selenium and thyroid more good news - jeffrey dach md
DESCRIPTION
Thyroid seleniumTRANSCRIPT
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 1/19
Jeffrey Dach MDBioidentical Hormones and Natural Thyroid
Selenium and Thyroid More Good NewsPosted on January 1, 2014
Selenium and the Thyroid, More Good Newsfrom Mainstream Medicine
by Jeffrey Dach MD
A Feb 2013 article in Clinical Endocrinologydeclares “More Good News!!” on Selenium and theThyroid.(1) They go on to state,
“In patients with Hashimoto’s disease and inpregnant women with antiTPO antibodies, seleniumsupplementation decreases antithyroid antibody
levels and improves the ultrasound structure of the thyroid gland.“(1)
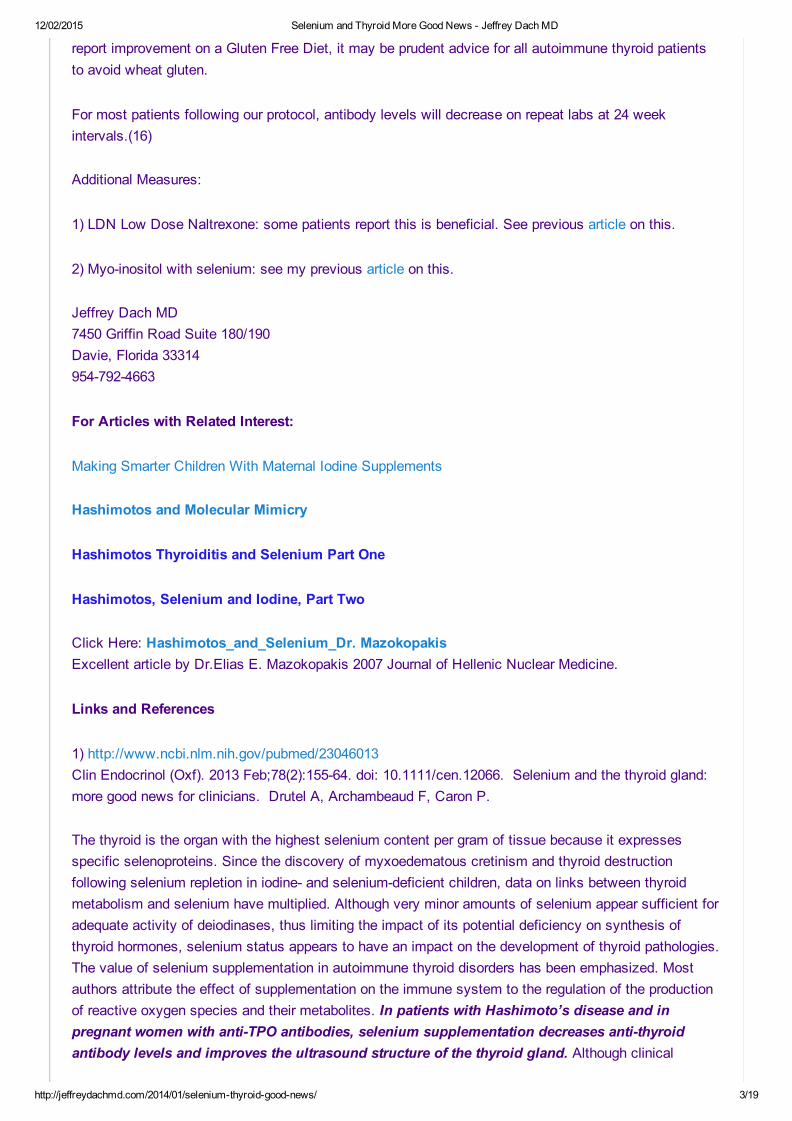
Selenium Deficient Soil Map of US
Regular readers of my blog will know that I havebeen writing for years about the benefits ofselenium in Hashimoto’s thyroiditis. I even haveseveral chapters devoted to selenium in my book,Bioidentical Hormones 101, published 3 yearsago. It is nice to know that mainstreamendocrinology is finally catching up to what wehave been doing in the office for many years now.
We live in a selenium deficient area (see above leftmap). Our office routine is to test everyone for selenium level and give selenium supplements whenfound low.
The Iodine in Hashimoto’s Controversy
Iodine supplementation in Hashimoto’s Autoimmune Thyroiditis patients is controversial, and manypatients read on the internet that Iodine should never be given to a Hashimoto’s patient, because it mayworsen the inflammation and cause thyroid storm..
However, Iodine is an essential mineral, and iodine deficiency, called IDD (Iodine Deficiency Disorder) is

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 2/19
associated with adverse health outcomes.(21,22) Maternal iodine deficiency can lead toneurodevelopment delay in the baby.
Left image Iodine in flask courtesy of wikimedia
Starting Selenium First Before IodineSupplementation!
Many Hashimotos patients have normal iodine levelson testing. However, for the iodine deficient patient,we would like to devise a protocol to provide iodinesupplementation safely without aggravating theinflammatory thyroid disease. This can be done withan initial period of selenium supplementation whichprotects the thyroid cells from oxidative damage fromhydrogen peroxide used to incorporate Iodine into
thyroid hormone. After two to four weeks of selenium supplementation, it is then safe to start low doseiodine in the range of 225 mcg per day..
For Hashimoto’s patients who test low for Iodine, our protocol starts off with selenium supplementationof 200400 mcg per day for two to four weeks, after which, low dose Iodine (225 mcg per day ) isstarted. A number of studies have shown that this dosage of Iodine causes no harm in AutoImmuneThyroiditis patients. (3)(9)(13)
How to Reduce Antibody Levels in Hashimoto’s
The three most useful interventions for reducing antibody levels in the Hashimoto’s patient are:
1) Selenium supplementation as discussed above.2) TSH suppression with thyroid medication.(2,3,17,18) Conventional endocrinologists use Synthroid(levothyroxine) with a treatment goal of TSH in the lower half of the normal range. In our treatmentprotocol, we use natural dessicated thyroid (NDT), also called NatureThroid), and our goal is tosuppress the TSH below the normal range.
The use of suppressive doses of thyroid medication has been reported in the medical literature asextremely beneficial in reducing antibody levels. (2,3,17,18) We have found this true in clinical practiceas well.
3) Gluten Sensitivity Testing and Gluten Free Diet
In a Dutch study of 104 patients with Hashimoto’s thyroiditis , sixteen (15%) were positive for antigliadinantibodies and gluten sensitivity.(19) The authors recommended routine testing of all HAshimotosthyroiditis patients for gluten reactivity. We have done this and our clinical experience is in agreement.
Another study yielded a 5.5% positive test rate for autoimmune thyroid patients when tested for antigliadin antibodies.(20) The actual rate may be much higher when more sophisticated testing methodsare used. In addition, in some cases, testing may yield false negative results. Since many patients
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 3/19
report improvement on a Gluten Free Diet, it may be prudent advice for all autoimmune thyroid patientsto avoid wheat gluten.
