self-care and case management in long-term conditions: the ... · sdo project (08/1715/201)...
TRANSCRIPT

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 1
Self-care and Case Management in Long-term Conditions: The Effective Management of Critical Interfaces
Report for the National Insitute for Health Research Service Delivery and Organisation programme
April 2010 David Challis, University of Manchester
Jane Hughes, University of Manchester
Kathryn Berzins, University of Manchester
Siobhan Reilly, University of Manchester
Jessica Abell, University of Manchester
Karen Stewart, University of Manchester
Address for correspondence Professor David Challis Personal Social Services Research Unit University of Manchester Dover Street Building Oxford Road Manchester M13 9PL

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 2
Contents Preface ...................................................................... 6
Executive summary ................................................... 7 Background.............................................................................. 7 Aims ....................................................................................... 7 Methods .................................................................................. 7 Findings .................................................................................. 8
Literature review................................................................. 8 Survey .............................................................................. 8 A comparison of case and care management in different
settings .................................................................... 8 Case studies....................................................................... 9 Service user consultation ..................................................... 9
Conclusions.............................................................................. 9 Recommendations ...................................................................10
Chapter 1 Introduction ........................................... 11 1.1 Policy context ...................................................................11
1.1.1 Case management ................................................... 12 1.1.2 Long-term conditions................................................. 16 1.1.3 Self-care................................................................. 17 1.1.4 Implementation of case management within the
long-term conditions strategy .................................... 18 1.2 Research aims ..................................................................18 1.3 Overview of the report .......................................................19
Chapter 2 Literature review.................................... 21 2.1 Section One: Nurse case management .................................23
2.1.1 Method................................................................... 23 2.1.2 Findings ................................................................. 26 2.1.3 Summary of nurse case management interventions ...... 40
2.2 Section Two: Self-care support............................................40 2.2.1 Part one – self-care review findings ............................ 41 2.2.2 Part Two: UK based published literature ...................... 44
2.3 Section three: self-care support within nurse case management.....................................................................59 2.3.1 Findings ................................................................. 60 2.3.2 Summary of self-care support within nurse case
management interventions ........................................ 68 2.4 Discussion ........................................................................69 2.5 Summary .........................................................................71
2.5.1 How is nurse case management for long-term conditions implemented?.......................................................... 71
2.5.2 How are self-care support interventions implemented? .. 71 2.5.3 What impact do self-care support interventions have for
people with long-term conditions? .............................. 72 2.5.4 How is self-care supported within, or as a consequence
of,case management interventions?............................ 72 2.5.5 What impact does case management have upon
self-care?................................................................ 72
Chapter 3 Method ................................................... 73

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 3
3.1 Survey of case management for people with long-term conditions and self-care services ..........................................73 3.1.1 Questionnaire development ....................................... 73 3.1.2 Data collection......................................................... 74 3.1.3 Data management and analysis ................................. 74
3.2 Comparison of case/care management in different settings......74 3.2.1 National surveys ...................................................... 74 3.2.2 Data analysis .......................................................... 76
3.3 Stage two: case studies......................................................76 3.3.1 Site selection .................................................................76
3.3.2 Data collection......................................................... 79 3.3.3 Data management and analysis ................................. 80
3.4 Service user consultation....................................................80 3.4.1 Identification of user groups ...................................... 80 3.4.2 Data collection......................................................... 81 3.4.3 Data management and analysis ................................. 81
3.5 Summary .........................................................................81
Chapter 4 Survey .................................................... 82 4.1 Background ......................................................................82 4.2 Case management objectives ..............................................84 4.3 Links with other services ....................................................85 4.4 Self-care support services...................................................89 4.5 Staff mix and tasks............................................................95 4.6 Process of case management ..............................................99
4.6.1 Patient identification................................................. 99 4.6.2 Assessment.............................................................102 4.6.3 Care planning.........................................................103 4.6.4 Monitoring and review .............................................104
4.7 Information systems ........................................................107 4.8 Service development........................................................108 4.9 Summary .......................................................................110
4.9.1 Service description..................................................110 4.9.2 Case management objectives ...................................110 4.9.3 Links with other services..........................................110 4.9.4 Self-care support services ........................................111 4.9.5 Staff mix and tasks .................................................111 4.9.6 Case management ..................................................111 4.9.7 Information systems ...............................................112 4.9.8 Service development ...............................................112
Chapter 5 A comparison of case management and care management in different settings.......................... 113
5.1 Case/care management objectives.....................................113 5.2 Service characteristics and information systems...................118 5.3 Differentiation and integration within care and case
management systems.......................................................121 5.4 Summary .......................................................................123
5.4.1 Case/care management objectives ............................123 5.4.2 Service characteristics and information systems ..........124 5.4.3 Differentiation and integration within care and case
management systems..............................................124
Chapter 6 Case studies ......................................... 125 6.1 Case study sites ..............................................................125
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 4
6.2 Site one .........................................................................130 6.2.1 Links with other agencies .........................................130 6.2.2 Self-care support services ........................................132 6.2.3 Staff mix and tasks .................................................134 6.2.4 Process of case management....................................136 6.2.5 Information systems ...............................................138
6.3 Site two .........................................................................138 6.3.1 Links with other agencies .........................................139 6.3.2 Self-care support services ........................................141 6.3.3 Staff mix and tasks .................................................143 6.3.4 Process of case management....................................144 6.3.5 Information systems ...............................................146
6.4 Site three........................................................................147 6.4.1 Links with other agencies .........................................147 6.4.2 Self-care support services ........................................150 6.4.3 Staff mix and tasks .................................................153 6.4.4 Process of case management....................................154 6.4.5 Information systems ...............................................158
6.5 Site four.........................................................................158 6.5.1 Links with other agencies ..........................................159 6.5.2 Self-care support services ........................................160 6.5.3 Staff mix and tasks .................................................162 6.5.4 Process of case management....................................163 6.5.5 Information systems ...............................................166
6.6 Cross-site comparisons and emergent themes .....................167 6.6.1 Components of case management .............................167 6.6.2 The interface between self-care support and case
management ..........................................................169 6.6.3 Factors influencing variation in case management .......170
6.7 Summary .......................................................................171 6.7.1 Case study sites .....................................................171 6.7.2 Cross-site comparison and emerging themes ..............171
Chapter 7 Service user consultation ..................... 173 7.1 Knowledge and experience of self-care ...............................173 7.2 Preferences for self-care...................................................174 7.3 Priorities for a case management service ............................181 7.4 Summary .......................................................................182
Chapter 8 Concluding comments........................... 183 8.1 Methodological approach ..................................................183
8.1.1 Postal survey: response rate and categorisation of services .................................................................183
8.1.2 Limitations.............................................................184 8.1.3 Strengths ..............................................................185
8.2 Key messages from the research .......................................186 8.2.1 Literature review ....................................................186 8.2.2 Case management arrangements ..............................186 8.2.3 Self-care services and case management ...................187 8.2.4 Links between case management and other local
services .................................................................188 8.3 Emergent themes ............................................................190
8.3.1 Self-care support services within the NHS and social care model for long-term conditions...........................190
8.3.2 Programme fidelity within case management ..............191

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 5
8.3.3 Developing the workforce.........................................194 8.3.4 Service development ...............................................195
8.4 Recommendations for further research ...............................197 8.4.1 The nature of self-care support, target groups and
appropriate time frame ............................................198 8.4.2 Patient pathways within the long-term conditions
service ..................................................................198 8.4.3 Carers of patients with long-term conditions ...............198 8.4.4 The role of care plans in case management ................198 8.4.5 Outcomes for patients and carers of different
approaches to case management...............................199 8.4.6 Targeting within a long-term conditions service ...........199 8.4.7 Embedding case management in local services............199 8.4.8 Financial management arrangements in case
management ..........................................................199 8.5 End note ........................................................................200
References............................................................. 202
Appendix 1 References used to identify studies for inclusion in the review of nurse case management studies................................................................... 215
Appendix 2 Nurse case management studies data extraction tool ....................................................... 217
Appendix 3 References used to identify studies for inclusion in the review of uk self-care support studies................................................................... 219
Appendix 4 UK self-care support studies data extraction tool ....................................................... 224
Appendix 5 Survey of case management for people with long-term conditions and self-care services .. 226
Appendix 6 Service manager interview questions. 248
Appendix 7 Service manager topic guidelines....... 252
Appendix 8 Focus group topic guidelines.............. 253
Appendix 9 Service user consultation questions ... 255

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 6
Preface The Personal Social Services Research Unit at the University of Manchester was funded through the NIHR Service and Delivery Organisation Programme to investigate the role of self-care in case management for people with long-term conditions. Research into the Chronic Care Model which underpinned initial policy guidance on case management suggested that self-care support and arrangements for its delivery were most likely to improve how care was provided within the model. This research was commissioned to explore the influence of these two factors further and, in particular, links between the two.
There were a number of components in this study.
A literature review which explored nurse case management for adults with long-term conditions and evidence of interventions supporting self-care for older people with long-term conditions typical of the potential case management population.
A survey of case management for people with long-term conditions and self-care services in England.
A comparison of this data with previous national studies of care management undertaken by the Personal Social Services Research Unit.
Case studies of long-term conditions services in four primary care trusts selected because the findings from the survey suggested both that the role of self-care was demonstrably part of the service response within their locality and they exhibited different approaches to case management.
Overall, the completion of this report has been a team effort. Jane Hughes has been involved in the study since its inception and took responsibility for the completion of the report. Significant contributions have also been by other colleagues in the Personal Social Services Research Unit: Jessica Abell, Kathryn Berzins, Siobhan Reilly and, latterly, Karen Stewart. In addition, Sue Martin, Asha Myers and Angela Worden have assisted in the production of the final manuscript. I am also grateful for the assistance we have had from colleagues: Dr Ian Bowns and Professor Jackie Oldham who were co-applicants and Noreen Haselden, Sylvain Laxade and Louise Sutton who acted as consultants to the study.
A service user consultation exercise was undertaken as part of this study to ascertain the views of older people on some of the principal issues arising from the research. Four meetings were held in the North West of England. Access to two of these was facilitated by local Age Concern organisations; one via LMCP Care Link to a group primarily providing support to carers within the Asian community; and the fourth group was specially convened for this purpose by the service user advisor to the PSSRU. We are grateful to all who participated in these meetings and particularly to Pauline Blackwood, Noreen Haselden, Ahmed Lambert and Mary Murphy who were responsible for their organisation.
David Challis Professor of Community Care Research and Director PSSRU
February 2010

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 7
Executive summary
Background
It has been estimated that a large number of people suffer from a long-term condition and many of these are older people and significant users of health and social care resources. Three levels of care are specified in long-term conditions policy guidance: supported self-care for the majority of the chronic care population; disease/care management for patients who have multiple long-term conditions; and case management for those patients who are very high intensity users of unplanned secondary care. Additionally, self-care has been identified as integral to the maintenance of health and well-being for people with long-term conditions. The role of community matron was developed within the NHS and social care model for long-term conditions to undertake the case management role and within this assess the extent to which self-care support services might contribute to patient welfare.
Aims
This research had three aims. The first was to map current provision of NHS case management services in primary care for people with long-term conditions. A second aim was to classify programmes on observable features of case management implementation with particular focus upon the integration of care between primary and secondary care and between health and social care. Third, the research sought to identify the extent and nature of self-care initiatives within this service and to investigate the role of self-care initiatives as determinants of entry and, particularly, exit to the case management services.
Methods
A mixed method approach to data collection was undertaken. First, an extensive review of the literature was completed to provide a critical appraisal of the evidence relating to: case management by nurses for adults with long-term conditions; interventions supporting self-care typical of the potential case-managed population; and how case management might support self-care services. Second, a national postal survey of case management for people with long-term conditions and self-care services was undertaken. Third, findings from the survey were compared with previous studies of local authority care management arrangements for adults. Fourth, case studies of long-term conditions services in four primary care trusts were undertaken by means of a semi-structured interview with the service manager and a focus group of practitioners within each. Finally, a user consultation exercise was undertaken comprising four focus groups with the purpose of involving participants in analysing and interpreting the results of the research.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 8
Findings
Literature review
Nurse case management for people with long-term conditions was variably implemented. Case managers usually undertook key tasks such as assessment, care planning and implementation of the care plan and sometimes also monitoring and reviews. Implementation could also vary in terms of therapeutic interventions, illness management and care co-ordination, in addition to target client groups and available services. The variability between studies reflected different models of care, in addition to local implementation issues such as target client groups and the range of services at the disposal of the case manager.
Self-care interventions are often delivered using patient education, consisting of a combination of written materials and teaching sessions. Typically this is through a multi-disciplinary approach or by use of trained volunteers with experiential knowledge and can be condition specific or general, for example the Expert Patient Programme. Only modest evidence of benefit from these self-care interventions was identified with improved outcomes most likely in self efficacy, knowledge of illness and physical functioning. Self-care support within the nurse case management interventions tended to be less formalised, more individualised and delivered one-to-one in the home. Evidence relating to the impact of case management upon self-care related outcomes was inconclusive although an improvement in treatment adherence and reduced health service use was noted.
Survey
The national survey revealed considerable similarity between the objectives of the case management services and that self-care services were available in most areas, primarily accessible advice and information, generic self-care support training and disease specific self-care support training, although rarely used by case managed patients. Most case managers were nurses based in single discipline teams in primary care. Few were based in integrated health and social care settings although about half of the case management services reported formal links with local authority adult social care services. Case management services were more likely to have formal links with other primary care services such as community nursing and intermediate care. Links with secondary care services were mainly with specialist disease nursing and were rarely formalised with old age psychiatry and hospital pharmacy services. Most services reported an average active caseload per worker of fewer than fifty with referral criteria agreed locally incorporating the number of hospital admissions, age and disease. About half targeted their service on specific diseases or conditions. Assessment, implementation and monitoring of the care plan and providing patient education were almost universally reported as being part of the case manager role but it rarely incorporated financial assessments or budget management incorporating costed elements of the care plan.
A comparison of case and care management in different settings
Similarities in the goals and objectives of primary care trust case management and local authority care management arrangements were noted. The principal

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 9
differences reflected policy guidance with the latter emphasising inappropriate care home admission and a care management approach to the majority of users and the former a greater focus on improved health outcomes for patients and a more differentiated response to need apparent in the levels and qualifications of staff providing assistance and the intensity of the support provided.
Case studies
The four sites were selected to reflect different approaches to case management. They were categorised as either high or low on four domains: self-care services the presence of which was common to all; integration with social care services, a differentiated approach within the service and the performance of higher level case management tasks. The assessment of health needs and implementation, monitoring and review of care plans was undertaken in all sites. Three also reported care planning and arranging services. All provided hands on care and clinical oversight with three out of the four also providing patient advocacy, emotional support and medications review. Variation was, however, reported in terms of caseload size and the extent of integration with local authority adult social care services. All provided generic self-care support and self help groups, three provided advice and information and two provided technology and equipment to support self-care and self-care training, most of these being disease specific. Some self-care support was provided by case managers: all services provided patient education by this means and two contributed to self-care service provision and one to self-care programme development. All case managers referred on to self-care support services, most frequently for accessible advice and condition specific self-care support training.
Service user consultation
The user consultation exercise revealed priorities for service development not reflected in current policy guidance and service provision. In consideration of the range of self-care support services alternative therapies were a popular option and where group support was involved there was a preference for groups of people with the same condition rather than the generic Expert Patient Programme. Furthermore, users considered the provision of practical assistance should be a core element of a case management service.
Conclusions
The findings suggest that the local arrangements for the provision of case management and self-care services within the NHS and social care model for long-term conditions are more complex and less clearly defined than envisaged in policy guidance. Moreover there is considerable variation despite some similarities in arrangements across the country. This relates both to case management practice and its interface with self-care services which are often both at an early and partial stage of development. Furthermore, from the limited evidence available it would appear that for patients in receipt of case management, self-care support, if appropriate, is more likely to be part of the care plan provided by a nurse practitioner and not as a single response provided by other means. These

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 10
conclusions from primary data collection reflect those from the extensive literature review.
The development of case management in primary care trusts replicates earlier findings relating to the development of care management arrangements in local authority adult social care services although the former appear to be more targeted on people with complex needs. Furthermore, there is little evidence of integration between the two services, a pre-requisite to improving the patient experience.
Recommendations
Three broad areas for further research are identified. The first relates to the interface between self-care services and case management embracing the nature of self-care support, target groups and appropriate time frame for service receipt; patient pathways within the long-term conditions service; and the potential of self-care services to support carers. A second relates to programme fidelity within case management services and particularly the role of care plans and outcomes for patients and carers of different approaches. The third is more speculative, anticipating future service developments, specifically policy guidance relating to personal health budgets and the requirement for a single professional to promote access to all services identified in a care and support plan.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 11
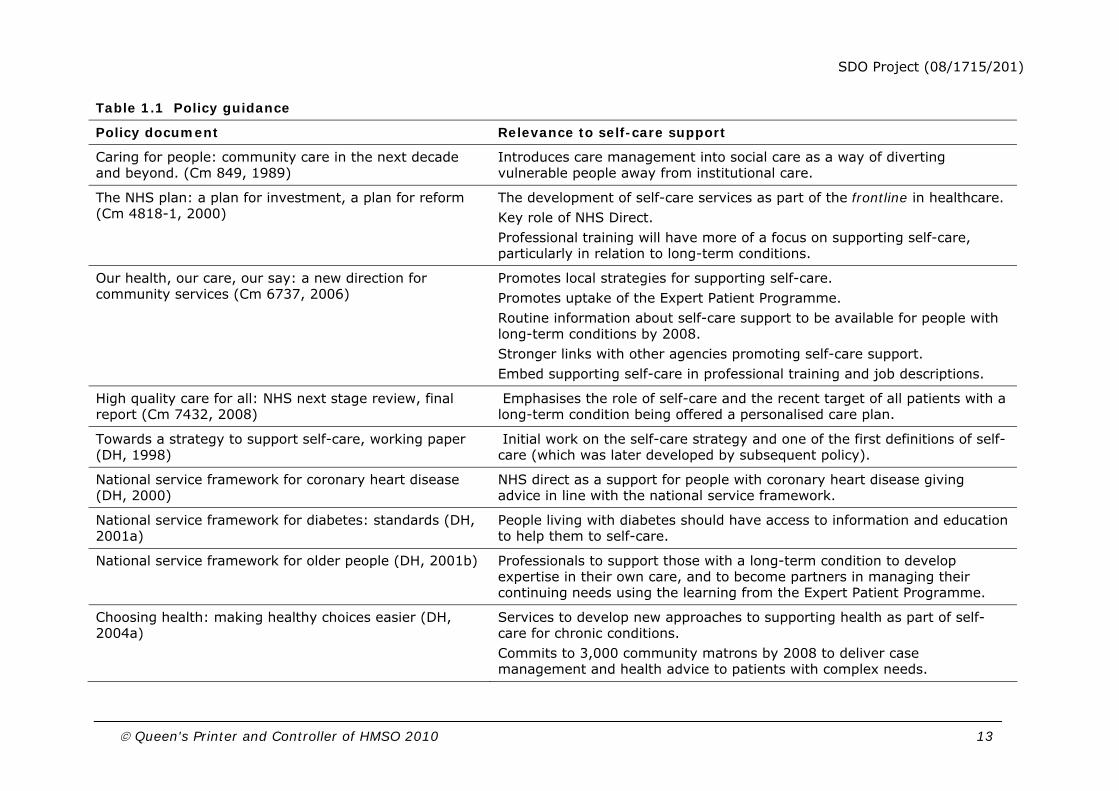
Chapter 1 Introduction This introductory chapter comprises three sections. Firstly, a brief overview of the national policy guidance and objectives for this area are provided and the relevance of the study to this policy context is considered. Secondly, the study aims and research questions are outlined and finally an overview of the structure of the report is provided. Table 1.1 provides a summary of the major policy guidance sequentially - White Papers first followed by Department of Health publications - and this logic is reflected in the references in the text throughout the report.
1.1 Policy context
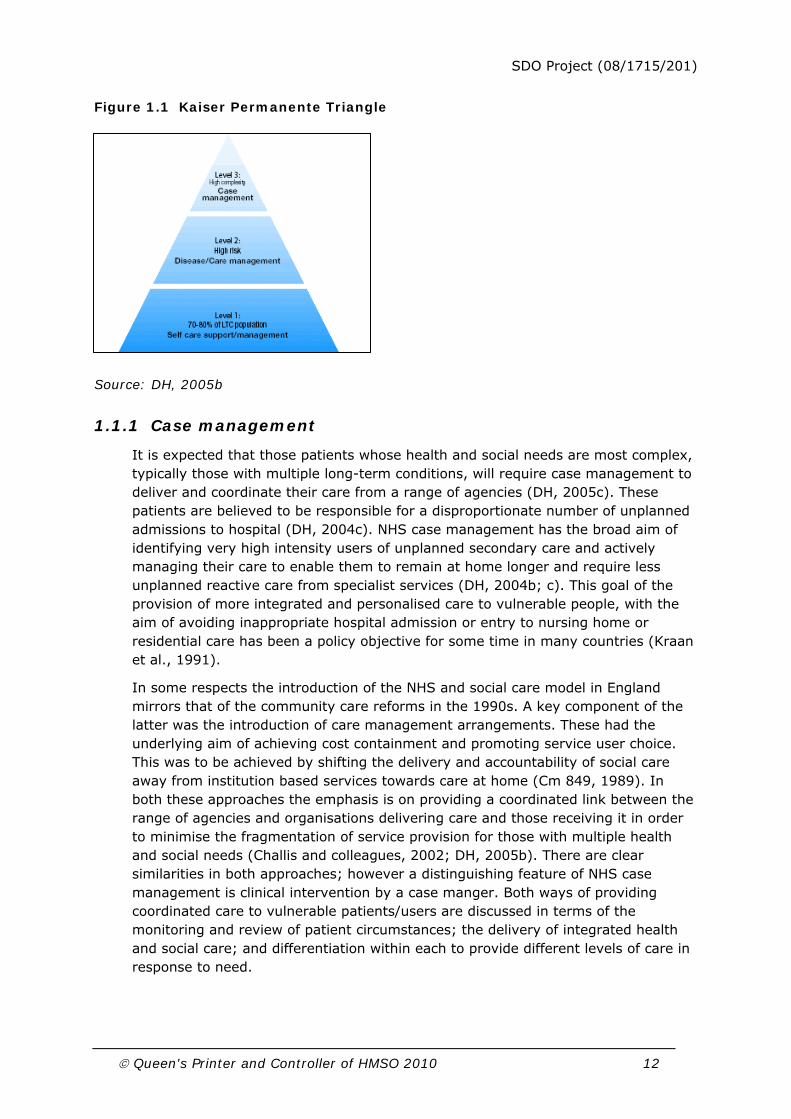
In England it is estimated that 15.4 million people suffer from a long-term condition, the majority of these aged over 60 and they use the greatest proportion of healthcare resources (DH, 2008). The NHS and social care model focuses on altering the ‘delivery system’ of care for a society where long-term conditions are prevalent, with the aim of reducing service costs and improving patients’ quality of life (DH, 2005c). It builds on an approach suggested in earlier NHS policies, such as the policy document The NHS Improvement Plan: Putting People at the Heart of Public Services (DH, 2004c) and recommends targeting service response to patients according to need. Within the long-term conditions model, this means that patients are stratified into three broad groups according to the level of support which they require. This approach is demonstrated by the Kaiser Permanente Triangle (Table 1.1), with three levels of care: supported self-care for the majority of the chronic care population; disease/care management for patients who have multiple long-term conditions; and case management for those patients who are very high intensity users of unplanned secondary care (DH, 2004b; 2004c; 2005b). The two levels of care at the top of the triangle will require more professional intervention to be delivered effectively. Underpinning this model is an emphasis on promoting better health in the population as a whole by providing advice and support about healthy choices. This broader focus on lifestyle is based on the premise of the importance of preventing the condition of patients from deteriorating and consequently requiring a more intensive level of support (DH, 2004a; 2005c). Another wider policy goal, providing people with increased choice about where they receive services and how, is also apparent in the NHS and social care model (Cm 6737, 2006; DH, 2004c).
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 12
Figure 1.1 Kaiser Permanente Triangle
Source: DH, 2005b
1.1.1 Case management
It is expected that those patients whose health and social needs are most complex, typically those with multiple long-term conditions, will require case management to deliver and coordinate their care from a range of agencies (DH, 2005c). These patients are believed to be responsible for a disproportionate number of unplanned admissions to hospital (DH, 2004c). NHS case management has the broad aim of identifying very high intensity users of unplanned secondary care and actively managing their care to enable them to remain at home longer and require less unplanned reactive care from specialist services (DH, 2004b; c). This goal of the provision of more integrated and personalised care to vulnerable people, with the aim of avoiding inappropriate hospital admission or entry to nursing home or residential care has been a policy objective for some time in many countries (Kraan et al., 1991).
In some respects the introduction of the NHS and social care model in England mirrors that of the community care reforms in the 1990s. A key component of the latter was the introduction of care management arrangements. These had the underlying aim of achieving cost containment and promoting service user choice. This was to be achieved by shifting the delivery and accountability of social care away from institution based services towards care at home (Cm 849, 1989). In both these approaches the emphasis is on providing a coordinated link between the range of agencies and organisations delivering care and those receiving it in order to minimise the fragmentation of service provision for those with multiple health and social needs (Challis and colleagues, 2002; DH, 2005b). There are clear similarities in both approaches; however a distinguishing feature of NHS case management is clinical intervention by a case manger. Both ways of providing coordinated care to vulnerable patients/users are discussed in terms of the monitoring and review of patient circumstances; the delivery of integrated health and social care; and differentiation within each to provide different levels of care in response to need.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 13
Table 1.1 Policy guidance
Policy document Relevance to self-care support
Caring for people: community care in the next decade and beyond. (Cm 849, 1989)
Introduces care management into social care as a way of diverting vulnerable people away from institutional care.
The NHS plan: a plan for investment, a plan for reform (Cm 4818-1, 2000)
The development of self-care services as part of the frontline in healthcare. Key role of NHS Direct. Professional training will have more of a focus on supporting self-care, particularly in relation to long-term conditions.
Our health, our care, our say: a new direction for community services (Cm 6737, 2006)
Promotes local strategies for supporting self-care. Promotes uptake of the Expert Patient Programme. Routine information about self-care support to be available for people with long-term conditions by 2008. Stronger links with other agencies promoting self-care support. Embed supporting self-care in professional training and job descriptions.
High quality care for all: NHS next stage review, final report (Cm 7432, 2008)
Emphasises the role of self-care and the recent target of all patients with a long-term condition being offered a personalised care plan.
Towards a strategy to support self-care, working paper (DH, 1998)
Initial work on the self-care strategy and one of the first definitions of self-care (which was later developed by subsequent policy).
National service framework for coronary heart disease (DH, 2000)
NHS direct as a support for people with coronary heart disease giving advice in line with the national service framework.
National service framework for diabetes: standards (DH, 2001a)
People living with diabetes should have access to information and education to help them to self-care.
National service framework for older people (DH, 2001b)
Professionals to support those with a long-term condition to develop expertise in their own care, and to become partners in managing their continuing needs using the learning from the Expert Patient Programme.
Choosing health: making healthy choices easier (DH, 2004a)
Services to develop new approaches to supporting health as part of self- care for chronic conditions. Commits to 3,000 community matrons by 2008 to deliver case management and health advice to patients with complex needs.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 14
Promotes use of the Expert Patient programme.
Improving chronic disease management. (DH, 2004b) Details the current position vis implementation of chronic disease management for primary care trust, NHS trust and strategic health authority management teams.
The NHS improvement plan: putting people at the heart of public services (DH, 2004c)
Introduces the long-term condition strategy (case management, disease management, self-care). Promotes the emphasis on care closer to home in the primary setting with an increased use of self-care and prevention.
The national service framework for long-term conditions (DH, 2005a)
Focus on neurological conditions but contains generic strategic advice for all long-term conditions and supports the promotion of self-care.
Supporting people with long-term conditions: an NHS and social care model to support local innovation and integration (DH, 2005b)
Encourages overall strategic approach to improving services for people with long-term conditions and take action to implement this strategy. Community matrons using a case management approach; a key role for vulnerable people with complex long-term conditions. Develop local strategies for supporting self-care and implementation of the Expert Patient Programme by 2008
Supporting people with long-term conditions: liberating the talents of nurses who care for people with long-term conditions. (DH, 2005c)
A companion to 2005b this document describes some of the roles involved in implementing the model and pays particular attention to the new role of community matron.
Self-care – A real choice: Self-care support – A practical option (DH, 2005d)
Practical examples of interventions to support self-care.
Self-care support: Baseline study of activity and development in self-care support in PCTs and local areas (DH, 2005e)
Explores how self-care support is organised and conducted within primary care trusts
Supporting self-care - a practical option: Diagnostic, monitoring and assistive tools, devices, technologies and equipment to support self-care (2006a)
Review of research on self-care tools, devices and technologies
Supporting people with long-term conditions to self-care: Importance of training for frontline staff and stronger links between

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 15
A guide to developing local strategies and good practice (DH, 2006b)
agencies providing self-care support Promotes use of information, self monitoring devices; self-care education and skills training; and support networks.
Improving care for patients with chronic obstructive pulmonary disease (Government News Network, 2006)
National service framework for with chronic obstructive pulmonary disease is due to be published and is expected to contain guidance for supporting self-care.
Self-care support summary of work in progress (DH, 2007)
Summary of work in progress – which is developing the evidence base on self- care support
Ten things you need to know about long-term conditions. (DH, 2008)
Outlines key demographic information about the long-term condition target population.
Supporting people with long-term conditions: commissioning personalised care planning, a guide for commissioners. (DH, 2009)
Practical guidance about implementing personalised care plans which emphasises the importance of including self-care support in these.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 16
Introducing a system of case management to manage the care of those with complex long-term needs has been identified as the first step in the NHS and social care model for improving the care for people with long-term conditions. The role of community matron (case managers with clinical nursing skills) has been specifically developed to undertake the case management function. It has been estimated that there are 250,000 high intensity users in England who require 3,000 community matrons to manage their care (DH, 2005b; 2004c). This approach was expected to contribute significantly to delivering the Public Service Agreement target of reducing bed days by five per cent by 2008 (DH, 2004c), improving outcomes by offering vulnerable people most at risk a personalised care plan (DH, 2005b). Recent policy has since seen this objective adjusted away from an emphasis on resource outcomes, instead stressing how everyone with a long-term condition will receive a personalised care plan agreed by the patient and a named professional (Cm 7432, 2008).
1.1.2 Long-term conditions
Level two of the long-term conditions strategy offers disease management to patients who have complex health needs associated with a specific condition (DH, 2005b). The long-term conditions strategy suggests that correctly identifying patients who require this level of care and then following a clear set of protocols for their specific condition will, amongst other outcomes, reduce their need for admission to hospital. Disease management is designed to improve the care offered to these patients using specialist services (from both primary and secondary care sources) and following disease specific pathways, such as those outlined by the national service frameworks.
Earlier national service frameworks which outlined the necessary support required for conditions such as diabetes (DH, 2001a) and coronary heart disease (DH, 2000), were published before the NHS and social care model (see Table 1.2) and do not directly reference this triangular model of care. However, these policies do share certain characteristics. They both refer to the underlying objective of promoting the independence for patients with a long-term health condition by providing them with support and information. Both also emphasise the need for specialist nurses and clinics, across primary and secondary care that cater for these specific conditions.
The common ground between these and the long-term conditions strategy is cemented by the national service framework for long-term conditions (DH, 2005a) which builds on the pyramid model mentioned above but with a discrete emphasis on how this will be implemented at a local level for those with neurological conditions. One of the distinguishing characteristics of this particular national service framework is its emphasis on supporting people with long-term neurological conditions to live as independently as possible. Its focus is on local implementation with regard to multidisciplinary working, for example the input of community pharmacy teams, referrals to specialist treatment and the provision of supported self-care. It is however, emphasised in this policy that the extent to which those requiring disease management will want to actively manage their own care will vary:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 17
“Not everyone with a long-term neurological condition will want to participate actively in their own care or be capable of managing their condition to this extent, particularly in the later stages when they may develop physical or communication difficulties. However, most will want to be involved in decisions about their care; to choose which treatment best suits their needs, and to share responsibility for managing their own condition in partnership with professional staff”
(DH, 2005a p21).
1.1.3 Self-care
Self-care is defined by the Department of Health as part of daily living to maintain health and well-being for people with long-term conditions. It includes the actions taken to minimise the impact these conditions have on their everyday lives. Table 1.1 demonstrates the recent policy initiatives which have included supported self-care for people with long-term conditions and describes their relevance. The methods by which health and social care services can support self-care for this group of people are: appropriate and accessible advice; health education; self-care skills training; self monitoring; and equipment (DH, 1998).
The Department of Health explored how self-care support was organised and conducted at primary care trust level. It found that there was no single supporting self-care strategy in place, self-care was not included in any ‘Local Delivery Plans’ and only one primary care trust had a lead officer for self-care. However, some primary care trusts did consider case management as having a key role in promoting self-care:
“The spread of the concept of case management seemed to have reached all of the PCTs and this in turn appeared to have raised the profile of self-care through awareness of its presence within the pyramid”
(DH, 2005, p12).
Part of the role of community matrons in managing patients identified as high risk is to assess the possibility of providing self-care skills training so that the individual is able to take better care of themselves (NHS Modernisation Agency and Skills for Health, 2005). Some people require a higher ratio of professional care and less self-care. Others will receive professional case management for a limited period only, and with the right level of support, can be empowered to improve existing symptoms and avoid flare-ups. Overall the NHS model for providing support to patients with long-term conditions (DH, 2005b) emphasises that this support needs to be targeted appropriately and personalised to individual requirements. Patients with long-term conditions will receive different services according to their level of need and the type of condition they are currently living with. Case management is the key component at the apex of the pyramid of need. However, if case management arrangements are to remain effective then systems need to be in place which enables patients both to enter and leave case management. Supported self–care (at the base of the pyramid) will be essential in ‘improving well-being, maintaining independence and quality of life’ (DH, 2005b p29) for those patients with long-term conditions and potentially reducing the need for professional involvement.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 18
1.1.4 Implementation of case management within the long-term conditions strategy
The roll out of case management through the development of the community matron role can be seen as part of a strategy to respond to the needs of a variety of levels of severity of need as shown in the pyramid of need (DH, 2005b). However, for this process to be successful it is important to conceive of this pyramid not just statically, in terms of horizontal slices of need groups, suitable for targeting. It also needs to be viewed vertically, in terms of the flows of patients between levels and in which direction (up or down). The extent of ‘downward flow’ in case management, at the apex of the pyramid, is likely to influence its capacity to take new cases without expansion of caseload size or staff numbers, and therefore ultimately to be sustainable. Another factor likely to affect flows through levels of the pyramid will be the degree of development of services at each level of the pyramid. In any one locality, if one level is well developed and another relatively under-developed, it is possible that there could be seepage or substitution at the margin of people from one level to another. Hence the effectiveness of this targeted pyramid of need is contingent on the development of and flow between the levels in any one locality.
Managing the progression of patients through the different stages of a service is not a new concept, either in case management literature or wider health policy. The practice of ‘bed blocking’, where patients remain in secondary care services unnecessarily has been a recent key policy issue, caused by a lack of appropriate services and clear care pathways for these patients (Henwood, 2004). Although a defining feature of case management has been its commitment to providing long-term care (Applebaum and Austin, 1990) for the most vulnerable patients, this is not considered to be an indeterminate service. The concept of advanced case management, introduced by Raiff and Shore (1993) makes the point that where appropriate, if the patient feels progress can be maintained independently or with less assistance, the transfer to another less intensive service is advantageous. This is especially relevant when considering the long-term conditions strategy described above. Patients will be regularly transferred into a more intensive service from a lower level in the pyramid (for example from disease into case management) but policy guidance is less clear about what will happen to those at the top of the pyramid.
This study is designed to address precisely these issues by examining vertical flows within the system, especially between case management at the apex of the triangle and supported self-care at the other.
1.2 Research aims
This research had three aims. The first was to map current provision of NHS case management services in primary care for people with long-term conditions. A second aim was to classify programmes on observable features of case management implementation with particular focus upon the integration of care between primary and secondary care and between health and social care. Finally, the research sought to identify the extent and nature of self-care initiatives within this service and to investigate the role of self-care initiatives as determinants of entry and, particularly, exit to the services. Arising from these aims, a number of

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 19
research questions were identified which guided more detailed areas of enquiry. These are listed Table 1.2.
Table 1.2 Research questions
What is the range of conditions catered for within a long-term conditions service?
Do primary care trusts have generic long-term conditions services and/or are they condition/patient group specific?
How do primary care trusts identify patients with long-term conditions?
Which occupational groups and grades of staff undertake case management within a long-term conditions service?
How do long-term conditions services relate to the End of Life Care Programme initiatives within localities?
To what extent and how are long-term conditions services aligned with local authority care management arrangements?
What range and type of self-care support is available and for whom is it provided within primary care trusts?
How are patients helped to access self-care programmes?
What contribution do long-term conditions services make to self-care programmes?
What is the role of self-care initiatives as a determinant of entry and exit to a long-term conditions service?
What proportion of case managed patients are/have been in receipt of formal self-care training programmes?
What arrangements are in place to facilitate transition between case management provided by a long-term conditions services and self care initiatives within localities?
How do self-care support services relate to caseload size and patient turnover in within a long-term conditions service?
What case management arrangements within a long-term conditions service are associated with more or less support for self-care?
What training do case managers receive about self-care services?
1.3 Overview of the report
The next chapter in this report (chapter two) provides a review of the relevant literature and explores the role of self-care within case management for people with long-term and chronic health conditions. It is in three distinct sections. Section one reviews the literature relating to nurse case management for adults with long-term conditions in the community. The second section, which comprises two separate parts, considers the research evidence of interventions supporting self-care for older people with long-term conditions. The final section brings together evidence from the previous sections to examine how self-care may be supported within, or as a consequence of, case management interventions. Chapter three offers a record

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 20
of the methods used by all the three stages of this study. It provides an account of the collection and analysis of the data and also describes the purpose and method of the service user consultation which was carried out as part of this research project.
Chapters four, five and six present the research findings from the three stages of this project. Chapter four describes the process data collected through a postal questionnaire, which was distributed to all case management leads in England. It discusses these findings question by question. Chapter five presents data from two previous national surveys, carried out by the Personal Social Services Research Unit, of case management arrangements for older people and people with physical disabilities, alongside survey data from the present study. The next chapter six presents the information collected from four case study sites. Chapter seven, the discussion section of the report, included a summary of the findings described in the previous three chapters. It also describes the service user consultation process, both the premise for including it at this stage of the research project and the views collected as part of this process. The final section of chapter seven is a discussion of the issues which have arisen from the findings of this research project and their implication for policy, practice and research.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 21
Chapter 2 Literature review As described in the previous chapter, UK Government policy has been promoting self-care for people with long-term conditions since 2000 to form a key part of the pyramid of care that has case management at its apex (See Figure 1.1). Self-care is defined by the Department of Health as part of daily living to maintain health and well-being, and for people with long-term conditions. It includes the actions taken to minimise the impact these conditions have on their everyday lives. The methods by which health and social care services can support self-care for this group of people are through: appropriate and accessible advice; health education; self-care skills training; self monitoring; and equipment (DH, 1998). There is little information available to ascertain how much of this activity is already happening in the UK, the impact it has on patients and to what extent it has been reported, particularly as little of it may be explicitly categorised as supporting self-care. This provides the context for the forthcoming literature review.
Case management has been the focus of many policy discussions both in health and social care over a considerable period of time (Applebaum and Austin, 1990). In England, NHS case management has been characterised as:
“.. the active management of high-risk people with complex needs, with case managers (usually nurses) taking responsibility for caseloads working in an integrated care system”
(DH, 2004b p6).
Using case management to manage the care of those with complex long-term needs has been identified as the first step in the NHS and social care model for improving the care for people with long-term conditions. The role of community matrons (case managers with clinical nursing skills) has been specifically developed to undertake the case management function and part of their role is assessing capacity for self-care (DH, 2005b).
Research carried out by the Department of Health (2005e) explored how self-care support is organised and conducted at primary care trust level. Using a random sample it found that there was no single supporting self-care strategy in place, self-care was not included in any Local Delivery Plans and only one primary care trust had a lead officer for self-care services. Although there appeared to be many self-care support activities happening, they were not necessarily contained within an overall strategy and often not labelled as such. Some primary care trusts saw case management as having a key role in promoting self-care:
“The spread of the concept of case management seemed to have reached all of the PCTs and this in turn appeared to have raised the profile of self-care through awareness of its presence within the pyramid”
(DH, 2005e p12).
Overall awareness of the potential for self-care was poor and little training was reported. The findings of this report describe a general lack of strategic direction for self-care support services, a lack of awareness amongst professionals and as a result, patchy and fragmented services. Despite this, the report also describes

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 22
positive initiatives being undertaken in supporting self-care, even if they were not explicitly labelled as such.
There are clear overlaps between supporting self-care and long-term conditions case management, usually nurse-led, although these have not appeared to been explored in previous literature. To do this, it is necessary to establish how nurse case management is implemented; what self-care support strategies have been found to have an impact; and to identify where these may already be part of nurse case management services.
This literature review aims to explore the role of self-care within case management for people with long-term and chronic health conditions. The review has been guided by five research questions:
How is nurse case management for long-term conditions implemented?
What impact do self-care support interventions have for people with long-term conditions?
How are self-care support interventions implemented?
How is self-care supported within, or as a consequence of, case management interventions?
What impact does case management have upon self-care?
The review is in three distinct sections. The method will be described separately at the start of each section. Each synthesis provides a critical appraisal of the evidence rather than a full meta-analysis.
The literature relating to nurse case management for adults with long-term conditions in the community is reviewed in section one. This outlines the implementation of case management approaches including the roles, core tasks and components of case management, along with the quality of implementation data and description of studies. Twenty-nine studies were included, with over half relating to case management for frail older people. The research evidence of interventions supporting self-care for older people with long-term conditions typical of the potential case management population is reviewed in section two. The section is split into two parts: part one gives an overview of 46 research reviews from the Cochrane Library and five other published reviews, in order to provide a broad context of the effectiveness of self-care support interventions. Part two looks more specifically at the research evidence regarding both the effects and implementation of 18 self-care support interventions in the UK context.
How self-care may be supported within, or as a consequence of, case management interventions is examined in section three. The potential impact of case management upon self-care is also explored. Twenty of the nurse case management studies reviewed in section one, which contained components that might support self-care, are re-examined. The review concludes with a discussion of the findings from the three sections and summarises the existing evidence in this area.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 23
2.1 Section One: Nurse case management
This section presents a structured review of literature which focuses upon comprehensive case management by nurses for adults with long-term conditions in the community to answer the question:
How is nurse case management for long-term conditions implemented?
The emphasis in this section is upon the implementation of case management approaches including the roles, core tasks and components of case management along with the quality of implementation data and description. The aim is to provide a consistent and comprehensive, description of the purpose, content and delivery of case management services evaluated in studies included in the review and to facilitate comprehension of nurse case management programme purposes and services.
2.1.1 Method
The review in this section focuses upon comprehensive case management (i.e. not just case finding or assessment) implemented by nurses for adults with any chronic disease or long-term condition residing in the community. Empirical research studies were primarily identified through citation tracking of previous related systematic and narrative literature reviews (Appendix 1). This was supplemented with some follow-up searching of electronic journals. Inclusion and exclusion criteria were applied to each potential reference (Table 2.1). Papers retrieved were read for reference to comprehensive case management interventions. We operationalised the term ‘comprehensive case management’ by reference to three main differentiating features: intensive client-case manager interaction (relatively small caseloads) the breadth of services encompassed (more than one service); and the duration of the case management intervention (longer term commitment, lasting a minimum of three months) (Applebaum and Austin, 1990).
Table 2.1 Section one - inclusion and exclusion criteria
Inclusion criteria
Participants Adults with one or more long-term condition/chronic disease
Country Any (published in English language)
Dates Data collected from 1980 onwards
Design Any empirical study
Location of intervention Community-based
Duration of intervention 3 months or more
Delivery of intervention Comprehensive case management interventions implemented by nurses (may have a disease specific component) and either relatively small caseloads (intensive) or more than one service spanned (breadth)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 24
Skill mix Nurses and any other professional group
Exclusion criteria
Participants Solely mental health service or palliative care service users
Service Hospital based services/residential homes/mental health services
Dates Published prior to 1980
Design Non-empirical, non-peer reviewed, grey literature
Location of intervention 'Hospital discharge' interventions with a primary goal of shortening in-patient hospital stays
Duration of intervention Less than 3 months
Delivery of intervention: Disease-specific models; predominantly telephone case management; intermediate care approaches; non-intensive client-case manager interaction (large caseloads) and breadth of services encompassed (few)
Skill mix Solely professional groups other than nurses
The content of articles meeting our inclusion criteria were reviewed using a data extraction form (Appendix 2). This was designed to extract the general characteristics of the research, professional group and location of case managers along with the core tasks and components of the case management interventions (Challis et al., 1995; 2002), including methods of identifying high-risk patients1. We recorded whether or not the core tasks and components of the case management interventions were implemented. One reviewer (SR) selected studies, and two reviewers (SR, KB) extracted data and assessed the methodological quality using a standardised instrument (Zaza et al., 2000). This measures and describes key characteristics of the studies across five categories: descriptions; sampling; measurement; data analysis; interpretation of results (Zaza et al., 2000). Clear instructions are provided to guide the decision making. Each study is assigned a score which is reduced to three main categories: Good quality (0-1); fair quality 2-4) and limited quality (≥5). The quality rating was used to provide guidance on the weight of each study finding in the synthesis and conclusions of the review. Any disagreements were resolved by consensus. Information was recorded in tabular form for each study, from which summary tables were produced. The process of the review is summarised in Figure 2.1.
1 A previous categorisation helped with classifying the various methods of identifying high-risk patients
(Hutt et al., 2004).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 25
Figure 2.1 Section one: literature review process
Empirical research primarily identified through citation tracking of related systematic and narrative literature reviews (see Appendix 1)
Inclusion and exclusion criteria applied to each potential reference (see Table 2.1)
29 studies included
Content of articles reviewed. Data extraction form used to collect and extract information into single study tables (See Appendix 2): Contextual details of each study (including population, design,
aims of interventions, skill mix and setting); Core tasks and components of the case management
interventions reported to have been implemented; Overall methodological quality detail on implementation of
interventions.
A selection of data was extracted into a summary table to guide the narrative synthesis (see Table 2.2).
Narrative synthesis comprising of a: Broad overview of the characteristics of the studies in terms of the aims of the research,
aims of the intervention, skill mix within teams and health care setting and caseload size. Discussion of the evidence relating to the core tasks of case management; management
of illness within the case management process; therapeutic intervention components; principal activities associated with complex care co-ordination; overall methodological quality and detail on implementation of interventions.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 26
2.1.2 Findings
The following synthesis is split into six sections. First, a broad overview of the characteristics of the studies in terms of the aims of the research, aims of the intervention, along with the professional group and location of case managers and data on caseload size is presented. The next five sections comprise of a narrative synthesis (Mays et al., 2005) of the evidence relating to the core tasks of case management; the management of illness within the case management process; therapeutic intervention components; tasks associated with complex care co-ordination and overall methodological quality. Primary references of studies included in the review are referred to in the text, using their corresponding number shown in Table 2.2. Any related references of studies included in the review are referred to in the conventional manner. This section concludes with a summary of the findings. Further discussion can be found at the end of section three.
2.1.2.1 Characteristics of the studies
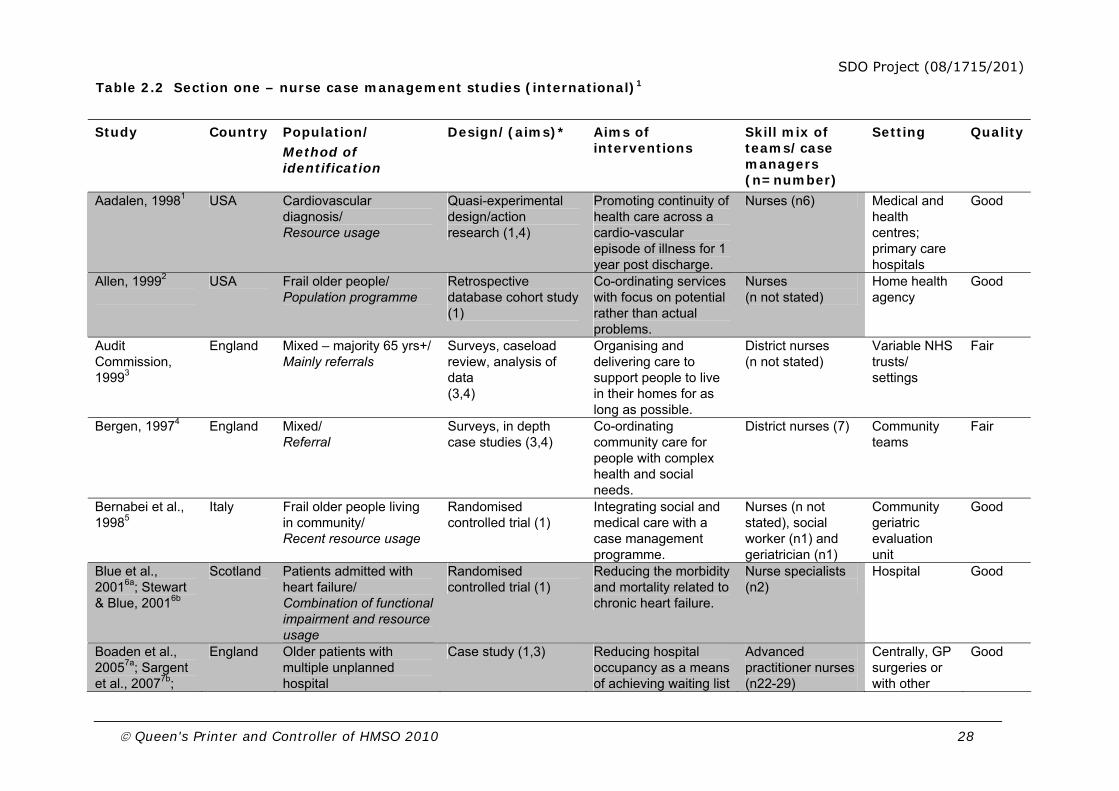
Twenty-nine studies were identified. The majority focused upon case management for frail older people (18 studies) but others targeted people with multiple chronic diseases, high cost care or at high risk of unplanned admissions (Table 2.2). Three studies provided nurse case management for people with heart failure or cardiovascular diagnosis and initiated the case management intervention in hospital, which was subsequently extended into the community1,6a,6b,23. Most studies identified were North American (15); others were based in England (9), Italy (2), Scotland (1), Canada (1) and Hong Kong (1).
Research aims and designs
The majority of studies (76%) were focused upon the effectiveness of services; fewer were focused upon the process of service delivery or how services are provided (38%). Over a quarter were concerned with the cost effectiveness of services (28%) and almost a quarter were concerned with what services were being provided (24%). Fourteen of the studies identified were randomised controlled trials and the majority (76%) were multi-site studies.
Aims of interventions
Many of the programmes covered within this review focused upon both client-oriented goals and organisational goals. For example, one demonstration project in the US aimed to improve patient health as a means of reducing the use of emergency rooms, in-patient hospital services, and other acute care services9. Similarly, in England, one of the community care demonstration projects aimed to prevent admissions to residential, nursing home or long-stay hospital care and to provide support to the carers of very frail older people11. On the other hand some projects focused solely upon administrative goals. For example, one programme aimed to reduce hospital occupancy as a means of achieving waiting list and waiting time targets7a and another aimed to reduce emergency medical admissions19. A number of studies were explicit in stating system-oriented goals,

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 27
often focused upon integrating fragmented care services. For example, one aimed to integrate social and medical care with a case management programme5.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 28
Table 2.2 Section one – nurse case management studies (international)1
Study Country Population/ Method of identification
Design/(aims)* Aims of interventions
Skill mix of teams/case managers (n=number)
Setting
Quality
Aadalen, 19981 USA Cardiovascular diagnosis/ Resource usage
Quasi-experimental design/action research (1,4)
Promoting continuity of health care across a cardio-vascular episode of illness for 1 year post discharge.
Nurses (n6) Medical and health centres; primary care hospitals
Good
Allen, 19992
USA Frail older people/ Population programme
Retrospective database cohort study (1)
Co-ordinating services with focus on potential rather than actual problems.
Nurses (n not stated)
Home health agency
Good
Audit Commission, 19993
England Mixed – majority 65 yrs+/ Mainly referrals
Surveys, caseload review, analysis of data (3,4)
Organising and delivering care to support people to live in their homes for as long as possible.
District nurses (n not stated)
Variable NHS trusts/ settings
Fair
Bergen, 19974
England Mixed/
Referral Surveys, in depth case studies (3,4)
Co-ordinating community care for people with complex health and social needs.
District nurses (7) Community teams
Fair
Bernabei et al., 19985
Italy Frail older people living in community/ Recent resource usage
Randomised controlled trial (1)
Integrating social and medical care with a case management programme.
Nurses (n not stated), social worker (n1) and geriatrician (n1)
Community geriatric evaluation unit
Good
Blue et al., 20016a; Stewart & Blue, 20016b
Scotland Patients admitted with heart failure/ Combination of functional impairment and resource usage
Randomised controlled trial (1)
Reducing the morbidity and mortality related to chronic heart failure.
Nurse specialists (n2)
Hospital
Good
Boaden et al., 20057a; Sargent et al., 20077b;
England Older patients with multiple unplanned hospital
Case study (1,3) Reducing hospital occupancy as a means of achieving waiting list
Advanced practitioner nurses (n22-29)
Centrally, GP surgeries or with other
Good

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 29
Gravelle et al., 20067c
admissions/Resource usage
and waiting time targets.
nurses
Boyd & Fisher 19968
USA Chronically ill older adults/Combination model
Controlled study (1)
Increasing continuity of care, decreasing duplication, enhancing quality of care and reducing waste.
Nurse (n1)
Community hospital
Limited
Brown et al., 20039
England Frail older people/ Referral
Non random comparative design (1)
Meeting the needs of older people and their carers.
Social workers and assistants, occupational therapists and assistants, district nurses(n not stated)
Large fund-holding practices
Fair
Brown et al., 200410a; Brown et al., 200710b
USA Multiple chronic conditions targeted (congestive heart failure 29%; coronary artery disease 24%; diabetes, 13%)/ Algorithm
Randomised controlled trial; surveys (1,3)
Improving patient health to reduce use of emergency rooms, in-patient hospital services, and other acute care services.
Registered nurses (n64; range 5-17)
Hospital Fair
Challis et al., 200211
England Older people at risk of admission to LTC/ Functional impairment
Outcome/process evaluation (1,2,3)
Preventing admissions to long-term care. Providing support to carers.
Nurse (n1), social workers (n2), physiotherapist (n1), registrar in community medicine (n1).
Primary health care
Good
Dorr et al., 200512
USA Multiple groups (diabetes diagnosis 27% selected for this study)/Referral
Retrospective matched cohort study (1)
Facilitating team collaboration, general patient education, adoption of multiple guidelines, continuity, regular follow-up.
Registered nurse/social workers (n7)
Ambulatory clinic
Good
Enguidanos et al., 200313
USA Frail older people/Combination of population programme, recent resource usage, functional impairment.
Randomised controlled trial (1,2)
To lower medical costs, improve satisfaction with care, increase care plan adherence, and improve quality of life.
Nurse/social worker (n2)
Medical centre
Good
Fiztgerald et al., 199414
USA Patients with a high risk of readmission/ Recent resource usage
Randomised controlled trial (1)
Meeting patient’s multiple needs; improving access to care and patient education; continuity and communication (in-patient to out-patient).
Nurses (n not stated)
Veterans Affairs Medical Centre
Good

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 30
Gagnon et al., 199915a; Schein et al., 200515b
Canada Frail older people/ Combination method
Randomised controlled trial (1,3)
Improving quality of life, satisfaction with care, functional status; reducing admissions to hospital and length of stay.
Nurses (n4) Community health centres
Fair
Kemper, 198816a; Carcagno & Kemper, 198816b
USA Frail older people/ Functional impairment
Randomised controlled trial (1,2)
Substituting case-managed care at home for care in nursing homes, thereby reduce long-term care costs and improving quality of life of elderly clients and their families.
Social worker and nurse (4-10 in each agency)
Variable: Public and private sector host agencies
Good
Landi et al., 199917a; Landi et al., 200117b
Italy Frail older people/ Population programme
Retrospective database cohort study (1,2)
Reorganising the care of frail older people in the community, adopting an integrated social and medical program along with case management approach.
Registered nurses (n not stated)
Community Geriatric Evaluation Unit
Good
Leung et al., 200418
Hong Kong
Frail older people discharged from hospital/ Recent resource usage
Randomised controlled trial (1,2)
Achieving integrated, quality and cost-effective care for frail elderly patients discharged from hospital.
Nurse and social worker (n2)
Not stated
Fair
Lyon et al., 200619
England
Older people/ Combination model
Observational study (1)
Reducing emergency medical admissions.
Social worker (n1) and district nurse (n1)
Primary health care
Fair
Lynch et al., 200020
USA
High risk population/ Predictive model
Time sequence case study (1)
Optimising co-ordination of medical care, increasing patient well being, community involvement and sense of purpose.
Nurses (n12) Not stated
Fair
Marshall et al., 200021a; Long, 200221b
USA Frail elderly people/Combination of functional impairment and resource usage
Randomised controlled trial (1,2)
Eliminating fragmented care, inappropriate utilisation, costs, and role confusion with co-ordinating chronic care.
Nurse and social worker (n2)
Medical office
Fair
Newcomer et al., 200422a Maravilla et al., 200522b
USA
Frail older people/ Population programme
Randomised controlled trial (1)
Achieving more timely and comprehensive care, improving patient health and reducing health care use.
Nurse (n6; 2 per affiliated medical groups)
Affiliated medical groups
Fair
Pugh et al., 200123
USA Coronary heart failure/ Resource usage
Randomised controlled trial (1,2)
Improving outcomes (functional status and quality of life) and keeping costs neutral.
Nurses (n2) Hospital Fair

