silencing the elusive sézary cell past, present, & · pdf filesilencing the...
TRANSCRIPT

Tuesday September 28, 2015
Silencing the Elusive Sézary cellPast, Present, & Future
Madeleine Duvic, MD
Prof of Dermatology &
Internal Medicine
Blanche Bender Chair in
Cancer Research
Dept of Dermatology
MD Anderson Cancer Center
Houston, Texas

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Clinical Trial or Research Support– Allos/Spectrum, Eisai, Galderma, Kyowa-Kirin, Merck, Millineum, Seattle Genetics, Rhizan, Innate Pharma, Tetrologics, Therakos, Valient
Consultant – Eisai, Galderma, Kyowa-Kirin, Ligand,
Disclosures
Consultant – Eisai, Galderma, Kyowa-Kirin, Ligand, Merck, Millennium, miRNA, Innate
Past Advisory Boards – Allos/Spectrum, Celgene, Eisai, Galderma, Seattle Genetics, Millinieum, Kyowa-Kirin
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
(1880-1956)
French Dermatologist -
Venereologist.
Described “cellules
monstrueuses”
Albert Sézary
monstrueuses”
(monster cells) in skin
and blood
Am J Dermatopathology
Aug 28(4):357-67, 2006
clinicaloptions.com/oncology
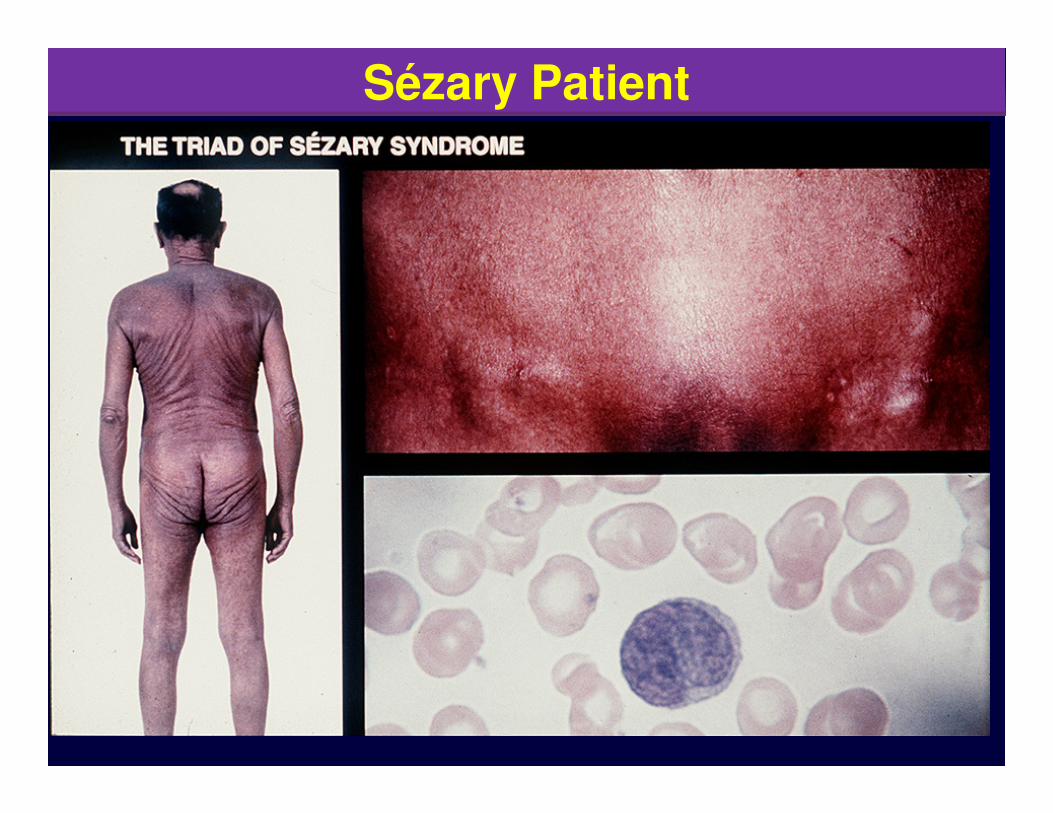
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeSézary Patient

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Variants recognized by Clinical-Pathologic features
Cutaneous T-Cell and NK-Cell Lymphomas
Mycosis fungoides - effector skin memory cells
MF variants and subtypes
Pagetoid reticulosis
Granulomatous slack skin
• WHO-EORTC Classification of CTCL
Willemze R, et al. Blood. 2005;105:3768-3785.
Granulomatous slack skin
Sézary syndrome - central memory T cells – leukemia CD4+CD26- or CD7-
Adult T-cell leukemia/lymphoma ATCL (HTLV-1+)
Primary cutaneous CD30+ lymphoma (ALCL) & Lymphoproliferative disorder (LyP)
Extranodal NK/T-cell lymphoma, nasal type (EBV+)
Primary cutaneous peripheral T-cell lymphoma, unspecified
Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma (provisional)
Cutaneous γ/δ T-cell lymphoma (provisional)
Primary cutaneous CD4+ small/medium-sized pleomorphic T-cell lymphoma (provisional)

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Why are SS patients red and get keratoderma?
� Why are they itch?
� Why is the SS cell nucleus cerebriform?
� Why does photopheresis improve both SS and GVHD?
Questions about Sezary Syndrome
GVHD?
� Can Antiboides or drugs selectively kill malignant T cells?
� Next Gen Sequencing: What are the genetic or epigenetic drivers of T cell proliferation and genomic instability.
� How can we cure SS?
clinicaloptions.com/oncology
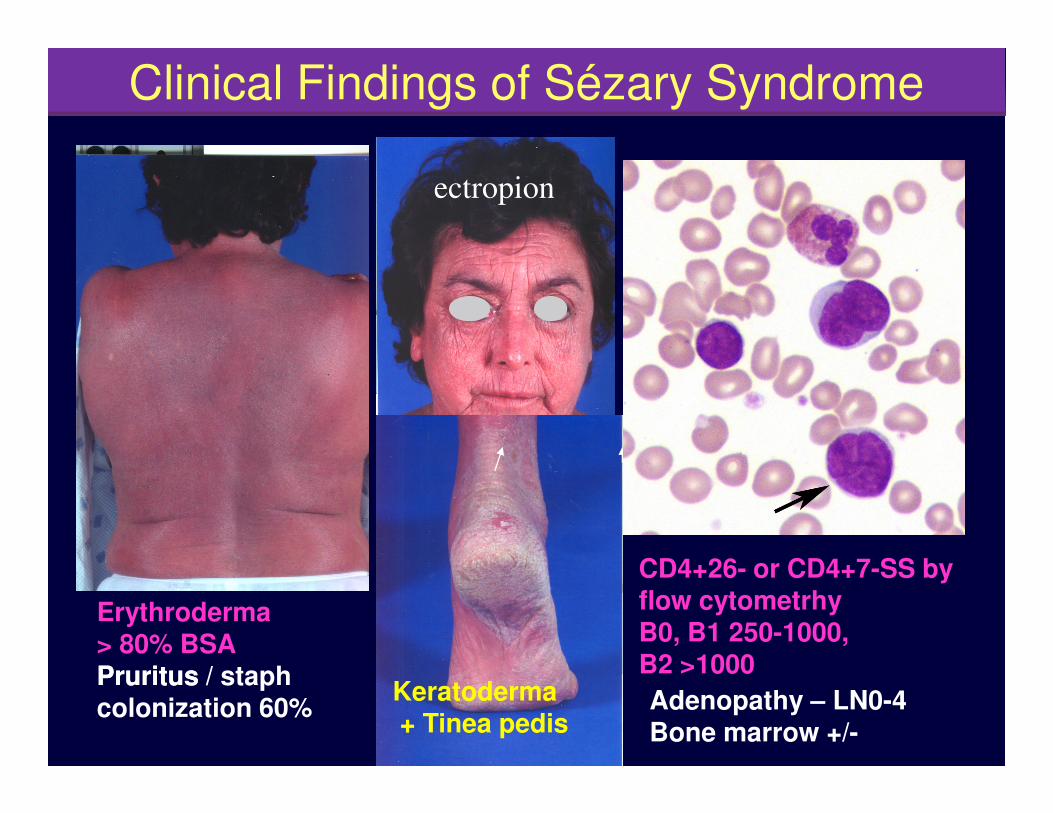
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeClinical Findings of Sézary Syndrome
ectropion
Erythroderma> 80% BSAPruritusPruritus / staph colonization 60%
Keratoderma+ Tinea pedis
CD4+26- or CD4+7-SS by flow cytometrhyB0, B1 250-1000, B2 >1000
Adenopathy – LN0-4Bone marrow +/-

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
74 yo WF - Sézary Syndrome x 7 years. ECP, bexarotene, & gemcitabine. Red with MRSA sepsis stopped on ampicillin. Ongoing CR x >10 years.
Why are SS patients red?
Baseline Week 8
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Sepsis is most common cause of death in SS patients.
� 1992 - SS cells proliferate in response to bacterial superantigens according to Vb usage.
� 1995 – Catheter associated sepsis in 11/12 ECP pts noting that IV Abs improve EE. Duvic JAAD 1996 35(4):573
•What we learnedStaph and Sézary Syndrome
� 1997 - 76% enterotoxin+ S.Aureus- ETS-1 - TSST- assocVb2 - no fever. Jackow CM, et al. Blood. 1997 Jan 1;89(1):32-40
� 48% of 107 E/SS pts colonized with S.A. or MRSA. 85% decolonized w treatment - Br J Dermatol 2008 Jul;159(1):105-12.
� Standard of care: Atopic skin care w antibiotics improves redness, LDH, SS number, pruritus, and OS

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC)
Elise Olsen, Eric Vonderheid, Nicola Pimpinelli, Rein Willemze, Youn Kim, Elise Olsen, Eric Vonderheid, Nicola Pimpinelli, Rein Willemze, Youn Kim,
Robert Knobler, Herschel Zackheim, Madeleine Duvic, Teresa Estrach,
Stanford Lamberg, Gary Wood, Reinhard Dummer, Annamari Ranki,
Gunter Burg, Peter Heald, Mark Pittelkow, Maria-Grazia Bernengo, Wolfram
Sterry, Liliane Laroche, Franz Trautinger, and Sean Whittaker, for the
ISCL/EORTC
Revised Blood and Node Staging - 2007
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
mSWAT Weighing Factors
� % involvement with patch x 1
� % involvement with plaque x 2
� % involvement with tumors (ulcers) x 4
Clinical Evlauation MF/Sézary Syndrome
---------------------------------------------------------
� mSWAT = sum of % lesions x factor
� BSA (body surface area) w/o weighing
� Sezary defined as >80% BSA or T4