For most patients following our protocol, antibody levels will decrease on repeat labs at 24 weekintervals.(16)
Additional Measures:
1) LDN Low Dose Naltrexone: some patients report this is beneficial. See previous article on this.
2) Myoinositol with selenium: see my previous article on this.
Jeffrey Dach MD7450 Griffin Road Suite 180/190Davie, Florida 333149547924663
For Articles with Related Interest:
Making Smarter Children With Maternal Iodine Supplements
Hashimotos and Molecular Mimicry
Hashimotos Thyroiditis and Selenium Part One
Hashimotos, Selenium and Iodine, Part Two
Click Here: Hashimotos_and_Selenium_Dr. MazokopakisExcellent article by Dr.Elias E. Mazokopakis 2007 Journal of Hellenic Nuclear Medicine.
Links and References
1) http://www.ncbi.nlm.nih.gov/pubmed/23046013Clin Endocrinol (Oxf). 2013 Feb;78(2):15564. doi: 10.1111/cen.12066. Selenium and the thyroid gland:more good news for clinicians. Drutel A, Archambeaud F, Caron P.
The thyroid is the organ with the highest selenium content per gram of tissue because it expressesspecific selenoproteins. Since the discovery of myxoedematous cretinism and thyroid destructionfollowing selenium repletion in iodine and seleniumdeficient children, data on links between thyroidmetabolism and selenium have multiplied. Although very minor amounts of selenium appear sufficient foradequate activity of deiodinases, thus limiting the impact of its potential deficiency on synthesis ofthyroid hormones, selenium status appears to have an impact on the development of thyroid pathologies.The value of selenium supplementation in autoimmune thyroid disorders has been emphasized. Mostauthors attribute the effect of supplementation on the immune system to the regulation of the productionof reactive oxygen species and their metabolites. In patients with Hashimoto’s disease and inpregnant women with antiTPO antibodies, selenium supplementation decreases antithyroidantibody levels and improves the ultrasound structure of the thyroid gland. Although clinical

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 4/19
applications still need to be defined for Hashimoto’s disease, they are very interesting for pregnantwomen given that supplementation significantly decreases the percentage of postpartum thyroiditis anddefinitive hypothyroidism. In Graves’ disease, selenium supplementation results in euthyroidism beingachieved more rapidly and appears to have a beneficial effect on mild inflammatory orbitopathy. A risk ofdiabetes has been reported following longterm selenium supplementation, but few data are available onthe side effects associated with such supplementation and further studies are required.
2) http://www.ncbi.nlm.nih.gov/pubmed/21508145J Clin Endocrinol Metab. 2011 Jul;96(7):220615. doi: 10.1210/jc.20102986. Epub 2011 Apr 20. Theeffect of levothyroxine and selenomethionine on lymphocyte and monocyte cytokine release in womenwith Hashimoto’s thyroiditis.Krysiak R, Okopien B. Department of Internal Medicine and Clinical Pharmacology, Medical Universityof Silesia, Medyków 18, PL 40752 Katowice, Poland.
No previous study determined monocyte and lymphocytesuppressing effects of levothyroxine andselenomethionine and assessed whether their coadministration is superior to treatment with only one ofthese drugs.OBJECTIVE:
Our objective was to compare the effect of levothyroxine and selenomethionine on monocyte andlymphocyte cytokine release and systemic inflammation in patients with Hashimoto’s thyroiditis.DESIGN, SETTING, PARTICIPANTS, AND INTERVENTION:
We conducted a randomized clinical trial involving a group of 170 ambulatory euthyroid women withrecently diagnosed and previously untreated Hashimoto’s thyroiditis and 41 matched healthy subjects.Participants were randomized in a doubleblind fashion to receive a 6month treatment withlevothyroxine, selenomethionine, levothyroxine plus selenomethionine, or placebo. One hundred sixtyfive patients completed the study.MAIN OUTCOME MEASURES:
Monocyte and lymphocyte release of proinflammatory cytokines and plasma levels of Creactive protein(CRP) were assessed.RESULTS:
Compared with the control subjects, monocytes and lymphocytes of Hashimoto’s thyroiditis patientsreleased greater amounts of all cytokines studied. Levothyroxine reduced monocyte release of TNFα,IL1β, IL6, and monocyte chemoattractant protein1, whereas selenomethionine inhibited lymphocyterelease of IL2, interferonγ, and TNFα, which was accompanied by a reduction in plasma CRP levels.The decrease in cytokine release and in plasma CRP levels was strongest when both drugs were giventogether.CONCLUSIONS: Despite affecting different types of inflammatory cells, levothyroxine andselenomethionine exhibit a similar systemic antiinflammatory effect in euthyroid females withHashimoto’s thyroiditis. This action, which correlates with a reduction in thyroid peroxidaseantibody titers, may be associated with clinical benefits in the prevention and management ofHashimoto’s thyroiditis, particularly in subjects receiving both agents.
3) http://www.ncbi.nlm.nih.gov/pubmed/10488481Nuklearmedizin. 1999;38(5):1449.
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 5/19
[Effect of iodine and thyroid hormones in the induction and therapy of Hashimoto’s thyroiditis]. [Article inGerman] Rink T, Schroth HJ, Holle LH, Garth H.
The effect of an iodine prophylaxis on the induction of Hashimoto’s thyroiditis as well as the influence ofvarious therapeutic approaches on the course of antithyroglobulin (TgAb) and antiperoxidase (TPOAb)antibodies in manifest diseases are evaluated. METHOD: A collective of 375 euthyroid subjectswithout relevant goiter received daily doses of 200 micrograms iodide, weekly doses of 1.53 milligramsiodide, or no medication. A second group of 377 patients suffering from Hashimoto’s thyroiditis wastreated with a nonsuppressive hormone medication, a suppressive hormone administration, acombination of a nonsuppressive hormone therapy with low dose iodide (50150 micrograms/day), mereiodide in doses of 200 micrograms/day, or received no therapy. The mean observation period in thesetwo groups was 860 and 848 days, respectively.RESULTS:
There was no significant increase of the antibody levels in the subgroup with 200 micrograms iodide/dayand in the nontreated subjects of the first collective. However, the group that received 1.53 milligramsiodide/week presented a distinct increase of the TgAb as well as the TPOAb, and the incidence ofHashimoto’s thyroiditis was 4fold higher than in the two other subgroups. The patients of the secondcollective revealed a significant decrease of the TgAb in the subgroups treated with up to 200micrograms iodide/day, while the reduction of the TPOAb depended on the thyrotropin level and wasmost significant in the suppressed group (p < 0.0001).CONCLUSION: To lower the incidence of autoimmune thyroid diseases in predisposed subjects, a dailyiodine supplementation seems to be superior to highdose weekly administrations. A hormone therapycombined with a daily, lowdose iodine medication is able to reduce the TgAb and the TPOAb levelseven in patients with Hashimoto’s thyroiditis.
