session 306: treating the obese acute spinal cord injured … · 2017-07-25 · bladder care,...
TRANSCRIPT
To comply with professional boards/associations standards:• I declare that I (or my family) do not have a financial relationship in any amount, occurring in the last 12 months with a commercial interest whose products or services are discussed in my presentation. Additionally, all planners involved do not have any financial relationship.•Requirements for successful completion are attendance for the full session along with a completed session evaluation.•Vyne Education and all current accreditation statuses does not imply endorsement of any commercial products displayed in conjunction with this activity.
Session 306: Treating the Obese Acute Spinal Cord Injured Patient
Stephanie Berger, MPT & Karin Seeley, PT
Leading the Way in Continuing Education and Professional Development. www.Vyne.com

In data collected from the SCI Model Systems from 2006‐2009 about 25% of traumatic SCI patients were obese.1
Similar dispositions as non‐obese Lower FIM scores Longer lengths of stay More complications
Obese SCI injuries more likely to be medical/surgical rather than traumatic2
We must be prepared to face the unique challenges associated with working with an obese or overweight patient who has sustained a SCI.
1. Describe common comorbidities and complications found in the obese patient & how they may impact SCI rehab.
2. Describe the different obese and overweight body types and how the distribution of their adipose tissue & center of gravity affects function.
3. Identify safe handling techniques and provide strategies for mobilizing obese spinal cord injured patients, including equipment options to assist with bowel and bladder care, hygiene, and mobility.

Difficult for EMTs to stabilize in the field Prolonged extrication Collars aren’t large enough Need to use sandbags instead of collars Splints for fractures don’t fit Back boards may not fit Intubation difficult Some ambulances cannot accommodate >500 lb5
Imaging in the obese trauma patient can be challenging. Plain radiographs can be of poor quality
due to the amount of penetration and difficulty in proper patient positioning to best measure alignment.6
FAST scans have poor wave penetration with decreased imaging3
CT is the only recommended imaging modality.3,7,8
A 2008 survey revealed that despite type of hospital only about 25% can scan a patient up to 450#.
▪ MRI capabilities are even more limited▪ Although open MRIs can accommodate larger weights ,images have less quality8
Transportation to radiology can also be an issue..
Obese patients may exceed the maximal allowable dose of radionuclide required for their weight.6,7
More extensive pre‐op and medical evaluation6,9
Obesity is a risk factor for post operative wound infection.6,9,10
Increased use of prophylactic antibiotics
High risk of aspiration during anesthesia induction3,6
Need to use open‐frame table during prone positioning to allow pannus to hang free
Longer incisions More extensive soft tissue dissection
Pharmacokinetics of analgesics differ due to increased adipose tissue and plasma volume
Not as effective
Patients with obstructive sleep apnea have increased risk of respiratory depression with narcotics
DVT prophylaxis: increased risk of epidural hematoma
Motion can occur at all spinal levels despite proper fit of the brace.
When bracing, there is less mechanical support and it is less tolerated than in thinner patients.
Fixation should be strongly considered in unstable thoracolumbar injuries in obese patients.
Pneumatic boots used to preventDVT and multipodus boots to prevent heel ulcers may not fit feet.
Breathing effort increases and efficiency of air exchange decreases; reductions in chest wall compliance make the amount of strength required to generate a breath much greater11
Excess adipose tissue creates an increased workload for supportive muscles
O2 consumption and CO2 production are increased
Resting functional residual lung capacity is decreased5
The incidence of reflux, hiatal hernias, and abdominal pressure are all increased which results in an increased risk for aspiration
Increased metabolic demand and cardiac output
Myocardial compliance decreases (~30%)
Increased risk of arrhythmias through fatty and ischemic changes to myocardium
Increased blood volume overall However is low as a percentage of body weight as compared to normal
Increased stroke volume index and stroke work index in proportion to body weight which can lead to left ventricular dilation and hypertrophy
This can lead to hypoxia and hypercapnea which can lead to vasoconstriction and in turn chronic pulmonary HTN and right sided heart failure
May need to assess BP at the forearm with a leg cuff but these readings are less reliable
Ultrasound/ Dopplers do not penetrate adipose tissue properly
IV access is more difficult6

More days on ventilator More days in ICU Obese polytrauma patients have increased risk of pelvic and LE injuries, complicating any SCI
Twice as likely to have major complications
Acute renal failure
Sepsis
Pressure ulcers
Formulate an interdisciplinary task force to consider all the needs of the patient
Ensure that proper equipment is available‐check weight limits
Ongoing training is necessary‐one time training is not enough!
Using the same brand throughout the entire facility simplifies training
When constructing or remodeling, consider the needs of the bariatric patient: wider doors, bigger rooms, structural integrity and having rooms with overhead lifts
Manual lifting and moving of patients increases the risk of injury14,15,16,17,22
Ceiling lifts result in lowest back loads15
Stress shifts to the wrists/knees
Ensure that enough staff members are available at key times: repositioning in bed, transfers, bathing, cathing, etc.14,16
Higher risk of depression and poor self‐esteem14,15
Nearly 80% of surveyed obese patients reported disrespectful treatment from the medical community19
Plan ahead privately with staff, not in front of the patient14
Choose a code word to request assistance from co‐workers14
Have proper equipment already in place22
Recognize that fear of injury is shared by both the patient and caregivers3,4,15,17,19
Patients will often report not needing assistance, or using inadequate techniques for cleanliness/hygiene (especially perianal care).
Offer to help with sensitivity
Ongoing education on weight management is necessary21
There are unique challenges to weight management in people with spinal cord injuries14,21
Dieticians can be valuable team members21
Loss of control with life can increase the desire to eat
Obesity and malnutrition are not mutually exclusive11
Critically ill patients with obesity use protein rather than fat stores as a primary source of energy5,11
This leads to a loss of muscle and lean body mass5

Equipment challenges Frequently custom made and/or expensive4,22
Coverage for items is based on weight, not body shape22
Needs to be addressed early in stay
Discharge to a skilled nursing facility can take time22
Lack of appropriate equipment Lack of staff
Home accessibility Width of doorways Capacity of home to accommodate size of recommended equipment4
Bathroom layout
Odds of rehospitalization are 1.53 times higher for obese persons than healthy weight2
Patients with SCI rely on caregiver assistance▪ Are your patient’s caregivers physically able to provide it?
Family training should be early and often due to the increased need for assistance in all aspects of care
▪ Especially bowel and bladder management
Equipment
Bariatric Beds often have nylon covered air mattresses to best manage skin but they put the patient at risk of sliding off the bed when going to short sit23
Overhead trapezes may assist with some patient mobility but prevent the use of lifts
Bed rails need to get fully out of the way if doing anything besides a lift transfer
Can the bariatric bed fit in the elevator or through the doorways?
