self-assessment examination of the american academy of dermatology
TRANSCRIPT
Self-Assessmen! I III I I
Serf-Assessment examination of the American Academy of Dermatology* donti,cation No 889-203
Learning objectives: At the conclusion of this self-assessment learning activity, physician participants should be able to assess their own diagnostic and patient management skills with respect to those of their colleagues in the field, use the results of the self-assessment to help determine personal learning needs that can be addressed through subsequent CME involvement, and enhance their ability to comply with the requirements for certification in the specialty of dermatology.
Instructions for Category 1 CME credit appear in the front advertising section. See last page of Contents for page number.
Instructions: In answering each question, refer to the specific directions provided. Because it is often necessary to provide information in questions occurring later in a series that give away answers to ear/ier questions, please answer the questions in each series in sequence.
QUESTIONS 1-9
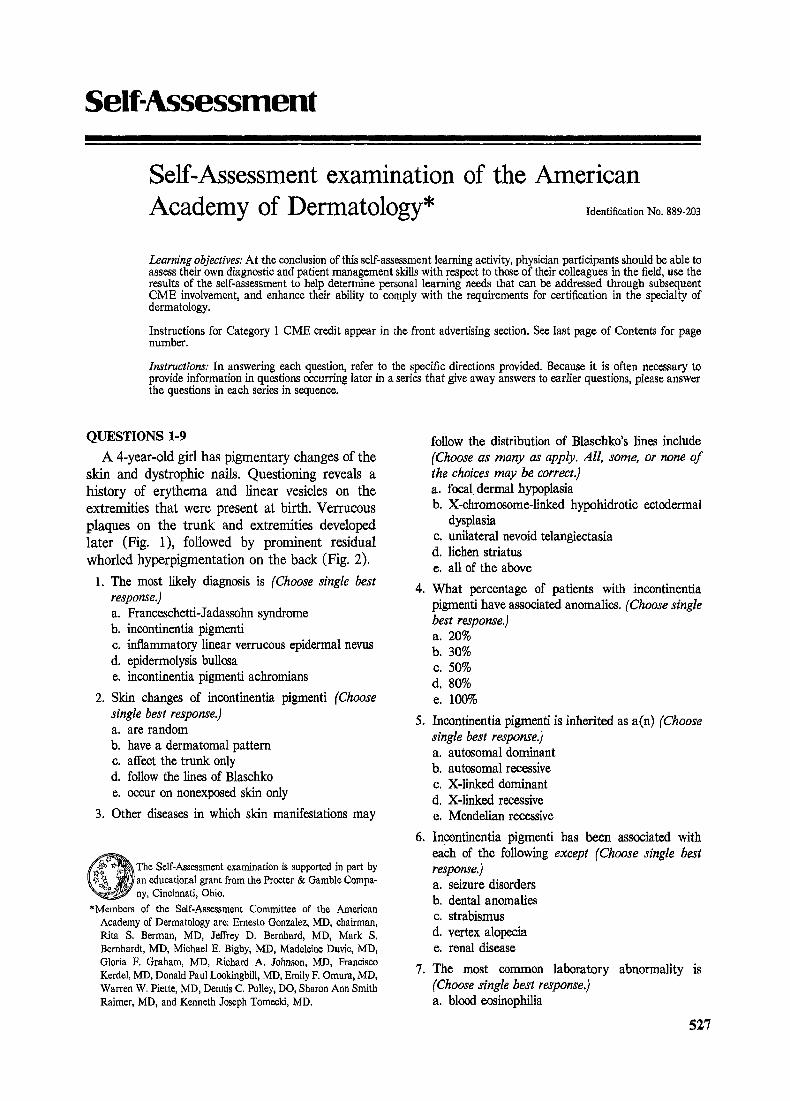
A 4-year-old girl has pigmentary changes of the skin and dystrophic nails. Questioning reveals a history of erythema and linear vesicles on the extremities that were present at birth. Verrucous plaques on the trunk and extremities developed later (Fig. 1), followed by prominent residual whorled hyperpigrnentation on the back (Fig. 2).