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Perivascular infiltrates without diagnostic epidermotrophism
� Sézary cells cerebriform
Leukemic CTCL and Sezary Syndrome are perivascular
� Sézary cells cerebriformmorphology
� CD4+CD26-
� CD4+CD7-
� Central memory T-cells
CD 25 CD 30Diwan AH, Prieto VG, Herling M, Duvic M, Jones D.
Am J Clin Pathol. 2005 Apr;123(4):510-5

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
% CD4+CD26-
CD4+26- in blood by stage using flow
Bernengo, M.G. The relevance of the CD4+CD26- subset in theidentification of circulating Sézary cells. Br J Dermatol 2001;144:125.
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeP
rob
ab
ility
of
Ove
rall
Su
rviv
al
0.6
0.8
1.0
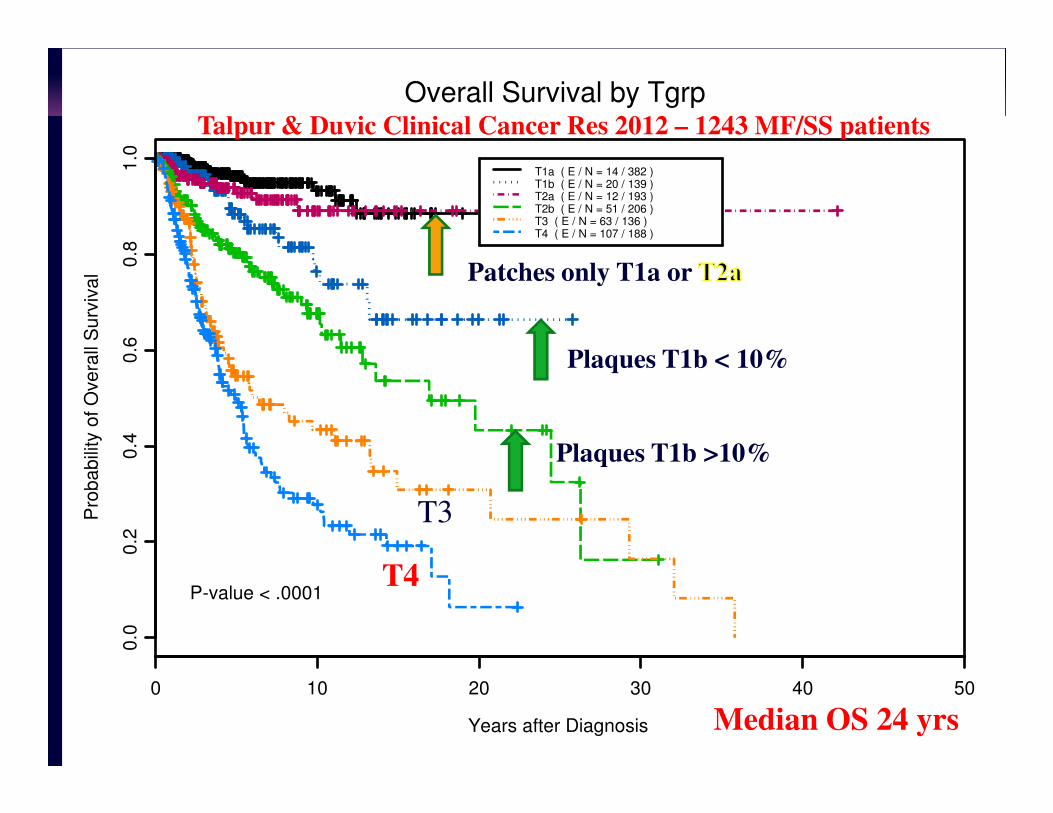
T1a ( E / N = 14 / 382 )T1b ( E / N = 20 / 139 )T2a ( E / N = 12 / 193 )T2b ( E / N = 51 / 206 )T3 ( E / N = 63 / 136 )T4 ( E / N = 107 / 188 )
Overall Survival by TgrpTalpur & Duvic Clinical Cancer Res 2012 – 1243 MF/SS patients
Patches only T1a or
Plaques T1b < 10%
Years after Diagnosis
Pro
ba
bili
ty o
f O
ve
rall
Su
rviv
al
0 10 20 30 40 50
0.0
0.2
0.4
P-value < .0001
Plaques T1b >10%
T3
T4
Median OS 24 yrs
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Pro
babili
ty o
f O
vera
ll S
urv
ival
0.6
0.8
1.0
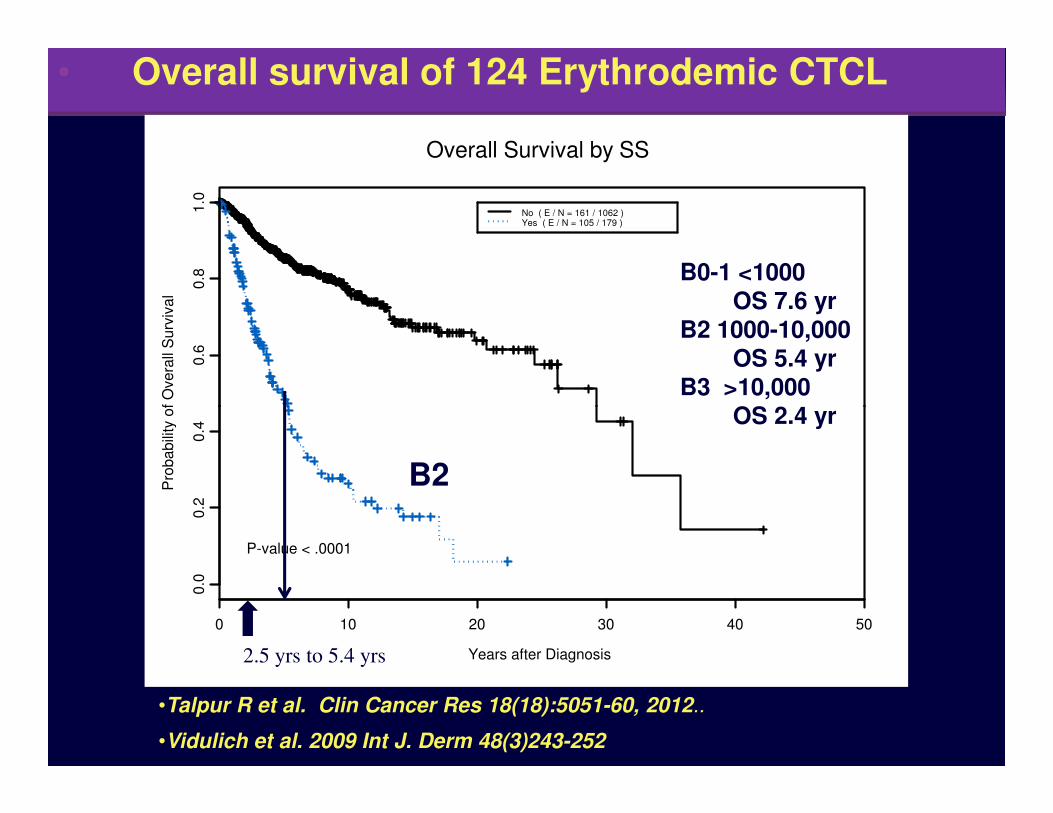
No ( E / N = 161 / 1062 )Yes ( E / N = 105 / 179 )
Overall Survival by SS
B0-1 <1000 OS 7.6 yr
B2 1000-10,000OS 5.4 yr
B3 >10,000OS 2.4 yr
• Overall survival of 124 Erythrodemic CTCL
Years after Diagnosis
Pro
babili
ty o
f O
vera
ll S
urv
ival
0 10 20 30 40 50
0.0
0.2
0.4
P-value < .0001
•Talpur R et al. Clin Cancer Res 18(18):5051-60, 2012..
•Vidulich et al. 2009 Int J. Derm 48(3)243-252
2.5 yrs to 5.4 yrs
OS 2.4 yr
B2