Beds that turn into chairs may be easier to get out of but can be very difficult to get back into
U‐SHAPED/ SPLIT LEG
Adjustable length hooks allow for different sitting angles
Straps can be crossed between legs or under both
Can be removed when up in wheelchair
Easily placed under patient (less rolling)
FULL BODY
Require significant rolling to get under patient.
Risk of sliding out if not positioned correctly
Cannot be removed when in wheelchair
Cannot be used to get on and off commode.
Becoming more common‐standard of care?
Difficult to get under a very large patient
At high risk for getting soiled and need frequent replacing
Are useful for bed to stretcher transfer
Can be used to reposition a patient who has slid down in the bed
(photo courtesy of Liko.com)
BENEFITS
Using a low‐friction glide sheet may help reduce the risk of caregiver injury17,18
More efficient and easier than draw sheets17,18
Better offloading than pillows or blankets18
Less costly18
CAUTIONS
Sliding down in bed
Accidental disposal during linen changes
Weight rating/bottoming out of positioning wedges
Model Make Materials Weight rating Cost (facility rates)
Comfort Glide Sheet Medline Nylon bottomMicrofiber coverAir permeable
575 lb standard1000 lb XL
$33
Comfort Glide Wedges
Medline High density foamNon slip bottom
575 lb standard1000 lb XL
$40.83
Tortoise Sundance Solutions
Low pressure air chamber ? $165 per unit (includes positioner)
Fluidized Positioner Sundance Solutions
MoldableMaintains its shape
?
PrevalonTurn and Position 2.0
Sage Glide sheet (nylon)and Anchor Wedges (foam)Micro Climate body pads
550 lb $120.25
$94.50/30
Know the Weight Capacity Lifts and Slings Treatment tables (hydraulics) Beds Stretchers Stairs Ambulances/ vans Walkers/crutches Wheelchairs Commodes Wall hung toilets only have a #250
capacity Transfer boards are rarely an issue except
when attempting to bridge very large gaps
Weight Capacity may be OK but size may not.
Make sure your Bariatric Room Kit includes the small stuff
Often overlooked are the items that do the most to embarrass the patient
Proper fitting gowns, diapers, and slippers
Sheets that fit the bed
Body Shapes
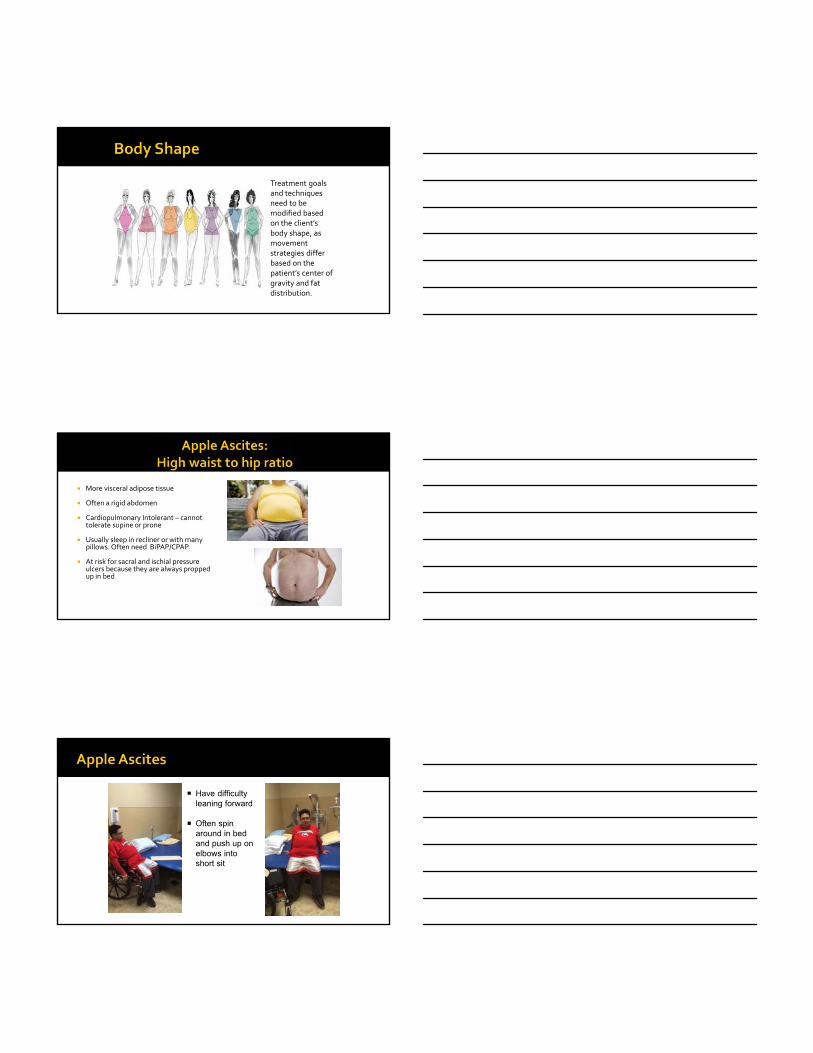
Treatment goals and techniques need to be modified based on the client’s body shape, as movement strategies differ based on the patient’s center of gravity and fat distribution.
More visceral adipose tissue
Often a rigid abdomen
Cardiopulmonary Intolerant – cannot tolerate supine or prone
Usually sleep in recliner or with many pillows. Often need BiPAP/CPAP.