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 31
*Focus of research key: 1 = impact/effectiveness; 2 = cost effectiveness; 3 = process of service delivery; 4 = services provided.
1Studies shaded grey are reviewed further in section three
Ritchie et al., 200224
USA Frail elderly veterans living in rural areas/ Population based
Randomised controlled trial (1)
Integrating community-based, chronic geriatric care, health, functioning and community tenure.
Nurse and social worker teams (n not stated)
Not stated
Fair
Ross & Tissier 199725
England Elderly and physically disabled clients/ Referral
Multi-method case study (3,4)
Focus on general practice as a setting for assessment and care management by co-ordinating social worker and district nursing assessments.
Social worker (n1) and district nurse (n1)
Primary care and social services
Fair
Schore et al., 199926
USA High cost Medicare beneficiaries/ Resource usage
Randomised controlled trial (1,2,3,4)
Improving client health and thereby reducing total medical expenses, especially for costly in-patient care
Nurses (n2) and social worker (n1)
Hospital
Fair
Schraeder et al., 200527
USA Multiple chronic conditions targeted (Coronary artery disease 48%; diabetes 38%; chronic pulmonary disease 28%; atrial fibrillation 23%; congestive heart failure 20%)/ Population programme
Randomised controlled trial (1)
Improving client health thereby reducing total medical expenses, especially for costly in-patient care
Primary care team: physician, advanced practice nurse, nurse case manager, case assistant (n not stated)
Primary health care where possible
Fair
Tucker & Brown, 199728
England Frail older people and carers/ Referral
Multi-method case study design (1)
Meeting the needs of older people through the development of joint commissioning
Social workers; district nurses; OT’s (n not stated)
General practitioner fundholding practices
Fair
Weiner et al., 200329
England Oder people – majority with mental health problems/ Mainly referral
Survey (3,4)
Promoting convenient, user centred services and improving the integration of health and social care.
Community psychiatric, district and hospital nurses and occupational therapists (n not stated)
Social services, primary and secondary health care
Good

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 32
Skill mix within teams and healthcare setting
In almost half of the studies (48%) nurses were the only professional group implementing the case management role; they ranged from registered nurses, specialist nurses, district nurses to advanced practice nurses. Over a third of the studies (38%) employed both nurses and social workers and a few (14%) included other professionals too, usually occupational therapists, as case managers.
Most case managers were based in the community, usually primary health care, medical centres or offices which may accommodate core diagnostic services. Fewer were based at hospitals. It was not clearly reported where case managers were based in three studies18,20,24.
Caseload size
Fewer than half of the studies reported the caseload size of case managers (13; 45%); these were highly variable and ranged from 221 to 50012. Some of this variation may reflect differences between the reporting of ‘active’ cases and ‘maintained’ cases, although some studies reported both, for example, Newcomer and colleagues’ study (60 active cases, 250 maintained on caseload) (2004)22a. This study of preventative nurse case management for high-risk geriatric patients enrolled in a Medicare2 plan also reported that the intensity of the role varied according to risk priorities of patients (high: 17%; medium: 37% and low: 46%) and with average contact hours of 7.7 (sd 3.7) during the year. In this study factors associated with higher risk priorities were: co-morbidities; service utilisation inconsistent with condition; unsafe home environment; nutrition problems; and poly-pharmacy. Another study reported that case managers had between 350 and 500 active patients12. Clearly only a small proportion of these patients, if any, could be in receipt of a more intense service. Average caseloads of 130 were reported in one study site27. However nurse case managers were supported by advanced practice nurses and case assistants and averaged 8.2 (nurse case manager) and 3.2 (case assistant) contacts in the first year of service (increasing to 10.3 and 5.5 respectively in year 2) and a high proportion of patient contacts occurred via the telephone (62% nurse case managers; 94% case assistants) (27). It is impossible to indicate an optimal caseload size given the high variation between studies on types and level of severity of patients, methods of identification and key components of the case management intervention.
2.1.2.2 Core tasks of case management
The coverage of each case management task has been assessed separately for all the studies (Table 2.3). Although the key tasks of assessment, care planning and implementation of the care plan were common to all programmes, they were implemented with considerable variation. A number of qualitative aspects are highlighted.
2 Medicare in the US is health insurance for people age 65 or older, under age 65 with certain disabilities, and
any age with end-stage renal disease (permanent kidney failure requiring dialysis or a kidney transplant).
http://www.medicare.gov/publications/pubs/pdf/10050.pdf

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 33
Table 2.3 Case manager involvement in core tasks of case management by study (n29)
Core tasks n (%)
Case finding and screening 12 (41)
Assessment 29 (100)
Care planning 29 (100)
Implementation/management of care plan 29 (100)
Monitoring 22 (76)
Review 22 (76)
Case closure 9 (31)
Case finding and screening
Although not all studies were solely targeted upon patients with higher risks14,22a, the heterogeneity of the populations, settings and providers demonstrated a range of different methods used to identify high-risk patients for case management (Table 2.2). The majority of studies used data relating to recent resource usage to identify patients (24%); recent hospital admissions or history of previous admissions, or a combination of resource usage and functional impairment (usually with a disease-specific element) (21%). Only two studies, both focused on frail elderly populations, used functional impairment to identify older people at risk of admission to residential, nursing or long stay hospital care11,16a. Around a fifth of studies (21%) relied upon referrals of patients as their prime method of identification of clients3,4,10a,12,25,28,29. Clearly different methods have to be adopted to fit the local information systems available, which were often inadequate1,7a,10a. The methods of identification of patients often determined the level of involvement of case managers at this stage. In about two-fifths of studies (41%), case managers were clearly actively involved in the case finding or screening of patients.
Assessment
Whilst all studies assessed patients in order to develop a care plan, only some varied the intensity of the initial assessment according to the level of risk associated with the patient, as determined at the screening stage. As most targeted high-risk patients, assessments tended to be comprehensive. Some studies emphasised this case management task more than others4,24), highlighting specific training in geriatric assessment technology5 and assessment in the home environment6a,6b,24. Some studies described the benefits of shared assessments through the development of joint paperwork, joint visits and co-location that aided informal sharing of information10a,11,19,25,28. A number of practices were highlighted in speeding up this process: an integrated case management approach19, better screening processes16a and smaller caseloads10a.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 34
Although few studies provided specific details of specific assessment measures, comprehensive structured assessment measures were used in a number of studies16a,11,27,15a, the most frequent being the Minimum Data Set for Home Care5,17b,18,24. In many cases, assessments were completed by the nurses18,21a,27,29. One UK study reported that health staff often had difficulties with financial assessments required in the context of providing social care29. Several studies reported a high level of newly discovered unmet needs in patients, either unrecognised or otherwise not being monitored or treated7a,24, highlighting the
benefit of routine standardised comprehensive assessment in people with long-term conditions.
Almost half of the studies (48%) did not report any information on whether or not there was continuity between assessment and the other core tasks of case management. Of the remainder, most indicated a predominance of continuity of assessment and case management functions (41%). Only one study explicitly reported that these tasks were separated. In this study, each of the primary care team members had clearly defined roles. Patients in the high-risk category received intensive assessment, teaching, and co-ordination from the advanced practice nurse; regularly scheduled nurse case manager phone calls; and focused monitoring calls at least monthly from the case assistant27.
Care planning and implementation of the care plan
In these tasks, the assessment is translated into the development of a care plan and then executed and delivered by the case manager. Although all studies reported these as core functions of case management, not all described how the process was undertaken. Some ensured that all identified problems were addressed by using advanced information technology, including shared electronic medical records and access to resource directories and clinical guidelines12,20,22a. In one study the high-risk registry, care plans resided on a secure server accessible through user authentication and secured, encrypted transmissions20.
The process of care planning incorporates many components and may cross many settings rather than being episode-based. Case managers in many of the programmes relied upon making referrals to other services. In many of the studies it was clear that the breadth of services was not only dependent upon the scope of the intervention but also upon the availability of appropriate long-term care and community resources16a,11 and upon the knowledge, skills and experience of case managers26. The fragmentation of care for people with cognitive impairment was highlighted in a UK demonstration study, yet the advanced practice nurses had little experience of designing care plans for this group7a. Good negotiation and communication skills were also found to be necessary due to the frequent lack of consensus between professionals, relatives, carers and clients about the proposed care plan25.
Few studies reported adequate information to gauge the intensity of the intervention during the process of implementing the care plan but, overall a picture emerged of the many factors which influenced this. In addition to caseload size previously reported, a number of studies highlighted the detrimental effect on intensity of role conflict issues associated with combining the case management

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 35
role with other clinical responsibilities1,10a,25. Eleven studies (38%) reported the total number of hours or number of contacts per case, usually per year. For those reporting hours of contact, these ranged from 4.512 to the equivalent of 54 hours per year8. A number of studies noted that contacts were more frequent in the initial case management period and decreased as the patients became more independent in managing their condition6a,6b,13,23. One multi-site study reported an emphasis on telephone contacts10a whereas others reported more home visits, despite being actively encouraged to manage issues over the telephone15a. Telephone contacts were likely to be under-reported due to the burden of recording15a. One of the few studies that indicated the balance of time for different tasks, reported that more of the case managers' time was directed towards co-ordinating health and community-based services, rather than interacting directly with the patient13. A number of other studies noted that administrative tasks reduced time for direct work with patients and may have reduced the intensity and impact of the intervention7a,15a 16a.
Crucial to the effective implementation of case management is the degree of influence which case managers have over the form and content of services provided (Challis, 2003). Few studies (14%) clearly stated that case managers had some control over the supply or availability of services or other resources11,13,16a,19. Although a similar number of interventions (17%) used the team level for decisions regarding allocation of resources, the majority relied upon making referrals to necessary services. It has been argued that a brokerage model alone is insufficient to effect influence (Arnold, 1987) and is unlikely to be very effective (Austin, 1992). However, even those with more budgetary control could be limited in how far they could achieve their programme goals without adequate service provision. For example, despite hands-on personal care, home health care, homemaking and meals being the backbone of the direct service component in one demonstration study, they were in short supply16a.
Monitoring and review
Three quarters of the studies reported monitoring and review as case management tasks. This was in relation to monitoring patient health6a,6b,7a in order to anticipate health problems, prevent deterioration in health and unnecessary admissions. It also related to monitoring services provided2,5 and monitoring to test a patient's level of condition specific learning10a. Levels of monitoring were linked to the patient’s condition in some programmes. For example, in the UK Evercare demonstration programme, if a patient's condition improved dramatically he or she was placed in the green category (minimum monitoring) pending any change7a. In many cases monitoring was during scheduled telephone and patient contacts. Mostly monitoring was carried out directly by the nurse case managers; however in one study site, around half the case assistant’s time was spent in monitoring activities compared to around a fifth of the nurse case manager's time27. Similarly, nurse case managers' input was greater to assessment than monitoring or review functions in some English sites29. Mechanisms needed to monitor providers of care, in particular formal in-home services, were identified as a major need16a and these led to considerably more monitoring than anticipated. Techniques included the use of informal care givers and skilled care providers to monitor semi-skilled in-home

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 36
services, scheduling case manager visits to coincide with the service and providing checklists of tasks to be completed and generally increasing the case managers’ accessibility to patients16a. A number of services used computerised case management records to ensure that needs were not overlooked and that scheduled interventions occurred as planned22a,22b,15a,27.
Case closure and duration
Over half of the studies (55%) did not explicitly state the duration of involvement of the case managers or whether services were time-limited. Of those that did, seven clearly stated that they were not time-limited2,7a,9,11,16a,22a,27. Others offered services for one year6a,6b,14,25, ten months15a and six months23.
Less than a third of studies provided details on the case manager's ability to close a case. It is possible that this detail was omitted due to the presumed expectation that there was a long-term responsibility. However, some services were clearly time-limited6a,6b,15a or were only funded for a specific amount of time25, and yet failed to provided details on case closure. Exit from case management is discussed further in section three.
2.1.2.3 Management of illness within the case management process
Case management was mostly separated from the immediate activity of providing clinical care. Most case managers worked in a co-ordinating rather than a care-giving capacity. The majority (79%) of studies included one or more of the management of illness intervention components shown in Table 2.4. However, the quality of reporting sometimes made the extent or presence of these difficult to discern. A minority of nurses performed care delivery duties or ‘hands-on’ nursing aspects as part of the case management role2,6a,6b (Table 2.4). A few others continued with prior nursing responsibilities1,4,25,28,29, which often gave rise to tensions when it was combined with the case management functions.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 37
Table 2.4 Case manager involvement in management of illness and therapeutic interventions by study (n29)
n (%)
Management of illness components
Care delivery/‘hands-on’ nursing 6 (21)
Self-management education 16 (55)
Medication management 9 (31)
Patient reminders 7 (24)
Therapeutic intervention components
Psychological support (client) 16 (55)
Family support 16 (55)
Carer education 14 (48)
Counselling/therapy 7 (24)
Just over half of the studies reported providing patient self-management education and almost half provided carer education. Relatively few studies incorporated medication management as part of the case managers’ role (31%). Where this was the case it included: assessment and monitoring of medication adherence; explaining medications; regular monitoring to detect changes that may be required, and ensuring these were followed up by the relevant doctor or consultant. Few studies specifically mentioned that the case managers’ role incorporated reminding patients of appointments (24%). These intervention components related to self-management are explored in further detail in section three.
2.1.2.4 Therapeutic intervention components
Two-thirds (66%) of studies included one or more of the therapeutic intervention components: psychological support; family support; counselling/therapy; or carer education; in their intervention. Again it was usually difficult to determine the balance of time spent performing these tasks (Table 2.4). Most of these studies just listed these components rather than describing them in detail, though some did appear to have a more psycho-social focus. For example, in one study case managers made special efforts to support informal caregivers, including on-site or telephone counselling, health education training programmes, mutual support groups, and assistance in care planning and co-ordination to encourage them to continue their care18. A secondary analysis of the data relating to nurse case management interventions for frail older people15a showed the proportion of patients in receipt of coping assistance (67%), life span care (35%) (which mostly encompassed family or caregiver support) and active listening (24%)15b. Similarly psycho-social support was emphasised by both patients and carers, and viewed as equally important to clinical care7a,7b. In another study site, the balance towards emotional support was very low in terms of time spent, rather than actual support provided. In the second year this was calculated as seven per cent of the nurse case manager’s time and five per cent of the case assistant’s time27.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 38
2.1.2.5 Principal attributes associated with complex care co-ordination
Although case managers in almost all studies had a co-ordinating role with outside services (90%) or within their own multi-disciplinary team (79%), fewer had a broad purview of services in managing the care network (41%) (Table 2.5). These tended to have a broader focus, for example, advanced practice nurses were expected to know where and when each of their patients made use of the services of the broader health system and were seen as the primary co-ordinators of care7a. On the other hand, in the specialist nurse intervention for heart failure, patient clinical input and patient contact was stressed more than linkage to other services6a,6b. Few studies collected data on how much of their time was spent on co-ordinating services. One exception, was one of the demonstration sites in which Case assistants spent more than three times as much of their time with patients in co-ordination (26%) compared to the nurse case managers (7%)27.
Table 2.5 Case manager involvement in complex care co-ordination - principal activities by study (n29)
In relation to integration of care between health and social services, over half of the studies reported specific links (not shown). Frequently this related to nurse case managers being part of the same team as social workers (20; 69%). In eleven studies (38%) nurse and social work case managers worked together. This offered greater opportunities for multi-disciplinary working including: opportunities for discussing service users more often and in more detail; faster referral to colleagues; improvements in role understanding; shared assessments and case management processes through the development of joint paperwork and joint visits; and the most appropriate allocation of case manager(s).
In relation to managing the care network we also attempted to determine the extent and means of links between case managers and medical physicians or general practitioners. Such links are seen as facilitating more appropriate referrals and better targeting of patients22a,25, co-ordinating effective care, accessing medical advice, adherence to treatment plans, preventing hospital admissions26 and keeping physicians informed about the programme plans for their patients10a. Strategies to improve these links included co-location with primary care7a,2, regular meetings between case managers and general practitioners, written reports on patients, shared electronic records12, maintaining informal contacts and accompanying the patient on trips to the doctor10a. Some of the case managers in one study needed more training in interacting with medical practitioners16a and explicit mechanisms were necessary to increase physician involvement16a,16b. By
Principal activities n (%)
Co-ordination/liaison with other outside services 26 (90)
Co-ordination/liaison with multi-disciplinary team 23 (79)
Managing care network 12 (41)
Advice on benefits, financial and legal issues 4 (14)
Provider education 3 (10)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 39
contrast, a more recent demonstration study employed nurses with substantial experience who could work autonomously and confidently interact with physicians10a.
Few studies (14%) reported that part of the case management role extended to advice regarding benefits, financial or legal issues. Only three studies, explicitly included provider education as a specific component of the case managers role6a,6b,10a,22a. Provider education, which is further explored in section three, aims to maximise professional understanding of the case management approach and encourage adherence to evidence-based practice guidelines. Some programmes appeared to be more rigorous in ensuring physicians adhered to guidelines10a. Where patients were not receiving care consistent with the guidelines, care co-ordinators tried to work collaboratively with the patients’ physician to determine whether, and how to rectify the situation. This activity required a high level of tact and diplomacy and some programmes were more proactive in approaching physicians by having care co-ordinators ‘hold doctors to task’ about adherence to guidelines10a. In other studies, although case managers did not explicitly offer provider education, advanced information technology played a key role12,20,27. Many different evidence-based guidelines could be adopted at once. Multiple access to the range of features of a shared electronic medical record enabled the application of several guidelines and alerts for patients who require attention, facilitating smoother integration into primary care workflow.
2.1.2.6 Methodological quality and detail on intervention components
The methodological quality of the majority of studies were rated as ‘fair’ (52%) or ‘good’ (41%) (Zaza et al., 2000). Only two studies were rated as ‘limited’ (7%). Two-thirds of the studies rated ‘good’ were randomised controlled trials.
Most studies described the implementation of the interventions but there was a high degree of variability in the level of detail. Many of these did not state basic information, such as previous experience of nurses, level of training and supervision. Only seven studies presented sufficient implementation detail deemed appropriate to assist replication7a,10a,11,15a,16a,22a,27. Although many studies (24; 83%) measured some process data, over half failed to present any case management specific activity data, including some RCTs5,6a,6b,14. Case management intervention process data was comprehensive, useful and easily interpretable in only a few studies.
Related to this, few studies stated that treatment was standardised by using a manual or protocol and few included details on whether integrity or adherence to intended planned design was evaluated or monitored. One study reported the results of a review of selected cases by a nurse consultant who specialised in case management26. Oversights by programme case managers were identified suggesting that nurses adopting this role with no prior experience in community nursing may underestimate the importance of social and environmental factors in improving the health of the client. These difficulties of moving from a hospital setting to a less familiar territory of the community have been noted in other studies15a,23 and by Drennan and colleagues (2005).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 40
2.1.3 Summary of nurse case management interventions
This structured review of literature focused upon comprehensive case management by nurses for adults with long-term conditions in the community. The emphasis was upon the implementation of case management approaches including the roles, core tasks and components of case management along with the quality of implementation data and description. Twenty-nine studies were included, with over half relating to case management for frail older people. Other studies targeted people with multiple chronic diseases, high cost patients or those at high risk of hospital admissions. All studies reported case managers undertaking the core tasks of assessment, care planning and implementation of the care plan. Greater variation was evident in relation to the core tasks of case finding, monitoring, review and case closure. Few studies provided adequate implementation information.
The variation in case management interventions reported in the 29 studies covering over 120 sites was considerable, despite some overlap on core tasks. All studies reported case managers undertaking assessment, care planning and implementation of the care plan. However, greater variation was evident in relation to case finding, monitoring, review and case closure. Case management intervention components in terms of management of illness, therapeutic interventions and complex care co-ordination were also highly variable (Tables 2.4 and 2.5). The variability between studies reflected different models of care, in addition to local implementation issues such as target client groups and the range of services at the disposal of the case manager. As this review concentrates upon implementation processes rather than evidence of outcomes, the size of estimated impacts or effect sizes are not incorporated. This is explored in more detail in section three for those studies with self-care support components.
2.2 Section Two: Self-care support
This section addresses two key questions:
What impact do self-care support interventions have for people with long-term conditions?
How are self-care support interventions implemented?
The following section is a review of research evidence of interventions supporting self-care for older people with long-term conditions typical of the potential case-managed population. The section is split into two parts. Part one gives an overview of relevant research reviews from the Cochrane Library and five other published reviews found in the initial scoping exercise through electronic database searches in order to provide a broad context of the effectiveness of self-care support interventions. Part two looks more specifically at the research evidence regarding both the effects and implementation of self-care support interventions in the UK context.
Studies were identified using existing reviews, electronic and hand searching journals. Inclusion criteria were applied and data extracted from the studies included. These are then described with summary information presented in tabular form. The conclusions from part one and part two of the section are then compared with recommendations and supporting examples in the policy literature.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 41
2.2.1 Part one – self-care review findings
Part one of this section provides an overview of the research evidence of reviews of studies supporting self-care and the Cochrane Collaboration of interventions with the potential to support self-care. The method for selection of studies is shown in Table 2.6. The Cochrane Collaboration library reviews provide a comprehensive analysis of current medical treatments and other non-pharmacological interventions. The aim of describing the reviews is to provide a broad context of the effect of self-care support strategies. Reviews identified at this stage are used again in part two to identify UK self-care support research evidence.
2.2.1.1 Self-care literature reviews Table 2.6 Section two –selection of self-care studies
Reviews of self-management in long-term conditions were identified through initial scoping of the literature (n=5).
The Cochrane Collaboration library was hand searched for reviews relating to self-care support by firstly searching all reviews under the following headings: Airways 258); Consumers and Communication 40); Effective Practice and Organisation of Care 79); Heart 120); Hypertension (72); Metabolic and Endocrine Disorders 88); Musculoskeletal 197) and Stroke 148) (n=20)
The findings of the five reviews (Barlow et al., 2002; Weingarten et al. 2002; Newman et al., 2004; Warsi et al., 2004; Chodosh et al., 2005) were similar: there is evidence of beneficial impacts from self-care interventions but they are generally modest and the methods utilised make it difficult to generalise from the findings.
Barlow and colleagues (2002) concluded that the studies reviewed suggest that self-management interventions have beneficial effects for patients, at least in the short-term, with most achieving increases in self-management behaviour, knowledge and self efficacy. Warsi and colleagues (2004) found small to moderate positive benefits for some conditions, for example diabetes intervention having more positive outcomes than arthritis interventions, but felt there was evidence of publication bias. They recommend standardising methodologies for future self-care support intervention evaluations. Newman and colleagues (2004) similarly found clearer positive outcomes in interventions aimed at asthma and diabetes rather than arthritis. They suggest that this is because arthritis and its impact on the patient is more difficult to influence.
Weingarten and colleagues (2002) focus more on the effects of interventions on provider adherence, finding that commitment to guidelines was often significantly improved. One review article sought to assess the effectiveness of self-management programmes for hypertension, osteoarthritis and diabetes in older people (Chodosh et al., 2005). The results were uncertain, concluding that: “Chronic disease self-management programmes probably have a beneficial effect on some (but not all) physiologic outcomes that have been assessed in controlled trials.” (Chodosh et al., 2005).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 42
2.2.1.2 Cochrane reviews
The forty-six Cochrane reviews that were identified were classified in seven categories. These are briefly summarised from the abstracts below.
Complementary therapies (16 reviews)
Complementary therapies, although not a self-care support intervention, were included here as they are frequently used by patients with long-term conditions and are accessed outside the formal health services. Few reviews were able to make any conclusive recommendations as to the effectiveness of the therapies. Herbal medicines showed the most effectiveness of all the complementary therapies over a range of conditions although generally the methodologies adopted made the most effective dosage and courses of treatment difficult to identify. Physical interventions such as massage therapy were shown to benefit patients by significantly improving levels of agitation and other psychiatric symptoms (Thorgrimsen et al., 2003), but herbal and homeopathic remedies were not shown to have any significant effects.
Patient education (11 reviews)
Reviews of patient education, many of them group based, showed short-term benefits (Effing et al., 2002) and the use of self monitoring and written action plans were found to reduce the need for unscheduled appointments. Providing a pre-visit booklet or information session led to more questioning and self report active behaviour from the patient (Wetzels et al., 2006). Written action plans that allow patients to alter their medication or to know when to seek help were shown to lead to improvements in levels of knowledge and less consultations (Gibson et al., 2002). The delivery of patient group education was tentatively thought to result in greater improvements in knowledge compared with information alone (Forster et al., 2001); however these latter results were inconclusive.
Adherence to medication (5 reviews)
Medication adherence was seen to remain a problem with patients in the longer term, with no reviews identifying interventions that conclusively increased adherence. The intervention promoting the most significant improvement was that of reminder packaging which showed significant increases in adherence (Heneghan et al., 2005).
Diet and exercise (5 reviews)
There were several interventions focused on changing dietary habits and promoting exercise in people with long-term conditions. All the interventions that successfully promoted exercise showed that increased activity had positive benefits for patients. Interventions focused on diet showed less significant improvements. Reviews of diet and exercise interventions combined showed significant benefits for patients

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 43
with a range of long-term conditions (Joliffe et al., 2000; Lacasse et al., 2006; Thomas et al., 2006).
Communication applications and devices (4 reviews)
From the material reviewed there is little conclusive evidence of the potential benefits of applications and devices including telemedicine. One study reviewed twenty four randomised controlled trials using Interactive Health Communication Applications (Murray et al., 2005). These are computer-based packages that provide both health information and support for decision making or behaviour change. The review found that they had a significant positive effect on knowledge, social support and clinical outcomes. However, there was variability in both the interventions and the measured outcomes so the results are difficult to generalise. There was an acceptance of telemedicine techniques by patients as part of health care interactions (Murray et al., 2005) which is important in the development of these technologies.
Psychological interventions (3 reviews)
Yorke and colleagues (2005) reviewed fifteen randomised controlled trials of variable quality examining the effect of psychological interventions for patients with asthma. Two studies showed a reduction in medication after relaxation therapy and two studies showed an increase in quality of life after cognitive behavioural therapy. Rees and colleagues (2004) reviewed 36 trials of psychological interventions (in particular, stress management) on mortality and morbidity, psychological measures, quality of life, and cardiac risk factors, in patients with coronary heart disease. They found no evidence of effect on cardiac mortality or morbidity but did find small improvements in anxiety and depression. Poor methodological quality and variation prevented conclusions being made. Psychological interventions appear to be of most benefit in promoting relaxation and alleviating anxiety and depression, perhaps caused or exacerbated by the underlying long-term condition.
Nursing interventions and surveillance (2 reviews)
It was found that multiple interventions with an enhanced nursing role had favourable effects on patients’ health and the routine review and recall of patients improved their management. Griffin and Kinmonth (1997) reviewed five trials using systems of review and surveillance for people with diabetes mellitus. A range of outcomes were measured and the study found that structured care in the community with regular prompting for doctors and patients can result in a similar standard of service as hospital care. It was recommended that systems are developed that prompt recall and review of patients by general practitioners. Similarly, Renders and colleagues (2000) reviewed forty one interventions aimed at professionals’ management of patients with diabetes in primary care, out-patient and community settings with varied interventions and outcomes. It was found that multiple interventions with patient education and an enhanced nursing role had

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 44
favourable effects on patients’ health and the routine review and recall of patients improved management.
Summary
The findings of the five key reviews (Barlow et al., 2002; Weingarten et al., 2002; Newman et al., 2004; Warsi et al. 2004; Chodosh et al., 2005) showed modest evidence of effectiveness for self-care interventions. Similarly, although the evidence from the Cochrane Collaboration reviews is far from conclusive, some tentative conclusions can be made. No negative impacts of the self-care support interventions were shown.
It was expected that the process of reviewing the Cochrane literature would place interventions in a context of what type of self-care support interventions are currently seen as having a ‘traditionally’ valid evidence-base. However, many of the studies reviewed below were classed by the Cochrane reviewers as having poor methodology which further prevents firm conclusions from being drawn, particularly for those testing the efficacy of complementary therapies. These reviews showed the least positive outcomes with the exception of herbal medicines. Some of these were deemed to have the potential to treat long-term conditions but no recommendations could be made regarding dosage and regime.
Patient education appears to be best delivered using a combination of group education reinforced by written information, although the duration of retention of knowledge gained from these sessions is unclear. The evidence shows that exercise may be easier to influence than diet and patients seem accepting of the use of new technologies to help them manage long-term conditions. A combination of these approaches may maximise positive outcomes. These findings imply that people with long-term conditions may be a difficult group with which to promote adherence to medication. Although there are a range of possible interventions that have showed improvements, they appear to be hard to sustain over the longer term. Psychological interventions appear to be of most benefit in promoting relaxation and alleviating anxiety and depression, perhaps caused or exacerbated by the underlying long-term condition. It was found that multiple interventions with patient education and an enhanced nursing role had favourable effects on patients’ health and the routine review and recall of patients improved management.
2.2.2 Part Two: UK based published literature
This part of the review looks more specifically at the UK research evidence evaluating self-care support. It describes how this evidence was identified and the findings in terms of the intervention aims, content, implementation and outcomes.
Method
Empirical studies relating to self-care support for older people were identified by multiple methods to cover a broad spectrum of studies (Appendix 3). The literature review process is summarised in Figure 2.2. Data was extracted from each study and compiled to form a narrative synthesis describing the aims, components, delivery, outcomes and methodological quality of the studies.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 45
18 studies included (19 articles)
n 3 n 15 n 0
Narrative synthesis guided by data
extracted
Content of article reviewed and data extracted to guide the narrative synthesis: The overall aim of the intervention Mode of delivery (patient education) Where it was delivered (home/group) Who delivered it and using what methods (lay workers/professionals) The impact of the intervention Methodological quality
Inclusion and exclusion criteria applied to each potential reference
Electronic database search
1997 - 2008 (n 994)
References of reviews 1997 - 2008 (n 689)
Hand searching of journals
1997 - 2008 (n 0)
Figure 2.2 Section two: literature review process
The twenty Cochrane reviews and five further reviews (See part one earlier) were used to identify potentially relevant studies. The reference list of each review was examined and any relevant article cited was identified. An electronic database search was carried out using the strategy shown in Table 2.7.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 46
Table 2.7 Section two - electronic database search strategy and results
Databases searched: CINAHL, EMBASE, Ovid MEDLINE(R), PsycINFO
Keywords: (‘asthma’ or ‘COPD’ or ‘diabetes’ or ‘hypertension’ or ‘heart disease’ or ‘heart failure’ or ‘arthritis’ or ‘osteoarthritis’ or ‘Parkinson's’ or ‘Alzheimer's’ or ‘rheum$’ or ‘chronic’ or ‘complex’ or ‘long-term condition’) and (‘self-management’ or ‘self-care’ or ‘patient education’) and (‘case management’ or ‘primary care’ or ‘community’ or ‘lay’) and (‘programme’ or ‘trial’ or ‘strategy’ or ‘intervention’) not (‘bipolar’ or ‘students’ or ‘adolescent’ or ‘mental’ or ‘smoking’ or ‘substance’ or ‘alcohol’)
n1089
Limited to English language, n1055
Limited to 1997 – 2008, n994
To supplement the electronic searching, two journals (‘Patient Education and Counselling’ and ‘Chronic Illness’) were hand searched.
Inclusion criteria
All potential studies were subject to inclusion criteria (Table 2.8). These ensured that studies were less than 10 years old, related to interventions based in community settings and the findings peer reviewed. The mean age of patients had to be fifty or above, to ensure that the interventions were suitable for older people with long-term conditions. Although, fifty is still younger than many typical case-managed patients there is very little research looking at supported self-care with older people. No studies were identified where the patients’ mean age was over seventy five.
Initially titles were read for relevance and duplicates. Abstracts were then reviewed with regard to the inclusion and exclusion criteria and further studies discarded. The inclusion and exclusion criteria were applied to each study by one of the reviewers (KB).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 47
Table 2.8 Section two - inclusion and exclusion criteria
Inclusion criteria Participants: Adults, mean age ≥ 50 with one or more long-term condition Location of intervention: Community-based health or social care Country: UK Dates: Data collected from 1997 onwards Design: Any empirical study, peer reviewed Duration of intervention: More than 3 hours or more and ongoing for one month or more Delivery: Professionals or lay led Focus of study: Process and outcomes of delivering self-care support Exclusion criteria Participants: Solely mental health service or palliative care service users, mean age < 50 Location of intervention: Hospital based services/residential homes Country: Non UK Dates: Published prior to 1997 Design: Non-empirical, non-peer reviewed, grey literature Duration of intervention: Less than 3 hours or ongoing for less than one month
Data extraction
Prior to the extraction process taking place, the studies were initially read and then re-read. A standard form was used to extract the data from each study in a systematic manner summarising the key elements and outcomes of each intervention (See Appendix 4 for data extraction tool). This included the overall aim of the intervention and details of the patients taking part. The content of the intervention was summarised e.g. patient education; exercise programmes or cognitive behavioural techniques. The method of delivery was recorded; whether the intervention was delivered in groups or individually and whether it was delivered by professionals or by lay people. The outcomes of the intervention were noted, including physical functioning; illness knowledge; exercise and diet; pain; treatment adherence; psychological functioning and health service usage. Both significant and non-significant findings were recorded. Each study was rated for quality using a standardised instrument (Zaza et al., 2000). This measures and describes key characteristics of the studies across six categories: descriptions; sampling; measurement; analysis; interpretation of results. Clear instructions are provided to guide the decision making. Each study is assigned a score which are reduced to three main categories: Good quality (0-1); fair quality (2-4) and limited quality (≥5). The quality rating was used to provide guidance on the weight of each study finding in the synthesis and conclusions of the review.
Findings
A total of 1485 individual papers were identified through the methods described above. Two hundred and forty potential studies were identified in the Cochrane reviews, a further 449 were found through the review articles, and 994 through electronic searching. After the inclusion/exclusion criteria were applied, eighteen studies (19 articles) were retained for inclusion in this section of the review.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 48
The 18 studies included all described self-care support interventions. The majority (n12) focused on osteoarthritis, others evaluated interventions for diabetes (n2) and congestive obstructive pulmonary disease (n2), one focused on a stroke intervention and another on a generic long-term conditions intervention. The primary focus of all was inherently patient education. An overview of the studies can be seen in Table 2.9 and the components of the self-care support interventions are summarised in Table 2.10.
As in section one the references of studies included in the review are referred to in the text using their corresponding number shown in Table 2.9.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 49
Table 2.9 Section two - self-care studies (UK)
Study Title of paper Source Design Target condition
Mean age
Aim of intervention
Outcome measures
Barlow et al., 1998a30a;
1998b30b
A sharing caring and learning to take control: self-management training for people with arthritis
Cochrane Non-comparative pre-test, post test
Arthritis 59 Physical and psychological well-being
Self efficacy Symptom management Pain Fatigue Anxiety
Barlow et al., 199931
Instilling the strength to fight the pain and get on with life: learning to become an arthritis self manager through an adult education programme
References Non-comparative pre-test, post test
Arthritis 57 Increase self-management ability
Self efficacy Health service usage
Barlow et al., 200032
A randomised controlled study of the Arthritis Self-management Programme in the UK
Cochrane Randomised controlled trial
Arthritis 57 Improve self-management ability
Health status Health behaviours Use of services
Buszewicz et al., 2006 33
Self-management of arthritis in primary care: randomised controlled trial
Electronic databases
Randomised controlled trial
Arthritis 68 Improve quality of life
QOL Physical function Psychological function
Finnerty et al., 200134
The effectiveness of outpatient pulmonary rehab in chronic lung disease: a randomised controlled trial
Cochrane Randomised controlled trial
Congestive obstructive pulmonary disease
69 Improve health related quality of life
Physical function
Freeman et al., 200235
Use of a cognitive behavioural arthritis
References Randomised controlled
Arthritis 51 To improve physical function
Physical Function Erythrocyte

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 50
education programmes in newly diagnosed rheumatoid arthritis
trial and psychological status
sedimentation rate Pain Psychological status.
Griffiths et al., 200036
Results at 1 year of outpatient and pulmonary rehab: a randomised controlled trial
Cochrane Randomised controlled trial
Congestive obstructive pulmonary disease
68 Reduce health service usage Increase well-being
Use of health care Wellbeing
Hammond, 199937
A cross over trial evaluating an educational behavioural joint protection programme for people with rheumatoid arthritis
Cochrane Crossover trial
Arthritis 55 Improve joint protection
Adherence with joint protection
Hammond & Freeman, 200138
One year outcomes of a randomised controlled trial of an educational behavioural joint protection programme for people with rheumatoid arthritis
References Randomised controlled trial
Arthritis 51 Improve pain, joint protection and function, psychological status
Hand pain Joint protection
Helliwell et al., 199939
A 12-month randomised controlled trial of patient education on radiographic changes and quality of life in early rheumatoid arthritis
Cochrane Randomised controlled trial
Arthritis 56 Improve QOL and radiological movement
Radiological score Quality of life General health Joint function Illness knowledge GP attendance Pharmaceutical changes
Hill et al., 200140
Effect of patient education on adherence to drug treatment for rheumatoid arthritis: a randomised
Cochrane Randomised controlled trial
Arthritis Median 62
Improve rates of adherence to medication
Medication adherence

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 51
controlled trial
Kennedy et al., 200641
The effectiveness and cost effectiveness of a national lay-led self-care support programme for patients with long-term conditions: a pragmatic randomised controlled trial’.
Electronic databases
Randomised controlled trial
All 63 Improve self efficacy and energy
Self-efficacy, Reported energy Health services utilisation
Lord et al., 199942
Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee
Electronic databases
Randomised controlled trial
Arthritis 55 Clinical improvement
Western Ontario and McMaster Universities Arthritis Index
Rogers et al., 199943
Randomised controlled trial of a comprehensive stroke education program for patients and caregivers
Cochrane Randomised controlled trial
Stroke 75 To improve patient-and carer-perceived health status
Illness knowledge Satisfaction with services Emotional outcome Disability
Sharpe et al., 200144
A blind randomised controlled trial of a cognitive behavioural intervention for patients with recent onset rheumatoid arthritis: preventing psychological and physical morbidity
References Randomised controlled trial
Arthritis 55 Psychological function Physical function
Joint function Anxiety and Depression Coping Strategy Health Disease Psychological intervention
Skinner et al., 200645
Diabetes education and self-management for ongoing and newly diagnosed: process modelling of pilot study
References Non-comparative pre/post test
Diabetes 62 Illness beliefs QOL Exercise
Quality of life Metabolic control

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 52
Steed et al., 200546
Evaluation of the UCL diabetes self-management programme: a randomised controlled trial
References Randomised controlled trial
Diabetes 60 Improve self-management behaviour and quality of life
Self-Management Quality of life Mood Blood glucose levels Illness knowledge Self-efficacy Diabetes illness cognitions
Victor et al., 200347
Lack of benefit of a primary care-based nurse-led education programme for people with osteoarthritis of the knee
References Randomised controlled trial
Arthritis 63 Improve health status QOL Pain Psychological coping
Western Ontario and McMaster Universities Arthritis Index General health Illness knowledge

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 53
Table 2.10 Section two: components of self-care support interventions and outcomes
Components of self-care support Delivery of patient
education
Outcome measures with direction of effect Study Condition
Pat
ien
t ed
uca
tio
n
Exe
rcis
e p
rom
oti
on
Pai
n m
anag
emen
t
Med
icat
ion
ad
her
ence
Psy
cho
log
ical
su
pp
ort
Die
tary
ad
vice
Car
ers
edu
cati
on
Sel
f-ca
re s
up
po
rt
gro
up
s
Ind
ivid
ual
sel
f-ca
re s
up
po
rt
Wri
tten
mat
eria
ls
Ph
ysic
al
fun
ctio
nin
g
Illn
ess
kno
wle
dg
e
Exe
rcis
e an
d d
iet
Pai
n
Tre
atm
ent
adh
eren
ce
Dep
ress
ion
an
d
anxi
ety
Sel
f ef
fica
cy
Qu
alit
y o
f lif
e
Hea
lth
ser
vice
u
sag
e
Barlow et al., 1998a;30a 1998b30b
Arthritis ↑ ↑ ↔
Barlow et al., 199931 Arthritis ↓ ↑ ↔ Barlow et al., 200032 Arthritis ↔ ↔ ↓ ↑ Buszewicz et al., 200633
Arthritis ↓ ↑ ↔
Finnerty et al., 200134 COPD ↑ ↑ ↑ Freeman et al., 200235 Arthritis ↔ ↔ ↔ Griffiths et al, 200036 COPD ↔ ↑a↓b Hammond, 199937 Arthritis ↑ ↔ Hammond and Freeman, 200138
Arthritis ↑ ↔ ↓
Helliwell et al., 199939 Arthritis ↔ ↑ ↔ ↔ ↔ Hill et al., 200140 Arthritis ↑ Kennedy et al., 200641 All Long
Term Conditions
↑ ↑ ↔
Lord et al., 199942 Arthritis ↔ ↔ ↔ ↔ Rogers et al., 199943 Stroke ↔ ↑c ↔ ↔ Sharpe et al., 200144 Arthritis ↑ ↓ ↔ Steed et al., 200545 Diabetes ↔ ↑ ↔ ↔ ↑ Skinner et al., 200646 Diabetes ↑ ↑ ↔ ↔ Victor et al., 200347 Arthritis ↔ ↔ ↔ Total 18 16 13 4 15 9 6 16 2 11 12 6 3 5 5 6 7 7 7
↑ = statistically significant improvement; ↓ statistically significant decrease; ↔ = no statistically significant change. a Primary care; bHome visits; cCarer knowledge.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 54
Research aims and design
Each of the studies summarised here aimed to measure the impact of a self-care support intervention on the life of the patients. This was either measured through broader quality of life measures or specific scales for specific dimensions such as pain. All the studies were RCTs except three which used pretest/post test designs30,31,45.
Intervention aims
Two aims were common to all interventions:
All were focused on improving aspects of patients’ wider self-management and quality of life, by increasing self efficacy and knowledge.
All supported self-management by providing education using a combination of face-to-face sessions backed up by written materials for example, education leaflets and workbooks31.
Components of self-care support
Components of the self-care support interventions can be seen in Table 2.10. The promotion of exercise was a frequent aim as many of the studies were focused on arthritis and diabetes33,46. The number of interventions for people with arthritis also resulted in a high number of interventions that aimed to improve pain management41,46. No studies used any specialist equipment or technology to support self-care.
Improving patients’ self efficacy was cited by many interventions as a key aim of the intervention 30a,41. Self efficacy is thought to be one of the key predictors of self-care behaviour as the strength of an individual’s self efficacy affects their ability to change their behaviour to adapt to the challenges of a long-term condition (Krichbaum et al., 2003). It is central to Bandura’s social cognitive theory defined as: ‘the belief in one’s capabilities to organize and execute the courses of action required to manage prospective situations’ (Bandura, 1995). Many self-care support and patient education programs explicitly include aspects which aim to increase self efficacy. For example, the Arthritis Self-management Programme used by Barlow and colleagues30a,31,32 uses mastery experience, role modelling, persuasion and reinterpretation of physiological state. Self efficacy is measured by condition specific scales such as the Arthritis Self Efficacy Scale (Lorig et al., 1989) or the Multidimensional Diabetes Scale (Talbot et al., 1997) used by Steed and colleagues (2005)46.
Dietary advice formed a key part of the diabetes interventions due to the potential impact of diet on diabetes management45,46. Carer involvement was part of six interventions35,37,38,43,45. In the diabetes and arthritis interventions it involved patients being encouraged to invite their partner or carer to the education sessions45. The stroke intervention differed from other interventions due to the severity of disability being experienced by the participants, for this reason carers

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 55
were more involved in this intervention as they would be more likely to provide direct care to the patients43.
Delivery and impact of self-care support
A number of factors were relevant to the delivery and impact: the content of patient education, leadership and mode of provision.
Patient education
Education was a focus of all the reviewed studies and was delivered through a variety of methods including teaching sessions, group discussion and written materials. The majority of courses were delivered using a combination of techniques usually short information sessions then group discussion around problem solving and individual goal setting.
All interventions were delivered in small groups except one40 which used one-to-one exercise sessions and another that involved individual sessions with a psychologist44. Group delivery (10/13, 76%) is more cost effective than one-to-one sessions45, allows discussion amongst the group and encourages the development of social relationships amongst attendees. In one case it was a key benefit of attending the group:
“Several participants expressed concern that there were few opportunities to meet with others after the end of the [group education].”31
One-to-one sessions allowed the educational experience to be very specifically tailored to the individual. Both the interventions using individual sessions showed at least one positive outcome, although the numbers are too small to attach any significance to this40,44. Eight interventions referred to using written materials to support the intervention, although only one study described having their written materials tested for accessibility40. Some studies used existing resources such as ‘The Arthritis Helpbook’31 whereas others devised and piloted their own materials47.
Group programmes lasted on average 8.4 hours over several weeks. A typical intervention consisted of a two hour weekly group for six weeks30a,33,34,41. Groups were often held in a clinic setting although one was provided as part of a wider curriculum of adult education courses at a college31. Several interventions took into consideration transport costs and timing to ensure that people in employment could attend. This can influence uptake as one study found that both timing and travel to the venue were reasons why people did not complete the course33.
Professional or lay leaders
In most studies (n=15, 83%) professionals (often nurses, e.g.42) delivered the intervention. Some interventions described a range of multi-disciplinary team members such as OT, physiotherapists and dieticians also delivering the intervention 34. Only one intervention, which used cognitive behavioural therapy,

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 56
was delivered by a psychologist44. No interventions used physicians exclusively, although there was physician input reported in one intervention38.
Three of the arthritis interventions used lay leaders30a,31,32. These were seen as an important aspect for patients, affecting the view they had of the course leaders:
“…knowing that trainers also had arthritis was an important aspect of the course experience. The trainers were looked upon not only as positive role models but also as people who really understand the needs of people with arthritis.”31
The Expert Patient Programme also uses volunteer lay people with experience of long-term conditions as tutors, often recruited from people who have completed the course themselves41.
Recruitment and delivery
The examples from UK peer reviewed literature show that the initiatives were all delivered through primary or secondary health services, except one that used existing adult education services but was advertised through health services and a voluntary organisation providing arthritis support, the Arthritis Care Network30a. Another arthritis intervention also used this network to deliver courses32. Seven used out-patient departments to recruit, three recruited through general practitioners47and one used a day hospital43. There was little other information provided as to where the courses were delivered, although one was held at a GP surgery47.
Outcomes of self-care support
The average follow-up period for the reviewed studies was 8 months with the longest final follow-up period being 12 months36 and the shortest 3 months46. Longer follow-up periods have been recommended as the modest effects of self-care support interventions may, in part be due to the short term follow up periods of most studies35. Of the 18 studies, over three-quarters (78%) showed at least one significant positive effect in at least one outcome, although improvements were generally modest. All key outcome measures of the studies were not fully measured by any of the interventions. It is difficult to summarise outcomes across all 18 studies because of the use of a wide range of different outcome measures. However, these are classified in broader groups (Table 2.10). Although the majority of the interventions had some positive outcomes, none showed large differences between pre and post intervention.
Physical functioning (including pain, exercise and diet)
Improvements in a range of physical functions were most frequently reported as significant. Energy was increased in those attending the EPP41 and joint protection and function were improved in three of the 13 arthritis studies37,38,44.
Exercise formed a component of 16 of the interventions although only three reported it as an outcome measure30a,32,34. Of these three, two studies reported an

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 57
increase30a,34. No studies reported any significant changes in diet (although this is difficult to accurately measure).
Pain management appeared to be difficult to improve with only one study reporting any significant decrease31 describing the effect as ‘modest’. This effect is particularly low considering 13 studies (72%) had pain management as a component of their intervention 33,41. Medication adherence was found to be improved in one study which was the focus of this intervention40.
The two diabetes studies linked increased illness knowledge or changed illness beliefs to behaviour change45,46. Of the six studies (33%) that explicitly measured knowledge increase, three found patients’ knowledge had significantly increased39,45,46 and another43 found significant increases in knowledge in carers.
Psychological functioning (depression, anxiety, self efficacy and
quality of life)
The different psychological aspects of living with a long-term condition were reported across eight studies. These included reduced depression and anxiety 32,33,44, increased self efficacy 30a,30b,33,41 and overall quality of life 34,46.
Self efficacy, thought to be a key part of all self-care was shown to be improved by five interventions (28%)33. All four interventions that used lay leaders reported significant increases in self efficacy, although three of these used the same intervention (the Arthritis Self-management Programme) showing that this programme, which had a strong focus on increasing self efficacy, has positive effects in this area30a,31,32,41.
‘Quality of life’ was explicitly measured by five studies, two of which reported positive changes34,46 although this area is particularly difficult to summarise due to its overlap with both increased self efficacy and other outcomes such as ‘well-being’36 and ‘psychological status’35.
Health service use
There was little impact on health service use. Although three studies reported changes, these were mixed. One study36 found their intervention group had more primary care appointments but less home visits and although number of admissions remained the same the intervention group had less days in hospital. One study reported a reduction in GP visits38 and another30a reported no change in the number of visits but patients perceived improved communication with GPs. Overall, only one study38 reported a decrease in service use for their intervention patients.
Carer involvement
Of those studies that involved carers only one reported any positive outcomes specific to this group. One study43 found that knowledge was increased in carers of stroke patients but there were no other positive effects. Another45 reported 33 per

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 58
cent of patients bringing another person with them to the course but did not measure outcomes for these people.
Methodological quality and detail on implementation of interventions
All the studies were rated for quality. The majority (n15) were classed as ‘fair’ and three were rated as ‘good’33,41,45. None were judged to be of a ‘limited’ quality. As no study measured levels of exposure to the intervention in relation to outcomes so relationship between positive significant findings and ‘dosage’ of intervention was not measured. This affected the overall quality score of the studies as did attrition rates higher than 15 per cent, as was the case in eight studies.
The process of implementation was described by a number of studies; there were 15 studies that contained enough detail thought sufficient to assist replication. This was easier when standardised curricula had been used and were thus referenced 30a,37,46, although no studies reported to what extent the planned intervention was adhered to. Other studies did not use standard curricula but provided sufficient detail of the intervention within the article 38,43,47.
Some studies raised the possibility that positive results may have been influenced by selection bias due to the nature of the people volunteering to take part in the intervention as they may be more motivated to improve their condition31,33,37. The uptake of people eligible to take part varied across studies. Skinner reported the highest percentage of uptake at 84 per cent of eligible diabetes patients45, another46 had uptake of 51 per cent of all eligible patients, with 27 per cent not interested and 23 per cent too busy. Hammond (1999) had a similar 55 per cent uptake37. Rogers and colleagues (1999) found uptake ‘disappointingly low’ but as this was an intervention for stroke patients the level of disability was higher than in other studies43. Two studies44,46 found that the patients who failed to complete the course tended to be more ‘actively diseased’ and younger with higher levels of impairment. It could be argued that these are the patients who may most benefit from self-care support yet are difficult to engage in the intervention. Sharpe and colleagues (2005) recommended further research into reducing attrition with higher risk groups. No follow-up period was longer than one year and some studies suggested that study findings may change if longer follow-up periods were used35.
2.2.2.3 Summary of self-care support interventions
UK self-care support interventions have some key features in common. They all consist of patient education, using direct teaching reinforced by written materials. Delivery can take a multi-disciplinary approach or use trained volunteers with experiential knowledge of long-term conditions. The majority are focused on individual long-term conditions, most commonly osteoarthritis although the only nationwide intervention, the Expert Patient Programme, is aimed at all long-term conditions.
Most of the interventions report at least some positive outcomes for patients. The use of groups may have benefits of providing informal social support and shared knowledge and experiences although those interventions aimed at individuals also had positive outcomes. It appears that the psychological aspects of living with a

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 59
long-term condition are more frequently improved than the physical or clinical outcomes; it seems easier to change attitudes than actual behaviour.
This section has provided an overview of research findings from studies concerning self-care support interventions. There are limited positive impacts that can result from interventions; these are often modest and more related to psychological rather than physical symptoms. Interventions appear to be more effective for patients with diabetes rather than arthritis.
All self-care support interventions are problematic due to participants being self selecting; this may mean that improvements would have occurred in any event, as these patients may be more motivated to manage their conditions. A further difficulty is the relatively short follow-up periods may not capture longer term outcomes and initial improvements may be temporary.
2.3 Section three: self-care support within nurse case management
This section addresses the following two questions:
How is self-care supported within, or as a consequence of, case management interventions?
What impact does case management have upon self-care?
It explores how nurse case management interventions might support self-care by re-examining the studies described in section one.
Case management is a key component of managing people with long-term conditions who may also benefit from self-care support. The ways in which self-care support develops and is linked with case management arrangements are likely to be crucial to the overall effectiveness of support for people with long-term conditions. As such, self-care can be conceived of as both integral to the process of case management and an outcome. The interface with supported self-care is important in the maintenance of the differentiated pattern of support. The ways in which integration and differentiation are addressed in the development of long-term conditions case management are likely to be important determinants of its effectiveness. Some people require a higher ratio of professional care and less self-care whereas others will receive case management for a limited period, and with the right level of support, can be empowered to improve existing symptoms, avoid flare-ups, slow deterioration and prevent the development of complications (DH, 2005b). In England, it is expected that self-care strategies be considered and negotiated with each patient regardless of his or her level of care for chronic disease management (Metcalf, 2005; DH, 2006c). A tailored and stepped approach to patient education is vital in overcoming many of the barriers to self-care in people with complex long-term conditions (Riegel and Carlson, 2002). Studies repeatedly report poor patient and family knowledge and compliance as key contributors to avoidable hospital admissions and poor outcomes in chronic illness (Chen et al., 2000). Diverse combinations of illnesses are likely to require that case managers provide a large proportion of patient education, supplemented by community-based education programmes.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 60
As described earlier, the whole systems approach of Kennedy and colleagues (2006) highlighted the role of the nurse in delivering self-care support. Furthermore, the introduction of the community matron, using a case management approach, forms a key part of current long-term conditions strategy (DH, 2005b; 2005c) with part of the role of community matrons being to assess patients’ capacity for self-care (NHS Modernisation Agency and Skills for Health, 2005).These developments mean that the nursing role in supporting self-care through case management is likely to increase. The method employed in this section of the review is shown in Table 2.11.
Table 2.11 Section three – re-examination of nurse case management studies
The 29 studies of nurse case management reviewed in section one were re-examined to determine those with intervention components that had the potential to support self-care. Studies were re-examined with a focus on the components of self-care support identified in section two: patient education; provider education; exercise; medication and treatment management; patient and carer psychological support; dietary advice; carer education; and technology. Further details of these components were extracted and the findings summarised in tabular form. The studies were also reviewed in relation to reported outcomes that were identified as relevant to self-care support in the UK literature. These were: physical functioning; illness knowledge; exercise and diet; pain; treatment adherence; depression and anxiety; satisfaction; quality of life; and health service usage. Descriptions of exit from case management were reviewed in relation to self-care support. Findings in these outcome areas and the direction of effect are summarised in Table 2.12. Note: For full details of the method see section one
2.3.1 Findings
Twenty studies were included in this section. As in previous sections, the references of studies included in the review are referred to in the text using their corresponding number shown in Table 2.12. The majority focused on frail older people or people with long-term conditions. Three interventions were condition specific1,6a,6b,23. Most studies were North American (n14) with a further four from the UK and one from Hong Kong. Nine interventions included multi-disciplinary input in addition to nursing. All twenty studies focused on effective delivery of services to improve patient outcomes and fourteen aimed to decrease service use. Twelve studies were RCTs.
2.3.1.1 Components of self-care support
The twenty studies described varying components that had the potential to support self-care. These components and whether the study detected any significant positive outcome are reported in Table 2.12. Psychological support (n17) and education for patients and carers (n16) were frequently incorporated components to support self-care within the case management approaches. Sixteen studies included medication management and patient reminders (for example, to attend routine appointments). Six studies provided dietary advice and four provided advice on exercise. Three studies reported an element of provider education and five reported the use of technology and equipment to support self-care. No studies reported the use of complementary therapies.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 61
Table 2.12 Section three: components of self-care support interventions and outcomes in nurse case management studies
Study Components of self-care support Delivery of patient education
Outcome measures with direction of effect
Pa
tie
nt
ed
uc
atio
n
Pro
vid
er
ed
uc
ati
on
Ex
erc
ise
Me
dic
atio
n a
nd
tr
eatm
en
t m
an
ag
em
en
t/a
pp
oi
ntm
en
t re
min
de
rs
Pa
tie
nt
an
d c
are
r p
sy
ch
olo
gic
al
su
pp
ort
Die
tary
ad
vic
e
Ca
rer
ed
uc
atio
n
Te
ch
no
log
y
Se
lf-c
are
su
pp
ort
g
rou
ps
Ind
ivid
ua
l se
lf-c
are
s
up
po
rt
Wri
tte
n m
ater
ials
Ph
ys
ical
fu
nc
tio
nin
g
Illn
ess
kno
wle
dg
e
Ex
erc
ise
an
d d
iet
Pa
in
Tre
atm
en
t a
dh
ere
nce
De
pre
ssio
n a
nd
a
nx
iety
Sa
tisf
acti
on
Qu
alit
y o
f lif
e
He
alt
h s
erv
ice
us
e
Aadalen, 19981 ↔ ↔ ↑ Allen, 19992 Blue et al., 20016a; Stewart & Blue, 20016b
Boaden et al., 20057a; Sargent et al., 20077b; Gravelle et al., 20067c
↑d
↔ Boyd & Fisher, 19968 Brown et al., 200410a; Brown et al, 200710b
↔ ↔
↔ ↔ ↔ ↔ ↑
↔
Challis et al., 200211 Dorr et al., 200512 ↑ Enguidanos et al., 200313
↔ ↔ ↔
↔
Fitzgerald et al., 199414
a
↑b
Gagnon et al., 199915a; Schein et al., 200515b
↔ ↔ ↔ ↔
↔ ↔↑
Kemper, 198816a; Carcagno & Kemper, 1988 16b
↔ ↔ ↑c
↑ ↔

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 62
Leung et al., 2004 18 Lyon et al., 200619 Lynch et al., 2000 20 ↑
↑ = statistically significant improvement; ↓ statistically significant decrease; ↔ = no statistically significant change.
a Equipment only (occupational therapy); b Increased visits to general medical clinic – no difference in bed days; c Caregiver; d Qualitative information supporting improved psycho-social support for patients