The patients of the second collective revealed a significant decrease of the TgAb in the subgroupstreated with up to 200 micrograms iodide/day, while the reduction of the TPOAb depended on thethyrotropin level and was most significant in the suppressed group (p < 0.0001)
3a) http://www.ncbi.nlm.nih.gov/pubmed/18631004Thyroid. 2008 Jul;18(7):75560.Longterm followup of antithyroid peroxidase antibodies in patients with chronic autoimmune thyroiditis(Hashimoto’s thyroiditis) treated with levothyroxine.Schmidt M, Voell M, Rahlff I, Dietlein M, Kobe C,Faust M, Schicha H.
A number of studies show that the serum levels of antithyroid peroxidase antibodies (TPOAb) in patientswith Hashimoto’s thyroiditis decline during levothyroxine treatment, but do not provide quantitative dataor report the fraction of patients in whom test for TPOAb became negative (“normalization percentage”).The objective of the present study was to provide this information.METHODS:
This was a retrospective study of TPOAb concentrations in 36 women and 2 men (mean age 51 +/ 16years; range 1981 years) with Hashimoto’s thyroiditis as defined by the following criteria: elevatedplasma TPOAb and typical hypoechogenicity of the thyroid in highresolution sonography at firstpresentation or during followup and low pertechnetate uptake in thyroid scintigraphy. When first studied17 women and 1 man were not yet taking levothyroxine. The remaining 20 patients were receivinglevothyroxine. At initial examination 18 patients had serum thyroidstimulating hormone (TSH)
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 6/19
concentrations above normal. Results of up to eight (mean = 5.8) measurements obtained over a meanperiod of 50 months while patients were receiving levothyroxine were analyzed. In addition, serum TSH,free triiodothyronine (fT3), and free thyroxine (fT4) were measured, and ultrasound of the neck wasperformed at each followup examination.RESULTS:
In terms of TPOAb levels, 35 of 38 patients (92%) had a decrease, 2 patients had undulating levels, and1 patient had an inverse hyperbolic increase in her TPOAb levels. In the 35 patients in whom there weredecreasing TPOAb values, the mean of the first value was 4779 IU/mL with an SD of 4099 IU/mL. Themean decrease after 3 months was 8%, and after 1 year it was 45%. Five years after the first value,TPOAb levels were 1456 +/ 1219 IU/mL, a decrease of 70%. TPOAb levels became negative, < 100IU/mL, in only six patients, a normalization percentage of 16%. There were no correlations betweenchanges in thyroid volume and changes in TPOAb.CONCLUSION: Serum TPOAb levels decline in most patients with Hashimoto’s thyroiditis who aretaking levothyroxine, but after a mean of 50 months, TPOAb became negative in only a minority ofpatients.
———————————–
4) http://www.ncbi.nlm.nih.gov/pubmed/10395237https://www.jstage.jst.go.jp/article/endocrj1993/45/6/45_6_797/_articleEndocr J. 1998 Dec;45(6):797803.Urinary iodine and thyroid antibodies in Okinawa, Yamagata, Hyogo, and Nagano, Japan: thedifferences in iodine intake do not affect thyroid antibody positivity.Nagata K, Takasu N, Akamine H, Ohshiro C, Komiya I, Murakami K, Suzawa A, Nomura T.
Excess iodine intake may affect the development of Hashimoto’s thyroiditis. Kelp consumption is veryhigh in Okinawa. We expected a high prevalence of Hashimoto’s thyroiditis in Okinawa. We studiedurinary iodine excretion and the positivities of antithyroglobulin antibodies (TGAb) and antithyroidperoxidase antibodies (TPOAb) in the residents of Nishihara in Okinawa, Yamagata in Yamagata, Kobein Hyogo, and Hotaka in Nagano, Japan. TGAb and/or TPOAb were positive in 142 (13.7%) of 1039subjects in Nishihara, in 16 (16.0%) of 100 subjects in Yamagata, in 31 (13.4%) of 232 subjects in Kobe,and in 35 (13.9%) of 252 subjects in Hotaka; TGAb and/or TPOAb positivity was about the same inthese 4 areas. One tenth of the subjects with positive TGAb and/or TPOAb had hypothyroidism; thefrequencies of hypothyroidism in those with positive TGAb and/or TPOAb were about the same inNishihara, Yamagata, Kobe, and Hotaka. The iodine concentration in samples of morning urine correlatedwell with the 24h urine iodine excretion. The urinary iodine excretion was 1.5 mg/day in Nishihara. Therewere no differences between Nishihara and Yamagata in the urinary iodine concentration, but the urinaryiodine concentrations in Kobe and Hotaka were less than those in Nishihara or Yamagata. The amountsof iodine excretion in Kobe and Hotaka were moderate, and less than those in Nishihara or Yamagata.The amounts of iodine intake in Kobe and Hotaka were less than those in Nishihara or Yamagata, butTGAb and/or TPOAb positivity was about the same in Nishihara, Yamagata, Kobe, and Hotaka. Thedifferences in dietary iodine intake do not affect TGAb and/or TPOAb positivity.
5) http://www.ncbi.nlm.nih.gov/pubmed/9703374Eur J Endocrinol. 1998 Jul;139(1):238. Effect of small doses of iodine on thyroid function in patientswith Hashimoto’s thyroiditis residing in an area of mild iodine deficiency.Reinhardt W, Luster M, Rudorff KH, Heckmann C, Petrasch S, Lederbogen S, Haase R, Saller B,
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 7/19
Reiners C, Reinwein D, Mann K.
Several studies have suggested that iodine may influence thyroid hormone status, and perhaps antibodyproduction, in patients with autoimmune thyroid disease. To date, studies have been carried out usinglarge amounts of iodine. Therefore, we evaluated the effect of small doses of iodine on thyroid functionand thyroid antibody levels in euthyroid patients with Hashimoto’s thyroiditis who were living in an areaof mild dietary iodine deficiency.METHODS: Forty patients who tested positive for antithyroid (TPO) antibodies or with a moderate tosevere hypoechogenic pattern on ultrasound received 250 microg potassium iodide daily for 4 months(range 213 months). An additional 43 patients positive for TPO antibodies or with hypoechogenicity onultrasound served as a control group. All patients were TBII negative.RESULTS:
Seven patients in the iodinetreated group developed subclinical hypothyroidism and one patient becamehypothyroid. Three of the seven who were subclinically hypothyroid became euthyroid again when iodinetreatment was stopped. One patient developed hyperthyroidism with a concomitant increase in TBII titreto 17 U/l, but after iodine withdrawal this patient became euthyroid again. Only one patient in the controlgroup developed subclinical hypothyroidism during the same time period. All nine patients who developedthyroid dysfunction had reduced echogenicity on ultrasound. Four of the eight patients who developedsubclinical hypothyroidism had TSH concentrations greater than 3 mU/l. In 32 patients in the iodinetreated group and 42 in the control group, no significant changes in thyroid function, antibody titres orthyroid volume were observed.
