100 .......................................................... 100D4212 Gingivectomyorgingivoplasty,rest.,pertooth ......................................................40 ............................................................ 40D4240 Gingivalflapproc.,inc.rootplaning->3cont.teeth,perquad .............................345 .......................................................... 345D4241 Gingivalflapproc,inc.rootplaning-<=3cont.teeth,perquad............................106 .......................................................... 106D4245 Apicallypositionedflap..........................................................................................186 .......................................................... 186D4249 Clinicalcrownlengthening-hardtissue................................................................350 .......................................................... 576D4260 Osseoussurgery->3cont.teeth,perquad ..........................................................350 .......................................................... 499D4261 Osseoussurgery-<=3cont.teeth,perquad........................................................350 .......................................................... 392D4263 Bonereplacementgraft-retainednaturaltooth-firstsiteinquad. ......................350 .......................................................... 743D4264 Bonereplacementgraft-retainednaturaltooth-eachadd.siteinquad. ............350 .......................................................... 582D4265 Biologicmaterials ..................................................................................................350 .......................................................... 407D4266 Guidedtissueregen.-resorb.barrier,persite......................................................350 .......................................................... 815D4267 Guidedtissueregen.-non-resorb.barrier,persite ..............................................350 .......................................................... 797D4268 Surgicalrevisionproc.,pertooth...........................................................................350 .......................................................... 358D4270 Pediclesofttissuegraftprocedure ........................................................................350 .......................................................... 643D4273 Subepithelialconnectivetissuegraftproc. ............................................................350 .......................................................... 800D4274 Mesial/distalwedgeprocedure,singletooth .........................................................308 .......................................................... 308D4275 Softtissueallograft................................................................................................350 .......................................................... 854D4276 Comb.connec.tissue/doublepediclegraft,pertooth ...........................................350 ......................................................... 1019D4277 Freesofttissuegraft,pertooth .............................................................................350 .......................................................... 654D4278 Freesofttissuegraft,eachadd.tooth...................................................................100 .......................................................... 100D4320 Provisionalsplinting-intracoronal ........................................................................350 .......................................................... 427D4321 Provisionalsplinting-extracoronal .......................................................................350 .......................................................... 377D4341 Perioscalingandrootplaning->3contteeth,perquad. .....................................109 .......................................................... 109D4342 Perioscalingandrootplaning-<=3teeth,perquad ............................................63 ............................................................ 63D4346 Scalinginpresenceofgeneralizedmoderateorseveregingivalinflammation -fullmouth,afteroralevaluation ..........................................................................45 ............................................................ 45D4355 Fullmouthdebridement .........................................................................................89 ............................................................ 89D4381 Localizeddeliveryofchemotherapeuticagents .....................................................98 ............................................................ 98D4910 Periodontalmaintenance .......................................................................................74 ............................................................ 74 ORAL SURGERY1 D7111 Extraction,coronalremnants-deciduoustooth .....................................................56 ............................................................ 56D7140 Extraction,eruptedtoothorexposedroot ..............................................................69 ............................................................ 69D7210 Extraction,eruptedtoothreqelev,etc ..................................................................133 .......................................................... 133D7220 Removalofimpactedtooth-softtissue ................................................................151 .......................................................... 151D7230 Removalofimpactedtooth-partiallybony ...........................................................196 .......................................................... 196D7240 Removalofimpactedtooth-completelybony ......................................................241 .......................................................... 241D7241 Removalofimp.tooth-completelybony,withunusualsurg.complications ........217 .......................................................... 217D7250 Removalofresidualtoothroots ............................................................................141 .......................................................... 141D7251 Coronectomy-intentionalpartialtoothremoval......................................................217 .......................................................... 217D7260 Oroantralfistulaclosure ........................................................................................350 .......................................................... 578D7261 Primaryclosureofasinusperforation...................................................................350 .......................................................... 465D7270 Toothreimplant./stabiliz.ofacc.evulsed/displacedtooth .....................................226 .......................................................... 226D7272 Toothtransplantation .............................................................................................350 .......................................................... 615D7280 Exposureofanuneruptedtooth ............................................................................153 .......................................................... 153D7282 Mobil.oferupted/malpositionedtoothtoaideruption ...........................................231 .......................................................... 231D7283 Place.ofdevicetofacilitateerupt.ofimpactedtooth ............................................144 .......................................................... 144D7285 Biopsyoforaltissue-hard(bone,tooth) ..............................................................350 .......................................................... 387D7286 Biopsyoforaltissue-soft(allothers) ...................................................................295 .......................................................... 295D7287 Exfoliativecytologicalsamplecollection ................................................................28 ............................................................ 28D7288 Brushbiopsy-transepithelialsamplecollect .........................................................93 ............................................................ 93D7290 Surgicalrepositioningofteeth ...............................................................................350 .......................................................... 407D7291 Transseptalfiberotomy/supracrestalfiberotomy,byreport ...................................60 ............................................................ 60D7292 Surgicalplacementoftempanchdevice ..............................................................350 .......................................................... 546D7293 Surgicalplacementoftempanchreqflap .............................................................350 .......................................................... 566D7294 Surgicalplacement:w/oflap .................................................................................131 .......................................................... 131D7295 Boneharvesting-autogenousgraftingprocedure ..................................................173 .......................................................... 173D7310 Alveoloplastyinconj.w/extractions,>=4perquad. .............................................141 .......................................................... 141D7311 Alveoloplastyinconj.w/extractions,1-3perquad. ..............................................141 .......................................................... 141D7320 Alveoloplastynotinconj.w/extractions,>=4perquad. .......................................141 .......................................................... 141D7321 Alveoloplastynotinconj.w/extractions,1-3perquad. ........................................141 .......................................................... 141D7340 Vestibuloplasty-ridgeext.sec.epithel. ................................................................350 .......................................................... 923D7350 Vestibuloplasty-ridgeext.inc.grafts,etc .............................................................350 ......................................................... 1776D7410 Excisionofbenignlesionupto1.25cm ................................................................278 .......................................................... 278D7411 Excisionofbenignlesion>1.25cm ......................................................................225 .......................................................... 225D7412 Excisionofbenignlesion,complicated .................................................................313 .......................................................... 313D7413 Excisionofmalignantlesionupto1.25cm ...........................................................350 .......................................................... 572D7414 Excisionofmalignantlesion>1.25cm .................................................................350 .......................................................... 504
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)

D7415 Excisionofmalignantlesion,complicated.............................................................350 .......................................................... 813D7440 Exc.ofmalignanttumor-lesiondiam.<=1.25cm ..................................................350 .......................................................... 608D7441 Exc.ofmalignanttumor-lesiondiam.>1.25cm ....................................................350 .......................................................... 733D7450 Removalofbenignodoncyst/tumor-diam<=1.25cm..........................................350 .......................................................... 354D7451 Removalofbenignodoncyst/tumor-diam>1.25cm ............................................350 .......................................................... 543D7460 Removalofbenignnonodoncyst/tumor-diam<=1.25cm......................................350 .......................................................... 516D7461 Removalofbenignnonodoncyst/tumor-diam>1.25cm ........................................350 .......................................................... 718D7465 Destruct.oflesion(s)byphysorchemmethod .....................................................300 .......................................................... 300D7471 Removaloflateralexostosis .................................................................................350 .......................................................... 351D7472 Removaloftoruspalatinus....................................................................................350 .......................................................... 480D7473 Removaloftorusmandibularis..............................................................................350 .......................................................... 480D7485 Surgicalreductionofosseoustuberosity ..............................................................350 .......................................................... 568D7490 Radicalresectionofmaxillaormandible...............................................................350 ......................................................... 4408D7510 Incisionanddrainageofabscess-intraoralsofttissue .........................................96 ............................................................ 96D7511 Incision/drainageofabscess-intra.softtissue,comp..........................................112 .......................................................... 112D7520 Incision/drainageofabscess-extra.softtissue ...................................................116 .......................................................... 116D7521 Incision/drainageofabscess-extra.softtissue,comp.........................................120 .......................................................... 120D7530 Foreignbodyremfrommuc./skin/subcuttissue.....................................................87 ............................................................ 87D7540 Reactionproducingforeignbodiesremoval ..........................................................350 .......................................................... 584D7550 Partialostect/sequestrectnon-vitalbonerem. ......................................................336 .......................................................... 336D7560 Max.sinusotomyfortoothfragmentremoval ........................................................350 .......................................................... 745D7610 Maxillary-openreduction(teethimmobilized)......................................................350 ......................................................... 2195D7620 Maxillary-closedreduction(teethimmobilized) ...................................................350 ......................................................... 1658D7630 Mandible-openreduction(teethimmobilized) .....................................................350 ......................................................... 2397D7640 Mandible-closedreduction(teethimmobilize) .....................................................350 ......................................................... 1618D7650 Malarand/orzygomaticarch-openreduction ......................................................350 ......................................................... 1697D7660 Malarand/orzygomaticarch-closedreduction ....................................................350 ......................................................... 1330D7670 Alveolus-closedreduction ...................................................................................350 .......................................................... 530D7671 Alveolus-openreduction(incl.teethstabil.) ..........................................................350 .......................................................... 533D7680 Facialbones-complicatedreduction....................................................................350 ......................................................... 3765D7710 Maxillary-openreduction .....................................................................................350 ......................................................... 2433D7720 Maxillary-closedreduction...................................................................................350 ......................................................... 2538D7730 Mandible-openreduction.....................................................................................350 ......................................................... 2399D7740 Mandible-closedreduction ..................................................................................350 ......................................................... 1727D7750 Malarand/orzygomaticarch-openreduction ......................................................350 ......................................................... 2116D7760 Malarand/orzygomaticarch-closedreduction ....................................................350 ......................................................... 1601D7770 Alveolus-openreductionstabiliz.ofteeth............................................................350 ......................................................... 1197D7771 Alveolus,closedreductionstabiliz.ofteeth ..........................................................208 .......................................................... 208D7780 Facialbones-complicatedreduction....................................................................350 ......................................................... 4711D7810 Openreductionofdislocation................................................................................350 ......................................................... 2350D7820 Closedreductionofdislocation .............................................................................342 .......................................................... 