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeWhat Sezary saw What we know now
� Helper Central Memory CD4+CD45R0+CLA+4
� Perivascular infiltrate w/out epidermotropism
� Clonal TCR rearrangements
� Abnormal karyotypes� Abnormal karyotypes
� Th2 cytokines, T-Plastin, Twist, CCR4, CXCR3. KIRDL2, Foxp3, IL2R, Jak/stat5, IL31 itch
� Accumulation – loss of fasinduced apoptosis.
� Role of epigenetics HDACi
clinicaloptions.com/oncology
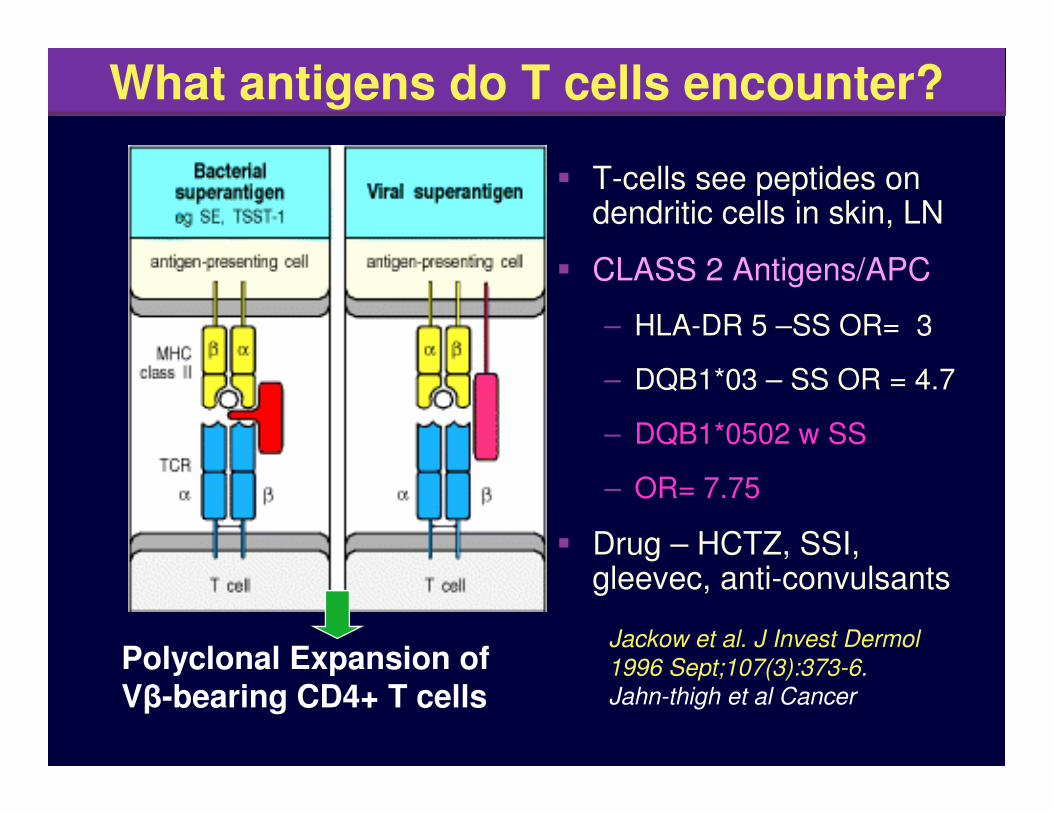
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeWhat antigens do T cells encounter?
� T-cells see peptides on dendritic cells in skin, LN
� CLASS 2 Antigens/APC
– HLA-DR 5 –SS OR= 3
– DQB1*03 – SS OR = 4.7
Polyclonal Expansion of Vβ-bearing CD4+ T cells
– DQB1*0502 w SS
– OR= 7.75
� Drug – HCTZ, SSI, gleevec, anti-convulsants
Jackow et al. J Invest Dermol
1996 Sept;107(3):373-6.
Jahn-thigh et al Cancer
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� PHOTOPHERESIS – Edelson- first immunotherapy 1988
� Denileukin diftitox - first fusion toxin – 1990s
� Bexarotene (Targretin) - first rexinoid in man 1990s
� Vorinostat first histone deacetylase inhibitor in man
� Romidepsin second HDACi, Belinostat (PTCL)
FDA Approved Therapies
� Romidepsin second HDACi, Belinostat (PTCL)
� Topical Nitrogen mustard in gel base – 2014
� Radiation – electron beam – lower doses 4 x 2, 12 v 36 Gy
� Not approved: Topical Steroids, topical retinoidsaoralsoriataine, tazarotene, UVA and PUVA phototherapy, Interferons, methotrexate, TRL agonists, PD1/PDL1
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Palliative skin directed care: culture for Staph, antibiotics, moisturize and use topical steroids wet wraps, NB-UVB, PUVA, TBSEB
� Itching: gabapentin – opiate antagonists
� First line: Rooks combination immunomodulatorytherapy: photopheresis, bexarotene +/- interferon alpha or gamma, GM-CSF, avoid po stds
Treatment of E-CTCL and SS
alpha or gamma, GM-CSF, avoid po stds
� Second line: HDAC-Inhibitors: Romidepsin, pentostatin, targeted therapies, antibodies (CCR4, CD52,CD30), TBSEB, chemotherapy
� allogeneic SCT ––TBEB + non-ablative allo SCT 75% CRs in SS- submitted JCO
Olsen et al J Am Acad Dermatol 64(2):352-404, 2/2011.
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
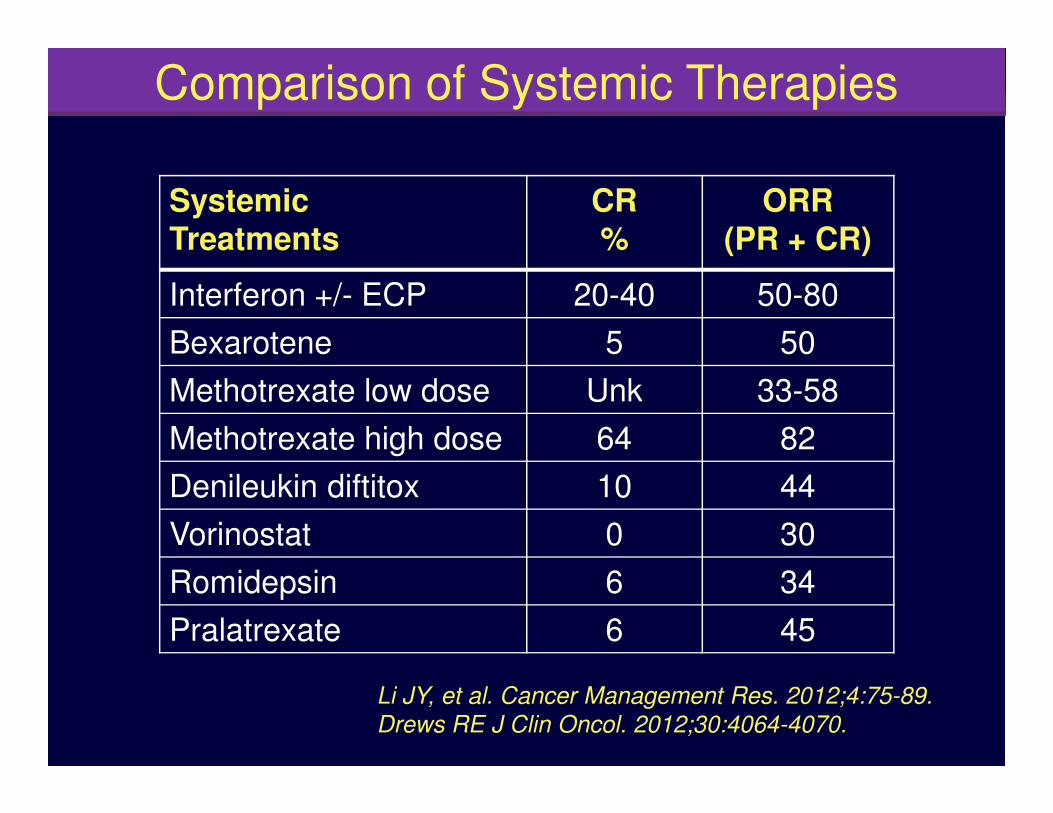
SystemicTreatments
CR%
ORR (PR + CR)
Interferon +/- ECP 20-40 50-80
Bexarotene 5 50
Methotrexate low dose Unk 33-58
Comparison of Systemic Therapies
Methotrexate low dose Unk 33-58
Methotrexate high dose 64 82
Denileukin diftitox 10 44
Vorinostat 0 30
Romidepsin 6 34
Pralatrexate 6 45
Li JY, et al. Cancer Management Res. 2012;4:75-89.
Drews RE J Clin Oncol. 2012;30:4064-4070.
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
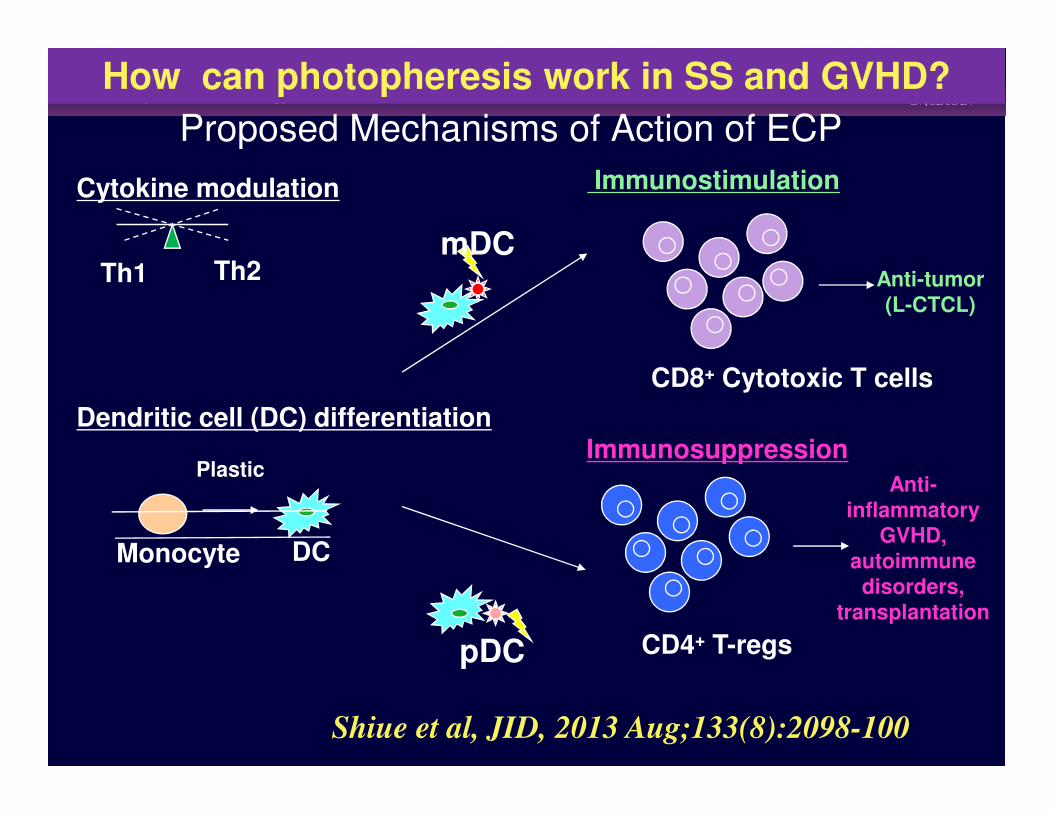
Th1 Th2
Cytokine modulation
Dendritic cell (DC) differentiation
Immunostimulation
CD8+ Cytotoxic T cells
Anti-tumor(L-CTCL)
mDC
Proposed Mechanisms of Action of ECP
How can photopheresis work in SS and GVHD?
Dendritic cell (DC) differentiationImmunosuppression
CD4+ T-regs
Anti-inflammatory
GVHD, autoimmune disorders,
transplantation
Plastic
Monocyte DC
pDC
Shiue et al, JID, 2013 Aug;133(8):2098-100

