severe traumatic brain injury - agency for … · guideline no: 0/c/07:0055-01:02 picu guideline:...
TRANSCRIPT
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
This document reflects what is currently regarded as safe practice. However, as in any clinical situation, there may be factors which cannot be covered by a single set of guidelines. This document does not replace the need for the application of clinical judgement to each individual presentation. Approved by: SCHN Policy, Procedure & Guideline Committee PICU Management Date Effective: 1st May 2013 Review Period: 3 years Team Leader: Staff Specialist Area/Dept: PICU, CHW
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 1 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
SEVERE TRAUMATIC BRAIN INJURY PRACTICE GUIDELINE ©
DOCUMENT SUMMARY/KEY POINTS
This practice guideline describes the management of infants and children in PICU with severe traumatic brain injury.
All management is in conjunction with the neurosurgical team.
• Goal is to optimise cerebral perfusion (CPP) by lowering intracranial pressure (ICP) and maintaining a mean blood pressure (MBP) normal for age.
• Prevent and treat hyperthermia.
• Prevent and treat seizures.
• Avoid hypoxaemia, hypotension, hypercarbia and acidosis.
• Prevent complications such as contractures and decubitus ulcers.
• Manage associated spinal injury.
• Detect associated injuries – do a trauma call on all patients if not already done.
• Notify intensivist and neurosurgeon if GCS falls, unequal pupils, asymmetric tone, any sign of herniation, seizures, rising ICP, falling CPP.
• Manage airway and ventilation.
• Provide optimal analgesia and sedation.
• Follow escalation algorithm for refractory ICP.
Related Policies
• Intracranial Pressure Monitoring (I.C.P.) Via Rickham's Reservoir, Codman Monitor Or Lumbar Catheter: http://chw.schn.health.nsw.gov.au/o/documents/policies/procedures/2006-8077.pdf
• Intracranial Pressure Monitoring Systems in PICU: Management: http://chw.schn.health.nsw.gov.au/o/documents/policies/guidelines/2007-0004.pdf
• Guidelines for the use of pressure relief beds in PICU: http://chw.schn.health.nsw.gov.au/o/documents/policies/guidelines/2007-0023.pdf
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
This document reflects what are currently regarded as safe practice. However, as in any clinical situation there may be factors that cannot be covered by a single set of guidelines. This document does not replace the need for the application of clinical judgement to each individual presentation.
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 2 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
CHANGE SUMMARY
• Reformatting Algorithm A and B
• Update reference regarding guidelines for TBI management
• Adjustment regarding the indication of the use of hypothermia in children TBI, as directed by the current literature
• Insertion of hyperlink to related policies
READ ACKNOWLEDGEMENT
• Training/Assessment required – All PICU nursing staff undertaking “Clinical competency: Management of extra ventricular drains (EVD)”
• Read Acknowledge Only - All PICU nursing staff involved in the care of patients with severe traumatic brain injury. PICU intensivist and all other medical staff involved in the management of a patient with severe traumatic brain injury
KEY PERFORMANCE INDICATORS
• Incidence of occipital pressure sore over a 3 year period
• Time to c-spine clearance for patients with TBI over a 3 year period
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 3 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
TABLE OF CONTENTS Head Injury Treatment Goal: Algorithm A ............................................................................ 4 Head Injury Treatment Goal: Algorithm B (Equipment & Patient Check) ......................... 5 Management Goals in Severe Traumatic Brain Injury ........................................................ 6 Retrieval of Patients with Severe Traumatic Brain Injury ................................................... 6 Admission to PICU ................................................................................................................. 6 Neurological Assessment and Special Observations ........................................................ 7 When to notify Intensivist or Neurosurgeon ............................................................................................ 8 Principles of Management ..................................................................................................... 8 Airway ...................................................................................................................................................... 8 Ventilation ................................................................................................................................................ 9 Cardiovascular function ......................................................................................................................... 10 Table 1. Age related mean systemic artery pressure (modified from Shann et al. Drug doses, 12th ed, 2003)................................................................................................................................................ 10 Renal function, fluids and electrolytes ................................................................................................... 10 Positioning and pressure area care ....................................................................................................... 11 Spinal cord ............................................................................................................................................. 11 Analgesia and sedation ......................................................................................................................... 12 Thermal regulation ................................................................................................................................. 13 Seizures ................................................................................................................................................. 13 Nutrition, metabolic requirements and stress ulcer prophylaxis ............................................................ 13 Autonomic Dysfunction Syndrome ........................................................................................................ 14 General .................................................................................................................................................. 14 Management of Raised ICP or Inadequate CPP ................................................................ 15 Check the patient ................................................................................................................................... 15 Check the machinery ............................................................................................................................. 16 Recurrent ICP spikes with procedures and interventions ..................................................................... 16 Refractory Intracranial Hypertension ..................................................................................................... 16
Ensure adequate sedation and analgesia ......................................................................... 16 Neuromuscular Blockade ................................................................................................... 16 CSF Drainage .................................................................................................................... 16 Osmotic Agents ................................................................................................................. 16 Continuous CSF drainage ................................................................................................. 17 Barbiturate coma ............................................................................................................... 17 Craniectomy....................................................................................................................... 17 Hypothermia ...................................................................................................................... 17 Hyperventilation ................................................................................................................. 18
