seronegative spondyloarthropathies m.valešová. spectrum ankylosing spondylitis psoriatic arthritis...
TRANSCRIPT
Seronegative Spondyloarthropathies
M.Valešová
Spectrum
• Ankylosing spondylitis
• Psoriatic arthritis
• Reactive arthritis
• Enteropathic arthritis
• Undifferentiated spondyloarthritis
• Juvenile AS
Ankylosing spondylitis(AS)
Demography AS
• Prevalence AS 0.05-0.23%, 3-4X male
• UHCW catchment area – 375-1700 AS pts
Burden of AS
• SMR 1.5
• 10% less labour participation
• 15% constraints at work
• Poor quality of life cf worse than RA
Aetiology• AS has been closely associated with the expression of the HLA-B27 gene
• The response to the therapeutic blockade of TNFalpha indicates that this cytokine plays a central role in AS
• Examination of inflamed SI joints in AS patients has demonstrated high levels of CD4+ and CD8+ T cells and macrophages.
• The overlapping features with reactive arthritis and IBD (SpAs) suggests a possible role for intestinal bacteria in the pathogenesis of AS.

• Features AS?

Physical signs and diagnosis
Diagnostic criteria – Modified New York criteria
• Radiologic criteria : sacroiliitis - grade 2 bilaterally or grade 3-4 unilaterally
• Clinical criteria : LBP and stiffness > 3 months improved with exercise and not relieved by rest, limitation of L/spine motion in frontal and sagittal planes, limitation of chest expansion relative to normal values correlated with age and sex