342D7830 Manipulationunderanesthesia .............................................................................283 .......................................................... 283D7840 Condylectomy .......................................................................................................350 ......................................................... 3181D7850 Surgicaldiscectomy,with/withoutimplant .............................................................350 ......................................................... 2977D7854 Synovectomy .........................................................................................................350 ......................................................... 3337D7858 Jointreconstruction ...............................................................................................350 ......................................................... 6461D7860 Arthrotomy .............................................................................................................350 ......................................................... 1731D7865 Arthroplasty ...........................................................................................................350 ......................................................... 4846D7870 Arthrocentesis .......................................................................................................158 .......................................................... 158D7871 Non-arthroscopiclysisandlavage ........................................................................350 .......................................................... 551D7872 Arthroscopy-diagnosis,w/orw/outbiopsy ..........................................................350 ......................................................... 1500D7873 Arthroscopy-surgical-lavage/lysisofadhesion ......................................................350 ......................................................... 1644D7874 Arthroscopy-surgical:discreposit/stabiliz ...........................................................350 ......................................................... 2077D7875 Arthroscopy-surgical:synovectomy ....................................................................350 ......................................................... 2221D7876 Arthroscopy-surgical:discectomy .......................................................................350 ......................................................... 2308D7877 Arthroscopy-surgical:debridement .....................................................................350 ......................................................... 2135D7880 Occlusalorthoticdevice,“byreport”......................................................................272 .......................................................... 272D7910 Sutureofrecentsmallwoundsupto5cm .............................................................59 ............................................................ 59D7911 Complicatedsuture,<=5cm .................................................................................69 ............................................................ 69D7912 Complicatedsuture,>5cm ...................................................................................79 ............................................................ 79D7920 Skingraft-identifydefect......................................................................................350 ......................................................... 1483D7921 Collectionapplicationofbloodconcentrate............................................................40 ............................................................ 40D7940 Osteoplasty-fororthognathicdeformities ............................................................350 ......................................................... 1191D7941 Osteotomy-mandibularrami ................................................................................350 ......................................................... 4682D7943 Osteotomy-mandibularramiwithbonegraft .......................................................350 ......................................................... 4224D7944 Osteotomy-segmented/subapical-persext/quad.................................................350 ......................................................... 3702D7945 Osteotomy-bodyofmandible ..............................................................................350 ......................................................... 4328D7946 LeFortI(maxillary-total) ......................................................................................350 ......................................................... 5244D7947 LeFortI(maxillary-segmented) ...........................................................................350 ......................................................... 4798D7948 LeFortIIorLeFortIII .............................................................................................350 ......................................................... 5940D7949 LeFortIIorLeFortIII-withbonegraft ..................................................................350 ......................................................... 7267D7950 Osseous,osteoperiosteal,orcartilagegraft..........................................................313 .......................................................... 313D7951 SinusAugmentationvialateralapproach ..............................................................350 .......................................................... 617D7952 Sinusaugmentationviaverticalapproach ............................................................319 .......................................................... 319D7955 Repairofmaxillofacialsoftandhardtissue...........................................................321 .......................................................... 321D7960 Frenulectomy(frenectomy/frenotomy)-separateproc. ........................................263 .......................................................... 263D7963 Frenuloplasty.........................................................................................................293 .......................................................... 293D7970 Excisionofhyperplastictissue-perarch ..............................................................233 .......................................................... 233D7971 Excisionofpericoronalgingiva..............................................................................131 .......................................................... 131D7972 Surgicalreductionoffibroustuberosity .................................................................350 .......................................................... 521
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)
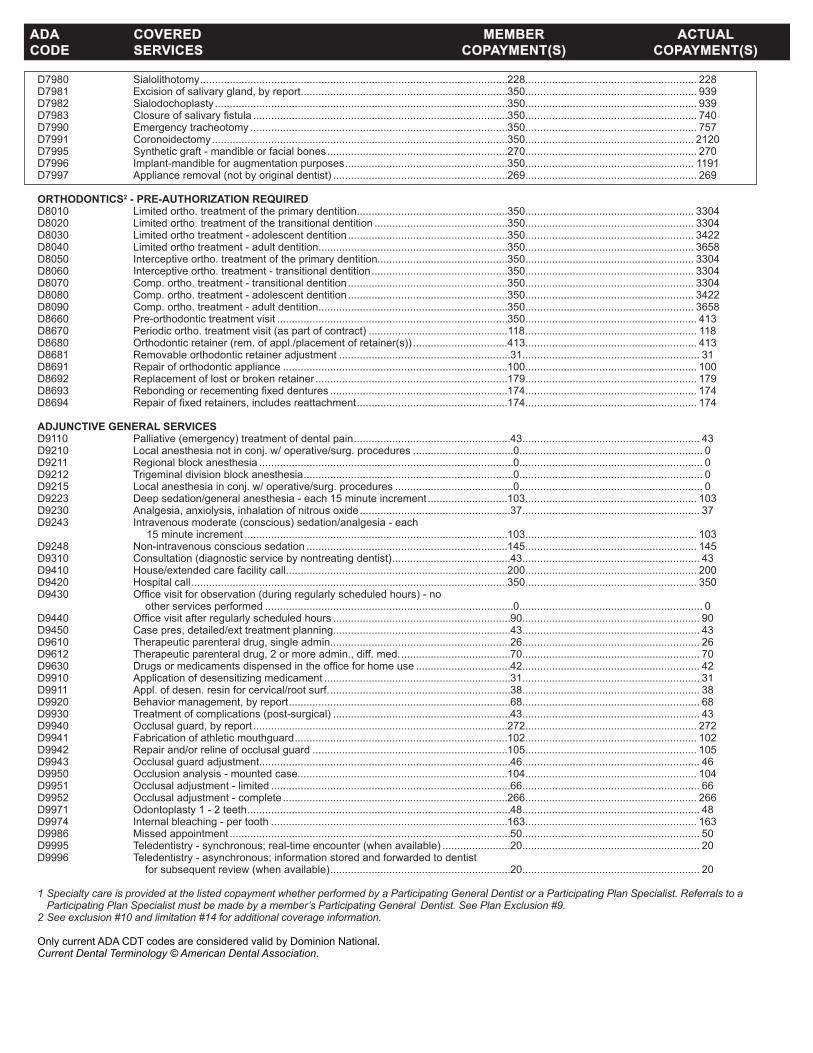
D7980 Sialolithotomy ........................................................................................................228 .......................................................... 228D7981 Excisionofsalivarygland,byreport......................................................................350 .......................................................... 939D7982 Sialodochoplasty ...................................................................................................350 .......................................................... 939D7983 Closureofsalivaryfistula ......................................................................................350 .......................................................... 740D7990 Emergencytracheotomy .......................................................................................350 .......................................................... 757D7991 Coronoidectomy ....................................................................................................350 ......................................................... 2120D7995 Syntheticgraft-mandibleorfacialbones .............................................................270 .......................................................... 270D7996 Implant-mandibleforaugmentationpurposes .......................................................350 ......................................................... 1191D7997 Applianceremoval(notbyoriginaldentist) ...........................................................269 .......................................................... 269 ORTHODONTICS2 - PRE-AUTHORIZATION REQUIRED D8010 Limitedortho.treatmentoftheprimarydentition...................................................350 ......................................................... 3304D8020 Limitedortho.treatmentofthetransitionaldentition .............................................350 ......................................................... 3304D8030 Limitedorthotreatment-adolescentdentition ......................................................350 ......................................................... 3422D8040 Limitedorthotreatment-adultdentition................................................................350 ......................................................... 3658D8050 Interceptiveortho.treatmentoftheprimarydentition............................................350 ......................................................... 3304D8060 Interceptiveortho.treatment-transitionaldentition ..............................................350 ......................................................... 3304D8070 Comp.ortho.treatment-transitionaldentition ......................................................350 ......................................................... 3304D8080 Comp.ortho.treatment-adolescentdentition ......................................................350 ......................................................... 3422D8090 Comp.ortho.treatment-adultdentition................................................................350 ......................................................... 3658D8660 Pre-orthodontictreatmentvisit ..............................................................................350 .......................................................... 413D8670 Periodicortho.treatmentvisit(aspartofcontract) ...............................................118 .......................................................... 118D8680 Orthodonticretainer(rem.ofappl./placementofretainer(s)) ................................413 .......................................................... 413D8681 Removableorthodonticretaineradjustment ..........................................................31 ............................................................ 31D8691 Repairoforthodonticappliance ............................................................................100 .......................................................... 100D8692 Replacementoflostorbrokenretainer .................................................................179 .......................................................... 179D8693 Rebondingorrecementingfixeddentures ............................................................174 .......................................................... 174D8694 Repairoffixedretainers,includesreattachment ...................................................174 .......................................................... 174 ADJUNCTIVE GENERAL SERVICES D9110 Palliative(emergency)treatmentofdentalpain .....................................................43 ............................................................ 43D9210 Localanesthesianotinconj.w/operative/surg.procedures ..................................0 .............................................................. 0D9211 Regionalblockanesthesia ......................................................................................0 .............................................................. 0D9212 Trigeminaldivisionblockanesthesia .......................................................................0 .............................................................. 0D9215 Localanesthesiainconj.w/operative/surg.procedures ........................................0 .............................................................. 0D9223 Deepsedation/generalanesthesia-each15minuteincrement ...........................103 .......................................................... 103D9230 Analgesia,anxiolysis,inhalationofnitrousoxide ...................................................37 ............................................................ 37D9243 Intravenousmoderate(conscious)sedation/analgesia-each 15minuteincrement .........................................................................................103 .......................................................... 103D9248 Non-intravenousconscioussedation ....................................................................145 .......................................................... 145D9310 Consultation(diagnosticservicebynontreatingdentist) ........................................43 ............................................................ 43D9410 House/extendedcarefacilitycall...........................................................................200 .......................................................... 200D9420 Hospitalcall ...........................................................................................................350 .......................................................... 350D9430 Officevisitforobservation(duringregularlyscheduledhours)-no otherservicesperformed ....................................................................................0 .............................................................. 0D9440 Officevisitafterregularlyscheduledhours ............................................................90 ............................................................ 90D9450 Casepres,detailed/exttreatmentplanning............................................................43 ............................................................ 43D9610 Therapeuticparenteraldrug,singleadmin.............................................................26 ............................................................ 26D9612 Therapeuticparenteraldrug,2ormoreadmin.,diff.med. .....................................70 ............................................................ 70D9630 Drugsormedicamentsdispensedintheofficeforhomeuse ................................42 ............................................................ 42D9910 Applicationofdesensitizingmedicament ...............................................................31 ............................................................ 31D9911 Appl.ofdesen.resinforcervical/rootsurf. .............................................................38 ............................................................ 38D9920 Behaviormanagement,byreport ...........................................................................68 ............................................................ 68D9930 Treatmentofcomplications(post-surgical) ............................................................43 ............................................................ 43D9940 Occlusalguard,byreport ......................................................................................272 .......................................................... 272D9941 Fabricationofathleticmouthguard ........................................................................102 .......................................................... 102D9942 Repairand/orrelineofocclusalguard ..................................................................105 .......................................................... 105D9943 Occlusalguardadjustment.....................................................................................46 ............................................................ 46D9950 Occlusionanalysis-mountedcase.......................................................................104 .......................................................... 104D9951 Occlusaladjustment-limited .................................................................................66 ............................................................ 66D9952 Occlusaladjustment-complete ............................................................................266 .......................................................... 266D9971 Odontoplasty1-2teeth .........................................................................................48 ............................................................ 48D9974 Internalbleaching-pertooth ................................................................................163 .......................................................... 163D9986 Missedappointment ...............................................................................................50 ............................................................ 50D9995 Teledentistry-synchronous;real-timeencounter(whenavailable) .......................20 ............................................................ 20D9996 Teledentistry-asynchronous;informationstoredandforwardedtodentist forsubsequentreview(whenavailable) .............................................................20 ............................................................ 20
1 Specialty care is provided at the listed copayment whether performed by a Participating General Dentist or a Participating Plan Specialist. Referrals to a Participating Plan Specialist must be made by a member’s Participating General Dentist. See Plan Exclusion #9.2 See exclusion #10 and limitation #14 for additional coverage information.
OnlycurrentADACDTcodesareconsideredvalidbyDominionNational.Current Dental Terminology © American Dental Association.