Hand Ventilation .................................................................................................................................... 18 Weaning from ICP Therapy ................................................................................................. 18 Appendix ............................................................................................................................... 19 Intracranial Pressure (ICP) .................................................................................................................... 19 Cerebral Perfusion Pressure (CPP) ...................................................................................................... 20 Table 2. Target CPP by age .................................................................................................................. 20 Herniation .............................................................................................................................................. 21 References ............................................................................................................................ 22
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 4 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
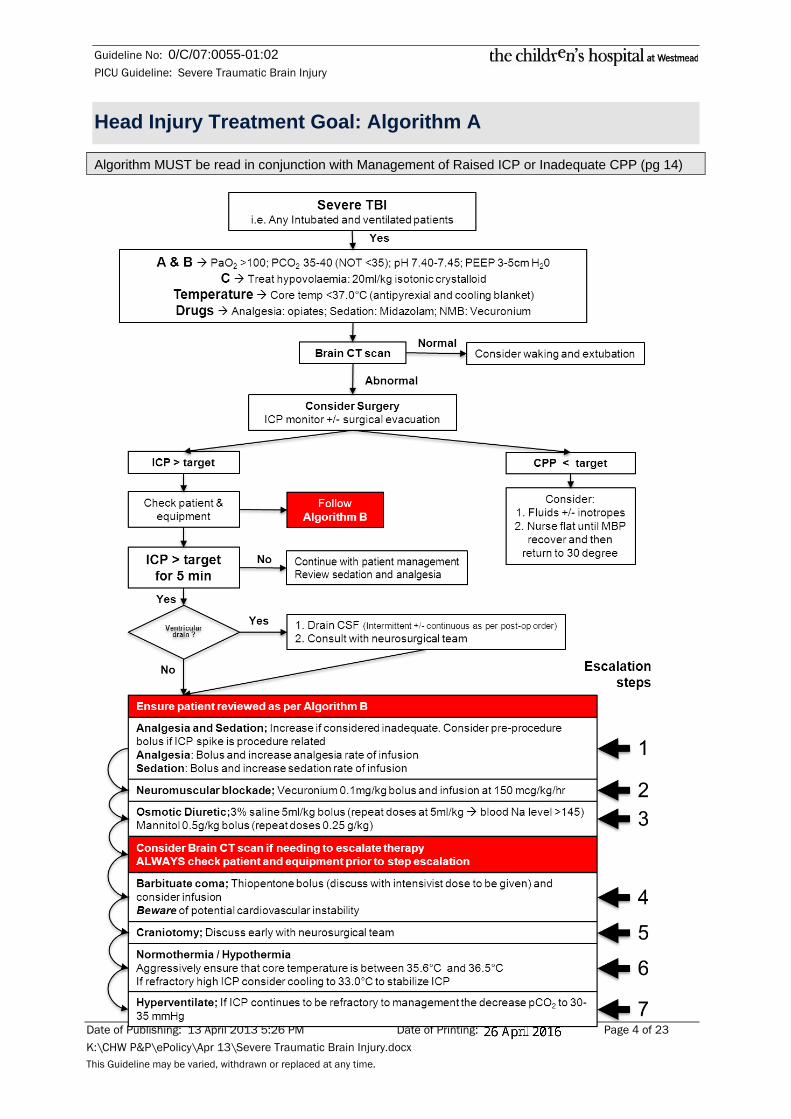
Head Injury Treatment Goal: Algorithm A
Algorithm MUST be read in conjunction with Management of Raised ICP or Inadequate CPP (pg 14)

Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 5 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Head Injury Treatment Goal: Algorithm B (Equipment & Patient Check)
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 6 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Management Goals in Severe Traumatic Brain Injury
The goals of management are:
• Maintenance of adequate cerebral perfusion with well oxygenated blood;
• Control of increased intracranial pressure (ICP) by reducing the volume of cranial vault contents;
• Early recognition of, and where possible, prevention of events known to contribute to secondary brain injury. These are:
o hypotension, hypoxaemia, hypercarbia, acidosis, hyperthermia and seizures;
• Recognition of events that may require neurosurgical intervention; and
• Prevention of other complications including musculoskeletal contractures and decubitus ulcers.
Many of the therapies used in the treatment of the patient with severe head injury are considered controversial because they have not undergone rigorous scientific evaluation. This document takes into consideration the data from recent studies, however treatment modalities may change, as new information becomes available.
Management necessitates frequent neurological assessment. Therapies used may include intubation/ventilation, sedation, analgesia, neuromuscular blockade, hyperventilation, hypothermia, osmotic diuresis, anticonvulsant and antimircobial.
Retrieval of Patients with Severe Traumatic Brain Injury
A neurosurgeon should be involved in the retrieval phone calls with NETS.
Admission to PICU
A “Trauma consult” page needs to be placed by PICU when a child with a head injury arrive directly to the PICU from other hospitals. Neurosurgeons need to be called separately.
• If the patient is stable assess for other injuries (secondary survey):
o Cervical and thoracic spine (see CHW Policy on Cervical Spinal (suspected) Injury: Patient management: http://chw.schn.health.nsw.gov.au/o/documents/policies/guidelines/2012-8014.pdf
o Chest
o Abdomen and pelvis - urine and stool for occult blood, serum amylase
o Extremities
• Facilitate imaging: note that the time to definitive care may be limited by time to perform a CT scan, it may be necessary for PICU to meet the NETS team at the CT scanner.
• Consider Tetanus toxoid/immunoglobulin if there are abrasions or open lacerations (Give if the last Tetanus immunisation was give >5 years ago)
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 7 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Neurological Assessment and Special Observations
• Perform nursing clinical assessment hourly (or more frequently if the patient is unstable) Organise nursing care to minimise stimulation. This should include:
o Glasgow Coma Scale (GCS)
o Pupils assessment - size, shape and reactivity.
o Observation and description of voluntary/involuntary movements, changes in muscle tone, tremors, seizure activity and asymmetry of movement or tone. All unusual movements should be recorded separately, including time of onset, duration, and brief description (including focality). Note: Tachycardia, hypertension and pupillary signs in patients receiving neuromuscular blockers may indicate seizure activity. These episodes should be recorded as noted above.
o Assess and record any CSF leak from ears, nose or elsewhere.
• Record CPP and ICP (if monitored) In this Intensive Care Unit, the arterial transducer (measuring MBP) is placed by having the three way tap on the transducer level with the patient’s right atrium (mid axilla at the fifth intercostal space), and the intracranial pressure transducer (measuring ICP) is placed by having the three way tap on the transducer at the level of the foramen of Monro (the level of the external auditory meatus). See separate policy “Intracranial Pressure Monitoring (I.C.P.) Via Rickham's Reservoir, Codman Monitor Or Lumbar Catheter” for zeroing and calibration of ICP monitoring devices and for a diagram of the position of the foramen of Monro.
• Ensure drain height is as prescribed by neurosurgeons (normally in cm)
• Measure and record CSF loss from external ventricular drainage devices.
• Measure and record head circumference daily for neonates and infants, or any child with large or multiple skull fractures. A rapidly increasing head circumference may be suggestive of post traumatic hydrocephalus.
• Observe for signs of autonomic dysfunction (sometimes called dysautonomia). This is most likely to occur during the recovery phase of head injury, after the cessation of neuromuscular blockade. (See Autonomic Dysfunction Syndrome, page 14)
• Assessments must be performed twice daily. Patients that are not muscle relaxed should have a thorough neurological examination performed by the medical officer.
• All patients should have the following tested:
o cough reflex;
o gag reflex;
o corneal reflexes (attention not to injury the cornea)
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 8 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
When to notify Intensivist or Neurosurgeon • Deteriorating level of consciousness as measured by GCS (decrease > 3 points or to
less than GCS 8 if not previously at this level)
• Onset of focal signs:
o pupillary inequality
o hemiparesis
• Clinical signs consistent with herniation (see Appendix, page 18)
• Clinical signs suggestive of seizure activity (see above & Seizures, page 14)
• Raised ICP or low CPP. The Intensivist in consultation with the Neurosurgeon will determine at what level the ICP or CPP should be treated, and this will be individualised for each patient. Broad guidelines for intervention are:
o Recurrent ICP spikes > 15 mmHg (with or without stimuli)
o ICP plateau waves > 20 mmHg for more than 3 minutes
o CPP < Age specific goals (see Target CPP by age in the algorithm, page 5)
In the above circumstances, an urgent cerebral CT scan should be considered after appropriate medical therapy has been initiated.
