siblings and peers: making your life a misery? the ... · siblings and peers: making your life a...
TRANSCRIPT

Siblings and Peers: Making Your Life a Misery?
Dieter Wolke
Professor, Ph.D. Dr rer nat h.c. Dipl-Psych AFBPsS C.Psychol.
Department of Psychology andDivision of Mental Health and Wellbeing, Warwick Medical School
The longterm effects of Childhood Bullying

Overview
• Parenting – is it overrated
• Bullying ≠ conduct disorder
• What are the consequences in childhood and adulthood?
• Peer bullying often starts with sibling bullying
• Normal rite of passage or need for action?
Copyright: Dieter Wolke (Do not reproduce without permission)

The Psychoanalysts
Sigmund Freud Alfred Adler



Evolution and Fitness
Why would natural selection craft an organism whose futureis entirely influenced by its early experiences?
• The future is uncertain
It does not make any sense to put all eggs in one basketand rely on parents to make us fit for all uncertainties of thefuture
Who else matters?

Now add:
• Nursery/Kindergarten• Primary school• Time with friends• Time with siblings• Time on social media
Conclusion
We spend tens of thousands ofhours with peers > than withparents

Why?• Our parents are not with us forever• Desire to have friends (social and practical support)• Desire for fun with peers and find partner (rewards)• Desire to have friends who are always there for us (protection)• To access support, reward and protection: Need to FIT IN

TV series Friends: How real is it?
Friends: you can choose
Other Peers: siblings, class/work mates –
a forced group

Youths get most victimised by siblingsand peers: NSPCC- Study

Definition of Bullying
Bullying is defined as1. aggressive behaviour or
intentional harm-doingby an individual orgroup that
2. is carried outrepeatedly over time in
3. an interpersonalrelationshipcharacterized by animbalance of power
Gladden, R. M., Vivolo-Kantor, A. M., Hamburger, M. E., & Lumpkin, C. D. (2014). Bullying SurveillanceAmong Youths: Uniform Definitions for Public Health and Recommended Data Elements, Version 1.0. .Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control andPrevention and U.S. Department of Education.

Types of bullying
•Direct/Overt
Name calling, teasing, racial slurs
Obscene gestures
Hitting, kicking, pushing
Threatening, stealing
•Relational
Leaving out on purpose
Spreading nasty rumours
purposeful damage to social relationships

Prevalence of Bullying Victimisation in Europe
Analitis, F., Velderman, M. K., Ravens-Sieberer, U., Detmar, S., Erhart, M., Herdman, M., et al.(2009). Being Bullied: Associated Factors in Children and Adolescents 8 to 18 Years Old in 11European Countries. Pediatrics, 123(2), 569-577.
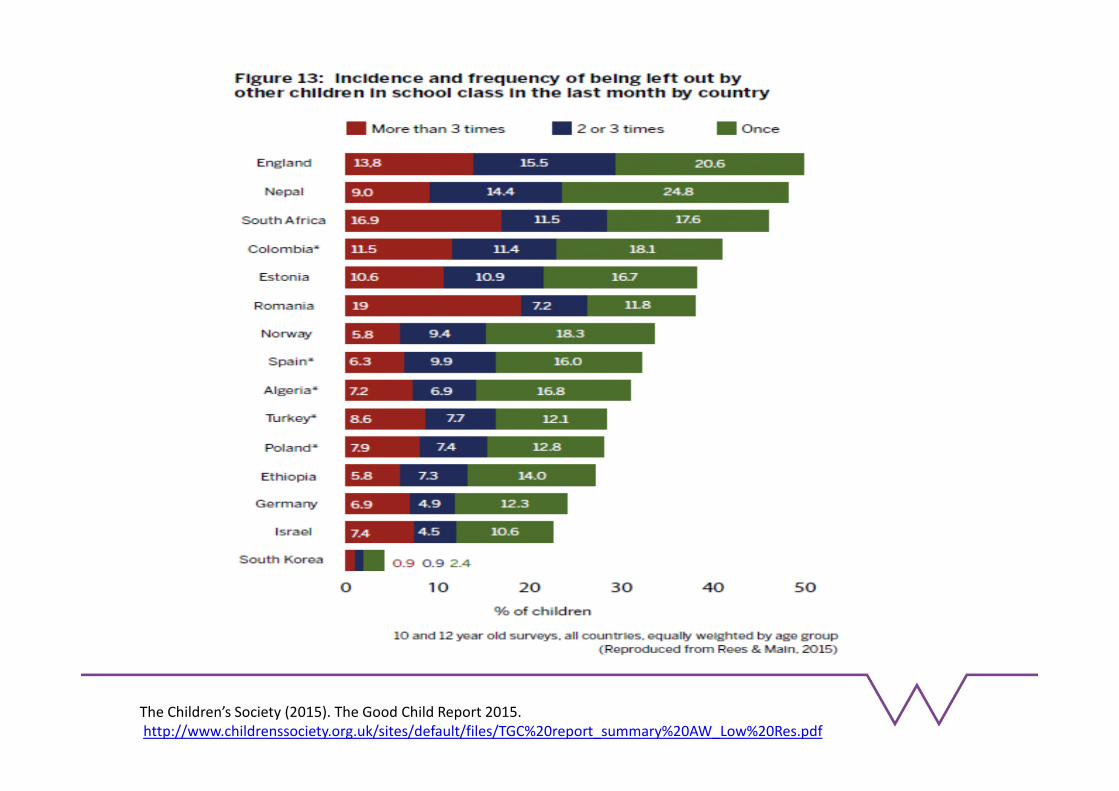
The Children’s Society (2015). The Good Child Report 2015.http://www.childrenssociety.org.uk/sites/default/files/TGC%20report_summary%20AW_Low%20Res.pdf