CONCLUSIONS: Small amounts of supplementary iodine (250 microg) cause slight butsignificant changes in thyroid hormone function in predisposed individuals.
My comment : predisposed ? by what —?selenium deficiency ??
—————————–
6) http://www.ncbi.nlm.nih.gov/pubmed/12699595
Thyroid. 2003 Feb;13(2):199203.Introduction of iodized salt to severely iodinedeficient children does not provoke thyroidautoimmunity: a oneyear prospective trial in northern Morocco. Zimmermann MB, Moretti D, ChaoukiN, Torresani T.
To determine if introduction of iodized salt induces thyroid autoimmunity in goitrous children, weconducted a prospective trial in iodinedeficient Moroccan schoolchildren (n = 323). Local salt wasiodized at 25 microg iodine per gram of salt and distributed to households. Before introduction of iodizedsalt and at 10, 20, 40, and 52 weeks, we measured antithyroid peroxidase antibodies (TPOAb),antithyroglobulin antibodies (TgAb), urinary iodine (UI), and thyroid hormones, and examined the thyroidusing ultrasound. At baseline, median UI was 17 microg/L and the prevalence of goiter andhypothyroidism was 72% and 18%, respectively. Provision of iodized salt maintained median UI at 150200 microg/L for the year (p < 0.0001). There was a significant increase in mean total thyroxine (T(4))and a significant reduction in the prevalence of hypothyroidism (p < 0.001). There was a transientincrease in the prevalence of detectable antibodies after introduction of iodized salt (p < 0.0001) withlevels returning to baseline at 1 year. Only congruent with 1% of children had elevated TPOAb and none
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 8/19
had elevated TgAb over the course of the study, and no child with elevated TPOAb had abnormalthyrotropin (TSH) or T(4) concentrations. None developed clinical or ultrasonographic evidence of thyroidautoimmune disease and/or iodineinduced hypothyroidism or hyperthyroidism. Rapid introduction ofiodized salt does not provoke significant thyroid autoimmunity in severely iodinedeficient childrenfollowed for 1 year.
———————————————
?selenium status ????
7) http://www.ncbi.nlm.nih.gov/pubmed/9758438Eur J Endocrinol. 1998 Sep;139(3):2907.Iodide induces thyroid autoimmunity in patients with endemic goitre: a randomised, doubleblind, placebocontrolled trial.Kahaly GJ, Dienes HP, Beyer J, Hommel G.
Iodine is essential for normal thyroid function and the majority of individuals tolerate a wide range ofdietary levels. However, a subset of individuals, on exposure to iodine, develop thyroid dysfunction. Inthis doubleblind trial, we evaluated the efficacy and tolerability of lowdose iodine compared with thoseof levothyroxine (T4) in patients with endemic goitre.METHODS:
Sixtytwo patients were assigned randomly to groups to receive iodine (0.5 mg/day) or T4 (0.125 mg/day)for 6 months. Subsequently, both groups were subject to placebo for another 6 months. Thyroidsonography, determination of thyroidrelated hormones and antibodies, and urinary excretion of iodinewere carried out at baseline and at 1, 6 and 12 months.RESULTS:
At 6 months, markedly increased urinary values of iodine were found in patients receiving iodine (36microg/24 h at baseline, 415 microg/24 h at 6 months) compared with those receiving T4 (47 microg/ 24h at baseline, 165 microg/24 h at 6 months; P < 0.0001 compared with iodine group). T4 administrationengendered a greater (P < 0.01) decrease in thyroid volume (from 32 ml to 17 ml, P < 0.0001) than didintake of iodine (3 3 ml to 21 ml. P < 0.005). High microsomal and thyroglobulin autoantibody titres werepresent in six of 31 patients (19%) receiving iodine, and iodineinduced hypo and hyperthyroidismdeveloped in four and two of them, respectively. Fineneedle biopsy revealed marked lymphocyteinfiltration in all six. After withdrawal of iodine thyroid dysfunction remitted spontaneously and antibodytitres and lymphocyte infiltration decreased markedly. Followup of these six patients for an additional 3years showed normalisation of antibody titres in four of them.CONCLUSION:
Although nearly comparable results were obtained with both treatment regimens regarding thyroid size,partly reversible iodineinduced thyroid dysfunction and autoimmunity were observed amongpatients with endemic goitre.
Selenium status not tested…???
8) http://www.ncbi.nlm.nih.gov/pubmed/10907993Thyroid. 2000 Jun;10(6):4937.

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 9/19
The effect of iodine administration on the development of thyroid autoimmunity in patients with nontoxicgoiter. Papanastasiou L, Alevizaki M, Piperingos G, Mantzos E, TseleniBalafouta S, Koutras DA.
OBJECTIVE: Previous studies, mostly performed in iodinedeficient areas, have suggested that theadministration of iodine to patients with endemic goiter may be associated with the development ofthyroid autoantibodies (ThAbs); however, this has not been a consistent finding. In this study, weevaluated the effect of iodine on thyroid function and on the development of indices of autoimmunity(ThAbs and lymphocytic infiltration) in an iodine replete area.METHODS:
Iodized oil (1 mL) was administered intramuscularly to 40 euthyroid patients with nontoxic goiter,adequate iodine intake, and absent or normal levels of ThAbs. Blood and urinary samples were taken attime 0, 3, 6, and 12 months after iodine administration. Thyroid volume was evaluated and fineneedleaspiration (FNA) was performed at 0, 6, and 12 months.RESULTS: Seven patients developed abnormal levels of ThAbs at some time between 3 and 12 monthsafter iodine administration (p = 0.017). Mean antithyroglobulin (Tg) antibody levels increased at 6 monthswithout reaching abnormal levels, but did not reach statistical significance (p = 0.062). Lymphocyticinfiltration was detected in FNA smears in 10 cases before and in 27 cases after treatment (p = 0.0003).Triiodothyronine (T3) decreased at 12 months of followup, while thyroxine (T4) and thyrotropin (TSH)levels did not change significantly. A decrease in the mean levels of thyroglobulin as well as a smallreduction in goiter size was observed at 6 and 12 months.CONCLUSION: The administration of iodized oil to patients with small nontoxic goiter in aniodinereplete area was accompanied by the development of abnormal levels of ThAbs in somecases and by an increase in thyroid lymphocytic infiltration.
In some cases ??? were these cases selenium deficient ???
———————————–
9) http://www.ncbi.nlm.nih.gov/pubmed/9011485Dtsch Med Wochenschr. 1996 Dec 20;121(5152):158791.[Therapy of endemic goiter with iodide or lthyroxine in older patients]. [Article in German] Feldkamp J,Seppel T, Mühlmeyer M, Becker A, Santen R, Schlaghecke R, Horster FA.