Principles of Management
Airway Most children with severe head injury will require endotracheal intubation to maintain an adequate airway and gas exchange. (See separate policy Guidelines for Intubation and the Continuing Care of the Intubated/Ventilated Patient). Intubation should be performed in any patient with a GCS of ≤ 8. Intubation should be performed following rapid sequence induction, with the patient’s head manually stabilised by a second person experienced in this technique.
Nasal endotracheal tubes (and nasogastric tubes) should not be inserted into patients with suspected base of skull fracture.
• A gastric tube should be inserted in all intubated head injury patients (see precaution in previous paragraph re nasal route).
• Neuromuscular blockers may be indicated to assist with control of raised intracranial pressure.
Neuromuscular blockers mask signs of neurological deterioration (with the exception of pupillary light response) and therefore are not usually indicated in stable patients with ICP < 20 mmHg, or in patients without intracranial pressure monitoring.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 9 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Ventilation • Ventilate to prevent hypoxia, hypercarbia and acidosis. These may all cause
vasodilatation of cerebral blood vessels and can exacerbate intracranial hypertension.
o Adjust FiO2 to maintain arterial saturation ≥ 97%.
o Commence with a PEEP of 3-5 cm H2O. This level will protect from atelectasis and does not raise ICP. If the patient has significant lung disease, the PEEP should be increased as would normally occur.
o Maintain PaCO2 in the lower end of normal range (PaCO2 35-40 mmHg is acceptable). Most evidence shows that cerebral blood flow is significantly reduced in the day after severe head injury, and that hyperventilation will further decrease cerebral blood flow and may cause cerebral ischaemia. The ROUTINE use of hyperventilation is NOT indicated, however, SHORT TERM use of hyperventilation may be necessary if there is an acute neurological deterioration when awaiting a CT scan and/or surgery (see Hand Ventilation page 19). Longer term hyperventilation (PaCO2 25-30 mmHg) may be considered if there is intracranial hypertension refractory to sedation, neuromuscular blockade, CSF drainage, osmotic diuretics and hypothermia. The decision to hyperventilate should only be made in consultation with the Intensivist and Neurosurgeon. End tidal CO2 (ETCO2) must be monitored in all patients during both mechanical and hand ventilation, and during transport to other departments. In the only prospective, randomised trial, the neurological outcome of hyperventilated patients was worse than for normoventilated patients. (Brain Trauma Foundation Taskforce; 1996)
o Endotracheal (ET) suction should be performed only when clinically necessary with attention to ICP and CPP. Airway stimulation in particular may cause intracranial hypertension. If significant elevation of ICP occurs with suctioning, pre procedure sedation should be utilised and the suction catheter should not be passed more than 0.5 cm beyond the end of the ET tube (see Analgesia and sedation, page 12). Preference to use in-line suction equipment to minimise ventilation disturbance during ETT suctioning.
Hand ventilation may be employed prior to suction, but do not lower the ETCO2 by more than 5 mmHg below the baseline.
• Physiotherapists should assess patients and plan chest physiotherapy interventions to reduce adverse effects of ventilation and muscle relaxation. These interventions should be discussed with the Intensivist and arranged by nursing staff. If a procedure causes raised ICP and decreased CPP, then extra boluses of sedation or analgesia prior to the procedure may reduce spikes (see Analgesia and sedation, page 12).
• Note that brief ICP spikes which recover to baseline quickly are acceptable and do not need treatment.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 10 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Cardiovascular function • Adequate perfusion of the brain is a priority and hypotension should be avoided
because of its adverse effects on CPP.
Data suggests that hypotension during the acute, post injury period is the most important cause of secondary brain injury and therefore should be treated aggressively.
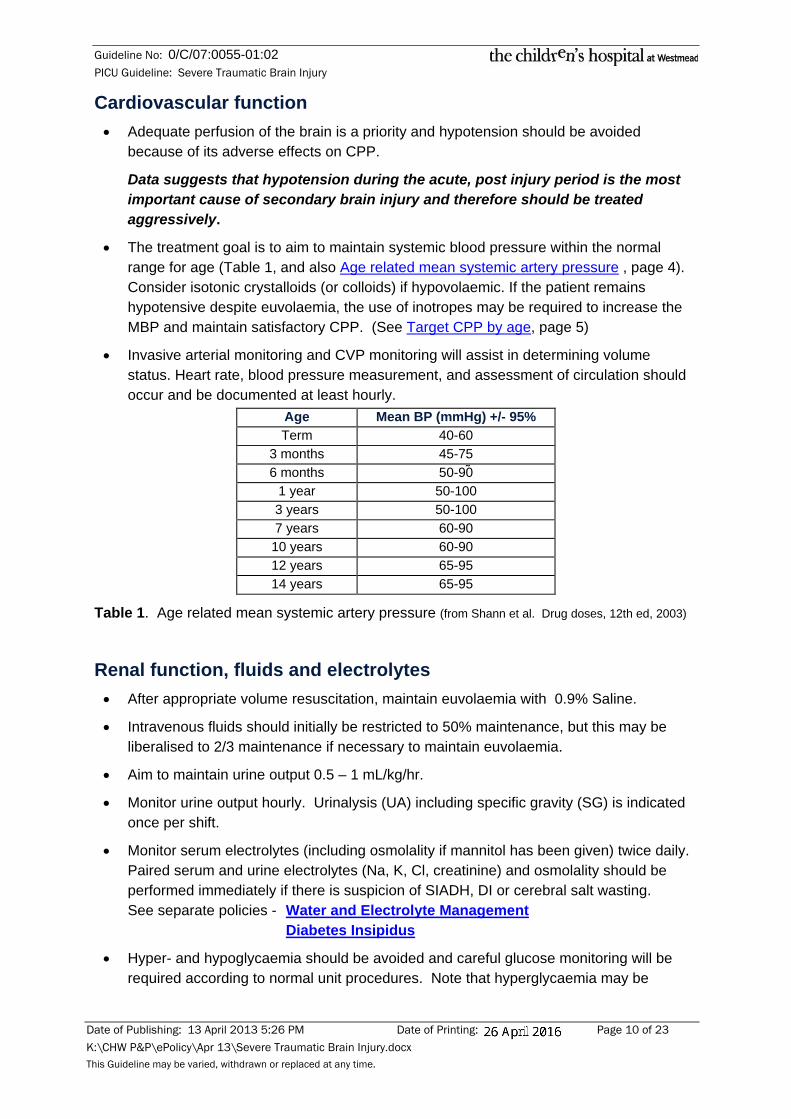
• The treatment goal is to aim to maintain systemic blood pressure within the normal range for age (Table 1, and also Age related mean systemic artery pressure , page 4). Consider isotonic crystalloids (or colloids) if hypovolaemic. If the patient remains hypotensive despite euvolaemia, the use of inotropes may be required to increase the MBP and maintain satisfactory CPP. (See Target CPP by age, page 5)
• Invasive arterial monitoring and CVP monitoring will assist in determining volume status. Heart rate, blood pressure measurement, and assessment of circulation should occur and be documented at least hourly.