Motivation to bully?
Why do children, adolescents oradults (e.g. at work) bully others?
Why do we find it in most mammalsand cultures?

Bullying: An Evolutionary Adaptation?
Found in modern society, modern hunter-gatherers and ancientcivilizations
It is not maladaptation in societies at a staggering scale but doesserve an adaptive purpose for a few (bullies).
Evolutionary: access to resources, survival (protection),dominance, reduced stress and more mating opportunities
Modern Society (resources – access jobs, money and status togain access to reproductive success)
Bullying is found in all SES groups, ethnic groups and increased thescarcer and more unequal the resources.

Bullies are found in all SES groups
Tippett, N. & Wolke, D. (2014) Bullying andSocioeconomic Status: A meta-analysis.American Journal of Public Health,doi:10.2105/AJPH.2014.301960

Society: Income Inequality and Bullyingothers (r=.62)
Elgar FJ, Craig W, Boyce W, Morgan A, Vella-Zarb R. Income Inequality and School Bullying:Multilevel Study of Adolescents in 37 Countries. The Journal of adolescent health : officialpublication of the Society for Adolescent Medicine. 10/01 2009;45(4):351-359.
Bullying ≠ Conduct Disorder
Two types of Bullies: How they differ
Bullies: popular (but controversial), high socialstatus, confident, not impulsive, good emotionrecognition, good social skills, but callous (?) – allSES groups
Bully/victims: least popular, low in hierarchy, lowself-esteem – defeated, impulsive, poor emotionrecognition and social skills - more like conductdisordered children, more likely lower SES

Victims and bullies – A simplification!Major Roles in bullying
“Pure” Bullies - perpetrate the aggression; nevervictims
“Pure” Victims - being bullied; never bully others
Bully/victims – get victimised and bully othersfrequently
Neutral – not involved in bullying

Being Bullied: A normal rite of passage oradverse consequences?

ALSPAC Study – from pregnancy intoadulthood
Based in the old county of Avon, BristolSouth West England
110 miles from London
Situated within the postcode BSnumbers of Bristol including smallareas of Gloucestershire, Somersetand Bath
N: 14.000pregnancies

William Copeland Jane Costello Adrian Angold
http://devepi.duhs.duke.edu/studies.html