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
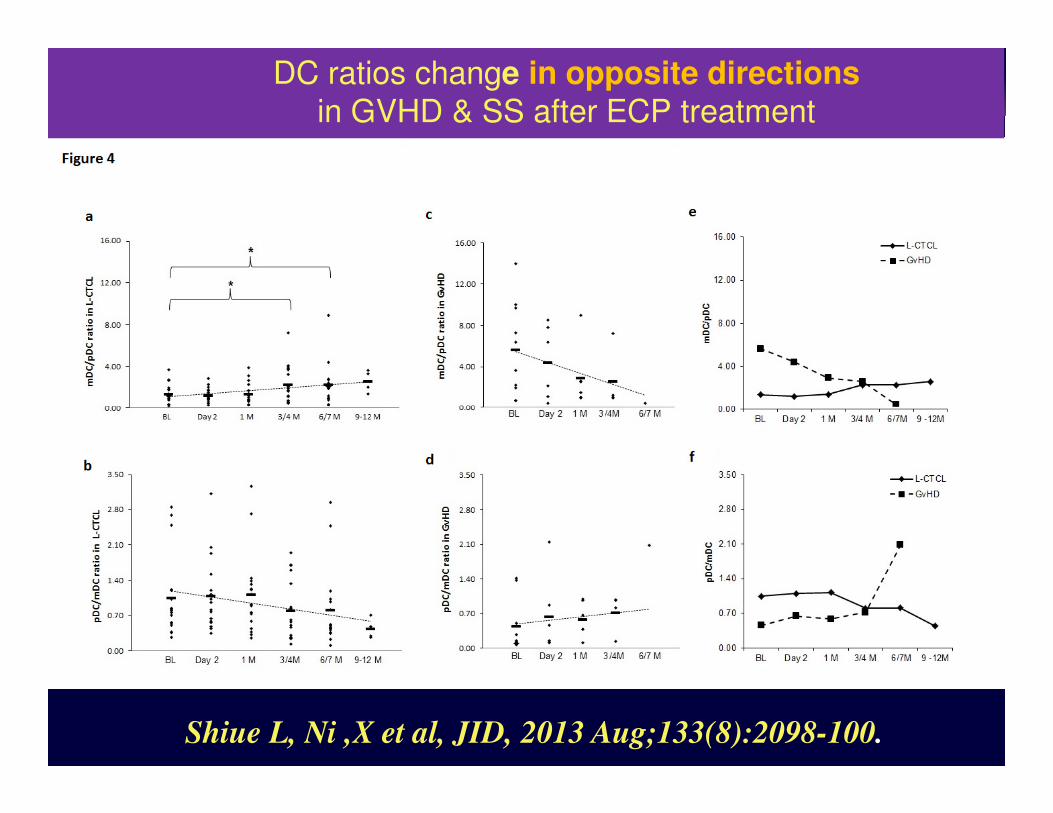
Monocytoid CD11c+ DCs increase in GVHD & SS Plasmacytoid DC CD123+ up in GVHD, down in SS
Shiue L, Ni X et al, JID, 2013 Aug;133(8):2098-100.
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeDC ratios change in opposite directionsin GVHD & SS after ECP treatment
Shiue L, Ni ,X et al, JID, 2013 Aug;133(8):2098-100.
Allogeneic Stem Cell Transplantation for Cutaneous T-cell Lymphoma: Updated results from a single centerUpdated results from a single center
Journal of Clinical Oncology
First 19 patients
Update on 48 patients from
2001 to present
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
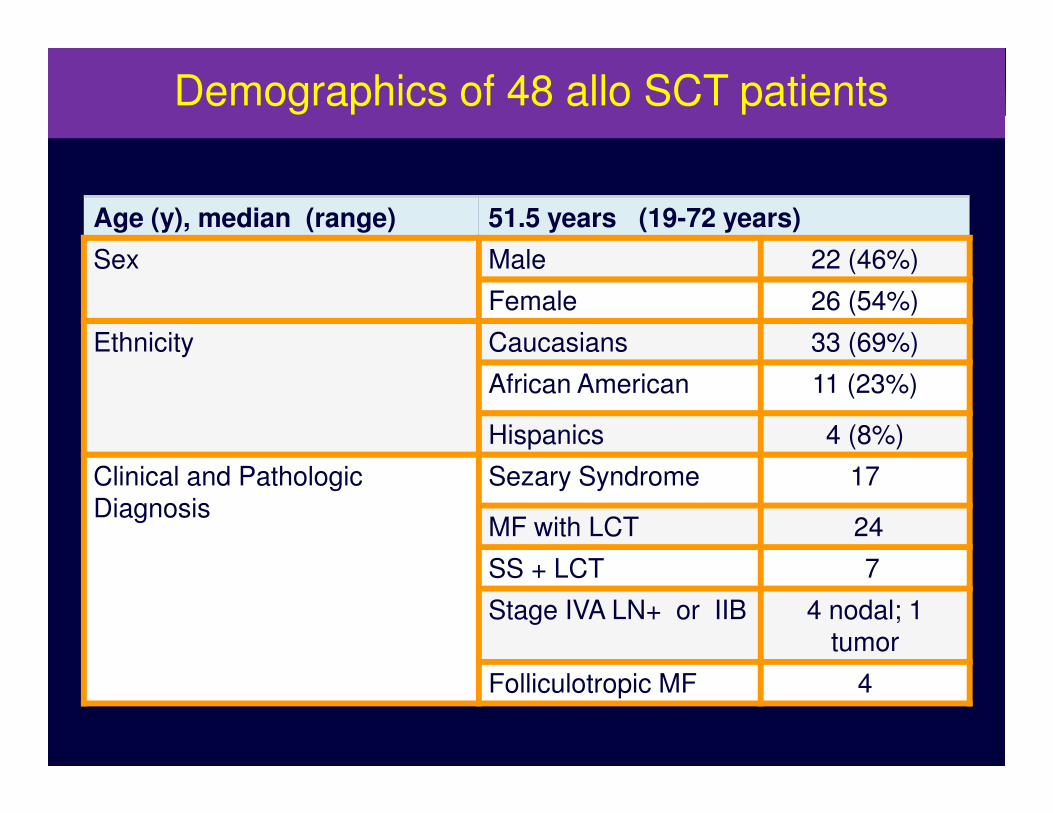
Age (y), median (range) 51.5 years (19-72 years)
Sex Male 22 (46%)
Female 26 (54%)
Ethnicity Caucasians 33 (69%)
African American 11 (23%)
Demographics of 48 allo SCT patients
Hispanics 4 (8%)
Clinical and PathologicDiagnosis
Sezary Syndrome 17
MF with LCT 24
SS + LCT 7
Stage IVA LN+ or IIB 4 nodal; 1 tumor
Folliculotropic MF 4
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
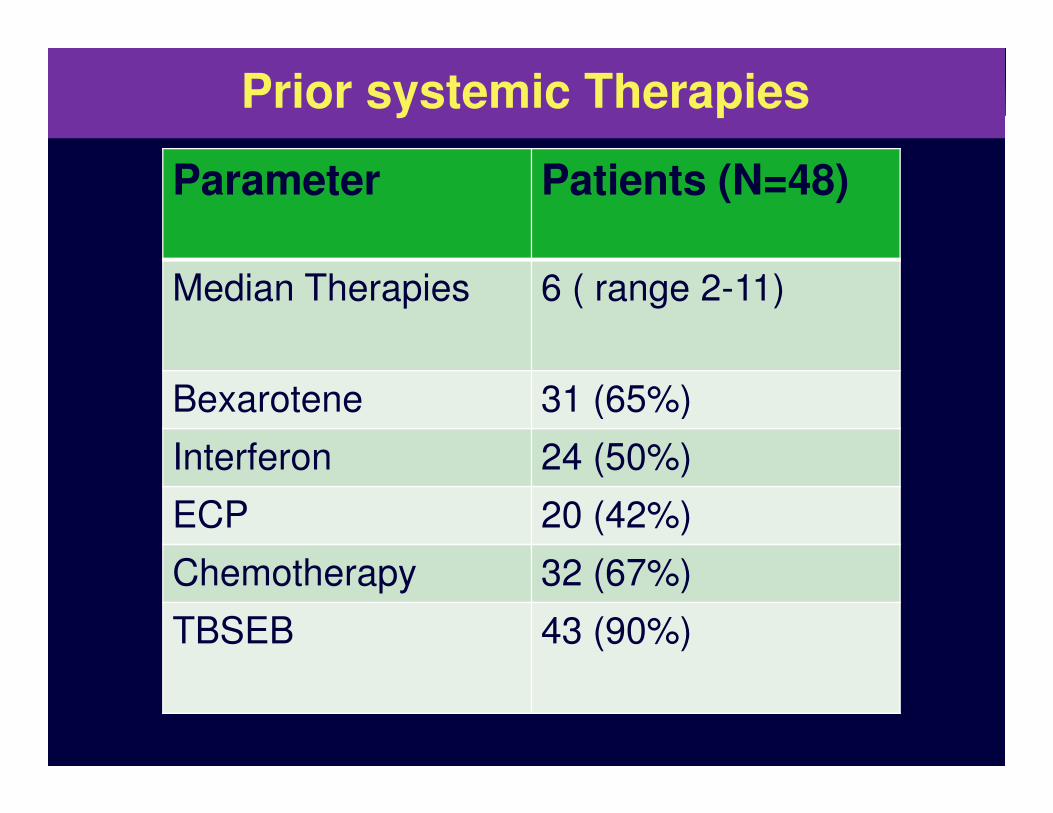
Parameter Patients (N=48)
Median Therapies 6 ( range 2-11)
Bexarotene 31 (65%)
Prior systemic Therapies
Bexarotene 31 (65%)
Interferon 24 (50%)
ECP 20 (42%)
Chemotherapy 32 (67%)
TBSEB 43 (90%)