To compare the efficacy of iodide (300 micrograms daily) with that of levothyroxine (1.5 micrograms/kgdaily) in the treatment of endemic goitre in middleaged and elderly persons. The possible occurrence ofantibodies against thyroid peroxidase and thyroglobulin was also tested.PATIENTS AND METHODS: 67 patients (54 women, 13 men; aged over 40 years, average 53.5 years)with endemic goitre, excluding toxic goitre, were randomly treated with either iodine or thyroxine. Every 3months for one year their thyroid volume was obtained by ultrasound and the activities of thyroidhormone (TH) and thyroid stimulating hormone (TSH) and the concentration of antibodies againstperoxidase and thyroglobulin were measured.RESULTS: In patients on levothyroxine the thyroid volume had already markedly decreased after 3months (P < 0.0001), diminishing by 15.4% at 12 months. Volume reduction in the group on iodine was16.2% at one year. There was no significant difference between the two medications and no case ofantibody production in the iodine group.CONCLUSIONS: Treatment of endemic goitre with iodine alone is efficacious even in middleaged orelderly patients, toxic goitre having been excluded. There was no evidence of antibody production

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 10/19
against thyroid antigens at the stated iodine dosage.
————————————
Pharmacist advocates selenium and iodine for HAshimotos
10) http://articles.sunsentinel.com/20131206/news/flsuzycohen12081320131202_1_iodinehashimotoseleniumstatus
http://heraldreview.com/news/opinion/editorial/columnists/cohen/dearpharmacistiodineseleniumkeystohashimotos/article_62f4461c5d4011e39a06001a4bcf887a.html
Dear Pharmacist: Iodine, selenium keys to Hashimoto’s
Dear Pharmacist: I have Hashimoto thyroiditis, can I take thyroid supplements that contain iodine? —K.S., Seattle, Wash.
A: Hashimoto’s (Hashi’s) is an autoimmune condition that affects the thyroid gland, causing clinicalsymptoms of hypothyroidism. I know there’s controversy regarding iodine supplementation. I am awarethat a sudden increase in iodine can cause a bad reaction, but I don’t think Hashi sufferers should avoidiodine altogether. Iodine levels have fallen more than 50 percent during the last 40 years. During thatsame time, Hashi’s has increased at epidemic rates. Common sense will tell you iodine is not the causefor this rise in Hashimoto’s.
This next statement is huge: Hashimoto’s disease is far impacted more by your selenium status, thaniodine. If you take iodine in the presence of selenium deficiency, it’s bad news (and the same can besaid for excessive selenium). That’s the key, selenium deficiency causes an intolerance of iodine,especially high dose iodine.
When I hear of a Hashi sufferer having a bad experience with iodine, all that says to me is thatthey were selenium deficient, or they took a bad form of iodine or too high of a dose.
——————————
Mario Fujiwara on iodine AND HASHIMOTOS
11) http://perfecthealthdiet.com/2011/05/iodineandhashimotosthyroiditisparti/Iodine and Hashimoto’s Thyroiditis, Part IPosted by Paul Jaminet on May 24, 2011 Leave a comment (206) Go to commentsMario Renato Iwakura is a Brazilian engineer and Hashimoto’s thyroiditis patient who is intimatelyfamiliar with the hypothyroidism literature. the place of iodine and selenium supplementation in treatmentof hypothyroid disorders.
12) http://perfecthealthdiet.com/2011/05/iodineandhashimotosthyroiditispart2/Iodine and Hashimoto’s Thyroiditis, Part 2Posted by Paul Jaminet on May 26, 2011

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 11/19
Mario Renato Iwakura on the place of iodine and selenium supplementation in treatment ofhypothyroidism continues. This is part 2.
A few months after I was diagnosed with Hashimoto’s I started 50 mg/day iodine plus 200 mcg/dayselenium. If I were starting today, I would follow Paul’s recommendation to start with selenium and a lowdose of iodine, and increase the iodine dose slowly. I would not take any kelp, because of potentialthyrotoxic contaminants.
——————————————————13) http://www.ncbi.nlm.nih.gov/pubmed/10603730Med Klin (Munich). 1999 Nov 15;94(11):597602.[Iodine therapy for iodine deficiency goiter and autoimmune thyroiditis. A prospective study]. [Article inGerman] Meng W, Schindler A, Spieker K, Krabbe S, Behnke N, Schulze W, Blümel C. :
There is epidemiological and clinical evidence that iodine may induce or promote the manifestation ofautoimmune thyroiditis. For this reason it is important to know if substitution of alimentary iodinedeficiency or iodine treatment of endemic goitre can cause formation of thyroid antibodies. On the otherhand the practical importance of this phenomenon should be evaluated.PATIENTS AND METHODS: During a prospective study we examined 209 patients with endemicnontoxic goitre and 53 healthy people. For treatment were used 200 micrograms iodine/d (n = 119),500 micrograms iodine/d (n = 27), 1.5 mg iodine/week (n = 41), 150 micrograms iodine/d plus 75 to 100micrograms T4/d (n = 26), 100 micrograms iodine plus 100 micrograms T4/d (n = 24). The observationtook 1 year with a 3month interval for check ups including clinical examination, ultrasound, TSH, T3,fT4, TPO and thyreoglobuline antibodies and urinary iodine.RESULTS: After 12 months 7.5% of iodine treated persons had produced antibodies, most ofthem at low levels. In healthy people we found increased antibodylevels in 3.8%, in patients with goitrein 9.0%, in patients with nodular goitres in 11.1%.
500 micrograms iodine caused the most antibody reaction in 14.8%. People treated with 200micrograms iodine/d showed positive antibody levels in 5%. T4 seems to reduce antibodyreactions. Pathological antibodylevels were not found in patients with combined iodine/T4 andsingleT4 therapy. Among the 22 primary pathological antibody levels only 4 increased further (18.2%).Three of them belonged to the group of 5 persons treated with 500 micrograms iodine/d. Primary highantibody values were normalized in 5 patients (22.7%). Hypothyroid disturbances were not found.Ultrasound did not show any alterations, and the reduction of thyroid volumes in antibodypositivepatients was not affected. Median urinary iodine excretion during the observationinterval was 5.2 to 7.2micrograms/dl.CONCLUSIONS: Possible antibody reactions have no clinical importance at all. Individual cases mustbe observed. Low iodine doses should be preferred. Combined iodine/T4 treatment seems to havean advantage regarding immunological thyroidal reactions.
14) http://www.ncbi.nlm.nih.gov/pubmed/20039895Clin Endocrinol (Oxf). 2010 Oct;73(4):5359. doi: 10.1111/j.13652265.2009.03758.x.Influence of physiological dietary selenium supplementation on the natural course of autoimmunethyroiditis. Nacamulli D, Mian C, Petricca D, Lazzarotto F, Barollo S, Pozza D, Masiero S, Faggian D,Plebani M, Girelli ME, Mantero F, Betterle C.