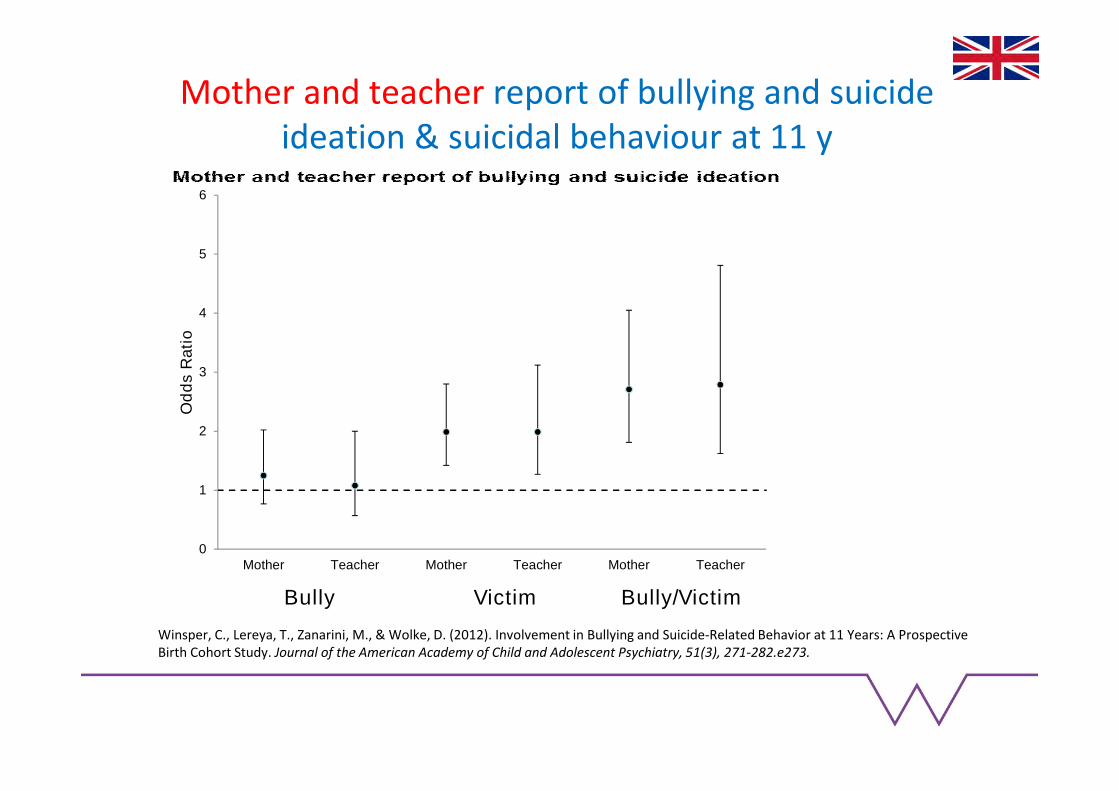
Mother and teacher report of bullying and suicideideation & suicidal behaviour at 11 y
1 2 3 4 5 6 7 8
0
1
2
3
4
5
6
0
1
2
3
4
5
6
Mother Teacher Mother Teacher Mother Teacher
Od
ds
Ra
tio
Bully Victim Bully/Victim
Winsper, C., Lereya, T., Zanarini, M., & Wolke, D. (2012). Involvement in Bullying and Suicide-Related Behavior at 11 Years: A ProspectiveBirth Cohort Study. Journal of the American Academy of Child and Adolescent Psychiatry, 51(3), 271-282.e273.

Being bullied directly increased the risk of self-harm (Populationattributable Fraction (PAF) > 20%)
It means: if bullying could be eliminated (and everything else stays thesame) 20% of self-harm cases could be prevented!
Compare this to obesity (BMI > 30) - it occurs in 15% of the population -but accounts for only 2.8% of all myocardial infarctions
Yusuf S, Hawken S, Ôunpuu S, et al. Obesity and the risk of myocardial infarction in 27000 participants from 52 countries:a case- control study. The Lancet. 2005;366(9497):1640-1649.

Depression

Odds ratios (ORs) for ICD-10 depression at 18 years byvictimisation at 13 years (adjusted analysis)
Bowes, L., Joinson, C., Wolke, D., & Lewis, G.(2015). Peer victimisation duringadolescence and its impact on depression inearly adulthood: prospective cohort study inthe United Kingdom. BMJ, 350.0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
ICD 10 - Depression
not victim
occasionalvictim
frequent victim


Epidemiology of psychotic disorders –Prevalence of psychosis continuum
Lifetime prevalence rate of schizophrenia approx. 0.4%Van Os et al. (2009) Psychol Med, 39, 179-195
Saha et al. (2005) PloS Medicine, 2, e141