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 63
Most studies gave few details of the process of the self-care support interventions. Consequently, the difficulty of relating elements of interventions to the outcomes made it difficult for conclusions regarding positive impact to be drawn.
Patient education
Patient education was a key component of case management in many studies (n16; 75%) and thus mentioned in three quarters of the 20 studies. Table 2.12 summarises the methods of providing patient education reported by the studies as well as showing which studies had any positive outcomes. The educational interventions were delivered in two ways, the majority by the case managers with the individual (66%), the others via groups. Four interventions either provided or referred patients to community-based support and education groups; these were usually disease specific 12,22a. Exercise groups were made available to patients in Challis and colleagues (2002) and Newcomer and colleagues (2004).
Patient education was mostly condition specific, which could lead to difficulties in producing patient education material for the full range of chronic conditions that their patients experienced26 Some projects devised their own educational material6 and some used a standard curriculum10a. Over half of the studies reported the use of written materials that were tailored to the individual patient. For example, a booklet providing information about heart failure, treatment, dietary advice, medication, contact details and planned visits, was devised for patients in one study6. Written information was often posted to patients on entry into the intervention and then followed up in discussion, either over the telephone, or in person, at a later date22a. Other media were used, for example, Pugh reports the use of a video in addition to printed materials23. Assessing patients’ capacity for learning was highlighted in many studies for example, tailoring the education program to match the individual patient10a.
No interventions used lay leaders. Case managers were formally trained as educators in a number of interventions, for example, two out of seven case managers were diabetes educators in the study reported by Dorr and colleagues12. The majority of the 15 demonstration projects reported by Brown and colleagues (2007) provided training for their case managers, particularly in using lay terminology to promote understanding and using curricula with patients10b.
The location and timing of education was found to be important. Some studies found that patients did not retain the education provided in a hospital setting1 and both patients and families appreciated when case managers spent time explaining and educating about the illness and treatment post discharge1. Several projects used guidelines to ensure patients were contacted post discharge and provided with information and advice14. Some projects also signed patients up to continuing information, for example, a quarterly newsletter for people with diabetes26. Education was also provided in relation to managing the health system and accessing other community services22a. Family and carer education was viewed as either being necessary when the patient did not respond to the educational intervention, or as a routine part of the case management intervention10a.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 64
Provider education
Provider education is designed to maximise professional understanding of the case management approach and encourage adherence to evidence-based practice guidelines. This is relevant to supporting self-care as guidelines ensure consistency for the patient and form part of patient education regarding both the processes of health services and the likely reaction to events6,10a,22a. Few interventions referred to provider education. One study described relevant agencies receiving education about the case management programme in order to facilitate referrals22a. Four of the demonstration projects reported by Brown and colleagues (2007) used provider education with the aim of improving practice10b. They compared treatment plans with evidence-based guidance and made recommendations to physicians. One programme additionally provided formal, incentivised education regarding treatment guidelines for physicians.
Exercise and dietary advice
Four interventions described the promotion of suitable exercise for patients 6,7a,10a,11. It was given most focus in an intervention for people with heart failure6. Four studies described providing dietary advice to patients6,7a,10a,14.
Medication and treatment management
Medication management was identified as a particular problem for patients, with greater adherence being a specific goal for some studies8 where it was expected that case managers providing information and education about medication and monitoring its use would promote adherence. Patient reminders were used to encourage attendance at routine appointments and follow up when a patient had not attended. These were used by seven studies and usually consisted of the case manager writing to, or telephoning a patient prior to the appointment14. Patients not attending appointments would be followed up and supported in attending for example, with transport or accompaniment22a. Patients were encouraged to monitor their symptoms6,7a and report warning signs, although Pugh and colleagues (2001) reported that some patients were reluctant to do this, fearing readmission to hospital23.
Patient and carer psychological support
A high proportion of studies described providing psychological support to the patient. This could be as part of the general process of therapeutic relationship building, seen as a crucial part of the case management process8; as part of the process of identifying needs24; or more focused on specific areas such as ascertaining the patients’ willingness to change behaviours and their wishes for future care. For example, one study5a focused on coping assistance (defined as supporting patients in problem solving and increasing mastery) and another reported20 on increasing self-reliance. Counselling and therapy were a more specific

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 65
extension of this, for example, addressing patients’ needs with regard to specific psychological issues such as grief15a.
Carer education
Carer education and family support was seen as an important factor in many interventions11. This entailed getting to know the patient’s family and supporting them to support the patient directly or to support the patient to self-care. Other family orientated interventions involved providing information and education to family and carers so as to improve the effectiveness of the care they directly provided to the patient. Patients and carers were found to value the development of this relationship and the related support in several interventions7b.
Technology and equipment
Three studies reported the use of technology or equipment to support self-care. One project reported the use of timers and medication management boxes to promote adherence22a. Brown and colleagues (2007) found that the demonstration site that used telemonitoring received the timeliest alerts to adverse events10b. However, some professionals reported that the patients were becoming dependent on these devices and attempted to promote other methods. Other equipment to promote greater independence in mobility and bathing was reported by Challis and colleagues (2002)11.
2.3.1.2 Impact of the interventions upon self-care related outcomes
The outcomes of the nurse case management interventions were far from conclusive. Just under three-quarters recorded at least one significant positive outcome. The studies were reviewed for outcomes similar to those reported in the UK literature (see section two). Nine studies reported positive outcomes which were relevant to improved self-care. However, little detail was given about these outcomes and their relationship with individual elements of the process of the case management interventions. Furthermore, interventions reporting positive outcomes did not have any common features. No studies reported self efficacy as an outcome measure, so this has been omitted from the table and replaced with satisfaction which was reported by several studies1,13,16a,18. As in the UK self-care literature (discussed in section two) the authors of several studies reported that length of follow-up may have been too short to detect significant outcomes 10b.
Only one study comprehensively reported outcomes in relation to self-management behaviours10b. It reported the findings of a number of case management and disease management programmes at a two-year follow-up. The demonstration programmes were all different, for example, some programmes were condition specific and others were generic. However, there were some common themes and approaches that allowed an overall evaluation to be carried out. The findings showed no significant effects of the interventions on self-care or adherence to treatment outcomes. Individual programmes showed some positive effects on self-care behaviours but no pattern could be detected. Just over half of the physicians

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 66
of patients included in the programme felt there was an overall improvement in patients’ self-management behaviours (51%). Individual demonstration programmes differed widely on these self-management outcomes; for example, one programme reported 83 per cent of physicians rating patients’ medication adherence as ‘very good or excellent’ compared with only 14 per cent from another programme. However, these perceived improvements did not translate into measured improvements in patient self-management behaviour.
Physical functioning (including pain)
Nine of the interventions measured functioning as an outcome but only one found any significant improvements. This may be a particularly difficult area to show improvement in due to the nature of the conditions experienced by the case managed patients. Similarly, three studies measured reported pain as an outcome but none found any significant improvements10b,15a,26.
Illness knowledge
Only one intervention reported illness knowledge as an outcome measure. In the 14 interventions reported by Brown and colleagues (2007), patient education was a focus of all but one of the case management programmes and its impact was measured through the patients’ self reports10b. Although significant numbers of patients reported having received health education, this did not translate into changed behaviours. It was suggested that patients who had received health education may have reported their health related activities more stringently, or may have had higher baseline levels to begin with.
Exercise and diet
Exercise and diet appear to be difficult areas to influence with no significant changes being detected. In Brown and colleagues (2007) physicians perceived that the case management programme had had a positive effect on 36 per cent of their patients’ diet but this was not supported by objective measures10b. Only one other study measured diet related outcome26 and found significantly improved weight monitoring but did not report any changes in actual diet. Brown and colleagues (2007) again report the perception of physicians of improvements in exercise habits, less positive than for diet with only 22 per cent feeling that the programme had impacted on this area of their patients’ lives10b. One other study measured exercise but reported no significant improvements26.
Treatment adherence
Three studies measured treatment adherence as an outcome10b,12,26 and two reported significant improvements12,26. The other found no significant differences10b.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 67
Psychological functioning (depression, anxiety, satisfaction and quality
of life)
Five studies reported anxiety and depression as outcomes and none found any significant changes1,10b,13,15a,22a. Satisfaction with services was found to be significantly improved in two of the four interventions that measured it1,13,15a,16a. One study found greater satisfaction expressed by patients1 and the other found no significant improvements in patients but improved carer satisfaction16a. The psycho-social benefits of case management were found to be greatly valued by patients in one study, although these findings were reported qualitatively7c. Quality of life changes were reported by two studies15a,16a, with one finding an increase16a and the other no change15a.
Health service use
Health service use was a key outcome for nearly all of the nurse case management interventions with all but four explicitly measuring it. Seven studies reported reduced rates of service usage2,6,8,11,18,19,20. However, only two of the studies were RCTs6,18 where alternative explanations, such as regression towards the mean, could be ruled out. Two studies saw increased service usage but the aim of one intervention was to identify unmet needs so this was indicative of success24. The other saw general medical appointments increase as a result of the intervention, although bed days did not significantly change14. The results of the Evercare demonstration study found no significant effect on rates of emergency admissions or emergency bed days7c.
Carer involvement
Carer involvement played a major role in many of the nurse case management interventions, due to the needs of the targeted patients, although the effects on carers were only measured by one study16a.
2.3.1.3 Exit from case management
A key part of the relationship between self-care and case management is the potential for a patient to move from case management into supported self-care. Few of the nurse case management studies discussed exit from case management. Those that did described the majority of exits as being through death or entry into residential care10b,18,22a,23. Only one study made reference to the possibility of patients’ health improving, so that case management was no longer appropriate7a. The original model had been one that described patients remaining in the service for life, albeit with the possibility of a much reduced minimum monitoring service if health improves. However, there were procedures for discharge once the patient’s needs were met, or they had chosen to leave. One site found that one-fifth of its patients were not suitable for long-term follow-up due to being judged as at low risk. These patients were discharged but could contact the service if they experienced any exacerbations of illness. Previous patients of the service were also flagged on emergency admissions systems so that follow-up and, if necessary, case

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 68
management could continue. In another site, patients who had improved were never discharged, but instead received a minimal monitoring service7a.
2.1.3.4 Methodological quality and detail on implementation of interventions
The methodological quality of the studies were all rated either ‘fair’ (n=9) or ‘good’ (n=9). As described in section one there was variability of detail provided regarding general implementation, which also applied specifically to self-care support. Similar to the UK self-care support studies, some interventions used standardised patient information for promotion of self-care that would facilitate replication.
Many of the outcome measures used by the studies did not specifically assess changes to self-care behaviour so there may have been improvements in self-care that were not explicitly measured or reported. For example, patient education was less of a focus in the nurse case management studies than the UK literature (reviewed in section one), so only one study measured increased knowledge10b. Additionally this review has focused on the quantitative outcomes and there have been other psycho-social benefits reported 7c,30a that can only be described qualitatively and cannot be captured adequately in summary tables.
2.3.2 Summary of self-care support within nurse case management interventions
Supporting self-care is clearly an important feature of nurse case management approaches; nearly three quarters of the studies reviewed in section one incorporated some elements of them. Four points are of particular note. Firstly, the most common activity was that of patient education. This tended to be delivered on an individual basis and was supported by some form of curriculum and written materials. The low use of groups may be due to the high level of needs typical of patients using case management which may prevent them from taking part in such activities.
Secondly, psychological support for both patients and their carers played a role in both assessing and providing support. This is both difficult to describe and measure but it appears that being able to develop a relationship with the case manager was seen as beneficial to both patients and carers.
Thirdly, medication and appointment management was not commonly reported although it is suspected that education around both medication and regular monitoring is commonly included in patient education. The lack of use of technology is similar to that found in the UK literature. Only two studies described the use of technology10b,22a and even then in one study the case managers were concerned that patients might become dependent on it10b.
Finally, as with the evidence reviewed in section one it is not possible to draw firm conclusions. The complexity and variation of the interventions and lack of description of their process and the relationship of process to outcome militate against this.
The case manager, as a key contact, is potentially in an ideal position to both deliver and refer patients on to self-care support. These studies show that it is

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 69
almost certainly already happening but what is not known is to what extent and what forms of support are being used.
2.4 Discussion
In attempting to answer the five key questions for this literature review, outlined in the introduction, we have encountered a number of problems consistent with the methodological challenges of synthesising such a wide range of research. These are highlighted in the following discussion along with our main findings and how the three reviews compare in terms of delivery and outcomes. It is worth noting that sections one and three and one of section two relate to the international literature and part two of section two is UK based. All literature was however restricted to the English language.
Nurse case management for people with long-term conditions is variably implemented. Although the overall methodological quality of studies reviewed in section one was mostly good, those providing methodologically sound process data relating to the case management intervention were in the minority. There was often insufficient detail for us to understand how the core tasks and components were operationalised and to judge the breadth, intensity and duration of intervention. Furthermore, although self-care support does appear to be a feature of many nurse case management interventions, this could have been under-reported due to the emphasis upon describing the whole nurse case management intervention. These variations in quality of reporting and the difficulties in collecting standardised information on each core task and self-care element make replicating or generalising from many of the studies difficult. They also require some caution to be exercised when interpreting the results of these studies.
These difficulties may partly be explained by the fact that case management, in the context of long-term conditions, is a complex intervention, with the role involving several components, making it difficult to establish with any precision which is the 'active ingredient' (Loveman et al., 2003). As section three demonstrates, this certainly presents difficulties in establishing the true impact of nurse case management. This absence of a clear understanding of case management is an obstacle to moving forward research and practice in this area. Each section of this review highlights the need for a shift in the emphasis to concretely specifying what and how case management services and self-care support are provided to people with long-term conditions, offering consistent and coherent implementation along with measuring what is actually being provided. Although most studies reviewed employed more than one case manager, few provided sufficient detail to be sure the extent to which the intervention was provided in a consistent way. In order to facilitate the replication of the same model or intervention in different studies, the measurement of implementation and processes needs to be at the centre of future research.
There is a limit to the generalisability of the generic self-care support literature findings to the case managed population. Patients eligible for case management interventions were likely to be older and have more complex needs (sections one and three) than those targeted in the UK self-care support interventions (section two, part two). However, many of the key elements of self-care support, for

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 70
example, patient education and psychological support were identified in the nurse case management interventions.
The focus of the self-care support interventions (section two, part two) was most commonly patient education, usually delivered in a group setting with psychological support a further important component. There was also a strong focus on the promotion of exercise, whereas this is much less a part of nurse case management (section three). Similarly, carer involvement is an important of nurse case management, whereas it plays a greatly reduced role in self-care support interventions. The main similarities lay with the focus on patient education and psychological support which featured in the majority of both the self-care support and nurse case management interventions. There were differences in the delivery of patient education, which again reflects the different populations. Within nurse case management interventions it tended to be less formalised and more individualised, delivered one-to-one in the home, and groups were less frequently used. No UK self-care initiatives involved explicit provider education and none significantly used any sort of technology. Medication and treatment management was more evident in the nurse case management interventions reflecting the needs of the patient group.
Previous reviews of the literature on self-care support (section two, part one) have shown that self-care support can have modest beneficial impacts for people with long-term conditions. The evidence shows that changes in psychological health outcomes were more likely than actual changes in behaviour, although the duration of these effects are unknown. The UK research evidence reviewed in section two, part two supports the findings of previous reviews, showing that most interventions indicate modest improvements in at least one self-care related outcome. Significant improvements tended to be in physical functioning, self efficacy and knowledge of illness. When the UK research evidence was compared to the nurse case management evidence, there were some notable differences in outcomes. Health service usage was measured by over a third of the self-care support studies and all but three of the nurse case management studies. Only two of the self-care support studies showed reductions in health service usage. The nurse case management interventions tended to have a greater degree of success here with just over a third of the studies involving self-care support showing a decrease in service use. However, only two of these studies were randomised controlled trials, where the reduction could be attributed to the effect of the intervention. A larger proportion of nurse case management studies had significant effects on treatment adherence which may be due to the comprehensive nature of the intervention. Not all benefits of self-care support or case management interventions may have been captured by the outcomes measured. Patients in self-care support groups reported the increased social support they gained from the intervention31 and case managed patients valued the relationship they developed with their case manager7b, which are both difficult effects to measure.
Government policy in England promotes self-care support for all people (Cm 6737, 2006). This includes those who are supported by case management for people with the most complex long-term conditions (DH, 2005b). This multi-faceted literature review has shown that when self-care is supported there are potential patient benefits. The evidence reviewed in section three along with a recent investigation in some primary care trusts in England, (DH, 2005e) suggests that this support

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 71
appears to already be happening in nurse case management interventions, although it may not be explicitly identified as such.
However, the role of self-care support within nurse case management has not been specifically explored and particularly within a UK NHS context. This lack of focus surrounding self-care support means it is difficult to tell from the existing literature whether different models of case management are related to more or less use of self-care support services. It is not yet known what types of self-care support are currently available to UK nurse case managers and the extent to which they are used as part of the case management process.
A further important area of enquiry is the nature of the relationship between self-care and exit from case management. Caseload size is to a large part contingent on the appropriate use of mechanisms to determine entry into case management (case finding and screening) and strategies for exiting the service. Furthermore the size of caseload, combined with the level of need of recipients, will to a large part determine the service they receive as well as the monitoring and review phases of the process. Exit from case management was not discussed by many of the interventions reviewed and few details were provided relating to caseload turnover and whether patients were able to leave the service due to improvements in their condition. The relationship between case management and self-care support services is likely to be crucial to the possibility of a transition between case management services and self-care and to the capacity of case management to continue functioning once caseloads are full.
2.5 Summary
This review has explored five questions relating to nurse case management and self-care support. The principal findings are summarised below in relation to these questions.
2.5.1 How is nurse case management for long-term conditions implemented?
Nurse case management for people with long-term conditions is variably implemented. Based on the studies reviewed in section one, there was often insufficient detail for us to understand how the core tasks and components were operationalised. Nurse case management was implemented by case managers undertaking key tasks such as assessment, care planning and implementation of the care plan. Some studies also reported a focus on monitoring and reviews. Implementation could also vary in terms of therapeutic interventions, illness management and care co-ordination, in addition to target client groups and available services. The variability between studies reflected different models of care, in addition to local implementation issues such as target client groups and the range of services at the disposal of the case manager.
2.5.2 How are self-care support interventions implemented?
The literature reviewed in section two (part two) showed that self-care interventions are most commonly delivered using patient education, consisting of a combination of written materials and teaching sessions. Psychological intervention

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 72
was an additional feature aiming to promote relaxation and alleviating anxiety and depression. Delivery can take a multi-disciplinary approach or can use trained volunteers with experiential knowledge and can be condition specific or general for example, the Expert Patient Programme.
2.5.3 What impact do self-care support interventions have for people with long-term conditions?
The findings of previous reviews section two (part one) showed modest evidence of benefit from self-care interventions. These findings were supported by the UK research evidence, section two (part two) showing that most interventions have modest improvements in at least one self-care related outcome. Improved outcomes tended to be in self efficacy, knowledge of illness and physical functioning. The use of groups may have unplanned benefits of providing informal social support and shared knowledge.
2.5.4 How is self-care supported within, or as a consequence of, case management interventions?
Although a feature of most studies reviewed in section three, self-care support within the nurse case management interventions tended to be less formalised, more individualised and delivered one-to-one in the home. The most common activity was that of patient education mostly delivered on an individual basis and supported by some form of curriculum. This education could also include medication and appointment management. Psychological support for both patients and their carers played an additional role in both assessing and providing support.
2.5.5 What impact does case management have upon self-care?
It is not possible to draw firm conclusions from the case management intervention studies reviewed in section three, as few self-care related outcomes were measured. Health service usage was measured by nearly all the nurse case management studies with just over a third involving self-care support showing a decrease in service use. A larger proportion of nurse case management studies had significant effects on treatment adherence which may be due to the comprehensive nature of the intervention.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 73
Chapter 3 Method This study was commissioned to explore the NHS and social care model for improving care for people with long-term conditions with a particular focus on the role of self-care support services. As noted in the introduction, it had three aims. First, to map current provision of NHS case management services in primary care for people with long-term conditions. Second, to classify approaches to case management implementation, focussing on integration of care between primary and secondary care and between health and social care. Third, to identify the extent and nature of self-care initiatives within this service and to investigate their links with entry to and exit from it. An application was made to the National Research Ethics Service for ethical review of the study and it received a favourable opinion on the 7th September 2007 from the Cambridgeshire 4 Research Ethics Committee (Number: 07H0305/59).
The collection and analysis of the data are described in this chapter. Both qualitative and quantitative approaches were used and the data collection comprised four elements:
A survey of case management for people with long-term conditions and self-care services.
A comparison of this data with previous studies of care management undertaken by the Personal Social Services Research Unit.
Case studies of long-term conditions services in four primary care trusts.
Service user perspectives on the relative merits of different approaches to case management and self-care services
This work was informed by the three part literature review reported by Chapter two of which a detailed methodology for each part is described alongside the findings.
In developing the methodology two concepts central to the case management literature, integration and differentiation, were important. English policy guidance envisaged that case management for people with long-term conditions would be provided within in an integrated care system, spanning primary and secondary healthcare and local authority social care services. Within this model it was envisaged that there would be a range of services, providing the opportunity to deliver different levels of care to patients a variety of needs. In the context of case management this constitutes a differentiated approach.
3.1 Survey of case management for people with long-term conditions and self-care services
3.1.1 Questionnaire development
A questionnaire was developed by the research team to reflect key issues relating to case management and self-care for people with long-term conditions. Its development was informed by: the relevant literature; existing survey tools used in earlier PSSRU projects; and reviews of variations in care management

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 74
arrangements (Challis and colleagues, 2009; 2004; Xie et al., 2008a; Weiner et al., 2002; 1998). The questionnaire was piloted in ten primary care trusts and revised by the research team, including all the applicants. Particular attention was paid to its design and length to minimise respondent burden. The full questionnaire contained fifty questions and is included in Appendix 5.
The broad domains covered by the questionnaire were:
Service background
Case management objectives
Links with other services
Self-care support services
Staff mix and tasks
Process of case management (patient identification; assessment; care planning; monitoring and review)
Information systems
Service development
3.1.2 Data collection
A database of contacts for primary care trust community nursing services was compiled. A paper version of the survey was sent to Directors of Nursing in each of the 152 primary care trusts in October 2007. Respondents were requested to forward it to an appropriate person with lead responsibility for case management services in the primary care trust for them to complete and return to the Personal Social Services Research Unit. An electronic version and a web based-version were also available on request. A second mail out of the survey to non-respondents was made in February 2008 and telephone contacts began in March 2008. To address the initial low response rate, a shortened version of the questionnaire more suitable for use in a telephone interview was developed. It mainly comprised the questions necessary for the classification of services and these are marked with an asterisk in Appendix 5. Data collection continued until November 2008.
3.1.3 Data management and analysis
Data were analysed using SPSS for Windows (version 14). Categorical variables were defined for entry of the data into the database. For the open-ended questions, coding frames were prepared from the responses provided.
3.2 Comparison of case/care management in different settings
3.2.1 National surveys
This involved a comparison of some of the findings of the primary care trust case management survey with two national surveys of local authority care management services for older people and for younger adults with a physical disability previously undertaken by the PSSRU at Manchester University (Weiner et al., 2002; Xie et al.,
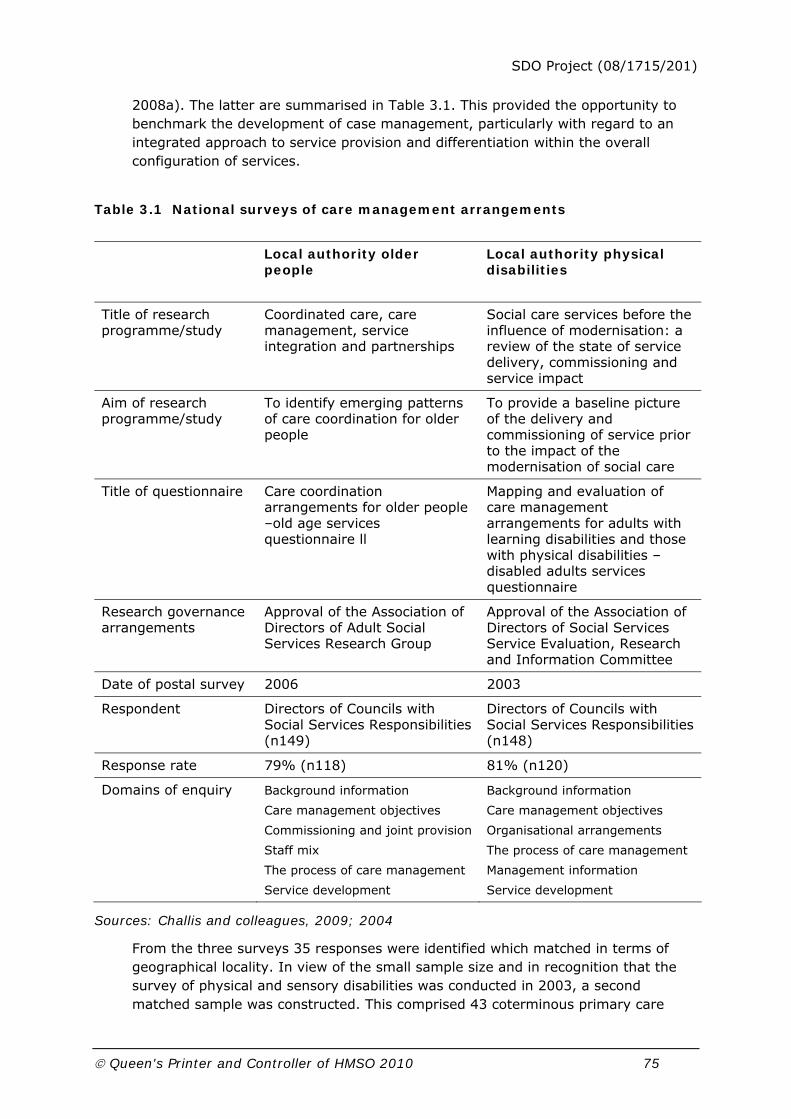
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 75
2008a). The latter are summarised in Table 3.1. This provided the opportunity to benchmark the development of case management, particularly with regard to an integrated approach to service provision and differentiation within the overall configuration of services.
Table 3.1 National surveys of care management arrangements
Local authority older people
Local authority physical disabilities
Title of research programme/study
Coordinated care, care management, service integration and partnerships
Social care services before the influence of modernisation: a review of the state of service delivery, commissioning and service impact
Aim of research programme/study
To identify emerging patterns of care coordination for older people
To provide a baseline picture of the delivery and commissioning of service prior to the impact of the modernisation of social care
Title of questionnaire Care coordination arrangements for older people –old age services questionnaire ll
Mapping and evaluation of care management arrangements for adults with learning disabilities and those with physical disabilities – disabled adults services questionnaire
Research governance arrangements
Approval of the Association of Directors of Adult Social Services Research Group
Approval of the Association of Directors of Social Services Service Evaluation, Research and Information Committee
Date of postal survey 2006 2003
Respondent Directors of Councils with Social Services Responsibilities (n149)
Directors of Councils with Social Services Responsibilities (n148)
Response rate 79% (n118) 81% (n120)
Domains of enquiry Background information
Care management objectives
Commissioning and joint provision
Staff mix
The process of care management
Service development
Background information
Care management objectives
Organisational arrangements
The process of care management
Management information
Service development
Sources: Challis and colleagues, 2009; 2004
From the three surveys 35 responses were identified which matched in terms of geographical locality. In view of the small sample size and in recognition that the survey of physical and sensory disabilities was conducted in 2003, a second matched sample was constructed. This comprised 43 coterminous primary care

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 76
trust case management services and local authority old age care management services. The size of both samples is a reflection of the response rates to the three surveys and the lack of coterminosity between primary care trust and local authority boundaries at the time the data was collected.
3.2.2 Data analysis
Each of the three surveys had two sections in common which explored the goals and service objectives of care/case management. More detailed information relating to service characteristics and information systems was available from two of the surveys: local authority care management arrangements for older people and PCT case management arrangements for people with long-term conditions. These domains of enquiry are summarised in Table 3.2. Data from the three surveys were analysed using StatXact (Mehta and Patel, 1998) and exact probability Chi squared tests were used to detect significant differences between groups. When comparing the two surveys, data were analysed using SPSS for Windows (version 14) and Fishers Exact test (2 sided p value) was used to detect differences between the two groups. The unit of analysis was local authority or primary care trust.
Table 3.2 Matched datasets: domains of enquiry
Domains of enquiry Local authority older people (n43)
Primary care Trust long-term conditions (n43)
Local authority physical disabilities (n35)
Goals
Service arrangements
Service characteristics
Information systems
Two summary measures were developed, the first an indicator of integration and the second an indicator of differentiation. These utilised previous work examining these features in services for older people (Challis and colleagues, 2006); including old age mental health services (Reilly et al., 2003) and were developed using a subset of the variables from the four domains of enquiry in Table 3.2. Each variable was given the value of 1 or 0 depending upon whether the attribute was present or absent for the responding local authority or trust. This gave a possible score between 0 and 6, where a higher score represented a higher degree of integration or differentiation.
3.3 Stage two: case studies
3.3.1 Site selection
Data from the first 50 respondents of the survey of case management arrangements were used to categorise primary care trusts across four domains.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 77
These were identified a priori, informed by previous literature (Challis and colleagues, 2001; 2007), the research questions and the data available. Each was judged to be within either of two overarching categories: organisation and practice. The four domains were:
Self-care support (Organisation)
Integration (Organisation)
The process of case management (Practice)3
Differentiation within case management arrangements(Practice)4
For each of these, a new composite variable was generated to provide a primary indicator score for the domain. These are summarised in Table 3.3 below. Another variable was identified to validate it. When each pair of dichotomous variables (i.e. the indicator and the validating variable) were cross tabulated using Kappa Coefficients, there was a significant association (at the five per cent level of significance). This confirmed the utility of the variables in the a priori classification.
Table 3 3 Criteria of classification
Description Measures Score
Range of self-care support services in the locality and links between them and the case management service
Types of local services (maximum of 6) plus directory of local services (1) links with case management service (1) managerial involvement in commissioning self-care services (1) lead officer for self-care in PCT (1)
High: 7 plus Low: 6 or less
Extent of integration with other NHS services and local authority adult social care services
Links with: local authority social care services(1) intermediate care services (2) and other primary care services (3)
High: 4 plus Low: 3 or less
Number of case management tasks in addition to assessment of need undertaken by practitioners within the service
Tasks (maximum of 7): financial assessment, care planning, service allocation, implementation of care plan, budget management, monitoring, review
High: 6 or 7 Low: 5 or less
Differentiation within the case management service permitting a different level of service to those with the greatest level of need
Caseload size less than 30 (1) intensity of involvement as a criteria of case allocation (1) less than 50% of team caseload visited weekly (1)
High: 2 or 3 Low: 1 or 0
3 The aim of this domain was to capture the level of activity in respect of the core task of case management.
4 Differentiation was defined as consisting of four defining features: variability in response to need in terms of
level of staff and resource provided; some staff with small caseloads; the presence of intensive care
management; the provision of care management to a wider group of clients (Hughes et al., 2002; after Challis and
colleagues, 1998)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 78
Table 3.4 shows the distribution of the primary care trusts in each of the four domains. The assumption was that most of the 15 services in the bottom right cell would have only recently introduced NHS case management; they were additionally judged as having little support for self-care and did not score for two key aspects of case management. These were disregarded, as Challis and colleagues, (2007) reported such sites in a similar categorisation often migrated to other cells as the service developed. All cells containing less than five per cent of responses (<3) were discarded. Since within this research study there was a focus on self-care, those cells not showing evidence of this (on the basis of survey responses) were also discarded.
Table 3.4 Classification of primary care trusts (n=50)
Case management tasks Integration Self-care support Differentiation
Yes No
High 2 2 High
Low 3 3
High 2 4
High
Low Low 0 5
High 2 4 High
Low 0 4
High 2 2
Low
Low
Low 0 15
This process provided four different approaches to case management, illustrated by Table 3.5. A hierarchy of preferred primary care trusts in which to complete the fieldwork was created for each of these approaches. Selection was based on a number of factors: overall scores for the four key domains; geography (location and authority type); and a willingness and ability of the service to participate in the research. Managers in the four identified sites were contacted to ascertain whether they were suitable and willing to take part in the case study stage of the research. Each agreed and subsequently successful applications were made to their primary care trust research and development departments for authorisation to carry out the research.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 79
Table 3.5 Approaches to case management in selected sites
Sites Measures
1 2 3 4
Extent of integration with other NHS services and local authority adult social care services
High High Low Low
Range of self-care support services in the locality and links between them and case management service
High High High High
Differentiation within the case management service permitting a different level of service to those with the greatest level of need
Low Low High Low
Number of case management tasks in addition to assessment of need undertaken by practitioners within the service
High Low Low Low
3.3.2 Data collection
In this phase of the study the extent and nature of self-care initiatives and the features of case management, in particular the links with other services, staff mix and tasks, information systems and the process of case management were explored. Two perspectives were sought on the case management service: that of the service manager who was anticipated to have more strategic involvement and that of the case managers, with experience of routine patient contacts. An initial visit was arranged to interview the service manager. The second meeting comprised a focus group of practitioners. However, at one site a separate interview with the service manager was not possible and this person participated in the focus group. Names and addresses were only retained if the participant wished to be kept informed as to the findings of the research, in which case they gave consent for their details to be kept on a specific mailing list to be destroyed after the findings have been disseminated.
For each manager a semi-structured interview schedule was prepared reflecting core elements common to all and service specific avenues of enquiry. There were three components: a summary of the survey responses to be validated by the interview; questions arising from these survey responses5 and key features of case management services derived from the literature6. The composition of each focus group was determined by the service manager in consultation with the researcher. Case managers were invited to participate together with other key staff, for example, self-care support project workers, if appropriate. The focus group interview schedules were again informed by the survey findings and the literature review, as well as the earlier interview with the service manager7.
5 See Appendix 6 for interview schedule.
6 See Appendix 7 for framework.
7 See Appendix 8 for focus groups schedules.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 80
3.3.3 Data management and analysis
The interviews with managers and focus groups were carried out between June and November 2008 and were between 60 and 90 minutes in length. Data generated by the interviews was anonymised and stored on a password protected university computer. Interviews were transcribed verbatim and analysed using Atlas ti. (version 4.2). The same researcher carried out the interviews and the analysis, allowing continuity between the stages of the research process (Bowling, 1997).
Thematic analysis, a method for identifying, analysing and reporting pattern (themes) within data that provides an organisation of data, followed by an interpretation was used. This has been described as a foundational method for qualitative analysis as it may also be used as a tool within other forms of qualitative analysis, for example, grounded theory analysis. It can however, as utilised here, be a method in its own right (Braun and Clarke, 2006). This approach has been adapted from Braun and Clarke (2006) and influenced by Fereday and Muir-Cochrane (2006), it combines a data driven inductive analysis (Boyatzis, 1998) with a predetermined deductive approach stemming from an a priori template of codes (Crabtree and Miller, 1999) determined by the survey, which in turn, were determined by the literature, to interpret the data (Fereday and Muir-Cochrane, 2006).
The analysis was dependent on the development of first codes and then themes. After familiarisation with the data, some codes were created in vivo using the actual word or phrase the interviewee had used; others were created a priori, influenced by key issues that had arisen from the literature review and the researcher’s recollections of the actual interview process. The next stage was to unify the data into several themes to enable the findings of the research to be described in a cohesive manner. The domains of the questionnaire detailed in 3.1 were used initially. These were further refined with sub-themes being identified in the data. After each transcript had been coded and reviewed some codes had little associated text and were incorporated into a similar one. Others that contained unwieldy amounts of text were divided. Next themes from either within or across the case studies were described. Illustrations were taken from the text to support them and to ensure that the interpretation remained connected to the words of the interviewees.
3.4 Service user consultation
Utilising findings from the survey of case management arrangements, the purpose of this consultation was to ascertain views on types of self-care support available and priorities for case management services.
3.4.1 Identification of user groups
Four consultations were undertaken in the North West of England. Three were longstanding groups accessed through existing contacts with the research team. Access to two of these was facilitated by local Age Concern organisations and one via LMCP Care Link to a group primarily providing support to carers within the Asian community. The fourth group was specially convened for this purpose by the

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 81
service user advisor to the Personal Social Services Research Unit and consultant to this study.
3.4.2 Data collection
Three researchers facilitated each group. All participants were provided both verbal and written information about the research and given the opportunity to ask questions before being asked to give their written consent to participating in the consultation.
The consultation consisted of two parts: completion of a brief questionnaire and a discussion. Participants were asked which long-term condition(s) they were experiencing; to select from a list self-care support services which would help them manage their long-term condition(s); and to indicate which of four priorities a case management service should have8. The ensuing discussion was guided by issues raised during the completion of this brief questionnaire. It was digitally recorded for transcription in three of the groups, one group did not consent to this and written notes were taken.
3.4.3 Data management and analysis
The consultation responses were analysed using SPSS for Windows (version 14) for the quantitative data and Atlas ti. (version 4.2) for the qualitative data. As noted in the introduction, the responses were used to inform the discussion of the broader research findings in Chapter 7
3.5 Summary
A mixed method approach was employed in this study informed by the findings from the literature review reported in Chapter two. First, a national survey of case management for people long-term conditions was undertaken. This is reported in Chapter four. Second, findings from this survey were compared with two undertaken in respect of local authority care management arrangements. The results of this constitute Chapter five of this report. Third, case studies of case management services for people long-term conditions were undertaken were undertaken in four sites. These are reported in Chapter six. Observations from the service user consultations are included in Chapter seven.
8 See Appendix 9 for service user consultation questionnaire.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 82
Chapter 4 Survey One hundred and fifty two questionnaires were distributed to primary care trusts in England. Fifty-six full questionnaires were returned (37%). In addition to this, 35 responses to a shortened version of the questionnaire were collected by telephone. Therefore, for all questions there is a sample of at least 56 responses and for certain questions there is a sample of 91 (60%). The number of primary care trusts included for each question is specified in the table. This section will describe these findings describing the nature and organisation of case management arrangements9. The data is reported using the following headings: background; case management objectives; links with other services; self-care support services; staff mix and tasks; process of active case management (patient identification; assessment; care planning, monitoring and review); and service development.
4.1 Background
All respondents were asked to provide information regarding the demographic characteristics of their trust and also the ‘roll out’ of their case management service. As indicated in Table 4.1, over three quarters of the primary care trusts had between 30-90 general practitioner practices in their jurisdiction. The average (median) number of GP practices was 52. Only five primary care trusts had more than 91 practices within their area. Primary care trusts were also asked to estimate the size of the resident population they served. These ranged from 51,300 to 760,000. The majority had a resident population somewhere between 100,000 and 300,000. Almost two thirds routinely negotiated with only one local authority suggesting catchment areas for primary care trusts were aligned closely to the boundaries of their local authority. However, several (5) needed to negotiate on a regular basis with at least five different local authorities.
Table 4.2 reveals that about half of the primary care trusts reported that their current case management service was based on a previous initiative. Several specific case management models such as Evercare, Castlefields, Unicare and the European Prototype for Integrated Care) were reported in this context.
There was a great deal of variation (over 6 years) between when the first patient was accepted into the case management service in the primary care trusts. The Public Service Agreement target stated that from 2005 vulnerable people at risk would be offered a personalised care plan (DH, 2004c). As can be seen in Table 4.3, the majority of primary care trusts began accepting patients into their case management service during and after this date.
9 The terms case management and active case management (ACM) are used interchangeably throughout the
questionnaire to reflect local terminology.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 83
Table 4.1 Characteristics of primary care trusts (n=91)
n %
Number of GP practices Up to 30 31-60 61-90 91+ Size of resident population Up to 100,000 100,001 - 300,000 300,001 - 500,000 500,001 - 700,000 700,001 + Number of local authorities routinely negotiated with 0 1 2 3 4 5+
14 42 22 5 1 48 26 5 3 1 55 14 8 4 5
17 51 26 6 1 58 29 5 3 1 63 16 9 5 6
Sources: Question 1: How many GP practices are within your primary care trust?; Question 2: What is the size of the resident population served by your primary care trust?; Question 4: How many local authorities does your active case management service routinely negotiate with?
Table 4.2 Derived from previous initiative (n=91)
n %
Yes No
45 46
51 49
Source: Question 5: Is your current ACM service(s) based on a previous initiative(s)?
Table 4.3 Date operational (n=91)
n %
Pre 2005 2005 and later
17 74
19 67

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 84
Source: Question 6: On what date was the first patient accepted into the ACM service?
4.2 Case management objectives
There was a great deal of similarity between the objectives of the case management services. All respondents to the questionnaire reported that their aim was to increase the independence and improve the health of people with long-term conditions. Nearly all had the further objectives of improving care co-ordination; improving quality of life and reducing preventable hospitalisation. As can be seen in Table 4.4, fewer reported the use of case management services to improve accountability and prevent unnecessary residential and nursing home care.
Table 4.4 Goals of case management service (n=56)
n %
To increase the independence of people with long-term conditions To improve the health of people with long-term conditions To improve the extent and scope of services To improve the coordination of care to people living in the community To improve the quality of life of people with long-term conditions To divert people away from inappropriate hospitalisation To promote self-care support for people with long-term conditions To arrange more speedy and effective hospital discharge To provide more intensive long-term support in the community To reduce hospital length of stay To assist in the rehabilitation of people with long- term conditions To divert people from inappropriate residential and nursing home care To achieve improved accountability
56 56 55 55 55 55 53 52 50 42 40 29 24
100 100 98 98 98 98 95 93 89 75 71 52 43
Source: Question 7: Which of these statements describe the goals of your ACM service for people with long-term conditions?
Nearly all respondents reported that their case management service was a way of providing long-term support and coordinated care (see Table 4.5), and a means of assessing needs and implementing care plans. Evidence of discrimination as to which patients were supported by case management was evident with only one third of respondents stating that this was a service provided to a majority of patients.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 85
Table 4.5 Case management service arrangements (n=56)
n %
A means of providing long-term support and coordinated care An activity by which needs are assessed and care plans implemented An activity by which people with complex needs receive intensive help different in nature and scope to other patients A response to complex needs involving multiple services A specific job undertaken by designated members of staff who are called case managers A means of promoting the development of new forms and styles of service response An activity involving the coordination, delivery and monitoring of services to such a degree of complexity that caseloads are, as a consequence, small A single member of staff responsible for assessment, care planning, monitoring and review tasks for a particular patient A way of categorising or describing the arrangements through which people coming to the service are assessed and a response made to their needs A response provided only to a limited number of these patients A response provided to the majority of these patients
55 53 47 43 37 36 35 32 29 20 19
98 95 84 77 66 64 63 57 52 36 34
Source: Question 8: Which of these statements describe your department’s ACM service arrangements for people with long-term conditions?
Table 4.6 shows that in three quarters of primary care trusts, case management services were based on a geographical locality model. Some primary care trusts used different models to deliver their service.
Table 4.6 Service delivery arrangements (n=56)
n %
A geographical locality based model (pan GP practice) A GP practice population model Integrated health and social care teams Disease group based service/s Other arrangement
42 24 14 16 5
75 43 25 29 9
Source: Question 9: Which of the following best describes how ACM for people with long-term conditions is primarily being delivered in your primary care trust?
4.3 Links with other services
Fifty two per cent (n=29) of respondents reported formal agreements with the local authorities. Table 4.7 shows that over one third of these agreements were concerned with how active case managers accessed social care resources.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 86
Table 4.7 Agreements with local authorities (n=56)
n %
How active case managers access social care service resources Assessment tools for entry into ACM Eligibility criteria for ACM Respective target populations for ACM and care management in social care Other
21 18 16 11 1
38 32 29 20 2
Source: Question10b: If yes, is there an agreement with social care services partners over:
As can be seen in Table 4.8 formal agreements within health services were more widespread than those with local authorities with over four fifths of the primary care trusts having agreements with community nursing services. The most frequent agreements with acute services were with specialist disease nursing. Three quarters of the primary care trusts had agreements with intermediate care schemes to prevent hospital admission. There were very few agreements with old age psychiatry and hospital pharmacy services. No detail was given as to the ‘other’ category.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 87
Table 4.8 Agreements with health care providers
n %
Acute/Foundation trusts (n=56) Specialist disease nursing Accident and emergency Geriatric medicine General medicine Cardiology Old age psychiatry Hospital pharmacy Intermediate care services (n=91) Schemes to prevent hospital admission Schemes to facilitate early discharge from hospital Ambulance trust (n=56) Emergency hospital admissions Primary care services (n=91) Community nursing services Community physiotherapy services Community pharmacy services Other
30 22 18 16 14 6 3 76 62 12 80 50 41 6
54 39 32 29 25 11 5 83 68 21 88 55 45 11
Source: Question 11: Please indicate with which of the following services your ACM service has developed a formal agreement.
Just under a third of the primary care trusts reported their case management service having dedicated physician sessions (Table 4.9). Of those primary care trusts that had these and provided detail the most frequently reported was a geriatrician (35%; 6/17).
Table 4.9 Physician sessions (n=56)
n %
Yes No
17 39
30 60
Source: Question: 12a: Do you have any dedicated specialist physician sessions to support ACM?
Table 4.10 shows that nearly all the case management services had links with an End of Life programme, with nearly half specifying the use of two protocols: the Liverpool Care Pathway or Gold Standard.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 88
Table 4.10 Links with End of Life programme (n=56)
n %
Yes No
50 6
89 11
Source: Question 13a: Does your ACM service have any links with an End of Life Care Programme initiative in your area?
Thirty per cent of case management services reported specific out of hours provision for their patients (Table 4.11). Of those that provided any details, the majority said this took the form of an alert or flagging system that informed the case management service if a patient had requested emergency support.
Table 4.11 Out of hours arrangements (n=56)
n %
Yes No
17 39
30 60
Source: Question 14a: Are there specific arrangements for ACM patients with an emergency outside of normal working hours? Yes, specific arrangements; No, standard primary care arrangements
Respondents were asked to indicate whether their service had formal arrangements for sharing information about individual patients with partner organisations. Table 4.12 shows that over two thirds of primary care trusts had these for sharing documents within the Single Assessment Process (DH, 2005c) with local authorities. A slightly smaller proportion had similar arrangements with intermediate care services. The exchange of written information between the case management service and partner organisations was reported by over half the respondents. A fifth used single case files as a way of sharing information between agencies although more reported the sharing of information by means of patient held records.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 89
Table 4.12 Information sharing arrangements (n=91)
Acute/ Foundation NHS trusts
Local authority
Intermediate care services
n % n % n %
Joint access to computerised client record systems Case managers have access to agency patient records to extract and import information Multidisciplinary locality meetings Via a designated person (e.g. a nurse working in local authority social care services) Shared assessment documents within the Single Assessment Process Shared assessment documents outside the Single Assessment Process Shared review documents Single case file Exchange of written information Patient-held records Disease registers GP Disease registers
17 21 30 18 37 18 11 9 50 35 16 0
19 24 34 20 42 20 12 10 56 39 18 0
19 15 37 23 60 22 20 12 53 40 5 1
21 16 42 26 67 25 22 13 60 45 6 1
31 23 39 21 54 28 23 18 51 51 11 0
35 24 44 24 61 31 26 20 57 57 12 0
Source: Question 15: Does your ACM service have formal arrangements for sharing information about individual patients with partner organisations?
4.4 Self-care support services
Just under half of the primary care trusts had a designated lead for their self-care support services and a third had been involved in the development of the strategy for commissioning of such services (Table 4.13).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 90
Table 4.13 Development of self-care support services (n=91)
n %
Designated lead for self-care support services Yes No Has case management lead been involved in the development of self-care support services? Yes No
40 51 34 57
45 55 38 62
Source: Question 16: Does your primary care trust have a designated lead for self-care support services?
Source: Question 17: Have you, as ACM lead, been involved in the development of the commissioning strategy for self-care support services in your primary care trust?
All the respondents were asked about any formal links between the case management service and voluntary organisations which support self-care for patients with long-term conditions (Table 4.14). Over half of the primary care trusts had links. Those respondents who completed the full questionnaire were asked to specify with which organisations they had links and Age Concern or a locally developed organisation were the most commonly reported. There were also links with disease specific organisations such as Diabetes UK and Breathe Easy (support for respiratory problems). Some services also reported links with Crossroads carers support services.
Table 4.14 Links with voluntary organisations (n=91)
n %
Yes No
50 41
57 43
Source: Question 18a: Does your ACM service have any formal links with voluntary organisations specifically designed to support self-care for patients with long-term conditions?
Table 4.15 shows that a high proportion of primary care trusts had self-care support services available. The most frequently reported was generic self-care support training with 85 per cent of respondents reporting that as available in their primary care trust. That was closely followed by condition specific groups (83%) and accessible advice and information (82%). Around two thirds of respondents reported self help groups (67%), technology (64%) and informal therapeutic support (60%). The least reported service was alternative therapies available in less than a quarter of primary care trusts (24%).
Less than half of the respondents reported that case managed patients frequently used self-care support services. The service reported as being most frequently used

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 91
by case managed patients was condition specific self-care support training (47%), such as a group for people with diabetes. This was followed by using accessible patient information leaflets (42%). Under a third reported frequent use of informal therapeutic support (31%), generic self-care support (31%), self help groups (30%) and technology (28%). Only eleven percent of case managed patients were thought to frequently use alternative therapies.
Nearly three quarters (74%) of respondents reported that alternative therapies were never used by case managed patients. About two fifths indicated that informal therapeutic support (45%), self help groups (42%) and technology (40%) were not used. Just under a third of respondents reported that generic self-care support services were never used (30%) About a quarter thought that accessible advice (26%) and condition specific self-care support (24%) were never used.
Table 4.15 Self-care support services - availability and use (n=91)
Frequency of use by case managed patients
Self-care support services Funded by primary care trust Frequently Sometimes Never
n % n % n % n %
Informal therapeutic intervention e.g. during contact with professional Accessible advice and information e.g. patient information booklets Technology and equipment to promote self-care e.g. home monitoring equipment Self-care support training (generic) e.g. Expert Patient Programme Self-care support training (condition specific) e.g. diabetes Self help groups e.g. arthritis support group Alternative therapies e.g. acupuncture
54 74 58 77 75 61 22
60 82 64 85 83 67 24
27 37 25 27 41 26 9
31 42 28 31 47 30 11
21 28 28 35 26 25 13
24 32 32 40 30 28 15
39 23 35 26 21 37 63
45 26 40 30 24 42 74
Source: Question 19: Please tell us whether your primary care trust funds or provides any of the following self-care support services and estimate their frequency of use by case managed patients?
For each of the services respondents indicated were provided by their primary care trust for case managed patients, they were asked to specify which long-term conditions they were targeted towards (n=91). As can be seen in Figure 4.1 the majority of self-care support services were targeted towards diabetes (n=333),

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 92
chronic obstructive pulmonary disease (n=323) and coronary heart disease (n=264).
Figure 4.1 Number of self-care support services provided by condition (n=637)
Source: Question 20: Following on from your previous answer, please indicate where self-care support services are currently operating in your primary care trust/locality for patients in receipt of ACM in each disease category
Table 4.16 explores the use of these services by type of service and condition. The most frequently provided service for all conditions except coronary heart disease was accessible advice and information. For this condition the most frequently reported self-care support service was technology and equipment, with nearly three quarters of primary care trusts providing this. Informal therapeutic support was the next most reported service for coronary heart disease followed by advice and information. Just over four fifths of primary care trusts provided informal therapeutic support and over half provided condition specific self-care support for chronic obstructive pulmonary disease and a similar number reported patients with chronic obstructive pulmonary disease using generic self-care support services. Both generic and condition specific training groups were used by over three fifths of patients with diabetes. Over half of primary care trusts had self help groups for diabetes support and informal therapeutic support. Less than half of all primary care trusts reported services for the remaining conditions (multiple conditions; asthma; hypertension; stroke and transient ischaemic attack; musculoskeletal and other) the most reported apart from advice and information was informal therapeutic interventions and generic self-care support.
0
50
100
150
200
250
300
350
CHD
COPD
Diabe
tes
Mul
tiple
con
ditio
ns
Asthm
a
Hyper
tens
ion
Stroke
Mus
culo
-Ske
letal
Oth
er
Nu
mb
er o
f se
rvic
es

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 93
Table 4.16 Type of self-care support services by condition (n=91)
Self-care support service
Disease category
Informal therapeutic intervention
Accessible advice and information
Technology and equipment to promote self-care
Self-care support training (generic)
Self-care support training (condition specific)
Self help groups
Alternative therapies
n % n % n % n % n % n % n %
Coronary heart disease
55 62 46 52 66 74 32 36 41 46 42 47 6 7
Chronic obstructive pulmonary disease
54 61 73 83 44 49 49 55 55 62 42 47 6 7
Diabetes 51 57 73 82 40 45 54 61 60 67 50 56 5 6
Multiple conditions 31 35 42 47 21 24 32 36 19 21 17 19 3 3
Asthma 40 45 54 59 21 23 34 37 20 22 21 23 2 2
Hypertension 31 35 48 54 19 21 25 28 9 10 7 8 2 2
Stroke and transient ischaemic attack
32 36 53 60 17 19 31 35 21 24 30 34 3 3
Musculoskeletal 37 42 52 58 16 18 32 36 22 25 16 18 7 8
Other 11 12 13 14 10 11 17 19 11 12 8 9 1 1
Source: Question 20: Following on from your previous answer, please indicate where self-care support services are currently operating in your primary care trust/locality for patients in receipt of ACM in each disease category

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 94
Respondents were asked to estimate the proportion of patients on the case management service caseload who were currently using the self-care support services available to them. Nearly one third (31%) of respondents found it difficult to estimate this, perhaps indicating that it is not widely known how many case managed patients are engaged in self-care support services, or that the definition of self-care is unclear. Of those that were able to answer this question the majority of primary care trusts felt that fewer than 20 per cent of the caseload were using such services and only three services estimated over 60 per cent of patients were doing so (Figure 4.2).
Figure 4.2 Proportion of patients using self-care support services (n=91)
Source: Question 21: What proportion of the active case management caseload would you estimate are currently using self-care support services?
Table 4.17 shows that two thirds of primary care trusts did not have a directory of local services of self-care support available to case managers. However, a third of respondents reported that in their primary care trust there was a directory of local self-care services available for case managers to refer to and a further third stated that such a directory was being developed.
0
10
20
30
40
50
60
0 1 to 20 21 to 40 41 to 60 61 to 80 81 to 100
Percentage of patients
Per
cen
tag
e o
f P
CT
s
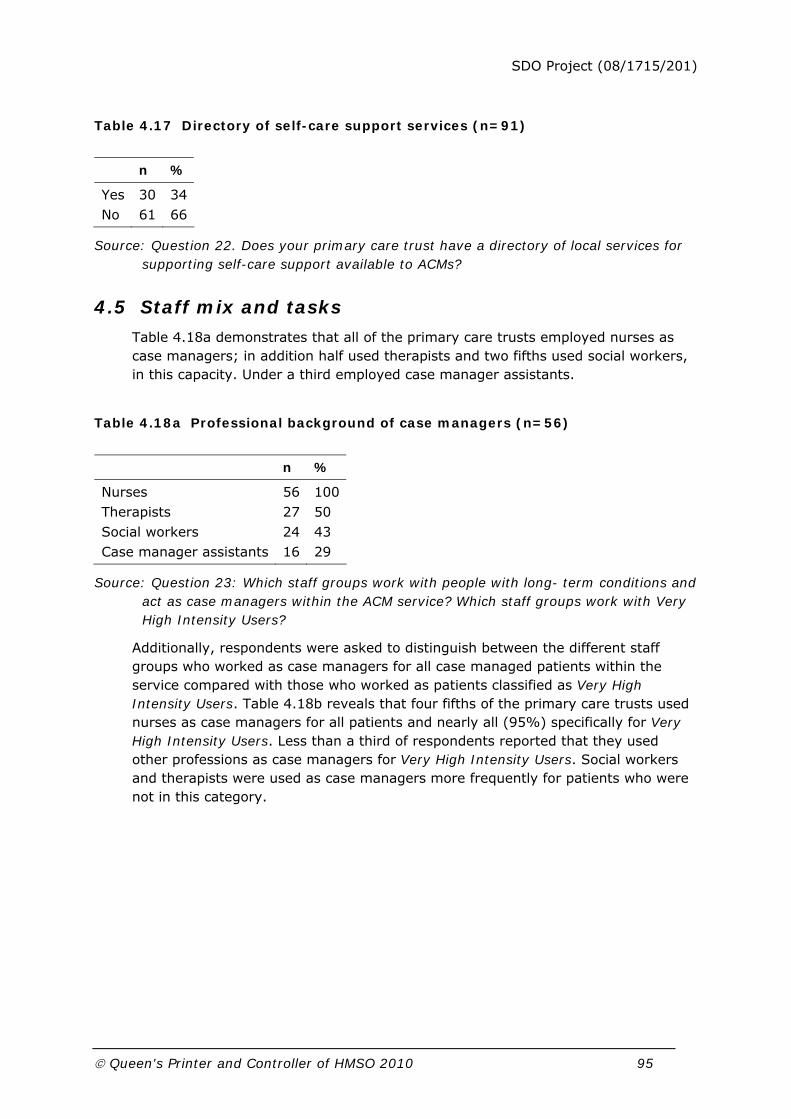
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 95
Table 4.17 Directory of self-care support services (n=91)
n %
Yes No
30 61
34 66
Source: Question 22. Does your primary care trust have a directory of local services for supporting self-care support available to ACMs?
4.5 Staff mix and tasks
Table 4.18a demonstrates that all of the primary care trusts employed nurses as case managers; in addition half used therapists and two fifths used social workers, in this capacity. Under a third employed case manager assistants.
Table 4.18a Professional background of case managers (n=56)
n %
Nurses Therapists Social workers Case manager assistants
56 27 24 16
100 50 43 29
Source: Question 23: Which staff groups work with people with long- term conditions and act as case managers within the ACM service? Which staff groups work with Very High Intensity Users?
Additionally, respondents were asked to distinguish between the different staff groups who worked as case managers for all case managed patients within the service compared with those who worked as patients classified as Very High Intensity Users. Table 4.18b reveals that four fifths of the primary care trusts used nurses as case managers for all patients and nearly all (95%) specifically for Very High Intensity Users. Less than a third of respondents reported that they used other professions as case managers for Very High Intensity Users. Social workers and therapists were used as case managers more frequently for patients who were not in this category.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 96
Table 4.18b Professional background of case managers by patient group (n=56)
Case managers
Case managers for Very High Intensity Users
n % n %
Nurses Therapists Social workers Case manager assistants/support workers/assistant practitioners
47 29 20 13
84 52 36 23
53 15 10 9
95 27 18 17
Source: Question 23: Which staff groups work with people with long- term conditions and act as case managers within the ACM service? Which staff groups work with Very High Intensity Users?
More specifically Table 4.18c demonstrates that over half of the respondents reported that their primary care trusts used community matrons as case managers for Very High Intensity Users compared to less than a quarter who used social workers.
Table 4.18c Community matrons and social workers as case managers by patient group (n=91)
Case managers
Case managers for Very High Intensity Users
n % n %
Community matrons Social workers
39 52
43 59
52 20
59 23
Source: Question 23: Which staff groups work with people with long- term conditions and act as case managers within the ACM service? Which staff groups work with Very High Intensity Users?
Nearly four fifths of the case managers were based in nurse teams in primary care and over two thirds in hospitals. Fewer were based in integrated teams or GP practices, as is illustrated in 4.19.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 97
Table 4.19 Location of case managers (n=56)
n %
Nurse team in primary health care GP practices Health and social care integrated team Hospital Local authority social care services team Health and social care integrated old age team Other Intermediate care Health and social care integrated old age mental health team
44 16 16 9 8 4 4 3 3
79 29 29 16 14 7 7 5 5
Source: Question 24: Where are case managers/case manager assistants for people with long-term conditions, or those undertaking the equivalent role, based?
Table 4.20 shows that nearly all of the case managers were managed solely by health services staff with less than a quarter having any joint arrangements.
Table 4.20 Management arrangements (n=56)
n %
Health services only Jointly managed, with health services holding the major responsibility Local authority social care only Jointly managed, with social care services holding the major responsibility
48 9 6 4
86 16 11 7
Source: Question 25: Which organisation provides the manager for case managers?
Three quarters of respondents reported a programme of training for case managers in their primary care trust (Table 4.21). It was mostly focused on advancing clinical and assessment skills and some case managers were undertaking higher education courses as well as specific clinical training.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 98
Table 4.21 Training programme for case managers (n=56)
n %
Yes No
42 14
75 25
Source: Question 26a: Do you have a programme of training for your ACM service for the year ending March 2008?
Less than two fifths of the primary care trusts reported training specific to self-care (Table 4.22). Little further detail was provided but this was most often reported as being disease specific.
Table 4.22 Self-care specific training (n=56)
n %
Yes No
22 34
39 61
Source: Question 27a: Does your ACM service initiate or participate in any staff training initiatives specific to self-care or self-care support?
Table 4.23 shows that some tasks were almost universally reported as being usually part of the case manager role. Assessing health care needs, care planning, implementation and monitoring of the care plan, reviews and providing patient education and clinical oversight were reported by almost all the primary care trusts. Assessment of social care needs arranging and allocating services, medications review and patient advocacy were undertaken by four fifths of the case managers. Over three quarters recorded that the provision of emotional/therapeutic support was provided by case managers. Almost two thirds of respondents usually provided hands on care (64%). Less than half reported assisting patients to access self-care support with 48 per cent assessing for entry into self-care support services and over two fifths directly referring patients (44%). Less than a third routinely contributed to the provision of self-care support (32%) and only one fifth to the development of self-care support programmes. Very few respondents reported that financial assessment and case budget management were tasks which case managers undertook regularly as part of their role.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 99
Table 4.23 Tasks undertaken by case managers
Usually Sometimes Never
n % n % n %
Assessment (n=56) Assessment of health care needs Assessment of social care needs Assessment for entry into self-care support services Care coordination (n=91) Financial assessment Care planning Arranging/allocating services Implementation of care plan Case budget management/budget holding Monitoring the implementation of the care plan Reviews Direct clinical and emotional support (n=56) Hands on care Clinical oversight Patient advocacy Provision of emotional/therapeutic support Prescribing/medications review Self-care support (n=56) Provide patient information and education Refer patient to self-care support services Contribute to the provision of self-care support services Contribute to the development of self-care support programmes
54 47 27 10 84 76 86 4 86 88 36 52 45 43 47 54 25 18 11
96 84 48 11 93 85 96 5 96 98 64 93 80 77 84 96 44 32 20
0 8 18 35 5 11 3 17 3 2 17 3 9 11 7 1 27 29 31
0 14 32 40 6 12 3 20 3 2 30 5 16 20 13 2 48 52 55
2 1 7 43 1 2 1 65 1 0 3 0 1 1 2 0 2 7 13
4 2 13 49 1 2 1 76 1 - 5 0 2 2 4 0 4 13 23
Source: Question 28: Do case managers undertake the following tasks?
4.6 Process of case management
4.6.1 Patient identification
Eighty six per cent of primary care trusts were reported having locally agreed referral criteria (Table 4.24). The most frequently cited were the number of hospital admissions followed by age and disease.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 100
Table 4.24 Referral criteria (n=56)
Source: Question 29b: If yes, what do they include?
Table 4.25 Targeting within case management service (n=56)
n %
Yes No
30 26
54 46
Source: Question 30a. Is ACM in your primary care trust targeted at specific diseases or conditions?
Fifty four per cent of the primary care trusts targeted their case management service on specific diseases or conditions (Table 4.25). Table 4.26 demonstrates that the most common were chronic obstructive pulmonary disease and coronary heart disease. However, over two fifths of respondents stated that their service was targeted on diabetes (46%) and multiple conditions (41%). When primary care trusts had more than one target group, these groups also included chronic obstructive pulmonary disease (32%) and coronary heart disease (28%). It was interesting to note the focus upon identified physical disorders rather than a comprehensive illness model.
n %
Number of hospital admissions Age Disease Recognised tool e.g. Castlefields tool Other
36 32 32 16 9
64 57 57 29 16

