self reported health after...
TRANSCRIPT
BackgroundIt has during the recent years become increasingly evident that assessments of neurological function and disability are not suffi-cient to evaluate the whole impact of stroke on patients.In order to assess post-stroke prognosis it is therefore necessary to add measures of self-rated health in areas that do not only fo-cus on stroke-related deficits or impairments as well as possess knowledge of the progress of these over time.
aimTo describe the course of self-reported mental – and physical health in a population of first-time stroke patients and analyse whether gender, age, education level, diagnose, stroke severity and comorbidity at time of admission affected the health course.
methodsA cohort of patients admitted with first time stroke in the Central Denmark Region (CDR) (n=2195) in the period 1.oct. 2008 – 31. dec 2011 was followed over a 2 year period with registers and 5 repetitive questionnaires.The course of self-reported health was described using SF-12, Physical Component Summary (PCS) and Mental Component Summary (MCS).Data was analysed in longitudinal regression models after the use of multiple imputation.
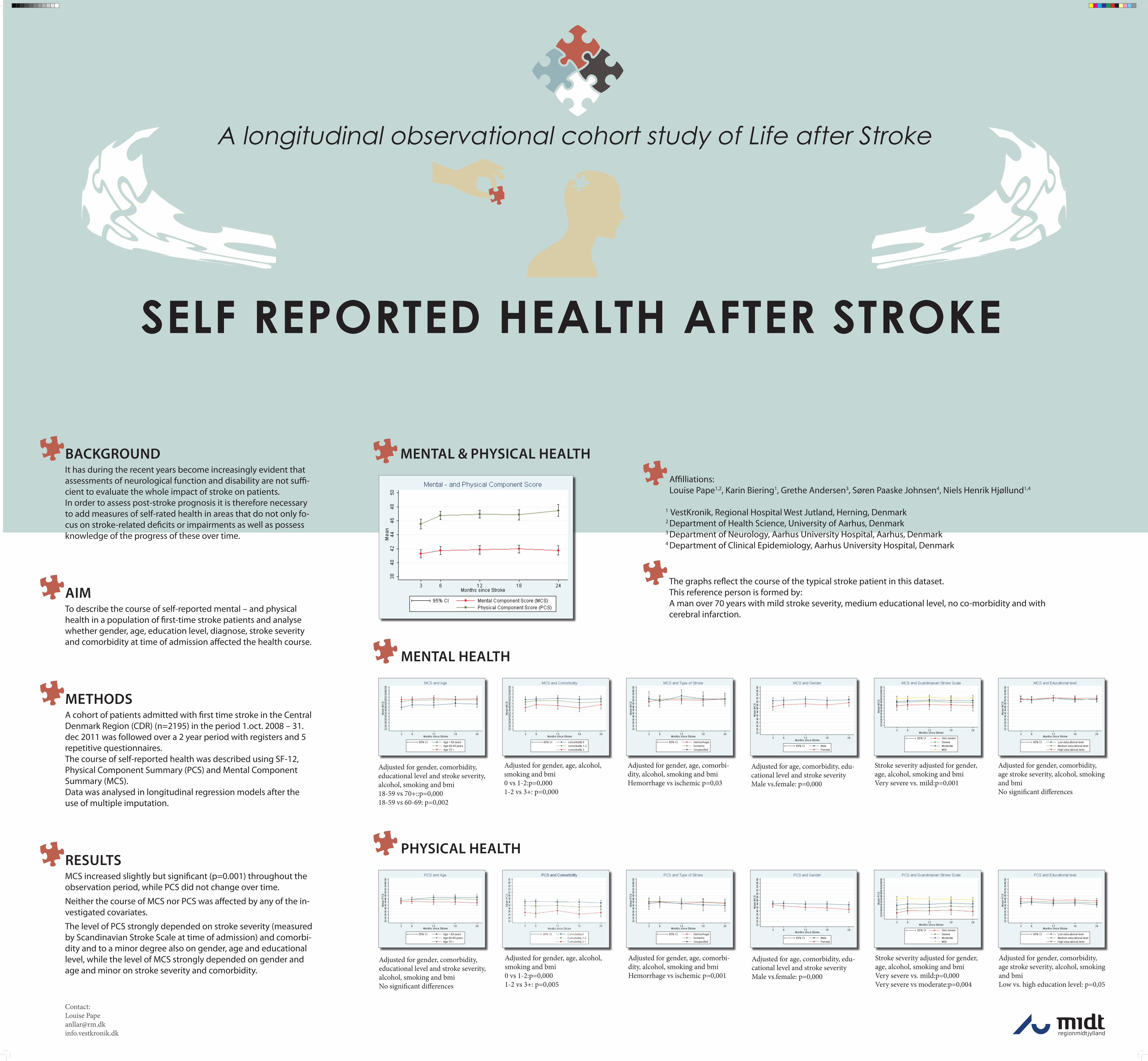
resultsMCS increased slightly but significant (p=0.001) throughout the observation period, while PCS did not change over time.
Neither the course of MCS nor PCS was affected by any of the in-vestigated covariates.
The level of PCS strongly depended on stroke severity (measured by Scandinavian Stroke Scale at time of admission) and comorbi-dity and to a minor degree also on gender, age and educational level, while the level of MCS strongly depended on gender and age and minor on stroke severity and comorbidity.
The graphs reflect the course of the typical stroke patient in this dataset.This reference person is formed by:A man over 70 years with mild stroke severity, medium educational level, no co-morbidity and with cerebral infarction.
A longitudinal observational cohort study of Life after Stroke
Self reported health after Stroke
mental health
mental & physical health
physical health
Adjusted for gender, comorbidity, educational level and stroke severity, alcohol, smoking and bmi18-59 vs 70+::p=0,00018-59 vs 60-69: p=0,002
Adjusted for gender, comorbidity, educational level and stroke severity, alcohol, smoking and bmiNo significant differences
Adjusted for gender, age, alcohol, smoking and bmi0 vs 1-2:p=0,0001-2 vs 3+: p=0,000
Adjusted for gender, age, alcohol, smoking and bmi0 vs 1-2:p=0,0001-2 vs 3+: p=0,005
Adjusted for gender, age, comorbi-dity, alcohol, smoking and bmiHemorrhage vs ischemic p=0,03
Adjusted for gender, age, comorbi-dity, alcohol, smoking and bmiHemorrhage vs ischemic p=0,001
Adjusted for age, comorbidity, edu-cational level and stroke severityMale vs.female: p=0,000
Adjusted for age, comorbidity, edu-cational level and stroke severityMale vs.female: p=0,000
Stroke severity adjusted for gender, age, alcohol, smoking and bmiVery severe vs. mild:p=0,001
Stroke severity adjusted for gender, age, alcohol, smoking and bmiVery severe vs. mild:p=0,000Very severe vs moderate:p=0,004
Adjusted for gender, comorbidity, age stroke severity, alcohol, smoking and bmiNo significant differences
Adjusted for gender, comorbidity, age stroke severity, alcohol, smoking and bmiLow vs. high education level: p=0,05
Affilliations: Louise Pape1,2, Karin Biering1, Grethe Andersen3, Søren Paaske Johnsen4, Niels Henrik Hjøllund1,4
1 VestKronik, Regional Hospital West Jutland, Herning, Denmark 2 Department of Health Science, University of Aarhus, Denmark 3 Department of Neurology, Aarhus University Hospital, Aarhus, Denmark 4 Department of Clinical Epidemiology, Aarhus University Hospital, Denmark
Contact:Louise [email protected]