At risk for sacral and ischial pressure ulcers because they are always propped up in bed
Have difficulty leaning forward
Often spin around in bed and push up on elbows into short sit
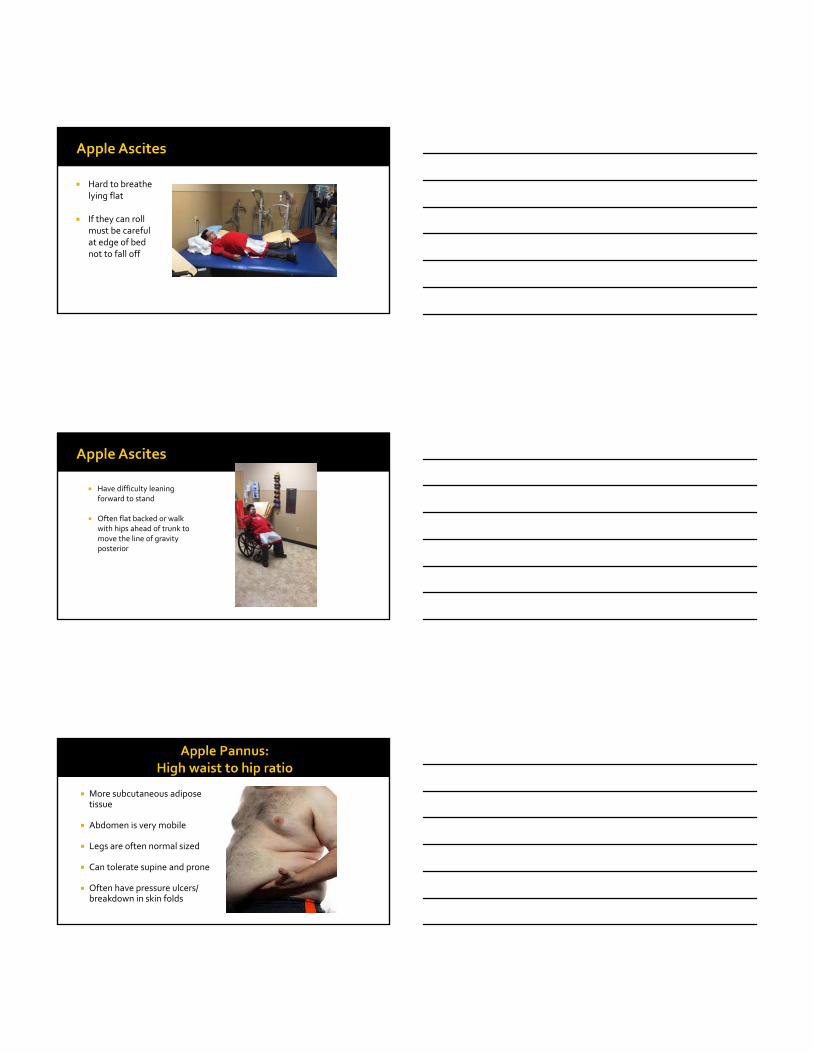
Hard to breathe lying flat
If they can roll must be careful at edge of bed not to fall off
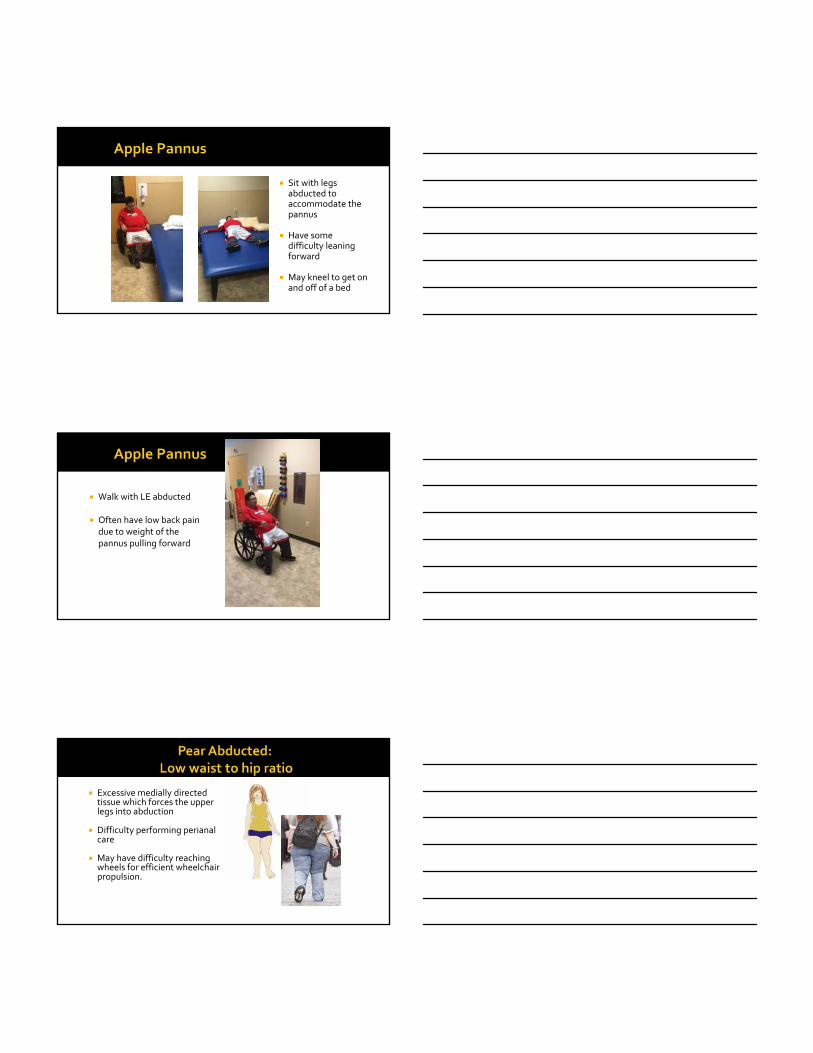
Have difficulty leaning forward to stand
Often flat backed or walk with hips ahead of trunk to move the line of gravity posterior
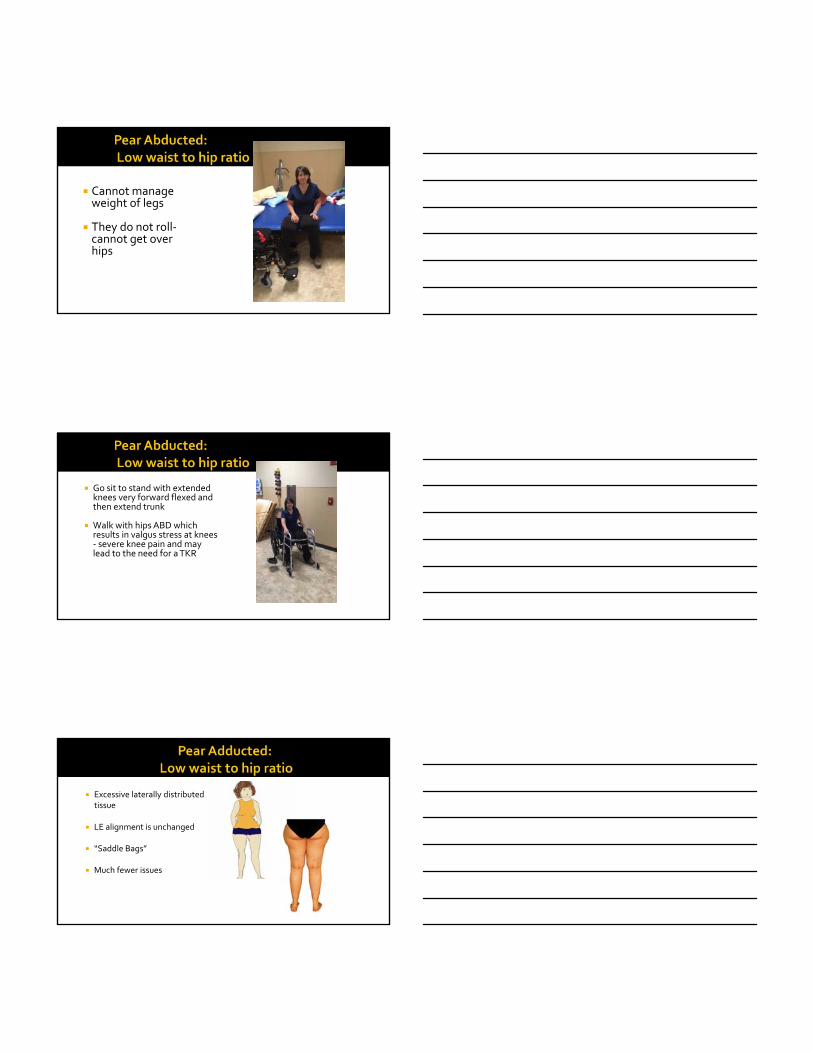
More subcutaneous adipose tissue
Abdomen is very mobile
Legs are often normal sized
Can tolerate supine and prone
Often have pressure ulcers/ breakdown in skin folds
Sit with legs abducted to accommodate the pannus
Have some difficulty leaning forward
May kneel to get on and off of a bed
Walk with LE abducted
Often have low back pain due to weight of the pannus pulling forward
Excessive medially directed tissue which forces the upper legs into abduction
Difficulty performing perianal care
May have difficulty reaching wheels for efficient wheelchair propulsion.