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 101
Table 4.26 Targeted conditions (n=56)
n %
Coronary heart disease Chronic obstructive pulmonary disease Diabetes Multiple conditions Other neurological conditions Asthma Hypertension Stroke and transient ischemic attack Musculoskeletal conditions Epilepsy Cancer Mental health Hypothyroidism Falls Other
28 28 26 23 17 16 15 11 8 8 7 5 3 3 1
50 50 46 41 30 29 27 20 14 14 13 9 5 5 2
Source: Question 30b: If yes, which long-term condition groups (the list below incorporates Quality and Outcomes Framework categories)?
Table 4.27 shows that patients were identified using a variety of methods. The most frequently reported were referrals from other professionals followed by PARR II (Billings et al., 2006) and the Single Assessment Process. There were no significant differences in the length of time the service had been established and the type of patient identification method used. Few primary care trusts used the combined predictive method (Dixon, 2007). Of these methods the most effective was judged to be referrals from other professionals, noted by over four fifths of respondents (86%).
Table 4.27 Method of patient identification (n=56)
n %
Referrals from other professionals Single Assessment Process documentation Patient at Risk of Re-hospitalisation II (PARR II) Disease registries Hand searching patient records Patient at Risk of Re-hospitalisation I (PARR I) Castlefields tool High-impact user manager (Dr Foster) Accident and emergency attendance Combined predictive model
48 30 30 23 21 20 14 13 10 6
86 54 54 41 38 36 25 23 18 11

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 102
Source: Question 31a: What are the main methods adopted for identifying high risk patients within your service? please indicate all main methods that apply to your service.
4.6.2 Assessment
Four fifths of primary care trusts used assessments within the Single Assessment Process as part of the assessment for case management (Table 4.28).
Table 4.28 Assessments within the Single Assessment Process (n=56)
n %
Yes No
45 11
80 20
Source: Question 32: In your area, are assessments made under the Single Assessment Process accepted as part of the assessment information for active case management?
Some respondents reported the use of more than one assessment tool. Two thirds specified the use of locally approved documentation within the Single Assessment Process and over a fifth a disease specific tool as illustrated in Table 4.29. Specific tools employed under the Single Assessment Process are also cited in the table.
Table 4.29 Assessment tools (n=56)
n %
Locally approved Single Assessment Process tool Disease specific Easycare FACE MDS Other
37 12 9 8 3 1
66 22 16 14 5 2
Source: Question 33: Which assessment tools are in use by case managers?
Very few case managers could assess for local authority funded social care services, of those that could homecare services were the most frequently reported (Table 4.30).
Table 4.30 Case managers assess for local authority social care services (n=56)
n %
Yes No
9 47
16 84

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 103
Source: Question 34a: Can ACM service staff undertake assessments for provision of local authority funded social care services?
4.6.3 Care planning
As shown in Table 4.31, patient care plans nearly all contained details of primary health care services and over half contained details of intermediate and social care services. Less than a quarter reported details of acute health services.
Table 4.31 Content of care plans (n=56)
Usually Sometimes Never
n % n % n %
Case management/primary care services Acute foundation trust services Intermediate care services Social care services
48 13 29 34
86 23 52 61
6 19 22 18
11 34 39 32
2 23 4 4
4 41 7 7
Source: Question 35: For ACM patients, do care plans routinely detail the contribution made by the following:
Only thirteen per cent of case managers could authorise the use of any local authority services, most frequently domiciliary care (Table 4.32), and important indicator of the extent of substantive service integration.
Table 4.32 Service authorisation by case managers (n=56)
n %
Domiciliary care Day care Respite care Preventative services Other
7 2 3 0 1
13 4 5 0 2
Source: Question 36b: If yes, which resources?
All questionnaire respondents were asked how cases were allocated within their service. Table 4.33 shows that three fifths reported that cases were allocated by either the level of qualification of the member staff responsible for their care or the intensity of involvement they required.
Table 4.33 Criteria for case allocation (n=56)
n %
Level of staff qualification Intensity of involvement
52 51
61 60

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 104
Allocation as staff available Time limited, short term intensive involvement e.g. 13 weeks Length of contact
31 12 10
36 14 12
Source: Question 37: How are cases of different levels of need/complexity/risk allocated in your ACM service?
Those respondents who completed the full questionnaire were also asked whether they had a written policy to allocate cases of different levels of need to different levels of case management (Table 4.34). Only about a quarter of these primary care trusts had such a policy.
Table 4.34 Written policy on case allocation (n=56)
Figure 4.3 Mean caseload size
Source: Question 38: Does your ACM service have a written policy to allocate cases of different levels of need/complexity/risk to different levels of case management (e.g. low risk patients may be visited monthly and high risk patients may be visited weekly)?
4.6.4 Monitoring and review
Most respondents (69%) reported that within their service the average active caseload was less than 50 (Figure 4.3). Policy guidance suggests that the average caseload for a community matron should be between 50 and 80 (DH, 2005b),
n %
Yes No
15 41
27 73
0 10 20 30 40 50 60
C HDCOPD
DiabetesMultiple conditions
Other neurological conditionsAs thm a
H ypertensionStroke and Transient Ischaemic Attack
Musculoskeletal conditionsEpilepsyC ancer
Mental healthH ypothyroidism
FallsOther
percentage

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 105
although less than a quarter of respondents reported that they had an average caseload within this range, perhaps reflecting the relative youth of many services.
Source: Question 39: Please estimate a case manager’s average active caseload size?
In the majority of primary care trusts it was reported that the same practitioner usually remained responsible for a patient during their time with their service, particularly for those cases open for longer than three months (4.35).
Table 4.35 Continuity of case manager (n=56)
Usually Sometimes Never
n % n % n %
For cases closed within 3 months For cases open after 3 months for longer term monitoring/review
36 44
64 79
5 9
9 16
6 3
11 5
Source: Question 40: How often does the same practitioner within the ACM service remain responsible for assessment, case management, monitoring and review within a single patient episode?
Over 40 per cent of respondents reported that less than a quarter of their primary care trust’s active caseload was visited weekly; over a quarter estimated that over 50 per cent of the caseload was visited weekly. This variation suggests that the intensity of the case management service differed between primary care trusts (Table 4.36)
Table 4.36 Proportion of caseload visited weekly (n=56)
Proportion of cases (%)
0–25% 26–50% 51–75% 76–100%
n % n % n % n %
Caseload visited weekly 22 42 16 31 12 23 2 4
Source: Question 41: Please estimate the proportion of the overall active ACM caseload within your service that are visited at least weekly within your service.
Almost a third (30%) of respondents reported that up to a quarter of their patients were still in active case management after having been in the service for six months. A further third (32%) reported that up to half of their patients would be subject to routine monitoring. Just over a quarter (27%) reported that after six months, up to three quarters of their patients would be in disease management (Table 4.37).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 106
Table 4.37 Destination of patients after six months (n=56)
Proportion of cases (%)
0–25 26–50 51–75 76–100
n % n % n % n %
Case management Routine monitoring within case management Disease management
17 8 4
30 14 7
9 18 12
16 32 21
13 12 15
23 21 27
7 6 6
13 11 11
Source: Question 42: Six months from their entry please estimate the proportion of cases within your ACM service which typically fall within the following categories.
Eighty nine per cent of respondents reported that their service had review systems in place, the majority of reviews for active cases taking place face-to-face with the patient. Table 4.38 demonstrates that although over half also reported the use of information from carers and telephone conversations in this context. Inactive cases were most frequently reviewed by telephone.
Table 4.38 Method of review (n=56)
Active Inactive
n % n %
Case manager face to face contact with patient Information from carer Telephone Multi-disciplinary team - with patient Multi-disciplinary team - without patient Letter Assistant practitioner face to face contact with patient Other
44 30 30 27 21 10 9 6
79 54 54 48 38 18 16 11
9 14 33 3 9 11 8 1
16 25 59 5 16 20 14 2
Source: Question 43b: If yes, which of the following methods do you currently routinely employ for active and inactive cases?
Respondents were asked the three most common reasons for case closure in their service. The death of the patient accounted for the majority of case closures, for the remainder the most frequently cited reason was case management having no perceived benefit (Table 4.39). This isn’t indicative of high turnover and demand.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 107
Table 4.39 Reasons for case closure (n=56)
n %
Death No discernable benefit from case management service Leaving locality Moved to community nursing Moved to long-term care home Patient refusing service Moved to disease specific services Moved to self-care support Moved to social care services Moved to informal care Moved to other services
46 22 18 17 16 14 8 8 4 2 2
82 39 32 30 29 25 14 14 7 4
Source: Question 44: What are the three most common reasons for case closure in your ACM service?
4.7 Information systems
Forty five per cent of primary care trusts reported that they had a computerised client record system for assessment and case management. Table 4.40 shows that only one fifth of these were linked to other record systems within primary care.
Table 4.40 Type of computerised client record system (n=56)
n %
Linked to other record systems within primary care (e.g. Lorenzo) Case management service specific Other Liquid logic (joint health and social care access system)
11 9 6 2
20 16 11 4
Source: Question 45b: If yes, is it
As can be seen in Table 4.41, almost two fifths of the services could access all information on patients in receipt of case management electronically within their primary care trust or acute hospital service.
Table 4.41 Access to patient information (n=56)
n %
Case management patients can be identified on hospital record systems Case managers can electronically access all information on their patients within the primary care trust Case management service has a specific computerised client record system
22 21 15 15
39 38 27 27

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 108
None of the above
Source: Question 46: Which of these statements describe ACM information systems in your primary care trust?
Table 4.42 provides details of the types of information stored electronically within case management services. Over half stored information about patients’ personal details, ethnic origin and medical information and diagnoses electronically. Just over a quarter stored assessment documentation electronically. With regard to care plans about a third recorded their own input electronically and slightly less the input from other NHS services. A much smaller proportion recorded inputs from social care and self-care support services.
Table 4.42 Content of electronic record of patient information (n=56)
n %
Personal details Ethnic origin Medical information Diagnoses Single Assessment Process Specialist assessments Overview assessment Care plans Case management Other NHS services Social care services Self-care support services Voluntary organisation services Reviews
41 33 31 28 15 15 19 17 9 6 5 16
73 59 55 50 27 27 34 30 16 11 9 29
Source: Question 47: What information about individual patients is held in the electronic information system relating to the ACM service?
4.8 Service development
Table 4.43 shows that nearly a third of case management services had been subject to a formal evaluation.
Table 4.43 Formal service evaluation (n=56)
n %
Yes No
18 38
32 68

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 109
Source: Question 48: Has there been a formal evaluation of your ACM service?
Self-care was felt to be relevant to case management services with relation to promoting patients’ independence in nearly a quarter of primary care trusts (24%):
“To enable patients to become independent in the management of their long-term condition, which requires the use of self-care strategies.”
Primary care trust 48
Almost two fifths commented that they thought self-care support was a very relevant area (19%):
“Highly relevant, it underpins our work.”
Primary care trust 46
Ten per cent thought that it was an underdeveloped area in their primary care trust, one commenting that there was a lack of specific models of self-care support for case managed patients:
[There is a] “desperate need for self-care models for these patients.”
Primary care trust 15
Table 4.44 Areas for service development
Improved integration Workforce training and staff retention Patient identification and targeting Engaging partners Reduction of length of stay costs Increased service capacity Improved patient outcomes Evaluating service IT system development Caseload size stratification Training for self-care support
Source: Question 50: What are the key issues in developing your ACM service?
Table 4.44 shows the areas for service development that respondents thought were a priority for their case management service. The most frequently reported were improved integration, one respondent seeing the case management service as having to bring in other partner agencies:
“ACM is a catalyst for change within the pct clinical services and our partner organisations. Challenge has been in engaging partners who do not share budgets and therefore have competing priorities.”
Primary care trust 8
Sharing budgets was not the only differences that presented a challenge to integration:
“Different professional groups have different IT systems cultures, targets, incentives, custom and practice.”

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 110
Primary care trust 30
Workforce training and retention were issues for many primary care trusts; one was planning to use the self-care strategy to highlight training needs:
“Currently a self management strategy is being developed which will highlight training needs and awareness raising needs of self management support across health and social care.”
Primary care trust 23
4.9 Summary
4.9.1 Service description
The questionnaire achieved a response rate of 60 per cent. Over two thirds of the respondents reported they had between 30-90 GP practices in their jurisdiction. Most had a resident population somewhere between 100,000 and 300,000. The majority of services routinely negotiated with only one local authority and started accepting patients between 2004 and early 2007 into the case management service.
4.9.2 Case management objectives
There was a great deal of similarity between the objectives of the case management services. All had the aim of increasing the independence and improving the health of people with long-term conditions. Nearly all had the further objectives of improving care co-ordination; improving quality of life and reducing preventable hospitalisation. The biggest differences in objectives within the group were with the use of case management services to improve accountability and prevent unnecessary residential and nursing home care.
A majority of respondents reported that their case management service was a means of providing long-term support and coordinated care and a way of assessing needs and implementing care plans. Evidence of discrimination as to which patients were supported by the service was evident with only a third recording that this was a service provided to a majority of patients. Three quarters reported that their services were based on a geographical locality model.
4.9.3 Links with other services
Just over half of the case management services reported formal links with local authorities and over one third of these concerned how case managers accessed social care resources. Formal agreements within health services were more widespread than those with local authorities with three quarters having agreements with community nursing services. The most frequent agreements within acute services were with specialist disease nursing. Three quarters had agreements with intermediate care schemes to prevent hospital admission. There were very few agreements with old age psychiatry and hospital pharmacy services. Just under a third of respondents reported their service having dedicated physician sessions and a similar proportion reported specific out of hours provision for their patients.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 111
Most services had formal arrangements for sharing documents within the Single Assessment Process with local authorities. A similar proportion also had such arrangements with intermediate care services. The exchange of written information between the case management service and partner organisations was reported by over half of the respondents. Very few reported the use of single case files, in which professionals from different disciplines all record their input.
4.9.4 Self-care support services
Just under half of the respondents reported a designated lead for self-care support within their service. Respondents were asked about any formal links that might have been made between the case management service and voluntary organisations which support self-care for patients with long-term conditions. Links with Age Concern or other local organisations which provided self-care support were also noted in this context.
Self-care services were available in most areas, although these were not thought to be frequently used by case managed patients. Three services: accessible advice and information, generic self-care support training and disease specific self-care support training were available in over three quarters of the primary care trusts. Over three quarters of primary care trusts provided accessible advice and information to patients with diabetes and chronic obstructive pulmonary disease. Two thirds provided technology and equipment to those with coronary heart disease.
A large number of respondents found it difficult to estimate the proportion of patients on the case management service caseload who were currently using self-care support services. Of those that answered, the majority of primary care trusts stated that fewer than 20 per cent of the caseload were using such services.
4.9.5 Staff mix and tasks
The most frequently reported professional background for case managers was nursing; most were described as district nurses followed by community matrons, particularly for Very High Intensity Users. Nearly 80 per cent of the case managers were based in nurse teams in primary care with few based in integrated teams. Most case managers were managed solely by health services with less than a quarter having any joint arrangements. Three quarters of the primary care trusts reported a programme of training for their case managers, mostly focused on advancing clinical and assessment skills.
4.9.6 Case management
Some tasks were almost universally reported as being usually part of the case manager role. Assessing health care needs, implementation and monitoring of the care plan, reviews and providing patient education were reported by almost all the respondents. Very few reported that case managers carried out financial assessments or were budget holders in that some elements of the care plan were costed.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 112
4.9.6.1 Patient identification
The majority of respondents reported having locally agreed referral criteria for entry into their service, most frequently the number of hospital admissions followed by age and disease. Just over half targeted their service on specific diseases or conditions, the most common being chronic obstructive pulmonary disease and coronary heart disease. Patients were identified using a variety of methods; most frequently referrals from other professionals (judged most effective) followed by the clinical tool PARR II and the Single Assessment Process.
4.9.6.2 Assessment and care planning
The majority of case management services used assessments made within the Single Assessment Process. Very few case managers could assess for local authority funded social care services. Patients’ care plans nearly all contained details of primary health care services and over half contained details of intermediate and social care services. Less than a quarter reported details of acute services. Very few services had agreements whereby they could authorise the use of any local authority services. Just over a quarter had a written policy to allocate cases of different levels of need to different levels of case management, mostly by the level of qualification of the member staff responsible for their care or the intensity of involvement they required.
4.9.6.3 Monitoring and review
Most services had an average active caseload per worker of fewer than fifty. The majority reported that the same practitioner usually remained responsible for a patient during their time with their service, particularly for those open for longer than three months. About a third of respondents reported that less than a quarter of their active caseload was visited weekly; another third estimated that over half of the caseload was visited weekly.
Nearly all the services had review systems in place, the majority of reviews for active cases taking place face-to-face with the patient. The three most common reasons for case closure were the death of the patient, that the service was having no benefit and that the patient had left the locality.
4.9.7 Information systems
Less than half of the services had a computerised client record system and less than half of these were linked to other record systems. Over half stored information about patients’ personal details, ethnic origin and medical information and diagnoses. Less than half stored assessment and care plan information.
4.9.8 Service development
Nearly a third of case management services had been subject to a formal evaluation. The most frequently reported area for service development was improved integration with partner agencies followed by workforce training and retention.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 113
Chapter 5 A comparison of case management and care management in different settings
The aim of this chapter is to explore variations between three care/case management services within the context of some of the most relevant literature on the subject. As noted in the description of the method, this chapter will employ data from three national surveys: case management for people with long-term conditions; care management arrangements for older people; and also for adults with physical and sensory disabilities. In order to promote clarity in the reporting of information from these surveys terminology which is different to some of that employed in the previous chapter is used. The most obvious change is the use of the term, ‘primary care trust case management’ to describe the assistance offered to people with long-term conditions, thereby making a clear distinction between this and the two care management services provided by local authorities.
This chapter is divided into three parts. First, the objectives of these three case/care management services are presented. Second, the service characteristics and information systems of local authority care management arrangements for older people and primary care trust case management for long-term conditions are compared. Third, these data are used to develop composite scores for differentiation and integration. These are concepts identified in the case management literature which assist in assessing the development of care/case management systems and are described in more detail subsequently. Where appropriate the second and third sections of this chapter include references to the findings from the survey of local authority care management arrangements for people with physical and sensory disabilities.
5.1 Case/care management objectives
Local authority care management has been described as a service ‘open to different interpretations’ (Challis et al., 2005). One way to identify how an organisation might describe their service has been to ask those with responsibility for it to select statements which best describe both the aspirations (goals) of the service and current organisational arrangements. In this way we seek to capture the strategic vision for a service and gain an insight into its operational practice. Data are reported in respect of three services.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 114
Table 5.1 Case/care management goals
Local authority older people n=43 (%)
Primary care trust long-term conditions n=43 (%)
Local authority physical disabilities n=35 (%)
Chi square exact test1
To provide more intensive long-term support in the community
40 (93) 38 (88) 32 (91) NS
To improve the extent and scope of services
32 (74) 33 (77) 32 (91) NS
To improve the coordination of care to people living in the community
41 (95) 42 (98) 35 (10) NS
To improve the quality of life of people
42 (98) 42 (98) 35 (100) NS
To divert people away from inappropriate hospitalisation
41 (95) 43 (100) - NS
To arrange more speedy and effective hospital discharge
42 (98) 41 (95) - NS
To assist in the rehabilitation of people
42 (98) 35 (81) 31 (89) 0.051
To achieve improved accountability
29 (67) 19 (44) 27 (77) 0.008
To divert people from inappropriate residential and nursing home care
42 (98 23 (53) 35 (100) <0.001
To increase the independence of people
42 (98 43 (100) 34 (97) NS
To improve the health of people 34 (79) 43 (100) - 0.002
Source: 1. Mehta and Patel (1998)
As indicated in Table 5.1 there was very little variation between the goals of the primary care trust case management and local authority care management arrangements for all three user groups. Around 90 per cent of all groups reported that the goals of their service were to improve coordination of care for people living in the community; improve quality of life; provide intensive support in the community; and increase independence. A similar proportion of case management services and care management services for older people also cited preventing inappropriate admission and facilitating discharge from hospital as goals for their service. The last two findings reflect perhaps the shared populations of these services, which both target older people with complex health problems who often require hospital treatment. Table 5.1 also revealed that within each of the three user groups achieving improved accountability was the least frequently reported as a goal of care/case management. However, when a pan group comparison was made a significant difference (p=0.008) between the two local authority and the

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 115
primary care trust led services was noted, suggesting that this goal of improved accountability was less important in the latter.
Other areas of significant difference between the goals of the respective services were reported. One of these related to diverting people away from inappropriate admission to residential and nursing home care (p<0.001). Here both local authority care management services were more likely to report this than the primary care trust case management service. The latter is not surprising since an underlying objective of local authority care management for older people has been to provide care at home rather than within care homes and more broadly an objective of the community care reforms was to maintain people in their own homes wherever possible (Challis and colleagues, 2005; Cm 849, 1989). On the other hand and perhaps reflecting the focus on broader health related targets of the NHS, significantly more primary care trust case management services had improving health as a goal (p=0.002). Interestingly, when the two local authority care management services and the primary care trust case management services were compared, significantly (p=0.051), more local authorities had rehabilitation as a service objective.
Finally it is relevant to note that Table 5.1 also revealed that many of the goals of the local authority services for adults with physical and sensory disabilities are similar to those of local authority services for older people. This perhaps illustrates the importance of the culture, values and orientation of the local authority on case/care management services and suggests that these might differ from the primary care trust setting of case management. However, more care management services for physically disabled adults reported a goal to improve the extent and scope of services than was the case in older people’s services. It has been suggested that there is a reasonably high degree of specialisation for the teams providing services to this user group (Xie et al., 2008a) which may influence their service development focus. This observation is supported by the high number of respondents working with this user group who considered case management to be a means of promoting the development of new forms of service response, noted below in Table 5.2.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 116
Table 5.2 Case/care management service arrangements
Local authority older people n=43 (%)
Primary care trust long- term conditions n=43 (%)
Local authority physical disabilities n=35 (%)
Chi square exact test
A specific job undertaken by designated members of staff who are called care managers
24 (56)
26 (61)
19 (54)
NS
A single member of staff responsible for assessment, care planning, monitoring and review tasks for a particular service user
24 (56)
24 (56)
22 (63)
NS
A way of categorising the arrangements through which people coming to the agency are assessed and a response made to their needs
30 (70)
22 (51)
26 (74)
0.08
A response provided to the majority of service users
30 (70) 16 (37)
26 (74)
<0.001
A response provided only to a limited number of service users
5 (12)
15 (35)
5 (14)
0.01
An activity by which people with complex needs receive intensive help different in nature and scope to other service users
18 (42)
36 (84)
15 (43)
<0.001
A means of providing long-term support and coordinated care incorporating assessment and review at home
30 (70)
43 (100)
– <0.001
An activity by which needs are assessed and care plans implemented
41 (95)
40 (93)
33 (94)
NS
An activity involving the coordination, delivery and monitoring of services to a degree of complexity, such that caseloads are small
5 (12)
29 (67)
11 (31)
<0.001
A response to complex needs involving multiple services
27 (64)
28 (65)
33 (94)
0.003
A means of promoting the development of new forms of service response
17 (41) 25 (60) 18 (51) NS

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 117
Overall there seemed to be consistency across the services for all three user groups, regarding the characteristics and purpose of the case/care manager role. Over 90 per cent of all three groups reported that service arrangements were an activity by which needs were assessed and care plans implemented. Similar percentages of respondents for all user groups also reported that within their service there was a specific job undertaken by designated members of staff known as care/case managers and this person was responsible for assessment, care planning, monitoring and review for a single service user.
Variation was, however, evident when respondents were describing other service arrangements. In all three services relatively few respondents described their service as one which provided assistance to only a limited number of service users although significantly more (p=0.01) primary care trusts agreed with this description. Around 70 per cent of the local authority groups reported care management as a response provided to a majority of service users, a significantly different (p<0.001) finding to that for case management services within the primary care trust. A similar trend (which almost reached statistical significance) between settings appertained to the description of the service as a way of categorising arrangements for assessing and responding to individual needs with this more likely to be apparent in local authority care management arrangements.
In respect of only one service descriptor did physical disability and sensory services differ from the other two. Respondents were significantly more (p=0.003) likely to describe their approach to case management as providing for people with complex needs involving multiple services. This may reflect the fact that occupational therapists, acting as care managers, frequently oversee housing adaptations as part of their care management role for this user group and that the strategic service commissioning aspect of care management for adults with physical and sensory disabilities is at a slightly more advanced stage of development than within older people’s services (Challis and colleagues, 2005).
In addition, there were differences between primary care trust and local authority services, both those relating to older people and those for adults with physical and sensory disabilities in respect of two service descriptions. Significantly more (p<0.001) primary care trusts reported that case management was an activity by which people with complex needs receive intensive help different in nature and scope to other service users. Conversely, lower percentages of both services provided by the local authority for both service user groups were described as being characterised by small caseloads, suggesting that intensive care management was the exception rather than the norm (Challis and colleagues, 1995). Also, it was reported that significantly more (p<0.001) primary care trusts describe their case management arrangements as involving the coordination, delivery and monitoring of services complex circumstances, with small caseloads. Furthermore, when just local authority services for older people were compared with primary care trust services, respondents from the latter were significantly more (p<0.001) likely to describe their service as providing long-term support and coordinated care at home. This suggests that these two services, although sharing a target population, focused the resources of their service differently. Primary care trust case management was more likely to target their service resources at a selected few with complex needs, although this was not always interpreted as providing a response to a limited number of service users.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 118
Whilst it is necessary for case/care management to face in a patient/client direction (concentrating on coordinating services) it is also important that it also informs the commissioning process and new forms of services response if appropriate (Challis and colleagues, 1995). Service development, specifically promoting new forms of service response was not reported by many respondents. The low response in respect of local authority care management services suggests that even with a well established service, developing new forms of service response often requires particular direction and will not simply evolve.
5.2 Service characteristics and information systems Table 5.3 Case/care management service characteristics
Table 5.3 compares the characteristics of older people’s services in the local authority and primary care trust case management services for matched areas. Significantly higher numbers of primary care trusts than local authorities (p<0.001) reported having guidance for entry into case/care management different to other elements of the service. Here we assume that the respondents based in primary
Local authority older people n=43 (%)
Primary care trust long-term conditions n=43 (%)
Fisher’s exact test (2 sided p value)
Eligibility criteria
Guidance for entry into case/care management different to elements of the service
21(49)
37 (86) <0.001
Staff acting as case/care managers
Nurses Occupational therapists Social workers Case manager assistants/support workers/assistant practitioners/community care workers
11 (26) 20 (47) 42 (98) 36 (84)
42 (98) 18 (42) 16 (37) 14 (33)
<0.001 NS <0.001 <0.001
Location of care/case managers
Health and social care integrated team Primary care nurse team Local authority adult services team Hospital Other
26 (61) 7 (16) 42 (97) 36 (86) 9 (21
15 (35) 38 (88) 7 (16) 7 (16) 5 (12)
0.030 <0.001 <0.001 <0.001 NS
Care/case managers’ managing agency
Primary care trust/health services only Jointly managed, with health services holding the major responsibility Jointly managed, with social care services holding the major responsibility Any joint management Local authority only
3 (8) 11 (26) 11 (26) 19 (44) 36 (84)
32 (91) 8 (19) 4 (9) 9 (21) 5 (12)
<0.001 NS NS 0.037 <0.001

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 119
care trusts are referring to the approach, summarised in chapter one, which specified three tiers of service for people with long-term conditions: supported self-care for the majority of the chronic care population; disease/care management for patients who have multiple long-term conditions; and case management for those patients who are very high intensity users of unplanned secondary care (DH, 2005b). Local authority responses are also likely to have been related to policy guidance which differs in emphasis. Within localities implementation is mediated by historical patterns of service and longstanding concerns over the application of eligibility criteria in respect of the provision of social care (Audit Commission, 1996; Challis and colleagues, 1997; Cm 4169, 1998). Subsequent guidance required local authorities to operate a single eligibility decision for all adults seeking social care support derived from a national framework and existing legislation and based on risks arising from needs associated with various forms of disability, impairment and difficulty. In addition, local authorities were to emphasise enablement and early intervention to promote independence rather than involvement at the point of crisis such as hospitalisation (DH, 2002; 2008). This suggests that the response of local authorities in Table 5.3 refers to guidance for entry into case management separate and distinct from the initial decision which determines eligibility for care management, and different again from the more universal services provided in response to the requirement from central government to provide this within the umbrella term of ‘preventative’ services.
As might be expected, due to the traditional association of these organisations with certain roles, all but one primary care trust (98%) employed nurses as case managers and all but one local authority employed social workers as care managers (98%). A higher but non-significant percentage of primary care trusts employed social workers than local authorities employed nurses, showing perhaps there was potentially more interagency working in their case management services. Other national surveys of care management arrangements have also indicated that lower proportions of primary care trust staff (mainly nurses) work as care managers for both older people and adults with physical and sensory disabilities, than for two other principal service user groups, adults with mental health problems and those with learning disabilities (Weiner et al., 2002; Venables et al., 2005; Xie et al., 2008a; b). Significantly more local authorities than primary care trusts reported employing non-professional staff such as community care workers (p<0.001) to work as case managers for older people. Finally it is relevant to note that Table 5.2 also shows just under half of both organisations employed occupational therapists as case managers, despite suggestions that this job role can contribute significantly to the care management process (Mountain, 2000). It has been reported elsewhere that a slightly higher proportion of services for adults with physical and sensory disabilities have occupational therapists as care managers (Xie et al., 2008a).
As can be see in Table 5.3, the majority of case/care managers were based in their own agency, with primary care trust case managers in primary care nurse teams (p<0.001) and care managers in local authority adult services teams (p<0.001), perhaps missing an opportunity for co-location and developing integrated practices between health and social care services. Table 5.3 also reveals significantly more local authority care managers were based in integrated teams (p=0.030) and hospitals (p<0.001). The case/care managers were mainly managed by their

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 120
employing agency although significantly higher numbers of local authority care managers were jointly managed (p=0.037).
Table 5.4 Information systems
While the successful sharing of information, especially electronically, is vital to multi agency working (Challis and colleagues, 1995; Glasby, 2003; Weiner et al., 2002) it has often been slow to develop. An evaluation of the implementation of the Single Assessment Process in services for older people revealed that the practice of routinely sharing information electronically was still some way in the future, although social care services had perhaps more developed systems than primary care trust services, particularly with regard to the electronic storage of information (Abendstern et al., 2010). As shown in Table 5.4, a similar picture is evident here. All the local authorities had a computerised records system compared with only half of the primary care trusts in the survey (p<0.001). All the local authorities also stored information about personal details (p<0.001) and ethnic origin (p<0.001), compared to less than three quarters of the primary care trusts. In both agencies, less than a quarter of these systems were linked to GP practice systems, indicating relatively poor information sharing with general practice (medical practitioners and nurses based in these settings), replicating a similar observation in relation to information sharing in the context of the Single Assessment Process (Abendstern et al., 2010). Table 5.4 also reveals that similar numbers of local authority care management services and primary care trust case management services stored diagnoses and other medical information. However, more local authorities stored assessment (p<0.001), care plan (p<0.001) and review information (p<0.001) than primary care trusts.
Local authority older people n=43 (%)
Primary care trust long-term conditions n=43 (%)
Fisher’s exact test (2 sided p value)
Presence of a computerised client record system for assessment and care management
Yes 43 (100) 20 (47) <0.001
Record system linked to general practice
Yes 7 (16) 9 (21) NS
Type if information about individual patients held in the electronic information system relating to the case/care management service
Personal details Ethnic origin Medical information Diagnoses Single Assessment Process Care plans Reviews
43 (100) 43 (100) 25 (58) 21 (49) 41 (95) 37 (86) 38 (88)
31 (72) 25 (58) 21 (49) 19 (44) 11 (26) 15 (35) 12 (28)
<0.001 <0.001 NS NS <0.001 <0.001 <0.001

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 121
5.3 Differentiation and integration within care and case management systems
In this section we again focus on findings from the surveys of local authority care and primary care trust case management. As noted in the introduction to this chapter, when considering variation between the approaches to care/case management two concepts are useful: integration, the extent to which a service spans health and social care boundaries; and differentiation, whether case/care management arrangements vary according to user’s needs (Challis et al., 2005). The previous section demonstrated that the degree of integration could be assessed using many indicators, from primary care trust staff working as care managers to the presence of joint commissioning or financial arrangements. Differentiation is often measured by whether there is variability in response in terms of staff level or resources and specifically whether intensive care management is provided to some whilst care management is offered to the majority. Intensive care management is defined as a specific service targeted at those with complex needs at risk of admission to institutional care (Challis and Davies, 1986; Applebaum and Austin, 1990; Challis, 1994; Challis et al., 2001) which is located within a wider network of other appropriate services (Challis et al., 1995). Although variations in care management arrangements are often found in social care for different user groups, for example for adults with physical and sensory disabilities and older people, arrangements indicative of intensive care management were rarely reported (Xie et. al, 2008a; Weiner et al., 2002).
Table 5.5 Indicators of differentiation and integration
Indicators of differentiation To provide more intensive long term support in the community
A response provided only to a limited number of service users
An activity by which people with complex needs receive intensive help different in nature and scope to other service users
An activity involving the coordination, delivery and monitoring of services to a degree of complexity, such that caseloads are small
Eligibility criteria, guidance for entry into case/care management different to elements of the service
Policy to allocate cases of different levels of need/complexity/risk to different staff groups
Indicators of integration Goal of improving the coordination of care to people living in the community
A response to complex needs involving multiple services
Social workers acting as case managers and nurses acting as care managers
Case managers based in health and social care integrated team
Joint management arrangements
Record system linked to GP practices

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 122
Table 5.6 Differentiation and integration scores
Primary care trust long-term conditions mean (sd) n=43
Local authority older people mean (sd) n=43
t-test (independent sample)
Integration score 2.77 (1.09) 3.05 (1.23) NS
Differentiation score
3.93 (1.20) 2.65 (0.99) <0.0001
To investigate the influence of these further within care/case management arrangements measures of integration and differentiation from the items in Table 5.5 were developed. These build upon other work examining these features in services for older people (Challis and colleagues, 2006); including old age mental health services (Reilly et al., 2003). The scores reflect the number of attributes present for each domain, integration and differentiation, listed in Table 5.5. Table 5.6 shows there was a significant difference between the score for differentiation between case management in primary care trusts and local authority care management for older people. There was no significant difference in integration scores between the two samples, although overall, local authorities did score more highly than primary care trusts. However, there was an indication from certain variables that local authority social care may have developed this concept of integration further, for example a higher proportion held electronic information (Table 5.4). Integration at a strategic level can be promoted by the use of joint management structures. As noted in the previous section the majority of care and case managers were managed within their originating agency showing that this arrangement was being little used. However, where this was the case, again significantly higher numbers of local authority care managers were jointly managed.
Differences between the services with regard to integration and differentiation within care/case management could be attributed to different approaches to the targeting of service provision, reflecting different policy imperatives. Primary care trust case management is intended to offer the service to people with certain defined need criteria. These services were less likely to report their service was a response to the majority of users. In addition they were more likely to score highly on other indicators of differentiation. Together these suggest such services would target resources to those with complex needs. Conversely care management services were more likely to be offered as a response to the majority of users. These findings reflect the principal focus of guidance at the inception of both care and case management within their respective services (Cm 849, 1989; DH, 2005; 2004c). Despite these indicators of a differentiated response from the primary care trust case management services, other research has demonstrated that the targeting of resources to appropriate individuals is a more complex process than represented in these summary scores, which occurs throughout the case management process; from the initial screening of a target population to assessment and possible eventual discharge (Abell et al., 2010a).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 123
Primary care trust case management, as mentioned above is a newly implemented service, especially when compared to local authority care management and it might have been anticipated that this would score more highly on the indicators of integration in Table 5.5. One of the key elements supporting integrated services is the sharing of information about individual patients (Brown et al., 2003; Lyon et al., 2006) although there was a significant imbalance in access to computerised record systems, the local authorities had near universal access compared to less than half of the primary care trusts. The more developed technology of the local authorities was reflected in their having assessments, care plans and review information electronically stored, as noted in Table 5.4. However it should be noted that the case management service was introduced by national policy as an integrated model between the primary care trust and the local authority, the organisation responsible for the delivery of social care (Jacobs et al., 2006) and it advocated an integrated approach to case management practice (DH, 2005b). Despite this the findings described above suggest that the anticipated links between the sectors have not yet emerged and this has been confirmed in other research exploring case management services (Abell et al., 2010b).
One of the hallmarks of a differentiated care/case management service is one in which intensive care management is located alongside other services (Hughes et al., 2005). However, it is rarely reported and care management often applied as a universal service response to the majority of users, rather than targeted at complex cases (Challis, 1999). This facet of lack of differentiation has been observed as a concern in a number of policy documents throughout the 1990s (Challis, 1999) and later. These results are reinforced by the survey of services for adults with physical disabilities reported earlier in this chapter, where there was little evidence of targeting or differentiation apparent (Challis and colleagues, 2004 et al., Xie et al., 2008a). The findings of this chapter, and particularly those of this section, suggest that primary care trust case management services are more differentiated than their local authority equivalent. Nevertheless other research into case management for people with long term conditions suggested that this does not necessarily equate to the provision of a type of service which could be described as intensive case management (Abell et al., 2010a).
5.4 Summary
5.4.1 Case/care management objectives
There were broad similarities in the stated goals and service objectives of primary care trust case management and local authority care management arrangements for older people and those with physical and sensory disabilities. This perhaps reflects the shared target populations of the services; those with long-term, multiple health and social care needs. More particularly local authority case management and primary care trust case management shared the service objectives of preventing inappropriate hospital admission and facilitating timely discharge.
Overall, principal differences between primary care trust case management and local authority care management arrangements for older people tended to reflect policy guidance. Hence local authority care management services emphasised the

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 124
longstanding objectives of diverting users from inappropriate care home placement concurrently with providing a care management approach to the majority of users. On the other hand primary care trust case management services also reflected a dichotomy of approach with a greater focus on improved health outcomes for patients and possessing certain features of intensive case management. In the remainder of this summary, observations relate to two services: local authority care management for older people and primary care trust case management.
5.4.2 Service characteristics and information systems
For both local authority care management and primary care trust case management the application of local service specific eligibility criteria is constrained by national guidance. The finding that entry into case management was more likely to be prescribed by this within primary care trust case management is perhaps a reflection of both the wider range of services provided by local authority old age services and longer experience of the managing the complexities of operationalising eligibility criteria.
Services tended to employ staff from occupational groups traditionally associated with their organisation and staff were most often located in and managed by their employing organisation. All local authorities had a computerised record system and were better placed to make use of electronic methods of information storage and transfer than was the case in primary care trust case management services.
5.4.3 Differentiation and integration within care and case management systems
Composite indicators of integration and differentiation were developed using findings from the two previous sections. The principal finding in this section was that primary care trust case management services scored more highly on the indicator of differentiation than local authority care management services for older people. This implies that overall this service seeks to provide a response appropriate to the level of assessed need, targeting most assistance on the most highly dependent patients. Conversely, no significant difference between the two services was highlighted by the composite indicator of integration. This finding is perhaps surprising given the relative longevity of the service. However, in respect of certain components of it, local authority care management services did demonstrate statistically significant differences when compared with primary care trust case management services.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 125
Chapter 6 Case studies The aim of this chapter is describe the findings from the case studies of case management services for people with long-term conditions which were undertaken in four sites. As described in Chapter three, they were chosen because the findings from the postal survey suggested both that the role of self-care was demonstrably part of the service response within their locality and they showed different approaches to case management in terms of the range of tasks undertaken; the degree to which the approach differed according to level of need; and the degree to which the long-term conditions services was integrated with other sectors of the local health and social care economy. The selection of sites was based on a number of factors: overall scores for the four key domains; geography (location and authority type); and a willingness and ability of the service to participate in the research.
Data collection activities are also described in chapter 3. For each manager a semi-structured interview schedule was prepared with three components: a summary of the survey responses to be validated by the interview; questions arising from these survey responses10 and key features of case management services derived from the literature11. The composition of each focus group was determined by the service manager in consultation with the researcher and informed by this and the survey findings. The focus group interview schedules were again informed by the survey findings and the literature review, as well as the earlier interview with the service manager12. Each of the managers interviewed had responsibility for the delivery and development of the long-term conditions service in their locality. The size of the focus groups ranged from five to 11 members.
This chapter begins with a description of the case management services for people with long-term conditions and the self-care services in the localities selected for more detailed enquiry. Next the case management service in each of the four sites is described in detail. At the beginning of each the characteristics of the service are detailed based on the classification in Table 3.3. Five domains of enquiry are employed to describe it: links with other agencies; self-care support services; staff mix and tasks; the process of case management; and information systems, reflecting principal areas of enquiry in the postal survey which was informed by the literature review. Finally, cross cutting and emergent themes from the detailed analysis of organisation and practice in the four sites are summarised.
6.1 Case study sites
The characteristics of the services selected for more detailed study of their modes of working are summarised in Table 6.1. This provides additional descriptive details
10 See Appendix 6 for interview schedule.
11 See Appendix 7 for framework.
12 See Appendix 8 for focus groups schedules.
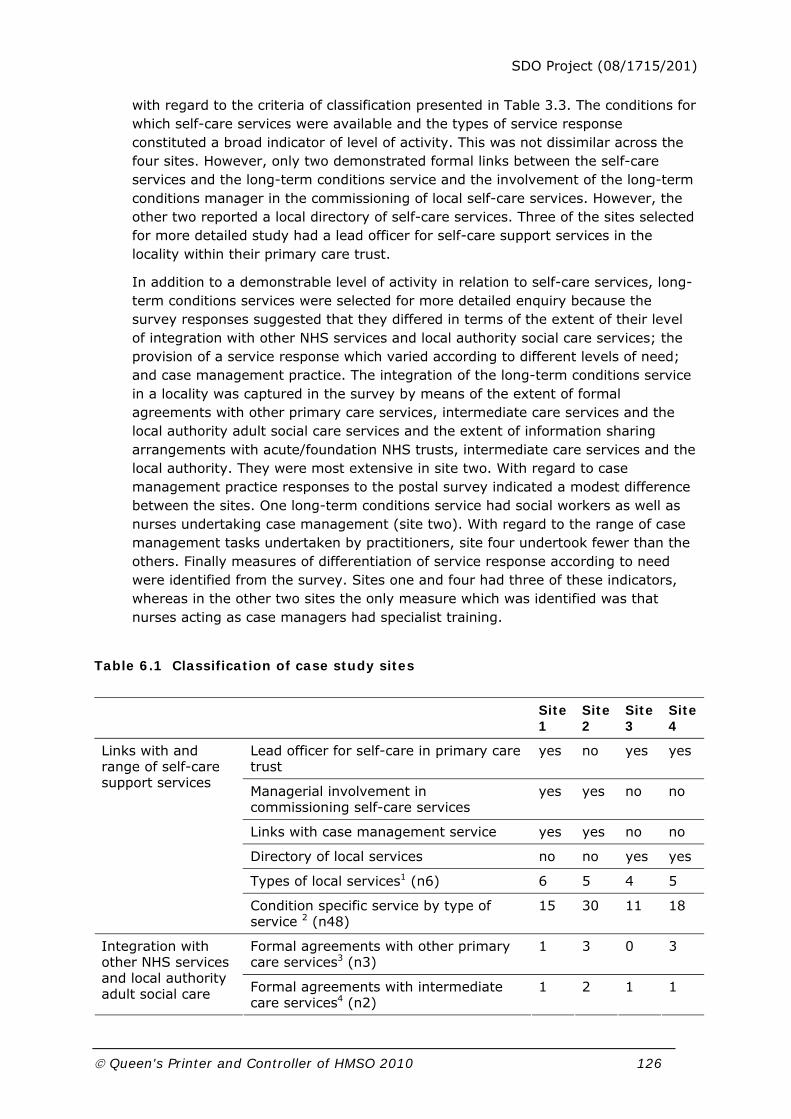
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 126
with regard to the criteria of classification presented in Table 3.3. The conditions for which self-care services were available and the types of service response constituted a broad indicator of level of activity. This was not dissimilar across the four sites. However, only two demonstrated formal links between the self-care services and the long-term conditions service and the involvement of the long-term conditions manager in the commissioning of local self-care services. However, the other two reported a local directory of self-care services. Three of the sites selected for more detailed study had a lead officer for self-care support services in the locality within their primary care trust.
In addition to a demonstrable level of activity in relation to self-care services, long-term conditions services were selected for more detailed enquiry because the survey responses suggested that they differed in terms of the extent of their level of integration with other NHS services and local authority social care services; the provision of a service response which varied according to different levels of need; and case management practice. The integration of the long-term conditions service in a locality was captured in the survey by means of the extent of formal agreements with other primary care services, intermediate care services and the local authority adult social care services and the extent of information sharing arrangements with acute/foundation NHS trusts, intermediate care services and the local authority. They were most extensive in site two. With regard to case management practice responses to the postal survey indicated a modest difference between the sites. One long-term conditions service had social workers as well as nurses undertaking case management (site two). With regard to the range of case management tasks undertaken by practitioners, site four undertook fewer than the others. Finally measures of differentiation of service response according to need were identified from the survey. Sites one and four had three of these indicators, whereas in the other two sites the only measure which was identified was that nurses acting as case managers had specialist training.
Table 6.1 Classification of case study sites
Site 1
Site 2
Site 3
Site 4
Lead officer for self-care in primary care trust
yes no yes yes
Managerial involvement in commissioning self-care services
yes yes no no
Links with case management service yes yes no no
Directory of local services no no yes yes
Types of local services1 (n6) 6 5 4 5
Links with and range of self-care support services
Condition specific service by type of service 2 (n48)
15 30 11 18
Formal agreements with other primary care services3 (n3)
1 3 0 3 Integration with other NHS services and local authority adult social care Formal agreements with intermediate
care services4 (n2) 1 2 1 1

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 127
Formal agreement with local authority social care services
no yes no no
Information sharing arrangements with acute/foundation NHS trusts5 (n11)
3 6 2 3
Information sharing arrangements with intermediate care services5 (n10)
0 3 2 2
services
Information sharing arrangements with local authority5 (n10)
2 3 3 1
Case management practice
Range of tasks in addition to assessment6 (n7)
5 5 5 2
Social workers within long-term conditions service
no yes no no
Caseload size 30 or less yes no no no
Allocation criteria: intensity of involvement
yes no no yes
More than 50% of caseload visited weekly
no no no yes
Service response differentiated according to level of need
Case managers include nurses with specialist qualifications
yes yes yes yes
1Types of local services: being able to talk to someone, information leaflets, special equipment, self-care support training, informal self help group, alternative therapies
2Conditions: asthma, chronic obstructive pulmonary disease, diabetes, hypertension, coronary heart disease, stroke and transient ischemic attack, musculoskeletal, multiple conditions
3Primary care services: nursing, pharmacy and physiotherapy
4Intermediate care services: schemes to prevent admission and facilitate discharge
5Information sharing arrangements: Joint access to computerised client record systems; case managers have access to hospital patient records; multi-disciplinary locality meetings; via a designated person; shared assessment documents within or outside the Single Assessment Process; shared review documents; single case file; exchange of written information; patient-held records and disease registers (acute/foundation NHS trusts only)
6Range of tasks in addition to assessment: financial assessment; care planning; arranging services; implementation of care plan; budget holding; monitoring the care plan; reviews
Table 6.2 provides some contextual information about each of the case study sites. At the time the fieldwork was undertaken in the summer of 2008 each of the case management services for people with long-term conditions had been in existence for at least eighteen months and in site four it had been operational for four years. Each service was provided by teams based in primary care trusts and three had multiple service delivery arrangements. These also provided a disease based service and two had practitioners linked with GP practices. One (site three) operated a part of its case management service for people with long-term
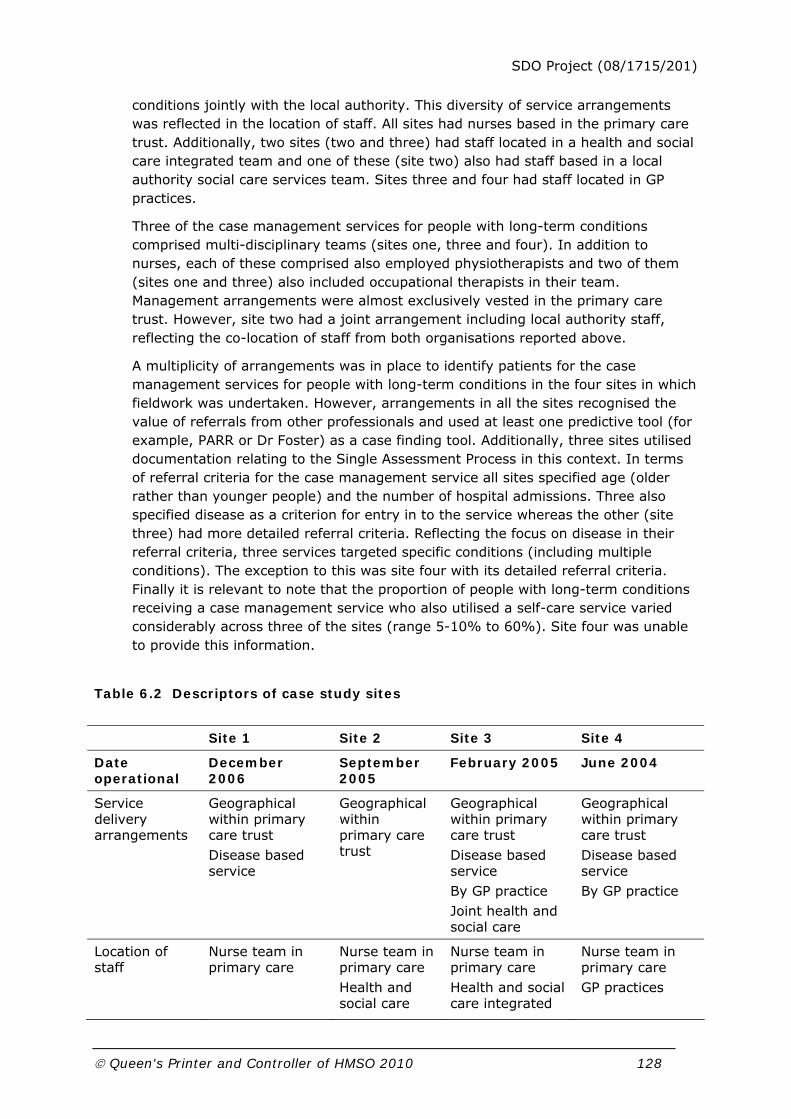
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 128
conditions jointly with the local authority. This diversity of service arrangements was reflected in the location of staff. All sites had nurses based in the primary care trust. Additionally, two sites (two and three) had staff located in a health and social care integrated team and one of these (site two) also had staff based in a local authority social care services team. Sites three and four had staff located in GP practices.
Three of the case management services for people with long-term conditions comprised multi-disciplinary teams (sites one, three and four). In addition to nurses, each of these comprised also employed physiotherapists and two of them (sites one and three) also included occupational therapists in their team. Management arrangements were almost exclusively vested in the primary care trust. However, site two had a joint arrangement including local authority staff, reflecting the co-location of staff from both organisations reported above.
A multiplicity of arrangements was in place to identify patients for the case management services for people with long-term conditions in the four sites in which fieldwork was undertaken. However, arrangements in all the sites recognised the value of referrals from other professionals and used at least one predictive tool (for example, PARR or Dr Foster) as a case finding tool. Additionally, three sites utilised documentation relating to the Single Assessment Process in this context. In terms of referral criteria for the case management service all sites specified age (older rather than younger people) and the number of hospital admissions. Three also specified disease as a criterion for entry in to the service whereas the other (site three) had more detailed referral criteria. Reflecting the focus on disease in their referral criteria, three services targeted specific conditions (including multiple conditions). The exception to this was site four with its detailed referral criteria. Finally it is relevant to note that the proportion of people with long-term conditions receiving a case management service who also utilised a self-care service varied considerably across three of the sites (range 5-10% to 60%). Site four was unable to provide this information.
Table 6.2 Descriptors of case study sites
Site 1 Site 2 Site 3 Site 4
Date operational
December 2006
September 2005
February 2005 June 2004
Service delivery arrangements
Geographical within primary care trust Disease based service
Geographical within primary care trust
Geographical within primary care trust Disease based service By GP practice Joint health and social care
Geographical within primary care trust Disease based service By GP practice
Location of staff
Nurse team in primary care
Nurse team in primary care Health and social care
Nurse team in primary care Health and social care integrated
Nurse team in primary care GP practices

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 129
integrated team Local authority social care team
team GP practices
Staff mix Nurses Physiotherapists Occupational therapists
Nurses Nurses Physiotherapists Occupational therapists
Nurses Physiotherapists
Management arrangements
Health services Health services Local authority
Health services Health services
Patient identification
Other professionals SAP documents PARR I Dr Foster
Other professionals SAP documents PARR II Hospital A & E data
Other professionals SAP documents PARR I & II Combined predictive model Patient records
Other professionals Dr Foster Patient records Disease registers
Referral criteria
Age Number of hospital admissions Disease
Age Number of hospital admissions Disease
Age No. hospital admissions Polypharmacy Falls Risk of medical decline Loss of ADLs Frequent GP contact Frequent ambulance call out Multiple A & E attendances No recent review of multiple needs Bereavement
Age Number of hospital admissions Disease
Targeting of conditions
CHD Neurological Asthma COPD Diabetes
CHD Neurological Asthma COPD Hypertension Multiple conditions
None CHD Neurological
Proportion 5-10% 60% 30% Not known
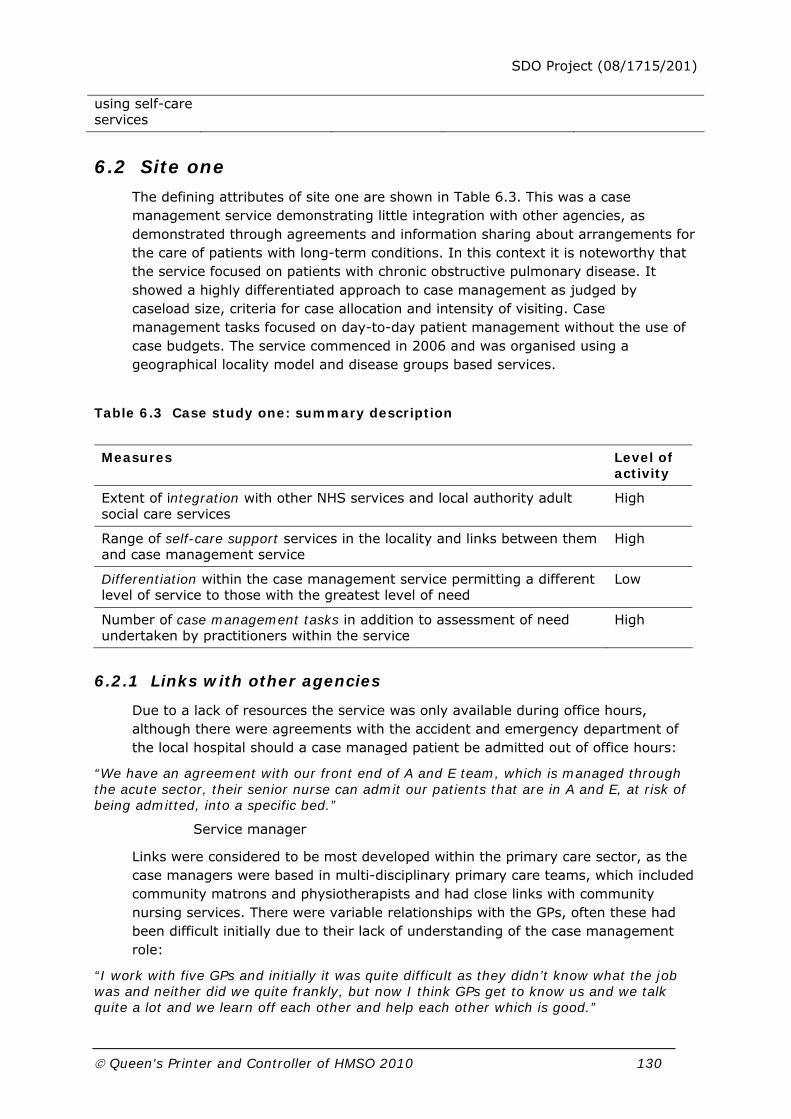
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 130
using self-care services
6.2 Site one
The defining attributes of site one are shown in Table 6.3. This was a case management service demonstrating little integration with other agencies, as demonstrated through agreements and information sharing about arrangements for the care of patients with long-term conditions. In this context it is noteworthy that the service focused on patients with chronic obstructive pulmonary disease. It showed a highly differentiated approach to case management as judged by caseload size, criteria for case allocation and intensity of visiting. Case management tasks focused on day-to-day patient management without the use of case budgets. The service commenced in 2006 and was organised using a geographical locality model and disease groups based services.
Table 6.3 Case study one: summary description
Measures Level of activity
Extent of integration with other NHS services and local authority adult social care services
High
Range of self-care support services in the locality and links between them and case management service
High
Differentiation within the case management service permitting a different level of service to those with the greatest level of need
Low
Number of case management tasks in addition to assessment of need undertaken by practitioners within the service
High
6.2.1 Links with other agencies
Due to a lack of resources the service was only available during office hours, although there were agreements with the accident and emergency department of the local hospital should a case managed patient be admitted out of office hours:
“We have an agreement with our front end of A and E team, which is managed through the acute sector, their senior nurse can admit our patients that are in A and E, at risk of being admitted, into a specific bed.”
Service manager
Links were considered to be most developed within the primary care sector, as the case managers were based in multi-disciplinary primary care teams, which included community matrons and physiotherapists and had close links with community nursing services. There were variable relationships with the GPs, often these had been difficult initially due to their lack of understanding of the case management role:
“I work with five GPs and initially it was quite difficult as they didn’t know what the job was and neither did we quite frankly, but now I think GPs get to know us and we talk quite a lot and we learn off each other and help each other which is good.”