Age Mean BP (mmHg) +/- 95% Term 40-60
3 months 45-75 6 months 50-90
1 year 50-100 3 years 50-100 7 years 60-90 10 years 60-90 12 years 65-95 14 years 65-95
Table 1. Age related mean systemic artery pressure (from Shann et al. Drug doses, 12th ed, 2003)
Renal function, fluids and electrolytes • After appropriate volume resuscitation, maintain euvolaemia with 0.9% Saline.
• Intravenous fluids should initially be restricted to 50% maintenance, but this may be liberalised to 2/3 maintenance if necessary to maintain euvolaemia.
• Aim to maintain urine output 0.5 – 1 mL/kg/hr.
• Monitor urine output hourly. Urinalysis (UA) including specific gravity (SG) is indicated once per shift.
• Monitor serum electrolytes (including osmolality if mannitol has been given) twice daily. Paired serum and urine electrolytes (Na, K, Cl, creatinine) and osmolality should be performed immediately if there is suspicion of SIADH, DI or cerebral salt wasting. See separate policies - Water and Electrolyte Management Diabetes Insipidus
• Hyper- and hypoglycaemia should be avoided and careful glucose monitoring will be required according to normal unit procedures. Note that hyperglycaemia may be
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 11 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
problematic if diabetes insipidus (DI) occurs, and urinary water loss is replaced with large volumes of 5% Dextrose. (See Policy on management of Diabetes Insipidus)
• Secretion of excessive antidiuretic hormone (SIADH), DI and cerebral salt wasting may be associated with severe head injury.
o SIADH can be suspected clinically by reduced urine output with high urine sodium and osmolality, in the presence of normal or increased circulating blood volume and a falling serum sodium.
o DI is clinically suspected when copious low osmolality urine output is present, the patient is volume depleted and serum sodium is rising.
o Cerebral salt wasting is characterised by a falling serum sodium, polyuria with a high urinary sodium concentration (>80 mmol/L) and hypovolaemia.
Positioning and pressure area care • Patients should be nursed supine with the trunk elevated 15 to 30°, and neutral head
alignment to optimise cerebral venous drainage. If the c-spine is not cleared then the entire bed can be placed on a 15° angle. Note that cervical collars, lateral neck rotation and the Trendelenberg position (head down) may interfere with venous drainage. The effect of head elevation on ICP, CPP and cerebral blood flow is controversial. It is likely that in the hypovolaemic patient with raised intracranial pressure, systemic blood pressure and possibly CPP will fall with head elevation. Under these circumstances, it is recommended that the patient be placed flat until cardiovascular stability is achieved. In general, at 15-30 degrees, ICP is reduced, however CPP may be unchanged, increased or decreased in recently published adult studies.
• Pressure area care (to prevent decubitus ulceration) will be required every 4 hours. The child should be turned quarter supine, side to side, maintaining neutral alignment of the head. (see CHW Policy on Cervical Spinal (suspected) Injury: Patient management) There are few if any contraindications to this degree of movement of the patient. If necessary, pre procedure sedation should be considered (see Analgesia and sedation, page 12).
• Physiotherapy should be consulted within 24 hours of admission so that treatment can be instituted for the prevention of contractures. Therapy may include splinting and/or casting.
Spinal cord Treat all head injured patients as a suspected cervical-spine fracture until proven otherwise. In children, spinal cord injury may occur without evidence of radiological abnormality (SCIWORA).
• The following radiographic evaluation of the cervical spine is indicated: o Lateral cervical spine (showing C6 <12 years old and T1 >12 years), o AP cervical spine, o CT of areas not clearly seen with the plain views is usually indicated. CT scan is
inadequate for complete evaluation of the spine, however. NB: radiation to the thyroid gland should be minimised.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 12 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
• Note that if there is good evidence to suggest a spinal cord injury, then MRI should be the evaluation of choice (discuss with radiologist before proceeding).
• Prevent rotation, extension and flexion of the neck. This is best done by immobilisation of the neck with an appropriately sized hard collar (a Aspen collar is preferred for longer term usage). Important to ensure that this collar is not too tight to impede venous drainage from the head.
• Prolonged usage of spinal collars promotes the occurrence of pressure ulceration and should be avoided if possible. If the spine has not been cleared, the spinal collar should be taken off briefly every day to allow inspection of potential pressure areas. The collar must remain in situ when routinely log rolled to minimise the risk of c-spine distortion.
• The spine should be clear in accordance with the CHW Policy on Cervical Spinal (suspected) Injury: Patient management. before permanent removal of the collar.
• The thoracolumbar spine should be examined/imaged (AP/lateral views) within 24 hours of PICU admission.
Analgesia and sedation • Adequate sedation and analgesia should be prescribed and assessed regularly in all
children. The adequacy of sedation and pain relief should be determined hourly and documented.
• Choice of analgesia and/or sedation should be individualised following consultation with the Intensivist and Neurosurgeon, however:
o Morphine is the analgesic of choice;
o Midazolam infusion is the sedative of choice and should be changed to diazepam according to PICU guidelines.
o Propofol infusion may be considered (see Protocol for Propofol use in the PICU in the sedation policy), however is expensive and should be given with caution because of the reports of sudden death with prolonged usage in children. (Kam et al 2007)
o The doses of some medications used to reduce rises in ICP are:
Morphine IV 50-100 microgram/kg/dose
Midazolam IV 50-100 microgram/kg/dose
Lignocaine ET 1 mg/kg/dose (if suctioning caused prolonged ICP spike)
CAUTION when using the following MUST review CVS stability
Thiopentone IV 0.5-1 mg/kg/dose
Propofol IV 0.5-1 mg/kg/dose
Caution: Narcotic analgesics and sedatives may mask neurological signs.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 13 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Thermal regulation • AVOID hyperthermia. Core body temperature should be kept below 37°C by the use of
antipyretics and/or a cooling blanket. Neuromuscular blockade must be implemented if shivering occurs in intubated and ventilated patients. Hyperthermia increases cerebral metabolic requirements, and potentially cerebral blood flow and ICP.
• Core body temperature may underestimate cerebral temperature by as much as 1-2°C.
• If ICP is refractory to other measures, induced hypothermia should be considered (see Management of Raised ICP or Inadequate CPP for further details, page 15). A recent publication suggests that early hyperthermia is an independent predictor for a GCS < 13 at PICU discharge.
Seizures • Seizures occur commonly after head injury. Seizure activity will increase cerebral
metabolic requirements and consequently increase both cerebral blood flow and ICP.
• Seizures should be controlled acutely with an intravenous benzodiazepine (diazepam or midazolam). Phenytoin and/or barbiturates may be considered if status epilepticus occurs.
• Prophylaxis with phenytoin should be used routinely ONLY if the patient is concurrently paralysed with neuromuscular blocking agents, has had focal signs, intracranial haemorrhage or a depressed skull fracture. In the acute phase, a midazolam infusion may be adequate seizure prophylaxis.
• If there is subtle evidence of seizure activity especially if on neuromuscular blocking agents (tachycardia, pupillary dilation or hypertension), an EEG or continuous EEG monitoring may be indicated. This should be performed after consultation with Neurology.