Cannot manage weight of legs
They do not roll‐cannot get over hips
Go sit to stand with extended knees very forward flexed and then extend trunk
Walk with hips ABD which results in valgus stress at knees ‐ severe knee pain and may lead to the need for a TKR
Excessive laterally distributed tissue
LE alignment is unchanged
“Saddle Bags”
Much fewer issues

May have difficulty reaching wheels for efficient wheelchair propulsion.
May also have difficulty with getting arms close enough to hips to get a good lift for transfers
Likely to have back pain with side‐lying
Few problems with sit to stand unless very heavy
Gait really unaffected
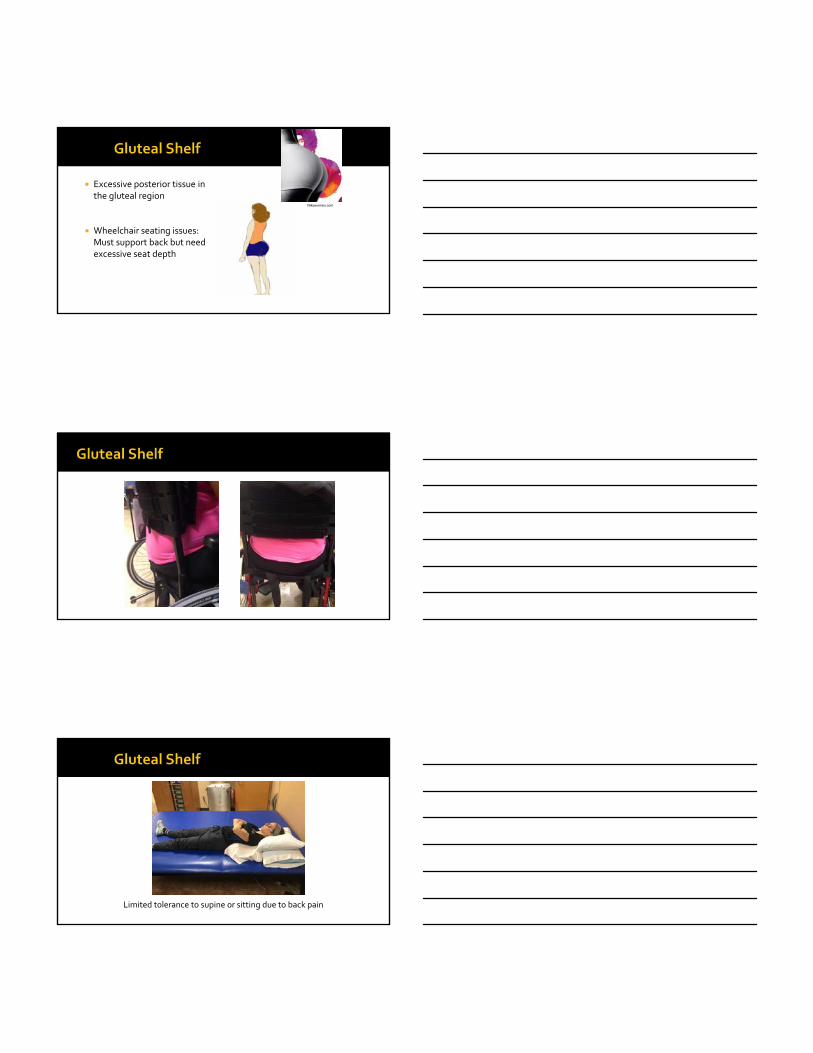
Excessive posterior tissue in the gluteal region
Wheelchair seating issues: Must support back but need excessive seat depth
Nikewomen.com
Limited tolerance to supine or sitting due to back pain
Watch buttocks scraping across tires in transfer
Moving the Patient
Bariatric patients will have about 30% less ROM due to tissue bulk
If a patient is Partial Weight Bearing make sure Ortho specifies a poundage rather than a percentage
Obesity may be a greater functional barrier to patients with paraplegia than patients with tetraplegia Goals of the paraplegic tend to require being able to support your own body weight Tetraplegic rely on others and or equipment1
Increased shoulder pain due to lifting and moving more weight
Use reverse Trendelenberg for scooting up in bed
Independent leg management may be impossible The apple can’t reach their legs
The pear can’t lift their legs
Falls can occur when rolling to side on too small of a bed, or the bed can actually tip over (line of gravity is too close to the edge)
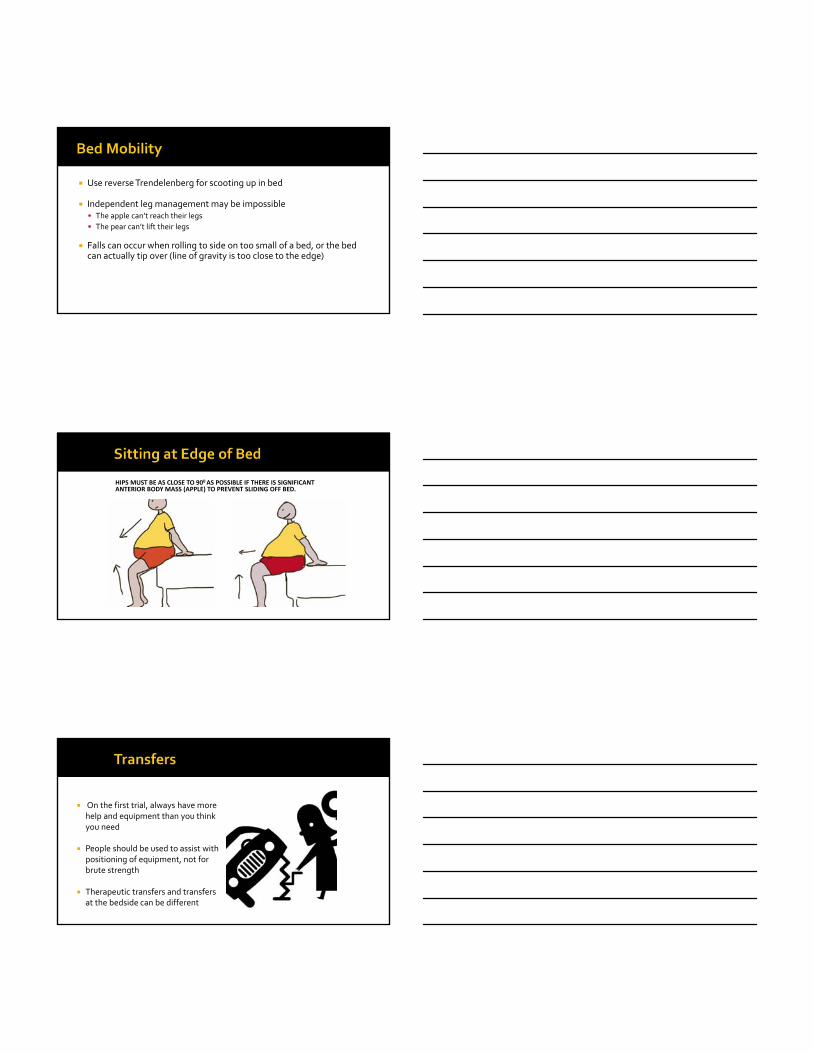
HIPS MUST BE AS CLOSE TO 900 AS POSSIBLE IF THERE IS SIGNIFICANT ANTERIOR BODY MASS (APPLE) TO PREVENT SLIDING OFF BED.
On the first trial, always have more help and equipment than you think you need
People should be used to assist with positioning of equipment, not for brute strength
Therapeutic transfers and transfers at the bedside can be different
De‐weighting the bones does not necessarily de‐weight the tissue as it can sag down and still not clear for a transfer