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 131
Community matron
There was confirmation that these initial difficulties had been largely overcome over time, in part due to the GPs recognising the benefits that case management had brought to their patients:
“I think he's seen the benefit, the community matron is making a difference… to patient care and quality of care, and he's so passionate about that… So I think that’s why.”
Service manager
It was felt that the good relationship between GPs and case managers led to prompter responses when patients required attention:
“A good example would be a community matron asked to go and see a patient by a GP, goes to see the patient, thinks: ‘Oh my goodness, this is really serious’, phones the GP and the GP comes straight out on a home visit a joint visit with the community matron. So once the relationship is there and the trust is there, it's very good.”
Service manager
One GP had become involved in supporting the community matrons’ professional development through mentoring.
As well as the agreement over case managed patients having access to a hospital bed, there were links with acute care services through case managers being involved in multi-disciplinary team meetings with hospital-based colleagues and there was a designated contact person with whom the case managers shared information.
The professional background of some of the case managers and managerial personnel was also thought to contribute to informal links with other local service providers:
“…Some of us have been around a long time in different roles and bring knowledge and expertise from different roles, so we've had these relationships in different ways with different people. For instance, my Director used to be the Joint Head of Older Peoples’ Services across the hospital and the primary care trust and she’d brokered really good relationships with the local authority and jointly funded posts and things like that… those relationships are still there.”
Service manager
However, relationships with practitioners in the local authority were less developed. Whilst there were some managerial joint posts, plans to co-locate services had not materialised, as the cost of renting the building had proved too costly for the local authority:
“This building is a great example as were all supposed to be here together but it’s too expensive so the local authority aren’t based here, so the logistics of it make it hard. You know if you pass people in the corridor it jogs the memory and makes the whole process smoother.”
Service manager
This had limited joint working and communication. There had been recent cuts in budgets that had further impacted on the potential to develop integrated work priorities but despite these challenges the service manager remained optimistic:
“I think because of the financial situation, both for the primary care trust and now for the local authority, who've been asked to make some swingeing savings that has caused

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 132
some challenges. But it's interesting, the way we're looking to address that is: ‘We know that if you can't provide that any more that’s going to have this impact on health, we need to do an impact assessment and bring it together and jointly look at what we're going to do to address that’, rather than: ‘We're not doing it. You’ve got to do it.’ So I think that although it might be rocky at the moment, I think that partnerships will improve I think. I don't think they will get worse.”
Service manager
Local authority budgetary constraints were also noted by case managers:
“The physio assesses and then social services say: ‘No, we don’t have the money’ so that comes back on the NHS. It’s all so disjointed and fragmented.”
Case manager
Patient information was exchanged by letter and multi-disciplinary meetings between practitioners in the local authorities and colleagues in the case management services.
Agreements with intermediate care services to prevent inappropriate admissions to hospital for case managed patients were under discussion. Within the intermediate care sector there were also schemes to facilitate early discharge from hospital. There were close links with the End of Life care co-ordinator due to one community matron being dedicated to nursing homes where this person was implementing the approach to palliative care known as the Gold Standard Framework.
6.2.2 Self-care support services
The self-care initiatives in the primary care trust were being led by the Public Health Department although the case management service manager had formal links with their strategy group and specifically with the patient participation manager whose role was to develop patient focused services and promote self management support services:
“Public health are really, they are, leading on the self-care, self management agenda for the primary care trust, and I sit on their strategy group.”
Service manager
Although the common location did not appear to have facilitated links with the local authority it had allowed links to develop with voluntary organisations:
“They [Diabetes UK] had a stand here every Thursday when we have our integrated diabetes clinics. So the links are there, they're very visible, they have notice board availability around. So we're trying to promote access to voluntary organisations.”
Service manager
Case managers were also invited to the voluntary organisation service planning meetings. The services provided by voluntary organisations were varied including information and advocacy as well as services providing direct support. These were thought to be both patient centred and patient led, albeit with professional support.
6.2.2.1 Self-care support provided by the primary care trust
The primary care trust offered a wide range of self-care support services including informal therapeutic intervention; accessible advice; technology to promote self-

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 133
care; generic self-care support training; alternative therapies; condition specific self-care support training; and self help groups:
“There is a stroke group and it’s patient centred. What we’re trying to do is say: ‘We can input and advise but it has to be your thing, it can go on for years but you have to run it.’ So they can manage the group themselves but we can input and advise.”
Service manager
The frequency of use of these services by case managed patients was variable, with most frequent access seeming to be to informal therapeutic advice and condition specific self-care support training, as well as alternative therapies, provided by the physiotherapy service.
The primary care trust provided the most services for chronic obstructive pulmonary disease and diabetes, including accessible advice and information, technology, self-care support training and self help groups. Coronary heart disease was provided for with accessible advice and information and technology and there was information available as well as a stroke group for those patients. Patients with musculoskeletal problems had access to advice and information as well as alternative therapies.
6.2.2.2 Self-care support provided by case managers
In this setting it was estimated that between five and 10 per cent of case managed patients were thought to be using self-care services. Doubts were expressed about the accessibility of some services for this group, particularly as to whether elderly people would be able to use supportive technology:
“The majority of elderly clients don’t get the computer or phone, they get mystified and can’t remember what option one was so I think those are real issues for people in self-care and self management.”
Case manager
However, case managers saw supporting self-care through patient education as an important part of their role:
“What I’ve found is when you go in and do an assessment, people are aware of chronic obstructive pulmonary disease but don’t have a clue what it is, so my first question is ‘Do you know what you’ve got, can you tell me?’ and then we break it down into small bits and it’s about empowering them to take charge.”
Community matron
The notion of empowerment was frequently referred to. The patient education provided by the case managers was reinforced by written information, a care plan, developed through a particular initiative for self-care in chronic obstructive pulmonary disease:
“It was suggested we put a bid in for something [to support self-care], we had a think about what we could do and we came up with chronic obstructive pulmonary disease. So it’s grown from there really, we got it and it’s particularly directed at elderly care…it’s a care plan. At the moment we are at the point where we are looking at the text and the wording in our leaflet.”
Case manager

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 134
The case managers felt that their caseload commitments were a barrier to them supporting patients to self-care, with an unavoidable emphasis on hospital discharge arrangements for their patients:
“But early discharge, all we’re doing is reacting. I want to work proactively. It hasn’t been possible.”
Case manager
Overall, there was a lot of interest and activity surrounding the support of self-care although the service manager thought that a culture of risk aversion in the NHS limited the potential for supporting self-care and this was particularly the case for those from an acute services background:
“I don't think it's around training the patients, I think it's about training our staff. And we've already identified that we have got a degree of risk averseness. And I do think that risk averseness and self-care go hand in hand. And I think it very much depends on your background, the amount of risk you're prepared to take. People with a very acute focus and background are much less likely to take risk than somebody who's had a great deal of community experience, because they know the risk that we can take and, the complexity and the severity of the disease that we can manage and safely manage, in the community.”
Service manager
Case managers would on occasion assess for entry to self-care and refer patients on to such services. They would usually contribute to the provision of self-care support services and sometimes contribute to the development of self-care support plans.
6.2.3 Staff mix and tasks
Case managers were located in multi-disciplinary teams in primary care with their line manager also being a primary care trust employee. The service manager would have liked a team of community matrons as she thought that this would lead to more cohesion and a better relationship with other agencies:
“My preference would be to recruit more community matrons, and base them in one team. I mean, working inter locality but if they're based in the same office you’ve got that cross working. I think probably if they were in a team together you would have better consistency and communication and collaboration with GPs and the hospital.”
Service manager
However, the service manager acknowledged the benefits from the community matrons being based in multi-disciplinary teams and co-located with other services:
“But we're fortunate to an extent that our community matrons are based in this office, and our therapy team is based in this office.”
Service manager
The multi-disciplinary team used specialist nurses (including those for multiple sclerosis and diabetes), community matrons and physiotherapists, many also with specialist roles, as case managers. There was flexibility within this, so if required, any case manager could bring in a nurse prescriber for a medications review:
“Each of our community matrons and even the case managers do have areas of special interest. And, so they would, if they weren't sure, they'd say to X____: ‘You're a tissue viability expert, can you come and give me an opinion.’

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 135
Interviewer: Right. So you're sharing information?
They share information and also you can learn from that person, so that the next time, it's just improving your skills as you're going along.”
Service manager
This consultation amongst the team allowed for individual case managers skills and knowledge to develop.
There was no current programme of training for case managers although the service manager had identified information technology as a training need, particularly for nurses:
“… some of our community matrons, they're really good with computers, others are petrified of them and I think it's a training need… If you're used to using a computer you can speedily put stuff on but if you're petrified of it, it takes you forever. So it is a training need, but that’s a training need across the board, particularly in nursing services. Therapy’s much more up to speed, much more.”
Service manager
Two of the community matrons had attended courses at local universities that appeared to be the same course but turned out to be different depending on which institution the course had been carried out.
“But, interestingly… if you look at the courses that they're both taking, they are totally, totally different. So we are getting no consistency here at all. One... They’ve gone to two different universities and they are poles apart in what they are receiving.”
Service manager
Consistency between institutions in terms of course content was perceived to be beneficial. However, the service manager did not think that all case managers required training to the same level and in the same specialisms:
“I don't for one minute think everybody needs to do the independent prescribing. And I actually, my personal view [is] it's a real waste of investment because most of the time these guys will be prescribing one or two types of antibiotic, nothing much more, and I can't understand why aren't we dealing with this under the patient group directive, rather than putting these people on three month courses to learn, pharmacology and pain pathways and things like that, that GPs don’t even know.”
Service manager
Training for case managers to support self-care, as described above, was thought to be a need with a focus on risk management.
All case managers carried out assessment, care planning, care plan implementation and monitoring, reviews, patient advocacy and clinical oversight. However, services were not costed and managers did not exercise any financial management responsibilities in this context. There was a perception that the case managers were all involved in direct care, particularly the community matrons:
“For the community matrons, I'd say they are, initially, very hands-on because it's the advanced assessment and it’s about trying to get that patient stable.”
Service manager

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 136
6.2.4 Process of case management
6.2.4.1 Patient identification
Referral criteria included age, hospital admissions and disease group. This targeting of specific conditions was seen as specifically the role of the community matron case managers and due to their low numbers only chronic obstructive pulmonary disease was directly targeted. This was seen by the case managers as the most important condition to target due to the high levels of service use amongst these patients:
“Because there are only four community matrons we look at chronic obstructive pulmonary disease because that is the type of patient who gets exacerbations, recurrent infection and goes into hospital a lot.”
Community matron
The identification of patients was generally through referrals from other professionals. The PARR tool was available through the primary care trust and information could be requested but there was a lack of administrative support to generate this information regularly:
“What the community matrons do is they have very close links with their GPs, and they also visit A and E, and the medical assessment unit regularly and go into the hospitals. It's professional to professional. Although I'm hoping that somebody will sort out PARR for me.”
Service manager
The service manager perceived the usefulness of PARR not in being through the identification of the very highest intensity users but of those falling in a broader high use category:
“…the top 20 very high users of A and E had been identified, and we looked at those patients to see do we know them or whatever. And of the top 20 patients, most of them were either out of the area, had mental health problems or substance misuse problems. If they didn’t have that, then they were known to our community matrons. Well, my personal view is you ignore them. You know, you'll never... You're not going to change that. So we've now asked for, and are just about to get the top 200. And what we'll do is we'll cross reference those against what's on our caseload and then they’ll go: ‘Right. Who haven't we got? And can we do anything about them?’”
Service manager
Cases were allocated by geography, rather than any other criteria:
“The community matrons are locality based; they case manage whoever is in their locality.”
Service manager
6.2.4.2 Assessment
FACE, a nationally accredited tool for assessing older people, and a disease specific assessment for patients with chronic obstructive pulmonary disease to facilitate early discharge were used by case managers within the Single Assessment Process.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 137
6.2.4.3 Care planning
Care plans did not detail the contribution made by primary, intermediate, acute and social care services. Case managers could not assess for or authorise any local authority funded services.
6.2.4.4 Monitoring and review
The caseloads were comparatively small compared to other case study sites, at 30 patients per case manager:
“On the whole it's 30 but the target is 60, which, in my personal view I think is ridiculous. If you're doing complex case management 60 is hugely high.”
Case manager
One of the community matrons had a caseload of 50 active cases, thought to be as a result of a good relationship with GPs:
“Our community matron has got 50 active people. These are truly active cases so she's pulling her hair out…
Interviewer: How has she ended up with 50?
Good rapport with the GPs, I think she's been very proactive in what she's done, the primary care trust have seen what are the local benefits of the community matrons can be.”
Service manager
Case managers tended to remain responsible for each case for its duration although there was the potential for input from other case managers depending on specialism. The frequency of visits was determined by the needs of the patient:
“It's triggered, by the clinical needs analysis really and assessments. So if somebody needs to be seen daily then they’ll see them daily if they think: ‘This is a weekly or I'm going to phone them on a monthly basis.”
Service manager
Reviews were initiated by the case managers unless the patient had been discharged from the service and then a crisis or admission had occurred:
“It [the review] would be initiated by us, predominantly. I think if it's initiated anywhere else it'd be because we've discharged them and then something had happened, a crisis, and somebody else was involved. Or there might be a review because the patient perhaps had suddenly pitched up at A and E or in the hospital, and they'd say I used to have that nice community matron. And they, they would then contact us and say could we come and pick up and support them back out.”
Service manager
Reviews were generally carried out face-to-face with the patient or over the telephone. Information was sought from the carer where there was one. Despite the reference to discharge there was very little actual case closure across the service, but patients were discharged if they had required no contact for several months:
“If we've got to a situation whereby, there’s been no contact for three months then, we'll be giving them a ring to see if they're okay. If they haven't been seen for three, six months then we will probably discharge them… when they're discharged they will always be given our number and said: ‘Look, if anything changes you can phone straight back.’”

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 138
Service manager
Patients could directly re-access the service if their circumstances changed.
6.2.5 Information systems
The case management service had its own electronic database, although this was little used by case managers, which was thought to be due to time pressures:
“Interviewee: We have a database for community matrons that was designed specifically for them. And they don’t use it, they really don’t.
Interviewer: Why not?
Interviewee: And I think probably it's a time pressure thing around it, but we will, within the next few months be on Rio… everybody in X____ is on Rio, our children’s services are on Rio, our therapy service is on Rio, our district nursing service and our other nursing services are the next to go. So that’s going to make for better reporting systems.”
Service manager
This system was not currently linked to other systems but it was thought that planned changes would allow for better information sharing at least within the primary care trust. The details that were stored about patients currently were their personal details; ethnic origin; medical information; diagnoses; case management input and reviews.
The service manager further saw improved information systems as a mechanism for demonstrating performance to be used to support service tenders:
“We really have to prove our performance, data has to improve, otherwise we're not going to get commissioned and you can't prove you're doing it cost-effectively. So, at the moment we are jumping up and down about that, very proactively.”
Service manager
6.3 Site two
The summary features of site two are shown in Table 6.4. This was a primary care trust which displayed a high degree of integration with other agencies as demonstrated through agreements and information sharing. The service showed low levels of differentiation within the case management process as indicated by caseload size, method of case allocation and intensity of visiting. Higher level case management tasks were in evidence, as well as routine care activities. Case management tasks were of day-to-day patient management without the use of case budgets. The service commenced in 2005 and was based on a geographical location model.
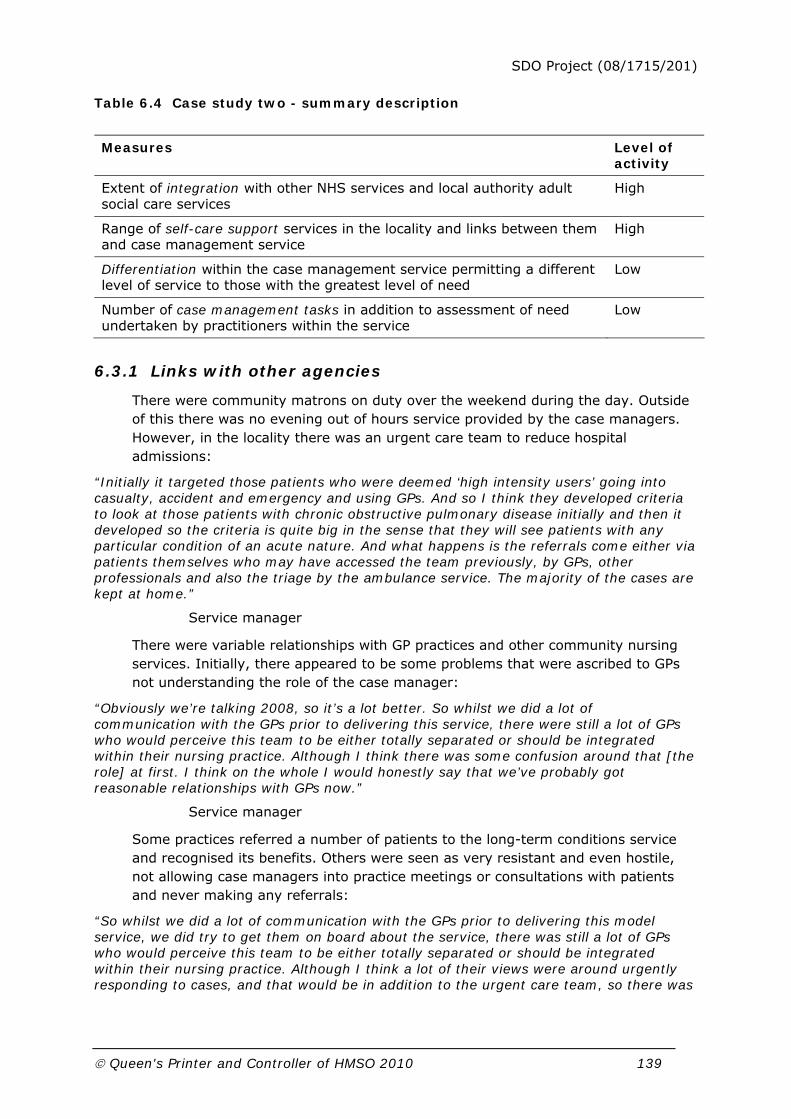
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 139
Table 6.4 Case study two - summary description
Measures Level of activity
Extent of integration with other NHS services and local authority adult social care services
High
Range of self-care support services in the locality and links between them and case management service
High
Differentiation within the case management service permitting a different level of service to those with the greatest level of need
Low
Number of case management tasks in addition to assessment of need undertaken by practitioners within the service
Low
6.3.1 Links with other agencies
There were community matrons on duty over the weekend during the day. Outside of this there was no evening out of hours service provided by the case managers. However, in the locality there was an urgent care team to reduce hospital admissions:
“Initially it targeted those patients who were deemed ‘high intensity users’ going into casualty, accident and emergency and using GPs. And so I think they developed criteria to look at those patients with chronic obstructive pulmonary disease initially and then it developed so the criteria is quite big in the sense that they will see patients with any particular condition of an acute nature. And what happens is the referrals come either via patients themselves who may have accessed the team previously, by GPs, other professionals and also the triage by the ambulance service. The majority of the cases are kept at home.”
Service manager
There were variable relationships with GP practices and other community nursing services. Initially, there appeared to be some problems that were ascribed to GPs not understanding the role of the case manager:
“Obviously we’re talking 2008, so it’s a lot better. So whilst we did a lot of communication with the GPs prior to delivering this service, there were still a lot of GPs who would perceive this team to be either totally separated or should be integrated within their nursing practice. Although I think there was some confusion around that [the role] at first. I think on the whole I would honestly say that we’ve probably got reasonable relationships with GPs now.”
Service manager
Some practices referred a number of patients to the long-term conditions service and recognised its benefits. Others were seen as very resistant and even hostile, not allowing case managers into practice meetings or consultations with patients and never making any referrals:
“So whilst we did a lot of communication with the GPs prior to delivering this model service, we did try to get them on board about the service, there was still a lot of GPs who would perceive this team to be either totally separated or should be integrated within their nursing practice. Although I think a lot of their views were around urgently responding to cases, and that would be in addition to the urgent care team, so there was

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 140
some confusion around that at first. I think on the whole I would honestly say that we’ve probably got reasonable relationships with, GPs across the whole of the city now.”
Service manager
Relationships were felt to have improved once GPs saw successes with their patients:
“And certainly the successes that we’ve had with those ‘high intensity user’ patients, well they can’t deny those.
Interviewer: But you felt they had to see it working?
I think that’s just on an individual basis. The GPs now embrace the community matrons into their practice meetings, the community matrons go along to any multi-disciplinary meetings especially in relation to palliative care patients. They’ve seen that they’ve got a lot to contribute to early discharges or at least supportive discharges and also the link with secondary care.”
Service manager
The background of case managers was thought to play an important role in the relationships with other agencies:
“We have specialist nurses from there [the acute trust], so their links alone have helped as well, because they find it easier to go back to secondary care where I would say that the staff that were predominantly, and have a background in community care find it easier to approach GPs, social workers etcetera.”
Service manager
This was supported by one case manager from an acute background saying that she felt very comfortable speaking to consultants in the hospitals but felt unsure of how to deal with GPs and thought this had facilitated the strong links the service had with the acute trust. The service manager had herself come from an acute background:
“Well you see my background was X____ acute trust so in fairness that was a strength that I already had because I had the links, so when we developed the community matrons it was relatively easy to go back to colleagues who were working in secondary care to ask for their support and some kind of cooperation. So we do have strong links with accident and emergency services. We have strong links, we’ve got links with the cardiology team and the respiratory team, diabetes teams.”
Case manager
On a day-to-day basis there were generally good relations with social workers who case managers mainly got to know through their patients, carrying out joint visits as required. Case managers could not authorise any local authority services although it was thought this would be very useful. They could refer people to a respite service run by the local authority.
At a strategic level, joint primary care trust and local authority posts had been introduced and at practice level joint health and social care worker posts had been introduced:
“We have a joint development where we have health and social care workers. So the training of those workers, because they’re employed by the local authority but they will be working and delivering some of the health care, that was a joint programme that was put together by the trust, working very closely with quite a number of, and a range of people across social services to develop.”
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 141
Service manager
There were formal agreements with the intermediate care service to access beds for which criteria had been agreed:
“It works very well. We do have an intermediate care area which we can access for respite purposes so it’s kind of respite and rehabilitation. And that works really well as well because we’ve been able to work together to look at the criteria for actually getting these patients admitted short term.”
Service manager
There were further links with End of Life services but this did not necessarily mean a patient was transferred to these services; the specialist team could assess and advise the case managers and other involved personnel:
“…when we talk about the palliative care aspect it could be that the specialist palliative care team have come in, given their advice, gave their support and then they step back out also because the community matron is case managing and supporting the district nurses in the delivery.”
Service manager
The service additionally had one weekly dedicated physician session for heart failure patients.
6.3.2 Self-care support services
The primary care trust did not have a designated lead for self-care support but the case management service manager had been involved at strategic level through audit activities:
“Well across our directorate we’ve developed…an integrated audit tool that looks at all the aspects of essence of care. So things like communication, self-care, incontinence, nutrition, environment and anything else that we’ve decided then to tag on to it, so equality, diversity, etcetera. Each of the senior team were then given an area to lead and I did have self-care as an area for me… so because of my attachment to that part of the audit tool I’ve now become involved in, a self-care project with the Organisation and Development Department.”
Service manager
There were links with voluntary organisations at both strategic and practice level:
“We have a visit to the Age Concern department scheduled on everybody’s induction and that so they go and they access that. And also the Age Concern manager is also on many of those integrated meetings with social services. So we probably do have a lot of informal links and it’s an area that the community matrons do access quite often.”
Service manager
The case managers thought they had generally good relationships with Age Concern and a couple of other local voluntary organisations. It was felt that many case managed patients needed social support rather than self-care support and could benefit more from befriending services.
6.3.2.1 Self-care support provided by the primary care trust
The primary care trust offered self-care support services including informal therapeutic intervention; accessible advice, technology to promote self-care;

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 142
generic self-care support training, condition specific self-care support training; self help groups and alternative therapies. Case managed patients were thought to frequently access informal support and advice and information. Condition specific training and technology to support self-care were also frequently used. Patients were thought to sometimes access generic self-care support training and self help groups.
The primary care trust provided specific services for asthma; chronic obstructive pulmonary disease; diabetes; hypertension and coronary heart disease. There was informal therapeutic support and advice and information available for all these conditions and all patients could access generic self-care support training. Technology was available for asthma, chronic obstructive pulmonary disease, diabetes and coronary heart disease as was condition specific self-care support training. There were self help groups for patients with asthma and coronary heart disease.
As noted in Table 6.2, 60 per cent of case managed patients were estimated to be using some form of self-care support.
6.3.2.2 Self-care support provided by case managers
Supporting self-care was perceived by case managers as a key part of their role. They had often been the first person to give information to patients about their condition even though they may have had the illness for many years. One case manager described sitting down and explaining what chronic obstructive pulmonary disease meant with a patient, how it affected them physically and what they could do to help themselves. The patient had been attending a clinic for years but had never received this basic information. Giving information to carers was seen as just as important, as they were providing the bulk of the direct care and were better equipped through the receipt of information. The case managers all had access to resources to provide information and education to patients.
Although the Expert Patient Programme was available, case managers did not think it was suitable for their patients due to their inability to attend meetings because of poor health and limited mobility. Expert Patient Programme was seen as being attractive to a certain type of patient, more motivated and interested and with less severe problems. The perception of case managers was that there was little self-care support specifically aimed at older and case managed patients. It was felt that older people expected to be looked after and did not always have interest in helping themselves and furthermore, that that should be their choice. It was thought that an individual version of Expert Patient Programme where somebody was visited by a health educator at home for a few weeks may be useful. The benefits of group support were also acknowledged:
“…some of the value of the work that’s required is to have it in groups, so from a psychological side then some of the things won’t come out unless it’s in a group and some of the coping and being able to have that discussion about coping skills and a change in behaviour needs to be in groups.”
Case manager
However, there was a perception from the case managers that most of their patients would not be able to access such groups.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 143
The case managers were involved in a programme of telehealth about which there were mixed feelings. They thought that it would help some patients and some it would make more anxious and they would ‘abuse’ it to get the human contact that they wanted. The face-to-face contact with a professional was seen by many patients as being the most important bit, providing reassurance and social support:
“However I would say again a strong view of mine is that in the client group that we have of community matrons who are long-term people, we really try to promote self-care and to get them out of this medical model so that they’re not relying on their GP to tell them that they’re feeling unwell that day but would do the symptom management. So we don’t particularly sign up to putting these machines into everybody at the moment, we’ve done some extensive work looking at what groups of patients might be best helped with that.”
Service manager
There was concern from the service manager that case managers may not recognise self-care support when they implemented it:
“If the case manager for example decides to get a ‘Nomad’ system, a medication system in the patient’s home, well that is one of the key principles of self-medication but I don’t know that every team member would see that as being part of self-care. So what we’re hoping to do is to put some realistic, kind of examples in that, in each of those and promote some kind of training and development really to promote peoples awareness about what self-care is as well.”
Service manager
There were strong links with disease specific services such as cardiology, respiratory and diabetes and these services provided self-care support through rehabilitation programmes:
“I mean we did develop a lot of community-based pulmonary rehabilitation for those patients which has been really beneficial, because obviously it’s the medium kind of patients with the illness that access that and it was more the social contact and the activity… Likewise with the heart failure patients, because we developed heart failure rehab but the numbers are low.”
Service manager
Again, these programmes were not always thought to be suitable for all age groups and the service manager recognised that some issues would be more relevant for some groups of patients:
“Some of the content of the course itself, because it’s not just about exercise, it’s about the education to support that, is not tailored appropriately because you may not be laying particular emphasis on say having an active sexual relationship, returning to work, things like that for a older age group than what you would be for that younger age group.”
Service manager
6.3.3 Staff mix and tasks
The teams consisted of nurses managed by other NHS personnel although some that were involved in a joint project with the local authority were managed through that. The case managers would have preferred a broader skill mix in the team with occupational therapists and physiotherapists and a social worker as they perceived that would speed up access to such services. There was a strong sense of team membership, thought to have been acquired through working in the same office,

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 144
which allowed case managers to help each other out with particularly demanding cases. Despite this sense of team cohesion case managers reported that staff retention was an issue due to the demands of the post.
There was a training programme in place for case managers including advanced clinical skills and nurse prescribing. The service manager was hoping to address the perceived problem with case managers awareness of what self-care support actually was by developing training based on common principles:
“It would be for all community-based staff, however we need to target who is likely to benefit most from this, what we’re hoping to do is to develop a tool [for training] based upon...the common core principles to support self-care.”
Service manager
There was additional training to promote case managers’ support of self-care which consisted of a rolling programme of more specific short courses:
“Because what we have already got is training for all staff on a rolling programme to be able to come along for inhaler technique training because we recognise that not everybody can actually support a patient to have the appropriate technique if they haven’t had that appropriate training themselves.”
Service manager
There were tensions between the case managers and district nursing staff as it was thought the latter did not understand the case manager role and could not understand why the case managers would often not do clinical work such as change dressings when they were in visiting a patient and save the district nurse a visit. One case manager felt that she lacked the clinical skills now that she was no longer a district nurse as she had not kept up to date and techniques had changed. One contributing factor was that case managers wore a uniform. This led to an expectation that they would be carrying out more clinical work than they felt they should be doing, from both other professionals and patients. They were all striving to assess patient needs and co-ordinate care, before stepping back and managing the overall care package, but the clinical requirement to medically assess patients was felt to blur the boundaries and give the role more focus on direct care.
6.3.4 Process of case management
6.3.4.1 Patient identification
The service was targeted at several conditions including chronic obstructive pulmonary disease and coronary heart disease and referral criteria additionally included age and hospital admissions although the criteria were described by the service manager as ‘fairly open’. This site opted to create a case management team from an existing cardiology team:
“We decided to then look at having six case managers who are, actually, the Community Cardiology Nursing Team.”
Service manager
Although the process of patient identification included PARR and assessments made within the Single Assessment Process, a lack of administrative support for these systems meant that the information was often out of date:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 145
“PARR has been used but lack of admin support makes it difficult to track the people down once they are identified, this is very time consuming.”
Service manager
Most of the referrals came from other professionals; although patients could self refer and have done, usually when they have a friend or relative receiving the service.
Cases were allocated by GP practice and one problem with this was not being able to ensure that one case manager did not have a large proportion of patients requiring intensive support. However, an advantage of allocating patients in this way was that there was closer alignment with local authority colleagues:
“Because of the cluster base they are closely aligned and they should know at least the names of the [local authority] staff working within their areas.”
Service manager
6.3.4.2 Assessment
The Single Assessment Process was used with Easycare as the assessment tool.
6.3.4.3 Care planning
The case manager role included carrying out assessments, care planning, care plan implementation and monitoring, reviews, patient advocacy and clinical oversight. Financial management by means of costed care plans was not part of the case manager role. Case managers could not assess for, or authorise any local authority services.
Care plans usually contained the contribution of primary, intermediate and social care services, acute services were sometimes detailed.
6.3.4.4 Monitoring and review
The average caseload size was 42 although there was a large range. Case managers felt that although this was manageable and allowed flexibility to respond to changing needs, the target caseload size of 80 would be impossible to manage unless many of the cases were dormant. Case managers additionally commented that they were often covering more than their own caseload due to annual leave and sickness absence.
The manager described a system of case categorisation:
“This has got to have been the biggest problem we have with regards to identifying the caseload then keeping them active or inactive, the targets were set and we had to meet them. Because if we had 26 community matrons or case managers in X____ and they each had to reach 80 by the end of the last year that, we’re talking in excess of 2,000 patients on the caseload which was unmanageable. So what we’re now trying to do is to determine in a categorised system at what point in case management are these patients, so that we can inactivate but keep somebody on a caseload.”
Service manager
However, case managers thought that the categorisation system was only useful for data collection and did not actually help manage their workload, up to a quarter of whom were thought to be visited weekly. As cases were allocated by GP practice

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 146
there was no flexibility for ensuring that one case manager did not have a caseload containing patients with very high levels of need as well as those with intense needs.
There was usually continuity of care, although it was possible to bring in specialist nurses if required. It was felt that the individual relationship with the case manager was very important. One case manager spoke of how she had been on annual leave for a fortnight and was surprised how little her patients had contacted her temporary replacement in the interim. As soon as she returned they had all phoned her requesting she come out, as it was her as an individual they wanted to see, not any case manager.
The service manager was aware of the demanding nature of some of the cases and was encouraging group responsibility where possible:
“I must admit although there’s a named person for the case managed we are at the position now where we’re trying to encourage some kind of group cover because… these patients can be so intense and are so demanding that we can get ‘burn out’ across the teams and that’s a real bugbear of mine. We don’t want to put our staff in the position where we just wear them down because of the intensity of the client, especially because they’re long-term patients, it’s not a snapshot and then out again. So we’re trying to encourage the staff to ensure that the patients know that there’s cover and that there might be occasions where somebody else would visit rather than them.”
Service manager
Cases were reviewed using a variety of methods including face-to-face with the patient and multi-disciplinary, as well as using information from the carer. Cases were rarely discharged from the service. Case managers attributed this to the nature of the patient’s condition although occasionally they would be transferred into a disease specific service but never to supported self-care. Most discharges from the service were inappropriate referrals in the first place. If a patient was discharged they could fast track themselves back in and would keep the contact number of the case manager with whom they had been involved.
6.3.5 Information systems
The case management service did not have an electronic records system but used handwritten patient held records. This had caused difficulties in terms of liaison with GPs:
“Some GP practices would have preferred for the community matrons to have access into their EMAS systems and make entries onto their EMAS systems about visits etcetera, whereas because we’re centralised and we have an obligation to have case notes in a patient’s home with a case management plan etcetera, we’ve not been in a position where we wanted to perpetuate a separate communication process. We do communicate, by email, telephone, the usual letters and things as other services often do.”
Service manager
Community matron case managers did have limited access to data about their patients on hospital systems but this was very much a one-way process:
“The community matron team working within the primary care trust have access to the hospital information system so we have been able to work together with secondary care to allow us that access so they can tap into HISS to find out patients’ results… but not from the other way… there’s nothing to access really apart from our notes.”

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 147
Service manager
Although there was a perceived need for a centralised system, problems were anticipated with its maintenance:
“Interviewer: Do you think it would be easier if there was one centralised system?
Interviewee: It would be ideal… one of the difficulties is obviously around who would take ownership of that record and making sure that record was updated at all times etcetera and was accurate.”
Service manager
The written records that were kept included personal details; ethnic origin; medical information; assessment, care plan and review documentation.
6.4 Site three
Table 6.5 summarises the features of site three. This was a case management service with low integration with other agencies, as demonstrated through agreements and information sharing. There was low differentiation as judged by caseload size, allocation and intensity of visiting and lower level case management tasks. The service commenced in 2005 and used GP population; geographical locality; integrated teams and disease group models across the primary care trust.
Table 6.5 Case study three - summary description
Measures Level of activity
Extent of integration with other NHS services and local authority adult social care services
Low
Range of self-care support services in the locality and links between them and case management service
High
Differentiation within the case management service permitting a different level of service to those with the greatest level of need
High
Number of case management tasks in addition to assessment of need undertaken by practitioners within the service
Low
6.4.1 Links with other agencies
There was no specific out of hours service for case managed patients but access to out of hours community nursing which provided a 24 hour telephone number. Although this was universally available case managers would specifically liaise with the service if they thought a patient may need support outside of office hours:
“What they do as well is, if they’ve got people, the case managers, who are having a bit of a difficult time and who are likely to become unwell or anxious they do brief the out of hours teams to expect the call, share a copy of the care plan and the information and they have a discussion.”
Service manager
Those based in community clinics were felt to have good links with other professionals and the wider community:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 148
“We’re having a locality model involving all of those staff and those disciplines from all of these organisations working together to get to know the community, and they’re based in community centres. You know, so right in the heart of where the public, and the community lies and they’re listening, they’ll pick things up, anybody can refer and you know it’s just about sharing that intelligence.”
Service manager
The relationship with GPs was variable. Whilst there appeared to be initial problems, these improved over time:
“They were very difficult at first and I was, like, totally blanked but now I’ve got a really good relationship.”
Service manager
It was suggested that some GPs did not understand the role of the case manager:
“Interviewee 3: I don’t think they have a great understanding of our role. I think they’ve been told that we’re coming out to prevent hospital admissions and they think that that’s a bit of an insult, that they’re admitting too many people, so they get a bit like: ‘I’m not referring to you because you’re trying to stop me admitting people’.
Interviewer: So it gets their back up?
Interviewee 3: Yeah and it's not until you actually sit down and say: ‘Well I’m not, I’m trying to keep your patients well with you so hopefully they won’t need to go into hospital when you go and see them, we want to stop them getting to that stage.’ I think it's been how, how we’ve been put across to them, that’s caused the friction.”
Case manager
A further problem was the perception of GPs that case managers were generating more work for them:
“Interviewee 4: One of the problems is because we can go in and assess, but can’t meet those needs, is that we’re generating more work for GPs and they see that as us going out and creating more work for them.
Interviewee 2: But you’re not really, because they’d have to go out and see that patient if you hadn’t seen them.
Interviewee 4. Yeah but what I’m saying is by you going out and requesting that visit, they see that as you generating more work for them.
Interviewee 3: Because the patient’s not actually rung for them.
Interviewee 4: It probably would be identified later on when they’re at a more acute stage but they would be admitted.”
Case managers
One case manager was acting as a practice nurse as well as a case manager which she felt had made her relations with GPs better. There were some tensions with the district nurses over the tasks that could be expected of the case managers and there were also tensions over grading:
“Interviewee 3: And it causes a lot of problems with district nurses because we’re a band higher than the district nurses who manage a team of people and we don’t.
Interviewer: So does that cause conflict?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 149
Interviewee 3: It can do because we’re supposed to be integrating with them, we’re a band 7, they’re a band 6, they’ve got team members and we haven’t, so understandably it causes conflict.
Interviewer: What, what would your solution to that be, band yourself lower or…?
Interviewee 1: No higher.”
Case managers
Thus an increase in grading and advanced skills training was conceived of as a means of widening the gap between the district nurses and the case managers thereby resulting in less confusion over roles.
There was a formal relationship with the cardiology services in the acute trust as well as the community matron presence in the wards to identify suitable patients. Some of the case managers were co-located with intermediate care services which was thought to promote links, particularly with a scheme to prevent hospital admission.
The links with the local authority were perceived as the most significant due to the different services they could offer:
“Interviewee 3: It's very rarely you’re asking district nurses to do anything for you but you’re always asking social services to do things.”
Case manager
There was a multi-disciplinary integrated pilot project with other professional colleagues in operation in the locality which some of the case managers were involved in:
“Interviewee 1: I lead the pilot in the X_____ so my personal relationship is really good because we meet weekly, we have a two hour meeting every week to discuss, service users, patients and that sort of thing… so for me personally I have quite a good relationship with family services and stuff.”
Case manager
The pilot project involved the primary care trust, local authority, housing services, police, transport services and the benefits agency. Those not involved in this pilot had a less positive attitude towards colleagues in the local authority social services:
“Interviewee 3: They are very, very slow in at responding to your phone calls, responding to referrals.
Interviewee 2: They have no sense of urgency… it's so frustrating when somebody’s going to end up in hospital because you can’t get carers for them.
Interviewee 3: But saying that it doesn’t speed them up because there’s no come back from an admission to hospital for them when there is to us.”
Case managers
The conflicting priorities of the two services were highlighted here as admission to hospital did not have the same significance to the local authority as it did for the case managers. Clearly aligning the goals of the different services is essential to effective collaboration. Where there was a working relationship and individual social workers were known to the case managers this had a positive impact on the work they were able to do and encourage a greater degree of flexibility:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 150
“Interviewer: In your experience if you know these people face to face and you chat with them and all that, do you think that makes a difference?
Interviewee 1: Yeah, I think that because of that, they do things that are off the book, so I might refer somebody to Social Care Direct on the Monday, when I go to my Wednesday meeting they won’t have had the referral, but they’ll still come out with me and do the visit and then wait for the referral to come, but that’s because of the relationship we have.”
Case manager
There were links with End of Life services through liaison with district and Macmillan nursing services. A primary care trust funded community geriatrician was also available for advice and to receive referrals.
6.4.2 Self-care support services
The primary care trust did have a lead for self-care support and the Public Health Department were also involved in the development of the primary care trust self-care strategy.
Most of the case managers reported having contacts with voluntary organisations and had been involved in some of their activities, but some of this had stopped as due to the practice based organisation of case management services not everyone attending patient outreach activities would live in the catchment area for eligibility for the service:
“Interviewee 1: Once or twice we were asked to do the Ageing Day, but got told we couldn’t do them.
Interviewer: Why was that?
Interviewee 1: Because there were patients there who weren’t linked to our surgery.
Interviewer: So you might have been raising expectations?
Interviewee 1: Yes.”
Case manager
6.4.2.1 Self-care support provided by the primary care trust
The primary care trust offered self-care support services including accessible advice, technology to promote self-care; generic self-care support training, condition specific self-care support training and self help groups. Case managed patients were thought to frequently access advice and information; generic and condition specific self-care support training and self help groups. Patients sometimes used self-care support technology.
The primary care trust provided specific services for chronic obstructive pulmonary disease; diabetes; hypertension; coronary heart disease and stroke in the form of advice and information. There were self help groups for diabetes, coronary heart disease and stroke. Thirty per cent of case managed patients were estimated to be using some form of self-care support.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 151
6.4.2.2 Self-care support provided by case managers
Case managers usually assessed for self-care support needs and often referred people on to such services. Many of the case managers felt that supporting self-care was already part of their role:
“Interviewee 1: I think you try your best to keep people independent as much as possible, so you’re already providing some self-care to try and keep them as independent as possible, so I think it’s part and parcel of what we probably already do and already have done for years, you’re trying to make them more independent, I mean the last thing we want is somebody dependent on you 24 hours a day.
Interviewee 3: It's the old health nurse role isn’t it?”
Case managers
However, there was a perception that the age of many of the patients may prevent them from being interested in caring for themselves more:
“Interviewee 2: I think the idea of self-care is good for younger ones but when you get to 80 plus or whatever they don’t want the self-care really, they want to be looked after.”
Case manager
However, there was an acknowledgement that other patients may be interested in learning more about managing their condition.
One key area for self-care support was around medication management, including education, promoting understanding and adherence:
“You know a few things might come and go but on the whole they will never ever stop taking any form of medication. So that’s a huge area of concern and work for us... I can’t really describe and put enough emphasis on the problems and the issues we have with medicines management. It’s just around the reviews and making sure that the dosage is right, that the person understands the importance of the times and then looking at how that medication can be taken differently, the types of, products available so that they can take it and manage it better.”
Service manager
The importance of supporting carers was referred to by both the service manager and the case managers:
“It’s not just about the person it’s about the rest of the family as well so that they really truly understand what this disease is, or what these diseases are that they’re living with.”
Service manager
“Interviewee 1: Well, we always have had a lot to do with the carers … the things that you needed to know about the patient, but actually to also build that other relationship about giving those carers confidence to look after that particular person…
Interviewee 2: It's about knowledge, isn’t it? Education and knowledge. I’m talking about educating patients and their family.
Interviewee 1: But you also, if you’re going in to do that assessment, you need to get to know them and understand what they need in their capacity, because looking after somebody doesn’t come naturally just because you’re a family member or a carer. Some people it frightens to death.”
Case managers

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 152
There was an initiative using telehealth being carried out jointly with the local authority. There were concerns that it may cause anxiety in some patients, although there were others it was thought would benefit from it:
“I think we might start with a specific condition, I don’t know, like chronic obstructive pulmonary disease patients we would be able to do some remote surveillance but we’d have to very, pick very carefully. They’ll be a specific client group that that would be really suitable for, that it wouldn’t increase their anxiety and make them even more anxious… so some people will embrace it and there are others that just it wouldn’t ever be, useful for. “
Service manager
The case managers reported varying experiences with their patients using telehealth services:
“Interviewer: How do the patients get on with the systems?
Interviewee 4: Grand.
Interviewee 3: Well one of mine was supposed to use one because her husband had fallen and they rang down and said: ‘What can we do?’ she said: ‘My husband’s fallen, I can’t get him up off floor’, ‘Right, I’ll send you an ambulance’ and she said: ‘Well I could’ve done that’.
Interviewee 3: Yeah he’d gone again, the same night, she didn’t buzz it, she rang her relatives because she felt she was bothering somebody and when they raised them they had to ring an ambulance anyway which was the idea of giving her it, so she didn’t do that.”
Case managers
There was already a text messaging service for this group although it was felt more useful to younger patients who were familiar with mobile telephones.
The case managers often referred patients on to other services that supported self-care. These were either disease specific services within the NHS, for example, pulmonary rehabilitation or voluntary organisations such as Age Concern, that offered a range of services to support independent living. These services had become the target for further funding from the primary care trust:
“It’s been recognised that there’s been significant underdevelopment and under-funding in voluntary organisations and development so we are outliers really, but as an organisation and certainly through the joint strategic partnership and planning board, we’re investing heavily now, as in millions of pounds, because we just can’t cope without them. You know they do shopping services, they’ll do pop in and you know absolutely tonnes, gardening schemes, handyman schemes, things that are so crucial to support people to stay in their home.
Interviewer: That nobody else does?
That nobody else does. We’ve had some fantastic projects and some good successes but it’s always been time-limited. You know that’s really frustrating.
Interviewer: Because funding is so short term?
Absolutely. But we’re trying to move into the longer term.”
Service manager
There was an Expert Patient Programme available in the area but it was not felt to be of relevance to the majority of case managed patients:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 153
“Interviewee 4: I haven’t got any of my patients that have done the Expert Patient Programme, I know about the Expert Patient Programme, I think the ones that tend to go on that are the ones that are interested in self-care anyway so therefore would not necessarily need us to do it.
Interviewee 1: And they’re not housebound ones, we tend to see a lot of housebound
Interviewee 2: These are, kind of, beyond Expert Patient, I think sometimes they’re the ones who have already decided to take control of their own conditions, where as we’re, kind of, in there almost with the ones that can’t or haven’t got the motivation to do it.”
Case managers
The case managers had some involvement with groups providing self-care support either through delivering formal sessions or attending more informally and had had some involvement with the development of self-care support programmes.
6.4.3 Staff mix and tasks
The teams were based in GP practices, integrated teams and nurse teams in primary care with their line manager also being a primary care trust employee. It was multi-disciplinary and included occupational therapists and physiotherapists as well as nurses, particularly for people with neurological conditions. No social workers were employed as case managers although this was something the service manager was keen to do in the future:
“We’ve not taken any social workers. That was something that we discussed initially but the organisations weren’t ready. I mean that would have been a tremendous leap and step forward.
Interviewer: Is that something you’d like to see in future?
Absolutely. Particularly through the experience that the [integrated pilot project] has provided, yes, I would really embrace that, absolutely.”
Service manager
There was a programme of training being delivered through higher education including long-term conditions and nurse prescribing. The case managers would have preferred more individual training to build on their own specialisms and experience:
“Interviewee 2: We’ve all, we’ve all come from different specialities and the training and needs are all different…
Interviewee 3: It's not recognised that we have specialisms… we have pre-heart failure community matrons and they work in a specialist area, the rest of us don’t work specialist, even though we might have all different specialities like Neuro and we’ve got Palliative Nurses and things like that, but we all still provide the same service.”
Case managers
“Interviewee 3: I think we’d be better off being more specialised because having a bigger interest in a smaller area is a lot easier than having a little interest in lots of areas.
Interviewee 1: Yeah and you can tap into those, instead of like, being a little bit of everything, you just tap into each other’s expertise.”
Case managers
Despite reporting that they would prefer individual training, case managers raised the problems caused by them not having attended similar training to each other:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 154
“Interviewee 2: You see that’s the problem there’s some of us that do prescribe but I haven’t got my Advanced Team Skills, I can’t listen to somebody’s chest, so I can’t tell them they’ve got a chest infection other than that they’re coughing, but I can prescribe, so my frustration is that that’s cut in half my work, I can’t, I’m very frustrated as to what I can do. I’m referring to GPs somebody that, that I could, after a short little course I could do myself, so that’s a frustration from me that I’ve got one and not another.”
Case manager
The service manager was aware that this was an issue and spoke of developing a training strategy to accommodate everyone:
“Interviewee: This is part of an ongoing, plan that we’ve got... we need a consistent approach to training and education. But I mean people have got different experiences and, different skills and competences so we’re trying to just make sure we’ve got a model that covers that.”
Service manager
The case managers also saw themselves as providing a lot of direct care although this had caused tensions with the district nursing service over who carried out what:
“Interviewee 1: If they needed a dressing, I would not do a dressing.
Interviewer: So would that be a district nurse then?
Interviewee 1: Yes, I’d refer to a district nurse because my skills are not with dressings.
Interviewee 3: Nor mine.
Interviewee 2: I don’t do dressings but I would share it, so when I go in I take over their role and do that dressing for that day, but I wouldn’t go every day to do the dressing. They do their days and then I’d do my bit when I go in.”
Case managers
The case managers saw their role as being one providing direct care and some commented that they expected to be working at a higher clinical level but were held back by the training required:
“Interviewee 1: I think the expectation is for it to be more clinical but the clinical skills and training to work at that advanced level, that’s what we need, because we’re at a certain level what we can work at, but the expectation of the job is a higher level and that’s where our frustration comes, is that they’re not far enough at the moment to reach that level.
Interviewer: So if you were prescribing, you might be less hands on because you’d be doing more higher level clinical work?
Interviewee 2: She hasn’t got prescribing, so she’s the opposite, she can do the listening, and knows what they want but can’t do it, so it’s because of the training issues, that’s why we’re so frustrated. Half of us can, half of us can’t, there’s not even a handful that can do both.”
Case managers
6.4.4 Process of case management
6.4.4.1 Patient identification
The service was not aimed at any specific condition. Although there were criteria for referral, it was thought that these were broad and acted as more of a guide:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 155
“Again it’s the intelligence and it’s what the GPs and the other practice nurses know and the district nurses know as well as the patient. And it’s a guideline, it’s not a criteria, it’s to give them somewhere to start but we do flex that and there are people who wouldn’t necessarily tick all of the boxes that would absolutely totally benefit from case management so they’re not excluded.
Interviewer: And I suppose that’s where the, referrals from the professionals comes in because they know the case?
Absolutely. It’s more than just numbers.”
Service manager
The case managers thought that they often received referrals about patients when other professionals did not know what else to do:
“Interviewee 4: because we get a lot of what’s in between, they don’t know where they need to go.
Interviewee 2: So they refer to us because…
Interviewee 4: We fill that gap.
Interviewee 2: But that’s usually because we know what services are around to, to do it.”
Case managers
They also reported a reluctance to reject referrals when they were at the stage of developing a caseload, if they were from a GP who did not often make a referral:
“Interviewee 2: Yeah the idea… our tool is the recurrent admissions, readmissions which is what we should be looking at and the thing is, at least with professionals you, you’re building up that relationship with them and if, a GP that very rarely refers, does refer, you don’t want to say, ‘Sorry I’m not looking for those people’ because you want, you want to build that up and make that easy for them so.”
Case managers
Although, referrals were felt to become more appropriate once the referring professionals acquired a better understanding of the service and saw positive outcomes in their other patients. There were further efforts being made by community matrons themselves to identify patients by going into the acute trust wards to identify patients who may be suitable for the service.
The service used PARR, the combined model and the Single Assessment Process to identify patients but it was thought that referrals from other professionals remained the most effective method. PARR was felt to be too restrictive by the service manager in not identifying all but the most severe patients:
“For the PARR, I think that we’re refining the information that’s on PARR but we don’t want to be too restrictive so we don’t want to lose potentially a cohort of patients that would benefit that are just below and we can do some more upstream work on.”
Service manager
A view that was echoed by the case managers:
“Interviewee 4: Well there’s that thing as well, if you take on a patient that has got the greatest need there’s very little that you can actually do because, they’ve gone past that stage…
Interviewee 3: I mean if somebody’s got 98 per cent chance of being readmitted then they’re going to go back in whatever you do.”

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 156
Case managers
The PARR information was also out of date by the time it reached the case managers:
“Interviewee 1: A couple of weeks ago I got to one surgery to look at patients that were appropriate and half of them were dead because it’s [the PARR information] four months out of date by the time we get it and we haven’t had it since.”
Case manager
The service sought to identify those with PARR scores slightly lower than high intensity, as these were deemed to have potential for successful intervention:
“…we don’t want to be too restrictive so we don’t want to lose potentially a cohort of patients that would benefit, that are just below and we can do some more upstream work on.”
Case manager
Although referrals from other professionals were thought to be the most effective way of targeting, there were still plenty of referrals received that were thought to be a result of other professionals not understanding the case management service:
“Interviewee 4: We get a lot of what falls between, they don’t know where they need to go.
Interviewee 2: So they refer to us because…
Interviewee 4: We fill that gap.
Interviewer: ‘We don’t know what to do with this person any more so we’ll refer to the community matrons’?
Interviewee 4: The GP keeps getting called out so they’ll refer to us.”
Case managers
Cases were allocated on the basis of GP attachment with some flexibility for prioritisation within that overall system:
“Interviewer: And what happens if you get referrals, what dictates who they come to?
Interviewee 2: It goes through a single GP contact.
Interviewee 4: We’re all GP attached so it goes to the relevant GP.
Interviewee 2: …they do look and try and do some sort of triage and prioritisation absolutely, no that’s really important.”
Case managers
6.4.4.2 Assessment
Assessments made within the Single Assessment Process were accepted as part of the assessment for case management; Easycare was the assessment tool which was used in this process.
6.4.4.3 Care planning
All case managers carried out assessment, care planning, care plan implementation and monitoring, reviews, patient advocacy and clinical oversight. Financial management by means of costed care plans, was not part of the case manager

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 157
role. Rather the case manager role was described by the service manager as having a high clinical component:
“They go and do all the assessments and examinations at an advanced level. They have to check postulations, abdominal palpations, do bloods, ECGs and the interpretation of, so all these things they need to be able to do and interpret a lot of the diagnostics.”
Service manager
Case managers could neither assess for nor authorise use of local authority services. Care plans usually contained the contribution of primary, intermediate and social care services. Service contributions from the acute sector were never detailed.
6.4.4.4 Monitoring and review
The average caseload size was 55, described as ‘hard work’ by the service manager but there was variation in the needs of the patients on the caseload:
“I don’t think you could sustain a fully active caseload, having somebody needing to be managed every week, of 55 patients because it’s not possible. But if they’re at different stages and it’s a review rather than an active management then 55 is absolutely fine and it’s wholly manageable.”
Service manager
Although there was generally continuity of care there was the potential for flexibility within the teams for other case managers to carry out different tasks with different patients within their own areas of expertise. Reviews were usually carried out by a case manager face-to-face with the patient but not necessarily always by the community matron case managers:
“The approach that we’re taking now it’s not just for him or her [the community matron] to do all the reviewing and things, it’s the team. So it could be one of community nurses... then we can either get the community matron or somebody else, a staff nurse or district nurse, so then we can respond accordingly.”
Service manager
The service manager was clear that cases were never discharged, but instead became dormant:
“Because of the nature of their disease and their conditions they’re never going to be at a point where they get better and are cured. So it’s just their level of needs change.”
Service manager
The case managers were less clear on the issue:
“Interviewee 1: There’s no discharge
Interviewee 3: We’re not allowed to discharge.
Interviewer: So, even if somebody’s had only one phone call in six months?
Interviewee 1: It's not clear actually. X_____ has said before with some people that maybe we should be able to do so, it's really not clear.
Interviewer: But it's not there, there’s no policy to say that.
Interviewee 1: That’s the thing though, we’re very unclear as to whether we can or not really, but at the minute we’re run by the rules we’re dealt.”
Case managers
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 158
Although, if a case were to be discharged they would maintain a link with the service and be able to fast track back in without being referred. There was usually continuity of care with patients remaining on the same case manager’s caseload throughout their time receiving the service.
6.4.5 Information systems
The primary care trust had a computerised client record system specific to the case management service. ‘System One’ was also used which allowed links to other IT systems in primary care services locally although this process was in development:
“Interviewer: Do the Case Managers have a stand alone system?
Interviewee: They do at the moment and we use System One as our clinical information system. Well it’s on a journey to be a clinical information system. Our, Family Service Colleagues use RAZE which is a different, information system for them and we’re trying to develop the links so we can share some of that information so we can’t do it electronically at the moment.”
Service manager
The information system only stored personal details with little other information available electronically.
6.5 Site four
The main features of site four are shown in Table 6.6. This was a case management service which demonstrated a high level of integrated service provision with other agencies, as demonstrated through agreements about access to services and information sharing. The service showed low levels of differentiation within the case management process as judged by caseload size, criteria for allocating cases and intensity of visiting and limited involvement in the core tasks of case management. The service commenced in 2004 and was delivered using a GP practice population model, a geographical locality model and disease group based services.
Table 6.6 Case study four: summary description
Measures Level of activity
Extent of integration with other NHS services and local authority adult social care services
Low
Range of self-care support services in the locality and links between them and case management service
High
Differentiation within the case management service permitting a different level of service to those with the greatest level of need
Low
Number of case management tasks in addition to assessment of need undertaken by practitioners within the service
Low

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 159
6.5.1 Links with other agencies
There was no specific out of hours service for case managed patients. There were links with other primary care services through case managers being co-located with district nurses and in GP practices as well as some shared information systems. The relationships with GPs were not particularly well developed and case managers felt that they were ‘tolerated’ although relations had improved as the service had developed. There was a particular issue in this service at the time the fieldwork was conducted about GPs not always accepting the physiotherapist case manager’s requests unless reinforced by a specialist nurse:
“Interviewee 1: Quite often we need to get back to the GP for something medical who may not listen very much and they deem it to not be our, our role. Not being experts, but that’s fine, because then we can ask the girls and say: ‘Oh, I’ve got this patient’ (laughs) perhaps write a letter I’ve consulted with X___, or X___ [specialist nurse case managers], and they recommend something so they’ve given it a bit more credence.
Interviewee 3: Sometimes they’ll ask us to go in because they want other ideas and stuff.
Interviewer: Right, you are getting referrals from GPs?
Interviewee 3: Yes, we all do.”
Case managers
Relationships had been developed with secondary services by recruiting specialist nurses from the acute trust to become cardiac specialist nurse case managers in the community:
“We wanted to recruit specialist nurses, it was a risk because we are a community service and normally they go the other way, don’t they? So what we did was go in and talk to the cardiac nurses in the [acute trust] and say: ‘Well, let’s look, do you think it would work?’ or whatever, and so these girls can go both ways. They are as comfortable in there as they are out here.”
Service manager
The service had also placed a community liaison nurse in the acute trust:
“In an attempt to manage patients’ transfers through the acute trust, we, got in place a liaison nurse post that’s actually based within the social work department at the acute trust, so although they’ve got lots of discharge teams and discharge co-ordinators, we’ve actually got a community nurse who is based in that team in the social work department, who therefore has really close links with the acute social workers, who then can also link out and liaise and follow the patients.”
Service manager
There were two separate local authorities within the primary care trust boundaries, relationships were better developed with one, which was a smaller locality. The links with the local authority were formally through the use of the Single Assessment Process, although there were several other links. The case managers had set up local joint meetings that had become well established:
“It came out of frustration of being a district nurse, actually, and getting a call on a Friday night to say: ‘We’ve got a lady, she’s had a fall, what are you going to do with her?’, ‘Uh?’ on a Friday, and not knowing a social worker who’s just on the end of the phone, so we sat down and we decided, and I talked to my counterpart in social services: ‘How about we meet once a month? Just the caring end of the team and see how we go.’

