sickle cell anemia & health disparities everardo cobos, md hematology division summer seminar on...
TRANSCRIPT

Sickle Cell Anemia & Health Disparities
Everardo Cobos, MD
Hematology Division
Summer Seminar on Health Disparities
Sickle Cell Anemia & Health Disparities: outline Review of sickle cell anemia Brief review of health disparities Interplay between sickle cell anemia and
health disparity Increase awareness of racial, ethnic, gender,
geographic disparities in health care among the general public and key stakeholders, and increase health care providers’ awareness of disparities
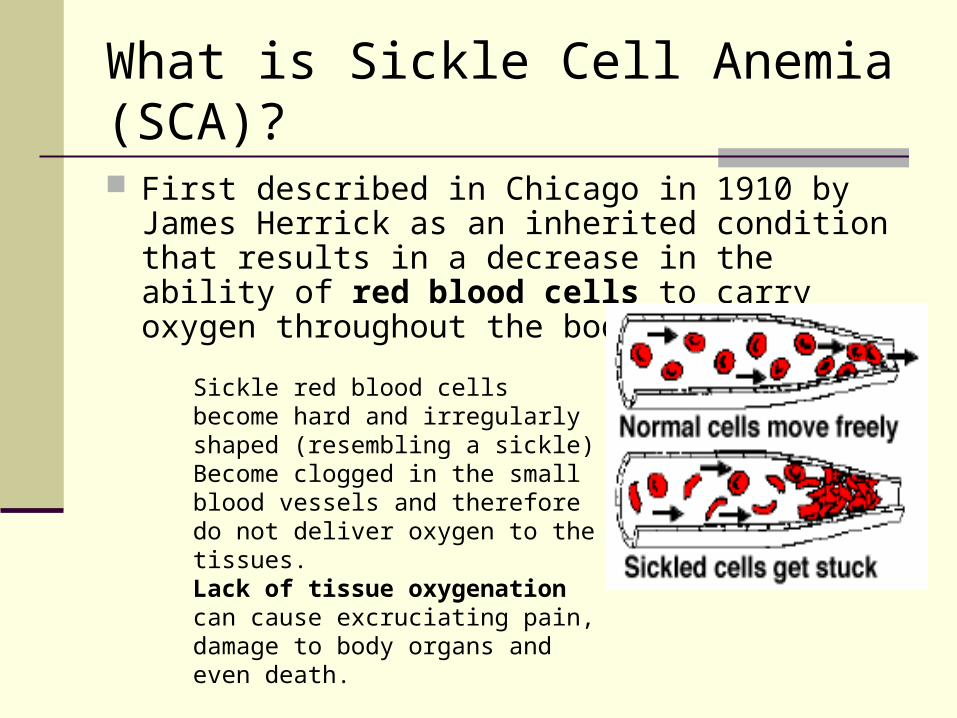
What is Sickle Cell Anemia (SCA)?
First described in Chicago in 1910 by James Herrick as an inherited condition that results in a decrease in the ability of red blood cells to carry oxygen throughout the body
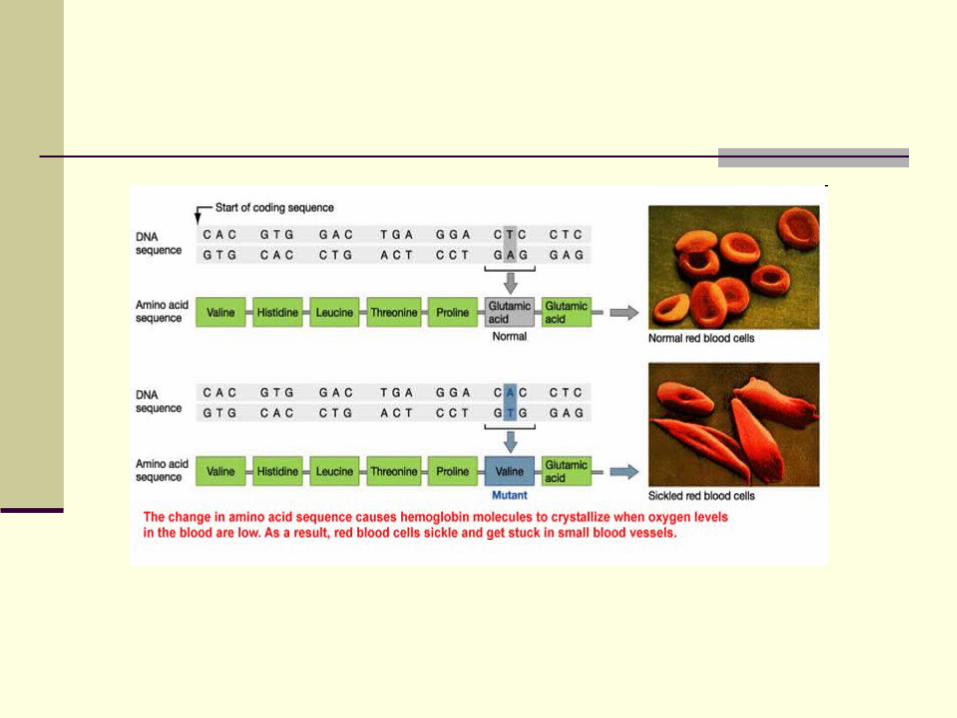
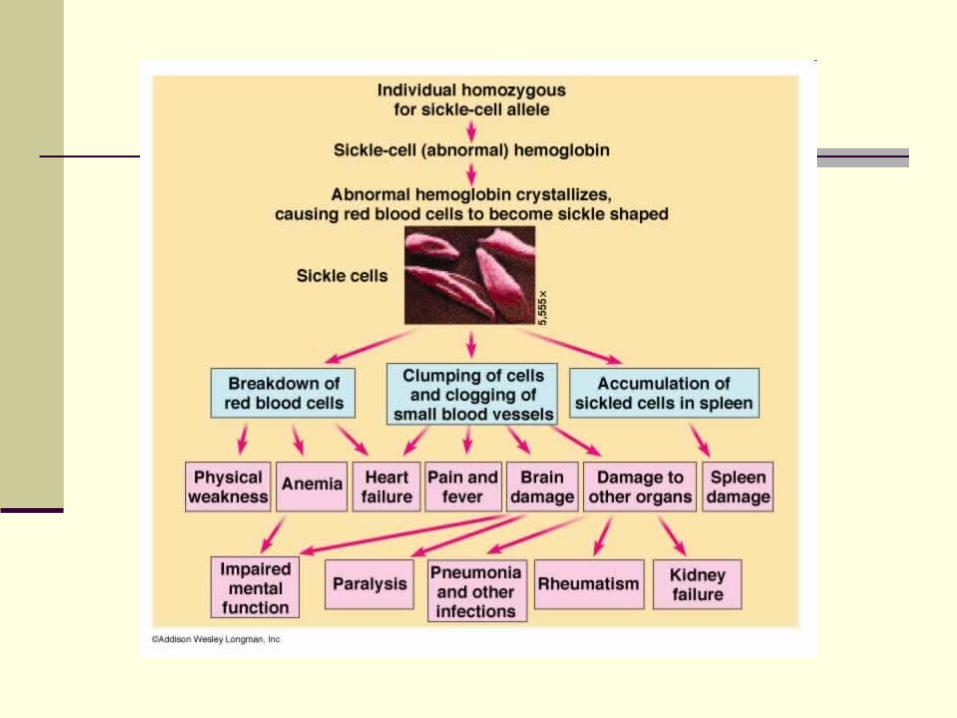
Sickle red blood cells become hard and irregularly shaped (resembling a sickle)Become clogged in the small blood vessels and therefore do not deliver oxygen to the tissues.Lack of tissue oxygenation can cause excruciating pain, damage to body organs and even death.