Pear shaped may not be able to get arms to the surface because they are so abducted (may need push up blocks)
Apple shaped may not be able to forward lean sufficiently to de‐weight bottom
Practice lateral motion on a mat first before going to a wheelchair
Obese people have limited trunk flexion and move feet backwards in performing sit to stand transfers24,25
This requires increased knee movement and torque/strength
There is an anterior displacement of the center of mass‐therefore need greater ankle torque to stabilize the body25,26
Egress Test developed by Michael Dionne, PT before doing a stand pivot transfer27
Clearing test: patient elevates and clears surface by 1”‐2”
Two reps of sit to full stand
Three steps marching in place
Advance step and return each foot (trailing leg keeps contact with starting surface)
If the patient needs more than contact guarding or cues, use a lift
Nursing Considerations
Struggle with standard staffing ratios but the care is far greater22
Use a lifting sling under a leg to assist with care
Have sufficient assistance for tasks: do not attempt to turn or mobilize the patient alone16
(photo courtesy of Liko.com)
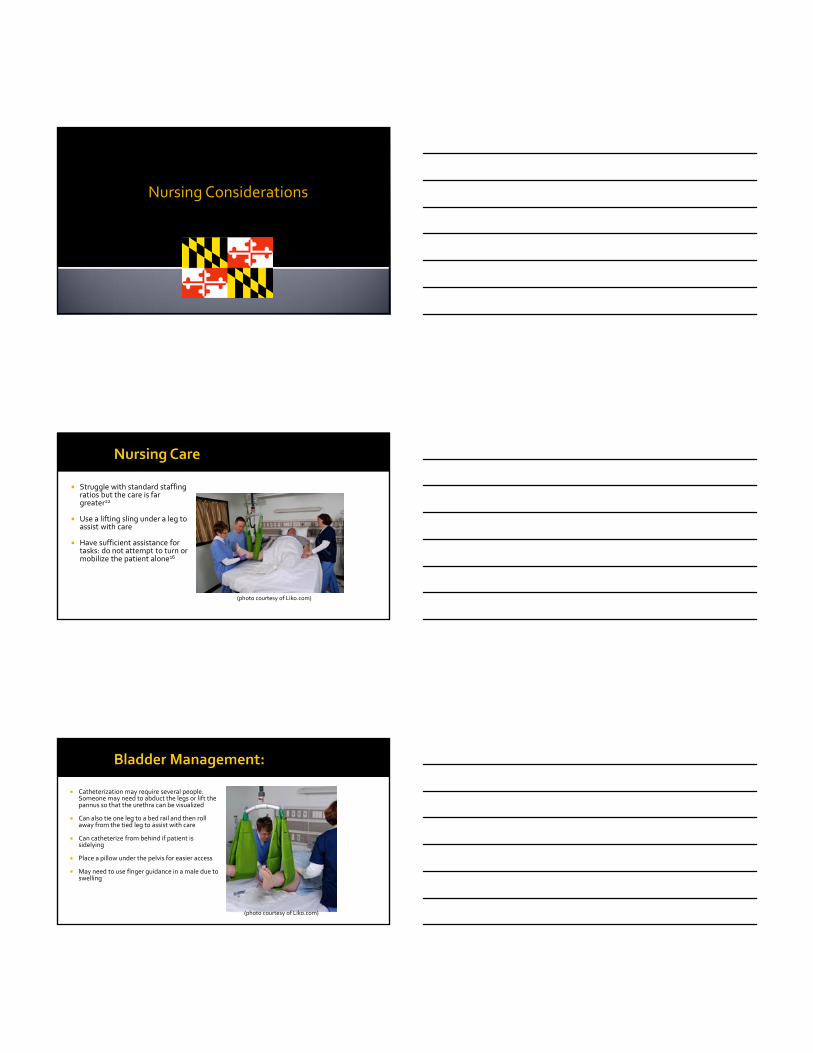
Catheterization may require several people. Someone may need to abduct the legs or lift the pannus so that the urethra can be visualized
Can also tie one leg to a bed rail and then roll away from the tied leg to assist with care
Can catheterize from behind if patient is sidelying
Place a pillow under the pelvis for easier access
May need to use finger guidance in a male due to swelling
(photo courtesy of Liko.com)

Adaptive equipment:
Men often need to use female urinals to access under the pannus
Thigh spreader
Labia spreader
Urethral locator
Most bariatric patients will have stress incontinence and need diapers (that fit)
Place suppository while in bed, then transfer to commode to allow gravity to assist with elimination
Bariatric commodes must allow for side, front or rear access for bowel training
Enemeez can reduce number of transfers necessary
This is a hard and dirty job and you may need more than standard gloves to access the patient
Suppository inserter to assist in reaching anus