1. The most likely diagnosis is (Choose single best response.) a. Franceschetti-Jadassohn syndrome b. incontinentia pigmenti c. inflammatory linear verrucous epidermal nevus d. epidermolysis bullosa e. incontinentia pigmenti achromians
2. Skin changes of incontinentia pigmenti (Choose single best response.) a. are random b. have a dermatomal pattern c. affect the trunk only d. follow the lines of Blaschko e. occur on nonexposed skin only
3. Other diseases in which skin manifestations may
O The Self-Assessment examination is supported in part by an educational grant from the Procter & Gamble Compa- ny, Cincinnati, Ohio.
*Members of the Self-Assessment Committee of the American Academy of Dermatology are: Ernesto Gonzalez, MD, chairman, Rita S. Berman, MD, Jeffrey D. Bernhard, MD, Mark S. Bernhardt, MD, Michael E. Bigby, MD, Madeleine Dude, MD, Gloria F. Graham, MD, Richard A. Johnson, MD, Francisco Kerdel, MD, Donald Paul Lookingbill, MD, Emily F. Omura, MD, Warren W. Piette, MD, Dennis C. Polley, DO, Sharon Ann Smith Raimer, MD, and Kenneth J~eph Tomecki, MD.
follow the distribution of Blaschko's lines include (Choose as many as apply. All, some, or none of the choices may be correct.) a. focal dermal hypoplasia b. X-ehromosome-finked hypohidrotic ectodermal
dysplasia c. unilateral nevoid telangiectasia d. fiehen striatus e. all of the above
4. What percentage of patients with incentinentia pigmenti have associated anomalies. (Choose single best response.) a. 20% b. 30% c. 50% d, 80% e. 100%
5. Incontinentia pigmenti is inherited as a(n) (Choose single best response.) a, autosomal dominant b. autosomal recessive c. X-linked dominant d. X-linked recessive e. Mendelian recessive
6. Incontinentia pigmenti has been associated with each of the following except (Choose single best response.) a. seizure disorders b. dental anomalies c. strabismus d. vertex alopecia e. renal disease
7. The most common laboratory abnormality is (Choose single best response.) a. blood eosinophilia