ADA COVERED MEMBER ACTUAL CODE SERVICES COPAYMENT(S) COPAYMENT(S)
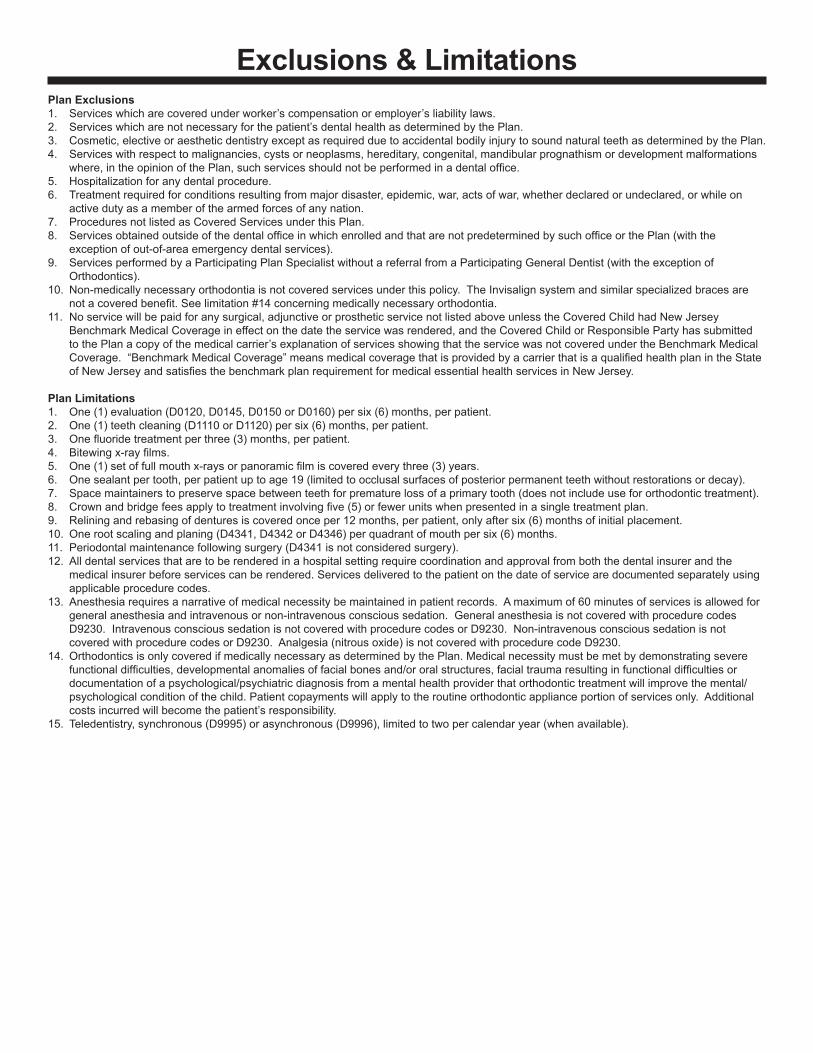
Plan Exclusions1. Serviceswhicharecoveredunderworker’scompensationoremployer’sliabilitylaws. 2. Serviceswhicharenotnecessaryforthepatient’sdentalhealthasdeterminedbythePlan.3. Cosmetic,electiveoraestheticdentistryexceptasrequiredduetoaccidentalbodilyinjurytosoundnaturalteethasdeterminedbythePlan.4. Serviceswithrespecttomalignancies,cystsorneoplasms,hereditary,congenital,mandibularprognathismordevelopmentmalformations where,intheopinionofthePlan,suchservicesshouldnotbeperformedinadentaloffice. 5. Hospitalizationforanydentalprocedure. 6. Treatmentrequiredforconditionsresultingfrommajordisaster,epidemic,war,actsofwar,whetherdeclaredorundeclared,orwhileon activedutyasamemberofthearmedforcesofanynation. 7. ProceduresnotlistedasCoveredServicesunderthisPlan. 8. ServicesobtainedoutsideofthedentalofficeinwhichenrolledandthatarenotpredeterminedbysuchofficeorthePlan(withthe exceptionofout-of-areaemergencydentalservices).9. ServicesperformedbyaParticipatingPlanSpecialistwithoutareferralfromaParticipatingGeneralDentist(withtheexceptionof Orthodontics). 10.Non-medicallynecessaryorthodontiaisnotcoveredservicesunderthispolicy.TheInvisalignsystemandsimilarspecializedbracesare notacoveredbenefit.Seelimitation#14concerningmedicallynecessaryorthodontia. 11.Noservicewillbepaidforanysurgical,adjunctiveorprostheticservicenotlistedaboveunlesstheCoveredChildhadNewJersey BenchmarkMedicalCoverageineffectonthedatetheservicewasrendered,andtheCoveredChildorResponsiblePartyhassubmitted tothePlanacopyofthemedicalcarrier’sexplanationofservicesshowingthattheservicewasnotcoveredundertheBenchmarkMedical Coverage.“BenchmarkMedicalCoverage”meansmedicalcoveragethatisprovidedbyacarrierthatisaqualifiedhealthplanintheState ofNewJerseyandsatisfiesthebenchmarkplanrequirementformedicalessentialhealthservicesinNewJersey.
Plan Limitations1. One(1)evaluation(D0120,D0145,D0150orD0160)persix(6)months,perpatient. 2. One(1)teethcleaning(D1110orD1120)persix(6)months,perpatient.3. Onefluoridetreatmentperthree(3)months,perpatient. 4. Bitewingx-rayfilms. 5. One(1)setoffullmouthx-raysorpanoramicfilmiscoveredeverythree(3)years. 6. Onesealantpertooth,perpatientuptoage19(limitedtoocclusalsurfacesofposteriorpermanentteethwithoutrestorationsordecay).7. Spacemaintainerstopreservespacebetweenteethforprematurelossofaprimarytooth(doesnotincludeusefororthodontictreatment).8. Crownandbridgefeesapplytotreatmentinvolvingfive(5)orfewerunitswhenpresentedinasingletreatmentplan. 9. Reliningandrebasingofdenturesiscoveredonceper12months,perpatient,onlyaftersix(6)monthsofinitialplacement. 10.Onerootscalingandplaning(D4341,D4342orD4346)perquadrantofmouthpersix(6)months. 11.Periodontalmaintenancefollowingsurgery(D4341isnotconsideredsurgery). 12.Alldentalservicesthataretoberenderedinahospitalsettingrequirecoordinationandapprovalfromboththedentalinsurerandthe medicalinsurerbeforeservicescanberendered.Servicesdeliveredtothepatientonthedateofservicearedocumentedseparatelyusing applicableprocedurecodes. 13.Anesthesiarequiresanarrativeofmedicalnecessitybemaintainedinpatientrecords.Amaximumof60minutesofservicesisallowedfor generalanesthesiaandintravenousornon-intravenousconscioussedation.Generalanesthesiaisnotcoveredwithprocedurecodes D9230.IntravenousconscioussedationisnotcoveredwithprocedurecodesorD9230.Non-intravenousconscioussedationisnot coveredwithprocedurecodesorD9230.Analgesia(nitrousoxide)isnotcoveredwithprocedurecodeD9230.14.OrthodonticsisonlycoveredifmedicallynecessaryasdeterminedbythePlan.Medicalnecessitymustbemetbydemonstratingsevere functionaldifficulties,developmentalanomaliesoffacialbonesand/ororalstructures,facialtraumaresultinginfunctionaldifficultiesor documentationofapsychological/psychiatricdiagnosisfromamentalhealthproviderthatorthodontictreatmentwillimprovethemental/ psychologicalconditionofthechild.Patientcopaymentswillapplytotheroutineorthodonticapplianceportionofservicesonly.Additional costsincurredwillbecomethepatient’sresponsibility. 15. Teledentistry,synchronous(D9995)orasynchronous(D9996),limitedtotwopercalendaryear(whenavailable).
Exclusions & Limitations

D2949 Restorative foundation for an indirect restoration ........... 0D2950 Core buildup, including any pins ................................. 125D2951 Pin retention - per tooth, in addition to restoration ........ 22D3110/20 Pulpcap-direct/indirect(excl.finalrestoration) ........... 32 CROWNS & BRIDGES♦
D2510 Inlay- metallic - one surface ........................................ 407D2520 Inlay- metallic - two surfaces ....................................... 407D2530 Inlay - metallic - three or more surfaces ...................... 425D2542 Onlay - metallic-two surfaces ...................................... 458D2543 Onlay - metallic - three surfaces ................................. 524D2544 Onlay - metallic - four or more surfaces ...................... 524D2610 Inlay - porcelain/ceramic - one surface ....................... 427D2620 Inlay - porcelain/ceramic - two surfaces ...................... 427D2630 Inlay - porcelain/ceramic - >=3 surfaces ..................... 445D2642 Onlay - porcelain/ceramic - two surfaces .................... 479D2643/44 Onlay - porcelain/ceramic - >=3 surfaces ................... 499D2650/51/52 Inlay-resin-basedcomposite->=1surface(s) ........... 440D2662/63/64 Onlay - resin-based composite - >=2 surfaces ........... 444D2710 Crown-resinbasedcomposite(indirect) ................... 272D2712 Crown-3/4resin-basedcomposite(indirect) ............. 485D2720/21/22 Crown - resin with metal ............................................. 495D2740 Crown - porcelain/ceramic substrate .......................... 560D2750/51/52 Crown - porcelain fused metal .................................... 523D2780/81/82 Crown - 3/4 cast with metal ......................................... 478D2783 Crown - 3/4 porcelain/ceramic .................................... 511D2790-94 Crown - full cast metal ................................................ 495D2910/20 Recement inlay, onlay/crown or partial coverage rest. ..... 43D2929 Procelain/cermaic crown - prim. tooth ......................... 560D2930 Prefab. stainless steel crown - prim. tooth .................. 110D2931 Prefab. stainless steel crown - perm. tooth ................. 121D2932 Prefabricated resin crown ........................................... 140D2952 Cast post and core in addition to crown ...................... 186D2954 Prefab. post and core in addition to crown .................. 154D2955 Postremoval(notinconj.withendo.therapy) ............ 105D2970 Temporarycrown(fracturedtooth) .................................. 0D2980 Crown repair, by report ............................................... 102D2981 Inlay repair .................................................................. 102D2982 Onlay repair ................................................................ 102D2983 Veneer repair .............................................................. 102D2990 Resininfitrationlesion ................................................... 41 PROSTHETICS (DENTURES)D5110/20 Complete denture - maxillary/mandibular ................... 697D5130/40 Immediate denture - maxillary/mandibular .................. 722D5211/12 Maxillary/mandibular partial denture - resin base ....... 649D5213/14 Maxillary/mandibular partial denture - cast metal ....... 750D5221/22 Immediate maxillary/mandibular partial denture - resin base ........................................................... 649D5223/24 Immediate maxillary/mandibular partial denture - cast metal ........................................................... 750D5225/26 Maxillary/mandibularpartialdenture-flexiblebase .... 750D5281 Rem. unilateral partial denture - one piece cast metal.... 419D5410/11 Adjust complete denture - maxillary/mandibular ........... 38D5421/22 Adjust partial denture - maxillary/mandibular ................ 38D5510/5610 Repairbrokencompletedenturebase(complete/resin) ...87D5520 Replace missing or broken teeth - complete denture ... 87D5620 Repair cast framework .................................................. 87D5630/60 Clasp repaired, replaced or added .............................. 115
D9439 Officevisit ..................................................................... 10 DIAGNOSTIC/PREVENTIVED0120 Periodic oral eval - established patient ........................... 0D0140 Limited oral eval - problem focused ................................ 0D0145 Oral eval for a patient under 3 years of age .................... 0D0150 Comprehensive oral eval - new or established patient ... 0D0160 Detailed and extensive oral eval - problem focused ....... 0D0170 Re-evaluation - limited, problem focused ........................ 0D0210 Intraoral-completeseries(includingbitewings) ........... 26D0220/30 Intraoral-periapicalfirstfilmandeachadditional ........... 0D0240 Intraoral-occlusalfilm .................................................... 0D0250 Extraoralfilm ................................................................... 0D0270-74 Bitewingx-rays-1-4films ............................................... 0D0277 Verticalbitewings-7to8films ........................................ 0D0330 Panoramicfilm .............................................................. 30D0340 2D cephalometric radiographic image ............................ 0D0350 Oral/facialphotographicimages(intraoral/extraoral) ...... 0D0351 3D photographic image ................................................... 0D0391 Interpretation of diagnostic image only ........................... 0D0460 Pulp vitality tests ............................................................. 0D0470 Diagnostic casts .............................................................. 0D0601/02/03 Caries risk assessment/documentation, withafindingoflow/moderate/highrisk .................... 0D1110 Prophylaxis(cleaning)-adult .......................................... 0D1120 Prophylaxis(cleaning)-child .......................................... 0D1206 Topicalfluoridevarnishformod/highriskcariespatients .... 0D1208 Topicalapplicationoffluoride .......................................... 0D1310 Nutritional counseling for control of dental disease ........ 0D1320/30 Oral hygiene instructions ................................................ 0D1351 Sealant - per tooth ........................................................ 21D1352 Prev resin rest. mod/high caries risk – perm. tooth ....... 21 SPACE MAINTAINERSD1510/20 Spacemaintainer-fixed/removable-unilateral .......... 143D1515/25 Spacemaintainer-fixed/removable-bilateral ............ 198D1550 Re-cementation of space maintainer ............................ 34 D1575 Distalshoespacemaintainer-fixed-unilateral ......... 143 RESTORATIVE DENTISTRY (FILLINGS) AMALGAMRESTORATIONS(SILVER)D2140 Amalgam - one surface, prim. or perm. ........................ 41D2150 Amalgam - two surfaces, prim. or perm. ....................... 51D2160 Amalgam - three surfaces, prim. or perm. .................... 64D2161 Amalgam - >=4 surfaces, prim. or perm. ...................... 78 RESIN/COMPOSITERESTORATIONS(TOOTHCOLORED)D2330 Resin-based composite - one surface, anterior ............ 69D2331 Resin-based composite - two surfaces, anterior ........... 83D2332 Resin-based composite - three surfaces, anterior ........ 99D2335 Resin-based composite - >=4 surfaces, anterior ........ 119D2390 Resin-based composite crown, anterior ...................... 192D2391 Resin-based composite - one surface, posterior .......... 73D2392 Resin-based composite - two surfaces, posterior ......... 87D2393 Resin-based composite - three surfaces, posterior .... 102D2394 Resin-based composite - >=4 surfaces, posterior ...... 123 D2940 Protective restoration ................................................... 39D2941 Interim therapeutic restoration, primary dentition .......... 31