• Diagnosis : radiologic criteria and at least one clinical
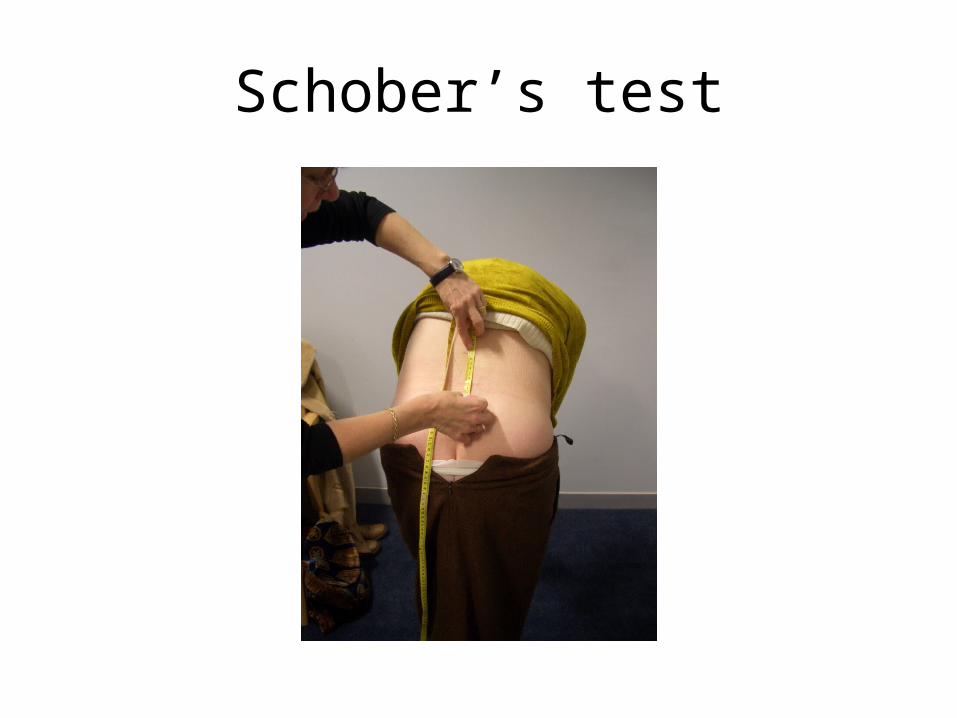
Schober’s test
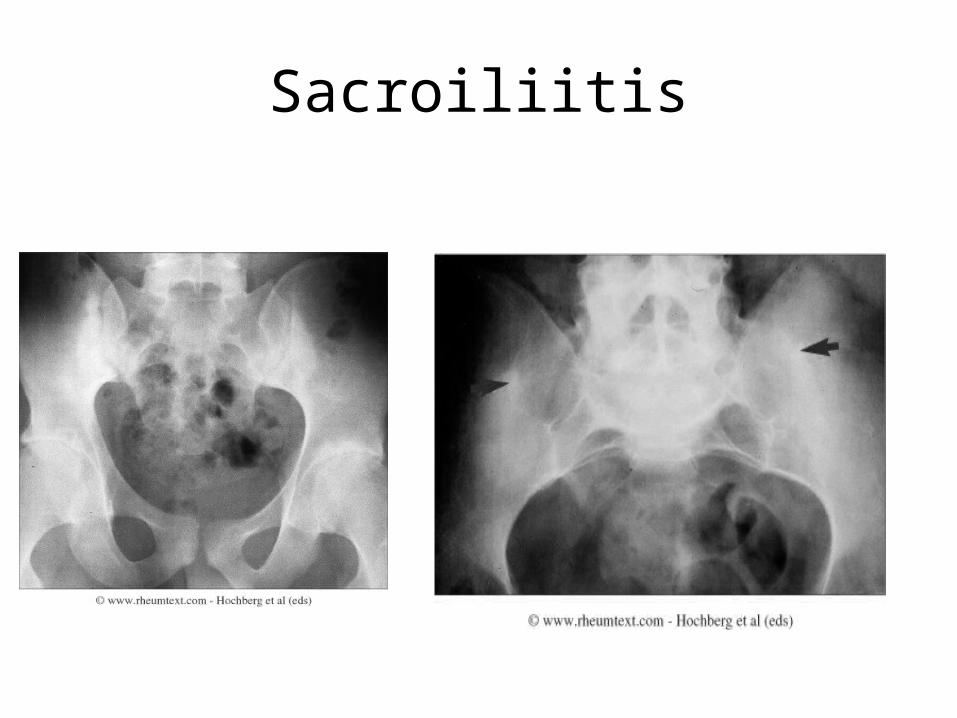
Sacroiliitis

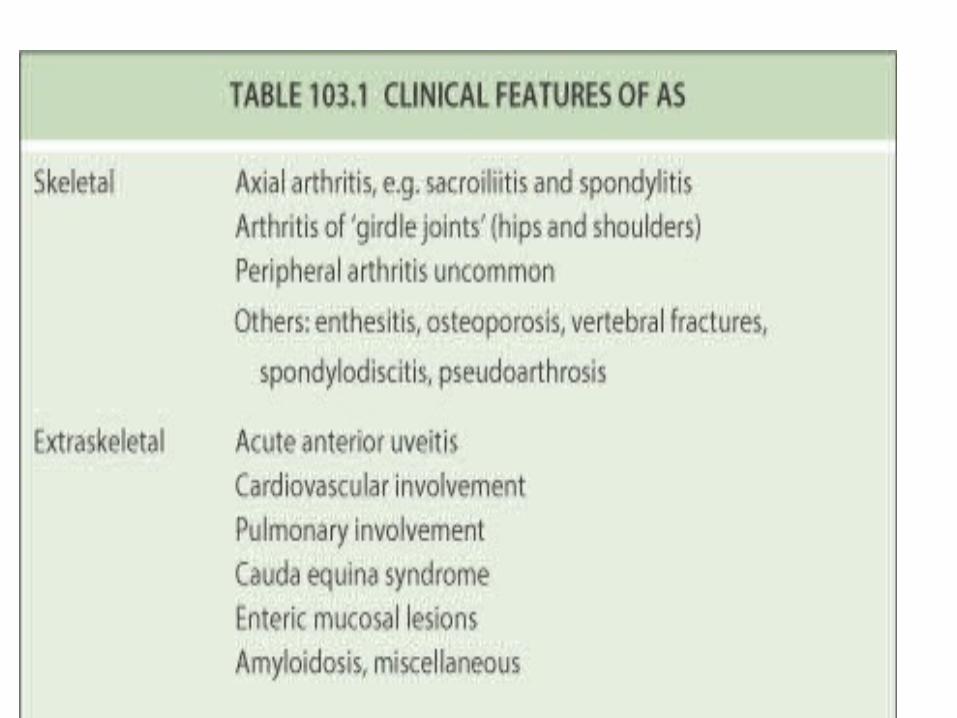
AS Clinical Features - axial
• Early AS
Romanus lesion
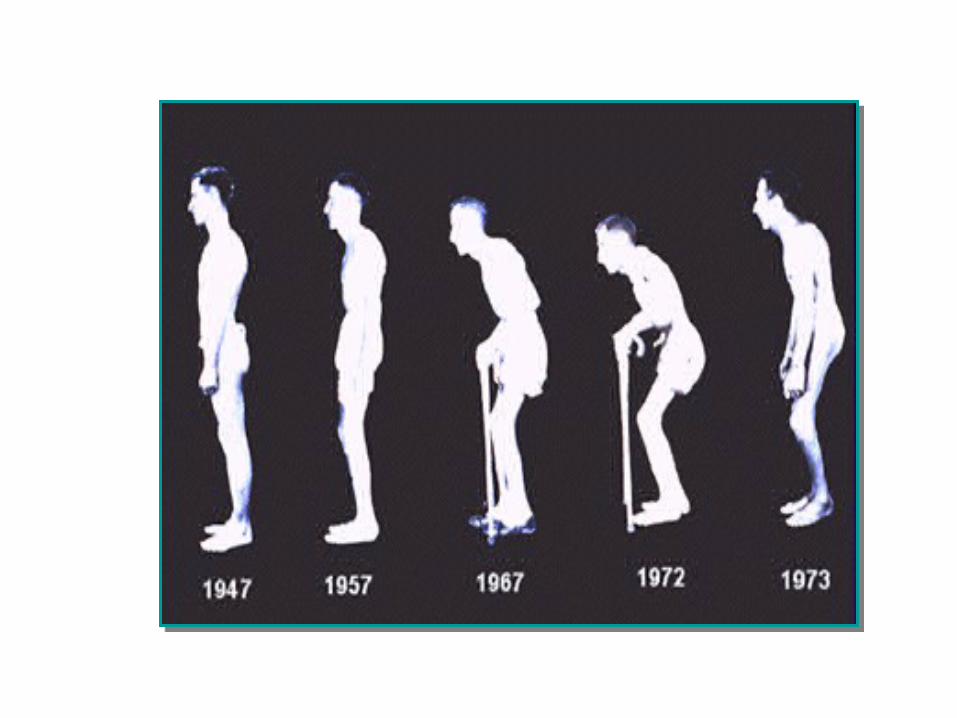
• Advanced AS
bony ankylosis
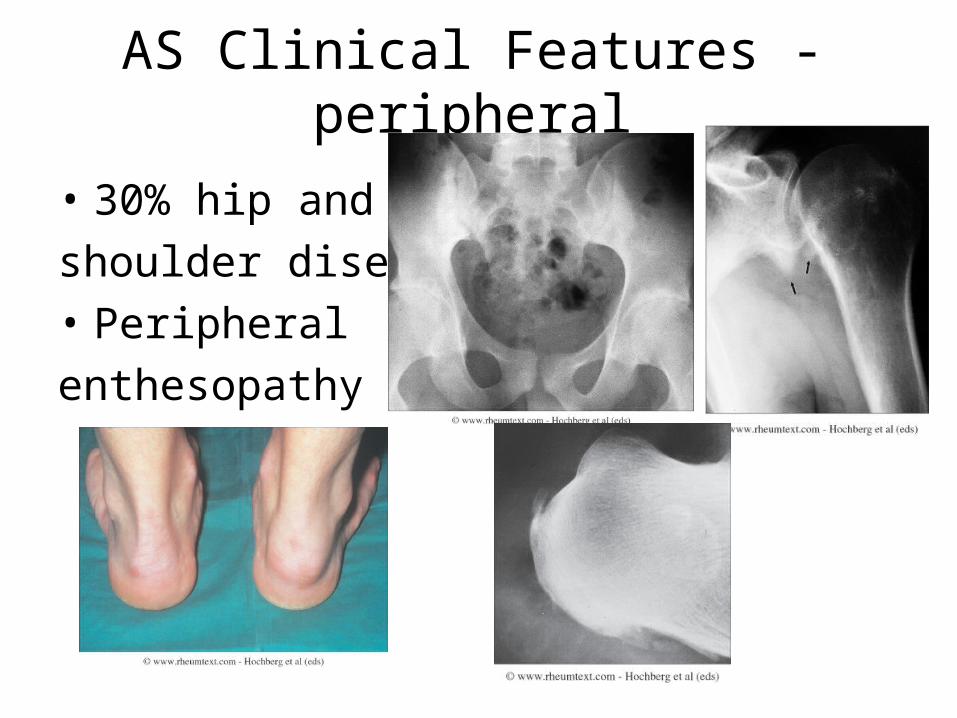
AS Clinical Features - peripheral
• 30% hip and
shoulder disease
• Peripheral
enthesopathy
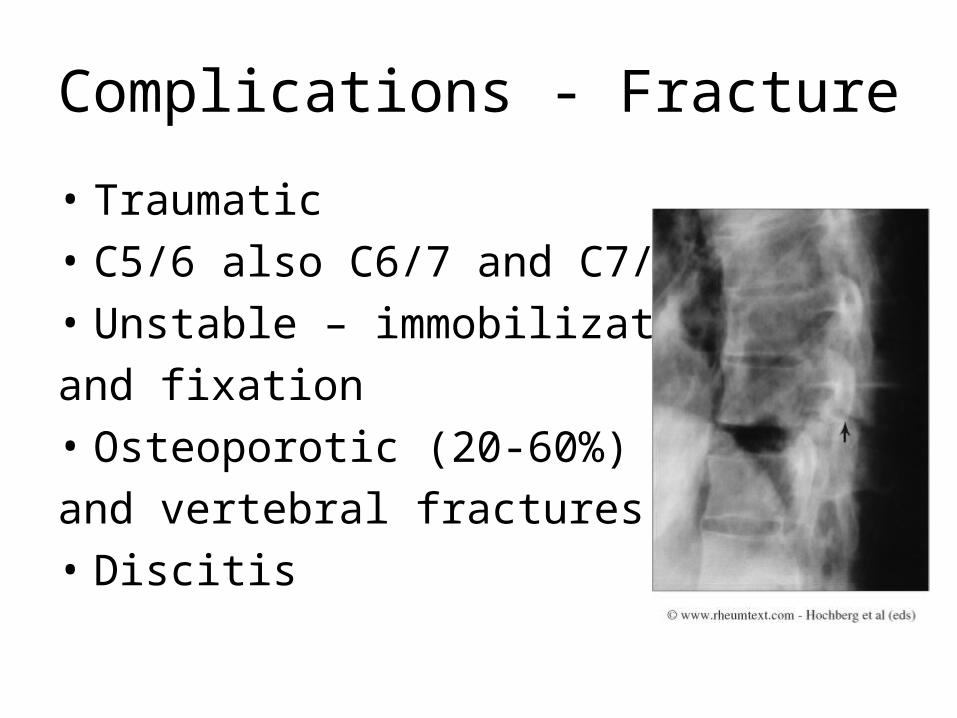
Complications - Fracture
• Traumatic
• C5/6 also C6/7 and C7/T1
• Unstable – immobilization