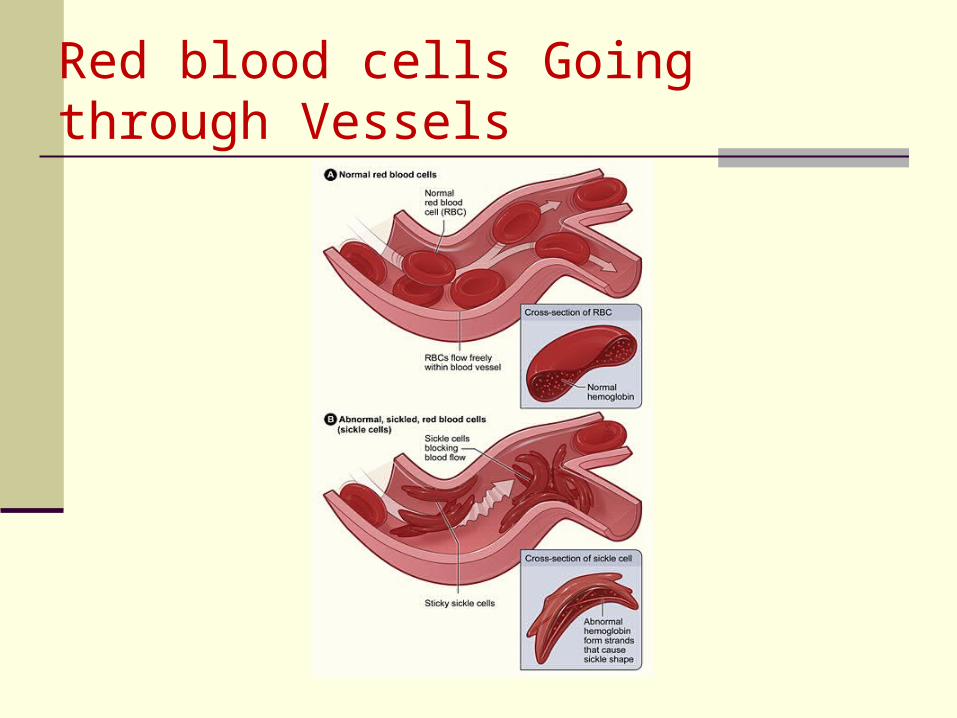
Red blood cells Going through Vessels

Sickle Cell Syndromes
Sickle cell trait Sickle cell anemia Hemoglobin SC Hemoglobin SE Sickle/Thal anemia Sickle cell HPHF
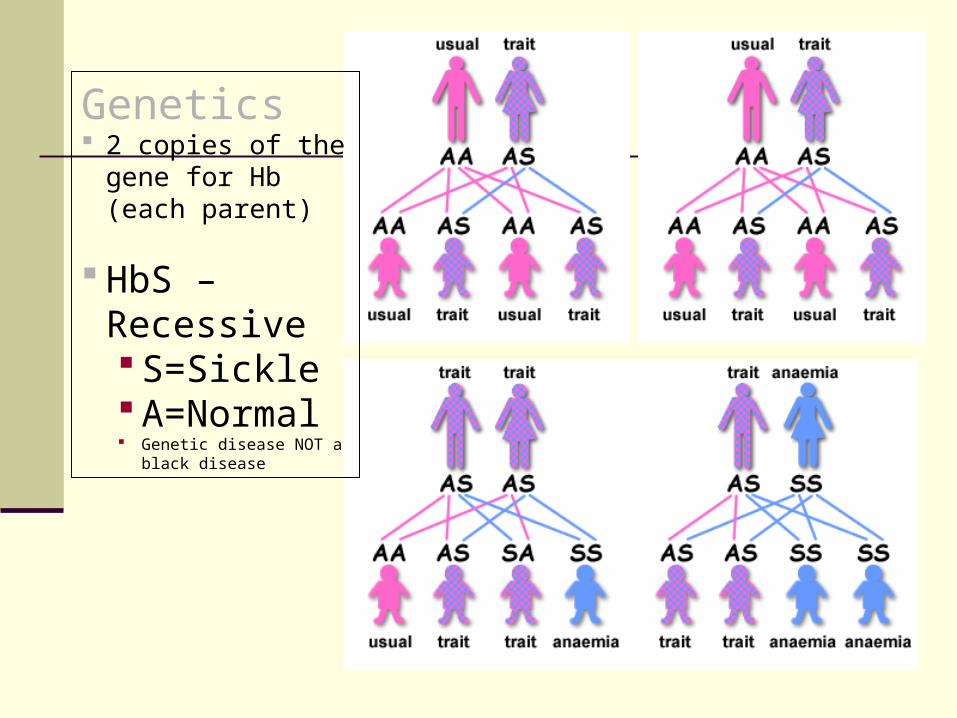
Genetics 2 copies of the
gene for Hb (each parent)
HbS –Recessive S=Sickle A=Normal Genetic disease NOT a
black disease
Some Genetic History
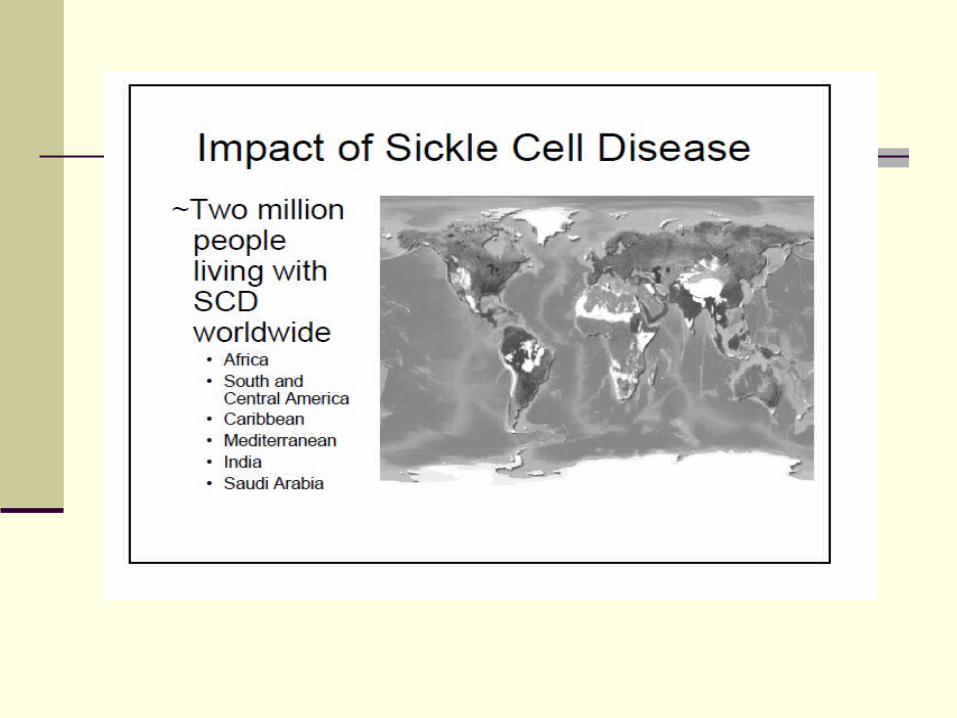
The error in the hemoglobin gene results from a genetic mutation that occurred many thousands of years ago in people in parts of Africa, the Mediterranean basin, the Middle East, and India.
A deadly form of malaria was very common at that
time Malaria epidemics caused the death of many In areas where malaria was a problem, children who