527
528 Self-Assessment examination
Journal of the American Academy of
Dermatology
Volume 20 Number 3 March 1989 Se l f -Assessment examinat ion 529
b. anemia c. leukopellia d. lymphocytosis e. thrombocytopenia
Some of the histologic features of incontinentia pigementi during the vesicular and verrucous stages are depicted in Figs. 3 and 4.
g. A biopsy specimen taken during the vesicular stage would probably show each of the following charac- teristics except (Choose single best response.) a. eosinophilic spongiosis b. subcorneal and intraepidermal vesiculation c. dermal infiltrate consisting of eosinophils and
mononuclear cells d. vasculitis e. occasional dyskeratotic keratinocytes
9. In counseling a woman with incontinentia pigmenti, your statements should include each of the follow- ing except (Choose single best response.) a. at least one pregnancy in four will probably
result in spontaneous miscarriage b. half of her female offspring will have the
disease e. daughters are likely to have manifestations at
least as severe as the mother; 30% of daughters will be more severely affected than the mother
d. teeth of children with incontinentia pigmenti are often severely affected
e. 50% of her female offspring will be sterile
QUESTIONS 10-19
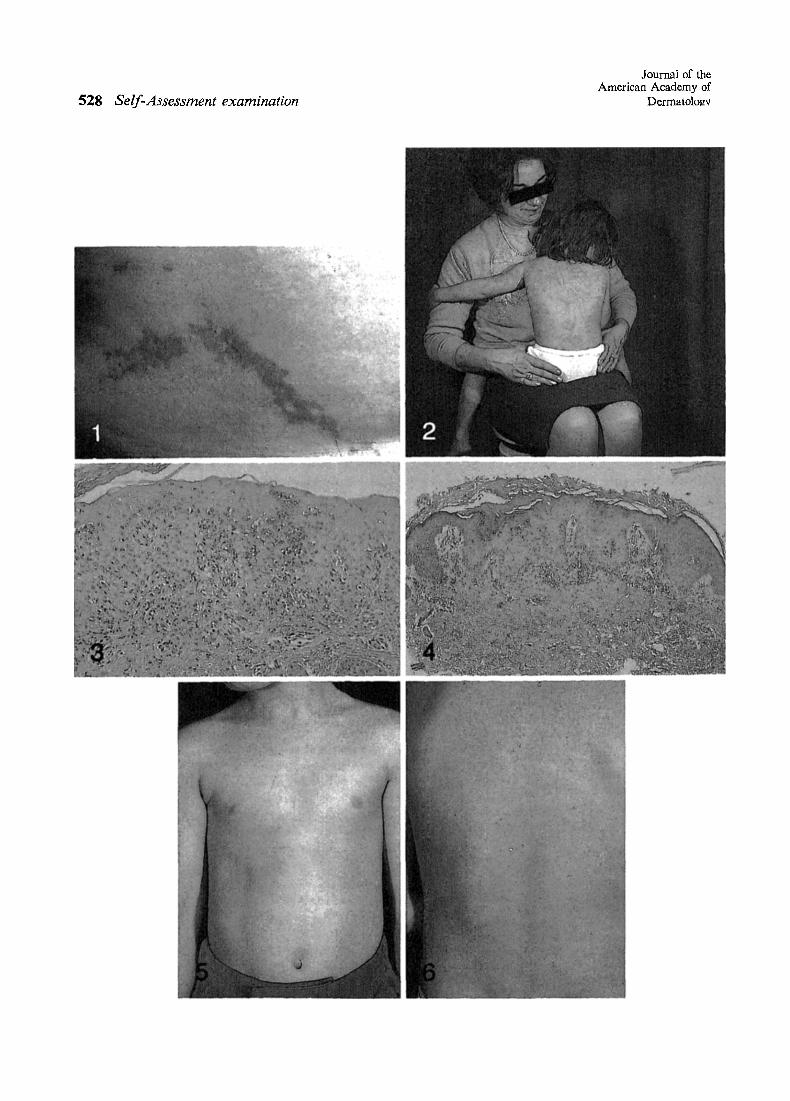
A 10-year-oN mentally retarded boy had hypo- pigmentation on the trunk. His mother reports that this had been present since the age of 3 months. He also had a seizure disorder. Physical examination revealed whorled hypopigmentation on theanterior and posterior aspects of the trunk (Figs. 5 and 6). 10. The disorder described is most consistent with
(Choose single best response.) a. nevus depigmentosus b. hypomelanosis of Ire (incontinentia pigmenti
achromians) c. the third stage of incontinentia pigmenti d. segmental vitiligo e. tuberous sclerosis
11. Associated findings include (Choose as many as apply. All, some, or none of the choices may be correct.) a. epicanthal folds b. hypertelorism