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 160
And that was a real success, everybody loved it and that has been the beginning for all this joint work.”
Service manager
There were further informal links between professionals through joint initiatives such as an intermediate care service provided by the local authority that aimed to prevent hospital admissions:
“They’re rapid response carers, who can go in if somebody has fallen or, they’ve just had an incontinence episode and need somebody to just go and assist them, because they’ve got MND or something, there was also telehealth that was added on. So we worked very closely with social services to support and develop all those services. X____ (cardiology specialist nurse case manager) has been working with the telehealth and the heart failure patients.”
Service manager
The local authority were seen as enthusiastic partners in joint working:
“I rang them up and I said: ‘You haven’t got a spare desk and a computer, have you, in the social work department?’ And they nearly took my hand off. They just want this to work, don’t they, they’re really, really keen to develop anything. I mean, all of the work around multi-agency working, is us, really, it just seems natural, it's not a chore, it's not a: ‘Oh, I wonder how they’re going to take that?’ It's everybody round the table, let’s get on with it.”
Service manager
There were additional links with voluntary organisations, these were particularly strong with one case manager who had previously worked for the Alzheimer’s Society. There were no dedicated physician services available although there were links with End of Life services.
6.5.2 Self-care support services
The primary care trust had a lead for self-care services although the case management service manager had not been involved in the development of the commissioning strategy for self-care.
There was a network of self-care services provided mainly by the voluntary organisations that case managed patients were often referred to. One advantage of these organisations was the group services that they ran:
“Interviewee 2: From my point of view, the charities can see a lot of patients at once and, yes, they set up like six support groups in three months.
Interviewer: Oh, right, are they support groups?
Interviewee 1: Support and information… it goes two ways, they help me as well, by giving people information, referring people on to me as well.”
Case managers
The case managers thought that these groups were usually suitable for their patients, although being disease specific the patients were often younger. One organisation was setting up a group specifically for younger people.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 161
6.5.2.1 Self-care support provided by the primary care trust
The primary care trust offered self-care support services including informal therapeutic interventions, accessible advice, technology to promote self-care; generic and condition specific self-care support training, and alternative therapies. Case managed patients were thought to frequently access advice and information; generic and condition specific self-care support training and alternative therapies. Patients sometimes used informal therapeutic support, self-care support technology and condition specific self-care support training.
The primary care trust provided specific services for asthma, chronic obstructive pulmonary disease; diabetes; and coronary heart disease and stroke. Informal therapeutic interventions, advice and information were offered for asthma, chronic obstructive pulmonary disease and diabetes as well as self-care support training and self help groups. It was not known what percentage of patients were thought to be using self-care support services.
6.5.2.2 Self-care support provided by case managers
The support of self-care was seen as a key part of the case manager role:
“I think in order to give the correct health support and social services support, then self-care has got to be the corner stone, really.”
Service manager
Case managers had been using a goal setting approach to work out individual goals with patients and then use these to plan care and support:
“Interviewee 1: It's done in a structured clinic. We’ll try and do all these assessments on the same day if we can. Sometimes that doesn’t work, but we try, so it's a one stop shop, and then set their goals with them and tell them what the service can do for them, but also making those goals. Their participation in an exercise plan, or going to the gym, or making sure they’re taking their drugs on time, or whatever, you have to adjust it to the patient.”
Case manager
It was thought that most patients did want to self-care as much as possible and the case manager’s role was to identify what patients were prepared to do for themselves and then support the rest:
“What you do with people is try and encourage them to do as much of a contribution as they want and then you hold the rest. I don’t think it's right to make people totally dependent on us, but I think you pick, you allow them to have some of it, but the bits that really are important and need support you manage.”
Case manager
It was thought that there were people with long-term conditions who were very isolated and that making colleagues in the acute trust aware of this had meant that support could be more effectively planned for such patients on discharge from hospital:
“I said to them to go out with a district nurse, go out with a specialist nurse. And the comments I’ve had back have been really rich. I said to one: ‘How did that go then?’, ‘Marvellous, I didn’t realise how, how many lonely, isolated people there were who didn’t have care.’ I said: ‘So next time Mr Smith comes in and you’re writing your discharge plan, you’ll know what he’s going home to.”

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 162
Service manager
There was telehealth provided for heart failure patients in a joint venture with the local authority which was well received by many of the patients:
“Interviewee 3: X____ (Cardiology specialist nurse case manager) has been working with telehealth and the heart failure patients and she’s got patients that have got that monitor themselves, and they know their parameters and they know exactly when to contact her if they’ve got a problem.
Interviewer: Do patients like that?
Interviewee 1: They do, a lot of them do it anyway, without the actual equipment. I try and educate all the patients, if their weight is up or they're out of breath, they just call, and my patients do call, regularly and they do monitor themselves, they do their own blood pressure, a lot of them, anyway. But the ones who have problems with sight, or other problems, the telehealth really comes into its own there, because they can’t actually see the readings, so that comes through to me, so I can keep an eye on them from that point of view.”
Case managers
Support for carers to support self-care was viewed as important and older carers’ needs were seen as different to others:
“I think, particularly when you’ve got older couples, for example, how easy is it going to be for that carer to, pick up new skills around providing care?”
Case manager
Thus, case managers usually assessed for self-care support needs and sometimes referred people on to such services. They sometimes contributed to the provision of services and the development of self-care support programmes.
6.5.3 Staff mix and tasks
The teams were made up of specialist nurses and physiotherapists managed by other NHS personnel. Some case managers were located in GP practices and others in community nursing teams. There was no programme of training currently underway for the case managers.
All case managers carried out assessment, care planning, care plan implementation and monitoring, reviews, patient advocacy and clinical oversight. Financial management by means of costed care plans, was not part of the case manager role. There were strong feelings around the provision of direct care within the team and the case manager role was perceived as containing as much direct care as the patient required during that contact:
“Interviewer: I suppose what I’m trying to identify is what is the case manager to you, is it somebody who does go in and do hands on clinical stuff, or is it somebody who stands back and gets district nurses in to do that?
Interviewee 3: You see, that’s the model I absolutely hate.
Interviewer: Right. You hate that?
Interviewee 3: As a nurse, that does not compute, it does not compute, you could have anybody in that role. Actually, for me it's about, you co-ordinate the care by working with the patient. It's about them directing the service, isn’t it, really, at the end of the day? It's about them. So you can’t do that if you, I could go in to a patient and think: ‘Yes,

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 163
you need this, this, this and this, and then walk away. That’s not care. That’s signposting, isn’t it?”
Case manager
There were parallels drawn with the historical practice of district nursing:
“Interviewee 2: You’re going in to that patient, you should be able to do everything that patient needs when you go in and a specialist element of your role is fabulous, isn’t it, it's absolutely fabulous, but you don’t forget everything else that you’ve learnt as well. Unless it is very, very specialist, I will say this, because I know you’re not going to quote me by name, but I see a case manager, as what should be the proper district nursing role, you shouldn’t need all this other stuff.
Interviewee 1: If the district nurses were entitled and able to do the job they’re supposed to do, that, to me, when they introduced all this case management and community matrons, I’m not saying they didn’t need some up skilling, but I saw it very much as what I used to do as a district nurse.
Interviewee 2: It was something I did when I was a district nurse, because I could change a stoma, I could give somebody advice about their continence, because to me, I was a generalist.”
Service manager and case manager
6.5.4 Process of case management
6.5.4.1 Patient identification
The referral criteria for the service included age, hospital admissions and disease, with the service specifically focusing on people with neurological conditions and heart problems. There had been targeting of patients using the Dr Foster tool in some areas of the primary care trust but there was a perception from some case managers that the most effective method of identifying suitable patients for case management came from referrals from other professionals, although views were equivocal on this:
“Interviewee 1: One of the things that we find is that, although you’ve got things like PARR the value of just the normal referrals from your professionals is much more accurate, in many ways.
Interviewee 2: Well, actually, we all said it in the beginning when we were looking at case management, the person who knows the patient better is the GP, they’ll be where you get your referrals from, but actually there’s evidence that now suggests it's absolutely not the case. And in [place], they’re using a combined tool so we’re going to hopefully do a pilot.”
Service manager and case manager
The service manager had used the PARR tool previously and found the information to be out of date:
“I used PARR in two thousand and something, and by the time I managed to get any information on the patient, he’s either moved, died or whatever, so it was absolutely no use whatever, and it was not any good for predicting admissions.”
Service manager
Cases were allocated by level of staff qualification and intensity of involvement.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 164
6.5.4.2 Assessment
Assessments made within the Single Assessment Process were accepted as part of the assessment information for active case management. The Easycare assessment tool was used to identify need.
6.5.4.3 Care planning
Care plans contained details of the contribution made by primary, acute, intermediate and social care services. Staff could neither assess for nor authorise local authority resources.
6.5.4.4 Monitoring and review
Caseload sizes were large due to the case managers being disease specific. One cardiology nurse specialist case manager had 500 people on her caseload and another had 150:
“Interviewee 2: I think my caseload is roughly about 500 at the moment, but they’re not all active at this time.
Interviewer: I think this is the thing about trying to describe what a caseload actually means because if you have a caseload of 500, that’s unmanageable, isn’t it, but when you describe that they are stratified within that...
Interviewee 1: I mean, there are probably 500 who need me, but not all the time.
Interviewer: How many visits do you do a week, would you say, in an average week?
Interviewee 2: I’ve got to work three clinics … I probably do ten home visits a week… I do telephone reviews as well.
Interviewee 1: I don’t see as many because I just do home visits… I see about five a day, yes. Yes. I'd say five is usually the average, because I devote so much time to each patient. You could be with one patient two hours, because that’s what they need, and another patient ten minutes, it just depends on what the patient needs.”
Case managers
The rural nature of the primary care trust led to transport difficulties but this did not mean that caseloads were reduced:
“Interviewer: How does that impact on your caseload, does that mean that you have to have a smaller caseload than you would necessarily have?
Interviewee 2: You just organise it better. I think one thing that people have got very good at around here. They’ve had to, with the geography and with, with the different things that happen.
Interviewee 2: I think we get very creative, yes. You tend to cluster your visits, Interviewee 1: Be very smart with your journey time.
Interviewer: Yes, so that you were stopping off along the way.
Interviewee 2: The reason people don’t get enough support is there’s not enough of us.”
Case managers
Due to these very large caseloads there was flexibility in who was seen first:
“Interviewee 1: And I must say, although it’ll take until, perhaps, March or April [four months] to see me in my clinic, there might well be another member of the team before

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 165
that. So you can then liaise with me and say: ‘This person needs to come up your list a bit.’ I give priority to newly diagnosed people and also people with medication issues.
Interviewee 2: I don’t have a waiting list at all, I should contact someone two days later, well, within 72 hours they should get a phone call at least and they should be seen within two weeks. But I normally see them within about three days.”
Case managers
Caseloads varied as they were condition specific and measures were being taken to use the large caseloads as evidence to support applications for funding for further case managers. There was usually continuity of care as patients stayed on the caseload of the same case manager. Over three-quarters of active cases were thought to be seen weekly.
Patients could be reviewed whenever it was thought necessary by the case manager:
“Interviewer: So you review people annually after admission, or?
Interviewee 2: It depends on how their doing and we’ve gone through the goals with them, and it just depends on what they need, really, in relation to how often we see them.
Interviewer: Right, so if you needed to review somebody because there’s a change in circumstances or something, you could just do that?
Interviewee 2: Yes. Certainly with people having relapses, and people who've got medication issues, then they need to be seen. Definitely.”
Service manager
These reviews would not necessarily involve consulting the multi-disciplinary but the outcomes would be communicated to them in writing. There was very little evidence of case closure, patients might become inactive and only be seen if their circumstances changed:
“Interviewee 2: My patients tend to stay on, they might go inactive, but then they can just bleep me and just say: ‘Can I come back on your caseload?’ or, ‘Can you just make another visit?’
Interviewee 1: A lot of the patients, are what I call SOS, they just call me when they need me. But I give them a three-monthly call as well, to ensure, if I haven’t heard from them, just make sure everything’s okay.
Interviewee 3: Some people are just contacts, aren’t they, they just know, they like to be on your numbers.”
Service manager and case manager
There were comparisons drawn with the traditional district nursing role and the community matron role where keeping people on a caseload was encouraged:
“Interviewee 1: Yes. But I think if you look at when the introduction of community matron or case manager, one of the things that we raised was, district nurses have been castigated for keeping people on the caseload, but now you’re saying to community matrons that's okay. So actually, you had a whole range of services that were already a social network for those people who didn’t have one and they were told they were wrong for doing that, but now it's okay to do it. But we all knew it was okay to do it, despite being told not to, we did.”
Case manager

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 166
The very large caseloads seemed to be more like disease registers where a person was listed as having the condition but not necessarily actively managed:
“Interviewee 3: Well, I’ve got 18 year olds, so it's a little bit different for me, that have obviously been diagnosed with MS and 40 and 50 year olds who’ve been diagnosed with Parkinson’s Disease.
Interviewer: But do you ever discharge anybody?
Interviewee 3: No, because, I wouldn’t like to think I wasn’t there for somebody if they needed someone. So, no, I don’t. I do keep them on my caseload, but I actually specify when I do the caseload whether it’s someone who can be managed or not.”
Case manager
In the unlikely event of a patient being discharged they were able to refer themselves back into the service.
6.5.5 Information systems
The case management service had been using their own computerised information system but there had been ongoing problems linking it to other services, despite a willingness from the primary care trust to do so:
“Interviewer: You talked about sharing information with them, are there any joint computer systems?
Interviewee 3: Not currently, they don’t speak to each other.
Interviewee 2: That’s a really big issue, at the moment.
Interviewee 3: We tried to introduce and pilot the electronic single assessment process which was social services and health, but I think it died a death because I don’t think it was very good for the social work team.
Interviewer: So is that no longer used… which is a shame, because everybody was, was very keen for it to work.”
Case managers
One problem had been that one local authority area had recently invested in an incompatible system:
“Interviewee 1: X___ had just gone onto Care First, or some similar system, so they weren’t going to change, because they’d obviously invested a lot of money.”
Case manager
However, a recent plan to introduce System One was viewed more positively:
“Interviewee 1: We’ve now gone onto System One, and I think it's a very positive move, I mean, I’ve sat through over the years, presentations about these computers systems and thought that’ll never work but, actually, last Friday evening I sat in on one and I thought: ‘You know, this could work.’”
Case manager
One case manager was already using System One and had found it improved communication with the GP practices and palliative care services as well as facilitating remote working:
“Interviewee 3: All my patients are of GPs that can resource into it and palliative care use it. All my clinics are run on this system, and I can put my consultations on the

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 167
system, so what I’ve actually done with a patient, medication reviews. I do all my GP letters on it, so my admin lady, because I’m not based with my admin, she can then look at my System One, see everything that I’ve done and then type the letters out and then attach them to their file. So everyone’s got a file on there.”
Case manager
The details stored in the system were personal details, medical information and diagnoses.
6.6 Cross-site comparisons and emergent themes
This section looks at themes from the components of case management across the sites, including staff mix, the extent to which the tasks of case management were undertaken, links with other services and information systems used. Aspects of the interface between self-care support and case management are also examined, followed finally by factors influencing variation in case management services.
6.6.1 Components of case management
6.6.1.1 Skill mix within teams and health care setting
All four sites utilised nurses as case managers and three also used physiotherapists and two of these also used occupational therapists. All services had some case managers based in nurse teams, two had case managers based in health and social care integrated teams and two in GP practices. All four sites managed case managers through health personnel although one site had some managed solely by the local authority as part of a joint project. Half the sites had a training programme providing training in clinical skills and prescribing. The same two sites also had self-care support staff training available focused on supporting the Expert Patient Programme and disease specific support.
6.6.1.2 Caseload size
Caseload sizes varied between 30 and up to 500 for one disease specific case manager although there was variation of activity within these. All four sites thought that a caseload of 80 patients requiring active case management was impossible to maintain. Although if patients were had different levels of need with some only requiring occasional review then larger caseloads of 55 were seen as more manageable.
6.6.1.3 Core tasks of case management
The case management tasks appeared similar across the four sites. All carried out assessment for health needs, implemented, monitored and reviewed care plans. Three out of four also carried out care planning and arranging services. All provided hands on care and clinical oversight with three out of the four also providing patient advocacy, emotional support and medications review.
Case finding and screening
All four sites had referral criteria including age and admissions. Three also had disease specific admission criteria and one also included polypharmacy, GP and ambulance contact as well as other risk factors such as falls. All but one service was
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 168
targeted. Three were targeted at specific conditions all including coronary heart disease and neurological conditions. The decision to target had been made by one primary care trust because of limited numbers of community matrons and another had opted to use an existing cardiology team.
Three sites identified patients using the Single Assessment Process and PARR (I and II) although all four sites took referrals from other professionals. The use of PARR as a patient identification tool was found to be problematic by all case study sites. This appeared to be due to lack of administrative support with the result that the information received was often out of date.
Three sites were specifically seeking to identify people with slightly lower PARR scores than the highest intensity users as they felt this was the group with the best potential for successful intervention.
Assessment
All four sites used Single Assessment Process, although in none could case managers either assess for, or authorise social care services.
Care planning and implementation of care plan
In two sites cases were allocated by qualification of staff and intensity of involvement predicted, one site allocated by GP practice and another had no policy. All services achieved a level of continuity for patients with the same practitioner usually retaining responsibility for a patient during their time in the service. Two services reported that up to a quarter of patients were visited weekly, one reported over three-quarters and the other between a quarter and a half.
Monitoring and review
All services carried out reviews of patients, all would use face-to-face meetings with the patients, and three would additionally use information from carers or review a patient over the telephone.
Case closure
The most common reason for case closure was the death of the patient. Two services said that the second most common reason was a patient moving to a long-term care home and two others reported patients moving to community nursing.
6.6.1.4 Links with other services
No service had an out of hours service that was different from usual primary care arrangements. All services were based with nurse teams in primary care and all but one service had formal agreements with these services. Three of the four sites had agreements with acute care and information was shared in writing by three sites and through disease registers, patient held records and a designated person in two

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 169
sites. Only one site had agreements with the local authority. No sites could either assess for or authorise local authority social care services. Information was shared using Single Assessment Process in three sites and through written information and multi-disciplinary meetings in two sites. All four sites had agreements with intermediate care and three shared information through Single Assessment Process (one non-Single Assessment Process). Two sites also used patient held records. All sites had established links with End of Life services and one had a weekly physician session for case managed patients. All services had links with voluntary organisations.
Across all sites relationships with GPs in particular had been initially problematic, although they were perceived as having improved over time. Some of these problems were ascribed to GPs not understanding the role of the case manager.
Those GPs who had seen benefits for their own patients had become more supportive over time and some very positive relationships had developed. Two of the sites had had additional problems with community nursing services, many concerning confusion of the case manager role particularly as to whether case managers should provide direct care to patients such as changing dressings.
All sites thought that the professional background of the case manager was important in informal network building, both as they had a good understanding of the processes in the services they had come from and furthermore through their existing contacts with their previous colleagues.
6.6.1.5 Information systems
All services had some form of record system, two of these were computerised and only one was linked to other primary care information systems. All services stored personal details of patients, three also stored medical information, diagnoses, Single Assessment Process, care plans and the case management service input. There were issues in all sites around the compatibility of information systems with other parts of the NHS and the local authority with only one site thinking that they were finally developing a system that may be successful.
6.6.2 The interface between self-care support and case management
Three of the four sites had a lead for self-care support and two had been directly involved at a strategic level, including the site without a designated lead. All but one site had links with voluntary organisations supporting self-care with three sites either having or developing a directory of self-care support services.
6.6.2.1 Components of self-care support
Primary care trusts provided a range of self-care support services; all provided generic self-care support usually in the form of the Expert Patient Programme. Advice and information was provided for diabetes in three sites and for asthma, chronic obstructive pulmonary disease and coronary heart disease. Two sites provided technology and equipment to support self-care, both for chronic obstructive pulmonary disease and coronary heart disease. Self-care training for specific conditions was provided in two sites, both offering courses for asthma,

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 170
chronic obstructive pulmonary disease and diabetes. Self help groups were available in all four sites and with three out of the four offering groups for people with diabetes, two sites offered groups for asthma, stroke coronary heart disease and chronic obstructive pulmonary disease. Two sites also offered alternative therapies, which were for musculoskeletal conditions. There was a wide range of estimated percentages of case managed patients using these services, from five to 60 per cent, although one site could not provide a figure.
Most frequently used by case managed patients were accessible advice and condition specific self-care support training. These were followed by technology and equipment and informal therapeutic interventions. Self help groups and alternative therapies were less frequently used. Some self-care support was being provided directly by case managers, all provided patient education and two contributed to self-care service provision and one to self-care programme development. All case managers referred on to self-care support services and two sites had disease specialist case managers.
There was concern expressed in all sites about the suitability of some services, notably the Expert Patient Programme, for case managed patients, usually due to their typical age and severity of conditions and subsequent limited mobility.
6.6.2.2 Carer education
The importance of supporting carers as a means to supporting self-care was noted by all case study sites. Older carers were seen as having particular needs around acquiring new skills.
6.6.2.3 Technology and equipment
Telecare was being used, often in conjunction with local authorities, it suited some patients, but the individual patients’ attitudes towards it were felt to be important as there was the potential for it to cause anxiety. Two of the sites thought it was important that patients were given the choice as to whether they wanted to access self-care support as it was not perceived as suitable for everybody. Voluntary sector organisations were playing a key role in the delivery of condition specific self-care support across all case study sites.
6.6.2.4 Exit from case management
Supported self-care was rarely seen as an exit from case management. Overall there was little throughput in any of the sites with only two ever contemplating discharging patients, the other two had no procedures for this, which may have been a result of the infancy of the service. If patients were discharged they were usually transferred to community nursing or a nursing home.
6.6.3 Factors influencing variation in case management
There were several factors influencing the local variation in case management services. Firstly, the effects of national targets had led to some existing disease specific services becoming case management teams so that the requisite numbers of case managers could be achieved within the specified timeframe.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 171
There was evidence of recent changes in primary care trusts having an impact on services. These changes included relatively recent merging of smaller primary care trusts resulting in there being two or more styles of case management service in operation in the same primary care trust. These mergers had also led to changes in management at both strategic and operational level and this had influenced the development of relationships with other partners, both within and outside health services.
As well as top down targets and organisational change, the local histories of the sites exerted an influence on the services being provided.
6.7 Summary
The final section of this Chapter of the report summarises the characteristics of the four sites where detailed study was undertaken and also common factors and themes.
6.7.1 Case study sites
The four sites selected for further investigation, following a postal survey, reflected different approaches to case management in the context of supporting self-care. The sites were categorised as either high or low on four domains: self-care, the presence of which was common to all; integration, differentiation and higher level case management tasks. Site one was categorised as high on three of the domains and low on differentiation; site two was categorised as high on two of the domains and low on differentiation and case management tasks; site three was categorised as high on two of the domains and low on integration and case management tasks; and site four was categorised as high on one domain and low on integration, differentiation and case management tasks.
6.7.2 Cross-site comparison and emerging themes
All four sites demonstrated higher levels of self-care support through the provision of services through the primary care trust or provided by the case managers themselves. The service that demonstrated higher differentiation reported the smallest caseloads. Of the two services demonstrating higher integration one had agreements with the local authority over service provision as well as some case managers managed through the local authority. The other service reported discharging cases to local authority services. The service with a wider range of case management tasks also had high integration with agreements with the local authority and some of the case managers were managed through the local authority.
All services had commenced after 2003. There were several features common to all four services, with all aiming to improve the co-ordination of care, quality of life and independence for people with long-term conditions. All services aimed to promote self-care support of their patients. A further aim was to divert people away from inappropriate hospitalisation, but when admission had taken place to reduce length of stay and arrange a quicker and more effective hospital discharge. All services consisted of a single member of staff responsible for assessment, care planning, monitoring and review tasks for a particular patient. Case management

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 172
was an activity by which people with complex needs received intensive help different in nature and scope to other patients, and a means of providing long-term support and co-ordinated care by which needs were assessed and care plans implemented involving multiple services. All services were delivered, at least in part, using a geographical locality with three also using disease groups and two using a GP practice model.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 173
Chapter 7 Service user consultation A service user consultation exercise was undertaken comprising four focus groups of older people with long-term conditions. The approach to this is described in Chapter 3. Participants were asked to complete a brief written questionnaire (Appendix 9) about their health status; their preferences for self-care support; and their priorities for a case management service. This was followed by an open discussion about participants’ experiences of self-care support and barriers they had encountered.
7.1 Knowledge and experience of self-care
Table 7.1 shows the range and number of long-term conditions that participants were experiencing. The most frequently reported was arthritis, followed by high or low blood pressure, diabetes and heart problems. Most people were experiencing two or more long-term conditions.
Table 7.1 Focus group participants – self reported health status (n=47)
n %
Number of long-term conditions 1 2 3 4 5 6
10 14 8 8 4 3
21 30 17 17 8 6
Range of conditions Arthritis/rheumatism High/low blood pressure Diabetes Heart problems Other1 Depression/mental health Chest and breathing problems Stroke Osteoporosis Gastric disorders Blood disorders
31 23 16 14 13 11 9 6 4 3 3
66 49 34 30 28 23 19 13 8 6 6

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 174
Source: Do you have any long standing health problem, disability or infirmity
1 Includes digestive problems, glaucoma, cancer, ulcer, thyroid problems, polio and hearing problems (all reported by less than 5%).
7.2 Preferences for self-care
Service users were asked to choose up to three types of self-care support which they would find most useful helping to manage their particular condition(s). The categorisation for the types of self-care support was derived from government guidance (DH, 1998). In addition alternative therapies were included due to their popularity as part of self-care for people with chronic conditions (Thorne et al., 2002). These categories of self-care support replicated those in the survey to managers as noted in Chapter 4.
Table 7.2 Focus group participants – self-care service priorities (n= 47)
n %
Alternative therapies Being able to talk to someone Special equipment A course for people with the same condition Information leaflets An informal self help group A course for people with all types of conditions
26 26 20 19 18 16 10
55 55 43 40 38 34 21
Source: Which three things do you think would be most useful in helping you manage this condition?
Table 7.2 reveals that alternative therapies and being able to talk to somebody about their condition were identified by the majority of participants as most helpful in the management of a long-term condition. Alternative therapies were seen as particularly important to those respondents we asked from the LMCP Care Link group, which primarily provides support to service users and carers within the Asian community, possibly because these therapies have a more established role in self-care in different cultures. A course for people with all types of conditions was the least preferred option with participants favouring support groups focused on a particular condition:
Interviewer: “And what was so useful about that, was it meeting similar people?
Interviewee 7: It was meeting similar people, sharing experiences, sharing how you cope with it and generally getting the feel of what was likely to happen in the future so that you were prepared for it.”
Focus Group 1
Some people found it useful to chat to other people with the same problems and share experiences rather than be taught information by a group leader:
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 175
Interviewee 4: “There’s a lot of pressure I think if it’s a course, if you’re all just friends together its better, if you’ve got a leader it’s a lot more formal. You’ve got enough to be going on with without having somebody tell you what to do.”
Focus Group 1
However, it was acknowledged that attending a more generic group like the Expert Patient Programme - a course for people with all types of conditions- may also be useful but mostly as it might be a good way to meet people with similar experiences.
In view of the small numbers involved in Table 7.3 no percentages have been recorded. Nevertheless it demonstrates that focus group participants clearly identify that the types of self-care support most valued by them varied by condition. Special equipment was most popular with people with breathing problems and perceived as least useful by people with osteoporosis. Alternative therapies were most popular with those who had experienced stroke and least popular with those people with diabetes. Information leaflets were most popular with those with mental health problems and least popular with those with respiratory problems. Having somebody to talk to about their condition was important to all the people who had experienced a stroke and of least importance to people with arthritis. The availability of a group for people with the same long-term conditions was seen as useful by people with diabetes, but less so by people who had experienced stroke. A generic course was seen as most useful by people with respiratory problems and least useful by those with mental health problems. Informal self help groups were seen as useful by more respondents who had experienced stroke and least useful by those with respiratory problems.
The number of conditions each respondent experienced was recoded to show those with three or more and those with less than three. The preferences for different types of self-care support were then compared for the respondents in these groups. Those with more than three conditions were significantly (p=0.05) more likely to prefer having the opportunity to talk to somebody about their conditions and those with fewer conditions significantly more likely to prefer information leaflets (p=0.05). This appears analogous to previous research that found that when people complete self assessment they often preferred another person to be there to assist them, particularly if they had greater needs (Challis et al., 2008b).
More generally there were mixed views on whether people should be expected to take part in self-care activities. Some participants thought that professionals did not have high expectations of patients’ ability to understand and be able to manage their condition(s):
Interviewee 2:”The doctor has never explained anything to me, the consultant has never explained exactly what could be done and I think that the doctors here don’t give people enough credit for having intelligence.”
Focus Group 1
Whereas other respondents felt there was often an assumption by medical staff that patients would do their own research prior to seeking professional advice:
Interviewee 4: “Do you not feel that the nurses, doctors, whatever, have a high expectation for people to work it out for themselves? They’re saying what did you come

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 176
for, they’re expecting you to tell them but the expectation is that you should know what’s wrong with you and be responsible for your own care. So there’s a responsibility on you?”
Focus Group 3

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 177
Table 7.3 Priorities for self-care services by condition (n=47)
Special equipment
Alternative therapies
Information leaflets
Being able to talk to someone
A course for people with the same condition
A course for people with all types of conditions
An informal self help group
n n n n n n n
Range of conditions
Arthritis/rheumatism (31)
15 21 10 17 10 5 12
High/low blood pressure (23)
11 15 8 15 10 4 14
Diabetes (16) 8 7 4 10 10 3 10
Heart problems (14) 8 8 4 10 4 3 9
Depression/mental health (11)
4 7 4 9 3 1 6
Chest and breathing problems (9)
6 6 1 5 5 3 1
Stroke (6) 3 5 1 6 1 1 5
Osteoporosis (4) 1 2 - 3 2 1 -
Number of long standing health problems
n (%) n (%) n (%) n (%) n (%) n (%) n (%)
Up to 3 (24) 3 + conditions (23)
8 (33) 12 (52)
12 (50) 14 (61)
13* (54) 5 (22)
10* (42) 16 (70)
10 (42) 9 (39)
5 (21) 5 (22)
8 (33) 8 (35)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 178
*significant at the 0.05 level
Source: Do you have any long standing health problem, disability or infirmity?
Source: Which three things do you think would be most useful in helping you manage this condition?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 179
Patients having the chance to learn more about their condition through self-care support was seen by respondents as a way of allowing people to choose to take more responsibility for managing their condition(s) if they wished to:
Interviewee 3: “The attitude used to be people didn’t need too much information but the world has changed enormously… I think there are some conditions where people don’t want to know what’s down the road so people must choose.”
Focus Group 3
Several other issues important to respondents, were identified in the wider discussion around service users’ experiences of self-care support, these were information, transport and practical help. Information about both the condition and the support services available was perceived as being useful but not always available. It was thought that health professionals did not always provide this and it was often not available in other languages if appropriate. Many participants had found information available on the internet but acknowledged that not everybody has access to such resources:
Interviewee 4: “When I last went to the doctor I was encouraged to look it up on the internet, which I didn’t mind.
Interviewee 2: But how did they know you were on the internet? I mean I’m not on the internet.
Interviewee 3: A lot of older people don’t have the internet.”
Focus Group 1
Transport to hospital appointments, and to a lesser extent self-care groups, was an important issue for participants, particularly those with no family locally who may be reliant on taking taxis:
Interviewee 1: “I had to go back to hospital so it cost me £60 in a taxi for a round trip, twice in two days.”
Focus Group 3
Existing patient transport schemes were reported to be not always well organised:
Interviewee 4: “It’s phenomenally badly arranged, you can spend a day in the bus and if you have health problems…
Interviewee 5: You see in X____ we have a community transport organisation and a community car scheme that’s fine but not here in X____.
Interviewee 1: You see I had a letter saying if you need help with transport get in touch with your doctor… Surely they can work out a system at the hospital where if people need transport they can fix it up there and then for the next appointment.”
Focus Group 1
There were particular issues raised regarding transport in rural areas, particularly with regard to attending hospital and GP appointments and self-care support groups.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 180
Overall, the willingness of service users to engage with self-care support was there, but the potential for participation was limited by the more practical barriers of transport and lack of day to day help with activities of daily living. This suggests that if these were perceived as a problem for focus group participants this would be magnified for older, less mobile service users with higher levels of need.
Interviewee 4: “I think it’s about mobility and transport more than anything, I don’t think it’s just about age, that’s not an issue. But if they can’t get there, there is a problem.”
Focus Group 3
The use of telemedicine was perceived as helpful with regard to the management of long-term conditions particularly in rural areas:
Interviewer: “Would you like a computer that did your blood pressure?
Interviewee 1: I think it would be very useful.
Interviewee 3: Diabetes services have a technology system and people have got used to various sorts of tests, some of which are carried out at home and monitoring your own results.
Interviewer: But people have appreciated it?
Interviewee 3: Oh yes, they love it.”
Focus Group 3
However, some focus group participants did not like the idea and would feel like they were being ‘watched’:
Interviewee 1: “As long as people don’t think its big brother watching you?
Interviewer: Would you be comfortable with that in your home?
Interviewee 3: Oh no.
Interviewee 1: There’re people who wouldn’t be comfortable.
Interviewee 3: I just wouldn’t, it’s like you said, it’s like big brother.”
Focus Group 2
Practical help with housework, shopping and banking were described as crucial to people who have been unwell, particularly after a hospital admission. Participants reported such services as being hard to access either through health and social services or via private arrangements:

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 181
Interviewee 1: “There’re all sorts of basic needs that aren’t being met for people who live by themselves.
Interviewee 4: Is that part of the health service or social services?
Interviewee 1: I rang and they gave me the name of this woman charging £12 an hour but she was fully booked. There’s a great need for these basic things.
Interviewee 3: I was laid up before Christmas. And the two things that bothered me were shopping and eventually it was going to be cash because I only had so much…
Interviewee 1: That’s another problem, getting to the bank…
Interviewer: So it sounds like these are very practical day to day things?
Interviewee 1: These are things that matter.
Interviewee 4: I mean I’m not looking forward to 6 weeks after the operation when they’ve told me I mustn’t do anything, I live on my own, I’ll have to do something…”
Focus Group 1
7.3 Priorities for a case management service
Including a question about the purpose of case management in this consultation exercise was felt to be helpful, since it would enable us to elicit user priorities about the different features of case management and compare them with those of managers. Service users were asked to consider which features were most important for a case management service, selecting from a list of goals similar to those in the survey (question 7) sent to managers in primary care trusts responsible for long-term conditions services. Table 7.4 shows that participants felt the key priorities for a case management service should be to improve the range of services available to care for people at home and to provide more intensive long-term support. Service users clearly placed more import on the meeting of basic needs first, before self-care could be supported.
Table 7.4 Focus group participants - case management service priorities (n=47)1
Aim of case management No.
To improve the range of health and social care services available to support people at home: by this we mean extra support to avoid unnecessary admission to hospital and facilitate early discharge.
20
To provide more intensive long-term support to people living at home: by this we mean more help than would normally be available from the community nursing services and social services.
16
To improve the coordination to care to people living at home: by this we mean the provision of the right kind of help by the most appropriate person at the right time. 6
To promote self-care support for people with long-term condition: by this we mean giving you advice to help you to manage your condition. 5

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 182
Source: What do you think should be the most important aim of case management for people with long-term conditions?
1 Some respondents selected more than one option
7.4 Summary
The consultation exercise showed that focus groups participants were interested in practising self-care. However, their priorities were different to those promoted by government policy in a number of ways. First, alternative therapies were a popular option although this type of self-care support is not typically specified in guidance. Second, where group support was involved there was a preference for groups of people with the same condition rather than the generic Expert Patient Programme. Furthermore, the consultation process identified that the provision of practical assistance in the home, especially after a hospital admission was important to the focus group participants.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 183
Chapter 8 Concluding comments This chapter is in five parts. The first is a critical appraisal of the methodology adopted in this study. In the second the findings of the study are reviewed. The third part explores the policy and practice implications of the findings. Fourth recommendations for further research are outlined. Finally, broad conclusions from the study are preceded by a summary of the approach and the principal findings.
To provide a context for this it is helpful to remind ourselves of the definition of case management and self-care service specified at the beginning of the report and which have been used throughout the conduct of the study. Here case management was described as:
“The active management of high-risk people with complex needs, with case managers (usually nurses) taking responsibility for caseloads working in an integrated care system”
(DH, 2004b; p6).
We also employed a definition of self-care from policy guidance issued by the Department of Health. It was described as being part of daily living to maintain health and well-being and, for people with long-term conditions, including actions taken to minimise the impact these have on their everyday lives. Five approaches to self-care are identified: appropriate and accessible advice; health education; self-care skills training; self monitoring; and equipment (DH, 1998).
This study had three aims. First, to map current provision of NHS case management services in primary care for people with long-term conditions. The second was to classify programmes on observable features of case management implementation with particular focus upon the integration of care between primary and secondary care and between health and social care. Finally it sought to identify the extent and nature of self-care initiatives within this service and to investigate the role of self-care initiatives as determinants of entry and, particularly, exit to the services. These aims were addressed by: a substantive literature review; the examination of data collected using the national survey of case management services; four case studies; and a comparison of the findings of the survey with data form local authority adult social care services relating to care management arrangements..
8.1 Methodological approach
The approach was underpinned by a comprehensive review of the policy and literature relating to both case management and self-care services for people with long-term conditions. The latter in particular informed the survey of long-term conditions services; the selection of case study sites; the foci of enquiry within them; the consultation with users; and the triangulation of the evidence presented subsequently.
8.1.1 Postal survey: response rate and categorisation of services
One hundred and fifty two questionnaires were distributed to primary care trusts in England. Fifty-six full questionnaires were returned and 35 responses to a shortened version of the questionnaire were collected by telephone (see Appendix 5 for further

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 184
details). Therefore, for all questions there is a sample of at least 56 responses (37%) and for certain questions the sample size is 91 (60%). The response rate was highest in the then Greater Manchester Health Authority (100%). Otherwise no substantial difference was noted across the country. Nevertheless a higher response rate was anticipated and the time frame for completion of the study required that the data collection in respect of the survey ceased 13 months after its initial distribution.
Data from the first 50 respondents of the survey of case management arrangements were used to categorise case management services and classified using two overarching themes (organisation and practice) and four domains (integration, self-care support, differentiation and case management tasks), identified a priori informed by previous literature, the research questions and the survey data. Due to the study focus on the interface between case management and self-care services, those primary care trusts (n=30) showing low levels of self-care support were disregarded for this aspect of the study. This classification process resulted in four models of case management with varied combinations of the domains.
8.1.2 Limitations
In addition to the low response rate to the postal survey of long-term conditions services described above, the study has a number of other limitations. These are discussed below.
One of the principal weaknesses is the reliance upon questionnaire data from each primary care trust to describe and categorise services. Such an approach cannot to fully capture the diversity and within location variation in service arrangements that might be anticipated. Inevitably this was reflected in the findings reported in Chapter 4 and the classification of services from which the case study sites were selected.
The criteria used for this also requires critical appraisal. A particular focus of the study was the interface between case management and self-care support and thus services which did not provide evidence of this were not selected for more detailed investigation. As a result of this strategy it could be argued that the insights afforded by the fieldwork in the case study sites into the overall picture of the national development of long-term conditions services is partial and limited those identified in the postal survey as having a range of self-care services in the locality and links between them and the case management service.
It is also noteworthy that there was relatively little discrimination between sites where case management engaged with self-care support based upon our data. Of course, all sites were at an early stage of development and differences might have become sharper as services developed. Nonetheless, the relatively poor patterns of engagement between case management and local authority social care services noted in the majority of sites was such that it is not unreasonable to conclude that it will have affected the degree of integration reflected in care plans for people with long-term conditions and therefore the support provided.
Furthermore, the involvement of users in the broadest sense of the word merits consideration in this context. It was explicit in the research proposal that user perspectives on the relative merits of different approaches to services provision would be sought. Thus we were, in effect, involving consumers in analysing and interpreting the results of the research (Hanley et al., 2000). As such we sought to engage with people with long-term conditions but not necessarily in receipt of

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 185
assistance for a long-term conditions service. Moreover, there was no attempt match their experience of service receipt with the self-care support services and, potentially, the case management services reported by individual respondents to our postal survey or those described in the case studies. Rather we sought use the service consultation to comment on and provide insights in to the some of the principal findings from the research derived form the literature review, the postal survey and the case studies.
Finally, it is relevant to note that overall whilst the findings from the study reflect its aims it does mean that broader contextual factors are omitted from the analysis and subsequent discussion. Thus, for example, whilst we have noted marked variations in the way case management services are organised and delivered and their links with self-care services we have not explored the extent to which these are associated with different degrees of access to care and effective support for patients with long-term conditions and their families. In short, the study does not address the impact of organisational arrangements on equity, efficiency and equality.
8.1.3 Strengths
A strength of this approach was that the grouping revealed multiple approaches to the relationship between case management and self-care services beyond the four different models employed as sites within the case studies.
Indeed some had no discernable relationship identifiable between the two. In others, case management had incorporated self-care informally as part of good practice. Whereas policy has tended to focus on self-care activities as sets of discrete projects the present study identified a more mixed picture, suggesting that the relationship is markedly more complex than that evident in the guidance (DH, 2006b).
More generally this study has helped to identify the core tasks of case management for people with long-term conditions. It revealed, for example, that some case management tasks were rarely undertaken, in particular services detailed in care plans were usually not costed and therefore the overall cost of the care package was not recorded. Without this budgets cannot be devolved to case managers, a development critical to the provision of more responsive patterns of care within case management (Challis, 1992). This is of considerable importance in view of the move towards personal budgets in healthcare (Cm 7432, 2008) and there are indications that lessons from the rollout of individual budgets in social care could inform the development of more personalised approaches to NHS funding and the shift in professional orientation which may be required as a consequence (Glendinning et al., 2008).
Furthermore, as demonstrated in Chapter 5 it was possible to compare data from the national survey of case management with those from earlier surveys of local authority care management arrangements (Challis et al., 2009; Xie et al., 2008a). This permitted a comparison of the similarities and differences in the approach and staff mix in the different service settings. It also enabled an assessment to be made about the extent to which case management for people with long-term conditions contains the key features of intensive case management defined as a specific service targeted at those with complex needs at risk of admission to institutional care located within a wider network of other appropriate services (Challis et al., 2001; 1995).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 186
8.2 Key messages from the research
8.2.1 Literature review
This study began with an extensive review of the literature relating to nurse case management (Reilly et al., 2010), the implementation of self-care support (Berzins et al., 2009) and the relationship between the two. There were three principal sets of findings. First, nurse case management is implemented in a variety of ways, often dependent on locally available services and target client groups, but generally involving nurses undertaking the core tasks of case management: assessment, care planning and implementation of the care plan. Implementation could also involve therapeutic interventions and disease management. Studies were found to have failed to systematically examine the processes that constituted case management, the content of which requires further understanding. Second, in the UK self-care support was found to be predominantly delivered using patient education, often supported by psychological interventions to reduce anxiety and depression. These were mostly condition specific but could also be generic and were delivered using professionals or volunteers. There were modest benefits from the interventions which tended to be in higher levels of self efficacy, illness knowledge and physical functioning. Third, self-care support was a feature of most of the reviewed nurse case management interventions, albeit less formal, typically consisting of individual education and advice regarding medication and appointment management as well as psychological support for patients and carers. However, few self-care related outcomes were measured. Of those that were, it was noted that use of health services sometimes decreased and on the other hand medication adherence increased.
8.2.2 Case management arrangements
Over half of case management services were targeted at people with chronic obstructive pulmonary disease, coronary heart disease, diabetes or people with multiple conditions. The case studies showed that some primary care trusts had converted existing disease specific nurse teams into case management teams, for example cardiac specialist nurses had become case managers in two sites. This meant that case management teams were at times less a new development and more a ‘rebadging’ of pre-existing initiatives. Data from the national survey revealed that almost four fifths of the case managers were based in nurse teams in primary care with few based in integrated teams. All primary care trusts surveyed used nurses as case managers, about a half used therapists and a smaller number social workers and assistants. This diversity was reflected in the case study sites three of which had therapists as case managers within their long-term conditions service whereas in the other one only nurses and none had social workers in their team.
The most frequently reported methods of patient identification for the case management service for people with long-term conditions were referrals from other professionals followed by those identified by PARR II, a case finding tool, (Billings et al., 2006) and via the Single Assessment Process. Of these the method judged most effective was referrals from other professionals, noted by the majority of respondents to the survey. The case studies suggested that there were problems using patient identification tools due to both lack of administrative support and the details generated being out of date. Over half of the survey respondents reported that cases were allocated on the basis of staff qualification or the predicted intensity of

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 187
involvement and this approach was replicated in two of the case study sites. The majority of long-term conditions services, including all of the case study sites, utilised documentation associated with the Single Assessment Process processes in their locality. In some cases this was a standardised assessment tool; such as Easycare (Philp, 2000) or FACE (Clifford, 2005), but more frequently locally developed tools were used.
The national survey revealed that most of the core tasks of case management were in operation: assessing health care needs, care planning, implementation and monitoring of the care plan, reviews and providing patient education and clinical oversight. A majority of respondents also reported carrying out the assessment of social care needs but few could authorise services such as domiciliary care provided by local authority social care services and an even smaller percentage of respondents reported that financial assessment and case Most services strove to provide continuity of care and had review systems in place, with the review undertaken by the case manager in conjunction with the service recipient. Interestingly, the survey findings indicated that the most frequently reported activities for case managers were arranging and allocating services as well as undertaking medication reviews, patient advocacy and providing emotional support and hands on care. Together these findings suggest a lack of clarity of role for case managers within long-term conditions services. Certainly the longstanding conflict between the care management role and responsibility for clinical needs was evident (Challis, 1994; Challis it al., 1995).
Furthermore, at the time the survey was undertaken it appeared that little priority was accorded to arrangements for patients to be discharged from the case management service, either to other services such as community nursing or to self-care support services. To what extent this failure to focus on processes to facilitate this in a planned and systematic way reflected the relative infancy of these services and the requirement to achieve caseload targets was not clear but it is likely to become an area of service development in the future.
As noted above, the study also explored variations between case management for people with long-term conditions; care management arrangements for older people; and adults with physical and sensory disabilities. Goals and service arrangements for care/case management were broadly similar for the three target groups. However, when local authority care management arrangements for older people and case management for long-term conditions provided by primary care trusts are compared in terms of their service characteristics and practice a picture emerges of the latter as a service more clearly targeted on people with complex needs, reflecting the different emphases in policy guidance.
8.2.3 Self-care services and case management
The promotion of self-care support for people with long-term conditions was adjudged to be a service objective for almost all survey respondents (See Chapter 4, Table 4.4) although less than half of them reported that they had been involved in the development of self-care support services. Additionally, survey respondents reported a focus on patient education and information in the case manager role although less than half reported that training for case managers specific to self-care services and support was available. Over half of the long-term conditions services, including three of the case study sites, reported links with voluntary organisations

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 188
providing self-care support. However, only a third of survey respondents reported that there was a directory of these local services of self-care support available to case managers.
The most frequently reported types of self-care support available in localities were generic courses, such as the Expert Patient Programme; condition specific groups; and advice and information. The survey revealed that the use of technology, self help groups and informal therapeutic support were also widely available but that this was not the case for alternative therapies. The most available type of self-care support for all conditions except coronary heart disease was advice and information. For this condition it was technology and equipment. For people with multiple conditions, generic self-care support was widely reported. Focus group discussions in the case study sites and within the service user consultation exercise revealed a concern about the suitability of self-care support services for case managed patients, due to their age, severity of conditions, subsequent limited mobility and overall frailty.
Most survey respondents reported that case managers undertook assessments to determine patient eligibility for entry into self-care services and did indeed refer patients to specific self-care support services. A minority also reported that their case managers contributed to both the development and provision of self-care services. The case study sites, selected in part because their case management services had links with self-care support services, confirmed these findings. In all four self-care support was provided by case managers, either through patient education on a one-to–one basis, by participation in the mainstream provision or the development of a specific self-care service.
Interestingly, observations from the case studies also suggested that although self-care support activities were taking place they were probably not recognised as such by case managers. As yet little attention had been paid locally to the linking of the formal processes of self-care and case management arrangements in localities. This lack of clarity of the interface between self-care support and case management perhaps also contributes to a situation in which the tasks associated with the former are not currently clearly defined in the care planning process and therefore not clearly documented in the subsequent care plan. Thus for example, case managers, community nurses and social workers, may undertake tasks such as arranging and ensuring attendance at hospital for outpatient appointments or attendance at self help groups, thereby facilitating wider activities without tending to record these in any specific way. This observation provides an insight into the finding from the survey that only that only a small number of people receiving case management were also reported as receiving a form of self-care support services.
8.2.4 Links between case management and other local services
Most survey respondents indicated that the objectives for their service included improvement of the extent and scope of services and the coordination of care to people living in the community, reflecting the policy objective of increasing service integration at a local level (Cm 7432, 2008; Cm 6737, 2006). Our study indicated that this was reflected in practice with, for example, about half of respondents reporting case managers used multi-disciplinary team meetings to review and share information about patients. The nature and extent of local links between case management services for people with long-term conditions and other services are summarised below.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 189
8.2.4.1 General practitioners
Over a quarter of survey respondents reporting that case managers were based in GP practices and, more generally, joint working was facilitated by the fact that most long-term conditions services were aligned with them. The case studies revealed evidence of mixed relationships with GPs. In some cases this was attributed to a lack of clarity over the case manager role, particularly when a service was first introduced. It was suggested that when GPs had seen benefits for their patients of the case management role within the long-term conditions service they became supportive of the service and its objectives.
8.2.4.2 Wider health services
Case management services for people with long-term conditions varied in the nature and extent of their links with other providers of healthcare both within their primary care trust and further a field. Most case managers were based in nurse teams in primary health care but over two thirds of survey respondents had case managers also based in hospitals. However, very few were located within intermediate care services and their management arrangements were almost exclusively undertaken by health services staff.
Most long-term conditions services had agreements with community nursing services and end of life care services within their primary care trust. Agreements with acute services and intermediate care services were also frequently reported. However, there were very few agreements with old age psychiatry and hospital pharmacy services and under a third of the long-term conditions services had access to medical advice via dedicated physician sessions.
Information was shared with other NHS services mostly through the Single Assessment Process and, more generally the exchange of written information. It was reported by survey respondents, for example, that information was shared with the intermediate care sector in a variety of ways: the Single Assessment Process, patient held records; and written information. Disease registers were the least reported as a means of communication between services. Care plans usually included services provided by the primary care trust and less frequently the intermediate care sector. The contribution of personnel based in the local acute/foundation trust to the care plan was much less frequently recorded, possibly because the patient was not in receipt of services from this sector of the NHS.
Survey respondents reported that a majority of case managers could access all information about their patients electronically within their primary care trust or acute hospital service. Conversely a minority reported that record systems of the long-term conditions services were integrated with others in their primary care trust. It was also noteworthy that all case study sites reported difficulties with regard to the transfer of information electronically both within the NHS and to their colleagues in the local authority social care services.
8.2.4.3 Local authority social care services
Over half of the long-term conditions services reported formal links with local authority adult social care service. Information was most frequently shared using the Single Assessment Process or other documentation. However, as noted above, few case managers could assess for or authorise local authority services such as domiciliary care. Nevertheless, it was estimated by the majority of survey

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 190
respondents that care plans routinely detailed the contribution of local authority social care services.
A hallmark of joint working, the use of a single case file shared between all professionals involved in the care plan compiled by case managers, was rarely reported by survey respondents. However, integrated service provision was fostered by the co-location of case managers for long-term conditions in integrated health and social care teams in more than half the long-term conditions services represented in our study sample although line management arrangements for these staff was usually from within the NHS. Interestingly, the case studies showed differing patterns of linkages with local authority services and, as evidenced by the pilot integration projects, a willingness to experiment in this context.
8.2.4.4 Voluntary organisations
The response to the national survey indicated that over half of the case management services had links with voluntary organisations, typically Age Concern or a locality specific organisation. However, very few long-term conditions services reported that care plans included the contribution of voluntary organisations providing self-care services to patient care. Reflecting one of the criteria for their selection, staff in three of the case study sites had involvement with local voluntary organisations providing self-care services. These included groups for particular conditions, as well as those providing more generic assistance such as respite care and practical help.
8.3 Emergent themes
8.3.1 Self-care support services within the NHS and social care model for long-term conditions
As noted in Chapter 2 the long-term conditions policy was predicated on the Kaiser Permanente Triangle as a basis for differentiation (DH, 2004b; c; 2005b), placing service user needs within three levels of care: supported self-care for the majority of the chronic care population; disease/care management for patients who have multiple long-term conditions; and case management for those patients who are very high intensity users of unplanned secondary care (DH, 2004b; c; 2005b). However, these are not mutually exclusive categorisations and the findings of this study show that case management consists of a series of core tasks as well as elements of disease management and supported self-care. The initial guidance described the latter as the first level of care but this study suggests that it remains an important component of both disease management and case management.
Many of the available self-care support services were similar to those identified in the literature review (Chapter 2) providing education and support for people experiencing arthritis, diabetes and chronic obstructive pulmonary disease. The findings from this study suggest that links with self-care support services were tenuous in practice. For example, self-care support services were not frequently used by case managed patients or routinely recorded in care plans. One reason for this may be the extent to which many self-care support services are in fact appropriate to meet the needs of the typical case managed patient. Issues of transport, mobility and complexity of needs were suggested by interviewees within the focus groups as barriers to participation for case managed patients. Additionally, it may of course be that case managed patients do not wish to use self-care support services. Interestingly, the

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 191
neurological conditions National Standards Framework (NSF) noted that patients must be willing to engage with services voluntarily (DH 2005a). As stated in the policy, self-care support must have the capacity to be individualised this may mean it is administrated by a case manager or another named person within the care plan (DH 2000b).
Previous research conducted by the Department of Health reported that only one primary care trust of those surveyed had a lead for self-care (DH 2005e). The picture in 2008 as evidenced by our study was different with regard to this with managers of long-term conditions services being involved in the development of a self-care strategy locally. However, our data also suggests that this involvement at a strategic level does not, for whatever reason, translate into self-care support services that are being frequently used by case managed patients. The case study sites demonstrated considerable activity at the interface between case management and self-care within the long-term conditions service. However, it must be remembered that these sites were deliberately selected as exemplars. Other primary care trusts identified in the survey appeared to have less developed self-care support services and thus there will be greater variation nationally than is shown between the four case studies.
The early research also demonstrated that some aspects of self-care support that were being carried out were not always being formally recognised as such (DH, 2005e). This was thought to still be the case amongst interviewees in this study. Informal patient education for example, regarding medication usage, constitutes supporting self-care. As it is difficult to define exactly where self-care starts and ends it may be inevitable that measuring its use outside of formal interventions remains difficult. Our study also suggests a lack of clarity about which types of self-care support are of most benefit to people with complex needs receiving case management. It is not necessarily the case that case management services require separate self-care support services solely for their patients but rather that existing services develop more flexible ways of working that are more responsive to the needs of the individual, taking into account factors such as mobility and capacity for learning. If such services were routinely available this may widen the options for people exiting case management into both disease management and supported self-care.
Overall, the findings from this study show that there is a recognition of the potential contribution self-care support can make to case management services and strategic work in this area is taking place at primary care trust level. However, the current services available may not be particularly accessible to case managed patients and different self-care service approaches may be required to address these barriers.
8.3.2 Programme fidelity within case management
Fidelity to the core elements of case management refers to the degree to which a particular service follows, or is consistent with a programme model, a well-defined set of interventions and procedures to help individuals achieve some desired goal (Reilly et al., 2010). It is a concept which has been explored previously in the case management literature relating to adults with long-term mental health problems (Bond et al., 2000). A recent review of case management for long-term conditions highlighted the need to specify what and how case management services should be provided to people with long-term conditions, offering consistent and coherent implementation along with measuring what is provided. It concluded that without