inherited one sickle hemoglobin gene and who, therefore, carried the sickle cell trait - had a survival advantage.
Unlike the children who had normal hemoglobin genes, they survived the malaria epidemics they grew up, had their own children, and passed on the gene- for sickle hemoglobin.
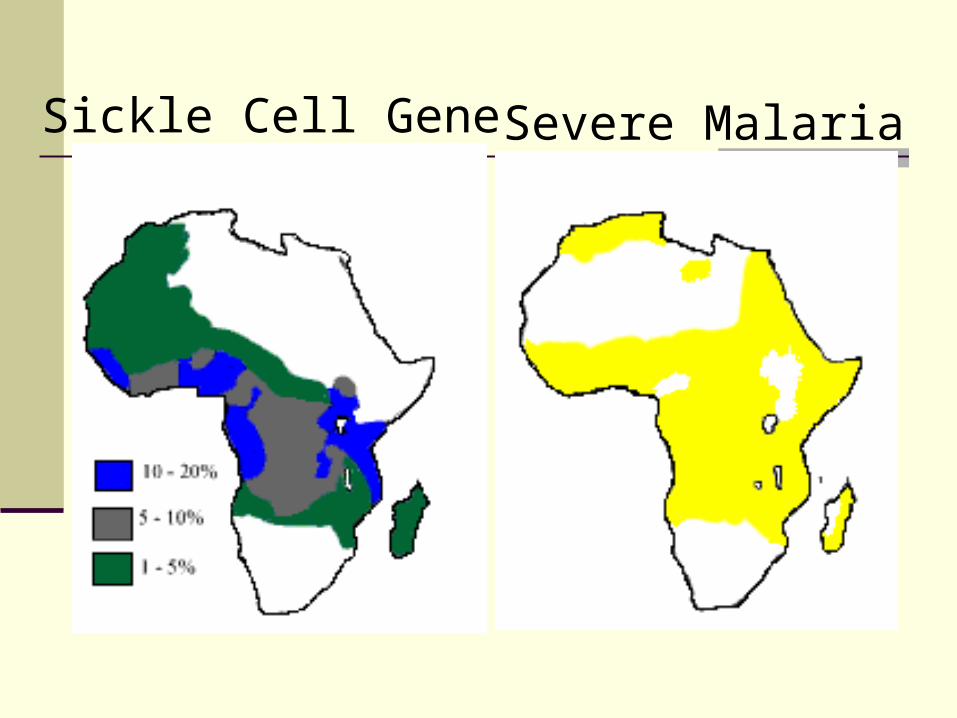
Sickle Cell Gene Severe Malaria
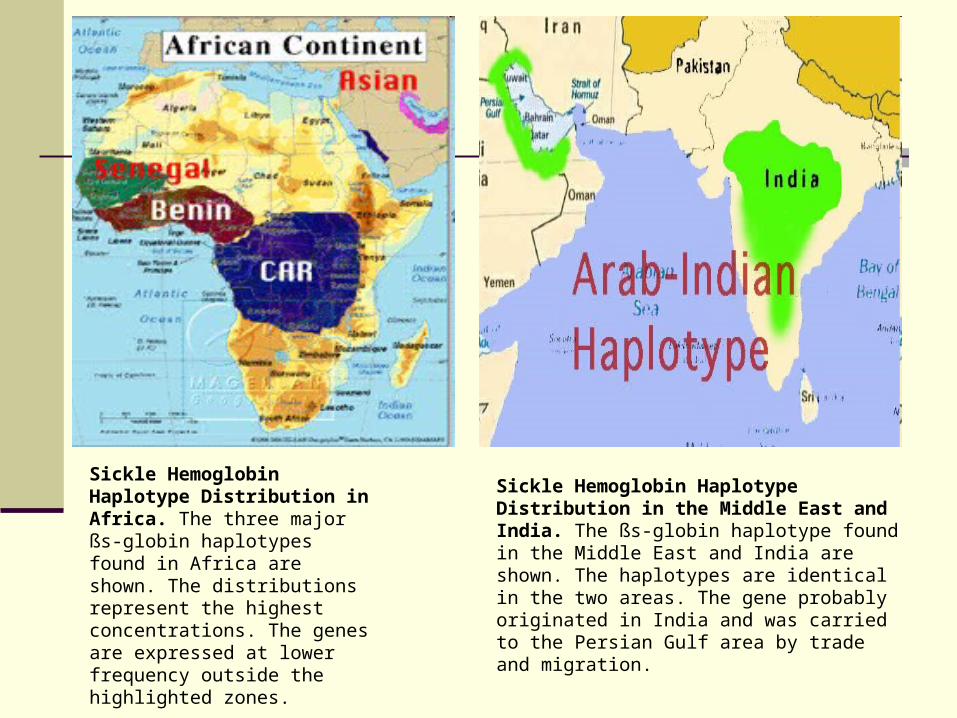
Sickle Hemoglobin Haplotype Distribution in Africa. The three major ßs-globin haplotypes found in Africa are shown. The distributions represent the highest concentrations. The genes are expressed at lower frequency outside the highlighted zones.
Sickle Hemoglobin Haplotype Distribution in the Middle East and India. The ßs-globin haplotype found in the Middle East and India are shown. The haplotypes are identical in the two areas. The gene probably originated in India and was carried to the Persian Gulf area by trade and migration.

Hemoglobin Haplotype
As populations migrated, the sickle cell-mutation spread to other Mediterranean areas, further into the Middle East and eventually into the Western Hemisphere.
In the United States and other countries where malaria is not a problem, the sickle hemoglobin gene no longer provides a survival advantage.
Instead, it may be a serious threat to the carrier's children, who may inherit two abnormal sickle hemoglobin genes and have sickle cell anemia.
