sha implementation louise ogilvie director health resources information
TRANSCRIPT

SHA Implementation
Louise Ogilvie
Director
Health Resources Information

CANADIAN HEALTH ACCOUNTS HISTORY
First systematic compilation by Health Canada in 1963.
Expenditures on personal health care by private and public sector, from 1953 to 1961.
Five categories: hospitals, prescribed drugs, physicians, dentists and other professionals.

CANADIAN HEALTH ACCOUNTS HISTORY
Health Canada maintained the National Health Accounts until 1995 when they were transferred to the new Canadian Institute for Health Information (CIHI).
CIHI was established in 1994 “To serve as the national mechanism to coordinate the development and maintenance of a comprehensive and integrated health information system in Canada”.
CANADIAN HEALTH ACCOUNTS
Reflect the structure of the Canadian Health Care System within its constitutional framework

CANADIAN HEALTH ACCOUNTS
PROVINCIAL/TERRITORIAL GOVERNMENTS
Have primary responsibility in the health care area.
FEDERAL GOVERNMENT
National conditions/criteria Fiscal Powers (Tax and Spending) Direct responsibility for certain groups (Indians, Veterans, RCMP, Armed Forces, federal inmates).

CANADIAN HEALTH ACCOUNTS
Historical series 1953–2003 Financial data
– 5 sources of finance (sectors) – 42 uses of funds (categories)
Actual/estimates/forecasts

CANADIAN HEALTH ACCOUNTSSources of Finance
Non-Consumption
Commercial Insurance Firms
Not-for-Profit Insurance Firms
TOTALHealth
Expenditures
Provincial Government Sector
Other Public Sector
Federal Direct Sector
Muncipal Government Sector
Social Security Funds
PUBLIC SECTOR
PRIVATE SECTOR Out-of-Pocket
Private Health Insurance
Workers' Compensation Boards
Quebec, Drug Insurance Fund

CANADIAN HEALTH ACCOUNTSTotal Health Expenditure by Use of Funds, 1999
Capital3.5%
Public Health & Admin 5.7%
Other Health Spending 8.6%
Other Institutions 9.5% Other Professionals
12.1%
Physicians 13.6%
Drugs 15.0%
Hospitals32.0%

CANADIAN HEALTH ACCOUNTS MAPPING TO ICHA-HF
Public Sector Good correspondence between the Canadian classification of sources of finance and the ICHA-HF.
Private Sector Direct correspondence only for out-of-pocket expenditure.
No ICHA-HF category clearly corresponds to “non-consumption”.