and fixation
• Osteoporotic (20-60%)
and vertebral fractures (8-15%)
• Discitis
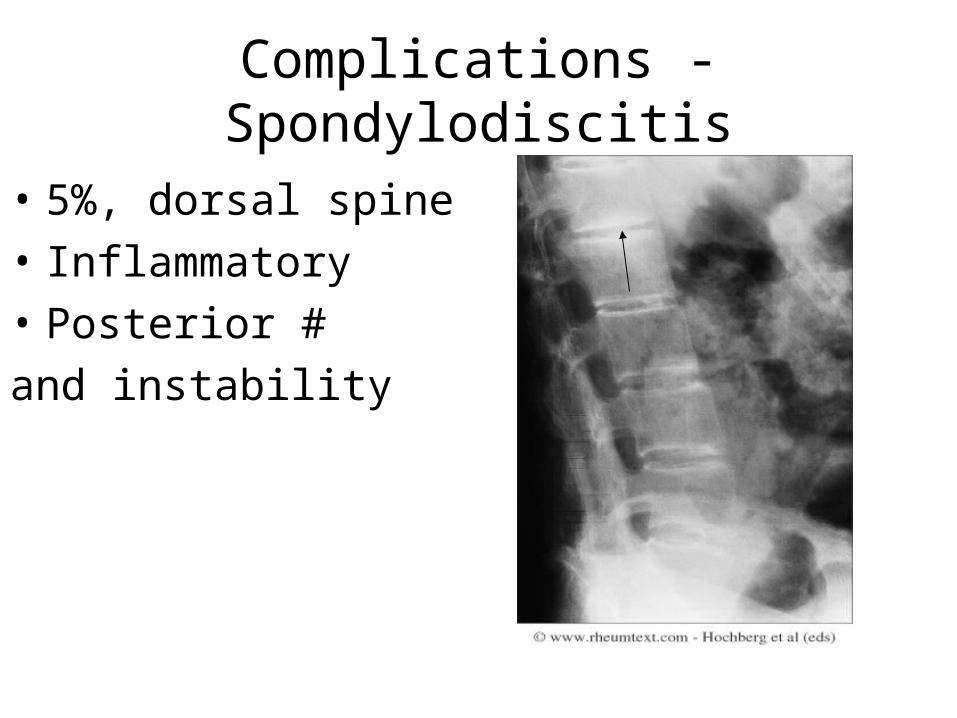
Complications - Spondylodiscitis
• 5%, dorsal spine
• Inflammatory
• Posterior #
and instability
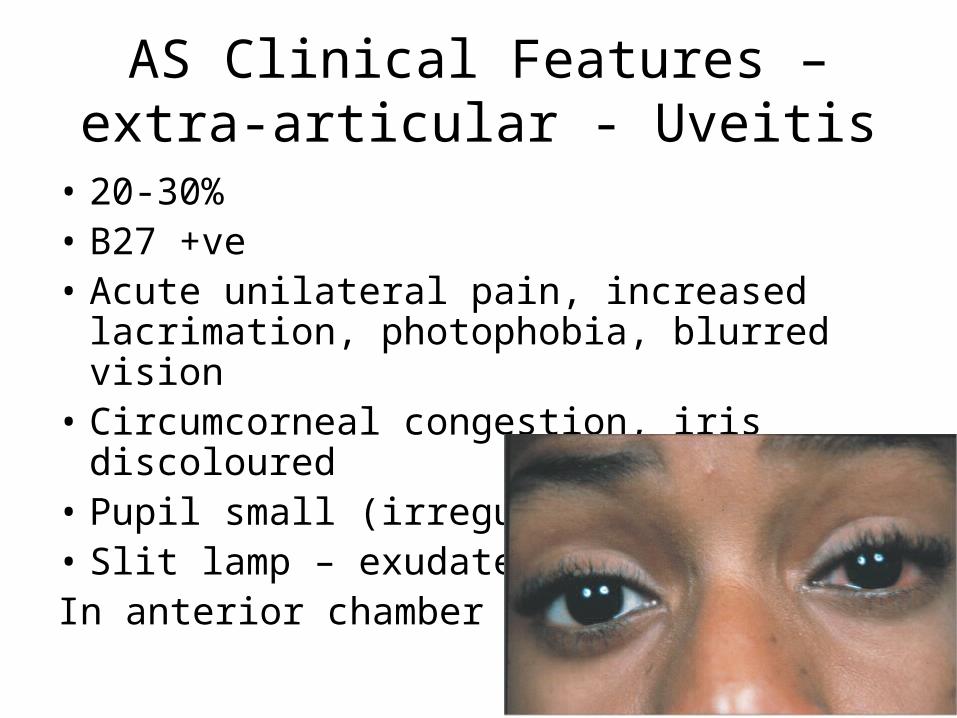
AS Clinical Features – extra-articular - Uveitis
• 20-30%• B27 +ve• Acute unilateral pain, increased
lacrimation, photophobia, blurred vision• Circumcorneal congestion, iris discoloured• Pupil small (irregular)• Slit lamp – exudatesIn anterior chamber
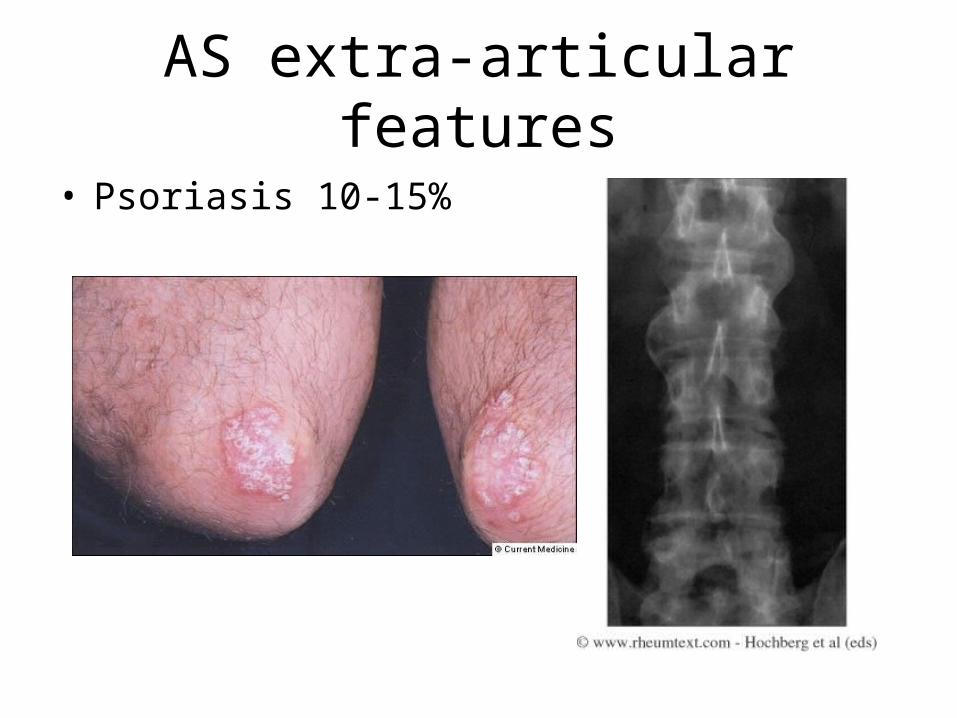
AS extra-articular features
• Psoriasis 10-15%

AS Clinical Features – extra-articular – Inflammatory bowel