Published evidence suggests that phenytoin is of value in preventing early seizures in the week after injury, but is of no value in the prophylaxis of late post traumatic epilepsy.
Nutrition, metabolic requirements and stress ulcer prophylaxis • Despite decreased cerebral metabolic rate for oxygen (CMRO2) post head injury,
resting energy expenditure is significantly increased. Patients who are not on neuromuscular blockers should be provided with 140-150% of the normal resting energy expenditure. For those patients on neuromuscular blockers, intake should be 100-120% of the normal resting energy expenditure.
• All patients will initially be nil by mouth and stress ulcer prophylaxis is indicated. See relevant Guidelines for GI Prophylaxis. If there has been no significant gastrointestinal haemorrhage, ulcer prophylaxis can be ceased when enteral nutrition is well established.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 14 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
• Nasogastric or orogastric feeding can commence when the general surgical team has ruled out other injuries (particularly abdominal trauma). Gastric feeding should be attempted even in the absence of bowel sounds or passage of flatus or stool. If gastric feeding is not tolerated, a transpyloric tube should be passed.
• Consider TPN if the patient cannot be enterally fed after 48 hours.
• If the patient is constipated, consider the administration of stool softeners. This may help to prevent the Valsalva manoeuvre (which will increase ICP).
Autonomic Dysfunction Syndrome (also called Dysautonomia, Thalamic storm, or brainstem seizures)
• This syndrome is characterised by dysfunction of the autonomic nervous system and the clinical signs are usually those of excessive sympathetic activity, including hypertension, tachycardia or bradycardia, diaphoresis (sweating), piloerection (goose bumps), flushing, fever and abnormal posturing. Seizures and drug withdrawal (opiates +/- benzodiazepines) are important differential diagnoses to consider.
• Precipitating factors can include:
o full bowel/bladder
o handling/procedures
o excessive noise/light
o uncomfortable posturing
• Treatment includes avoidance of precipitating factors. Pharmacologic intervention may be required and drugs of potential value may include clonidine, sedation (diazepam and/or morphine), beta blockers, and bromocriptine. All patients with autonomic dysfunction should have their management discussed with the Rehabilitation Service.
General • The secondary survey looking for other injuries should be repeated at 24 hours, and
again prior to discharge from PICU.
• Antibiotic coverage may be indicated if there are compound fractures.
• The prophylactic use of antibiotics should be discussed with the relevant Neurosurgeon.
• Rehabilitation Consultation should occur as soon as it seems likely that the patient will survive (this may be within 24 hours of admission). Contact the Rehabilitation Registrar via switchboard.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 15 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Management of Raised ICP or Inadequate CPP
(This section describes the process of escalation of therapy and should be read in conjunction with algorithms A and B, see page 4 and 5)
It is desirable to keep ICP ≤ 15-20 mm Hg, whilst maintaining an adequate systemic blood pressure and therefore CPP. CPP in general should be maintained in the vicinity of that described in table 2. However, as noted previously the levels at which intervention will occur will be individualised for each patient. Two problems may arise that warrant intervention. They are:
1. Inadequate CPP (with or without systemic hypotension)
2. Elevated ICP
Neither should be managed in isolation, but the two considered and treated simultaneously if necessary. Systemic hypotension should be avoided if possible and treated aggressively if it occurs.
Factors that may precipitate an ICP spike include:
• hypercapnia;
• hypoxia;
• Valsalva manoeuvre;
• pain/cough/agitation;
• medical procedures;
• position (e.g. neck flexion/rotation may obstruct venous return);
• progression of neurological process (e.g. enlargement of intracranial haemorrhage, worsening cerebral oedema), and
• systemic hypotension
In any patient where there is elevated ICP or decreased CPP, the following should occur:
1. Check the patient
2. Check the machinery
Check the patient 1. Are there any new neurologic signs?
o pupillary signs - sluggish reaction or unilateral/bilateral pupillary dilation
o extensor posturing or hemiparesis
o fall in the level of consciousness
o change in vital signs – hypertension (wide pulse pressure), bradycardia and irregular respirations (Cushing’s Reflex)
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 16 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
2. What is the mean blood pressure? Is the patient hypotensive? Is the patient hypovolaemic? (what is the CVP?)
3. What are the SaO2 and ET CO2?
4. What is the patient’s position? Is the head rotated or neck flexed?
5. Is the patient adequately sedated and analgised? In urinary retention or constipated?
6. If neuromuscular blockers are being given, is the patient still muscle relaxed?
Check the machinery • Is the ventilator working correctly? Low SaO2 and/or elevated ET CO2 may indicate a
problem with ventilation.
• Are all the transducers levelled and appropriately calibrated?
Recurrent ICP spikes with procedures and interventions Airway stimulation in particular may cause elevations in ICP. These spikes can be reduced by bolus doses of sedation or analgesia prior to the procedures (see Analgesia and sedation, page 12).
Refractory Intracranial Hypertension If ICP becomes refractory to usual measures, then the following therapies should be added in stepwise fashion.
• Ensure normocarbia (35-40 mm Hg)
Ensure adequate sedation and analgesia As noted, this may include pre procedure sedation.
Neuromuscular Blockade If not already muscle relaxed, commence intermittent vecuronium. If this is inadequate, then a continuous infusion of vecuronium may be considered.
Remember: neuromuscular blockade obscures neurological signs.
CSF Drainage CSF can be drained if a ventricular catheter (external ventricular drain or EVD) is in situ. This may be performed intermittently for 5 mins for ICP spikes greater than the target. This is probably the quickest way to achieve control of ICP.
Osmotic Agents There is some evidence to support the use of hypertonic saline to treat increased ICP, however there is limited paediatric experience. There is poor evidence to support the use of mannitol in children, however there is extensive paediatric experience, combined with good evidence of efficacy in adults.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 17 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
3% (Hypertonic) Saline: For acute deteriorations a bolus of 3mL/kg may be administered (may consider up to 5mL/kg if serum sodium low <135 mmo/L, signs of seizure or herniation). Hypertonic saline raises serum osmolality and depletes fluid from intracellular and interstitial spaces. Serum sodium levels will increase, and in one study NO patient with a serum sodium level >180 mmol/L had a good outcome. Serum sodium should be kept BELOW 160 mmo/L.
Mannitol: Mannitol (0.25-0.5 g/kg), can be given for acute deteriorations. If mannitol has not been given previously, give 0.5 g/kg; for repeat doses administer 0.25-0.5 g/kg. Mannitol raises serum osmolality and depletes fluid from intracellular and interstitial spaces. If repeated doses are prescribed, serum osmolality should be monitored to prevent complications such as rebound intracranial hypertension and acute renal failure and should be maintained in the range of 310-320 mOsm/L.
Serum osmolality can be estimated from the following formula:
• Estimated osmolality = 2 x (serum Na) + BSL + urea
This formula can be used when hypertonic saline has been administered, but will be lower than the measured osmolality if mannitol has been used (so called osmolar gap).