CANADIAN HEALTH ACCOUNTS MAPPING TO ICHA-HF: Public Sector
Canadian Health Accounts ICHA-HF Public Sector HF.1 General government Public sector less Social Security Funds
HF.1.1 General government excluding social security funds
Federal Direct Sector HF.1.1.1 Central government Provincial Government Sector HF.1.1.2 State/provincial government Municipal Government Sector HF.1.1.3 Local/municipal government Social Security Funds HF.1.2 Social security funds
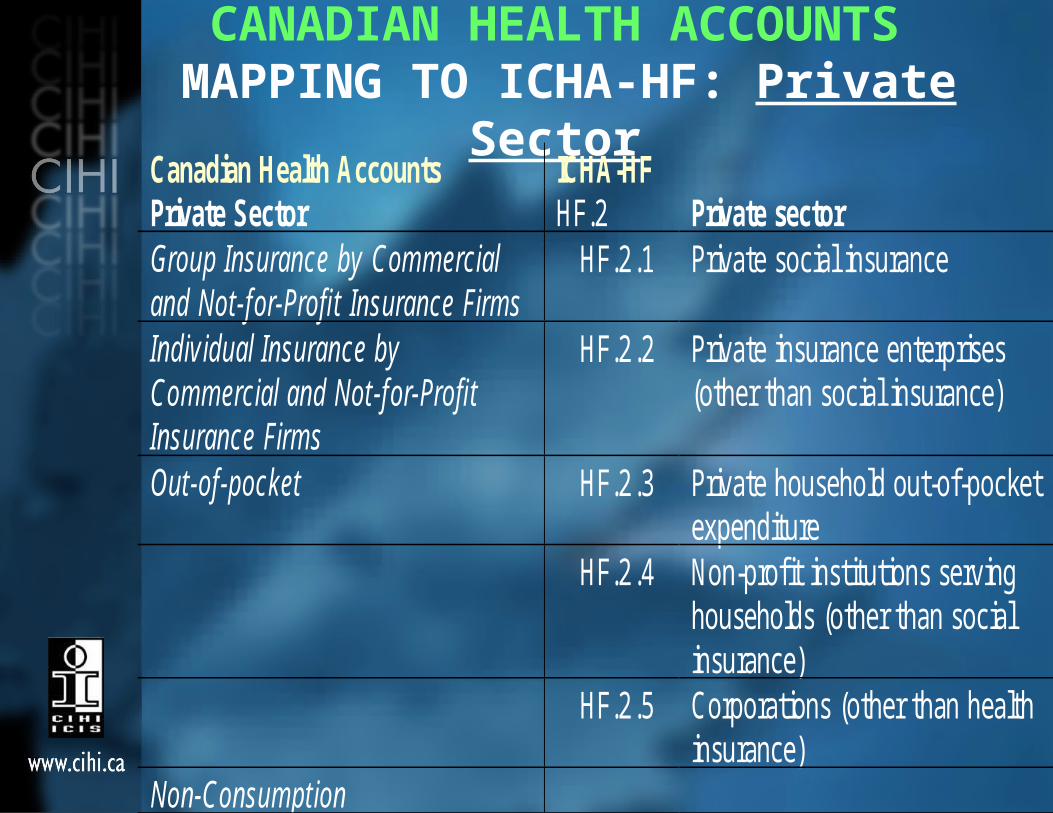
CANADIAN HEALTH ACCOUNTS MAPPING TO ICHA-HF: Private Sector
Canadian Health Accounts ICHA-HF Private Sector HF.2 Private sector Group Insurance by Commercial and Not-for-Profit Insurance Firms
HF.2.1 Private social insurance
Individual Insurance by Commercial and Not-for-Profit Insurance Firms
HF.2.2 Private insurance enterprises (other than social insurance)
Out-of-pocket HF.2.3 Private household out-of-pocket expenditure
HF.2.4 Non-profit institutions serving households (other than social insurance)
HF.2.5 Corporations (other than health insurance)
Non-Consumption

Total Health Expenditure by Source of Finance, (SHA), Canada,1999
State/provincial governments 65.2%
Local/municipal governments 0.7%
Private social insurance 10.2%
Social security funds
1.3%
Private household out-of-pocket
16.4%
Central
government
3.0%Non-
consumption
2.1%

CANADIAN HEALTH ACCOUNTS MAPPING TO ICHA-HC
Eight Broad Uses of Funds Were Mapped to ICHA-HC
Uses of Funds in Canadian Health Accounts
ICHA-HC
Hospitals 17 categories
Other Institutions 2 categories
Physicians 7 categories
Other Professionals 3 categories
Drugs 3 categories
Capital 1 category
Public Health and Administration
1 category
Other Health Spending 9 categories

CANADIAN HEALTH ACCOUNTS Hospitals: MAPPING TO ICHA-HC
Use of Funds in Canadian Health Accounts
ICHA-HC
Hospitals Canadian hospitals report their expenditures to CIHI according to the Guidelines for Management Information Systems in Canadian Health Service Organizations (MIS Guidelines). A mapping from the MIS accounts to the functional classification was prepared as shown in sub-chapter 4 of ROOM DOCUMENT 2/ANNEX.
HC.1.1 In-patient curative care HC.1.2 Day cases of curative care HC.1.3 Out-patient curative care HC.1.4 Services of curative home care HC.2.1 In-patient rehabilitative care HC.2.2 Day cases of rehabilitative care HC.2.3 Out-patient rehabilitative care HC.3.1 In-patient long-term nursing care HC.4.1 Clinical laboratory HC.4.2 Diagnostic imaging HC.4.3 Patient transport and emergency rescue HC.5.2 Therapeutic appliances and other medical durables HC.6.4 Prevention of non-communicable diseases HC.R.2 Education and training of health personnel HC.R.3 Research and development in health HC.R.4 Food, hygiene and drinking water control HC.R.5 Environmental Health

CANADIAN HEALTH ACCOUNTS Other Institutions: MAPPING TO ICHA-HC
Use of Funds in Canadian Health Accounts
ICHA-HC
Other Institutions
HC.1.1 In-patient curative care HC.3.1 In-patient long-term nursing care
Type I and lower care was excluded. Expenditures for Type II and Type III care were put under HC.3.1. Expenditures for care above Type III were put under HC.1.1