• GI - Clinically silent enteric mucosal lesions 30-60%
• UC and Crohn’s 5-15% spinal and 10-20% peripheral arthritis
AS Clinical Features – extra-articular - Cardiac
• 2%
• Increases with age, duration and peripheral arthritis
• Aortic regurgitation – 3.5% (after 15years) and 10% (after 30 years)
• Conduction defects – 2.7% (after 15years) and 8.5% (after 30 years)
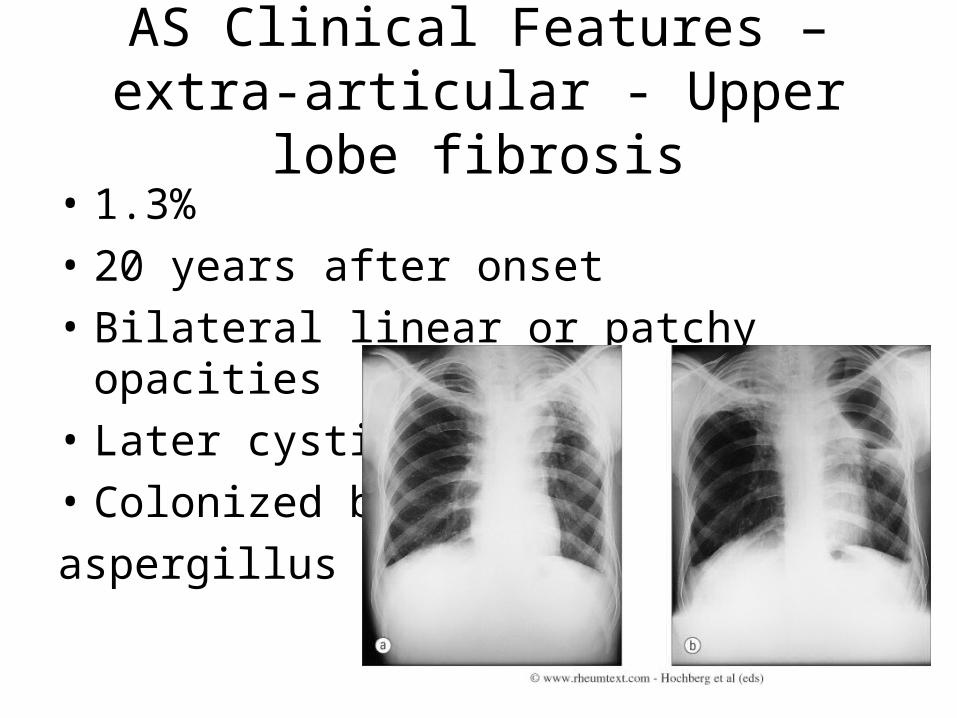
AS Clinical Features – extra-articular - Upper lobe fibrosis
• 1.3%
• 20 years after onset
• Bilateral linear or patchy opacities
• Later cystic
• Colonized by
aspergillus
AS Clinical Features – extra-articular
• Neurological – fracture dislocation, Cauda equina syndrome, atlanto-axial disease