Transanal irrigation system has a bag to collect stool
(photo courtesy of Liko.com)
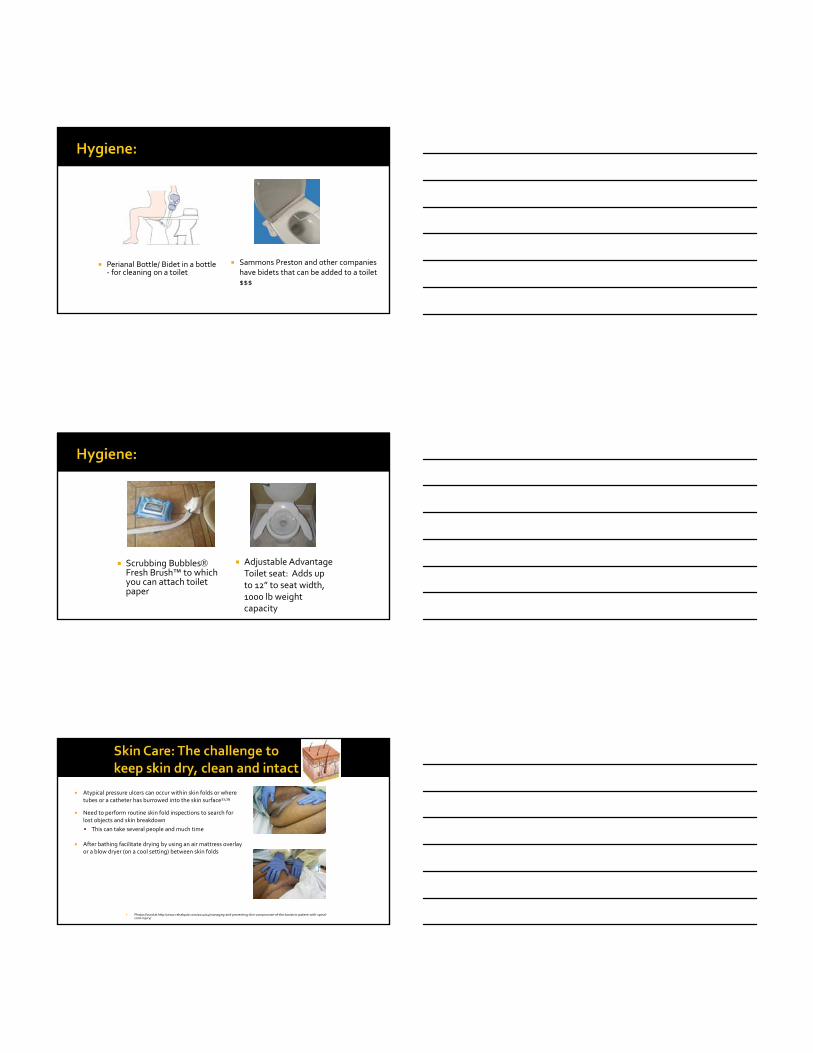
Perianal Bottle/ Bidet in a bottle ‐ for cleaning on a toilet
Sammons Preston and other companies have bidets that can be added to a toilet $$$
Scrubbing BubblesFresh Brush™ to which you can attach toilet paper
Adjustable Advantage Toilet seat: Adds up to 12” to seat width, 1000 lb weight capacity
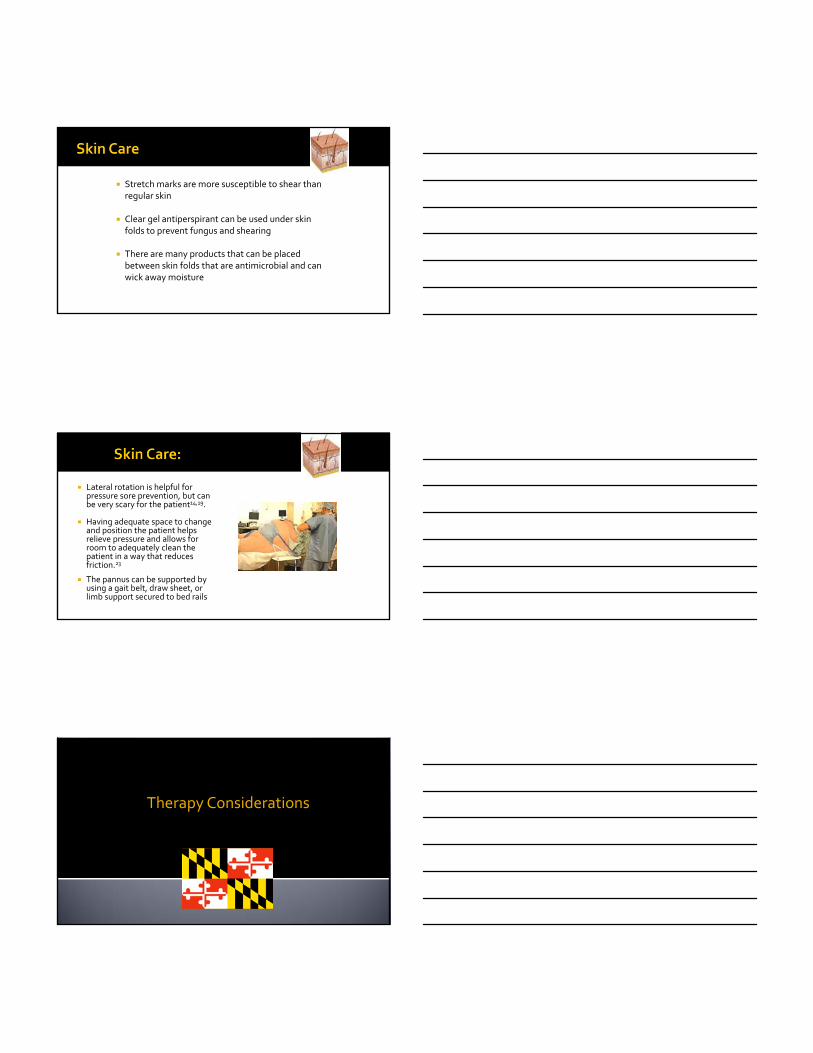
Atypical pressure ulcers can occur within skin folds or where tubes or a catheter has burrowed into the skin surface11,19
Need to perform routine skin fold inspections to search for lost objects and skin breakdown
This can take several people and much time
After bathing facilitate drying by using an air mattress overlay or a blow dryer (on a cool setting) between skin folds
Photos found at http://www.rehabpub.com/2012/04/managing‐and‐preventing‐skin‐compromise‐of‐the‐bariatric‐patient‐with‐spinal‐cord‐injury/
Stretch marks are more susceptible to shear than regular skin
Clear gel antiperspirant can be used under skin folds to prevent fungus and shearing
There are many products that can be placed between skin folds that are antimicrobial and can wick away moisture
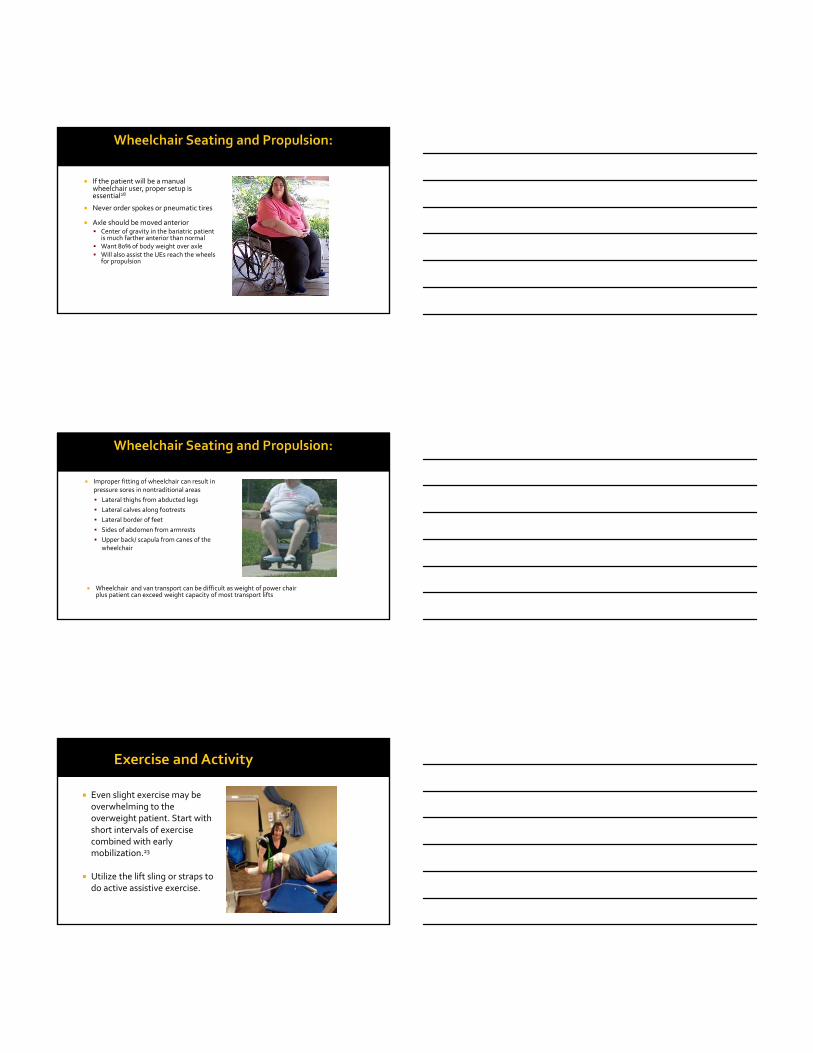
Lateral rotation is helpful for pressure sore prevention, but can be very scary for the patient14,19.
Having adequate space to change and position the patient helps relieve pressure and allows for room to adequately clean the patient in a way that reduces friction.23
The pannus can be supported by using a gait belt, draw sheet, or limb support secured to bed rails
Therapy Considerations

Have you done anything to your home to be more independent? For example, raising the height of the bed or furniture
Where and in what position did you sleep? How many pillows do you use in bed? How did you get in and out of bed?
How did you toilet and perform hygiene? Used a PVC pipe as a urinal Use a large towel to wipe
What type of clothing do you wear at home?
Where and from whom do you get your food?
Be open to how they have done things and try to accommodate their ways
Less ability to flex at trunk=harder to perform bathing and dressing