CANADIAN HEALTH ACCOUNTS Physicians: MAPPING TO ICHA-HC
Use of Funds in Canadian Health Accounts
ICHA-HC
Physicians
HC.1.1 In-patient curative care HC.1.2 Day cases of curative care HC.1.3 Out-patient curative care HC.1.4 Services of curative home care HC.3.1 In-patient long-term nursing care HC.4.1 Clinical laboratory HC.4.2 Diagnostic imaging
The National Physician Database at CIHI contains fee-for-service payments by provincial medical care plans, grouped by type of service according to the National Grouping System (NGS). A mapping from the NGS to the functional classification was prepared as shown in sub-chapter 4 of ROOM DOCUMENT 2/ANNEX.
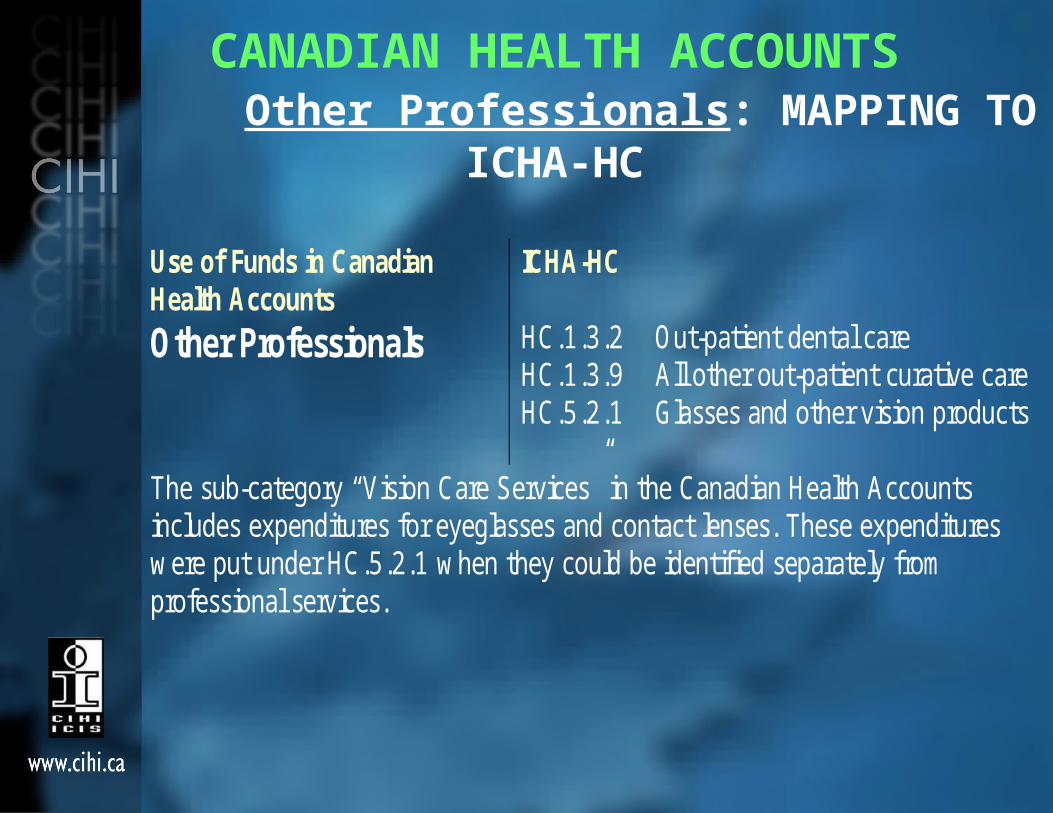
CANADIAN HEALTH ACCOUNTS Other Professionals: MAPPING TO ICHA-HC
Use of Funds in Canadian Health Accounts
ICHA-HC
Other Professionals
HC.1.3.2 Out-patient dental care HC.1.3.9 All other out-patient curative care HC.5.2.1 Glasses and other vision products
The sub-category “Vision Care Services” in the Canadian Health Accounts includes expenditures for eyeglasses and contact lenses. These expenditures were put under HC.5.2.1 when they could be identified separately from professional services.