Chronicity of Victimisation (Child Report) &Psychotic Experiences at 18 years
0
1
2
3
4
5
6
Model A Model B Model C
Od
ds
Rat
ios
UnstableVictim
StableVictim*
*
*
*
*
*
Model B: Adjusted for Sex, any DSM-IV diagnosis, IQ, internalizing/externalizing behaviourModel C: Adjusted for Sex, any DSM-IV diagnosis, IQ, internalizing/externalizing behaviour, depression symptoms at 12, 13 or 14 years and psychoticexperiences at 12 years
Wolke, D., Lereya, S. T., Fisher, H. L., Lewis, G., & Zammit, S. (2014). Bullying in elementary school and psychotic experiences at 18 years:a longitudinal, population-based cohort study. Psychological Medicine, 44(10), 2199-2211. doi: doi:10.1017/S0033291713002912

Bullying involvement at 9-16 years and early adultpsychiatric outcome (controlled for childhood
psychiatric problems and family factors)1 2 3 4 5 6
0
5
10
15
20
25
0
5
10
15
20
25
Bully Victim Bully/Victim
Od
ds
Rati
os
Peer Victimisation Status
Depressive Disorders1 2 3 4
0
1
2
3
4
5
6
7
8
9
10
0
1
2
3
4
5
6
7
8
9
10
Bully Victim Bully/VictimO
dd
sR
ati
os
Peer Victimisation Status
Anxiety Disorders

Bullying gets under the skin:Roles in Bullying and chronic lowgrade inflammation (c-reactiveprotein levels changes in blood)
In Childhood From Child to Adulthood
Copeland, W. E., Wolke, D., Lereya, S. T., Shanahan, L., Worthman, C., & Costello, E. J. (2014). Childhood bullyinginvolvement predicts low-grade systemic inflammation into adulthood. Proceedings of the National Academy ofSciences. doi: 10.1073/pnas.1323641111

Brown, V., Clery, E., & Ferguson, C. . (2011). Estimating the prevalence of young people absent from school due tobullying. National Centre for Social research. (Vol. 1, pp. 1-61).

Adult Outcomes of Bullying
Baby Toddler Preschool Teen Adult
Victimisation
SocialPoor
relationshipswith parents,few friends,
noconfidante
WealthPoor school
performance,less income,
dismissed fromjobs, Poor in
managingfinances
HealthPsychiatric,seriousillness,smoking,slow recovery

Summary of Findings
Being bullied by peers has wide ranging and non-specific effects on mental health – it increases the riskof psychopathology (from depression to psychoticexperiences and suicide), general health, wealth andsocial relationships/wellbeing – affects productivityof society
Bully/victims and chronically bullied children havethe worst long term outcomes
Bullies: no adverse effects on health, little adverseeffect on wealth and social relationships in adulthood.

Read a short summary of long termconsequences
Archives of Disease in Childhood, 2015http://dx.doi.org/10.1136/archdischild-2014-306667


Frequency of Maltreatment & Bullying
Total N = 4,026 for ALSPAC and 1,420 for GSMS
Categories Frequencies ALSPAC Frequencies GSMS
None 2205 (54.8) 682 (58.9)
Only Maltreatment 341 (8.5) 207 (15.0)
Only Bullied 1197 (29.7) 225 (16.3)
Both 283 (7.0) 159 (9.8)
Lereya, S. T., Copeland, W. E., Costello, E. J., & Wolke, D. Adult mental health consequences of peerbullying and maltreatment in childhood: two cohorts in two countries. The Lancet Psychiatry. doi:10.1016/S2215-0366(15)00165-0

Overall Mental Health ProblemMaltreatment & Being Bullied
0
1
2
3
4
5
6
7
8
9
10
ALSPAC GSMS
Od
ds
Rat
ios
Maltreatment only
Being bullied only
Both
******
***
***

Being Bullied at Ages 7 & 11 and PsychiatricOutcomes at Age 45
Takizawa, R., Maughan, B., & Arseneault, L. (2014). Adult Health Outcomes of Childhood BullyingVictimization: Evidence From a Five-Decade Longitudinal British Birth Cohort. AJP. 18 April online
0
1
2
3
4
5
6
Depression Anxiety Suicidality
Od
ds
Rat
ios
Occasionally Bullied
Frequently Bullied
Placed in Care