Our study aimed to investigate whether physiological doses of selenium (Se) influence the natural course
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 12/19
of autoimmune thyroiditis (AIT). DESIGN AND PATIENTS: A total of 76 consecutive patients (65 F, 11M, median 43, range 1575 years) with AIT, normal or slightly elevated TSH and fT4 within thenormal range were divided into two groups:
Group 0 (30 cases) was given no treatment whileGroup 1 (46 cases) was treated with sodium selenite 80 μg/day as a single oral dose for 12 months.
Thyroperoxidase and thyroglobulin autoantibodies (TPOAb; TgAb), TSH, fT4 and urine iodineconcentrations (UIC) were measured at baseline and after 6 and 12 months of followup. Thyroidultrasonography (US) was performed at each followup point. Echogenicity was measured byhistographic analysis of grayscale pixels (gsp) ranging from 0 = black to 255 = white.RESULTS:
Thyroid echogenicity decreased significantly in both groups after 6 months, but after 12 months, it hadchanged no more in Group 1, whereas it had dropped further in Group 0. No significant variation in TPOAb or TgAb levels was observed between the two groups after 6 months, but both values decreasedsignificantly after 12 months in Group 1, and five patients in this group became negative for TPOAb.TSH and FT4 showed no significant variations in either group.CONCLUSIONS: Dietary supplementation with physiological doses of Se seems to be effective inpreventing a reduction in thyroid echogenicity after 6 months of treatment and in reducing TPOAb andTgAb after 12 months, but does not modify TSH or FT4.
15) http://www.ncbi.nlm.nih.gov/pubmed/23158484Zhonghua Yi Xue Za Zhi. 2012 Aug 28;92(32):225660.[Effects of selenium supplementation on antibodies of autoimmune thyroiditis].[Article in Chinese] Zhu L,Bai X, Teng WP, Shan ZY, Wang WW, Fan CL, Wang H, Zhang HM.
To evaluate the effects of selenium (Se) supplementation on concentrations of thyroid peroxidaseantibodies (TPOAb) and TPOAb IgG subclasses in autoimmune thyroiditis (AIT) patients with differentthyroid functional status.METHODS: A blind and placebocontrolled prospective study was performed for a total of 134 caseswith AIT and thyroid peroxidase antibodies above 300 U/ml. Their mean age was 41 years (range:1570). All of them were recruited from Department of Endocrinology, First Affiliated Hospital of ChinaMedical University from June 2008 to June 2009 and divided into
2 groups according to thyroid function:
euthyroidism or subclinical hypothyroidism (n = 89) andhypothyroidism (n = 45).
Then they were randomized into 2 groups:seleniumtreated and placebotreated.
And 49 cases in subclinical autoimmune thyroiditis group and 28 cases in hypothyroidism group received200 µg oral selenium yeast daily for 6 months while others placebo. Serum concentrations ofTPOAb, TPOAb IgG subclasses, thyroidstimulating hormone (TSH), free thyroxine (FT(4)) and Se weremeasured at baseline and after 3 and 6 months of followup.
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 13/19
RESULTS: The TPOAb levels showed an overall decrease of 4.3% at 3 months and of 12.6% at 6months (both P < 0.05) postsupplementation in subclinical autoimmune thyroiditis patients. In overthypothyroidism patients, the overall decrease of TPOAb concentrations was 21.9% at 3 months and20.4% at 6 months (both P < 0.05) compared with those at pretreatment. The predominant TPOAb IgGsubclasses in sera from the AIT patients were IgG1, IgG3 and IgG4 and the positive percentages 72%,41% and 72% respectively. The positive rate and concentrations of IgG3 in the patients withhypothyroidism were significantly higher than those of subclinical autoimmune thyroiditis (P < 0.05).Significant decreases in IgG1 and IgG3 levels were noted in subclinical autoimmune thyroiditis group at 6months postsupplementation (P < 0.05). IgG1 levels in overt hypothyroidism decreased significantlycompared with those at presupplementation (P < 0.05). In all patients with supplementation (n = 77), theTPOAb levels decreased in 52 at 6 months while increase or no change occurred in 25. The positivepercentage and concentrations of IgG1 in patients whose TPOAb levels decreased at 6 months postsupplementation were markedly higher than those whose TPOAb levels increased (P < 0.05).CONCLUSION: Se is effective in reducing TPOAb concentrations and the predominantdecreasing TPOAb IgG subclasses are IgG1 and IgG3. And a high level of IgG1 subclass may explainthe difficult decline of TPOAb.
—————————————————————
Excellent article on Selenium and Hashimotos by Dr.Elias E. Mazokopakis 2007 Journal of HellenicNuclear Medicine.
16) http://www.ncbi.nlm.nih.gov/pubmed/17450242(Free Full Text): Hashimotos_and_Selenium_Dr. MazokopakisHell J Nucl Med. 2007 JanApr;10(1):68.Hashimoto’s thyroiditis and the role of selenium. Current concepts.Mazokopakis EE, Chatzipavlidou V.Hashimoto’s thyroiditis (HT) is part of the spectrum of autoimmune thyroid diseases. Clinicalmanifestations of HT are variable and commonly include diffuse or nodular goiter with euthyroidism,subclinical hypothyroidism and permanent hypothyroidism. Uncommonly, HT causes acute destructionof thyroid tissue and release of stored thyroid hormones, causing transient thyrotoxicosis(hashitoxicosis). The contribution of methods and techniques of nuclear medicine to diagnosis anddifferential diagnosis of HT is indisputable. In HT patients with overt hypothyroidism Lthyroxine (LT(4))should be given in the usual replacement doses, but in HT patients with a large goiter and normal orelevated serum thyroidstimulating hormone (TSH), LT(4) may be given in doses sufficient tosuppress serum TSH. Symptomatic patients with hashitoxicosis and low 24hour thyroid radioactiveiodine ((123)I or (123)I) uptake (RIU) may be treated with betablockers (as propranolol) and sodiumipodate or iopanoic acid (iodinated contrast agents) that block the peripheral conversion of T(4) to T(3).Recent clinical studies have documented the suppressive effect of selenium treatment on serum antithyroid peroxidase concentrations in patients with HT.