Generally easier performing ADL’s sitting at side of bed if able and a bit sideways so they can lean laterally rather than directly forward over the belly
Inability to reach all areas of body (e.g. back, feet) for bathing
Increased girth causes patient to sit farther from table for table‐top tasks
greater energy expenditure
increased difficulty
Full strength in the arms does not necessarily indicate that a person can propel a manual wheelchair28
Can they perform sufficient pressure relief?
Apparent short arm syndrome because arm length is lost on abduction from body can make w/c propulsion difficult
Greater body weight + added weight of heavy duty frame increases the rolling resistance of the wheelchair28
Propelling a manual chair with the heavier load increases the risk of shoulder pathology29
May be able to propel short distances, then become too fatigued to perform ADL’s or transfers
If the patient will be a manual wheelchair user, proper setup is essential28
Never order spokes or pneumatic tires
Axle should be moved anterior Center of gravity in the bariatric patient
is much farther anterior than normal Want 80% of body weight over axle Will also assist the UEs reach the wheels
for propulsion
Improper fitting of wheelchair can result in pressure sores in nontraditional areas
Lateral thighs from abducted legs
Lateral calves along footrests
Lateral border of feet
Sides of abdomen from armrests
Upper back/ scapula from canes of the wheelchair
Wheelchair and van transport can be difficult as weight of power chair plus patient can exceed weight capacity of most transport lifts
Even slight exercise may be overwhelming to the overweight patient. Start with short intervals of exercise combined with early mobilization.23
Utilize the lift sling or straps to do active assistive exercise.
Gait belts will change position as soft tissue is affected by gravity. Place either in the arm pits or below the belly where it may also help to support the pannus.
Check the belt tautness once standing. Watch your hand grip; do not wrap the belt around your wrist. You need a quick release or you will injure your wrist and shoulder if the patient falls.