History

Medical Complications
1. pain episodes
2. strokes
3. increased infections
4. leg ulcers
5. bone damage
6. yellow eyes or jaundice
7. early gallstones
8. lung blockage
9. kidney damage and loss of body water in urine
10.painful erections in men (priapism)
11.blood blockage in the spleen or liver (sequestration)
12.eye damage
13.low red blood cell counts (anemia)
14.delayed growth

Infectious complications Prominent early in life Leading cause of morbidity and mortality Great improvement in the prognosis related to newborn
screening for sickle cell disease, vaccination for childhood illnesses, the use of prophylactic antibiotics, and aggressive diagnosis and treatment of febrile events
Acute splenic sequestration Episodes of rapid increase in splenic size and decrease
in hemoglobin Potential source of morbidity and mortality early in life
for children with sickle cell anemia and at any age for those with Hb SC disease and sickle thalassemia
Serious Complications
Strokes Up to 15% of children may have overt or silent strokes
during childhood Chronic transfusion therapy reduces the recurrence
rate of overt stroke which may approach 75% without intervention
Bone disease Early risk is primarily from osteomyelitis
Infectious usually painful inflammatory disease of bone often of bacterial origin and may result in bone tissue death
Avascular necrosis of the femur and humerus Death of bone tissue due to disrupted blood
supply Marked by severe pain in the affected region and
by weakened bone that may flatten and collapse
Serious Complications
Serious Complications
Leg ulcers Seen in patients older than 10 years of age Resistant to therapy and cause significant morbidity
Ophthalmic complications Proliferative retinopathy, vitreous hemorrhage, & retinal detachment
Priapism Distressing complication that occurs at all ages Difficult to treat Causes a high incidence of impotence
Chronic Anemia Associated with fatigue, irritability, jaundice, pain, delayed puberty, leg
sores, eye problems, gum disease
Serious Complications: PAINRecurrent Pain Episodes or Sickling
Crises
Occur at any age but appear to be particularly frequent during late adolescence and early adult life Unpredictable Red Blood Cells get stuck in the small veins and prevent
normal blood flow Characterized by severe severe pain in the back, chest,
abdomen, extremities, and head Highly disruptive to life Most common reasons for individuals to seek health
care

1. Sickle Cell Anemia Sickle hemoglobin (HbS) + Sickle hemoglobin (HbS)
Most Severe – No HbA
Three common types of Sickle Cell Disorders
Other Sickling Disorders
Other types of Hb combine with sickle Hb
2. Hemoglobin S-C disease Sickle hemoglobin (HbS) + (HbC)
3. Hemoglobin S-Beta thalassemia Beta thalassaemia gene reduces the amount of HbA
that can be made Sickle hemoglobin (HbS) + reduced HbA Milder form of Sickle Cell Disorder than sickle cell
anemia
“‘Sickle Cell Anemia: It's Not a “Black Disease”’
One of the common misconceptions is that only black people get sickle cell, but this is not the case.
There are many different ethnicities that can have sickle cell.


“of all forms of inequality,
injustice in health care is
the most shocking and
inhumane”
Martin Luther King, Jr

Health disparitiesIOM STUDY CHARGE Assess the extent of racial and ethnic differences in healthcare that are
not otherwise attributable to known factors such as access to care (e.g., ability to pay or insurance coverage);
Evaluate potential sources of racial and ethnic disparities in healthcare, including the role of bias, discrimination, and stereotyping at the individual (provider and patient), institutional, and health system levels; and,
Provide recommendations regarding interventions to eliminate healthcare disparities.
Evidence of Racial and Ethnic Disparities in Healthcare
Disparities consistently found across a wide range of disease areas and clinical services
Disparities are found even when clinical factors, such as stage of disease presentation, co-morbidities, age, and severity of disease are taken into account
Disparities are found across a range of clinical settings, including public and private hospitals, teaching and non-teaching hospitals, etc.
Disparities in care are associated with higher mortality among minorities (e.g., Bach et al., 1999; Peterson et al., 1997; Bennett et al., 1995)

Black and White Differences in Specialty Procedure Black and White Differences in Specialty Procedure Utilization Among Medicare Beneficiaries Age 65 Utilization Among Medicare Beneficiaries Age 65
and Olderand Older
Black White Black-to-
White Ratio
Angioplasty (procedures per 1,000 beneficiaries per year)
2.5 5.4 0.46
Coronary Artery Bypass Graft Surgery (procedures per 1,000 beneficiaries per year)
1.9 4.8 0.40
Mammography (procedures per 100 women per year)
17.1 26.0 0.66
Hip Fracture Repair (procedures per 100 women per year)
2.9 7.0 0.42
Amputation of All or Part of Limb (procedures per 1,000 beneficiaries per year)
6.7 1.9 3.64
Bilateral Orchiectomy (procedures per 1,000 beneficiaries per year)
2.0 0.8 2.45
Source: Gornick et al., 1996

Non
-Min
orit
y
Min
orit
yDifference
Clinical Appropriateness and Need
Patient Preferences
The Operation of Healthcare Systems and the Legal and Regulatory Climate
Discrimination: Biases andPrejudice, Stereotyping, andUncertainty
Disparity
Qua
lity
of H
ealth
Car
eDifferences, Disparities, and Discrimination: Populations with Equal Access to Health Care
Populations with Equal Access to Health Care
Racial and ethnic disparities in health care exist and, because they are associated with worse outcomes in many cases, are unacceptable. Racial and ethnic disparities in health care occur in the context of broader historic and contemporary social and economic inequality, and evidence of persistent racial and ethnic discrimination in many sectors of American life. Many sources – including health systems, health care providers, patients, and utilization managers – contribute to racial and ethnic disparities in health care.