Thyroxine decreases antibody levels in HASHimotos
17) http://www.ncbi.nlm.nih.gov/pubmed/20154430Intern Med. 2010;49(4):26771. Epub 2010 Feb 15.Elevation of serum immunoglobulin G in Hashimoto’s thyroiditis and decrease after treatment with Lthyroxine in hypothyroid patients.Yamauchi K, Yamada T, Sato A, Inazawa K, Aizawa T.We undertook an investigation on the frequency and magnitude of elevated serum immunoglobulin G

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 14/19
(IgG), and effects of treatment with Lthyroxine (T(4)) in patients with Hashimoto’s thyroiditis.METHODS: Ninetyseven consecutive cases of Hashimoto’s thyroiditis, 104 patients with simple goiter,and 75 normal subjects were analyzed retrospectively. Serum total T(4), thyroid stimulating hormone(TSH), microsomal hemagglutination antibody (MHA) titer, and IgG were determined in all subjects.RESULTS: IgG was significantly elevated in patients with Hashimoto’s thyroiditis as a group, andelevation above the upper limit of the normal range was found mostly in patients with hypothyroidism.There is a significant negative correlation between serum total T(4) and IgG, and a significant positivecorrelation between TSH and IgG in patients with Hashimoto’s thyroiditis. In addition, MHA titer waspositively correlated with serum IgG. In a longitudinal analysis of hypothyroid patients with Hashimoto’sthyroiditis, restoration of euthyroidism by LT(4) administration was associated with a consistentdecrease in serum IgG.CONCLUSION: Serum IgG concentration is increased in patients with Hashimoto’s thyroiditis,particularly in hypothyroid patients, and treatment with LT(4) in such patients lowers IgG levels.
18) http://www.ncbi.nlm.nih.gov/pubmed/8837324Thyroid. 1996 Jun;6(3):1838. Effect of Lthyroxine administration on antithyroid antibody levels, lipidprofile, and thyroid volume in patients with Hashimoto’s thyroiditis. Romaldini JH, Biancalana MM,Figueiredo DI, Farah CS, Mathias PC.The changes in the serum thyroid autoantibodies, antithyroglobulin (TgAb) and antithyroidperoxidase(TPOAb), lipid profile, and thyroid volume following Lthyroxine (LT4) therapy is still a controversialmatter. We studied 23 patients with goiter due to Hashimoto’s thyroiditis; 10 had clinical hypothyroidism(CH) and 13 had subclinical hypothyroidism (SH). Both groups received LT4 (2.0 to 2.5micrograms/kg/day) for a median period of 6 months. Serum concentration of TgAb (normal value: < 200mUI/mL) and TPOAb (normal value: < 150 mUI/mL) were measured by a sensitive IRMA using 125IproteinA. Thyroid volume was determined by ultrasound (normal value: 814 mL). At the end of theobservation period the median serum TSH concentration decreased significantly in both groups (42.9 to0.55 in CH and 2.4 to 0.74 mU/L in SH patients) and serum FT4I levels increased only in the CH group(0.87 to 2.1; p < 0.05). Serum TgAb concentration did not change in SH patients (72 to 218 mUI/mL) butdeclined in CH patients (364.5 to 75 mU/mL; p < 0.05). TPOAb levels also fell in the CH group (871 to194 mUI/mL; p < 0.05) and no significant change was noted in SH patients (260 to 116 mUI/mL).Further, a significant correlation was obtained between TSH and either TPOAb concentration (rs =0.569, p < 0.01) or thyroid volume (rs = 0.488, p < 0.05) in the CH group but not in SH patients (rs =0.232, NS). LDLcholesterol was higher in the CH (159.4 mg/dL) compared with the SH group (116mg/dL). Moreover, only in the CH patients was there a significant fall in total cholesterol (224.5 to 165.5mg/dL, p < 0.05) and in LDLcholesterol (159.4 to 104.3 mg/dL, p < 0.05) values. The thyroid volumedecreased in all patients with CH and in 77% (10/13) of SH patients and a significant median in thethyroid volume decrease was found (39.7% of initial volume in the CH group and 80.9% in SH patients; p< 0.01). The influence of LT4 on both thyroid autoantibody levels and thyroid volume might beexplained by reduction of antigenic substance through a decreased stimulation of thyroid tissueby circulating TSH as was seen in CH but not in SH patients. The benefits of the administration of LT4 replacement therapy in SH patients due to Hashimoto’s thyroiditis remain to be clarified.
Hashimotos Gluten and Celiac serology
19) http://www.ncbi.nlm.nih.gov/pubmed/17461476World J Gastroenterol. 2007 Mar 21;13(11):171522.Coeliac disease in Dutch patients with Hashimoto’s thyroiditis and vice versa. Hadithi M, de Boer H,Meijer JW, Willekens F, Kerckhaert JA, Heijmans R, Peña AS, Stehouwer CD, Mulder CJ.
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 15/19
To define the association between Hashimoto’s thyroiditis and coeliac disease in Dutch patients.METHODS: A total of 104 consecutive patients with Hashimoto’s thyroiditis underwent coeliacserological tests (antigliadins, transglutaminase and endomysium antibodies) and HLADQ typing.Small intestinal biopsy was performed when any of coeliac serological tests was positive. On the otherhand, 184 patients with coeliac disease were subjected to thyroid biochemical (thyroid stimulatinghormone and free thyroxine) and thyroid serological tests (thyroglobulin and thyroid peroxidaseantibodies).RESULTS: Of 104 patients with Hashimoto’s thyroiditis, sixteen (15%) were positive for coeliacserology and five patients with documented villous atrophy were diagnosed with coeliac disease (4.8%;95% CI 0.78.9). HLADQ2 (and/or DQ8) was present in all the five and 53 patients with Hashimoto’sthyroiditis (50%; 95% CI 4362). Of 184 patients with coeliac disease, 39 (21%) were positive forthyroid serology. Based on thyroid biochemistry, the 39 patients were subclassified into euthyroidism inten (5%; 95% CI 29), subclinical hypothyroidism in seven (3.8%; 95% CI 1.87.6), and overthypothyroidism (Hashimoto’s thyroiditis) in 22 (12%; 95% CI 816). Moreover, four patients with coeliacdisease had Graves’ disease (2%; 95% CI 0.85) and one patient had postpartum thyroiditis.CONCLUSION: The data from a Dutch population confirm the association between Hashimoto’sthyroiditis and coeliac disease. Screening patients with Hashimoto’s thyroiditis for coeliac diseaseand vice versa is recommended.
20) http://www.ncbi.nlm.nih.gov/pubmed/15244201Hepatogastroenterology. 2003 Dec;50 Suppl 2:cclxxixcclxxx.The presence of the antigliadin antibodies in autoimmune thyroid diseases. Akçay MN, Akçay G.To investigate the presence of the antigliadin antibodies in the patients with Graves’ disease andHashimoto’s thyroiditis.METHODOLOGY:Four hundred patients with autoimmune thyroid disease (280 Graves’ disease and 120Hashimoto’s thyroiditis ) were included in the study. The patients with celiac sprue patients wereexcluded. For the diagnosis of autoimmune thyroiditis, blood levels of thyrotropin (TSH), free thyroxine(FT4), and the titration of thyroid autoantibodies (TgAb and TmAb) were measured, and the thyroid glandwas ultrasonographycally evaluated. After the diagnosis of autoimmune thyroid disease was established,the titration of antigliadin antibodies (Ig A and B) were routinely detected.RESULTS:Twenty two patients (5.5 per cent) with autoimmune thyroiditis had positive antigliadinantibodies. Polyglandular endocrine syndrome was diagnosed in most of these patients.CONCLUSIONS:We claim that polyglandular endocrine syndrome is the commonest cause of positivityof antigliadin antibodies in the patients with autoimmune thyroid disease.