Traditional spotting techniques will not be effective as most larger patients fall forward nowhere near the trailing wheelchair
When larger patients do fall they tend to externally rotate the hips so block the knees more laterally to better
prevent the fall
May need to rest a pannus on a walker with a seat or a board across the walker bar
Use a bed sheet around the hips and buttocks to assist in transfers and ambulation
Larger patients ambulate with an increased sway pattern and greater step width with circumduction to advance their legs25. Try not to block this.
Use mechanical devices to provide support
(photo courtesy of Liko.com)
Traditional ambulation training aides, bracing and new technology options may not be an option for the bariatric patient
Through proper training, both caregivers and staff can learn the best ways to perform hygiene, including bowel and bladder management, properly and with dignity as well as mobilize the patient without injury to the patient or caregiver.
Stephanie Berger PT, MPT
Karin Seeley PT
1. Stenson, K.W; Deutsch, A; Heinemann, A.W; Chen, D. (2011). Obesity and Inpatient Rehabilitation Outcomes for Patients With a Traumatic Spinal
Cord Injury. Arch of Phys Med Rehab, 92(3): 384‐390.
2. Tian W; Hsieh, C; DeJong G; et al. (2013). Role of Body Weight in Therapy Participation and Rehabilitation Outcomes Among Individuals with
Traumatic Spinal Cord Injury. Arch of Phys Med Rehab, 94(4 Suppl 2):S125‐36.
3. Koba, Patricia. (2016). Identifying Obstacles for the Obese Trauma Patient. Journal of Trauma Nursing 23.1: 45‐48.
4. Ziglar, M.K. (2006). Obesity and the Trauma Patient: Challenges and Guidelines for Care. Journal of Trauma Nursing, 13(1)22‐27.
5. Bushard, S. (2002). Trauma in Patients Who are Morbidly Obese. AORN. 76(4): 585‐589.
6. Elgafy, Hossein, et al. (2016). Critical Care of Obese Patients During and After Spine Surgery. World Journal of Critical Care Medicine 5.1: 83.
7. Uppot, R.N; Sahanti, D.V; Hahn, P.F; et al. (2007). Impact of Obesity on Medical Imaging and Image‐Guided Intervention. AJR. 188:433‐440.
8. Ginde, A.A; Foianin, A; Renner, D.M; et al. (2008). The Challenge of CT and MRI Imaging of Obese Individuals Who Present to the Emergency
Department: A National Survey. Obesity. 16(11): 2549‐51.
9. Perry, K. I., and S. J. MacDonald. (2016). The Obese Patient: A Problem of Larger Consequence. Bone & Joint Journal 98.1 Supple A: 3‐5
10. Greenleaf, R.M; ltman, D.T. (2011). Evaluation and Treatment of Spinal Injuries in the Obese Patient. Orthop Clin N Am 42: 85‐93.
11. Charlesbois, D; Wilmoth, D. (2004). Critical Care of Patients with Obesity. Crit Care Nurse. 24:19‐27.
12. Licht, Heather, et al. (2015). The Relationship of Obesity to Increasing Health‐Care Burden in the Setting of Orthopaedic Polytrauma. J Bone Joint Surg Am 97.22: e73.
13. Dhungel, Vinayak, et al. (2015). Obesity Delays Functional Recovery in Trauma Patients. Journal of Surgical Research 193.1: 415‐420.
14. Practical Approaches to Adapting Nursing Care: The Bariatric Spinal Cord Injured Patient. Presented at Contemporary Forums Spinal Cord Injury Conference, Boston. May 2010.
15. Choi, Sang D., and Kathryn Brings. (2016). Work‐Related Musculoskeletal Risks Associated with Nurses and Nursing Assistants Handling Overweight and Obese Patients: A Literature Review. Work Preprint:
1‐10.
16. Hallmark, Beth, Patricia Mechan, and Lynne Shores. (2015). Ergonomics: Safe Patient Handling and Mobility. Nursing Clinics of North America 50.1: 153‐166.
17. Theou O.; Soon Z.; et al. (2011). Changing the Sheets: A New System to Reduce Strain During Patient Repositioning. Nursing Research. 60(5):302‐308.
18. Edger, M. (2017). Effect of a Patient‐Repositioning Device in an Intensive Care Unit on Hospital‐Acquired Pressure Injury Occurences and Cost: A Before‐After Study. J Wound Ostomy Continence Nurs.
44(3):236‐240.
19. Camden, S.G; Shaver, J; Cole, K. (2007). Promoting the Patient’s Dignity and Preventing Caregiver Injury While Caring for a Morbidly Obese Woman with Skin Tears and a Pressure Ulcer. Bariatric Nursing
and Surgical Patient Care. 2(1): 77‐82.
20. Mastrovgiovanni, D; Phillips, EM; Fine, CK. (2003). The Bariatric Spinal Cord –Injured Person: Challenges in Preventing and Healing Skin Problems. Top Spinal Cord Inj Rebahil. 9(2): 38‐44.
21. Wong, S., et al. (2015). Knowledge, Attitudes and Practices of Medical Staff towards Obesity Management in Patients with Spinal Cord Injuries: an International Survey of Four Western European
Countries. Spinal Cord 53.1: 24‐31.
22. Lumley, Elizabeth, et al. (2015). A Qualitative Study to Explore the Attitude of Clinical Staff to the Challenges of Caring for Obese Patients. Journal of Clinical Nursing
24.23‐24: 3594‐3604.
23. Veach, M. (2012). Handle with Care Reducing Hospitalization time for the Bariatric Patient. Advance for PT and Rehab Med. 23(11): 26.
24. Sibella, F; Galli, M; Romei, M; Montesano, A; Crivellini, M. (2003). Biomechanical analysis of sit‐to‐stand movement in normal and obese subjects. Clinical
Biomechanicals. 18:745‐750.
25. Wearing, SC; Hennig, EM; Byrne, NM; Steele, JR; Hills, AP. (2006).The biomechanics of restricted movement in adult obesity. Obesity Reviews. 7:13‐24.
26. Singh, Bhupinder, et al. (2015). Biomechanical Loads During Common Rehabilitation Exercises in Obese Individuals. International Journal of Sports Physical Therapy 10.2:
189.
27. Dionne, M; Introducing the Egress Test. (2004). Advance Healthcare Network for Physical Therapy and Rehab Medicine. 15(13): 39.
28. Fitzgerald, S; Kelleher, A. (2007). Mobility Challenges in Individuals with a Spinal Cord Injury with Increased Body Weight. Top Spinal Cord Inj Rehabil. 12(4): 54‐63.
29. Hatchett, Patricia E., et al. (2016). Body Mass Index Changes over 3 years and Effect of Obesity on Community Mobility for Persons with Chronic Spinal Cord Injury. The
Journal of Spinal Cord Medicine. 34.9:421‐432.