SUMMARY OF FINDINGS
Disparities in the Clinical Encounter: The Core Paradox
How could well-meaning and highly educated health professionals, working in their usual circumstances with diverse populations of patients, create a pattern of care that appears to be discriminatory?
Disparities in the Clinical Encounter: The Core Paradox
Possibilities examined: bias (prejudice), uncertainty, stereotyping
Bias – no evidence suggests that providers are more likely than the general public to express biases, but some evidence suggests that unconscious biases may exist
Uncertainty – a plausible hypothesis, particularly when providers treat patients that are dissimilar in cultural or linguistic background
Stereotyping – evidence suggests that physicians, like everyone else, use these ‘cognitive shortcuts’
SUMMARY OF RECOMMENDATIONS
GENERAL RECOMMENDATIONS
Increase awareness of racial, ethnic, gender, geographic disparities in health care among the general public and key stakeholders, and increase health care providers’ awareness of disparities.
Sickle cell disease history/awareness
1920 described in literature 1949 Linus Pauling “Sickle Cell Disease; A
Molecular Disease”, Science 1968-1972; period of political
activity/awareness for sickle cell disease MLK health disparities & sickle cell “A warm december”; Sidney Portier TV movie Bill Cosby Marcus Welby, MD
President Richard Nixon surprised many in his health message by putting sickle cell disease into the glowing spotlight of presidential politics. He said, "There are moments in biomedical research when problems begin to break open and results begin to pour in. We believe that cancer research has reached such a point. A second targeted disease for constrained research should be sickle cell anemia. It is a sad and shameful fact," he said, "that the causes of this disease have been largely neglected throughout our history. We cannot rewrite the record of neglect, but we certainly can reverse it."

Funding:
There are huge disparities between the amounts of federal dollars allocated to sickle cell when compared to other disorders. For example, there are three times as many babies born with SCD than with cystic fibrosis, 8,000 versus 2,500. For every baby born with cystic fibrosis there are $2,733 research dollars spent to find a cure in contrast to $345.58 spent for every baby born with SCD (National Institutes of Health)
Source: http://www.nbcchicago.com/brchannel/FP-HLX-Background-Information-on-Sickle-Cell-Disease.html#ixzz0uHEhUidB
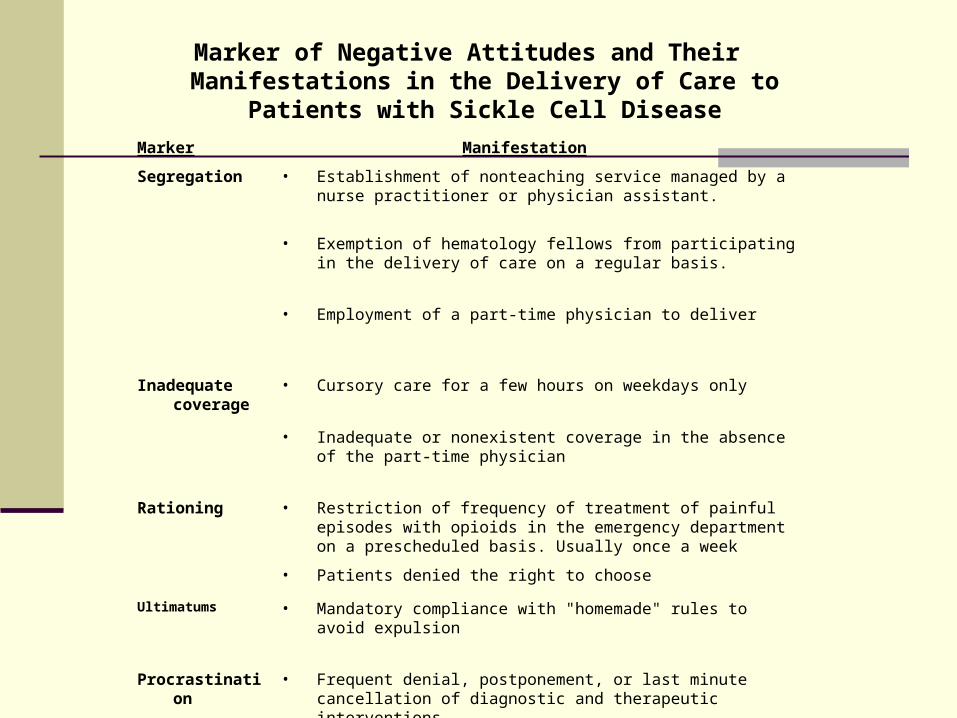
Marker of Negative Attitudes and Their Manifestations in the Delivery of Care to Patients with Sickle Cell
Disease
Marker Manifestation
Segregation • Establishment of nonteaching service managed by a nurse practitioner or physician assistant.