Continuous CSF drainage Check ICP by turning the tap off to the drain and on to the transducer every 30 min.
Barbiturate coma Thiopentone coma may be induced to decrease cerebral metabolism and decrease ICP.
Consider an intravenous bolus of 3-5 mg/kg (dependent on cardiovascular stability), and then infuse at a rate 1-2mg/kg/hr. Ideally, this should occur under continuous EEG monitoring with a goal of achieving burst-suppression. If continuous monitoring is unavailable, then an EEG should be performed within 24-48 hours of commencement (if infusion still present).
Barbiturates commonly cause myocardial depression and peripheral vasodilatation, and therefore inotropic support may be required during thiopentone infusion to maintain an adequate blood pressure and CPP. Invasive monitoring (arterial line and central venous pressure) is indicated. Thiopentone levels should be monitored (discuss with Biochemistry).
There is reasonable evidence that barbiturates reduce ICP, but there is less evidence to suggest that outcome is improved.
Craniectomy Discussion with the neurosurgical team should occur as soon as possible as they may need to discuss the possibility to perform a bifrontal decompressive craniectomy.
From the adult literature (DECRA study) there is evidence that a bifrontal decompressive cranieotomy decreased ICP and ICU length of stay but it was associated with more unfavourable outcomes.
Hypothermia Core body temperature should be kept below 37°C in all patients by the use of antipyretics and/or a cooling blanket (see Thermal regulation, page 13). If ICP remains elevated despite medical interventions then cool to 33-35°C.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 18 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
The role of Hypothermia in TBI has been reviewed in paediatric studies. To date the evidence suggests that it does help in reducing ICP but does not help to improve long term neurological outcome (HiTBIC and CoolKids papers in press).
Hyperventilation If ICP is poorly controlled, modest hyperventilation should be considered after consultation with the Intensivist and Neurosurgeon. PaCO2 should be lowered to the low 30’s, using ETCO2 and arterial blood gas monitoring. Note that PaCO2 < 30 mmHg has been associated with worst neurological outcomes.
Hand Ventilation • Hand ventilation for raised ICP is intended to increase minute ventilation via an increase
in tidal volume and/or an increase in rate. The subsequent drop in CO2 will induce cerebral vasoconstriction, leading to a reduction in ICP. A sharp decrease in PaCO2 may cause excessive cerebral vasoconstriction, which may worsen perfusion to marginal areas.
• Hand ventilation should occur ONLY when there is a corresponding and critical fall in the CPP. The appropriate CPP will be determined on an individual basis.
• ETCO2 monitoring must be left in place during hand ventilation and the person delivering ventilation must attempt to control the delivery of ventilation so that CO2 is reduced to an appropriate level, usually to a measurement of 5 mmHg less than had been achieved via the mechanical ventilator at the time when the patient’s ICP became elevated.
• It is desirable to maintain adequate CPP during hand ventilation.
Weaning from ICP Therapy
Once stability of ICP has been maintained for 24-48 hours, therapies can be gradually withdrawn in the reverse manner to which they were commenced. The order of weaning is usually:
• Normalise PaCO2
• If Hypothermia has been used then increase temp by NOT FASTER than 1°C every 4 hours. If the ICP increases then the patient should be re-cooled to the preceding temp.
• Cease paralysis (note that normalisation of PaCO2 should always occur before cessation of paralysis, as a rebound increase in cerebral blood flow and hence ICP may occur)
• Reduce sedation
• Remove ICP monitor
• Extubate
At each level of weaning, ICP and clinical signs should be carefully monitored for signs of rebound for a minimum of 4 hours before proceeding to the next step.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 19 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Appendix
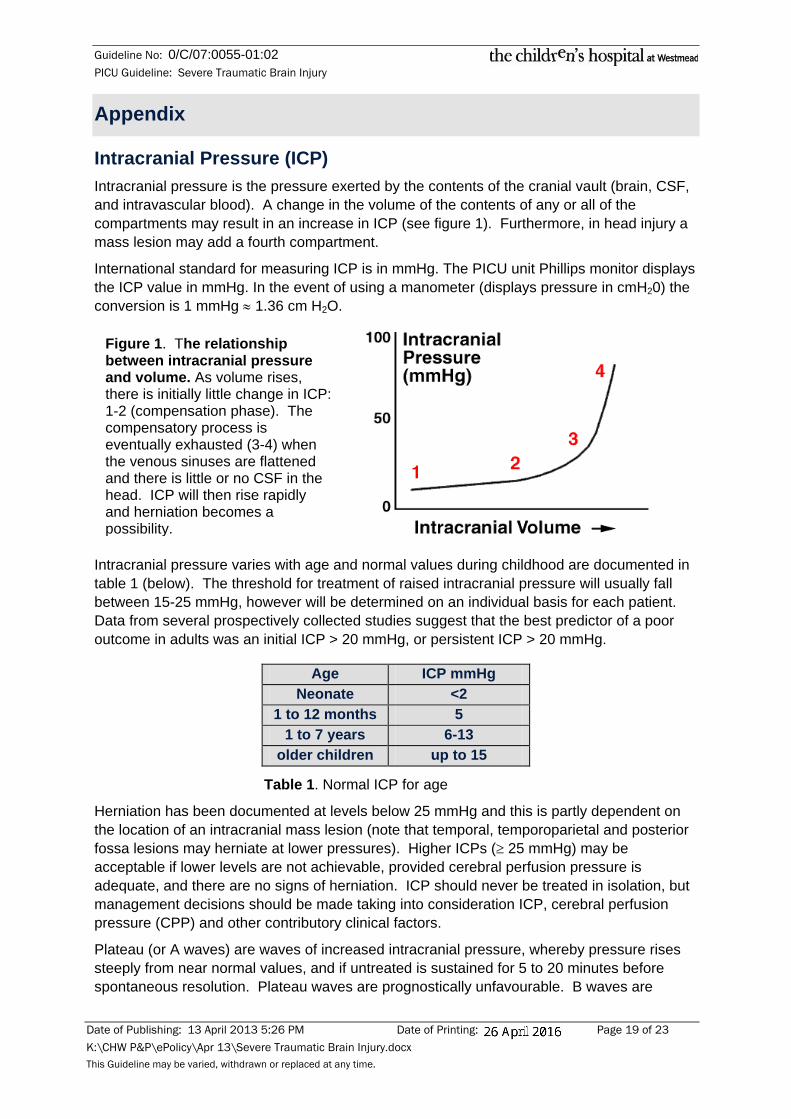
Intracranial Pressure (ICP) Intracranial pressure is the pressure exerted by the contents of the cranial vault (brain, CSF, and intravascular blood). A change in the volume of the contents of any or all of the compartments may result in an increase in ICP (see figure 1). Furthermore, in head injury a mass lesion may add a fourth compartment.
International standard for measuring ICP is in mmHg. The PICU unit Phillips monitor displays the ICP value in mmHg. In the event of using a manometer (displays pressure in cmH20) the conversion is 1 mmHg ≈ 1.36 cm H2O.