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 192
such specificity and transparency of the content of interventions, evaluations of case management will have limited utility and evidence based practice will be unattainable (Reilly et al., 2010). Here the concept of programme fidelity is explored in the context of entry into case management and care planning using data from the study as appropriate.
8.3.2.1 Entry into case management
The current policy model (DH, 2005b) could be considered as viewing those people experiencing one long-term condition as suitable for disease management and only when co-morbidities occur, requiring a more complex and coordinated approach, should patients be eligible for case management. As shown in Figure 7.1 this study has demonstrated that the case management service for people with long-term conditions is targeted locally on patients with specific conditions, reflecting common health priorities. It is interesting to note that the two of the most cited target conditions (coronary heart disease and diabetes) all have a corresponding national service framework (DH, 2000b; DH, 2001a) in place and another (chronic obstructive pulmonary disease) is in development. Implicitly this is a service targeted on patients experiencing physical illness who are frequently admitted to acute hospitals and not those with dementia or other long-term mental health problems.
Figure 8.1 Case management services: target conditions (n=56)
Source: Table 26, Chapter 4
Our study suggests that the targeting of case management at specific conditions blurs the boundaries between case management and disease management. Where disease specific case management services had developed they often appeared to be a ‘re-branding’ of an existing disease management service within the primary care trust, meaning that case management had essentially replaced disease management
0 10 20 30 40 50 60
CHDCOPD
DiabetesMultiple conditions
Other neurological conditionsAsthma
HypertensionStroke and Transient Ischaemic Attack
Musculoskeletal conditionsEpilepsyCancer
Mental healthHypothyroidism
FallsOther
percentage

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 193
services. It is thought that this practice (possibly carried out as a response to the requirement to have a case management service established by a certain date) runs the risk of moving some people into the case managed tier of service receipt who may have their needs met by disease management services alone. In particular, disease specific services run the risk of targeting people for case management at an early and less helpful stage because of the presence of disease rather than level of frailty or need, leading to very large caseloads. These, due to their numbers, act more like disease registers than to cases being actively managed as defined in policy guidance (DH, 2004b). This was most clearly demonstrated by the cardiac specialist case managers in the fourth case study.
Findings from this study also suggest that there are currently two principal ways of entering case management, patient identification through a case finding tool or referral from a professional. It was often felt that the latter allowed professional judgement to be exercised and was considered the most effect method; although typically both were used in tandem. The professional judgement of the referrer and the representative of the case management service together may be the most effective way of identifying patients with multiple symptoms indicative of co-morbidities not necessarily attributable to a single condition, as was the case in a previous study (Challis et al., 2008a). It may be that multiple conditions are more important than single disease markers although a myriad of factors, many of them social and patient specific are often precursors of emergency hospital admission (Challiner et al. 2003; Hudson et al., 1995). Typically, these are older patients who are not managed well within the acute hospital setting (Rockwood et al., 2007). Their overall frailty contributes to the chronicity of the illnesses and for them the long-term conditions case management service may be of benefit.
With regard to case finding, screening at the point of entry to the service appears to be more of a first stage in the assessment process rather than an opportunity for diversion to other services: disease management; self-care support, local authority adult social care; GP; or community nursing. It may be that established links between the case management service and other local services promote diversion, prior to entry into the long-term conditions service. However, it is important to recognise that at this point there is the additional opportunity to prevent duplication of service. For example, if the local authority is already providing a care management service, the involvement of the long-term conditions case management service may not be the most appropriate response to increased health needs. Rather the incorporation of health services within the care management care plan already in place may be more appropriate offering the patient a more integrated response and affording both services the opportunity to respond more efficiently to individual need.
Similar to previous research (Challis et al., 2009) the most frequently used form of assessment documentation reported by survey respondents for use in the case management service for people with long-term conditions was that developed locally for older people within the Single Assessment Process. This may indicate that services are moving away from a more standardised approach to assessment and thereby risk reducing the validity and reliability of the methods used (Stewart et al.1999). The features of long-term conditions are similar nationwide so the lack of a standard assessment framework is notable and may contribute to the variety of local developments in terms of practice and patient outcome.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 194
8.3.2.2 Care planning
The process of care planning and its implementation were identified as core tasks of case management in this study. It is also recognised in national policy as a key area for future development, viewed as: the basis for planning and delivering care for people with long-term conditions; a means of underpinning partnerships between patients and services; and facilitating improved patient information (Cm 7432, 2008; DH, 2009). The effective implementation of a care plan requires that case managers have a caseload which permits them to monitor and adjust its components to reflect changes in the level of patient need. Thus caseload size must be an important component of targeting within case management service for people with long-term conditions. The case study sites revealed interesting information about caseload size within the service. The concept of a team caseload is helpful here. Typically they are stratified with some cases considered ‘dormant’ yet still included to meet policy targets. Sometimes a similar policy might be adopted in relation to the caseload of a case manager. Thus in practice case managers might be actively engaged with a subset of patients on theirs or the teams caseload.
Previous research has highlighted other targeting mechanisms within the case management process which will influence the implementation of the care plan (Abell et al., 2010a). Two of these were also evident in this study: the qualifications of staff acting as case managers and the frequency of visiting. The first of these is particularly relevant in the context of the development of the long-term conditions service because of the stratification of nurses based on previous experience and specific training evidenced in this study. The latter is characteristic of an intensive case management service, as noted in Chapter 5, a specific service targeted at those with complex needs (Challis et al., 2001). Both these factors are measures of a differentiated response to case management whereby the response to individual need differs in terms of staff skill and frequency of visiting (Hughes et al., 2006). It could be argued that another hallmark of a targeted case management service is one which has clearly defined criteria for exit, possibly to other elements of a long-term conditions service. Generally speaking this feature was absent from the services in our study.
8.3.3 Developing the workforce
It did appear within the study that there was a concern about the balance of responsibilities for case managers between their responsibility to act as case managers, and the demands upon them as trained nurses with clinical expertise. The former responsibility requires them to take an oversight and responsibility for the range and coordination of care, support and treatment received by a patient. The latter demands that as the nearest trained clinical worker they take responsibility for addressing particular nursing or other needs. Such pressures can become a considerable source of role conflict for staff where role expectations are not made clear. There are examples, in the UK and elsewhere, when staff have been expected to act on a part time basis in traditional clinical or related roles, say as district nurses or social workers and part time, as case managers, that such role confusion has led to less effective performance of roles or considerable effort to define when they are in each particular role (Challis et al., 1990; 2002; Department of Health, 1993; 1994; Kendig et al., 1992).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 195
The professional training and background of staff will influence their orientation to the task of supporting people with long-term conditions, so in order for case management to become the primary role of the case manager rather than clinical tasks it must feature in training. It is interesting to note that respondents to our survey stated that their most frequently provided training for nurses was aspects of supporting people with long-term conditions or the development of advanced clinical skills. If the content of the practice of case management itself does not feature within training programmes, then it is not likely to become ‘core business’. One of the issues to emerge from the case studies was the confusion surrounding the case manager role with that of other professionals involved in their care, specifically district nurses and GPs. In one case study site the case managers themselves were not clear about their own role and had anticipated it being less of a clinical role. Before the role can be effectively communicated to other professionals the case managers themselves must be clear of their remit and where the boundaries lie between case managers and district nurses in particular.
Previous research has found that patients with more complex and demanding needs may require more than one individual to undertake case management responsibilities and hence it became a shared responsibility amongst the wider team and recognised as part of a team and not an individual caseload (Stein et al., 1990). Such an approach has been used to avoid the risk that certain cases may prove very demanding and lead to staff ‘burn out’. It is interesting that in our study it was noted in a staff focus group discussion that often more than one case manager would attend to a single patient’s needs to try to limit the demands of people with very intense needs on a single case manager.
Our study revealed a multiplicity of grades and types of worker in case management services. In social care there has been considerable debate as to which patients are allocated which type or level of worker and hence a vagueness of differentiation of response. However, this has been attenuated as a problem by the relatively limited range of staff grades that might be involved, generally qualified social workers or non professionally trained staff. In long-term conditions case management the range of potential staff appears much greater and with it there is greater need for clarity in differentiation of response at the practitioner level. As noted above, this is a salient observation in a service setting characterised by considerable investment in developing differentiation through targeting and case finding processes.
8.3.4 Service development
Following the introduction of the community care reforms, variation between local authorities in the development of care management arrangements for all adult user groups has been noted, attributed to the general nature of the initial guidance (Weiner et al., 2002; Venables et al., 2005; Xie et al., 2008a;b). In older peoples’ services care management arrangements were characterised by an absence of specialist intensive services or selective case management. Only half of the local authorities demonstrated evidence of a differentiated service by targeting staff and resources according to need and there was little evidence of integration with health staff (Weiner et al., 2002). A similar state of affairs might develop within the case management service for people with long-term conditions in view of the broad nature of the initial guidance and the recent removal of the public service agreement target of a five per cent reduction in emergency hospital admission. It is possible that patients with similar needs will have very different experiences depending on which

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 196
primary care trust services are provided by, given a similar lack of guidance as to the precise form and content of case management to date. Furthermore, there is a debate as to whether the development of case management should focus on long or short term benefits. Many primary care trusts in our study demonstrated that they had had short term goals reflecting the targets of establishing case management and then the anticipated long-term outcomes of reduced admissions. However, the intermediate processes, such as programme fidelity within case management arrangements, as illustrated above, remain insufficiently defined. This is likely to be an important area for the development of case management where the content of the intervention needs to be related to the precise goals it is designed to achieve (Challis, 2000; 2003). In the absence of this clarity, a variety of forms of case management are likely to continue to develop, not necessarily of proven efficacy.
The reduction of inappropriate hospital admission as a government target and means for identifying suitable patients can also be seen to have been problematic for the development of case management. To date, research has demonstrated that the use of hospital admissions as a performance indicator does not adequately measure the success of interventions aiming to reduce admissions amongst older people as these rates fall without any intervention (Roland et al., 2005). Furthermore, an early study of case management for people with long-term conditions reported that those with initially high levels of emergency admissions decreased over time, and the admissions of those with initially few admissions increased, showing a regression to the mean (Challis et al., 2008a). Gravelle and colleagues (2006), found from the Evercare Programme, that this form of case management introduced an additional range of services in primary care but there was no associated reduction in hospital admissions. Some of this effect may have been attributable to the targeting processes employed; resulting in support for additional cases thereby masking any effect upon hospital admissions. Parker and colleagues (2002) found that discharge interventions that included both hospital and community interfaces had the greatest impact on readmission to hospital. In the absence of the hospital admissions target the focus will be upon the achievement of patient quality rankings (Cm 7432, 2008). To promote joint working between health and social services to achieve this may require a degree of alignment of performance indicators.
A successful case management service is often measured by its ability to co-ordinate a range of services (often from different sectors) to meet the specific needs of the service user (Challis et al., 1995). When a new case management service is implemented therefore, it cannot be viewed as a service to be developed in isolation but one that must quickly establish links to existing services in the area. Links between case management in the primary care trust and local social care services will certainly be key. National policy has emphasised the importance of integrating health and social care services, both at structural and process level through joint working practices, assessment and care planning (Cm 6737, 2006). Due to the shared target population and goals, the local systems of local authority care management and NHS case management might be considered as interdependent. If one area is less developed and the other better developed the demand for the latter is likely to rise. Integrated working practices will be important between these two sectors at every level of the service, from strategic joint commissioning to the local knowledge of case managers. It will also be important to recognise the potential contribution of the voluntary sector, both in respect of their existing contribution to self-care services and in the development of newer services such as those relating to the support of carers of people with long-term conditions. However as this study has

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 197
highlighted, it is often difficult to establish necessary links with services within the same sector (and same service model) and therefore developing integrated practices as mentioned above will require specific focus.
Thus an optimal service configuration must include clear opportunities for the movement of patients between case management, disease management and supported self-care, associated with the use of effective assessment and regular review. The role of other services both within and outside the NHS must also be considered particularly care management provided by the local authority and self-care support provided by voluntary organisations. Within NHS services there was little involvement of geriatric medicine, with few services in our study reporting a formal link. Given the arguments of the “founders” of geriatric medicine about complexity and multiplicity of disease in some older people; interactions between social and clinical needs (Isaacs, 1981); and the need for service linkages to respond effectively it seems that this has not happened, despite the age of most people receiving case management (Challis et al., 2008a). The evaluation of the Evercare pilot projects describes geriatricians working as mentors to advanced primary nurses as making a ‘valuable contribution’ to case management and suggests their involvement should be promoted by the NHS (Boaden et al., 2006).
The national survey conducted as part of this study showed little evidence of routine linkage with local authority services, which has been a feature of recent policy. The Darzi review (Cm 7432, 2008), building on the integration focus of the White Paper, Our Health, Our Care, Our Say (Cm 6737, 2006) promoted the development of integrated services between hospital, community and social services through the use of integrated care organisations to respond to local need. Patients referred for case management are likely to have complex health and social care needs. Whilst their daily health needs will be met through services within the primary care sector their social care needs, for example, help with rising and retiring and the provision of meals, will be met by the local authority. This requires a level of joint working, rather than parallel working, in order to ensure that a cost efficient service is delivered.
8.4 Recommendations for further research
This study has demonstrated that not only is there variation in the range of self-care services in a locality and their links with the long-term conditions service but a much wider issue about the extent to which self-care support should be integral to the care plans of those in receipt of case management from the long-term conditions service. Thus our findings suggest that the local service delivery model is more complex than that described in the Kaiser Permanente Triangle (DH, 2005b) and in this context a number of areas for further enquiry are detailed below. All are derived from the principal themes emerging from the research discussed in the previous section. The first three (8.4.1, 8.4.2 and 8.4.3) relate to the interface between self-care services and case management which is at the centre of this study. The next two (8.4.4 and 8.4.5) seek to further explore the nature of the case management intervention and offer a means of categorising and evaluating different approaches, thereby addressing the issue of programme fidelity. Closely linked to this is the issue of targeting within the long-term conditions service which is identified as a further area of enquiry (8.4.6). One means of targeting is the identification of different grades of staff to undertake the many tasks within a long-term conditions service, thereby addressing an important component in the developing workforce agenda for the service. Finally two areas for further enquiry are identified which link to future service

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 198
development. One is derived form the requirement for case management to link with other local health and social care services identified in the previous section (8.4.7) and the other as a consequence of a policy announcement made during the course of the study (8.4.8). These areas for future research are not explicitly prioritised although it could be argued that further exploration of the two areas relating to programme fidelity may contribute most to the effectiveness of the service in the longer term.
8.4.1 The nature of self-care support, target groups and appropriate time frame
Policy guidance on self-care support services has influenced their development in localities (DH, 2006b). This study has demonstrated that the types of self-care services valued by people with long-term conditions extend beyond this initial specification. Furthermore, this study has shown that the type of support valued by people varies according to specific long-term conditions, their severity and individual choice. The perspective of people using self-care services is an area for further enquiry which would inform service commissioning.
8.4.2 Patient pathways within the long-term conditions service
At the introduction of the long-term conditions strategy three levels of care were identified: supported self-care for the majority of the chronic care population; disease/care management for patients who have multiple long-term conditions; and case management for those patients who are very high intensity users of unplanned secondary care (DH, 2004b; 2004c; 2005b). This study has identified both the complexity of the interface between case management and self-care support and two distinctly different approaches to its provision. First, a bespoke approach delivered by the case manager in the context of routine communication with patients and, second, that delivered through universal methods such as group and written information. Further enquiry into the role of self-care support in the patient pathway would inform both practice and the commissioning of self-care support services.
8.4.3 Carers of patients with long-term conditions
Over a number of years policy guidance has made explicit reference to the crucial contribution of carers to the care of all vulnerable adults emphasising the importance of taking into account their wishes in the formulation of a care plan (Cm 4169, 1998; Department of Health, 2001b; Cm 6499, 2005; HM Government, 2008). In this study it was noted that self-care support for people with complex needs currently does not explicitly address the needs of carers. The incorporation of a carer perspective into the commissioning of self-care services is an area of enquiry worthy of further consideration.
8.4.4 The role of care plans in case management
Subsequent to the introduction of case management for people with long-term conditions, policy guidance has specified a requirement that everybody with a long-term condition will have a care plan by 2010 (Cm 7432, 2008). This study has revealed that although care planning is reported as a core task, frequently there was an emphasis on including services provided within the primary care trust and those
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 199
provided by other sectors of the NHS and the local authority were less likely to be included. The policy emphasis on improving the patient experience recognises the importance a comprehensive approach to care planning and the development of practice in this area will be worthy of further investigation in time.
8.4.5 Outcomes for patients and carers of different approaches to case management
Policy guidance has emphasised the importance of a focus on improved outcomes for patients in terms of quality of life together with recognition that localities would adopt different approaches (DH 2005b). This study sought to identify key areas of variation, to systematically categorise them and by means of a case study approach explore them in more detail. A logical next step would be to undertake more detailed research to explore the relative merits of different approaches for patients and carers. This would include an evaluation of the relative cost-effectiveness of these different approaches in achieving outcomes for patients and carers. Such a study would use the perspective of formal health and social care providers and patients and include the direct costs of primary, community, secondary and tertiary health care services. The outcomes would include health status, well being and quality adjusted life years.
8.4.6 Targeting within a long-term conditions service
The Kaiser Permanente Triangle identified three components of a long-term conditions service: self-care support; disease management for a single condition and case management for multiple conditions (DH, 2005b). Our study has both revealed multiple linkages between them and a failure to distinguish adequately between the type of support provided to those with a single condition from that required by those with multiple conditions. This may manifest itself in a case management approach being applied to patients with a range of needs rather than focussed on those with the most complex. The case management literature indicates that targeting mechanisms are important in maintaining the focus of a service and this will become an increasingly important issue warranting further debate and enquiry.
8.4.7 Embedding case management in local services
Recent policy guidance has emphasised that within a long-term conditions service it is important that there is a lead professional whose role is to promote access to the services required to meet the needs set out in the care plan (Cm 7432, 2008; DH, 2009). This study has revealed significant variation in both the number of formal agreements and means of exchanging information between long-term conditions services and other providers of health and social care in the locality. It was also apparent at an informal level. This is an area for further service development and further research at both a strategic and practice level would inform.
8.4.8 Financial management arrangements in case management
Policy guidance subsequent to the introduction of case management for people with long-term conditions specifies the introduction of personal budgets into the service (Cm 7432, 2008). This study highlighted that few services have mechanisms in place which identify the costs of services or any mechanism for monitoring the cost of

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 200
individual care packages and support. In the not too distant future this is an area which will receive greater scrutiny and would therefore benefit from early exploratory research.
8.5 End note
This study was conducted in a context in which policy guidance identified self-care as integral to the maintenance of health and well-being for people with long-term conditions. It has been estimated that a large number of people suffer from a long-term condition and many of these are older people and significant users of healthcare resources. Government guidance recommends that patients receive help appropriate to their level of need: supported self-care; disease care management or case management. The role of community matron has been developed to undertake the case management role and within this assess the extent to which self-care support services might contribute to patient welfare. As noted previously this research had three aims. First to map NHS case management services in primary care for people with long-term conditions. A second aim was to classify programmes on features of case management implementation with particular focus upon the integration of care between primary and secondary care and between health and social care. Finally, to sought to identify the extent and nature of self-care initiatives within this service and to investigate their role initiatives as determinants of service entry and exit.
At the beginning of the investigation a literature review explored the role of self-care within case management for people with long-term conditions: it scoped the nurse case management literature; summarised interventions supporting self-care for older people; and appraised how self-care may be supported within case management interventions. These findings informed the development of research instruments. Collection and analysis of the data described in this report took a mixed methods approach comprising three elements: a survey relating to self-care and case management arrangements; interviews and focus groups in four case study sites; and comparison of the survey data with previous survey data. Finally, the views of older people on the principal issues arising from the research were canvassed.
A number of key findings emerged from the study relating to the nature of case management, its links with other local services and the development of local self-care services. The majority of case management services were targeted at people with chronic obstructive pulmonary disease, coronary heart disease, diabetes or multiple conditions, typically identified via a referrals from other professionals, a case finding tool or via local implementation of the Single Assessment Process. All services undertook the assessment of health and social care needs but fewer undertook care planning and service allocation, monitoring and review, together with associated financial management tasks within the case management process. Additionally, some case managers also provided patient advocacy, emotional support and hands on care as well as conducting medication reviews. Together these findings suggest: considerable variation in case management arrangements; a different emphasis in the case management process compared with local authority care management arrangements; as well as greater clarity in the identification of their target population.
The improvement of the extent and scope of services and the overall coordination of care to people living in the community were widely reported service objectives. Our study revealed that links between case management services for people with long-

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 201
term conditions were most developed with other services provided by primary care trusts, particularly community nursing services, reflecting their shared management structure and often their co-location. In contrast links with local authority social care services, reflected in joint initiatives and working practices, were more variable and most often reported in the use of shared assessment documentation. Similarly there was evidence of variation in working relationships with general practitioners but overall indications of burgeoning relationships. In both settings co-location was a significant factor in promoting working relationships.
Furthermore, the promotion of self-care support was an explicit goal for the majority of long-term conditions services represented in our study. Within localities the most frequently reported types of self-care support available were generic courses, such as the Expert Patient Programme; condition specific groups; and advice and information. More generally the type of support valued by people varied according to specific long-term conditions, their severity and individual choice. In the long-term conditions service there were indications that education and guidance in respect of self-care was part of the support patients received from case managers although it was often not explicitly recognised as such. It was also suggested that often patients receiving case management experienced limited mobility and were generally frail and these factors prevented them from participating in self-care support groups.
From this we have identified three principal conclusions. First, the case management services reviewed were relatively new and considerable variation in approach was evident across the country, mirroring earlier developments in local authority care management arrangements. However, a key difference was that the case management service was more explicitly targeted on those with the most complex needs. Second, being a nurse-led service, links within the primary care sector were strong, reflecting its origins. On the other hand, there were poorer links with both other health services and social care although examples of pilot initiatives to promote joint working were found. Third, self-care initiatives existed within localities but they are not always accessible to case managed patients although some case managers provided self-care support, such as patient education through their routine contact with patients.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 202
References Note: Studies referred to in chapter 2 section 2.1 of the literature review are marked by numbers 1-29. Studies referred to in chapter 2 section 2.2 of the literature review are marked by numbers 30-47.
1Aadalen, S.P. (1998) Methodological challenges to prospective study of an innovation: interregional nursing care management of cardiovascular patients, Journal of Evaluation in Clinical Practice, 4, 3, 197-223.
Abell, J., Hughes, J., Reilly, S., Berzins, K. and Challis, D. (2010) Case Management for Long-Term Conditions: Developing Targeting Processes, Care Management Journals, 11, 1, 11-18.
Abell, J., Hughes, J., Reilly, S., Berzins, K. and Challis, D. (2010) Case Management for Long
Term Conditions: The Role of Networks within Health and Social Care Services, Journal of Integrated Care, 18, 1, 46-53.
Abendstern, M., Hughes, J., Clarkson, P., Sutcliffe, C., Wilson, K. and Challis, D. (2010) We need
to ‘talk’: communication between PCTs and other health and social care agencies following the
introduction of the Single Assessment Process for older people in England, Primary Healthcare Research and Development, 11, 61-71.
2Allen, S. (1999) Description and outcomes of a Medicare case management program by nurses, Home Health Care Services Quarterly, 18, 2, 43-69.
Applebaum, R. and Austin, C. (1990) Long-term Care Case Management: Design and Evaluation, New York: Springer.
Arnold, D. (1987) The brokerage model of long-term care: a rose by any other name, Home Health Care Services Quarterly, 8, 2, 23-43.
Audit Commission (1996) Balancing the Care Equation: Progress with Community Care, Community Care Bulletin Number 3, March 1996, London: HMSO.
3Audit Commission (1999) First Assessment: A Review of District Nursing Services in England and Wales, London, Audit Commission.
Austin, C. (1992) When the Whole is More than the Sum of its Parts: Case Management Issues from a Systems Perspective, Paper presented at the First International Conference on Long-term Care Case Management, February, Seattle, Washington.
Bandura, A. (1995) Self-Efficacy in Changing Societies, Cambridge, Cambridge University Press.
30aBarlow, J.H., Turner, A.P. and Wright, C.C. (1998a) Sharing caring and learning to take control: self-management training for people with arthritis, Psychology, Health and Medicine, 3, 4, 387-93.
30bBarlow, J.H. Turner, A.P. and Wright, C.C. (1998b) Long-term outcomes of an arthritis self-management programme, British Journal of Rheumatology, 37, 1315-19.
31Barlow, J.H., Williams, B. and Wright, C.C. (1999) Instilling the strength to fight the pain and get on with life: learning to become an arthritis self manager through an adult education programme, Health Education Research, 14, 4, 533-44.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 203
32Barlow, J. H., Turner, A. P. and Wright, C.C. (2000) A randomized controlled study of the Arthritis Self-management Programme in the UK, Health Education Research, 15, 6, 665-80.
Barlow, J., Wright, C., Sheasby, J. Turner, A. and Hainsworth, J. (2002) Self-management approaches for people with chronic conditions: a review, Patient Education and Counseling, 48, 177-87.
4Bergen, A. (1997) The role of community nurses as care managers, British Journal of Community Health Nursing, 2, 10, 466-74.
5Bernabei, R., Landi, F., Gambassi, G., Sgadari, A., Zuccala, G., Mor, V., Rubenstein, L. and Carbonin, P. (1998) Randomised trial of impact of model of integrated care and case management for older people living in the community, British Medical Journal, 316, 7141, 1348-51.
Berzins, K., Reilly, S., Abell, J., Hughes, J. and Challis, D. (2009) UK self care support initiatives for older patients with long term conditions: a review, Chronic Illness, 5, 96-72.
Billings, A., Dixon, J., Mijanovich, T. and Wennberg, D. (2006) Case finding for patients at risk of readmission to hospital: development of algorithm, to identify high risk patients, British Medical Journal, 333, 327-32.
6aBlue, L., Lang, E., McMurray, J., Davie, A., McDonagh, T., Murdoch, D., Petrie, M., Connolly, E., Norrie, J., Round, C., Ford, I. and Morrison, C. (2001) Randomised controlled trial of specialist nurse intervention in heart failure, British Medical Journa,l 323, 7315, 715-18.
7aBoaden, R., Dusheiko, M., Gravelle, H., Parker, S., Pickard, S., Roland, M., Sargent, P. and Sheaff, R. (2005) Evercare Evaluation Interim Report: Implications for Supporting People with Long-term Conditions in the NHS, Manchester, National Primary Care Research and Development Centre.
Boaden, R., Dusheiko, M., Gravelle, H., Parker, St., Pickard, S., Roland, M., Sargent, P. and Sheaff, R. (2006) Evercare Evaluation: Final Report. Manchester: National Primary Care Research and Development Centre.
Bond, G., Evans, G., Salyers, M.P., Williams, J. and Kim, H.W. (2000) Measurement of fidelity in psychiatric rehabilitation, Mental Health Services Research, 2, 2, 75-87.
Bowling, A. (1997) Research Methods in Health Investigating Health and Health Services, Buckingham: Open University Press.
Boyatzis, R. E. (1998) Transforming Qualitative Information: Thematic Analysis and Code Development, Sage, London.
8Boyd, M. and Fisher, B. (1996) Community-based case management for chronically ill older adults. Nursing Management, 27, 11, 31-2.
Braun, V. and Clarke, V., (2006) Using thematic analysis in psychology. Qualitative Research in Psychology, 3, 77-/101.
9Brown, L., Tucker, C. and Domokos, T. (2003) Evaluating the impact of integrated health and social care teams on older people living in the community, Health and Social Care in the Community, 11, 2, 85-94.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 204
10aBrown, R., Schore, J., Archibald, N., Chen, A., Peikes, D., Sautter, K., Lavin, B., Aliotta, S. and Ensor, T. (2004) Coordinating Care for Medicare Beneficiaries: Early Experiences of 15 Demonstration Programs, Their Patients, and Providers. Report to Congres,. Princeton, NJ, Mathematica Policy Research, Inc..
10bBrown, R., Peikes, D., Chen, A., Ng, J., Schore, J. and Soh, C. (2007) The Evaluation of the Medicare Coordinated Care Demonstration: Findings for the First Two Years, Princeton, NJ, Mathematica Policy Research Inc..
33Buszewicz, M., Rait, G., Griffin, M., Nazareth, I., Patel, A., Atkinson, A., Barlow, J. and Haines, A. (2006) Self-management of arthritis in primary care: randomised controlled trial, British Medical Journal, 333, 7574, 879-882.
16bCarcagno, G.J. and Kemper, P. (1988) The evaluation of the National Long-term Care Demonstration. 1. An overview of the channeling demonstration and its evaluation, Health Services Research, 23, 1, 1-22.
Challiner, Y., Carpenter, G.I., Potter, J. and Maxwell, C. (2003) Performance indicators for hospital services for older people, Age and Ageing, 32, 343-346.
Challis, D. (1992) Community care of elderly people: bringing together scarcity and choice, needs and costs, Financial Accountability and Management, 8, 2, 77-95.
Challis, D. (1994) Implementing Caring for People: care management. Factors Influencing its Development in the Implementation of Community Care, London: Department of Health.
Challis, D (1999) Assessment and care management: development since the community care reforms, in the Royal Commission on Long Term Care, With Respect to Old Age: Long Term Care – Rights and Responsibilities, Community Care and Informal Care, Research Volume 3, Part 1, Evaluating the Impact of Caring for People, M. Henwood and G. Wistow (eds) Cm 4192-II/3, London: The Stationery Office.
Challis, D. (2000) Care management in the United Kingdom, in: R. Applebaum and M. White (eds) Case Management Around the Globe, San Francisco: American Society on Aging.
Challis, D. (2003) Achieving coordinated and integrated care among long-term care services: the role of care management. In: Brodsky, J., Habib, J. and Hirschfeld, M. (eds) Key Policy Issues in Long-term Care, Geneva, World Health Organisation.
Challis, D., Abell, J., Reilly, S., Hughes, J., Berzins, K. and Brand, C. (2008a) Evaluating Active Case Management in Greater Manchester. discussion paper (M185). PSSRU, University of Manchester [not publicly available].
Challis, D., Chessum, R., Chesterman, J., Luckett, R. and Traske, K. (1990) Case Management in Social and Health Care: The Gateshead Community Care Scheme, Canterbury, Personal Social Services Research Unit, University of Kent.
11Challis, D., Chesterman, J., Luckett, R., Stewart, K. and Chessum, R. (2002) Care Management in Social and Primary Health Care: The Gateshead Community Care Scheme, Aldershot, Ashgate.
Challis, D., Darton, R., Johnson, L., Stone, M. and Traske, K. (1995) Care Management and Health Care of Older People: The Darlington Community Care Project, Aldershot, Ashgate.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 205
Challis, D., Darton, R., Hughes, J., Huxley, P. and Stewart, K. (1998) Emerging models of care management for older people and those with mental health problems in the United Kingdom, Journal of Case Management, 7, 4, 153-60.
Challis, D., Darton, R., Hughes, J., Stewart, K., and Weiner, K. (2001) Intensive care management at home: An alternative to institutional care? Age and Ageing, 30, 5, 409-413.
Challis, D., and Davies, B. (1986) Case Management in Community Care: An Evaluated Experiment in the Home Care of the Elderly, Aldershot: Gower:
Challis, D., Hughes, J., Clarkson, P., Tucker, S., O’Shea, S., Brand, C., Abendstern, M. and Wenborn, J. (2008b) Enhancing the Efficiency and Effectiveness of Assessment in Community Care, Volume II Self Assessment Pilot Projects: User Needs and Outcomes, Discussion Paper, M178, Personal Social Services Research Unit, University of Manchester at Manchester [not publicly available].
Challis, D.J., Hughes, J., Evans, S. and Gill, J. (1997) Research Briefing: Eligibility Criteria for Social Services for Older People in England, Age Concern England and the Continuing Care Conference, Discussion Paper M012, Personal Social Services Research Unit, University of Manchester at Manchester [not publicly available].
Challis, D., Hughes, J., Jacobs, S., Stewart, K. and K. Weiner (2007) Are different forms of care management for older people in England associated with variations in case-mix, service use and care managers' time use? Ageing and Society, 27, 25-48.
Challis, D., Hughes, J., Sutcliffe, C. and Xie, C. (2009) Care Coordination Arrangements for Older People Discussion Paper, M216, Personal Social Services Research Unit, University of Manchester at Manchester [not publicly available].
Challis, D., Stewart, K., Donnelly, M., Weiner, K. and Hughes, J. (2006) 'Care management for older people: does integration make a difference?' Journal of Interprofessional Care, 20, 4, 335-348.
Challis, D., Weiner, K., Darton, R., Hughes, J. and Stewart, K. (2001) Emerging patterns of care management: arrangements for older people in England, Social Policy and Administration, 35, 6, 672-87.
Challis, D., Xie, C., Hughes, J., Jacobs, S., Reilly, S and Stewart, K. (2004) Social Care Services at the Beginning of the 21st Century- Findings, Discussion Paper M098, Personal Social Services Research Unit, University of Manchester at Manchester [not publicly available].
Challis, D., Xie, C., Hughes, J., Jacobs, S., Reilly, S. and Stewart, K. (2005) Social Care Services at the Beginning of the 21st Century- Summary and Conclusions, Discussion Paper, M105, Personal Social Services Research Unit, University of Manchester at Manchester [not publicly available].
Chen, A., Brown, R., Archibold, A., Alliotta, S. and Fox, P.D. (2000) Best Practices in Coordinated Care, Princeton, NJ, Mathematica Policy Research, Inc.
Chodosh, J., Morton, S.C., Mojica, W., Maglione, M., Suttorp, M.J., Hilton, L., Rhodes, S. and Shekell, P. (2005) Meta analysis: chronic disease self-management programs for older adults, Annals of Internal Medicine, 143, 427-38.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 206
Clifford P. (2005) FACE: An integrated assessment and outcome system for health and social care, National Association of Primary Care Review, Winter 2005/2006, 60-61.
Cm 849 (1989) Caring for People: Community Care in the Next Decade and Beyond, London, HMSO.
Cm 4818-1 (2000) The NHS Plan. A Plan for Investment. A Plan for Reform, The Stationery Office: London.
Cm 6499 (2005) Independence, Well-being and Choice Our vision For The Future of Social Care for Adults in England, The Stationery Office: London.
Cm 6737 (2006) Our Health, Our Care, Our Say: A New Direction for Community Services, London: The Stationery Office.
Cm 7432. (2008) High Quality Care For All: NHS Next Stage Review Final Report, London: The Stationery Office.
Cm 4169 (1998) Modernising Social Services. Promoting Independence, Improving Protection, Raising Standards, London: The Stationery Office.
Crabtree, B. F. and Miller, W. L. (1999) Doing Qualitative Research, Sage, London.
Department of Health (1993) Monitoring and Development: Assessment Special Study, London, Department of Health.
Department of Health (1994) Implementing Caring For People: Care Management, London: Department of Health.
Department of Health (1998) Towards a Self-care Support Strategy, London: Department of Health.
Department of Health (2000a) The NHS Plan: a plan for investment, a plan for reform. London: Department of Health
Department of Health (2000b) Coronary heart disease: National service framework for coronary heart disease - modern standards and service models. London: Department of Health
Department of Health (2001a) National service framework for diabetes: standards. London: Department of Health
Department of Health (2001b) National Service Framework for older people and system reform. London: Department of Health
Department of Health (2002) Fair Access to Care Services Guidance on Eligibility Criteria for Adult Social Care, LAC (2002) 13, London: Department of Health.
Department of Health (2004a) Choosing Health: Making healthy choices easier. London: Department of Health
Department of Health (2004b) Improving Chronic Disease Management. London: Department of Health
Department of Health (2004c) The NHS Improvement Plan: Putting People at the Heart of Public Services, London: Department of Health.
Department of Health (2005a) The National Service Framework for long-term conditions. London: Department of Health

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 207
Department of Health (2005b) Supporting people with long-term conditions: An NHS and social care model to support local innovation and integration. London: Department of Health
Department of Health (2005c) Supporting people with long-term conditions: Liberating the talents of nurses who care for people with long-term conditions. London: Department of Health
Department of Health (2005d) Self-care – A Real Choice Self-care Support – A Practical Option. London: Department of Health
Department of Health (2005e) Self-care support: Baseline study of activity and development in self-care support in PCTs and local areas. London: Department of Health
Department of Health (2006a) Supporting Self Care - A Practical Option: Diagnostic, Monitoring and Assistive Tools, Devices, Technologies and Equipment to Support Self Care, London: Department of Health.
Department of Health (2006b) Supporting People with Long-term Conditions to Self-care: A Guide to Developing Local Strategies and Good Practice, London: Department of Health.
Department of Health (2006c) Practical examples of self-care support. London: Department of Health
Department of Health (2006d) Supporting people with long-term conditions to self-care: A guide to developing local strategies and good practice. London: Department of Health
Department of Health. (2007) Self-care Support summary of work in progress (2005-07). London: Department of Health
Department of Health (2008) Transforming Social Care, LAC (DH) (2008) 1, London: Department of Health.
Department of Health (2008) Ten Things You Need to Know About Long Term Conditions, http://www.dh.gov.uk/en/Healthcare/Longtermconditions/DH_084294 Accessed September 2008
Department of Health (2009) Supporting People with Long Term Conditions: Commissioning Personalised Care Planning, A Guide for Commissioners. London: Department of Health.
Dixon, J. (2007) Critical essay: improving management of chronic illness in the National Health Service: better incentives are the key, Chronic Illness, 3, 3, 181-193
12Dorr, D.A., Wilcox, A., Donnelly, S.M., Burns, L. and Clayton, P.D. (2005) Impact of generalist care managers on patients with diabetes, Health Services Research, 40, 5, 1400-21.
Drennan, V., Goodman, C. and Leyshon, S. (2005) Supporting People with Long Term Conditions: Supporting Experienced Hospital Nurses to Move into Community Matron Roles, London, Department of Health. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4123450

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 208
Effing, T., Monninkhof, E.M., van der Valk, P.D.L.P.M., van der Palen, J., van Herwaarden, C.L.A., Partidge, M.R., Walters, E.H. and Zielhuis, G.A. (2007) Self-management education for patients with chronic obstructive pulmonary disease, Cochrane Database of Systematic Reviews, 4, CD002990.
13Enguidanos, S.M., Gibbs, N.E., Simmons, W.J., Savoni, K.J., Jamison, P.M., Hackstaff, L., Griffin, A.M. and Cherin, D.A. (2003) Kaiser Permanente Community Partners Project: improving geriatric care management practices, Journal of the American Geriatrics Society, 51, 5, 710-14.
Fereday, J. and Muir-Cochrane, E. (2006) Demonstrating rigor using thematic analysis: a hybrid approach of inductive and deductive coding and theme development, International Journal of Qualitative Methods, 5, 1-11.
34Finnerty, J.P., Keeping, I., Bullough, I. and Jones, J. (2001) The effectiveness of outpatient pulmonary rehab in chronic lung disease, a randomized controlled trial, Chest, 119, 1705-1710.
14Fitzgerald, J.F., Smith, D.M., Martin, D.K., Freedman, J.A. and Katz, B.P. (1994) A case manager intervention to reduce readmissions, Archives of Internal Medicine, 154, 15, 1721-9.
Forster, A., Smith, J., Young, J., Knapp, P., House, A. and Wright, J. (2001) Information provision for stroke patients and their caregivers, Cochrane Database of Systematic Reviews, 3, CD001919.
35Freeman, K., Hammond, A. and Lincoln, N.B. (2002) Use of cognitive-behavioural arthritis education programmes in newly diagnosed rheumatoid arthritis, Clinical Rehabilitation, 16, 828.
15aGagnon, A., Schein, C., McVey, L. and Bergman, H. (1999) Randomized controlled trial of nurse case management of frail older people, Journal of the American Geriatrics Society, 47, 9, 1118-24.
Gibson, P.G., Powell, H., Coughlan, J., Wilson, A.J., Hensley, M.J., Abramson, M., Bauman, A. and Walters, E.H. (2002) Limited (information only) patient education programs for adults with asthma, Cochrane Database of Systematic Reviews, 1, CD001005.
Glendinning, C, Challis, DJ, Fernandez, J. L., Jacobs, SR, Jones, K., Knapp, M., Manthorpe, J., Moran, N., Netten, A., Stevens, M, Wilberforce, M. (2008) Evaluation of the Individual Budgets Pilot Programme, Social Policy Research Unit, University of York’ York.
Glasby, J. (2003) Hospital Discharge: Integrating Health and Social Care. Abingdon: Radcliffe Medical Press.
Government News Network (2006) Improving Care for Patients with Chronic Obstructive Pulmonary Disease, http://www.gnn.gov.uk/content/detail.asp?ReleaseID=210625&NewsAreaID=2 7cGravelle, H., Dusheiko, M., Sheaff, R., Sargent, P., Boaden, R., Pickard, S., Parker, S. and
Roland, M. (2006) Impact of case management (Evercare) on outcomes for frail elderly patients:
controlled before and after analysis of quantitative outcome data, British Medical Journal, 15
November 2006, dol: 10.1136/bmj.39020.413310.55 (abridged text, in print: BMJ 2007:334:31-4).

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 209
Griffin, S. and Kinmonth, A.L. (1998) Systems for routine surveillance for people with diabetes mellitus, Cochrane Database of Systematic Reviews, 1, CD000541.
36Griffiths, T., Burr, M., Campbell, I., Lewis-Jenkins, V., Mullins, J., Shiels, K., Turner-Lawlor, P., Payne, N., Newcombe, R. and Lonescu, A. (2000) Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation: a randomised controlled trial, The Lancet, 355, 9301, 362-8.
37Hammond, A. (1999) A cross over trial evaluating an educational behavioural joint protection programme for people with rheumatoid arthritis, Patient Education and Counseling, 37, 19–32.
38Hammond, A. and Freeman, K. (2001) One year outcomes of a randomized controlled trial of an educational behavioural joint protection programme for people with rheumatoid arthritis, Rheumatology, 40, 1044-51.
Hanley, B., Bradburn, J., Gorin, S., Barnes, M., Evans, C., Goodare, H., Kelson, M., Kent, A., Oliver, S. and Wallcraft, J. (2000) Involving Consumers in Research and Development in the NHS: briefing notes for researchers. Hampshire: Consumers in NHS Research Support Unit.
39Helliwell, P.S., O’Hara, M., Holdsworth, J., Hesselden, A., King, T. and Evans, P. (1999) A 12-month randomized controlled trial of patient education on radiographic changes and quality of life in early rheumatoid arthritis, Rheumatology, 38, 303-8.
Heneghan, C.J., Glasziou, P. and Perera, R. (2006) Reminder packaging for improving adherence to self-administered long-term medications, Cochrane Database of Systematic Reviews, 1, CD005025.
Henwood, M. (2004) Reimbursement and Delayed Discharges, Discussion Paper for the Integrated Care Network, Leeds: Integrated Care Network.
40Hill, J., Bird, H. and Johnson, S. (2001) Effect of patient education on adherence to drug treatment for rheumatoid arthritis: a randomised controlled trial, Annals of Rheumatic Diseases, 60, 869-75.
HM Government (2008) Carers at The Heart Of 21st Century Families and Communities: A Caring System On Your Side, A Life Of Your Own, London: Department of Health.
Hudson, M., Victor, C., Fulop, N, and Nazareth, B. (1995) Time to go home: getting to grips with ‘bedblocking’, British Journal of Health Care Management, 1, 8, 402-404.
Hughes, J., Sutcliffe, C. and Challis, D. (2005) Social Work in A. Burns (ed) Standards in Dementia Care, London: Taylor and Francis.
Hutt, R., Rosen, R. and McCauley, J. (2004) Case Managing Long-term Conditions: What Impact Does It Have in the Treatment of Older People? London: Kings Fund.
Isaacs, B. (1981) Is geriatrics a speciality? In T. Arie (ed) Health Care of the Elderly, London: Croon Helm.
Jacobs, S., Hughes, J., Challis, D., Stewart, K. and Weiner, K. (2006) From care management to case management: What can the NHS learn from the social care experience? Journal of Integrated Care, 14, 3, 22-31.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 210
Jolliffe, J.A., Rees, K., Taylor, R.S., Thompson, D., Oldridge, N. and Ebrahim, S. (2000) Exercise-based rehabilitation for coronary heart disease, Cochrane Database of Systematic Reviews, 1, CD001800.
16AKemper, P. (1988) The evaluation of the National Long-term Care Demonstration. 10. Overview of the findings, Health Services Research, 23, 1, 161-74.
Kendig, H.L., Hashimoto, A., and Coppard, L.C., (1992). Family support for the elderly: the international experience. Oxford: Oxford University Press
41Kennedy, A., Reeves, D., Bower, P., Lee, V., Middleton, E., Richardson, G., Gardner, C., Gately, C. and Rogers, A. (2006) The effectiveness and cost effectiveness of a national lay-led self-care support programme for patients with long-term conditions: a pragmatic randomised controlled trial, Journal of Epidemiology and Community Health, 61, 254-61.
Kraan, R., Baldock, J., Davies, B., Evers, A., Johansson, L., Knapen, M., Thorslund, M. and Tunissen, C. (1991) Care for the Elderly: Significant Innovations in Three European Countries, Boulder, Colorado: Campus/Westview.
Krichbaum, K., Aarestad, V. and Buethe, M. (2003) Exploring the connection between self-efficacy and effective diabetes self-management, Diabetes Education, 29, 653–62.
Lacasse, Y., Goldstein, R., Lasserson, T.J. and Martin S. (2006) Pulmonary rehabilitation for chronic obstructive pulmonary disease, Cochrane Database of Systematic Reviews, 4, CD003793.
17bLandi, F., Lattanzio, F., Gambassi, G., Zuccala, G. Sgadari, A., Panfilo, M., Ruffilli, M. and Bernabei, R. (1999) A model for integrated home care of frail older patients: The Silver Network project, Aging Clinical and Experimental Research, 11, 4, 262-72.
17aLandi, F., Onder, G., Russo, A., Tabaccanti, S., Rollo, S., Federici, S., Tua, E., Cesari, M. and Bernabei, R. (2001) A new model of integrated home care for the elderly impact on hospital use, Journal of Clinical Epidemiology, 54, 9, 968 – 970.
18Leung, A.C., Liu, C.P., Chow, N.W. and Chi, I. (2004) Cost-benefit analysis of a case management project for the community-dwelling frail elderly in Hong Kong, Journal of Applied Gerontology, 23, 1, 70-85.
21bLong, M. (2002) Case management model or case manager type? That is the question, Health Care Manager, 20, 4, 53-65.
42Lord, J., Victor, C., Littlejohns, P., Ross, F. M. and Axford, J. S. (1999) Economic evaluation of a primary care-based education programme for patients with osteoarthritis of the knee, Health Technology Assessment 3, 23, 1-55.
Lorig, K., Chastain, R.L., Ung, E., Shoor, S. and Holman, H. (1989) Development and evaluation of a scale to measure perceived self-efficacy in people with arthritis, Arthritis Rheumatology, 30, 1, 37-44.
Loveman, E., Royle, P. and Waugh, N. (2003) Specialist nurses in diabetes mellitus, Cochrane Database of Systematic Reviews 2, CD003286.
20Lynch, J., Forman, S., Graff, S. and Gunby, M. (2000) High-risk population health management. Achieving improved patient outcomes and near-term financial results, American Journal of Managed Care, 6, 7, 781-91.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 211
19Lyon, D., Miller, J. and Pine, K. (2006) The Castlefields integrated care model: the evidence summarised, Journal of Integrated Care, 14, 1, 7-12.
22bMaravilla, V., Graves, M. and Newcomer, R. (2005) Development of a standardized language for case management among high-risk elderly, Lippincotts Case Management, 10, 3–13.
21aMarshall, B., Long, M., Voss, J., Demma, K. and Skerl, K. (1999) Case management of the elderly in a health maintenance organization: The implications for program administration under managed care/practitioner application, Journal of Healthcare Management, 44, 6, 477-91.
Mays, N., Pope, C. and Popay, J. (2005) Systematically reviewing qualitative and quantitative evidence to inform management and policy-making in the health field, Journal of Health Services Research and Policy, 10, S1: 6-20.
Mehta, C. and Patel, N. (1998) Mehta, C. and Patel, N. (1998) StatXact 4, Cytel Software, Cambridge. MA Cambridge. MA.: Cytel Software.
Metcalf, J. (2005) The management of patients with long-term conditions, Nursing Standard, 19, 45, 53-60.
Mountain, G. (2000). Occupational Therapy in Social Services Departments: A Review of the Literature, London: College of Occupational Therapists, Exeter: Centre for Evidence-Based Social Services, University of Exeter.
Murray, E., Burns, J., See Tai, S., Lai, R. and Nazareth, I. (2005) Interactive Health Communication Applications for people with chronic disease, Cochrane Database of Systematic Reviews, 4, CD004274.
22aNewcomer, R., Maravilla, V., Faculjak, P. and Graves, M.T. (2004) Outcomes of preventive case management among high-risk elderly in three medical groups: a randomized clinical trial, Evaluation and the Health Professions, 27, 4, 323-48.
Newman, S., Steed, L. and Mulligan, K. (2004) Self-management interventions for chronic illness, The Lancet 364, 9444, 1523-37.
NHS Modernisation Agency and Skills for Health (2005) Case Management Competencies Framework for the Care of People with Long-term Conditions, London, Department of Health.
Parker, S., Peet, S., McPherson, A., Cannaby, A., Abrahms, K., Baker, R., Wilson, A., Lindesay, J., Parker, G. and Jones, D. (2002) A Systematic Review of Discharge Arrangements for Older People, Health Technology Assessment, 6, 4, York: York Publishing Services.
Philp, I. (2000) EASY-care: A systematic approach to the assessment of older people. Geriatric Medicine, 30, 15-19.
23Pugh, L., Havens, D., Xie, S., Robinson, J. and Blaha, C. (2001) Case management for elderly persons with heart failure: the quality of life and cost outcomes, MedSurg Nursing, 10, 2, 71-8.
Raiff, N. and Shore, B. (1993) Advanced Case Management New Strategies for the Nineties, Sage Human Services Guide 66, London: Sage Publications.
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 212
Rees, K., Taylor, R.S., Singh, S., Coats, A.J.S. and Ebrahim, S. (2004) Exercise based rehabilitation for heart failure, Cochrane Database of Systematic Reviews, 3, CD003331.
Reilly, S., Hughes, J. and Challis, D. (2010) Care management for long term conditions: implementation and processes, Ageing and Society, 30, 125-55.
Reilly, S., Challis, D. and Hughes, J. (2003) Does integration really make a difference?: a comparison of old age psychiatry services in England and Northern Ireland, International Journal of Geriatric Psychiatry, 18, 887-93.
Riegel, B., and Carlson, B. (2002) Facilitators and barriers to heart failure self-care, Patient Education and Counselling, 46, 287-95.
Renders, C.M., Valk, G.D., Griffin, S., Wagner, E.H., van Eijk, J.T.M. and Assendelft, W.J.J. (2000) Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings, Cochrane Database of Systematic Reviews, 4, CD001481.
24Ritchie, C., Wieland, D., Tully, C., Rowe, J., Sims, R. and Bodne, E. (2002) Coordination and advocacy for rural elders (CARE): a model of rural case management with veterans, The Gerontologist, 42, 3, 399-405.
Rockwood, K., Andrew, M., and Mitnitski, A. (2007) A comparison of two approaches to measuring frailty in elderly people. Journal of Gerontology: Biological Sciences and Medical Sciences, 62A, (7),738-743.
43Rogers, H., Atkinson, C., Bond, S., Suddes, M., Dobson, R. and Curless, R. (1999) Randomized controlled trial of a comprehensive stroke education program for patients and caregivers, Stroke, 30, 2585-91.
Roland, M., Dusheiko, M., Gravelle, H. and Parker, S., 2005. Follow up of people aged 65 and over with a history of emergency admissions: analysis of routine admission data. BMJ, 330:289-292
25Ross, F. and Tissier, J. (1997) The care management interface with general practice: a case study, Health and Social Care in the Community, 5, 3, 153-61.
7bSargent, P., Pickard, S., Sheaff, S., and Boaden, R. (2007) Patient and carer perceptions of case management for long-term conditions, Health and Social Care in the Community, 15, 6, 511-9.
15bSchein, C., Gagnon, A.J., Chan, L., Morin, I. and Grondines, J. (2005) The association between specific nurse case management interventions and elder health, Journal of the American Geriatrics Society, 53, 4, 597-602.
26Schore, J., Brown, R. and Cheh, V. (1999) Case management for high-cost Medicare beneficiaries, Health Care Financing Review, 20, 4, 87-101.
27Schraeder, C., Dworak, D., Stoll, J.F., Kucera, C., Waldschmidt, V. and Dworak, M.P. (2005) Managing elders with co-morbidities, Journal of Ambulatory Care Management, 28, 3, 201-9.
44Sharpe, L., Sensky, T., Timberlake, N., Ryan, B., Brewin, C.R. and Allard, S. (2001) A blind, randomized, controlled trial of cognitive-behavioural intervention for patients with recent onset rheumatoid arthritis: preventing psychological and physical morbidity, Pain, 89, 275-83.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 213
45Skinner, T.C., Carey, M. E., Cradock, S., Daly, H., Davies, M. J., Doherty, Y., Heller, S., Khunti, K. and Oliver, L. (2006) Diabetes education and self-management for ongoing and newly diagnosed: process modelling of pilot study, Patient Education and Counselling, 64, 369–77.
46Steed, L., Lankaster, J., Narnard, M., Hurel, S. and Newman, S. (2005) Evaluation of the UCL diabetes self-management programme: a randomized controlled trial, Journal of Health Psychology, 10, 2, 261–76.
Stein, L., Diamond, R., & Factor, R., 1990. A system approach to the care of persons with schizophrenia. In M. I. Herz, S. J. Keith, and J. P. Docherty (Eds.), Schizophrenia: Vol. 5 Psychological Therapies. Amsterdam: Elsevier Science Publishers.
6bStewart, S. and Blue, L. (2001) Key components of specialist nurse-led programmes in chronic heart failure. In: Stewart, S. and Blue, L. (eds) Improving Outcomes in Heart Failure: A Practical Guide to Specialist Nurse Intervention, London, BMJ Books.
Stewart, K., Challis, D., Carpenter, I. and Dickinson, E. (1999) Assessment approaches for older people receiving social care: content and coverage, International Journal of Geriatric Psychiatry, 14, 147-56.
Talbot, F., Nouwen, A., Gingras, J., Gosselin, M. and Audet, J. (1997) The assessment of diabetes-related cognitive and social factors: the multidimensional diabetes questionnaire, Journal of Behavioral Medicine, 20, 291–312.
Thomas, D.E., Elliott E.J. and Naughton, G.A. (2006) Exercise for type 2 diabetes mellitus, Cochrane Database of Systematic Reviews, 3, CD002968.
Thorgrimsen, L., Spector, A., Wiles, A. and Orrell, M. (2003) Aroma therapy for dementia, Cochrane Database of Systematic Reviews, 3, CD003150.
Thorne, S. Paterson, B., Russell, C. and Schultz, A. 2002. Complementary/alternative medicine in chronic illness as informed self-care decision making. Int J Nurs Stud. 39(7):671-83
28Tucker, C. and Brown, L. (1997) Moving Towards the Integration of Health and Social Care. An Evaluation of Different Models for Accessing Community Care Services for Adults and their Carer, Bath, Wiltshire Social Services and Department of Social and Policy Sciences, University of Bath.
Venables, D., Hughes, J., Stewart, K. and Challis, D. (2005) Variations in care management arrangements for people with mental health problems in England, Care Management Journals, 6, 3, 131-138.
47Victor, C.R., Triggs, E., Ross, F., Lord, J. and Axford, J. (2003) Lack of benefit of a primary care-based nurse-led education programme for people with osteoarthritis of the knee, Clinical Rheumatology, 24, 358–64.
Warsi, A., Wang, P.S., LaValley, M.P., Avorn, J. and Solomon, D.H. (2004) Self-management education programs in chronic disease: a systematic review and methodological critique of the literature, Archives of Internal Medicine, 164, 1641-9.
Weiner, K., Challis, D., Darton, R., Hughes, J. and Stewart, K. (1998) Mapping and Evaluation of Care Management Arrangements for Older People and Those with Mental Health Problems Phase I Questionnaires: Overview Questionnaire, Old Age