DMNPA18DBLINDPEDEHB All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.
Select Plan Basic Kids 702xs (PA)Description of Benefits & Member Copayments for Pediatric Services (under age 19)
Coverage continues through end of month in which the Member turns 19.
The dental plan is underwritten by Dominion Dental Services, Inc. d/b/a Dominion National.
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
Annual Out-of-Pocket Maximum: $350 per child per calendar year for medically necessary treatment (maximum of $700 for policy covering two or more children)

D5640 Replace broken teeth - per tooth .................................. 87D5650 Add tooth to existing partial denture ............................. 87D5670/71 Replace all teeth and acrylic on cast metal framework (maxillary/mandibular) ........................................... 287D5710/11 Rebase complete maxillary/mandibular denture ......... 260D5720/21 Rebase maxillary/mandibular partial denture .............. 260D5730/31 Relinecompletemaxillary/mandibulardenture(chairside) ..159D5740/41 Relinemaxillary/mandibularpartialdenture(chairside) .. 155D5750/51 Relinecompletemaxillary/mandibulardenture(lab) ... 224D5760/61 Relinemaxillary/mandibularpartialdenture(lab) ........ 224D5810/11 Interim complete denture - maxillary/mandibular ........ 362D5820/21 Interim partial denture - maxillary/mandibular ............. 362D5850/51 Tissue conditioning - maxillary/mandibular ................... 79 BRIDGES & PONTICS♦
D6010 Surgical placement of implant body, endosteal ......... 1716D6011 Second stage implant surgery .................................... 200D6012 Surgical placement of interim implant body .............. 1782D6013 Surgical placement of mini implant ............................. 572D6040 Surgical placement, eposteal implant ....................... 3564D6050 Surgical placement, transosteal implant ................... 4455D6055 Dental implant supported connecting bar ................. 1611D6056 Prefabricated abutment ............................................... 456D6058 Abutment supported porcelain/ceramic crown ............ 560D6059/60/61 Abutment supported porcelain fused to metal crown - metal .. 523D6062/63/64 Abutment supported cast metal crown - metal ............ 495D6065 Implant supported porcelain/ceramic crown ............... 560D6066 Implant supported porcelain fused to metal crown - titanium, titanium allow, high noble metal ............. 523D6067 Implant supported metal crown - titanium, titanium alloy, high noble metal .............. 523D6068 Abutment supported retainer for porc/ceramic ............ 788D6069 Abutment supp. retainer for porc/high noble ............... 843D6070 Abutment supp. retainer for porc/pred. base .............. 695D6071 Abutment supp. retainer for porc/noble ....................... 704D6072 Abutment supp retainer for cast high noble ................ 788D6073 Abutment supp. retainer for cast high noble ............... 749D6074 Abutment supp. retainer for cast noble metal ............. 758D6075 Implant supported retainer for ceramic FPD ............... 874D6076 Implant supported retainer for porc/metal FPD ........... 823D6077 Implant supported retainer for cast metal FPD ........... 872D6080 Implant maintenance procedures .................................. 61D6081 Scalinganddebridementinthepresenceofinflammation or mucositis of a single implant, including cleaning of theimplantsurfaces,withoutflapentryandclosure .....63 D6090 Repair implant supported prosthesis .......................... 362D6091 Replacement of precision attachment ........................... 34D6095 Repair implant abutment, by report ............................. 391D6100 Implant removal, by report .......................................... 241D6101 Debribement periimplant defect .................................... 90D6102 Deridement and osseous contouring periimplant defect... 180D6103 Bone graft repair perrimplant defect ........................... 600D6104 Bone graft at time of implant placement ..................... 600D6190 Radiographic surgical implant index, by report ............... 0D6210-14 Pontic - metal .............................................................. 495D6240/41/42 Pontic - porcelain fused to metal ................................. 523D6245 Pontic - porcelain/ceramic ........................................... 560D6250/51/52 Pontic - resin with metal .............................................. 495D6545 Ret.-castmetalforresinbondedfixedprosthesis ..... 251D6548 Ret.-porc./ceramicforresinbondedfixedprosthesis .. 393D6549 Resinretainer-forresinbondedfixedprosthesis ...... 251D6600 Inlay - porc./ceramic, two surfaces ............................. 427D6601 Inlay - porc./ceramic, >=3 surfaces ............................. 445D6602 Inlay - cast high noble metal, two surfaces ................. 407D6603 Inlay - cast high noble metal, >=3 surfaces ................ 425D6604 Inlay - cast predominantly base metal, two surfaces .... 407D6605 Inlay - cast predominantly base metal, >=3 surfaces ... 425D6606 Inlay - cast noble metal, two surfaces ......................... 407D6607 Inlay - cast noble metal, >=3 surfaces ........................ 425
D6608 Onlay -porc./ceramic, two surfaces ............................. 479D6609 Onlay - porc./ceramic, three or more surfaces ............ 499D6610 Onlay - cast high noble metal, two surfaces ............... 458D6611 Onlay - cast high noble metal, >=3 surfaces ............... 524D6612 Onlay - cast predominantly base metal, two surfaces .... 458D6613 Onlay - cast predominantly base metal, >=3 surfaces... 524D6614 Onlay - cast noble metal, two surfaces ....................... 458D6615 Onlay - cast noble metal, >=3 surfaces ...................... 524D6720/21/22 Crown - resin with metal ............................................. 495D6740 Crown - porcelain/ceramic .......................................... 560D6750/51/52 Crown - porcelain fused metal .................................... 523D6780/81/82 Crown - 3/4 cast metal ................................................ 470D6783 Crown - 3/4 porc./ceramic ........................................... 511D6790/91/92 Crown - full cast metal ................................................ 495D6930 Recementfixedpartialdenture ..................................... 69D6980 Fixed partial denture repair, by report ......................... 172 ADJUNCTIVE GENERAL SERVICESD9110 Palliative(emergency)treatmentofdentalpain ............ 43D9210/15 Local anesthesia ............................................................. 0D9211/12 Regional block anesthesia .............................................. 0D9223 Deep sedation/general anesthesia - each 15 min. .........103D9230 Analgesia, anxiolysis, inhalation of nitrous oxide .......... 37D9243 Intravenous conscious sedation/analgesia - each 15 min. 103D9310 Consultation(diagnosticservicebynontreatingdentist) ... 43D9610 Therapeutic parenteral drug, single admin. .................. 26D9910 Application of desensitizing medicament ...................... 31D9930 Treatmentofcomplications(post-surgical) ................... 43D9940 Occlusal guard, by report ............................................ 272D9950 Occlusion analysis - mounted case ............................ 104D9951 Occlusal adjustment - limited ........................................ 66D9952 Occlusal adjustment - complete .................................. 266D9986 Missed appointment ...................................................... 50D9995 Teledentistry - synchronous; real-time encounter (whenavailable) ..................................................... 20 D9996 Teledentistry - asynchronous; information stored and forwarded to dentist for subsequent review (whenavailable) ..................................................... 20 ENDODONTICS1 D3220 Therapeuticpulpotomy(excl.finalrestor.) .................... 81D3221 Pulpal debridement, prim. and perm. teeth ................... 94D3222 Partial pulpotomy for apexogenesis ............................ 160D3230 Pulpaltherapy-resorbablefilling,anterior ................. 160D3240 Pulpaltherapy-resorbablefilling,posterior ................ 164D3310 Endodontic therapy, anterior tooth .............................. 341D3320 Endodontic therapy, bicuspid tooth ............................. 418D3330 Endodontic therapy, molar .......................................... 512D3333 Internal root repair of perforation defects .................... 105D3346 Retreat of prev. root canal therapy, anterior ................ 387D3347 Retreat of prev. root canal therapy, bicuspid ............... 465D3348 Retreat of prev. root canal therapy, molar ................... 558D3351 Apexification/recalcification-initialvisit ...................... 202D3352 Apexification/recalcification-interimmed.repl. .......... 589D3353 Apexification/recalcification-finalvisit ........................ 449D3355 Pulpal regeneration - initial visit .................................. 202D3356 Pulpal regeneration - interim medication replacement ....589D3357 Pulpal regeneration - completion of treatment ............ 449D3410 Apicoectomy - anterior ................................................ 323D3421 Apicoectomy-bicuspid(firstroot) ....................................364D3425 Apicoectomy-molar(firstroot) ................................... 418D3426 Apicoectomy-(eachadd.root) ................................... 152D3427 Periradicular surgery w/o apicoectomy ....................... 266D3430 Retrogradefilling-perroot ......................................... 119D3450 Root amputation - per root .......................................... 234D3920 Hemisection, not inc. root canal therapy ..................... 234D3950 Canalprep/fittingofpreformeddowelorpost ............. 136
ADA MEMBERCODE BENEFIT COPAYMENT(S)
ADA MEMBERCODE BENEFIT COPAYMENT(S)
All fees exclude the cost of noble and precious metals. An additional fee will be charged if these materials are used.