• Exemption of hematology fellows from participating in the delivery of care on a regular basis.
• Employment of a part-time physician to deliver
Inadequate coverage
• Cursory care for a few hours on weekdays only
• Inadequate or nonexistent coverage in the absence of the part-time physician
Rationing • Restriction of frequency of treatment of painful episodes with opioids in the emergency department on a prescheduled basis. Usually once a week
• Patients denied the right to choose
Ultimatums • Mandatory compliance with "homemade" rules to avoid expulsion
Procrastination • Frequent denial, postponement, or last minute cancellation of diagnostic and therapeutic interventions
Treatment of Sickle Cell PainFostering Trust and Justice
William T. Zempsky, MD
JAMA. 2009;302(22):2479-2480.
The following scenario serves as an example of an emerging literature on injustice in health care.
A 19-year-old man with sickle cell disease presents to the emergency department with progressive leg and back pain. His hooded sweatshirt is pulled over his eyes, he is wearing headphones, and is singing along to an unheard tune. His attempts to manage his pain at home have been unsuccessful and he tells the nurse that his pain is a 9 on a 10-point scale. The nurse responds with apparent disbelief and says "Really?" then sends the patient to the waiting room where he sits for several hours before seeing a physician. The patient's request for a specific dose of morphine is met with doubt and disdain. This patient is stigmatized as a drug seeker or abuser, with little consideration for the complexities of his pain. Justice in this context is . . .

I woke up in severe pain.I tried to control it, but in vain.
I went to my primary care physicianHoping to achieve a remission.
He said, "You are a drug addict,And that's my verdict.
I do not believe what you say.There will be no prescription today.
You did not keep the terms of our agreementAnd, hence, there will be no treatment.“
I dragged myself to the emergency room.There I was also met with doubt and gloom.
I had to go through triageAnd wait for release from my quayage.
Hours passed at a pace that was slowBut my pain continued to grow.
Sleepy, hungry and thirsty, I collapsed.I opened my eyes with my pain enhanced.
They said I had a seizure,In addition to a high fever.
They rushed me into a stallAnd treated me with diminished gall.
Finally, I received pain meds with some relief.This greatly reduced my grief.
They decided to admit me to the hospitalA decision that was most acceptable.
I was happy to come to the end of my ordealAnd to be treated with respect and more zeal.
But I am most thankful to the seizure.It made a doubting physician a believer.
The Sickle Cell Pain Believer
Posted: February 10, 2010 Hematology News
Access to care, pain relief still problems for sickle cell patients
Even though expert panels recommend hydroxyurea therapy and clinical trial data assure its safety and efficacy,
confounding barriers continue to restrict its use.
Bioethicists Examine Trust Toward Physicians Among Adults With Sickle Cell DiseaseMain Category: Biology / Biochemistry
Article Date: 04 Jun 2010 - 18:00 PDT


Prevalence
o It is estimated the up to 80,000 people in America have Sickle Cell Disease
o 1/500 African Americans have Sickle Cell Disease
o 1/1000 -4000 Hispanics have Sickle Cell o 1/12 African Americans are carriers for
Sickle Cell o 1/50 Asians are carriers for Sickle Cello 1/100 Greeks are carriers for Sickle Cell