Intracranial pressure varies with age and normal values during childhood are documented in table 1 (below). The threshold for treatment of raised intracranial pressure will usually fall between 15-25 mmHg, however will be determined on an individual basis for each patient. Data from several prospectively collected studies suggest that the best predictor of a poor outcome in adults was an initial ICP > 20 mmHg, or persistent ICP > 20 mmHg.
Age ICP mmHg Neonate <2
1 to 12 months 5 1 to 7 years 6-13
older children up to 15
Table 1. Normal ICP for age
Herniation has been documented at levels below 25 mmHg and this is partly dependent on the location of an intracranial mass lesion (note that temporal, temporoparietal and posterior fossa lesions may herniate at lower pressures). Higher ICPs (≥ 25 mmHg) may be acceptable if lower levels are not achievable, provided cerebral perfusion pressure is adequate, and there are no signs of herniation. ICP should never be treated in isolation, but management decisions should be made taking into consideration ICP, cerebral perfusion pressure (CPP) and other contributory clinical factors.
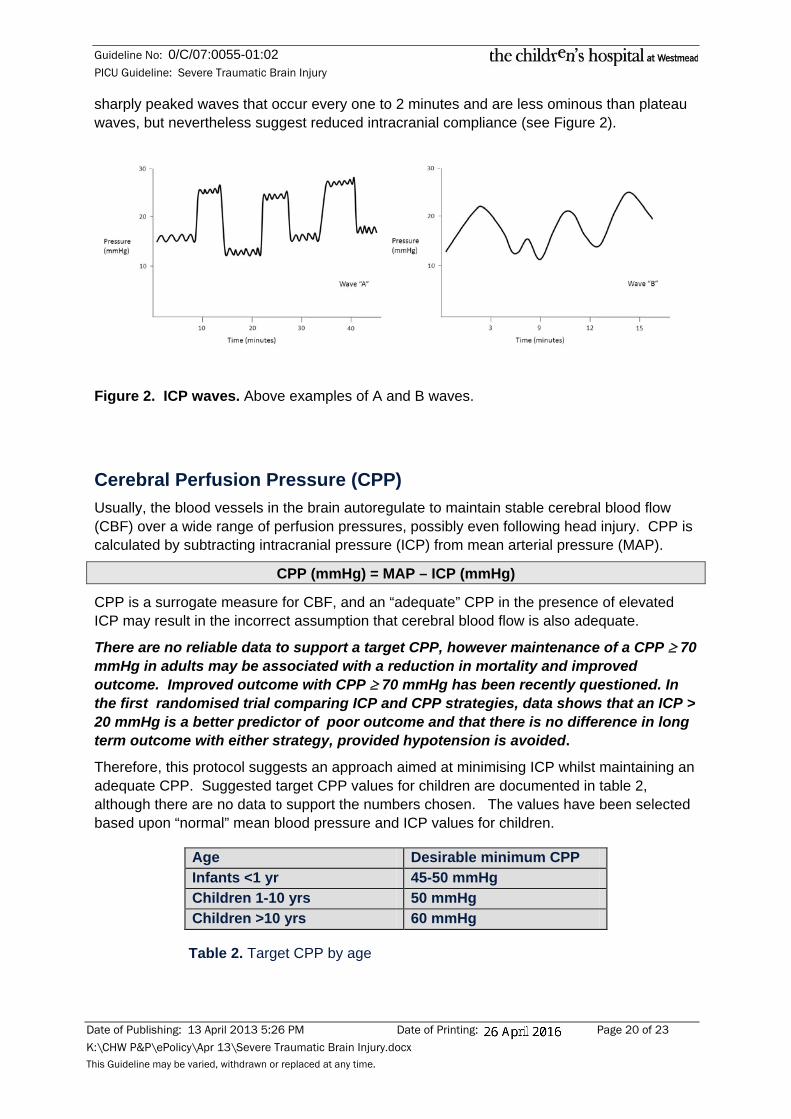
Plateau (or A waves) are waves of increased intracranial pressure, whereby pressure rises steeply from near normal values, and if untreated is sustained for 5 to 20 minutes before spontaneous resolution. Plateau waves are prognostically unfavourable. B waves are
Figure 1. The relationship between intracranial pressure and volume. As volume rises, there is initially little change in ICP: 1-2 (compensation phase). The compensatory process is eventually exhausted (3-4) when the venous sinuses are flattened and there is little or no CSF in the head. ICP will then rise rapidly and herniation becomes a possibility.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 20 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
sharply peaked waves that occur every one to 2 minutes and are less ominous than plateau waves, but nevertheless suggest reduced intracranial compliance (see Figure 2).
Figure 2. ICP waves. Above examples of A and B waves.
Cerebral Perfusion Pressure (CPP) Usually, the blood vessels in the brain autoregulate to maintain stable cerebral blood flow (CBF) over a wide range of perfusion pressures, possibly even following head injury. CPP is calculated by subtracting intracranial pressure (ICP) from mean arterial pressure (MAP).
CPP (mmHg) = MAP – ICP (mmHg)
CPP is a surrogate measure for CBF, and an “adequate” CPP in the presence of elevated ICP may result in the incorrect assumption that cerebral blood flow is also adequate.
There are no reliable data to support a target CPP, however maintenance of a CPP ≥ 70 mmHg in adults may be associated with a reduction in mortality and improved outcome. Improved outcome with CPP ≥ 70 mmHg has been recently questioned. In the first randomised trial comparing ICP and CPP strategies, data shows that an ICP > 20 mmHg is a better predictor of poor outcome and that there is no difference in long term outcome with either strategy, provided hypotension is avoided.
Therefore, this protocol suggests an approach aimed at minimising ICP whilst maintaining an adequate CPP. Suggested target CPP values for children are documented in table 2, although there are no data to support the numbers chosen. The values have been selected based upon “normal” mean blood pressure and ICP values for children.
Age Desirable minimum CPP Infants <1 yr 45-50 mmHg Children 1-10 yrs 50 mmHg Children >10 yrs 60 mmHg
Table 2. Target CPP by age
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 21 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Herniation Herniation occurs when intracranial pressure rises sufficiently to force the cranial contents across compartments (either dural compartments or the foramen magnum)
This is a medical/surgical emergency and death will occur rapidly (a mechanically ventilated patient will progress to brain death) if herniation cannot be promptly reversed.
Some signs suggestive of raised intracranial pressure and impending herniation are:
• fall in the level of consciousness
• extensor posturing or hemiparesis
• change in vital signs – hypertension, bradycardia and irregular respirations (Cushing’s Reflex)
• pupillary signs - sluggish reaction or unilateral/bilateral pupillary dilation
In general, the younger the child, the more non-specific the clinical signs of elevated ICP may be (due to CNS immaturity and greater reflex activity).
Several sites/types of herniation are described. The two most important are uncal and central (transtentorial) herniation. They may also occur together.