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 214
Services Questionnaire, Mental Health Questionnaire, Description of the Database, Discussion Paper M008, Personal Social Services Research Unit, University of Manchester, Manchester [not publicly available].
29Weiner, K., Hughes, J., Challis, D. and Pedersen, I. (2003) Integrating health and social care at the micro level: health care professionals as care managers for older people, Social Policy and Administration, 37, 5, 498-515.
Weiner, K., Stewart, K., Hughes, J., Challis, D. and Darton, R. (2002) Care management arrangements for older people in England: key areas of variation, Ageing and Society, 22, 419-39.
Weingarten, S.R., Henning, J.M., Badamgarav, E., Knight, K., Hasselblad, V., and Gano, A. (2002) Interventions used in disease management programmes for patients with chronic illness—which ones work? Meta-analysis of published reports, British Medical Journal, 325, 7370:925.
Wetzels, R., Harmsen, M., Van Weel, C., Grol, R. and Wensing, M. (2007) Interventions for improving older patients' involvement in primary care episodes, Cochrane Database of Systematic Reviews 1, CD004273.
Xie, C., Hughes, J., Challis, D. and Stewart, K. (2008a) Care management arrangements for people with physical and sensory disabilities: results of a national survey, Research Policy and Planning, 26, 2, 87-100.
Xie, C., Hughes, J., Challis, D., Stewart, K. and Cambridge, P. (2008b) Care management arrangements in learning disability services: results of a national study, Journal of Applied Research in Intellectual Disabilities, 21, 156-67.
Yorke, J., Fleming, S.L. and Shuldham, C.M. (2006) Psychological interventions for adults with asthma, Cochrane Database of Systematic Review,s 1, CD002982.
Zaza, S., Wright-DeAguero, L.K., Briss, P. A., Truman, B.I., Hopkins, D.P., Hennessy, M.H., Sosin, D.M., Anderson, L., Carande-Kulis, V.G., Teutsch, S.M. and Pappaioanou, M. (2000) Data collection instrument and procedure for systematic reviews in the guide to community preventive services, American Journal for Preventive Medicine, 18, 44-9.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 215
Appendix 1 References used to identify studies for inclusion in the review of nurse case management studies
Eastwood, A.J. and Sheldon, T.A. (1996) Organisation of asthma care: what difference does it make? A systematic review of the literature, Quality and Safety in Health Care, 5, 3, 134-43.
Hallberg, I.R. and Kristensson, J. (2004) Preventive home care of frail older people: a review of recent case management studies, Journal of Clinical Nursing, 13, S2, 112-20.
Hutt, R., Rosen, R. and McCauley, J. (2004) Case Managing Long-Term Conditions. What Impact Does It Have in the Treatment of Older People? London, Kings Fund.
Johri, M., Beland, F. and Bergman, H. (2003) International experiments in integrated care for the elderly: a synthesis of the evidence, International Journal of Geriatric Psychiatry, 18, 222-35.
Kharicha, K., Levin, E., Iliffe, S. and Davey, B. (2004) Social work, general practice and evidence-based policy in the collaborative care of older people: current problems and future possibilities, Health and Social Care in the Community, 12, 2, 134-41.
Loveman, E., Royle, P., and Waugh, N. (2003) Specialist nurses in diabetes mellitus, Cochrane Database of Systematic Reviews, 2, CD003286.
Norris, S.L., Nichols, P.J., Caspersen, C.J., Glasgow, R.E., Engelgau, M.M., Jack, J., Isham, G., Snyder, S.R. and Carande-Kulis, V.G. (2002) The effectiveness of disease and case management for people with diabetes: A systematic review, American Journal of Preventive Medicine, 22, 4, S1, 15-38.
Phelan, E., Cheadle, A., Schwartz, S., Snyder, S., Williams, B., Wagner, E. and LoGerfo, J. (2003) Promoting Health and Preventing Disability in Older Adults: Lessons from Intervention Studies Carried Out Through an Academic-Community Partnership, Family and Community Health, 26, 3, 214-20.
Raine, R., Haines, A., Sensky, T., Hutchings, A., Larkin, K. and Black, N. (2002) Systematic review of mental health interventions for patients with common somatic symptoms: can research evidence from secondary care be extrapolated to primary care? British Medical Journal, 325, 7372, 1082.
Renders, C.M., Valk, G.D., Griffin, S., Wagner, E.H., van Eijk, J.T.H.M. and Assendelft, W.J.J. (2001) Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings, Cochrane Database of Systematic Reviews, 1, CD001481.
Richards, S. and Coast, J. (2003) Interventions to improve access to health and social care after discharge from hospital: a systematic review, Journal of Health Services Research Policy, 8, 3, 171-9.
Rosen, A. and Teesson, M. (2001) Does case management work? The evidence and the abuse of evidence-based medicine, Australian and New Zealand Journal of Psychiatry, 35, 6, 731-46.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 216
Rummery, K. and Glendinning, C. (2000) Primary Care and Social Services: Developing New Partnerships for Older People, Abingdon, Radcliffe Medical Press.
Singh, D. (2005) Which Staff Improve Care for People With Long-Term Conditions? A Rapid Review of the Literature, NHS Modernisation Agency and The University of Birmingham Health Sevice Management Centre.
Taylor, S., Bestall, J., Cotter, S., Falshaw, M., Hood, S., Parsons, S., Wood, L. and Underwood, M. (2005) Clinical service organisation for heart failure, Cochrane Database of Systematic Reviews, 2, CD002752.
van Haastregt, J.C.M., Diederiks, J.P.M., van Rossum, E., de Witte, L.P. and Crebolder, H.F.J.M. (2000) Effects of preventive home visits to elderly people living in the community: systematic review, British Medical Journal, 320, 7237, 754-8.
Weingarten, S.R., Henning, J.M., Badamgarav, E., Knight, K., Hasselblad, V., Gano, A., Jr. and Ofman, J.J. (2002) Interventions used in disease management programmes for patients with chronic illness - which ones work? Meta-analysis of published reports, British Medical Journal, 325, 7370, 925.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 217
Appendix 2 Nurse case management studies data extraction tool
Study details
Country
Number of sites
Patient/diagnostic group
Design
Unit of analysis
Number of participants
Characteristics
Method of identification
Method of patient selection (based onHutt et al., 2004 review)
Eligibility criteria
Programme elements measured Structures
Processes
Outcomes
Costs
Setting Routine mainstream
Demonstration/research
Focus of research
Type of organisation
Case management Intervention
General description/focus of activity
Programme/intervention aim
Initiated in:
Professional group(s)
Range of case management tasks Case finding/screening
Assessment
Care planning
Implementation/management
Monitoring
Review
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 218
Case closure
Liaison/coordination with outside service
Liaison/coordination with MDT
Managing care network
Description of self care
Inclusion of self-care related components: Self-management education
Provider education
Medication management
Psychological support (client)
Family support
Counselling/therapy
Carer education
Patient reminders
Structured self-care training (groups or individual)
Use of technology/equipment to support self-care
Inclusion of other components: Home visits
Telephone calls
Legal/benefits/financial help
Other

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 219
Appendix 3 References used to identify studies for inclusion in the review of uk self-care support studies
Birks, J. and Grimley Evans, J. (2007) Ginkgo biloba for cognitive impairment and dementia, Cochrane Database of Systematic Reviews, 2, CD003120.
*Bosch-Capblanch, X., Abba, K., Prictor, M. and Garner, P. (2007) Contracts between patients and healthcare practitioners for improving patients' adherence to treatment, prevention and health promotion activities, Cochrane Database of Systematic Reviews, 2, CD004808.
Casimiro, L., Barnsley, L., Brosseau, L., Milne, S., Robinson, V.A., Tugwell, P. and Wells, G. (2005) Acupuncture and electroacupuncture for the treatment of rheumatoid arthritis, Cochrane Database of Systematic Reviews, 3, CD003788.
Currell, R., Urquhart, C., Wainwright, P. and Lewis, R. (2000) Telemedicine versus face to face patient care: effects on professional practice and health care outcomes, Cochrane Database of Systematic Reviews, 2, CD002098.
*Deakin, T., McShane, C.E., Cade, J.E., and Williams, R. (2005) Group based training for self-management strategies in people with type 2 diabetes mellitus, Cochrane Database of Systematic Reviews, 2, CD003417.
*Forster, A., Smith, J., Young, J., Knapp, P., House, A. and Wright, J. (2001) Information provision for stroke patients and their caregivers. Cochrane Database of Systematic Reviews, 3, CD001919.
*Gibson, P.G., Powell, H., Coughlan, J., Wilson, A.J., Abramson, M., Haywood, P., Bauman, A., Hensley, M.J. and Walters, E.H. (2002) Self-management education and regular practitioner review for adults with asthma, Cochrane Database of Systematic Reviews, 1,CD001117.
*Gillespie, L.D., Gillespie, W.J., Robertson, M.C., Lamb, S.E., Cumming, R.G. and Rowe, B.H. (2003) Interventions for preventing falls in elderly people, Cochrane Database of Systematic Reviews, 3,CD000340.
Griffin, S. and Kinmonth, A.L. (1997) Systems for routine surveillance for people with diabetes mellitus, Cochrane Database of Systematic Reviews, 2, CD000541.
Han, A., Judd, M.G., Robinson, V.A., Taixiang, W., Tugwell, P. and Wells, G. (2004) Tai chi for treating rheumatoid arthritis, Cochrane Database of Systematic Reviews,3, CD004849.
Haynes, R.B., Yao, X., Degani, A., Kripalani, S., Garg, A. and McDonald, H.P. (2007) Interventions for enhancing medication adherence, Cochrane Database of Systematic Reviews, 1, CD000011.
Heneghan, C.J., Glasziou, P. and Perera, R. (2006) Reminder packaging for improving adherence to self-administered long-term medications, Cochrane Database of Systematic Reviews, 1, CD005025.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 220
*Jolliffe, J.A., Rees, K., Taylor, R.S., Thompson, D., Oldridge, N. and Ebrahim, S. (2000) Exercise-based rehabilitation for coronary heart disease, Cochrane Database of Systematic Reviews, 4, CD001800.
*Lacasse, Y., Goldstein, R., Lasserson, T.J. and Martin, S. (2006) Pulmonary rehabilitation for chronic obstructive pulmonary disease, Cochrane Database of Systematic Reviews, 3, CD003793.
Lewin, S.A., Dick, J., Pond, P., Zwarenstein, M., Aja, G., van Wyk, B, Bosch-Capblanch, X. and Patrick, M. (2004) Lay health workers in primary and community health care, Cochrane Database of Systematic Reviews, 1, CD004015.
Little, C.V., Parsons, T. and Logan, S. (2000) Herbal therapy for treating osteoarthritis, Cochrane Database of Systematic Reviews, 1, CD002947.
Little, C.V. and Parsons, T. (200b) Herbal therapy for treating rheumatoid arthritis, Cochrane Database of Systematic Reviews,1, CD002948.
Lim, B., Manheimer, E., Lao, L., Ziea, E., Wisniewski, J., Liu, J. and Berman, B. (2006) Acupuncture for treatment of irritable bowel syndrome, Cochrane Database of Systematic Reviews, 4, CD005111.
Liu, J.P., Zhang, M., Wang, W.Y. and Grimsgaard, S. (2004) Chinese herbal medicines for type 2 diabetes mellitus, Cochrane Database of Systematic Reviews,3, CD003642.
Liu, J.P., Yang, M., Liu, Y.X. Wei, M.L. and Grimsgaard, S. (2006) Herbal medicines for treatment of irritable bowel syndrome, Cochrane Database of Systematic Reviews,1, CD004116.
Mccarney, R., Warner, J., Fisher, P. and Van Haselen, R. (2002) Homeopathy for dementia. Cochrane Database of Systematic Reviews, 1, CD003803.
McCarney, R.W., Linde, K. and Lasserson, T.J. (2003) Homeopathy for chronic asthma, Cochrane Database of Systematic Reviews, 3, CD000353.
*McKinstry, B., Ashcroft, R.E., Car, J., Freeman, G.K. and Sheikh, A. (2006) Interventions for improving patients' trust in doctors and groups of doctors, Cochrane Database of Systematic Reviews, 3, CD004134.
*Mistiaen, P. and Poot, E. (2006) Telephone follow-up, initiated by a hospital-based health professional, for post discharge problems in patients discharged from hospital to home, Cochrane Database of Systematic Reviews, 4, CD004510.
*Monninkhof, E.M., van der Valk, PP.D.L.P.M., van der Palen, J., van Herwaarden, C.L.A., Partidge, M.R., Walters, E.H. and Zielhuis, G.A. (2002) Self-management education for chronic obstructive pulmonary disease, Cochrane Database of Systematic Reviews, 3, CD002990.
Moore, H. Summerbell, C., Hooper, L., Cruickshank, K., Vyas, A., Johnstone, P., Ashton, V. and Kopelman, P. (2004) Dietary advice for treatment of type 2 diabetes mellitus in adults, Cochrane Database of Systematic Reviews, CD004097.
Murray, E., Burns, J., See Tai, S., Lai, R. and Nazareth, I. (2005) Interactive Health Communication Applications for people with chronic disease, Cochrane Database of Systematic Reviews, CD004274.

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 221
Peng, W.N., Zhao, H., Liu, Z.S. and Wang, S. (2007) Acupuncture for vascular dementia, Cochrane Database of Systematic Reviews, CD004987.
*Powell, H. and Gibson, P.G. (2002) Options for self-management education for adults with asthma, Cochrane Database of Systematic Reviews, CD004107.
*Ramaratnam, S., Baker, G.A. and Goldstein, L.H. (2005) Psychological treatments for epilepsy, Cochrane Database of Systematic Reviews, CD002029.
*Rees, K., Taylor, R.S., Singh, S., Coats, A.J.S. and Ebrahim, S. (2004) Exercise based rehabilitation for heart failure, Cochrane Database of Systematic Reviews, CD003331.
*Renders, C.M., Valk, G.D., Griffin, S., Wagner, E.H., van Eijk, J.T.M. and Assendelft, W.J.J. (2000) Interventions to improve the management of diabetes mellitus in primary care, outpatient and community settings, Cochrane Database of Systematic Reviews, CD001481.
*Riemsma, R.P., Kirwan, J.R., Taal, E. and Rasker, J.J. (2003) Patient education for adults with rheumatoid arthritis, Cochrane Database of Systematic Reviews, CD003688.
*Shaw, E.J., Stokes, T., Camosso-Stefinovic, J., Baker, R., Baker, G.A. and Jacoby, A. (2007) Self-management education for adults with epilepsy, Cochrane Database of Systematic Reviews, CD004723.
*Thomas, D.E., Elliott, E.J. and Naughton, G.A. (2006) Exercise for type 2 diabetes mellitus, Cochrane Database of Systematic Reviews, CD002968.
Thorgrimsen, L., Spector, A., Wiles, A. and Orrell, M. (2003) Aroma therapy for dementia, Cochrane Database of Systematic Reviews, CD003150.
Toelle, B.G. and Ramm, F.S.F. (2003) Written individualised management plans for asthma in children and adults, Cochrane Database of Systematic Reviews, CD002171.
Turnock, A.C., Walters, E.H., Walters, J.A.E. and Wood-Baker, R. (2005) Action plans for chronic obstructive pulmonary disease, Cochrane Database of Systematic Reviews, CD005074.
*Vermeire, E., Wens, J., Van Royen, P., Biot, Y., Hearnshaw, H. and Lindenmeyer, A. (2005) Interventions for improving adherence to treatment recommendations in people with type 2 diabetes mellitus, Cochrane Database of Systematic Reviews, CD003638.
Viggo Hansen, N., Jørgensen, T. and Ørtenblad, L. (2006) Massage and touch for dementia, Cochrane Database of Systematic Reviews, CD004989.
*Welschen, L.M.C., Bloemendal, E., Nijpels, G., Dekker, J.M., Heine, R.J., Stalman, W.A.B. and Bouter, L.M. (2005) Self-monitoring of blood glucose in patients with type 2 diabetes mellitus who are not using insulin, Cochrane Database of Systematic Reviews, CD005060.
Wetzels, R., Harmsen, M., Van Weel, C., Grol, R. and Wensing, M. (2006) Interventions for improving older patients' involvement in primary care episodes, Cochrane Database of Systematic Reviews, CD004273.
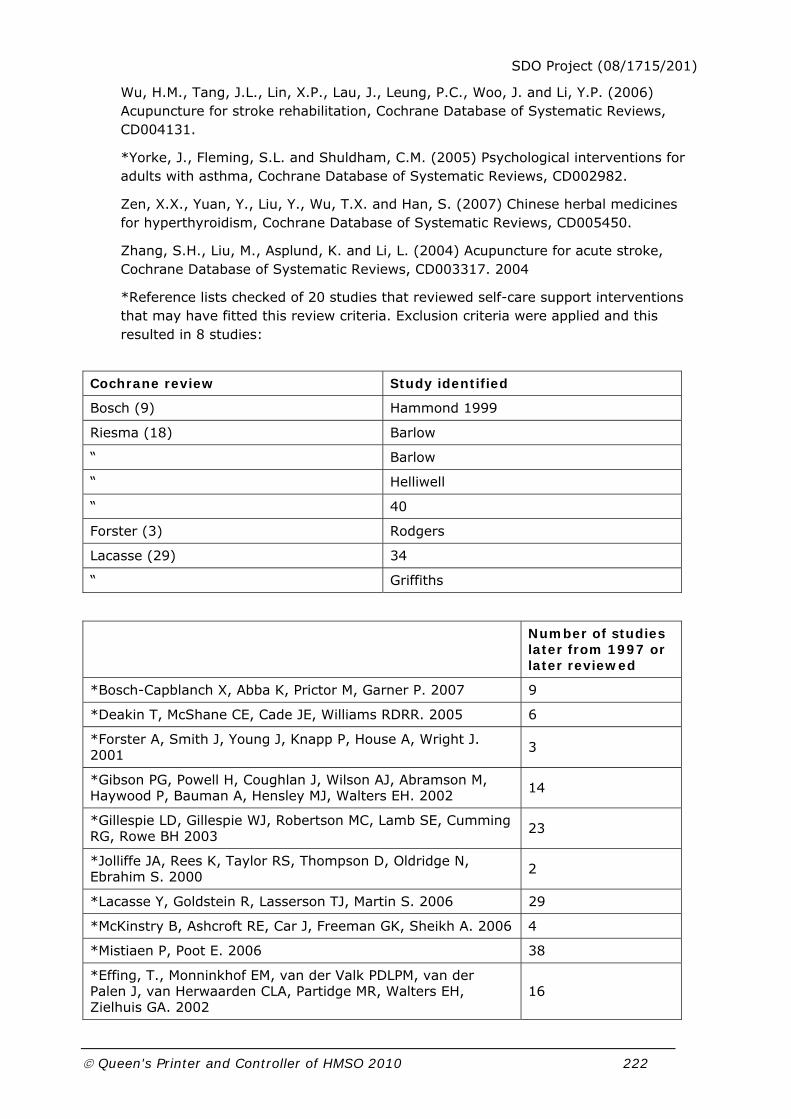
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 222
Wu, H.M., Tang, J.L., Lin, X.P., Lau, J., Leung, P.C., Woo, J. and Li, Y.P. (2006) Acupuncture for stroke rehabilitation, Cochrane Database of Systematic Reviews, CD004131.
*Yorke, J., Fleming, S.L. and Shuldham, C.M. (2005) Psychological interventions for adults with asthma, Cochrane Database of Systematic Reviews, CD002982.
Zen, X.X., Yuan, Y., Liu, Y., Wu, T.X. and Han, S. (2007) Chinese herbal medicines for hyperthyroidism, Cochrane Database of Systematic Reviews, CD005450.
Zhang, S.H., Liu, M., Asplund, K. and Li, L. (2004) Acupuncture for acute stroke, Cochrane Database of Systematic Reviews, CD003317. 2004
*Reference lists checked of 20 studies that reviewed self-care support interventions that may have fitted this review criteria. Exclusion criteria were applied and this resulted in 8 studies:
Cochrane review Study identified
Bosch (9) Hammond 1999
Riesma (18) Barlow
“ Barlow
“ Helliwell
“ 40
Forster (3) Rodgers
Lacasse (29) 34
“ Griffiths
Number of studies
later from 1997 or later reviewed
*Bosch-Capblanch X, Abba K, Prictor M, Garner P. 2007 9
*Deakin T, McShane CE, Cade JE, Williams RDRR. 2005 6
*Forster A, Smith J, Young J, Knapp P, House A, Wright J. 2001 3
*Gibson PG, Powell H, Coughlan J, Wilson AJ, Abramson M, Haywood P, Bauman A, Hensley MJ, Walters EH. 2002 14
*Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH 2003 23
*Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. 2000 2
*Lacasse Y, Goldstein R, Lasserson TJ, Martin S. 2006 29
*McKinstry B, Ashcroft RE, Car J, Freeman GK, Sheikh A. 2006 4
*Mistiaen P, Poot E. 2006 38
*Effing, T., Monninkhof EM, van der Valk PDLPM, van der Palen J, van Herwaarden CLA, Partidge MR, Walters EH, Zielhuis GA. 2002
16

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 223
*Powell H, Gibson PG. 2002 9
*Ramaratnam S, Baker GA, Goldstein LH. 2005 3
*Rees K, Taylor RS, Singh S, Coats AJS, Ebrahim S. 2004 18
*Renders CM, Valk GD, Griffin S, Wagner EH, van Eijk JThM, Assendelft WJJ. 2000 14
*Riemsma RP, Kirwan JR, Taal E, Rasker JJ. 2003 18
*Shaw EJ, Stokes T, Camosso-Stefinovic J, Baker R, Baker GA, Jacoby A. 2007 1
*Thomas DE, Elliott EJ, Naughton GA. 2006 10
*Vermeire E, Wens J, Van Royen P, Biot Y, Hearnshaw H, Lindenmeyer A. 2005 12
*Welschen LMC, Bloemendal E, Nijpels G, Dekker JM, Heine RJ, Stalman WAB, Bouter LM. 2005 3
*Yorke J, Fleming SL, Shuldham CM. 2005 8
References identified through reviews
Article Number of studies referenced
Barlow et al., 2002 145
Chodosh et al., 2006 53
Newman et al., 2004 78
Warsi et al., 2004 71
Weingarten et al.,2002 102
Total 449

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 224
Appendix 4 UK self-care support studies data extraction tool Study details
Title
Source
Design: Randomised
Controlled
Double blind
Target condition
Mean age
Aim of the intervention
Outcome measures
Delivery: Where it was delivered
Who delivered
Follow up period
Methodology quality score
Components of self-care support: Patient education
Exercise promotion
Pain management
Medication adherence
Psychological support
Dietary advice
Carers education
Delivery of patient education: Self-care support groups
Individual self-care support
Written materials
Outcome measures with direction of effect: Physical functioning
Illness knowledge
Exercise and diet
Pain
Treatment adherence
Depression and anxiety
Self efficacy

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 225
Quality of life
Health service usage

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 226
Appendix 5 Survey of case management for people with long-term conditions and self-care services
Questionnaire (50 questions)
Shortened version of the questionnaire used in telephone interviews (21 questions are marked with an asterisk)
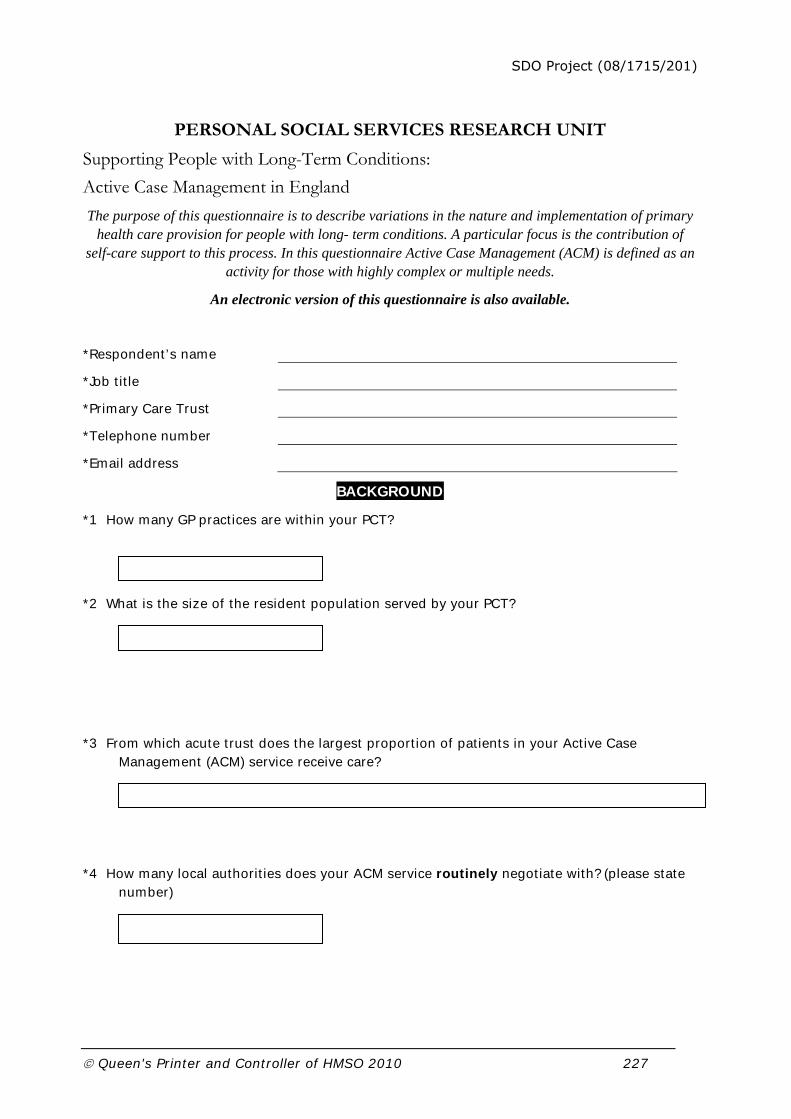
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 227
PERSONAL SOCIAL SERVICES RESEARCH UNIT
Supporting People with Long-Term Conditions:
Active Case Management in England
The purpose of this questionnaire is to describe variations in the nature and implementation of primary health care provision for people with long- term conditions. A particular focus is the contribution of
self-care support to this process. In this questionnaire Active Case Management (ACM) is defined as an activity for those with highly complex or multiple needs.
An electronic version of this questionnaire is also available.
*Respondent’s name
*Job title
*Primary Care Trust
*Telephone number
*Email address
BACKGROUND
*1 How many GP practices are within your PCT?
*2 What is the size of the resident population served by your PCT?
*3 From which acute trust does the largest proportion of patients in your Active Case Management (ACM) service receive care?
*4 How many local authorities does your ACM service routinely negotiate with? (please state number)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 228
*5 Is your current ACM service(s) based on a previous initiative(s)?
Yes No
If yes, please describe
*6 On what date was the first patient accepted into the ACM service?
Month Year
ORGANI
ON D DEVELOPMENT
CASE MANAGEMENT OBJECTIVES
7 Which of these statements describe the goals of your ACM service for people with long-term conditions? TICK ALL THAT APPLY
To provide more intensive long-term support in the community
To improve the extent and scope of services
To improve the coordination of care to people living in the community
To improve the quality of life of people with long-term conditions
To divert people away from inappropriate hospitalisation
To arrange more speedy and effective hospital discharge
To reduce hospital length of stay
To assist in the rehabilitation of people with long- term conditions
To achieve improved accountability
To divert people from inappropriate residential and nursing home care
To increase the independence of people with long-term conditions
To improve the health of people with long-term conditions
To promote self-care support for people with long-term conditions
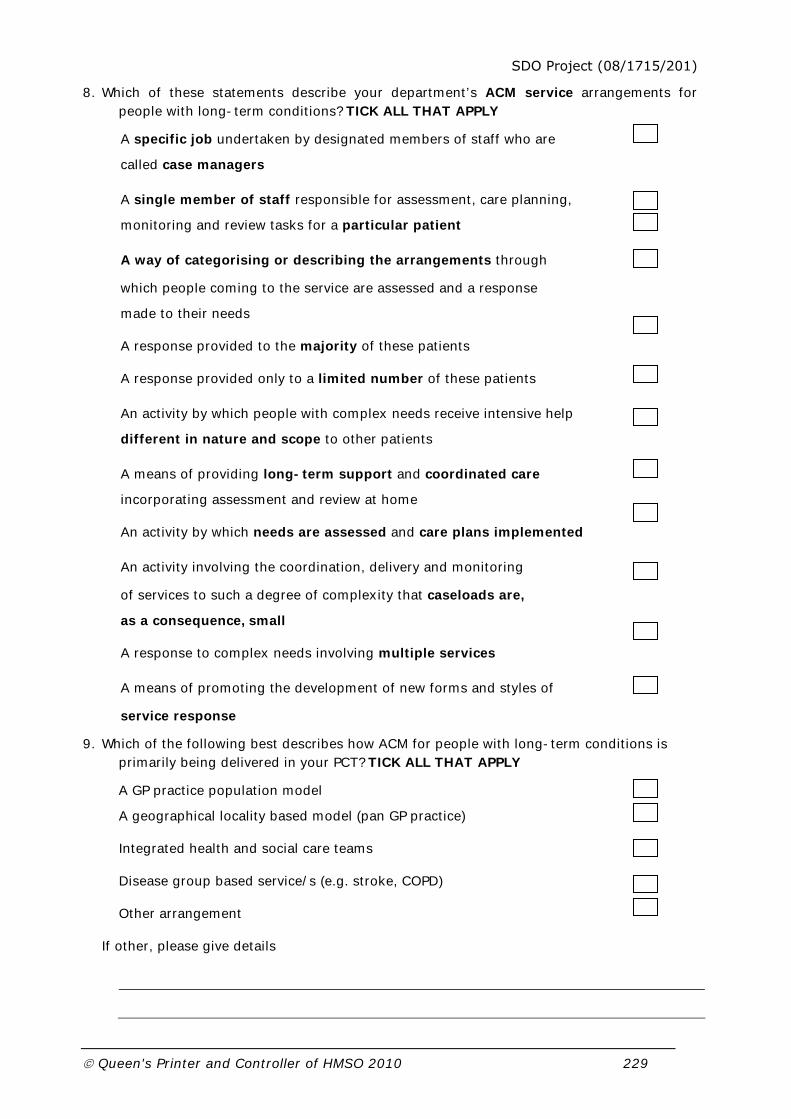
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 229
8. Which of these statements describe your department’s ACM service arrangements for people with long-term conditions? TICK ALL THAT APPLY
A specific job undertaken by designated members of staff who are
called case managers
A single member of staff responsible for assessment, care planning,
monitoring and review tasks for a particular patient
A way of categorising or describing the arrangements through
which people coming to the service are assessed and a response
made to their needs
A response provided to the majority of these patients
A response provided only to a limited number of these patients
An activity by which people with complex needs receive intensive help
different in nature and scope to other patients
A means of providing long-term support and coordinated care
incorporating assessment and review at home
An activity by which needs are assessed and care plans implemented
An activity involving the coordination, delivery and monitoring
of services to such a degree of complexity that caseloads are,
as a consequence, small
A response to complex needs involving multiple services
A means of promoting the development of new forms and styles of
service response
9. Which of the following best describes how ACM for people with long-term conditions is primarily being delivered in your PCT? TICK ALL THAT APPLY
A GP practice population model
A geographical locality based model (pan GP practice)
Integrated health and social care teams
Disease group based service/s (e.g. stroke, COPD)
Other arrangement
If other, please give details

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 230
LINKS WITH OTHER SERVICES
*10a. Does your PCT have agreements in place with local authority social care services for people with long-term conditions?
Yes No
10b. If yes, is there an agreement with social care services partners over:
TICK ALL THAT APPLY
Yes No Under discussion
Respective target populations for ACM and care management in social care
Eligibility criteria for ACM
Assessment tools for entry into ACM
How active case managers access social care service resources
Other, please specify

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 231
*11. Please indicate with which of the following services your ACM service has developed a formal agreement. TICK ALL THAT APPLY
Yes No Under discussion
Acute/Foundation trusts
Accident and emergency
Cardiology
General medicine
Geriatric medicine
Hospital pharmacy
Old age psychiatry
Specialist disease nursing e.g. COPD, epilepsy
*Intermediate care services
Schemes to prevent hospital admission e.g. hospital at home schemes
Schemes to facilitate early discharge from hospital
Ambulance trust
Emergency hospital admissions
*Primary care services
Community nursing services
Community pharmacy services
Community physiotherapy services
Other, please specify
12a. Do you have any dedicated specialist physician sessions to support ACM?
Yes No

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 232
12b. If yes, please describe in terms of specialty and number of programmed activities per week.
13a. Does your ACM service have any links with an End of Life Care Programme initiative in your area?
Yes No
13b. If yes, please specify
14a. Are there specific arrangements for ACM patients with an emergency outside of normal working hours?
Yes, specific arrangements
No, standard primary care arrangements
14b. If yes, please describe
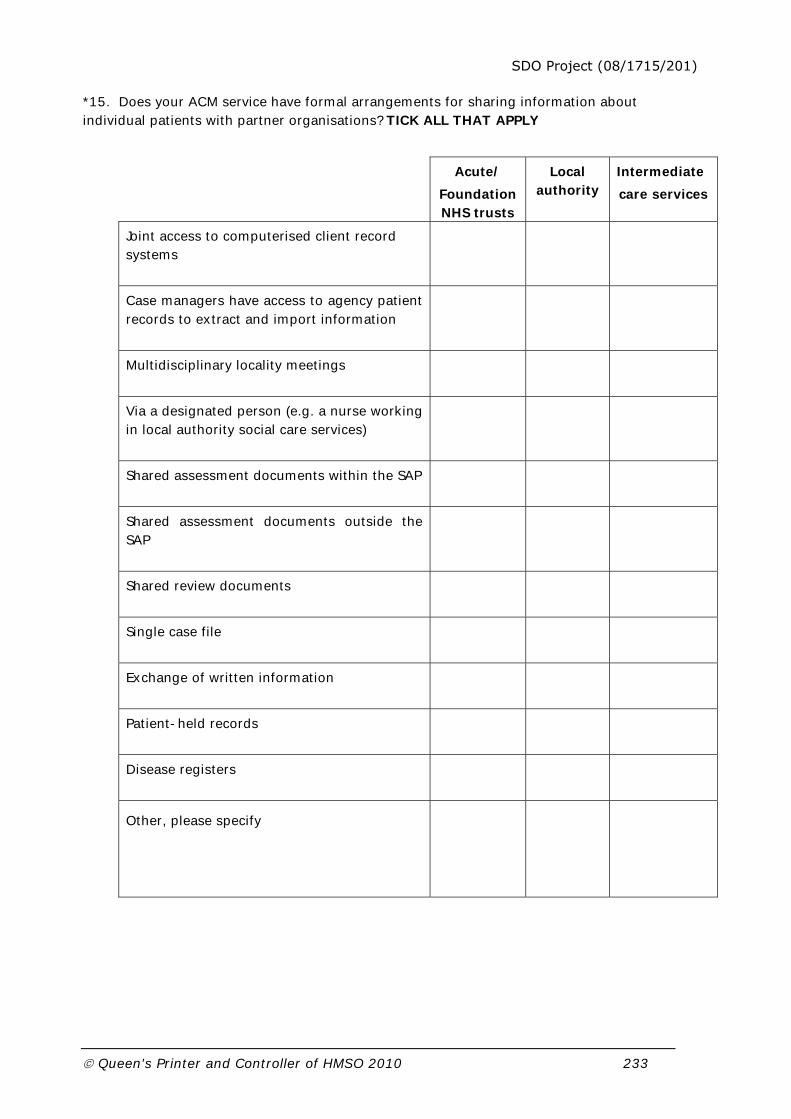
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 233
*15. Does your ACM service have formal arrangements for sharing information about individual patients with partner organisations? TICK ALL THAT APPLY
Acute/
Foundation NHS trusts
Local authority
Intermediate
care services
Joint access to computerised client record systems
Case managers have access to agency patient records to extract and import information
Multidisciplinary locality meetings
Via a designated person (e.g. a nurse working in local authority social care services)
Shared assessment documents within the SAP
Shared assessment documents outside the SAP
Shared review documents
Single case file
Exchange of written information
Patient-held records
Disease registers
Other, please specify

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 234
SELF-CARE SUPPORT SERVICES
*16. Does your PCT have a designated lead for self-care support services?
Yes No
*17. Have you, as ACM lead, been involved in the development of the commissioning strategy for self-care support services in your PCT?
Yes No
*18a. Does your ACM service have any formal links with voluntary organisations specifically designed to support self-care for patients with long-term conditions?
Yes No
18b. If yes, please specify
*19. Please tell us whether your PCT funds or provides any of the following self-care support services and estimate their frequency of use by case managed patients? PLEASE COMPLETE EACH ROW
Available? Frequency of use by case managed patients
Self-care support service
Yes No Frequently Sometimes Never
Informal therapeutic intervention e.g. during contact with professional
Accessible advice and information e.g. patient information booklets
Technology and equipment to promote self-care e.g. home monitoring equipment
Self-care support training (generic) e.g. Expert Patient Programme

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 235
Self-care support training (condition-specific) e.g. diabetes
Self -help groups e.g. arthritis support group
Alternative therapies e.g. acupuncture
Other, please specify
*20. Following on from your previous answer, please indicate where self-care support services are currently operating in your PCT/locality for patients in receipt of ACM in each disease category
PLEASE TICK ALL THAT APPLY FOR EACH DISEASE CATEGORY (ROW)
Self-care support service Disease category
Informal
therapeutic
intervention
Accessible
advice and
information
Technology
and
equipment
to promote
self-care
Self-care
support
training
(generic)
Self-care
support
training
(condition-
specific)
Self -
help
groups
Alternative
therapies
Asthma
Chronic
obstructive
pulmonary
Diabetes
Hypertension
Coronary
heart disease
Stroke and
transient
ischaemic
Musculo-
skeletal
Multiple
conditions
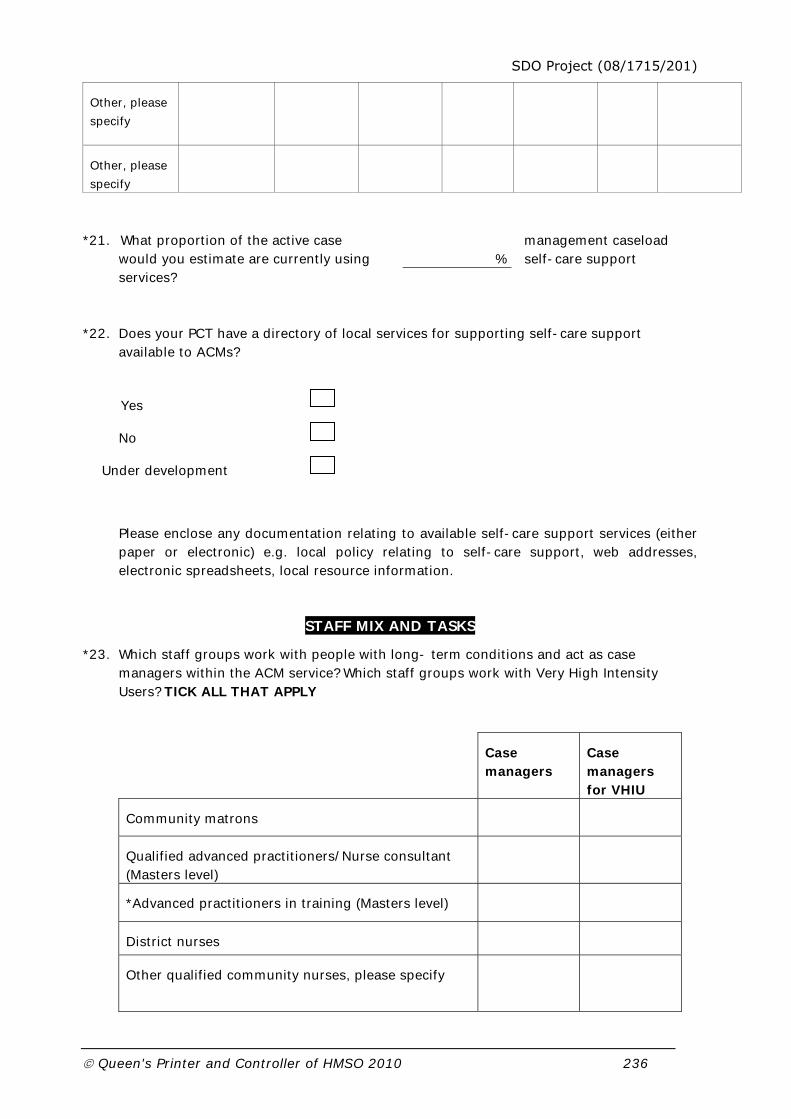
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 236
Other, please
specify
Other, please
specify
*21. What proportion of the active case management caseload would you estimate are currently using self-care support services?
*22. Does your PCT have a directory of local services for supporting self-care support available to ACMs?
Yes
No
Under development
Please enclose any documentation relating to available self-care support services (either paper or electronic) e.g. local policy relating to self-care support, web addresses, electronic spreadsheets, local resource information.
STAFF MIX AND TASKS
*23. Which staff groups work with people with long- term conditions and act as case managers within the ACM service? Which staff groups work with Very High Intensity Users? TICK ALL THAT APPLY
Case managers
Case managers for VHIU
Community matrons
Qualified advanced practitioners/Nurse consultant (Masters level)
*Advanced practitioners in training (Masters level)
District nurses
Other qualified community nurses, please specify
%

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 237
Qualified occupational therapists
Qualified physiotherapists
*Qualified social workers
Case manager assistants/support workers/assistant practitioners
Other, please specify
Other, please specify
24. Where are case managers/case manager assistants for people with long-term conditions, or those undertaking the equivalent role, based? TICK ALL THAT APPLY
(For staff working at more than one site, please tick their primary location.)
GP practices
Health and social care integrated team
Nurse team in primary health care
Health and social care integrated old age team
Health and social care integrated old age mental health team
Hospital
Local authority social care services team
Other, please specify
25. Which organisation provides the manager for case managers? TICK ALL THAT APPLY
Health services only
Jointly managed, with health services holding the major* responsibility
Jointly managed, with social care services holding the major* responsibility
Local authority social care only
Other, please specify

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 238
* By ‘major’ we mean responsibility for the day-to-day operation of the service including issues such as the allocation of referrals.
26a. Do you have a programme of training for your ACM service for the year ending March 2008?
Yes No
26b. If yes, what are the current priorities for this training programme?
27a. Does your ACM service initiate or participate in any staff training initiatives specific to self-care or self-care support?
Yes No
27b. If yes, please describe
OCF ACTIVE CASE MANAGEM

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 239
*28. Do case managers undertake the following tasks? TICK ONE BOX FOR EACH TASK
Usually Sometimes Never
Assessment of health care needs
Assessment of social care needs
Assessment for entry into self-care support services
*Financial assessment
*Care planning
*Arranging/allocating services
*Implementation of care plan
*Case budget management/budget holding
*Monitoring the implementation of the care plan
*Reviews
Hands on care
Clinical oversight
Patient advocacy
Provision of emotional/therapeutic support
Prescribing/medications review
Provide patient information and education
Refer patient to self-care support services
Contribute to the provision of self-care support services
Contribute to the development of self-care support programmes
PROCESS OF ACTIVE CASE MANAGEMENT
PATIENT IDENTIFICATION
29a. Does the ACM service have locally agreed written referral/eligibility criteria?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 240
Yes No
If yes, please include a copy when you return the completed questionnaire.
29b. If yes, what do they include? TICK ALL THAT APPLY
Age
Number of hospital admissions
Disease
Recognised tool e.g. Castlefields tool
Other, please specify
30a. Is ACM in your PCT targeted at specific diseases or conditions?
Yes No
30b. If yes, which long-term condition groups (the list below incorporates Quality and Outcomes Framework categories)? TICK ALL THAT APPLY
Asthma Chronic Obstructive Pulmonary DiseaseDiabetes Hypertension Cancer Coronary Heart Disease Stroke and Transient Ischaemic Attack (TIA)Epilepsy Other neurological conditions Hypothyroidism Mental health Multiple conditions Musculoskeletal conditions Other, please specify
30c. Of these, which, if any, are the priority groups in your PCT? Please specify

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 241
31a. What are the main methods adopted for identifying high risk patients within your service? please indicate all main methods that apply to your service.
Patient at Risk of Re-hospitalisation I (PARR I)
Patient at Risk of Re-hospitalisation II (PARR II)
Combined predictive model
High-impact user manager (Dr Foster)
Castlefields tool
Single Assessment Process (SAP) documentation
Referrals from other professionals
Hand searching patient records
Disease registries
Other, please specify
31b. Of these, which, is the most effective in your PCT? Please specify
ASSESSMENT
32. In your area, are assessments made under the SAP accepted as part of the assessment information for active case management?
Yes No
33. Which assessment tools are in use by case managers? TICK ALL THAT APPLY
Easycare
MDS
FACE

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 242
Locally approved Single Assessment Process (SAP) tool
Disease-specific (please specify)
Other, please specify
34a. Can ACM service staff undertake assessments for provision of local authority funded social care services?
Yes No
34b. If yes, for which services, please specify
CARE PLANNING
35. For ACM patients, do care plans routinely detail the contribution made by the following: PLEASE TICK ONE BOX PER LINE
Usually
Sometimes Never
ACM/Primary care services
Acute Foundation Trust services
Intermediate care services
Social care services
36a. Can case managers authorise the use of any local authority resources for patients?
Yes No

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 243
36b. If yes, which resources? TICK ALL THAT APPLY
Domiciliary care Day care
Respite care Other
If other, please specify
*37. How are cases of different levels of need/complexity/risk allocated in your ACM service?
TICK ALL THAT APPLY
Level of staff qualification
Length of contact
Intensity of involvement
Time limited, short term intensive involvement e.g. 13 weeks
Allocation as staff available
38. Does your ACM service have a written policy to allocate cases of different levels of need/complexity/risk to different levels of case management (e.g. low risk patients may be visited monthly and high risk patients may be visited weekly)?
Yes No
MONITORING AND REVIEW
*39. Please estimate a case manager’s average active caseload size?
40.How often does the same practitioner within the ACM service remain responsible for assessment, case management, monitoring and review within a single patient episode? PLEASE TICK ONE BOX PER LINE
Usually Sometimes Never
For cases closed within 3 months
For cases open after 3 months for longer term monitoring/review
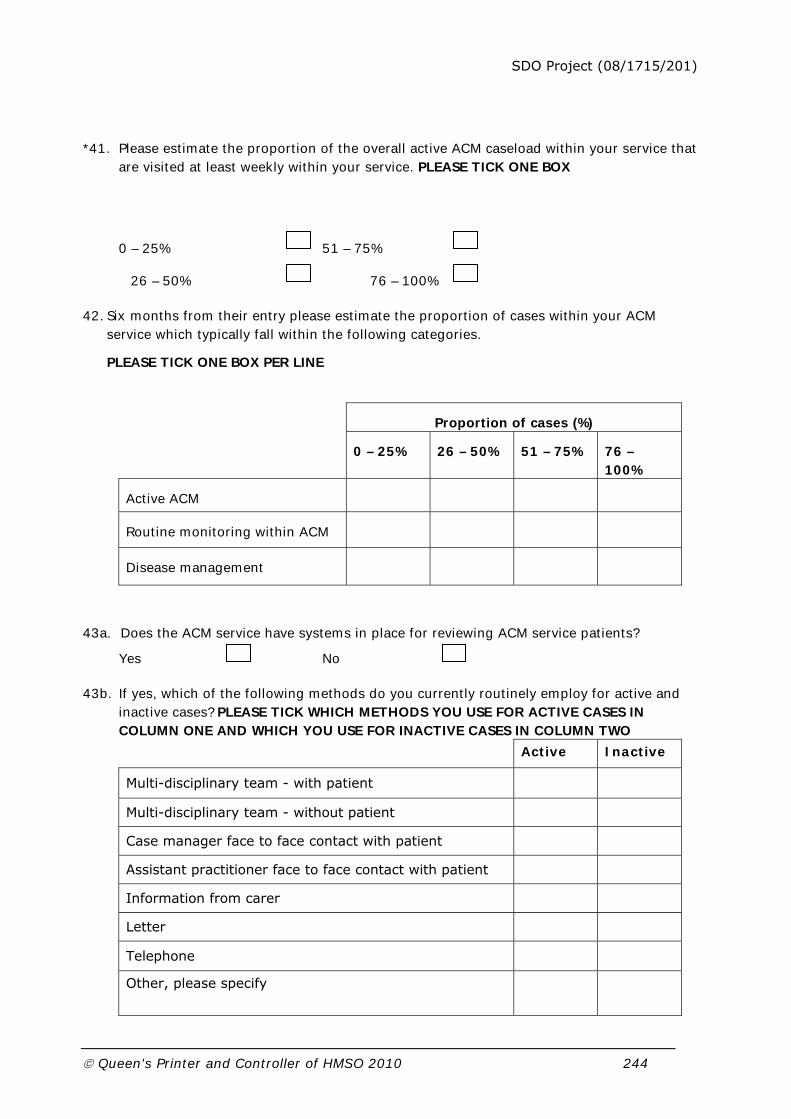
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 244
*41. Please estimate the proportion of the overall active ACM caseload within your service that are visited at least weekly within your service. PLEASE TICK ONE BOX
0 – 25% 51 – 75%
26 – 50% 76 – 100%
42. Six months from their entry please estimate the proportion of cases within your ACM service which typically fall within the following categories.
PLEASE TICK ONE BOX PER LINE
Proportion of cases (%)
0 – 25%
26 – 50% 51 – 75% 76 – 100%
Active ACM
Routine monitoring within ACM
Disease management
43a. Does the ACM service have systems in place for reviewing ACM service patients?
Yes No
43b. If yes, which of the following methods do you currently routinely employ for active and inactive cases? PLEASE TICK WHICH METHODS YOU USE FOR ACTIVE CASES IN COLUMN ONE AND WHICH YOU USE FOR INACTIVE CASES IN COLUMN TWO
Active Inactive
Multi-disciplinary team - with patient
Multi-disciplinary team - without patient
Case manager face to face contact with patient
Assistant practitioner face to face contact with patient
Information from carer
Letter
Telephone
Other, please specify

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 245
44. What are the three most common reasons for case closure in your ACM service?
TICK THE THREE MOST FREQUENT REASONS
Moved to disease-specific services
Moved to social care services
Moved to self-care support
Moved to long-term care home
Moved to community nursing
Moved to informal care
Patient refusing service
Leaving locality
No discernable benefit from ACM service
Death
Other, please specify
INFORMATION SYSTEMS
45a. Does your PCT have a computerised client record system for assessment and case management for ACM patients?
Yes No
45b. If yes, is it TICK ALL THAT APPLY
Linked to other record systems within primary care (e.g. Lorenzo)
ACM service specific
Other
If other, please describe
46. Which of these statements describe ACM information systems in your PCT? TICK ALL THAT APPLY

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 246
ACMs can electronically access all information on ACM patients within the PCT
ACM patients can be identified on hospital record systems
The ACM service has a specific computerised client record system
None of the above
47. What information about individual patients is held in the electronic information system relating to the ACM service? TICK ALL THAT APPLY
Personal details
Ethnic origin
Medical information
Diagnoses
SAP Assessments:
Specialist assessments
Overview assessment
Care plans:
ACM input
Social care services
Other NHS services
Voluntary organisation services
Self-care support services
Reviews
Other, please specify
SERVICE DEVELOPMENT
48. Has there been a formal evaluation of your ACM service?
Yes No
If yes, please enclose the report or summary of findings
49. What is the relevance of self-care to your ACM service?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 247
50. What are the key issues in developing your ACM service?
Please also use the space below to add any further comments to expand upon any issues of relevance covered or not covered in the questionnaire
Please remember to include the relevant documents relating to:
Documentation relating to available self-care support
services (either paper or electronic) e.g. local policy relating to self
care support, web addresses, electronic spreadsheets, local resource
information. (Q22)
Written eligibility criteria for ACM (Q29a)
Evaluation of your ACM service (Q50)
Thank you for your assistance in completing this form
Please return the questionnaire in the SAE by 16/11/2007 to:
Personal Social Services Research Unit
Dover Street Building
The University of Manchester
Oxford Road
Manchester, M139PL
Any queries telephone 0161 275 5681 or email [email protected]

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 248
Appendix 6 Service manager interview questions Core interview questions were asked to all case study sites. Where appropriate site specific questions were also asked and these are marked by the number of the site/s directed to.
1. BACKGROUND
Core
How long has the case management lead been in post?
Are there case management teams?
How are these teams defined?
How many teams are there?
Site specific
Was the previous initiative this service was based on a pilot of Community Matrons? (1)
Caseloads seem small in this service, does this conflict with it being a service provided to the majority? (2)
Is the 24 hour rapid response team only for case managed patients? (2)
2. LINKS WITH OTHER AGENCIES
Local authority
Core
Are there future plans for increased integration with the local authority?
Are there informal networks and links with the local authority?
Wider health services
Core
What are links like between the service and GPs?
Are there informal links with wider health services?
Site specific
There seems to be formal agreements in place with [specify health service/s here] could you discuss? (2, 4)
How have the discussion sessions between the case management service and the community geriatrician gone? (3)
Please describe your arrangements for sharing information with the acute trust through a designated person. (4).
3. SELF-CARE SUPPORT SERVICES

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 249
Core
Do case managers provide self-care support or do they refer on to other agencies?
Are there any self-care support services in your PCT targeted at older people?
Site specific
Are many referrals made to local self-care support services? (1, 2, 4)
Do case managers assess self-care support needs and refer patient on to these services? (1, 3, 4)
How do case managed patients find self-care groups and what is their experience of them? (2, 3, 4)
What kind of technology is available to support self-care of different conditions? (2, 3, 4)
Do case managers promote supported self-care with their patients? (1, 4)
How did links develop so that case managers contribute to self-care support services?
(2, 4)
What links are there with voluntary organisations that provide self-care? (3, 4)
How did the informal links with these voluntary organisations develop? (3, 4)
Since you have no self-care lead, what motivated you to develop formal links with Age Concern? (2)
Would a directory of local self-care support services be useful? (2)
What do the voluntary organisations you have informal links with offer? (3)
Do case managers themselves provide much self-care support through technology? (3)
Who (if not the case management lead) has developed the self-care support services? (4)
Could you estimate the percentage of case managed patients actually using self-care support services? (4)
4. STAFF MIX AND TASKS
Core
Does the amount of hands-on care vary depending on the professional background of the case manager or the needs of the patient?
Site specific
Is there any plan to develop self-care specific training? (1, 2, 3)
Do case managers undertake medication review? Or is this limited to certain staff depending on qualification? (1, 2, 4)
Which staff group(s) usually manages VHIU patients? (3)
Is the training provided by the heart failure support group for patients or staff? (3)
What does staff training to support self-care include? E.g. delivering patient education? (4)
Can staff share skills such as providing hands-on care? (4)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 250
5. PROCESS OF ACTIVE CASE MANAGEMENT
5.1 Patient Identification
Core
Does the case management service receive referrals from patients where disease based services/self-care has failed?
Are there many inappropriate referrals when using this method (insert main method of patient identification used by PCT)?
Site specific
Why is the method(s) of identification you use better than other systems? (2, 3)
Is there a waiting list for entrance into the service? (2, 3)
Is this a problem that PARR is not currently in use? (1)
5.2 Assessment
Core
What does the assessment contain?
Is it multi disciplinary?
5.3 Care planning
Core
Do care plans contain self-care support information?
Are these (review or case closure procedures) initiated by the case management service?
Are cases prioritised?
Site specific
Are patients passed between case managers if their needs change? How does this happen? (1, 3, 4)
Does allocating different levels of need to different staff mean the Advanced Practitioners caseload looks a lot different from the Assistant CM? (1, 3)
Does an average nurse caseload look different to a social work one or an Advanced Practitioner caseload from a physiotherapist one? (2, 3)
How are cases allocated (and is this with/without a written policy)? (2, 4)
Can experience and skills about case allocation be shared? (2)
5.4 Monitoring and review
Core
Is n the number of active cases?
How is an active case defined?
Are case load sizes as predicted?
Are there enough case managers to manage the case over its duration?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 251
How long is the average duration of a case?
Site specific
How many patients will still be receiving case management after six months? (1)
How is an inactive case defined? (1, 3, 4)
Which other services are people discharged to after case closure, for example disease management? (1)
Who in the multidisciplinary team who reviews inactive cases? For example is it staff from the health service or are staff from the local authority/voluntary organisations also involved? (4)
After case closure can people be fast tracked back into the case management service? (4)
What exactly is involved if a patient is discharged to self-care support? (4)
Death of a patient isn’t mentioned as a common reason for case closure for your PCT. What proportion of patients stay in the case management service for the rest of their life? (4)
6. INFORMATION SYSTEMS
Site specific
Should there be a computerised PCT client record system specific to the case management service? (2, 4)
What information is held on your computerised PCT client record system? (3)
How are decisions made about the patient communicated to other agencies, particularly the LA, who may be involved? (4)

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 252
Appendix 7 Service manager topic guidelines 1. SERVICE CHARACTERISTICS
Caseload size
Team structure and staff mix
Out of hours
Location
Continuity of care
Target group
2. SERVICE PROCESS
Methods of targeting
Care co-ordination (including devolved budgets)
Direct care
Case closure
3. LINKS WITH OTHER AGENCIES
Primary care
Acute care
Local authorities
Other
4. PROVISION OF SELF-CARE
Self-care support provided by case managers
Self-care support provided by others
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 253
Appendix 8 Focus group topic guidelines 1. SERVICE CHARACTERISTICS
Caseload size
Team structure and staff mix
Location
Out of hours
Continuity of care
Target group
2. SERVICE PROCESS
Targeting
Methods of targeting
Caseload manageability
Case allocation
Frequency of visiting
Movement within service and case closure
Frequency and initiation of reviews
Tasks
Day to day tasks
Clinical role
Coordination
Budget holding
3. LINKS WITH OTHER AGENCIES
Shared assessment
Authorisation of local authority services
Links with other agencies (local authority, GPs, wider health services)
Information sharing across agencies
Formal and informal networks
Links with voluntary organisation
4. PROVISION OF SELF-CARE
Is awareness of self-care increasing?
Is the Expert Patient Programme appropriate for case managed patients?
Is there training for case managers in self-care support?
What kinds of self-care support do case managers provide – patient and carer education?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 254
How is self-care support accessed?
Do case managers refer people on to other services?
Do case managers assess for self-care support?
What links are there with voluntary organisations for self-care support?
Are there age appropriate services?
What are patients’ attitudes towards self-care?
Is technology used to support self-care?
Are patients ever discharged to self-care from the case management service?

SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 255
Appendix 9 Service user consultation questions For completion by service users in the consultation groups these questions were presented in large
font and in an A3 booklet.
1. Do you have any long standing health problem, disability or infirmity? (Please circle the one that causes you the most problems)
Chest & breathing problems/Diabetes/High blood pressure/Heart problems/Stroke/Arthritis or rheumatism/Other_______________/Other________________/
2. Which three things you think would be most useful in helping you manage this condition?
A note of explanation:
Being able to talk to someone: Being able to talk to someone (e.g. a nurse) about the condition.
Information leaflets: Information leaflets that clearly explained how best to deal with the condition.
Special equipment: Special equipment to help with the condition e.g. a machine that would take your blood pressure every day, send it down the phone line or by using a computer and allow your nurse to monitor you from a distance.
A course for people with all types of long term conditions: Going to a course for people with all types of long term conditions that would give you advice on how to look after yourself, how to improve your energy, how to get the information you need from doctors and how to deal with worry about your condition.
Being able
to talk to
someone
Information
leaflets
Special
equipment
A course for
people with
all types of
long term
conditions
A course for
people with the
same condition
An informal
self help
group
Alternative
therapies
SDO Project (08/1715/201)
Queen's Printer and Controller of HMSO 2010 256
A course for people with the same condition: Going to a course for people with the same condition as you. Being told some of the ways to cope with the condition, e.g. if you have diabetes how to make sure your blood sugar stays level.
An informal self help group: Going to a more informal group for people with your condition, the purpose is to give information e.g. there may be speakers arranged to give advice and information but there is also a more social element of getting to know other people over the longer term.
Alternative therapies: Being able to access alternative therapies such as massage, aromatherapy, acupuncture and homeopathy to see if these can help your condition.
In this context case management can be described as,
‘An integrated process involving the identification of needs arising from long term health problems or infirmity, the creation of a plan to meet them and the coordination of health and care services specified in the plan over time, adjusting them in response to changed circumstances’.
3. What do you think should be the most important aim of case management for people with long-term conditions?
Please choose one of the following four options:
To promote self care support for people with long-term condition:
by this we mean giving you advice to help you to manage your condition.
To improve the coordination to care to people living at home:
by this we mean the provision of the right kind of help by the most appropriate person at the right
time.
To provide more intensive long-term support to people living at home:
by this we mean more help than would normally be available from the community nursing services
and social services.
To improve the range of health and social care services available to support people at home:
by this we extra support to avoid unnecessary admission to hospital and facilitate early discharge.

Disclaimer: This report presents independent research commissioned by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the NIHR SDO programme or the Department of Health. The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the NIHR SDO programme or the Department of Health” Addendum: This document is an output from a research project that was commissioned by the Service Delivery and Organisation (SDO) programme whilst it was managed by the National Coordinating Centre for the Service Delivery and Organisation (NCCSDO) at the London School of Hygiene & Tropical Medicine. The NIHR SDO programme is now managed by the National Institute for Health Research Evaluations, Trials and Studies Coordinating Centre (NETSCC) based at the University of Southampton. Although NETSCC, SDO has managed the project and conducted the editorial review of this document, we had no involvement in the commissioning, and therefore may not be able to comment on the background of this document. Should you have any queries please contact [email protected].