Health Consequences of Iodine Deficiency
21) http://www.ncbi.nlm.nih.gov/pubmed/19460960Endocr Rev. 2009 Jun;30(4):376408. doi: 10.1210/er.20090011. Epub 2009 May 21.Iodine deficiency.Zimmermann MB.Iodine deficiency has multiple adverse effects in humans, termed iodine deficiency disorders, due toinadequate thyroid hormone production. Globally, it is estimated that 2 billion individuals have aninsufficient iodine intake, and South Asia and subSaharan Africa are particularly affected. However,about 50% of Europe remains mildly iodine deficient, and iodine intakes in other industrialized countries,including the United States and Australia, have fallen in recent years. Iodine deficiency during pregnancyand infancy may impair growth and neurodevelopment of the offspring and increase infant mortality.Deficiency during childhood reduces somatic growth and cognitive and motor function. Assessmentmethods include urinary iodine concentration, goiter, newborn TSH, and blood thyroglobulin. But
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 16/19
assessment of iodine status in pregnancy is difficult, and it remains unclear whether iodine intakes aresufficient in this group, leading to calls for iodine supplementation during pregnancy in severalindustrialized countries. In most countries, the best strategy to control iodine deficiency in populations iscarefully monitored universal salt iodization, one of the most costeffective ways to contribute toeconomic and social development. Achieving optimal iodine intakes from iodized salt (in the range of150250 microg/d for adults) may minimize the amount of thyroid dysfunction in populations. Ensuringadequate iodine status during parenteral nutrition has become important, particularly in preterm infants,as the use of povidoneiodine disinfectants has declined. Introduction of iodized salt to regions of chroniciodine deficiency may transiently increase the incidence of thyroid disorders, but overall, the relativelysmall risks of iodine excess are far outweighed by the substantial risks of iodine deficiency.
22) http://www.ncbi.nlm.nih.gov/pubmed/18676011Lancet. 2008 Oct 4;372(9645):125162.Iodinedeficiency disorders. Zimmermann MB, Jooste PL, Pandav CS. 2 billion individuals worldwidehave insufficient iodine intake, with those in south Asia and subSaharan Africa particularly affected.Iodine deficiency has many adverse effects on growth and development. These effects are due toinadequate production of thyroid hormone and are termed iodinedeficiency disorders. Iodine deficiency isthe most common cause of preventable mental impairment worldwide. Assessment methods includeurinary iodine concentration, goitre, newborn thyroidstimulating hormone, and blood thyroglobulin. Innearly all countries, the best strategy to control iodine deficiency is iodisation of salt, which is one of themost costeffective ways to contribute to economic and social development. When iodisation of salt isnot possible, iodine supplements can be given to susceptible groups. Introduction of iodised salt toregions of chronic iodinedeficiency disorders might transiently increase the proportion of thyroiddisorders, but overall the small risks of iodine excess are far outweighed by the substantial risks ofiodine deficiency. International efforts to control iodinedeficiency disorders are slowing, and reaching thethird of the worldwide population that remains deficient poses major challenges.
Link to this article: http://wp.me/p3gFbV14G
Jeffrey Dach MD7450 Griffin Road Suite 180/190Davie, Florida 333149547924663
http://www.jeffreydach.com/http://www.drdach.com/http://www.naturalmedicine101.com/http://www.truemedmd.com/
Disclaimer click here: http://www.drdach.com/wst_page20.html
The reader is advised to discuss the comments on these pages with his/her personal physicians and toonly act upon the advice of his/her personal physician. Also note that concerning an answer whichappears as an electronically posted question, I am NOT creating a physician — patient relationship.Although identities will remain confidential as much as possible, as I can not control the media, I can nottake responsibility for any breaches of confidentiality that may occur.
Copyright (c) 2014 Jeffrey Dach MD All Rights Reserved. This article may be reproduced on the internet
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 17/19
11 THOUGHTS ON “SELENIUM AND THYROID MORE GOOD NEWS”
without permission, provided there is a link to this page and proper credit is given.
FAIR USE NOTICE: This site contains copyrighted material the use of which has not always beenspecifically authorized by the copyright owner. We are making such material available in our efforts toadvance understanding of issues of significance. We believe this constitutes a ‘fair use’ of any suchcopyrighted material as provided for in section 107 of the US Copyright Law. In accordance with Title 17U.S.C. Section 107, the material on this site is distributed without profit to those who have expressed aprior interest in receiving the included information for research and educational purposes.
SHARE THIS:
This entry was posted in Hashimotos, Iodine, jeffrey dach, selenium, Thyroid and taggedantibodies, iodine, selenium, thyroid by Jeffrey Dach MD. Bookmark the permalink[http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/] .
1K+ 11 More
LIKE THIS:
Like
Be the first to like this.
Michael Clearyon January 1, 2014 at 2:07 PM said:
Sylvia is taking 20 mcg thyroxine. Can she take up the selenium satisfactorily?
She has had Hashimotos and resorted to the iodine 44 treatment ten years ago
Thank you for your time. Please visit http://www.IJOPT.org thats us
Jeffrey Dach MDon January 13, 2014 at 11:55 AM said:
Hi Michael,
Selenium is an essential mineral and the only one which has a code sequence in ourDNA, so yes, it is very important for thyroid function and overall health as well.
Warmest regards, jeffrey dach md
12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 18/19
Pingback: Iodine Page 11 | Mark's Daily Apple Health and Fitness Forum page 11
Pingback: Iodine and Hashimoto's Autoimmune Thyroid Disease Jeffrey Dach MD
Pingback: MyoInositol for PCOS and Hashimotos Jeffrey Dach MD
Pingback: Production of Thyroid Hormone Jeffrey Dach MD
Pingback: Does anyone supplement with Iodine? Page 7 | Mark's Daily Apple Health andFitness Forum page 7
Pingback: The Use of Iodine in Graves Hyperthyroidism
Pingback: Hashimotos Thyroiditis, Manic Depression, Psychosis and Psychiatric Manifestations Jeffrey Dach MD
Pingback: Hashimotos Thyroid Disease and Molecular Mimicry Jeffrey Dach MD
Jenniferon April 8, 2014 at 2:56 PM said:
Thanks for putting this all together in one place! What’s your opinion on the best method fortesting for selenium deficiency?
RSS Links
RSS PostsRSS Comments

12/02/2015 Selenium and Thyroid More Good News Jeffrey Dach MD
http://jeffreydachmd.com/2014/01/seleniumthyroidgoodnews/ 19/19