CANADIAN HEALTH ACCOUNTS Drugs, Capital, Public Health and
Administration: MAPPING TO ICHA-HCUses of Funds in Canadian Health Accounts
ICHA-HC
Drugs HC.5.1.1 Prescribed medicines HC.5.1.2 Over-the-counter medicines HC.5.1.3 Other medical durables
Capital HC.R.1 Capital formation of health care provider institutions
Public Health and Administration
HC.6 Prevention and public health services
Other Health Spending
HC.3.3 Long-term nursing care: home care HC.4.3 Patient transport and emergency rescue HC.5.2 Therapeutic appliances and other medical durables HC.5.2.3 Hearing aids HC.6 Prevention and public heath HC.6.5 Occupational heath care HC.7 Health administration and health insurance HC.R.2 Education and training of health personnel HC.R.3 Research and development in health Undistributed

Current Health Expenditure, by Major Functional Category, (SHA),
Canada,1999
Undistributed0.9%
Health adm. & insurance2.0%
Prevention& public health 6.7%
Medical goods dispensed to out-patients 18.7%
Ancillary Services 8.6%Long-term nursing care 14.2%
Curative/rehabilitative care48.9%

Uses of Funds in Canadian Health Accounts Broken Down by Mode of
Production
Uses of Funds in Canadian Health Accounts
IHCA-Modes of Production
Hospitals In-patient care Services of day care Out-patient care
Home care Other Institutions In-patient care Physicians In-patient care
Services of day care Out-patient care
Home care Other Professionals Out-patient care Other Health Spending Home care

Current Health Expenditure, by Mode of Production, (SHA),
Canada,1999
Out-patient care26.2%
In-patient care32.0%
Not applicable (ancillary services, medical goods, prevention & public health, health adm. & insurance) 36.0%
(
Home care 2.1%
Day care2.9%
Undistributed 0.9%

CANADIAN HEALTH ACCOUNTS Institutions and Professional Services:
MAPPING TO ICHA-HP
Uses of Funds in Canadian Health Accounts
IHCA-HP
Hospitals HP.1 Hospitals
Other Institutions HP.2 Nursing and residential care facilities
Physicians HP.1 Hospitals HP.3.1 Offices of physicians HP.3.5 Medical and diagnostic laboratories HP.7.9 All other industries as secondary producer of health care
Other Professionals HP.3.2 Offices of dentists HP.3.3 Offices of other health practitioners HP.4.2 Retail sale and other suppliers of optical glasses and other vision products

CANADIAN HEALTH ACCOUNTS Drugs, Public Health/Admin, Other Health
Spending: MAPPING TO ICHA-HPUses of Funds in Canadian Health Accounts
IHCA-HP
Drugs HP.4.1 Dispensing chemists
Public Health and Administration
HP.5 Provision and admin. of public health programs
Other Health Spending HP.3.6 Providers of home health care services HP.3.9 All other providers of ambulatory health care HP.4.3 Retail sale and other suppliers of hearing aids HP.4.4 Retail sale and suppliers of medical appliances HP.5 Provision and admin. of public health programs HP.6.1 Government administration of health HP.6.3 Other social insurance HP.6.4 Other (private) insurance HP.7.1 Establishments as providers of occupational health care services

Current Health Expenditure, by Major Types of Providers, (SHA),
Canada,1999
Nursing and residential care facilities10.0%
Hospitals35.6%
Undistributed 0.9%
(
Providers of ambulatory health care26.4%
Provision and adm. of public health programmes6.2%
Retail sale and other providers of medical goods 18.7%
All other industries 0.3%
Gen. Health adm.
2.0%
What went well…Good correspondence between the Canadian classification of sources of finance for the public sector and the ICHA-HF.
Private insurance group plans meet the definition of HF.2.1 private social insurance.
Expenditures on drugs and capital could be directly mapped to the ICHA-HC.

What went well (cont’d)…About two thirds of hospital operating expenses could be directly allocated to as much as seventeen ICHA-HC categories.
Fee-for-service payments of physicians in private practice were allocated to seven ICHA-HC categories.
Good correspondence between some uses of funds and the ICHA-HP (e.g. Hospitals, Other Institutions, Other professionals).

Conclusions SHA implementation resulted in 3% reduction of
THE relative to Canadian Accounts. Furthermore, there are boundary differences
between the Canadian Accounts and the SHA. Examples include: Imports and exports are treated differently in
the Canadian Accounts and the SHA Auto Insurance is not included Canadian
Acc’ts. Non-medical care in residential facilities is
included in the SHA, not in Canadian Acc’ts. Alcohol-Drug Addiction facilities is included in
Canadian Acc’ts, not in SHA. No equivalent to Non-Consumption in the SHA.

Conclusions (cont’d) Limitations to extent that most Uses
of Funds in the Canadian Accounts could be mapped to ICHA-HC
The ICHA-HP is inconsistent with the way health care is financed in Canada.
The ICHA-HP is inconsistent with the way provider incomes are reported in Canada.