clinicaloptions.com/oncology
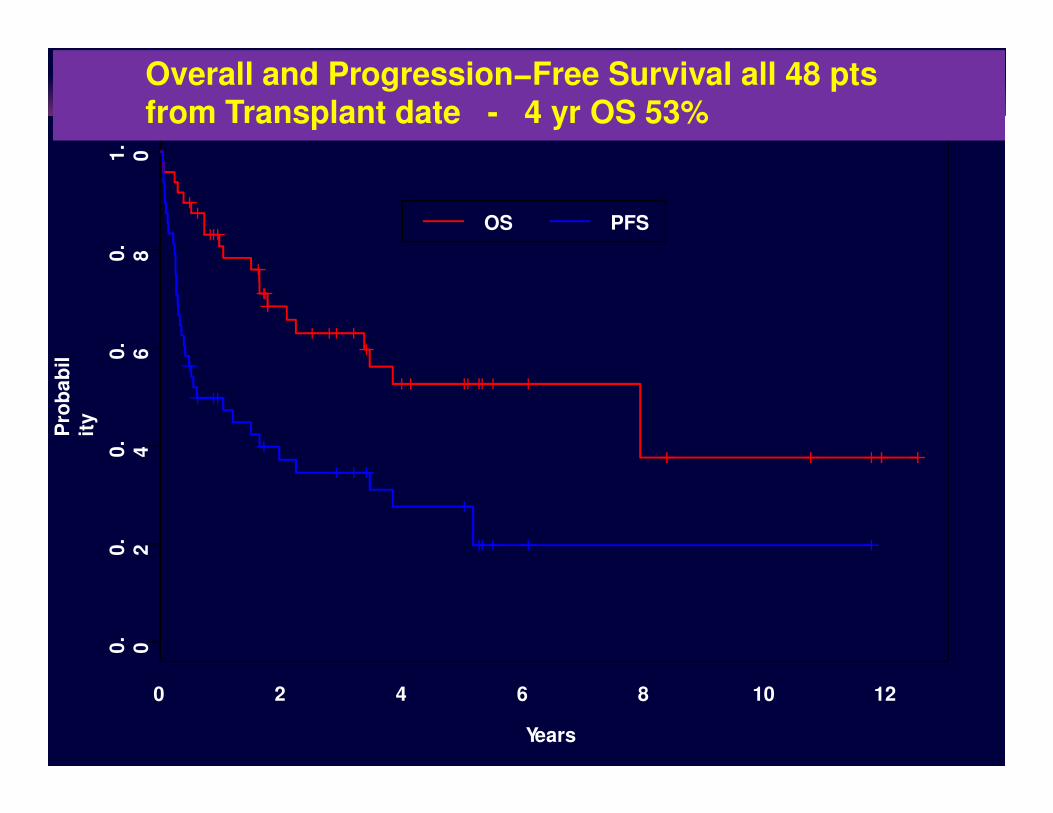
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeOverall Complete Response 58% (28 of 48)Relapse rate 33% (16 of 48) Mortality rate 44% (21/48)
Clinical Variant
N Responders
58%
(28/48)
Relapsed
33% (16/48)
Non-engraftment
8% (4/48)
Dead/Alive
44% (21/48)
SS 14 11 79% 3 21% 3/11
LCT 16 9 56% 4 25% 3 19% 6/10
SS + LCT 9 4 44% 5 56% 4/9
IVA
(LN+)
IIB
4
1
2 40% 2 40% 1 20% 1/4
Fol -MF 4 2 50% 2 50% 2/2
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
0.
60
.8
1.
0
Pro
ba
bil
OS PFS
Overall and Progression−Free Survival all 48 pts from Transplant date - 4 yr OS 53%
0 2 4 6 8 10 12
0.
00
.2
0.
4
Years
Pro
ba
bil
ity
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
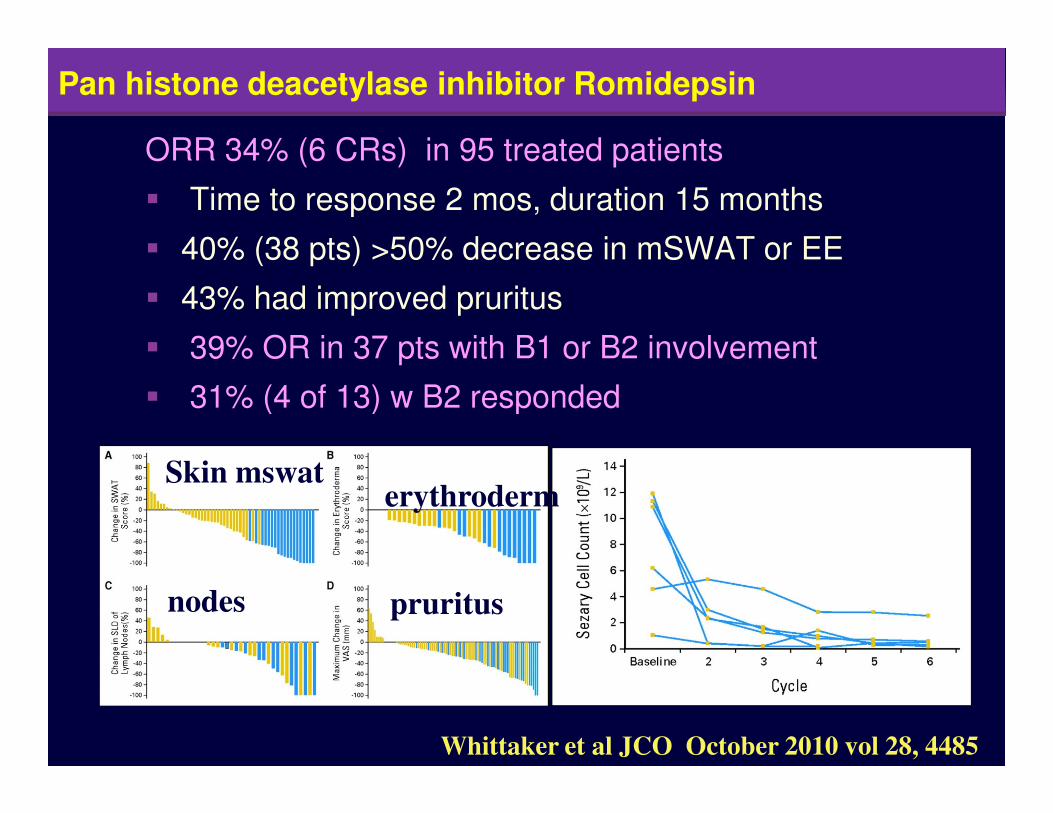
ORR 34% (6 CRs) in 95 treated patients
� Time to response 2 mos, duration 15 months
� 40% (38 pts) >50% decrease in mSWAT or EE
� 43% had improved pruritus
� 39% OR in 37 pts with B1 or B2 involvement
� 31% (4 of 13) w B2 responded
Pan Pan histone deacetylase inhibitor Romidepsin
� 31% (4 of 13) w B2 responded
Whittaker et al JCO October 2010 vol 28, 4485
erythroderm
pruritus
Skin mswat
nodes
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
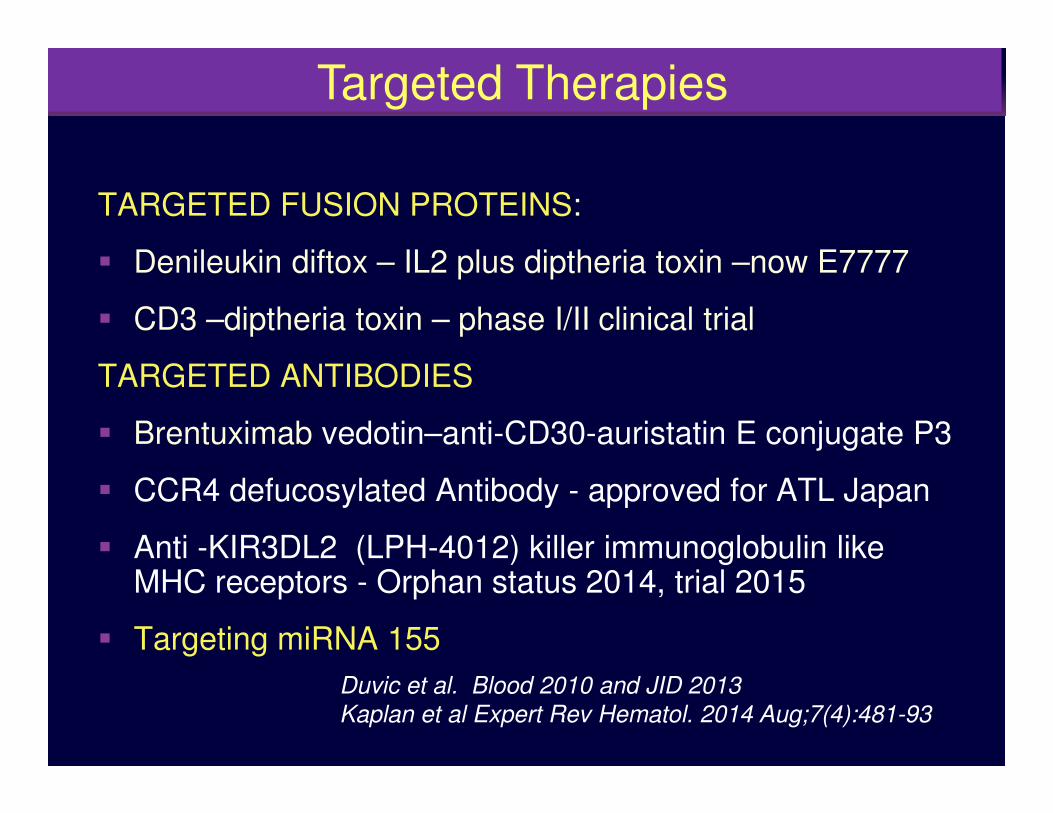
TARGETED FUSION PROTEINS:
� Denileukin diftox – IL2 plus diptheria toxin –now E7777
� CD3 –diptheria toxin – phase I/II clinical trial
TARGETED ANTIBODIES
Targeted Therapies
� Brentuximab vedotin–anti-CD30-auristatin E conjugate P3
� CCR4 defucosylated Antibody - approved for ATL Japan
� Anti -KIR3DL2 (LPH-4012) killer immunoglobulin like MHC receptors - Orphan status 2014, trial 2015
� Targeting miRNA 155
Duvic et al. Blood 2010 and JID 2013
Kaplan et al Expert Rev Hematol. 2014 Aug;7(4):481-93
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
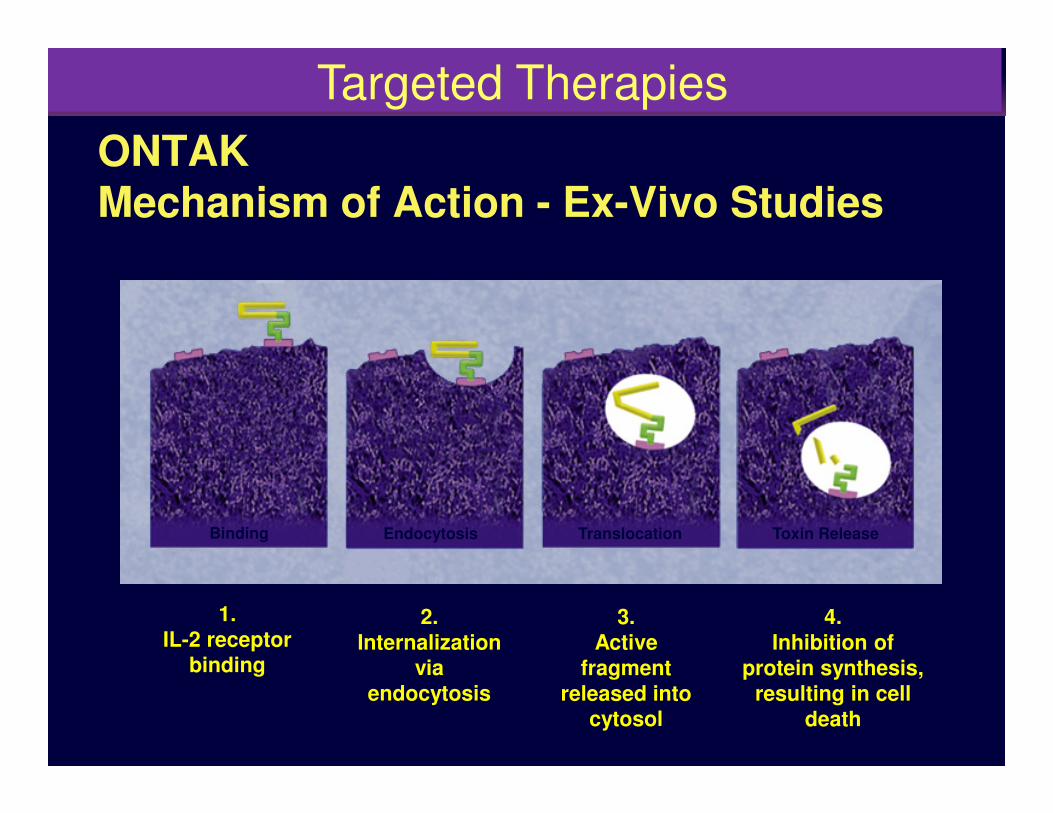
ONTAK Mechanism of Action - Ex-Vivo Studies
Targeted Therapies
Binding Endocytosis Translocation Toxin Release
1. IL-2 receptor
binding
2. Internalization
viaendocytosis
3. Active
fragmentreleased into
cytosol
4. Inhibition of
protein synthesis, resulting in cell
death

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Pivotal Phase 3 Trial of Denileukin Diftitoxin CTCL: Response Rates by Stage
44
50
40
30
Re
sp
on
se
(%
)
CR/CCR
PR
3032
Targeted Therapies
20
10
0
Re
sp
on
se
(%
)
199
25
IB16
IIA10
18%
18
III11
21
IIB19
11 20
13.4
IV15
6.6
Olsen et al. J Clin Oncol. 2001;19:376–388.