ADA MEMBERCODE BENEFIT COPAYMENT(S)
PERIODONTICS1 D0180 Comp. periodontal eval - new or established patient ...... 0D4210 Gingivectomy or gingivoplasty - >3 cont. teeth, per quad. .. 279D4211 Gingivectomy or gingivoplasty - <=3 teeth, per quad. .. 100D4212 Gingivectomy or gingivoplasty, rest., per tooth ............. 40D4240 Gingivalflapproc.,inc.rootplaning- >3 cont. teeth, per quad........................................ 345D4241 Gingivalflapproc,inc.rootplaning- <=3 cont. teeth, per quad ..................................... 106D4249 Clinical crown lengthening - hard tissue ..................... 576D4260 Osseous surgery - >3 cont. teeth, per quad ............... 499D4261 Osseous surgery - <=3 cont. teeth, per quad ............. 392D4268 Surgical revision proc., per tooth ................................ 358D4270 Pedicle soft tissue graft procedure .............................. 643D4273 Subepithelial connective tissue graft proc. .................. 800D4274 Mesial/distal wedge procedure, single tooth ............... 308D4277 Free soft tissue graft, per tooth ................................... 654D4278 Free soft tissue graft, each add. tooth ........................ 100D4341 Perio scaling and root planing - >3 cont teeth, per quad. . 109D4342 Perio scaling and root planing - <= 3 teeth, per quad ... 63D4346 Scaling in presence of generalized moderate or severegingivalinflammation-fullmouth, after oral evaluation .................................................. 45 D4355 Full mouth debridement ................................................ 89D4381 Localized delivery of chemotherapeutic agents ............ 98D4910 Periodontal maintenance .............................................. 74D4921 Gingival irrigation - per quadrant ..................................... 0 ORAL SURGERY1 D7111 Extraction, coronal remnants - deciduous tooth ............ 56D7140 Extraction, erupted tooth or exposed root ..................... 69D7210 Extraction, erupted tooth req. bone cut ....................... 133D7220 Removal of impacted tooth - soft tissue ...................... 151D7230 Removal of impacted tooth - partially bony ................. 196D7240 Removal of impacted tooth - completely bony ............ 241D7241 Removal of imp. tooth - completely bony, with unusual surg. complications .......................... 217D7250 Removal of residual tooth roots .................................. 141D7251 Coronectomy-intentional partial tooth removal ........... 217D7270 Tooth reimplant./stabiliz. of acc. evulsed/displaced tooth.... 226D7280 Surgical access of an unerupted tooth ........................ 153D7291 Transseptalfiberotomy/supracrestalfiberotomy,byreport ... 60D7310/20 Alveoloplasty, >=4 per quad. ....................................... 141D7311/21 Alveoloplasty, 1-3 per quad. ......................................... 141D7471 Removal of lateral exostosis ....................................... 351D7510 Incision and drainage of abscess - intraoral soft tissue .... 96D7910 Suture of recent small wounds up to 5 cm .................... 59D7921 Collection application of blood concentrate .................. 40D7960 Frenulectomy(frenectomy/frenotomy)-separateproc... 263D7971 Excision of pericoronal gingiva ................................... 131 ORTHODONTICS2 - PRE-AUTHORIZATION REQUIREDD8010 Limited ortho. treatment of the primary dentition ...... 3304D8020 Limited ortho. treatment of the transitional dentition ... 3304D8030 Limited ortho treatment - adolescent dentition .......... 3422D8050 Interceptive ortho. treatment of the primary dentition .. 3304D8060 Interceptive ortho. treatment - transitional dentition .. 3304D8070 Comp. ortho. treatment - transitional dentition .......... 3304D8080 Comp. ortho. treatment - adolescent dentition .......... 3422D8090 Comp. ortho. treatment - adult dentition ................... 3658D8210 Removable appliance therapy .................................... 770D8220 Fixed appliance therapy .............................................. 783D8660 Pre-orthodontic treatment visit .................................... 413D8670 Periodicortho.treatmentvisit(aspartofcontract) ..... 118D8680 Orthodonticret.(rem.ofappl./placementofretainer(s)) ... 413
1 Specialty care is provided at the listed copayment whether performed by a Participating General Dentist or a Participating Specialist. Referrals to a specialist must be made by a member’s Participating General Dentist. See Plan Exclusion #13. 2 See exclusion #15 and limitation #23 for additional coverage information.
Only current ADA CDT codes are considered valid by Dominion National Current Dental Terminology © American Dental Association.

Exclusions & LimitationsPlan Exclusions1. Services which are covered under worker’s compensation, employer’s liability laws or the Pennsylvania Motor Vehicle Financial Responsibility Law.2. Services which are not necessary for the patient’s dental health as determined by the Plan.3. Cosmetic, elective or aesthetic dentistry except as required due to accidental bodily injury to sound natural teeth as determined by the Plan.4. Oral surgery requiring the setting of fractures or dislocations.5. Services with respect to malignancies, cysts or neoplasms, hereditary, congenital, mandibular prognathism or development malformations where,intheopinionofthePlan,suchservicesshouldnotbeperformedinadentaloffice.6. Dispensing of drugs.7. Hospitalization for any dental procedure.8. Treatment required for conditions resulting from major disaster, epidemic, war, acts of war, whether declared or undeclared, or while on active duty as a member of the armed forces of any nation.9. Replacement due to loss or theft of prosthetic appliance.10. ProceduresnotlistedascoveredbenefitsunderthisPlan.11. ServicesobtainedoutsideofthedentalofficeinwhichenrolledandthatarenotpreauthorizedbysuchofficeorthePlan(withtheexception ofout-of-areaemergencydentalservices).12. ServicesrelatedtothetreatmentofTMD(TemporomandibularDisorder)exceptifTMDiscausedbysevere,dysfunctional,handicapping malocclusion that requires medically necessary orthodontia services.13. ServicesperformedbyaParticipatingSpecialistwithoutareferralfromaParticipatingGeneralDentist(withtheexceptionofOrthodontics). Participating dentists should refer to Specialty Care Referral Guidelines.14. Elective surgery including, but not limited to, extraction of non-pathologic, asymptomatic impacted teeth as determined by the Plan. The prophylactic removal of these teeth for medically necessary orthodontia services may be covered subject to review.15. Non-medically necessary orthodontia and Phase I Treatment codes D8010 and D8050 for medically necessary orthodontia are not coveredbenefitsunderthispolicy.DiscountsareprovidedtomembersthroughthePlan’sagreementswithitsparticipatingorthodontists. The provider agreements create no liability for payment by the Plan, and payments by the member for these services do not contribute totheOut-of-PocketMaximum.TheInvisalignsystemandsimilarspecializedbracesarenotacoveredbenefit.Seelimitation#23 concerning medically necessary orthodontia.
Plan Limitations1. One(1)evaluation(D0120,D0140,D0145,D0150,D0180)iscoveredpersix(6)months,perpatient.2. One(1)teethcleaning(D1110orD1120)persix(6)months,perpatient.3. One(1)fluorideapplicationeverysix(6)months,perpatient.4. One(1)setofbitewingx-raysarecoveredpersix(6)months.5. One(1)setoffullmouthx-raysorpanoramicfilmiscoveredeveryfive(5)years.Panoramicx-raysarelimitedtoagessix(6)andabove. Nomorethanone(1)setofx-raysarecoveredpervisit.6. One(1)sealantpertoothiscoveredper36months,perpatient(limitedtoocclusalsurfacesofposteriorpermanentteethwithout restorationsordecay).7. Replacementofaprimarystainlesssteelcrown(underage15),crown,dentureorotherprosthodonticapplianceiscoveredifitismore thanfive(5)yearsfromthedateoforiginalplacement.8. Crownandbridgefeesapplytotreatmentinvolvingfive(5)orfewerunitswhenpresentedinasingletreatmentplan.Additionalcrownor bridgeunits,beginningwiththesixthunit,areavailableattheprovider’sUsual,CustomaryandReasonable(UCR)fee,minus25%.9. One(1)reliningandrebasingofdenturesiscoveredper24months,perpatient.10. Periodontalscalingandrootplaning(D4341orD4342),limitedtoone(1)per24months,perpatient,perquadrant.11. Scalinginpresenceofgeneralizedmoderateorseveregingivalinflammation-fullmouth,afteroralevaluationandinlieuofacovered D1110/D1120, limited to once per two years. 12. Osseoussurgery(D4260orD4261),gingivalflapprocedure(D4240)andgingivectomyorgingivoplasy(D4210-D4212)arelimitedtoone (1)per36months.13. One(1)fullmouthdebridementiscoveredperlifetime,perpatient.14. ProcedureCodeD4381islimitedtoone(1)benefitpertoothforthree(3)teethperquadrant;oratotalof12teethforallfour(4)quadrants pertwelve(12)months.Musthavepocketdepthsoffive(5)millimetersorgreater.15. One(1)periodontalsurgeryofanytype,includinganyassociatedmaterial,iscoveredevery24months,perquadrantorsurgicalsite.16. Periodontalmaintenanceiscoveredfour(4)timespercalendaryearinadditiontoadultprophylaxis,within24monthsafterdefinitive periodontal therapy.17. One(1)scalinganddebridementinthepresenceofinflammationormucositisofasingleimplant,includingcleaningoftheimplant surfaces,withoutflapentryandclosure,pertwo(2)years. 18. Coronectomy,intentionalpartialtoothremoval,one(1)perlifetime. 19. Generalanesthesiaandanalgesic(onlywhenprovidedinconnectionwithacoveredprocedure(s)whendeterminedtobemedicallyor dentallynecessaryfordocumentedhandicappedoruncontrollablepatientsorjustifiablemedicalordentalconditions),including intravenous and non-intravenous sedation with a maximum of 60 minutes of services allowed (general anesthesia is not covered with procedure codes D9230 or D9243; intravenous conscious sedation is not covered with procedure code D9223; non-intravenous conscious sedation is not covered with procedure code D9223; requires a narrative of medical necessity be maintained in patient records.20. Occlusal guards are covered by report for patients 13 years of age or older when the purpose of the occlusal guard is for the treatment of bruxismordiagnosesotherthantemporomandibulardysfunction(TMD).Occlusalguardsarelimitedtoone(1)per12consecutive month period. 21. Fixed partial dentures, buildups, and posts and cores for members under 16 years of age are only covered if deemed necessary by the Plan.22. Onlays, crowns, and posts and cores for members 12 years of age or younger are only covered if deemed necessary by the Plan. Cast postsandcores(D2952)areprocessedasanalternatebenefitofaprefabricatedpostandcore.Postsareeligibleonlywhenprovidedas part of a crown buildup or implant and are considered integral to the buildup or implant. 23. Orthodontics is only covered if medically necessary as determined by the Plan. Patient copayments will apply to the routine orthodontic appliance portion of services only. Additional costs incurred will become the patient’s responsibility. 24. Teledentistry,synchronous(D9995)orasynchronous(D9996),limitedtotwopercalendaryear(whenavailable).