Implications & Conclusions
• Governmental efforts have focused almost exclusivelyon public policy to address parent maltreatment ofchildren and much less attention and resources hasbeen paid to peer bullying
• This imbalance requires attention
• More integrated policies and interventions are needed

Where does it come from and how to change it?
Socio-economic factors
Pregnancy
Individual Characteristics
Parenting
Siblings
Schools and Society
Wolke, D., Tippett, N., & Dantchev, S. (2015). Bullying inthe family: sibling bullying. The Lancet Psychiatry, 2(10),917-929. doi: http://dx.doi.org/10.1016/S2215-0366(15)00262-X

Siblings
Most children have siblings (>85%)
The most enduring relationship (outlive parents)
Different relationship trajectories – often get closeragain in older age/when have own children
Can learn from siblings
- positive
- negative
Can be supportive

Definitions of peer and sibling bullying
Peer Bullying Sibling Bullying
1. Aggressive behaviour or
intentional harm-doing by an
individual or group that
2. Is carried out repeatedly over
time in
3. An interpersonal relationship
characterized by an imbalance of
power
?

PrevalenceMost are bully-victims
Tippett, N., & Wolke, D. (2014). Aggression between siblings: Associations with the homeenvironment and peer bullying. Aggressive Behavior, n/a-n/a. doi: 10.1002/ab.21557

Relationships and Perception ofDanger/Insult Impact

Sibling Aggression
Victimisation Perpetration Interaction
(Victimisation x
Perpetration)
Peer Bullying
Victim 1.69 (1.38-2.07) 0.90 (0.68-1.19) 0.82 (0.60-1.13)
Bully 0.72 (0.39-1.35) 2.63 (1.69-4.09) 1.00 (0.55-1.82)
Bully-Victim 2.05 (0.72-5.80) 3.44 (1.27-9.29) 0.44 (0.13-1.44)
Controlled for the following potential confounds: demographic characteristics, family and sibling composition, parent-child relationshipsand socioeconomic factors

First Longitudinal Study of Sibling Bullyingon Adult Mental Health
Pedatrics, September, 8, 2014

Sibling Victimisation at 12 and Self-harm at 18*Linear Trend: 1.21 (1.09-1.35)
*Adjusted for pre-existing problems, peer victimisation, family circumstances andmaltreatmentBowes, Wolke et al. (2014.) Sibling victimisation and the emergence of depression in late
adolescence: a longitudinal study. Pediatrics, September 2014

http://www.bbc.co.uk/news/magazine-24867267: wished I had not been born

Wolke, D., Tippett, N., & Dantchev, S. (2015). Bullying in the family: siblingbullying. The Lancet Psychiatry, 2(10), 917-929. doi:http://dx.doi.org/10.1016/S2215-0366(15)00262-X

Arguments to ignore bullying and itsconsequences
It is so frequent – it is normal to bebullied…….
That does not mean it does not need to betreated(Fractures or broken bones are frequent 22-50% ofpopulation – why do we treat those – they are “normal”)

Bullying and the lawhttps://www.gov.uk/bullying-at-school/the-law
1. The law
Some forms of bullying are illegal and should be reported to the police.These include:
violence or assault
theft
repeated harassment or intimidation, eg name calling, threats andabusive phone calls, emails or text messages
hate crimes
Call 999 if you or someone else is in immediate danger.

Bullying and the lawhttps://www.gov.uk/bullying-at-school/the-law
2. Schools and the law
By law, all state (not private) schools must have a behaviour policy inplace that includes measures to prevent all forms of bullying amongpupils.
This policy is decided by the school. All teachers, pupils and parentsmust be told what it is.
3. Anti-discrimination law
Schools must also follow anti-discrimination law. This means staffmust act to prevent discrimination, harassment and victimisationwithin the school. This applies to all schools in England and Wales,and most schools in Scotland.
Northern Ireland has different anti-discrimination law

TO RAISE AWARENESS:Worked with All Party Parliamentary Group on bullying and charities:
Definition in the new Family and Child Bill – Depression as a special Need


http://www.ghipb.org/

Peers and sibling bullying
Lawyers can make a difference –
Consider bullying in life outcomes, address bullying inschool and work settings
Intervene not with law and sanctions butencourage positive and empathic actions
People who listen, accommodate and negotiatehave the highest social status (and not the bully)!