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
ALK-negative ALCL
MF
CCR4 Receptor on CD4+ lymphocytes
MF (transformed)
PTCL-U
Ishida T, et al. Clin Cancer Res. 2004 Aug 15;10(16):5494-500.
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
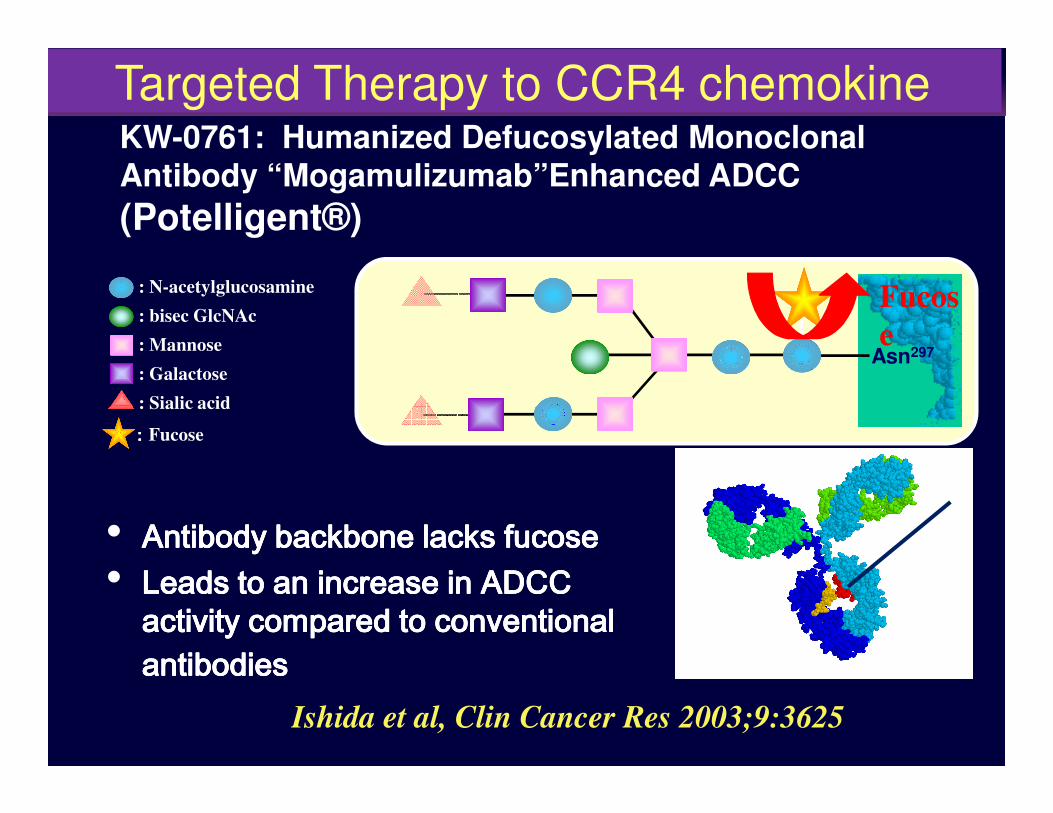
Asn297
: N-acetylglucosamine
: bisec GlcNAc
: Mannose
: Galactose
: Sialic acid
KW-0761: Humanized Defucosylated Monoclonal Antibody “Mogamulizumab”Enhanced ADCC
(Potelligent®)
Fucos
e
Targeted Therapy to CCR4 chemokine
: Sialic acid
:::: Fucose
• Antibody backbone lacks Antibody backbone lacks Antibody backbone lacks Antibody backbone lacks fucosefucosefucosefucose• Leads to an increase in ADCC Leads to an increase in ADCC Leads to an increase in ADCC Leads to an increase in ADCC
activity compared to conventional activity compared to conventional activity compared to conventional activity compared to conventional antibodiesantibodiesantibodiesantibodies
Ishida et al, Clin Cancer Res 2003;9:3625