c. bifid ribs d. visceral malignancy e. decreased sweating
12. Special histologie laboratory methods that help to establish the diagnosis include (Choose as many as apply. All, some, or none o f the choices may be correct.) a. dopa reaction b. von Kossa's stain c. Fontana-Masson stain d. electron microscopy e. Giemsa's stain
13. The mode of inheritance most commonly is (Choose single best response.) a. autosomal recessive b. X-linked recessive c. sporadic mutation d. X-linked dominant e. autosomal dominant
14. Electron microscopy of the hypopigmented areas shows (Choose as many as apply. All, some, or none of the choices may be correct.) a. increased number of melanosomes within mela-
nocytes but decreased numbers within keratino- cytes
b. decreased numbers of melanosomes within melanocytes and keratinocytes
c. increased numbers of stage II melanosomes and decreased numbers of stage III and IV melano- s e i n e s
d, stage I melanosomes e. normal number of melanocytes and melano-
s o m e s
Select the one lettered i tem that is most closely related to each numbered item:
a. Nevus depigrnentosus b. Incontinentia pigmenti achromians c. Both d. Neither
15. Commonly associated with abnormalities of the central nervous system
16. Warrants genetic counseling
17. Hypomelanosis tends to fade
18. Often follows a segmental distribution
19. Histologic examination characteristically shows incontinence of pigment
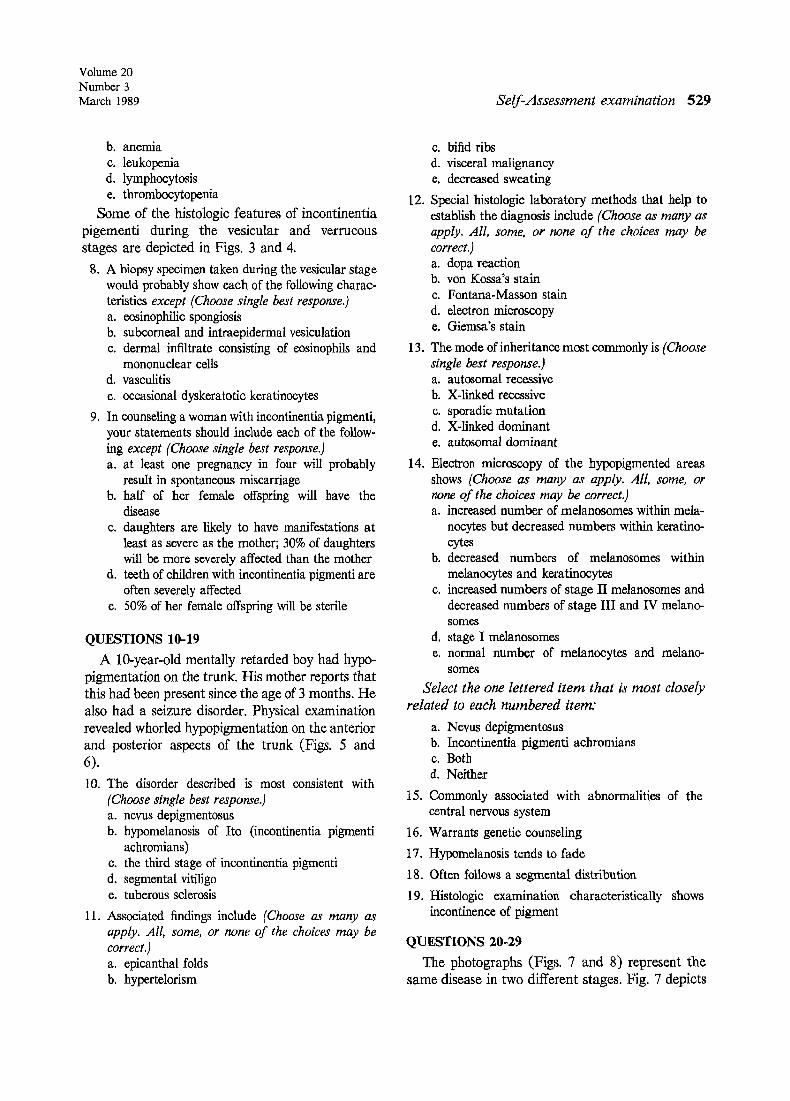
QUESTIONS 20-29 The photographs (Figs. 7 and 8) represent the
same disease in two different stages. Fig. 7 depicts
530 Self-Assessment examination
Journal of the American Academy of
Dermatology
Volume 20 Number 3 March 1989 Se l f -Assessment examination 531
a child with a macular hypopigmented whorl localized on the right side of the abdomen whereas Fig. 8 shows an erythematous, papulosquamous linear lesion along the medial aspect of a lower extremity in an adult patient.