D9439 Officevisit ......................................................................................................10 ........................................................10 DIAGNOSTIC/PREVENTIVED0120 Periodicoraleval-establishedpatient ...........................................................0 ..........................................................0D0140 Limitedoraleval-problemfocused ................................................................0 ..........................................................0D0145 Oralevalforapatientunder3yearsofage ....................................................0 ..........................................................0D0150 Comprehensiveoraleval-neworestablishedpatient ...................................0 ..........................................................0D0160 Detailedandextensiveoraleval-problemfocused .......................................0 ..........................................................0D0170 Re-evaluation-limited,problemfocused ........................................................0 ..........................................................0D0210 Intraoral-completeseries(includingbitewings) ............................................26 ........................................................26D0220/30 Intraoral-periapicalfirstfilmandeachadditional ...........................................0 ..........................................................0D0240 Intraoral-occlusalfilm ....................................................................................0 ..........................................................0D0250 Extraoral ..........................................................................................................0 ..........................................................0D0270-74 Bitewingx-rays-1-4films ...............................................................................0 ..........................................................0D0277 Verticalbitewings-7to8films ........................................................................0 ..........................................................0D0330 Panoramicfilm ...............................................................................................30 ........................................................30D0340 Cephalometricfilm ..........................................................................................0 ..........................................................0D0350 Oral/facialphotographicimages .....................................................................0 ..........................................................0D0351 3Dphotographicimage ...................................................................................0 ..........................................................0 D0460 Pulpvitalitytests .............................................................................................0 ..........................................................0D0470 Diagnosticcasts ..............................................................................................0 ..........................................................0D1110 Prophylaxis(cleaning)-adult ..........................................................................0 ..........................................................0D1120 Prophylaxis(cleaning)-child ..........................................................................0 ..........................................................0D1206 Topicalfluoridevarnishformod/highriskcariespatients ................................0 ..........................................................0D1208 Topicalapplicationoffluoride ..........................................................................0 ..........................................................0D1310 Nutritionalcounselingforcontrolofdentaldisease ........................................0 ..........................................................0D1320/30 Oralhygieneinstructions ................................................................................0 ..........................................................0D1351 Sealant-pertooth .........................................................................................21 ........................................................21D1352 Prevresinrest.mod/highcariesrisk–perm.tooth ........................................21 ........................................................21 SPACE MAINTAINERSD1510/20 Spacemaintainer-fixed/removable-unilateral ............................................143 ......................................................143D1515/25 Spacemaintainer-fixed/removable-bilateral ..............................................198 ......................................................198D1550 Re-cementationofspacemaintainer .............................................................34 ........................................................34D1555 Removaloffixedspacemaintainer,bynon-originatingdentist .....................44 ........................................................44D1575 Distalshoespacemaintainer-fixed-unilateral ...........................................143 ......................................................143
RESTORATIVE DENTISTRY (FILLINGS) AMALGAMRESTORATIONS(SILVER)D2140 Amalgam-onesurface,prim.orperm. .........................................................41 ........................................................41D2150 Amalgam-twosurfaces,prim.orperm. ........................................................51 ........................................................51D2160 Amalgam-threesurfaces,prim.orperm. .....................................................64 ........................................................64D2161 Amalgam->=4surfaces,prim.orperm. .......................................................78 ........................................................78 RESIN/COMPOSITERESTORATIONS(TOOTHCOLORED)D2330 Resin-basedcomposite-onesurface,anterior .............................................69 ........................................................69D2331 Resin-basedcomposite-twosurfaces,anterior ............................................83 ........................................................83D2332 Resin-basedcomposite-threesurfaces,anterior .........................................99 ........................................................99D2335 Resin-basedcomposite->=4surfaces,anterior .......................................... 119 ...................................................... 119D2390 Resin-basedcompositecrown,anterior ........................................................192 ......................................................192D2391 Resin-basedcomposite-onesurface,posterior ...........................................73 ........................................................73D2392 Resin-basedcomposite-twosurfaces,posterior ..........................................87 ........................................................87D2393 Resin-basedcomposite-threesurfaces,posterior ......................................102 ......................................................102D2394 Resin-basedcomposite->=4surfaces,posterior ........................................123 ......................................................123
D2940 Protectiverestoration .....................................................................................39 ........................................................39D2950 Corebuildup,includinganypins ...................................................................125 ......................................................125D2951 Pinretention-pertooth,inadditiontorestoration .........................................22 ........................................................22D3110/20 Pulpcap-direct/indirect(excl.finalrestoration) ............................................32 ........................................................32 CROWNS & BRIDGES♦
D2510/20 Inlay-metallic-onetotwosurfaces ..............................................................407 ......................................................407D2530 Inlay-metallic-threeormoresurfaces ........................................................425 ......................................................425D2542 Onlay-metallic-twosurfaces ........................................................................458 ......................................................458D2543/44 Onlay-metallic-threeormoresurfaces ......................................................524 ......................................................524D2610/20 Inlay-porcelain/ceramic-onetotwosurfaces .............................................427 ......................................................427
DMNVA18DBLINDPEDEHB ♦Allfeesexcludethecostofnobleandpreciousmetals.Anadditionalfeewillbechargedifthesematerialsareused.
ADA MEMBER ACTUAL CODE BENEFIT COPAYMENT(S) COPAYMENT(S)
Select Plan Basic Kids 702xs (VA)Description of Benefits & Member Copayments for Pediatric Services (under age 19)
CoveragecontinuesthroughendofmonthinwhichtheMemberturns19.
Underwritten by: Dominion Dental Services, Inc. d/b/a Dominion National
Annual Out-of-Pocket Maximum: $350 per child per calendar year for medically necessary treatment (maximum of $700 for policy covering two or more children). The member shall only be responsible for the copayment listed in Member Copayment column. Any procedure listed that has a Member Copayment above the annual out-of-pocket maximum may apply as these procedures are not considered medically necessary and are included as additional benefits. The Plan is responsible for the difference between the Actual Copayment and the Member Copayment for all medically necessary treatment.

D2630 Inlay-porcelain/ceramic->=3surfaces .......................................................445 ......................................................445D2642 Onlay-porcelain/ceramic-twosurfaces ......................................................479 ......................................................479D2643/44 Onlay-porcelain/ceramic->=3surfaces .....................................................350 ......................................................499D2650/51/52 Inlay-resin-basedcomposite->=1surface(s) .............................................440 ......................................................440D2662/63/64 Onlay-resin-basedcomposite->=2surfaces .............................................444 ......................................................444D2710 Crown-resinbasedcomposite(indirect) .....................................................272 ......................................................272D2712 Crown-3/4resin-basedcomposite(indirect) ...............................................485 ......................................................485D2720/21/22 Crown-resinwithmetal ...............................................................................350 ......................................................495D2740 Crown-porcelain/ceramicsubstrate ............................................................350 ......................................................560D2750/51/52 Crown-porcelainfusedtometal ..................................................................350 ......................................................523D2780/81/82 Crown-3/4castwithmetal ...........................................................................478 ......................................................478D2783 Crown-3/4porcelain/ceramic ...................................................................... 511 ...................................................... 511D2790-94 Crown-fullcastmetal ..................................................................................350 ......................................................495D2910/20 Recementinlay,onlay/crownorpartialcoveragerest. ..................................43 ........................................................43D2915 Recementcastorprefab.postandcore ........................................................82 ........................................................82D2929 Procelain/ceramiccrown-prim.tooth ...........................................................350 ......................................................560D2930 Prefab.stainlesssteelcrown-prim.tooth .................................................... 110 ...................................................... 110D2931 Prefab.stainlesssteelcrown-perm.tooth ...................................................121 ......................................................121D2932 Prefabricatedresincrown .............................................................................140 ......................................................140D2933 Prefab.stainlesssteelcrownw/resinwindow ..............................................271 ......................................................271D2934 Prefab.estheticcoatedprimarytooth ...........................................................296 ......................................................296D2941 Interimtherapeuticrestoration,primarydentition ...........................................31 ........................................................31D2952 Castpostandcoreinadditiontocrown ........................................................186 ......................................................186D2954 Prefab.postandcoreinadditiontocrown ....................................................154 ......................................................154D2955 Postremoval(notinconj.withendo.therapy) ..............................................105 ......................................................105D2962 Labialveneer(porcelainlaminate)-laboratory .............................................350 ......................................................449D2970 Temporarycrown(fracturedtooth) ..................................................................0 ..........................................................0D2980 Crownrepair,byreport .................................................................................102 ......................................................102 PROSTHETICS (DENTURES)D5110/20 Completedenture-maxillary/mandibular .....................................................350 ......................................................697D5130/40 Immediatedenture-maxillary/mandibular ....................................................350 ......................................................722D5211/12 Maxillary/mandibularpartialdenture-resinbase .........................................350 ......................................................649D5213/14 Maxillary/mandibularpartialdenture-castmetal .........................................350 ......................................................750D5221/22 Immediatemaxillary/mandibularpartialdenture ...........................................649 ......................................................649D5223/24 Immediatemaxillary/mandibularpartialdenture ...........................................750 ......................................................750D5225/26 Maxillary/mandibularpartialdenture-flexiblebase ......................................350 ......................................................750D5281 Rem.unilateralpartialdenture-onepiececastmetal ..................................350 ......................................................419D5410/11 Adjustcompletedenture-maxillary/mandibular ............................................38 ........................................................38D5421/22 Adjustpartialdenture-maxillary/mandibular .................................................38 ........................................................38D5510/5610 Repairbrokencompletedenturebase(complete/resin) ................................87 ........................................................87D5520 Replacemissingorbrokenteeth-completedenture ....................................87 ........................................................87D5620 Repaircastframework ...................................................................................87 ........................................................87D5630/60 Clasprepaired,replacedoradded ................................................................ 115 ...................................................... 115D5640 Replacebrokenteeth-pertooth ...................................................................87 ........................................................87D5650 Addtoothtoexistingpartialdenture ..............................................................87 ........................................................87D5670/71 Replaceallteeth/acryliconcastmetalframework(maxillary/mandibular) ...287 ......................................................287D5710/11 Rebasecompletemaxillary/mandibulardenture ...........................................260 ......................................................260D5720/21 Rebasemaxillary/mandibularpartialdenture ................................................260 ......................................................260D5730/31 Relinecompletemaxillary/mandibulardenture(chairside) .........................................159 ......................................................159D5740/41 Relinemaxillary/mandibularpartialdenture(chairside) .......................................155 ......................................................155D5750/51 Relinecompletemaxillary/mandibulardenture(lab) .....................................224 ......................................................224D5760/61 Relinemaxillary/mandibularpartialdenture(lab) ..........................................224 ......................................................224D5810/11 Interimcompletedenture-maxillary/mandibular ..........................................362 ......................................................362D5820/21 Interimpartialdenture-maxillary/mandibular ...............................................362 ......................................................362D5850/51 Tissueconditioning-maxillary/mandibular ....................................................79 ........................................................79D5951 Feedingaid ...................................................................................................350 .....................................................1395
BRIDGES & PONTICS♦
D6205 Pontic-indirectresinbasedcomposite ........................................................350 ......................................................445D6210-14 Pontic-metal ................................................................................................350 ......................................................495D6240/41/42 Pontic-porcelainfusedtometal ...................................................................350 ......................................................523D6245 Pontic-porcelain/ceramic .............................................................................350 ......................................................560D6250/51/52 Pontic-resinwithmetal ................................................................................350 ......................................................495D6545 Ret.-castmetalforresinbondedfixedprosthesis .......................................251 ......................................................251D6548 Ret.-porc./ceramicforresinbondedfixedprosthesis .....................................350 ......................................................393D6549 Resinret.forresinbondedfixedprosthesis ..................................................251 ......................................................251D6600 Inlay-porc./ceramic,twosurfaces ...............................................................427 ......................................................427D6601 Inlay-porc./ceramic,>=3surfaces ...............................................................445 ......................................................445D6602 Inlay-casthighnoblemetal,twosurfaces ...................................................407 ......................................................407D6603 Inlay-casthighnoblemetal,>=3surfaces ..................................................425 ......................................................425D6604 Inlay-castpredominantlybasemetal,twosurfaces ....................................407 ......................................................407D6605 Inlay-castpredominantlybasemetal,>=3surfaces ....................................425 ......................................................425D6606 Inlay-castnoblemetal,twosurfaces ...........................................................407 ......................................................407D6607 Inlay-castnoblemetal,>=3surfaces ..........................................................425 ......................................................425D6608 Onlay-porc./ceramic,twosurfaces ...............................................................479 ......................................................479D6609 Onlay-porc./ceramic,threeormoresurfaces ..............................................499 ......................................................499D6610 Onlay-casthighnoblemetal,twosurfaces .................................................458 ......................................................458D6611 Onlay-casthighnoblemetal,>=3surfaces .................................................524 ......................................................524D6612 Onlay-castpredominantlybasemetal,twosurfaces ..................................458 ......................................................458D6613 Onlay-castpredominantlybasemetal,>=3surfaces ..................................524 ......................................................524D6614 Onlay-castnoblemetal,twosurfaces .........................................................458 ......................................................458
ADA MEMBER ACTUAL CODE BENEFIT COPAYMENT(S) COPAYMENT(S)
♦Allfeesexcludethecostofnobleandpreciousmetals.Anadditionalfeewillbechargedifthesematerialsareused.