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeHumanized Anti-CCR4 Antibody: KW-0761Mogamulizumab (KW-0761)
Schedule q two weeks then q week IV
• Phase I/II studies in ATLL in Japan – approved
• Phase I/II US and Phase III Randomized Trial
Yano H, et al. Clin Cancer Res. 2007;13:6494-6500.Duvic M et al. Blood - March 19; 125 (12):1883-9
Ligands TARC, MDC
on endothelial cells.
Helper CD4 and T-regs
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
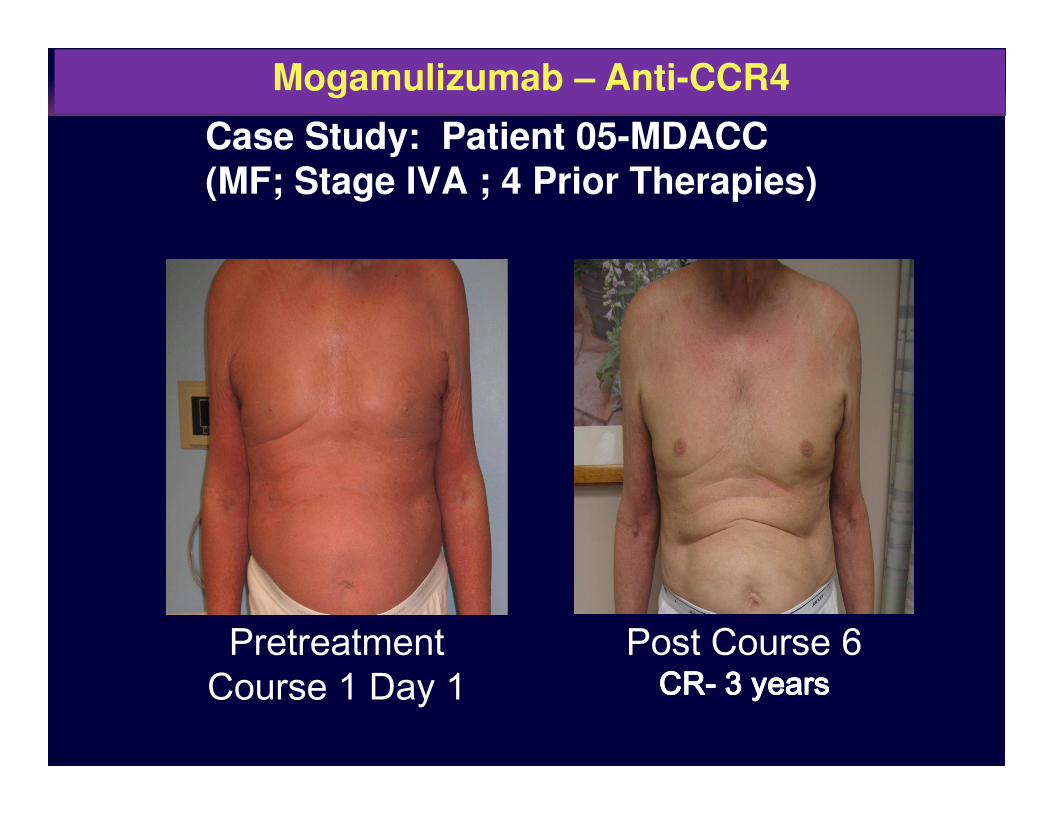
Case Study: Patient 05-MDACC(MF; Stage IVA ; 4 Prior Therapies)
Mogamulizumab – Anti-CCR4
PretreatmentCourse 1 Day 1
Post Course 6CRCRCRCR---- 3 years 3 years 3 years 3 years
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
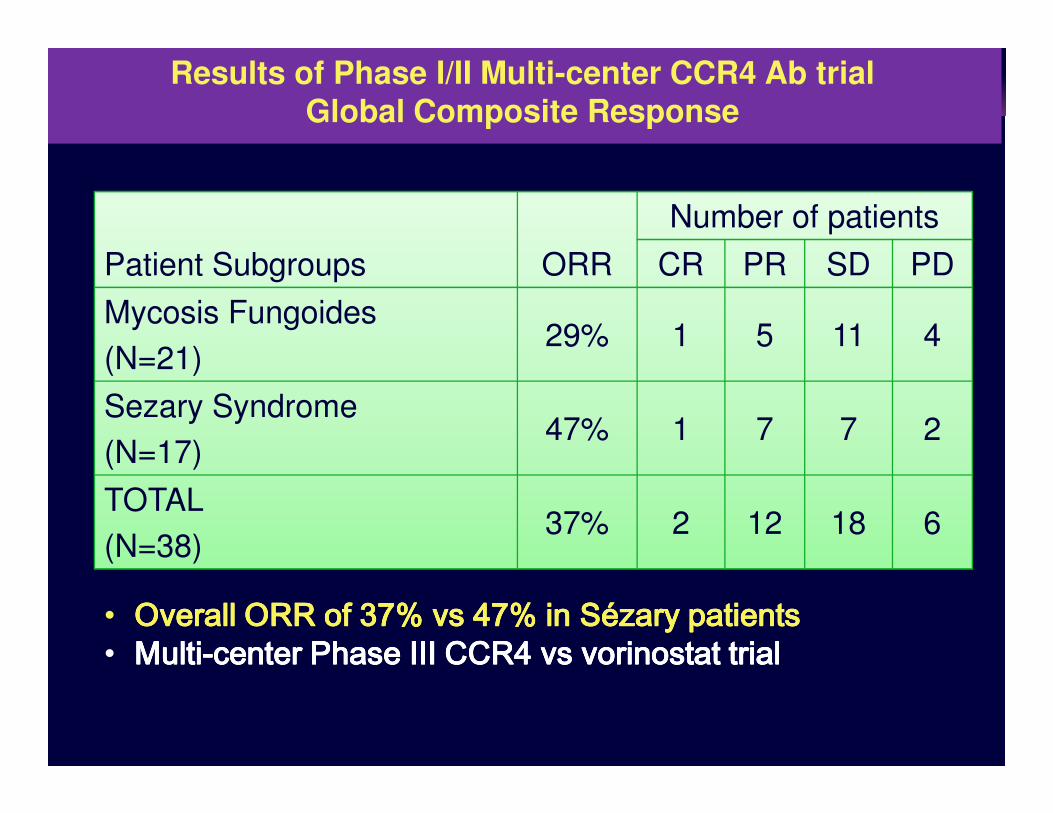
Patient Subgroups ORR
Number of patients
CR PR SD PD
Mycosis Fungoides
(N=21)29% 1 5 11 4
Sezary Syndrome
Results of Phase I/II Multi-center CCR4 Ab trialGlobal Composite Response
Sezary Syndrome
(N=17)47% 1 7 7 2
TOTAL
(N=38)37% 2 12 18 6
• Overall ORR of 37Overall ORR of 37Overall ORR of 37Overall ORR of 37% vs 47% in % vs 47% in % vs 47% in % vs 47% in SézarySézarySézarySézary patients patients patients patients • MultiMultiMultiMulti----center Phase III CCR4 center Phase III CCR4 center Phase III CCR4 center Phase III CCR4 vsvsvsvs vorinostatvorinostatvorinostatvorinostat trial trial trial trial
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
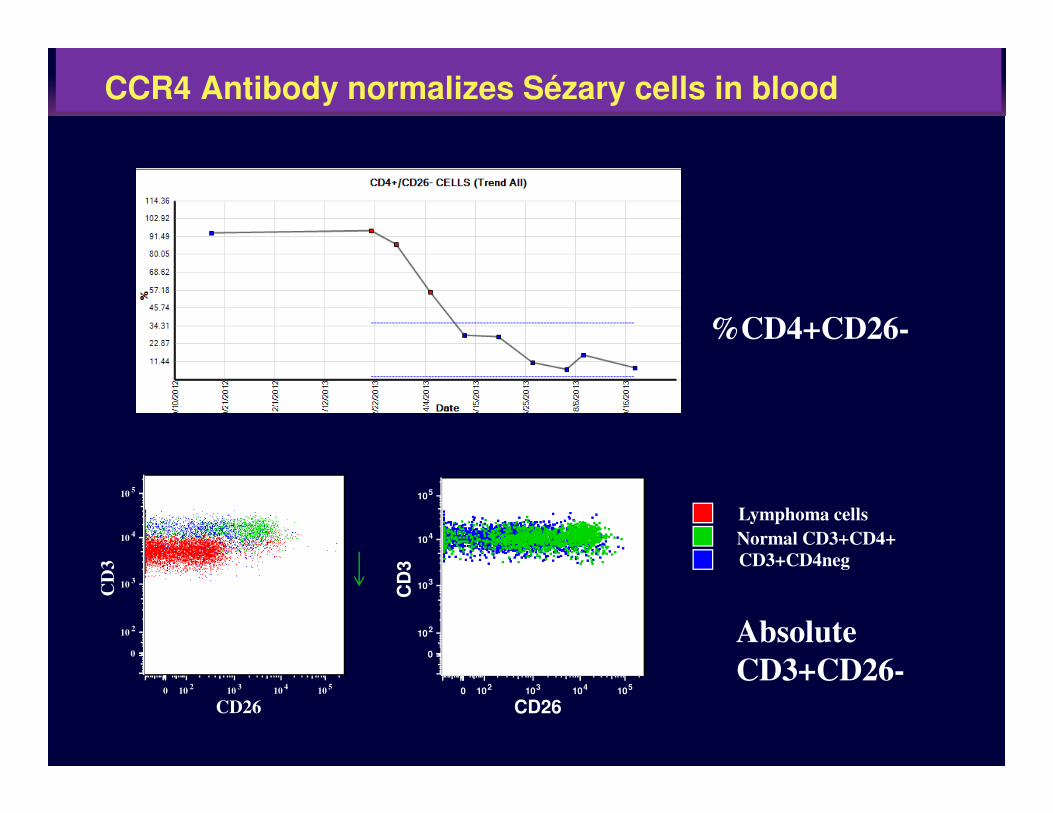
%CD4+CD26-
CCR4 Antibody normalizes Sézary cells in blood
Absolute
CD3+CD26-0 10
210
310
410
5
CD26
0
102
103
104
105
CD
3
0 102 103 104 105
CD26
0
102
103
104
105
CD
3 CD3+CD4neg
Normal CD3+CD4+
Lymphoma cells
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Reduction of regulatory T cells by Mogamulizumab, a defucosylated anti-CC chemokine receptor 4 antibody, in patients with aggressive/refractory mycosis fungoides and Sézary syndrome.
Ni X, Jorgensen JL, Goswami M, Challagundla P, Ni X, Jorgensen JL, Goswami M, Challagundla P, Decker WK, Kim YH, Duvic M.
Clin Cancer Res. 2015 Jan 15;21(2):274-85. doi:
10.1158/1078-0432.CCR-14-0830. Epub 2014 Nov 5
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
0.80
1.20
1.60
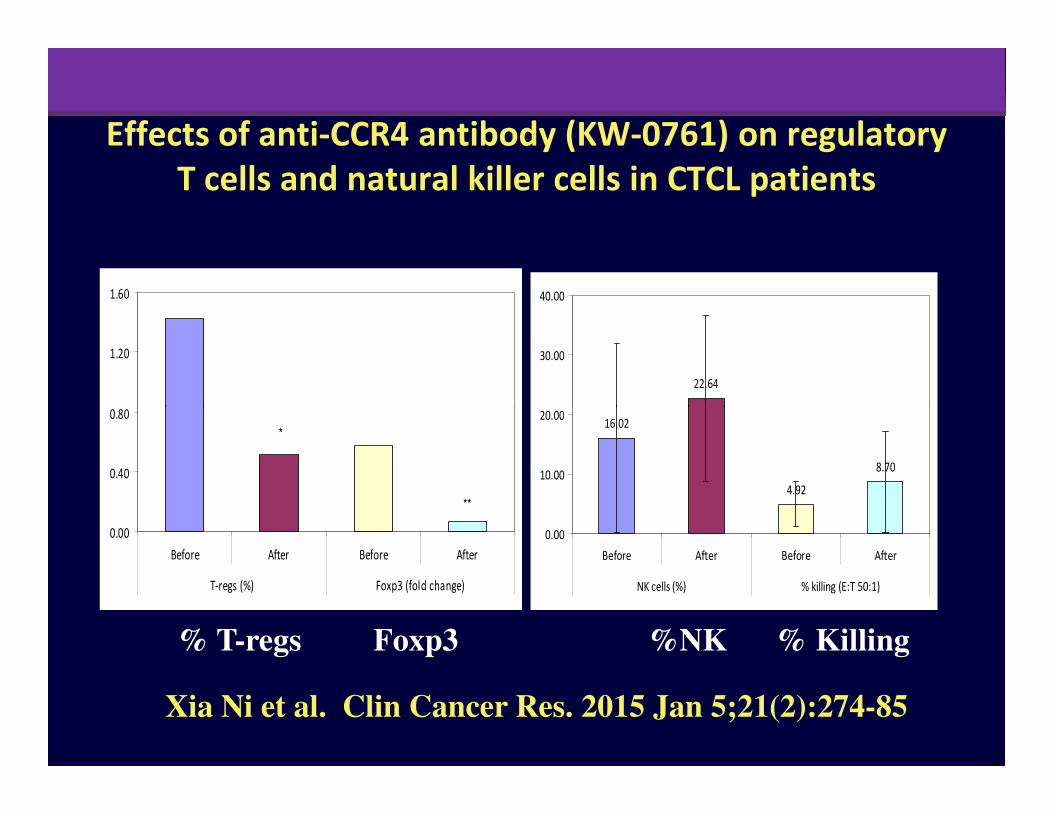
22.64
20.00
30.00
40.00
Effects of anti-CCR4 antibody (KW-0761) on regulatory
T cells and natural killer cells in CTCL patients
**
*
0.00
0.40
0.80
Before After Before After
T-regs (%) Foxp3 (fold change)
16.02
4.92
8.70
0.00
10.00
20.00
Before After Before After
NK cells (%) % killing (E:T 50:1)
Xia Ni et al. Clin Cancer Res. 2015 Jan 5;21(2):274-85
% T-regs Foxp3 %NK % Killing
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
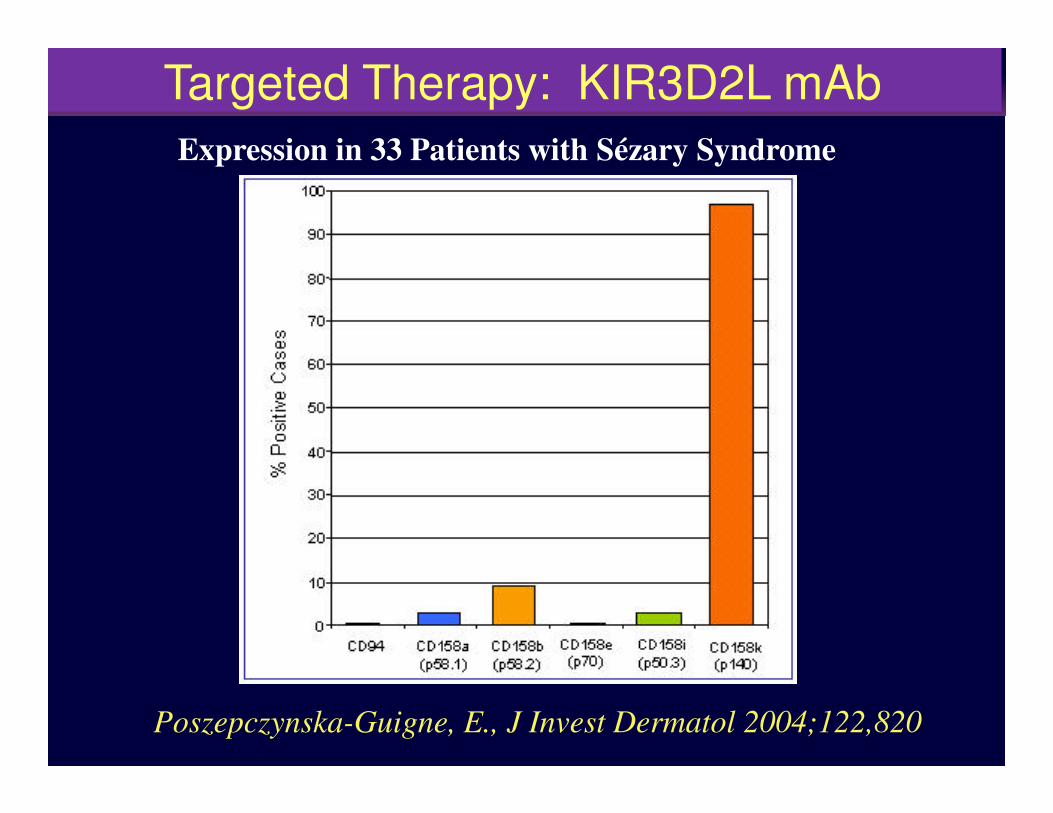
Expression in 33 Patients with Sézary Syndrome
Targeted Therapy: KIR3D2L mAb
Poszepczynska-Guigne, E., J Invest Dermatol 2004;122,820
clinicaloptions.com/oncology
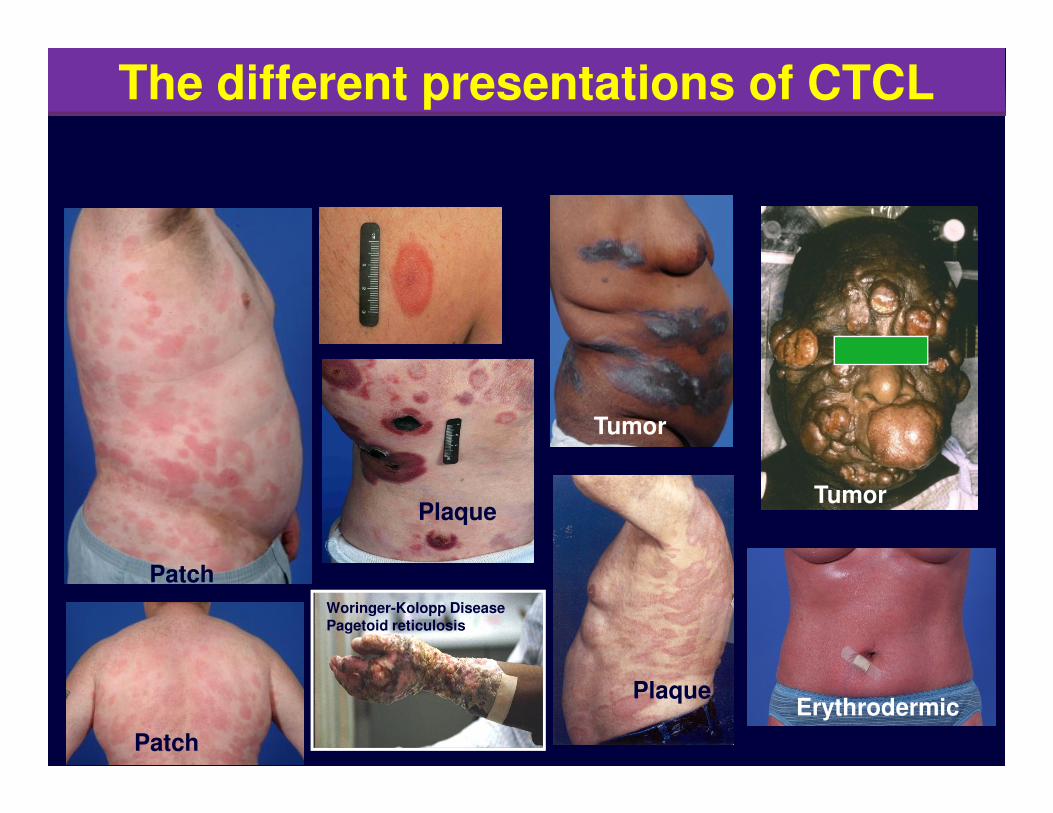
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeThe different presentations of CTCL
Patch
Patch
Plaque
Woringer-Kolopp DiseasePagetoid reticulosis
Erythrodermic
Tumor
Tumor
Plaque