20. Your best diagnosis is (Choose single best response.) a. incontinentia pigmenti achromians b. lichen nitidus c. linear psoriasis d. inflammatory linear verrucous epidermal nevus e. lichen striatus
21. The pattern of distribution of the lesions in both patients follows the configuration of (Choose single best response.) a. dermatomes b. Voigt's lines c. Blasehko's lines d. vascular lines e. Futclier's lines
22. Cutaneous structures that participate in the mor- phologic manifestation of diseases having the distri- bution of Blaschko's lines include (Choose as many as apply. All, some, or none of the choices may be correct.) a. epidermis b. appendages e. vascular system d. subcutaneous fat e. all of the above
23. Diseases that promSnently display the morphologic distribution of Blaschko's lines include (Choose as many as apply. All, some, or none of the choices may be correct.) a. autosomal dominant genodermatoses b. X-linked genodermatoses c. some nevoid skin diseases d. autosomal recessive genodermatoses e. some acquired skin diseases
24. Each of the following nevoid skin diseases can show Blaschko's lines distribution except (Choose single best response.) a. unilateral nevoid telangiectasia b. nevus comedonicus c. Becker's nevus d. nevus flammeus e. linear epidermal nevus
Select the one lettered item that is most closely
related to each numbered item:
a. dermatomal lines b. Blaschko's lines
c. both d. neither
25. X-linked dominant chondrodysplasia punctata (Cortradi's disease)
26. V-shaped distribution over spinal cord and anterior aspect of neck
27. interlocking ("zipper") distribution over spines
28. linear vertical lines over anterior aspect of trunk
29. may represent a functional X-chromosome mosa- icism
QUESTIONS 30-37
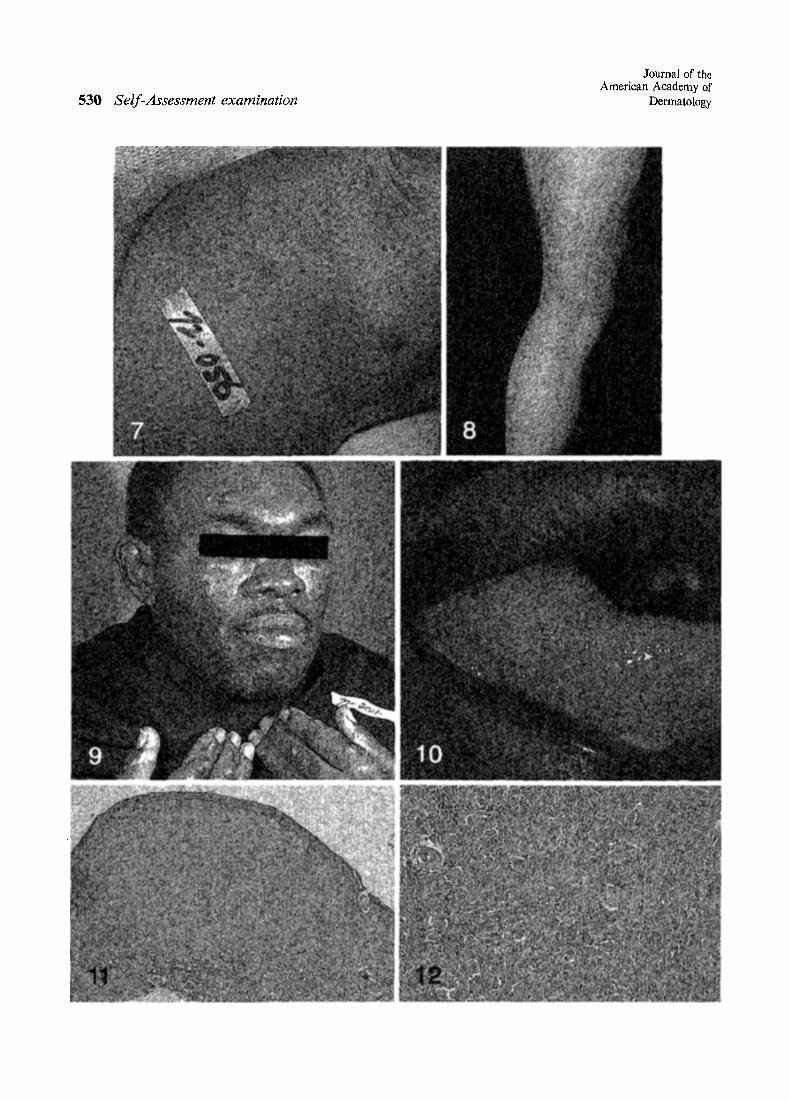
A 40-year-old black man has had painless nodules on the face and dorsa of his hands for 6 months (Fig. 9). Four months ago, progressive polyarthritis also developed involving hands, feet, wrists, knees, elbows, and shoulders. Physical examination reveals flesh-colored, firm nodules on face and dorsa of the hands; the nodules on the face show some translucency. Erythematous soft nod- ules are also present along the lateral aspect of the tongue (Fig. 10).
30. The most likely diagnosis is (Choose single best response.) a. rheumatoid arthritis b. sarcoidesis c. multicentrie reticulohistiocytosis d. tuberculosis
31. Oral lesions in patients with this entity occur in (Choose single best response.) a. 5% b. 25% c. 40% d. 50%