D6615 Onlay-castnoblemetal,>=3surfaces ........................................................524 ......................................................524D6710 Crown-indirectresinbasedcomposite ........................................................350 ......................................................445D6720/21/22 Crown-resinwithmetal ...............................................................................350 ......................................................495D6740 Crown-porcelain/ceramic ............................................................................350 ......................................................560D6750/51/52 Crown-porcelainfusedtometal ..................................................................350 ......................................................523D6780/81/82 Crown-3/4castmetal ..................................................................................470 ......................................................470D6783 Crown-3/4porc./ceramic ............................................................................. 511 ...................................................... 511D6790-94 Crown-fullcastmetal ..................................................................................350 ......................................................495D6930 Recementfixedpartialdenture ......................................................................69 ........................................................69D6980 Fixedpartialdenturerepair,byreport ...........................................................172 ......................................................172
ADJUNCTIVE GENERAL SERVICESD9110 Palliative(emergency)treatmentofdentalpain .............................................43 ........................................................43D9210/15 Localanesthesia .............................................................................................0 ..........................................................0D9211/12 Regionalblockanesthesia ..............................................................................0 ..........................................................0D9223 Deepsedation/generalanesthesia-each15min.increment.................................103 ......................................................103D9230 Analgesia,anxiolysis,inhalationofnitrousoxide ...........................................37 ........................................................37D9243 Intravenousconscioussedation/analgesia-each15min.increment.. .........103 ......................................................103D9248 Non-intravenousconscioussedation ............................................................145 ......................................................145D9310 Consultation(diagnosticservicebynontreatingdentist) ..................................43 ........................................................43D9420 Hospitalcall ...................................................................................................350 ......................................................350D9440 Officevisitafterregularlyscheduledhours ....................................................90 ........................................................90D9610 Therapeuticparenteraldrug,singleadmin. ...................................................26 ........................................................26D9612 Therapeuticparenteraldrug,2ormoreadmin.,diff.med. .................................70 ........................................................70D9630 Drugsormedicamentsdispensedintheofficeforhomeuse ........................42 ........................................................42D9910 Applicationofdesensitizingmedicament .......................................................31 ........................................................31D9920 Behaviormanagement,byreport ...................................................................68 ........................................................68D9930 Treatmentofcomplications(post-surgical) ....................................................43 ........................................................43D9940 Occlusalguard,byreport(forgrindingandclenchingofteeth) ....................272 ......................................................272D9950 Occlusionanalysis-mountedcase ..............................................................104 ......................................................104D9951 Occlusaladjustment-limited .........................................................................66 ........................................................66D9952 Occlusaladjustment-complete ....................................................................266 ......................................................266D9986 Missedappointment .......................................................................................50 ........................................................50 D9995 Teledentistry–synchronous;real-timeencounter(whenavailable) ..............20 ........................................................20 D9996 Teledentistry–asynchronous;informationstoredandforwardedto dentistforsubsequentreview(whenavailable) ........................................20 ........................................................20 ENDODONTICS1 D3220 Therapeuticpulpotomy(excl.finalrestor.) .....................................................81 ........................................................81D3221 Pulpaldebridement,prim.andperm.teeth ....................................................94 ........................................................94D3230 Pulpaltherapy-resorbablefilling,anterior ...................................................160 ......................................................160D3240 Pulpaltherapy-resorbablefilling,posterior ..................................................164 ......................................................164D3310 Endodontictherapy,anteriortooth ................................................................341 ......................................................341D3320 Endodontictherapy,bicuspidtooth ...............................................................350 ......................................................418D3330 Endodontictherapy,molar ............................................................................350 ......................................................512D3333 Internalrootrepairofperforationdefects ......................................................105 ......................................................105D3346 Retreatofprev.rootcanaltherapy,anterior ..................................................350 ......................................................387D3347 Retreatofprev.rootcanaltherapy,bicuspid .................................................350 ......................................................465D3348 Retreatofprev.rootcanaltherapy,molar .....................................................350 ......................................................558D3351 Apexification/recalcification-initialvisit ........................................................202 ......................................................202D3352 Apexification/recalcification-interimmed.repl. ............................................350 ......................................................589D3353 Apexification/recalcification-finalvisit ..........................................................350 ......................................................449D3355 Pulpalregeneration-initialvisit ....................................................................202 ......................................................202D3356 Pulpalregeneration-interimmedication ......................................................589 ......................................................589D3357 Pulpalregeneration-completionoftreatment ..............................................449 ......................................................449D3410 Apicoectomy-anterior ..................................................................................323 ......................................................323D3421 Apicoectomy-bicuspid(firstroot) .................................................................350 ......................................................364D3425 Apicoectomy-molar(firstroot) .....................................................................350 ......................................................418D3426 Apicoectomy-(eachadd.root) .....................................................................152 ......................................................152D3427 Periradicularsurgeryw/oapicoectomy .........................................................266 ......................................................266D3428 Bonegraftinconj.w/periradicularsurg.,pertooth,singlesite .......................743 ......................................................743D3429 Bonegraftinconj.w/periradicularsurg.,add.contiguoustooth,samesite .582 ......................................................582D3430 Retrogradefilling-perroot ........................................................................... 119 ...................................................... 119D3450 Rootamputation-perroot ............................................................................234 ......................................................234D3920 Hemisection,notinc.rootcanaltherapy .......................................................234 ......................................................234D3950 Canalprep/fittingofpreformeddowelorpost ...............................................136 ......................................................136
PERIODONTICS1 D0180 Comp.periodontaleval-neworestablishedpatient ......................................0 ..........................................................0D4210 Gingivectomyorgingivoplasty->3cont.teeth,perquad. .................................279 ......................................................279D4211 Gingivectomyorgingivoplasty-<=3teeth,perquad. ...................................100 ......................................................100D4240 Gingivalflapproc.,inc.rootplaning->3cont.teeth,perquad.....................345 ......................................................345D4241 Gingivalflapproc,inc.rootplaning-<=3cont.teeth,perquad ...................106 ......................................................106D4249 Clinicalcrownlengthening-hardtissue .......................................................350 ......................................................576D4260 Osseoussurgery->3cont.teeth,perquad..................................................350 ......................................................499D4261 Osseoussurgery-<=3cont.teeth,perquad ...............................................350 ......................................................392D4263 Bonereplacementgraft,firstsiteinquad. ....................................................350 ......................................................743D4264 Bonereplacementgraft,eachadd.siteinquad. ..........................................350 ......................................................582D4268 Surgicalrevisionproc.,pertooth ..................................................................358 ......................................................358D4270 Pediclesofttissuegraftprocedure ................................................................350 ......................................................643D4273 Subepithelialconnectivetissuegraftproc. ....................................................350 ......................................................800D4274 Mesial/distalwedgeprocedure,singletooth .................................................308 ......................................................308D4277 Freesofttissuegraft,pertooth .....................................................................350 ......................................................654
ADA MEMBER ACTUAL CODE BENEFIT COPAYMENT(S) COPAYMENT(S)

1 Specialty care is provided at the listed copayment whether performed by a Participating General Dentist or a Participating Specialist. Referrals to a specialist must be made by a member’s Participating General Dentist. See Plan Exclusion #13.2 Phase I Treatment codes D8010 and D8050 are provided at a 15% reduction from the orthodontist’s UCR fees. See exclusion #15 and limitation #23 for additional coverage information.
OnlycurrentADACDTcodesareconsideredvalidbyDominionNational.Current Dental Terminology © American Dental Association.