1. Uncal (temporal) herniation. Pure uncal herniation is caused by a unilateral hemispheric mass lesion often within or adjacent to the temporal lobe. The medial portion of the temporal lobe (the uncus) is forced medially and downward over the tentorium. There is ipsilateral pupillary dilation because of compression of the parasympathetic fibres travelling with the 3rd cranial n. As noted, supratentorial lesions on one side may initially result in uncal herniation. Central herniation occurs as a consequence of a more generalised supratentorial process, however, as ICP increases further, uncal herniation can progress to bilateral transtentorial temporal lobe herniation. The terms central transtentorial herniation, cranial-caudal transtentorial herniation, or rostro-caudal transtentorial herniation more accurately describe what is generally meant by "transtentorial herniation".
2. Cingulate (subfalcine) hernitation. A unilateral supratentorial mass or haemorrhage results in a midline shift. If the pressure pushing the brain to one side is great enough, one of the hemispheres is pushed under the falx (subfalcine).
3. Cerebellar (tonsillar) herniation. A mass effect in the posterior fossa causes the cerebellar tonsils to herniate inferiorly through the foramen magnum compressing the medulla and upper cervical spinal cord. Conscious patients complain of neck pain and vomiting. They may have nystagmus, pupillary dilatation, bradycardia, hypertension and respiratory depression. Early tonsillar herniation is difficult to recognise in an unconscious patient.
4. Transcalvarial (traumatic or post operative) herniation. Cerebral oedema or a mass effect may cause herniation at the site of a fracture or through a craniectomy.
5. Ascending transtentorial herniation (superior vermian herniation). This involves upward herniation of the vermis and cerebellar hemispheres through the tentorial incisura due to a mass effect in the posterior fossa.
Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 22 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
References
1. Journal of Neurotrauma 1996 13 (11) Note that this issue of the journal is dedicated to evidence based management of severe head injury (Brain Trauma Foundation Taskforce)
2. Brain Trauma Foundation Taskforce. Guidelines for cerebral perfusion pressure. Journal of Neurotrauma 1996 13 (11) 693-7
3. Brain Trauma Foundation Taskforce. The use of hyperventilation in the acute management of severe traumatic brain injury. Journal of Neurotrauma 1996 13 (11) 699-703
4. Newton RW. Intracranial pressure and its monitoring in childhood: a review. J. Royal Soc. Med. 1987; 80566-70
5. Rumana CS, Gopinath SP. Uzura M et al. Brain temperature exceeds systemic temperature in head-injured patients. Crit Care Med. 1998; 26:562-7.
6. Lang EW, Chestnut R. Intracranial pressure and cerebral perfusion pressure in severe head injury. New Horizons 1995 3: 400-409
7. Juul N, Morris GF, Marshall SB, Marshall LF. Intracranial hypertension and cerebral perfusion pressure: influence on neurological deterioration and outcome in severe head injury. The Executive Committee of the International Selfotel Trial. Neurosurg 2000 Jan;92 (1):1-6
8. Rosner M.Cerebral perfusion pressure: management protocol and clinical results. J Neurosurg. 1995 Dec;83(6):949-62
9. Robertson CS, Valadka AB, Hannay HJ, Contant CF, Gopinath SP, Cormio M, Uzura M, Grossman RG. Prevention of secondary ischemic insults after severe head injury. Crit Care Med. 1999 27(10):2086-95.
10. Marion DW, Firlik A, McLaughlin MR. Rosner MJ, Rosner SD, Johnson AH. Hyperventilation therapy for severe traumatic brain injury. New Horizons 1995 3: 439-447
11. Marion DW, Penrod LE, Kelsey SF, Obrist WD, Kochanek PM, Palmer AM, Wisniewski SR, DeKosky ST. Treatment of traumatic brain injury with moderate hypothermia. N Eng. J. Med 1997;336: 540-6
12. Natale JE, Joseph JG, Helfaer MA, Shaffner DH. Early hyperthermia after traumatic brain injury in children: risk factors, influence on length of stay, and effect on short term neurologic status. Crit Care Med 2000; 28:2608-15.
13. Meixensberger J, Baunach S, Amscher J et al. Influence of body position on tissue-pO2, cerebral perfusion pressure and intracranial pressure in patients with acute brain injury. Neurological Research. 1997; 19: 249-53
14. Feldman Z, Kanter MJ, Robertson CS et al. Effect of head elevation on intracranial pressure, cerebral perfusion pressure, and cerebral blood flow in head-injured patients. J. of Neurosurgery 1992; 76: 207-11.
15. Schierhout G. Roberts I. Prophylactic antiepileptic agents after head injury: a systematic review.Journal of Neurology, Neurosurgery & Psychiatry. 1998;64:108-12.
16. Sullivan T, Conine TA, Goodman M. Serial casting to prevent equinus in acute traumatic head injury. Physiotherapy 1988;40,6:346.
17. Yarkony GM, Sahgal V. Contractures. A major complication of craniocerebral trauma. Clin. Orthopaedics & Related Research. 1987; 219:93-96.
18. Brimioulle S, Moraine J, Norrenberg, Kahn RJ. Effects of positioning and exercise on intracranial pressure in the neurosurgical intensive care unit. Physical Therapy 1997;77:1682-689.
19. McGuire G, Crossley D, Richards J, Wong D. Effects of varying levels of positive end-expiratory pressure on intracranial pressure and cerebral perfusion pressure. Crit Care Med 1997;25:1059-62
20. Clifton Gl, Miller ER, Choi SC, Levin HS, McCauley S et al. Lack of effect of induction of hypothermia after acute brain injury. N. Engl J. Med 2001; 344:556-63
21. Taylor A, Butt W, Rosenfeld J, Shann F, Ditchfield M, et al. A randomized trial of very early decompressive craniectomy in children with traumatic brain injury and sustained intracranial hypertension. Childs Nerv. Syst 2001; 17(3): 154-62
22. Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, et al Decompressive Craniectomy in Diffuse Traumatic Brain Injury, N. Engl. J. Med. 2011; 364:1493-1502
23. Kam PC, Cardone D. Propofol infusion syndrome. Review. Anaesthesia. 2007 Jul;62(7):690-701.

Guideline No: 0/C/07:0055-01:02 PICU Guideline: Severe Traumatic Brain Injury
Date of Publishing: 13 April 2013 5:26 PM Date of Printing: Page 23 of 23 K:\CHW P&P\ePolicy\Apr 13\Severe Traumatic Brain Injury.docx This Guideline may be varied, withdrawn or replaced at any time.
Prepared by David Schell
Revised by Elena Cavazzoni
Revised date 1st December 2012
Copyright notice and disclaimer:
The use of this document outside Sydney Children's Hospitals Network (SCHN), or its reproduction in whole or in part, is subject to acknowledgement that it is a policy of SCHN. SCHN has done everything practicable to make this document accurate, up-to-date and in accordance with accepted standards & legislation at the date of publication. SCHN is not responsible for consequences arising from the use of this document outside SCHN. A current version of this document is only available electronically from the Hospitals. If this document is printed, it is only valid to the date of printing.