• Renal – amyloidosis, IgA nephropathy, analgesic nephropathy
Investigations
• L/spine and SIJ x-rays
• CRP and ESR
• HLA B-27 – high clinical suspicion but x-ray not diagnostic – if positive worth referring as MRI can confirm pre-radiographic AS
AS – treatment
• Physiotherapy
• NSAIDS
• ‘DMARDs’ and steroids
• TNF alpha blockade
• Surgery
Psoriatic arthritis (PsA)
Demography - PsA
• No widely accepted criteria for diagnosis of PsA
• BSR guidelines estimate prevalence of 0.1% -1% - 500-1000 patients in UHCW
• Peak age of onset: 35-50 years
• Equal sex distribution
Burden of PsA
• 40%–57% have deforming arthritis
• 11%–19% are disabled
• Mortality is increased, compared with general population
PsA – clinical features
5 clinical subgroups:
• (Symmetrical) polyarthritis (RA-like) – 50% cases
• Asymmetrical oligoarthritis - 35% cases
• DIP disease - 5% cases
• Spondylitis (axial involvement) – 5% cases
• Arthritis mutilans - 5% cases
……..but much overlap

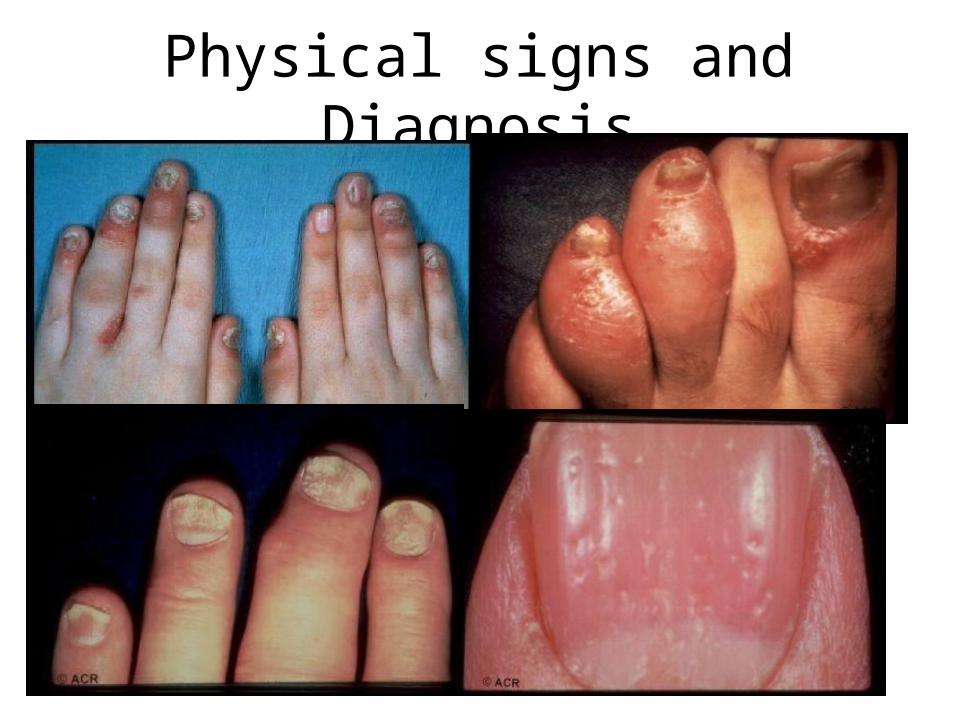
Physical signs and Diagnosis
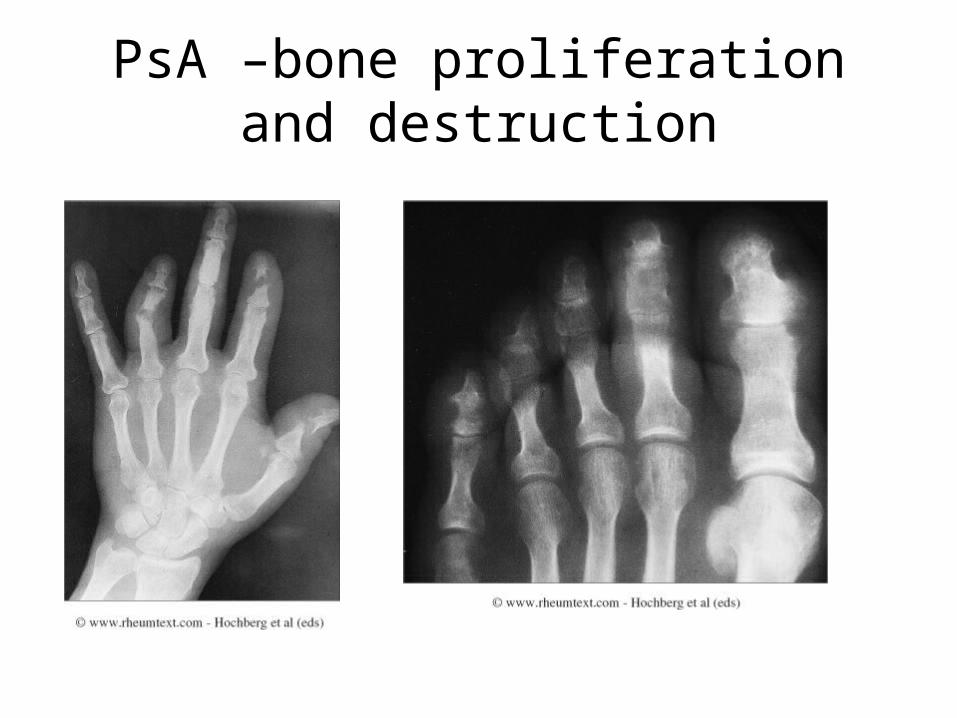
PsA –bone proliferation and destruction

Treatment
• NSAIDs• DMARDs – Sulphasalazine, Methotrexate,
Leflunomide, Cyclosporin• Steroids• TNF alpha blockade• OT, PT• Surgery• Dermatology input

• Reactive arthritis features ?
Reactive arthritis
• Young adults, equal sex
• Incidence of 30-40/100,000
• Post urethritis/cervicitis or infectious diarrhoea eg campylobacter, salmonella, shigella, yersinia,chlamydia – 1-6 weeks
• Sero-ve features + conjunctivitis, balanitis, oral ulcers, pustular psoriasis

Reactive arthritis
• Culture – throat, urine, stool, urethra/cervix
• Treatment – NSAIDs, steroids –intra-articular, antibiotics – chlamydia, DMARDs eg sulphasalazine
Summary
• Young adults
• Enthesitis, peripheral arthritis, spinal inflammation
• Psoriasis, inflammatory bowel disease, anterior uveitis, prior GU/GI infection
• B27 screening in inflammatory back pain with normal x-rays
• TNF alpha blockers – new hope