32. The polyarthritis described in this condition has the following characteristics: (Choose as many as apply. All, some, or none o f the choices may be correct.) a. Highly responsive to nonsteroidal anti-inflam-
matory agents b. Can produce "accordion" fingers c. Is symmetric d. Has predilection for the distal interphalangeal
joints of the fingers e. Arthritis mufilans will develop in half of the
patients
A biopsy specimen was taken from one of the cu- taneous nodules in this patient and was examined microscopically as depicted in Figs. 11 and 12.
532 Sel f -Assessment examinat ion
Journal of the American Academy of
Dermatology
33. Each of the following characteristic findings can be seen histologically except (Choose single best response.) a. dermal infiltrate with large mononuclear and
multinur giant cells b. cells with eosinophilic, ground-glass cytoplasm c. diastase-resistant muein positive for periodic
acid--Schiff stain d. large numbers of Birbeck granules on electron
microscopic examination e. cells with cytoplasm rich in organelles (lyso-
somes) on electron microscopic examination
34. Other organs that can be affected in this condition include (Choose as many as apply. All, some, or none of the choices may be correct.) a. bone b. muscle c. heart d. thyroid gland e. eye
35. The association of internaI malignancy with this condition has been recorded in (Choose single best response.) a. most cases b. very rare cases c. about one fourth of the cases d. all cases e. none of the cases
36.
37.
For cases not associated with internal malignancy, the prognosis of the acute disease is (Choose as many as apply. All, some, or none o f the choices may be correct.) a. very poor b. remission of skin and joint inflammatory
changes in approximately 8 years e. disabling sequelae with arthritis mutilans in 50%
of cases d. excellent when treated with systemic corticoste-
roids e. very unpredictable
Although response to therapy has been variable, the literature suggests the following: (Choose as many as apply. All, some, or none o f the choices may be correct.) a. Systemic corticosteroids provide the best thera-
peutic response. b. Nonsteroidal anti-inflammatory agents fre-
quently help the skin and joint symptoms. c. Response to steroids and nonsteroidal anti-
inflammatory agents, albeit variable, is usually poor.
d. Cyclophosphamide and other cytotoxic agents have been found to be effective in some cases.
e. No treatment is worth trying.