D4278 Freesofttissuegraft,eachadd.tooth ..........................................................100 ......................................................100D4320 Provisionalsplinting-intracoronal ................................................................350 ......................................................427D4321 Provisionalsplinting-extracoronal ...............................................................350 ......................................................377D4341 Perioscalingandrootplaning->3contteeth,perquad. ...................................109 ......................................................109D4342 Perioscalingandrootplaning-<=3teeth,perquad ....................................63 ........................................................63D4346 Scalinginpresenceofgeneralizedmoderateorseveregingival inflammation-fullmouth,afteroralevaluation .........................................45 ........................................................45 D4355 Fullmouthdebridement .................................................................................89 ........................................................89D4381 Localizeddeliveryofchemotherapeuticagents .............................................98 ........................................................98D4910 Periodontalmaintenance ...............................................................................74 ........................................................74
ORAL SURGERY1
D7111 Extraction,coronalremnants-deciduoustooth .............................................56 ........................................................56D7140 Extraction,eruptedtoothorexposedroot ......................................................69 ........................................................69D7210 Extraction,eruptedtoothreq.bonecut .........................................................133 ......................................................133D7220 Removalofimpactedtooth-softtissue ........................................................151 ......................................................151D7230 Removalofimpactedtooth-partiallybony ...................................................196 ......................................................196D7240 Removalofimpactedtooth-completelybony ..............................................241 ......................................................241D7241 Removalofimp.tooth-completelybony,withunusualsurg.complications 217 ......................................................217D7250 Removalofresidualtoothroots ....................................................................141 ......................................................141D7251 Coronectomy-intentionalpartialtoothremoval .............................................217 ......................................................217 D7260 Oroantralfistulaclosure ................................................................................350 ......................................................578D7261 Primaryclosureofasinusperforation ..........................................................350 ......................................................465D7270 Toothreimplant./stabiliz.ofacc.evulsed/displacedtooth.....................................226 ......................................................226D7280 Exposureofanuneruptedtooth ....................................................................153 ......................................................153D7282 Mobil.oferupted/malpositionedtoothtoaideruption ...................................231 ......................................................231D7283 Place.ofdevicetofacilitateerupt.ofimpactedtooth ....................................144 ......................................................144D7285 Biopsyoforaltissue-hard(bone,tooth) ......................................................350 ......................................................387D7286 Biopsyoforaltissue-soft(allothers) ...........................................................295 ......................................................295D7288 Brushbiopsy-transepithelialsamplecollect .................................................93 ........................................................93D7291 Transseptalfiberotomy/supracrestalfiberotomy,byreport ...........................60 ........................................................60D7310/20 Alveoloplasty,perquadrant ...........................................................................141 ......................................................141D7311/21 Alveoloplastyinconj.With/outextractions ....................................................141 ......................................................141D7450 Removalofbenignodoncyst/tumor-diam<=1.25cm .................................350 ......................................................354D7451 Removalofbenignodoncyst/tumor-diam>1.25cm....................................350 ......................................................543D7471 Removaloflateralexostosis .........................................................................350 ......................................................351D7472/73 Removaloftoruspalatinus/mandibularis ......................................................350 ......................................................480D7485 Surgicalreductionofosseoustuberosity ......................................................568 ......................................................568D7510 Incisionanddrainageofabscess-intraoralsofttissue .................................96 ........................................................96D7511 Incision/drainageofabscess-intra.softtissue,comp. ................................ 112 ...................................................... 112D7880 OcclusalorthoticdeviceforTMJ,“byreport” ................................................272 ......................................................272D7960 Frenulectomy(frenectomy/frenotomy)-separateproc. .......................................263 ......................................................263D7963 Frenuloplasty ................................................................................................293 ......................................................293D7970 Excisionofhyperplastictissue-perarch ......................................................233 ......................................................233D7971 Excisionofpericoronalgingiva .....................................................................131 ......................................................131D7972 Surgicalreductionoffibroustuberosity .........................................................521 ......................................................521
ORTHODONTICS2 - PRE-AUTHORIZATION REQUIREDD8020 Limitedortho.treatmentofthetransitionaldentition .......................................350 .....................................................3304D8030 Lim.orthotreatment-adolescentdentition ...................................................350 .....................................................3422D8040 Lim.orthotreatment-adultdentition ...........................................................3658 ....................................................3658D8070 Comp.ortho.treatment-transitionaldentition .............................................3304 ....................................................3304D8080 Comp.ortho.treatment-adolescentdentition ..............................................350 .....................................................3422D8090 Comp.ortho.treatment-adultdentition ......................................................3658 ....................................................3658D8210 Removableappliancetherapy(includingappliancesforthumbsucking andtonguethrusting) ...............................................................................350 ......................................................770D8220 Fixedappliancetherapy(includingappliancesforthumbsucking andtonguethrusting) ...............................................................................350 ......................................................783D8660 Pre-orthodontictreatmentvisit ......................................................................350 ......................................................413D8670 Periodicortho.treatmentvisit(aspartofcontract) .......................................118 ......................................................118D8680 Orthodonticret.(rem.ofappl./placementofretainer(s)) ......................................413 ......................................................413D8692 Replacementoflostorbrokenretainer .........................................................179 ......................................................179D8694 Repairoffixedretainers,includesreattachment ...........................................174 ......................................................174D8999 Unspecifiedorthodonticprocedure,byreport .................................................0 ..........................................................0
ADA MEMBER ACTUAL CODE BENEFIT COPAYMENT(S) COPAYMENT(S)

Exclusions & LimitationsPlan Exclusions1. Serviceswhicharecoveredunderworker’scompensationoremployer’sliabilitylaws.2. Serviceswhicharenotnecessaryforthepatient’sdentalhealthasdeterminedbythePlan.3. Cosmetic,electiveoraestheticdentistryexceptasrequiredduetoaccidentalbodilyinjurytosoundnaturalteethasdeterminedbythe Plan.4. Oralsurgeryrequiringthesettingoffracturesordislocations.5. Serviceswithrespecttomalignancies,cystsorneoplasms,hereditary,congenital,mandibularprognathismordevelopmentmalformations where,intheopinionofthePlan,suchservicesshouldnotbeperformedinadentaloffice.6. Dispensingofdrugs.7. Hospitalizationforanydentalprocedure.8. Treatmentrequiredforconditionsresultingfrommajordisaster,epidemic,war,actsofwar,whetherdeclaredorundeclared,orwhileon activedutyasamemberofthearmedforcesofanynation.9. Replacementduetolossortheftofprostheticappliance.10. ProceduresnotlistedascoveredbenefitsunderthisPlan.11. ServicesobtainedoutsideofthedentalofficeinwhichenrolledandthatarenotpreauthorizedbysuchofficeorthePlan(withtheexception ofout-of-areaemergencydentalservices).12. ServicesrelatedtothetreatmentofTMD(TemporomandibularDisorder)exceptifTMDiscausedbysevere,dysfunctional,handicapping malocclusionthatrequiresmedicallynecessaryorthodontiaservices.13. ServicesperformedbyaParticipatingSpecialistwithoutareferralfromaParticipatingGeneralDentist(withtheexceptionofOrthodontics andpalliativeemergencypaintreatment).ParticipatingdentistsshouldrefertoSpecialtyCareReferralGuidelines.14. Electivesurgeryincluding,butnotlimitedto,extractionofnon-pathologic,asymptomaticimpactedteethasdeterminedbythePlan.The prophylacticremovaloftheseteethformedicallynecessaryorthodontiaservicesmaybecoveredsubjecttoreview.15. Non-medicallynecessaryorthodontiaandPhaseITreatmentcodesD8010andD8050formedicallynecessaryorthodontiaarenot coveredbenefitsunderthispolicy.DiscountsareprovidedtomembersthroughthePlan’sagreementswithitsparticipatingorthodontists. TheprovideragreementscreatenoliabilityforpaymentbythePlan,andpaymentsbythememberfortheseservicesdonotcontribute totheOut-of-PocketMaximum.TheInvisalignsystemandsimilarspecializedbracesarenotacoveredbenefit.Seelimitation#23 concerningmedicallynecessaryorthodontia.
Plan Limitations1. One(1)evaluation(D0120,D0145orD0150)persix(6)months,perpatient.2. One(1)teethcleaning(D1110orD1120)persix(6)months,perpatient.3. One(1)fluoridetreatmentiscoveredpersix(6)months,perpatient.4. One(1)sealantpertooth,perlifetime,perpatient(limitedtoocclusalsurfacesofposteriorpermanentteethwithoutrestorationsordecay).5. One(1)spacemaintainer(D1510,D1520,D1515orD1525)iscoveredper12months,perquadrant(unilateral)orperarch(bilateral),per patient;one(1)distalshoespacemaintainer(D1575),fixed,unilateralper24months.6. Replacementofafillingiscoveredifitismorethan12monthsfromthedateoforiginalplacement.7. Replacementofacrown,dentureorlabialveneeriscoveredifitismorethanfive(5)yearsfromthedateoforiginalplacement.8. Replacementofaprimarystainlesssteelcrowniscoveredifitismorethanthree(3)yearsfromthedateoforiginalplacement,pertooth, perpatient.9. Crownandbridgefeesapplytotreatmentinvolvingfiveorfewerunitswhenpresentedinasingletreatmentplan.Additionalcrownor bridgeunits,beginningwiththesixthunit,areavailableattheprovider’sUsual,Customary,andReasonable(UCR)fee,minus25%.10. Reliningandrebasingofdenturesiscoveredonceper24months,perpatient,onlyaftersix(6)monthsofinitialplacement.11. Rootcanaltreatmentiscoveredoncepertooth,perlifetime,perpatient.Retreatmentofpreviousrootcanaltherapyiscoveredonceper tooth,perlifetime,perpatient.12. Periodontalscalingandrootplaning(D4341orD4342),osseoussurgery(D4260orD4261)andgingivectomyorgingivoplasy(D4210or D4211)arelimitedtoone(1)per24months,perquadrant,perpatient.13. Scalinginpresenceofgeneralizedmoderateorseveregingivalinflammation-fullmouth,afteroralevaluationandinlieuofacovered D1110,limitedtooncepertwoyears.14. Fullmouthdebridementiscoveredonceper12months,perpatient.15. ProcedureCodeD4381islimitedtoone(1)benefitpertoothforthree(3)teethperquadrant;oratotalof12teethforallfour(4)quadrants pertwelve(12)months,perpatient.Musthavepocketdepthsoffive(5)millimetersorgreater.16. Periodontalsurgeryofanytype,includinganyassociatedmaterial,iscoveredonceevery24months,perquadrantorsurgicalsite,per patient.17. Periodontalmaintenanceafteractivetherapyiscoveredfour(4)timesper12months,perpatient.18. Coronectomy,intentionalpartialtoothremoval,one(1)perlifetime. 19. Alldentalservicesthataretoberenderedinahospitalsettingrequirecoordinationandapprovalfromboththedentalinsurerandthe medicalinsurerbeforeservicescanberendered.Servicesdeliveredtothepatientonthedateofservicearedocumentedseparatelyusing applicableprocedurecodes.20. Anesthesiarequiresanarrativeofmedicalnecessitybemaintainedinpatientrecords.Amaximumof60minutesofservicesareallowed forgeneralanesthesiaandintravenousornon-intravenousconscioussedation.Theroutineadministrationofinhalationanalgesiaororal sedationisgenerallyconsideredpartofthetreatmentprocedure,unlessitsuseisdocumentedinthepatientrecordasnecessaryto completetreatment.21. Occlusalguard,byreport(forgrindingandclenchingofteeth).22. Apexification,apicoectomyandclinicalcrownlengtheningareeachcoveredoncepertooth,perprovider,perlifetime.23. OrthodonticsisonlycoveredifmedicallynecessaryasdeterminedbythePlan.Patientcopaymentswillapplytotheroutineorthodontic applianceportionofservicesonly.Additionalcostsincurredwillbecomethepatient’sresponsibility. 24. Teledentistry,synchronous(D9995)orasynchronous(D9996),limitedtotwopercalendaryear(whenavailable).