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
EpidermotropicLarge cell
Tumor stage
+/- large cell
Large cell
Transformation?
Advanced >IIB: Tumors (LCT), Nodes, Blood, Viscera
Large cell
Spread to Blood
Sezary syndrome
+/- large cell
Systemic Large Cell
Transformation (LN)Refractory
Disease
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeP
rob
ab
ility
of
Pro
gre
ssio
n-f
ree
Su
rviv
al
0.6
0.8
1.0
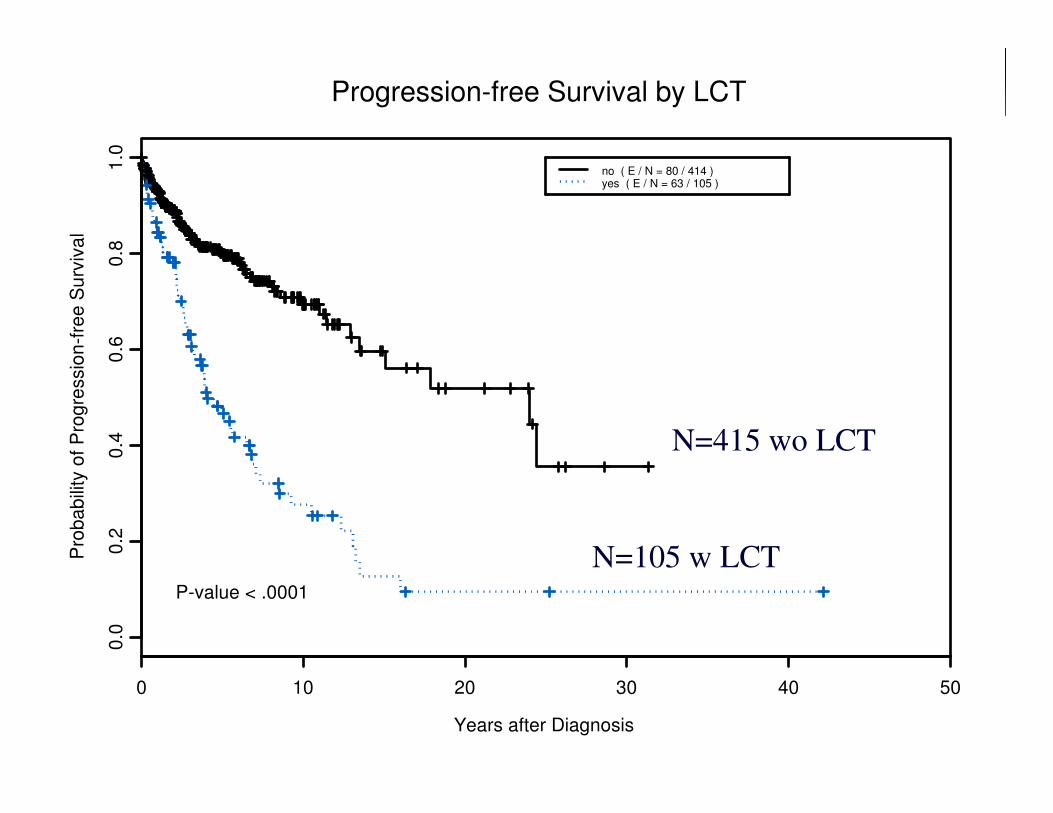
no ( E / N = 80 / 414 )yes ( E / N = 63 / 105 )
Progression-free Survival by LCT
Years after Diagnosis
Pro
ba
bili
ty o
f P
rog
ressio
n-f
ree
Su
rviv
al
0 10 20 30 40 50
0.0
0.2
0.4
P-value < .0001
N=105 w LCT
N=415 wo LCT
clinicaloptions.com/oncology
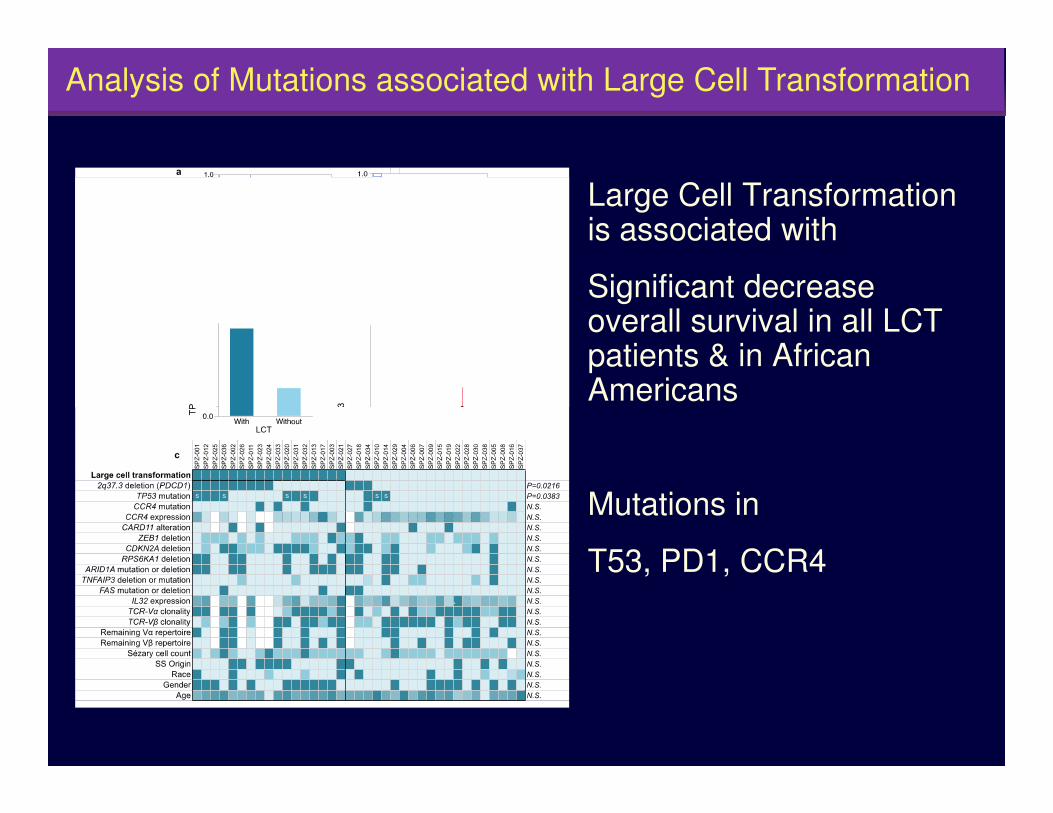
Current Concepts in T-Cell Lymphoma: Applying Evidence to PracticeAnalysis of Mutations associated with Large Cell Transformation
Large Cell Transformation is associated with
Significant decrease overall survival in all LCT patients & in African AmericansAmericans
Mutations in
T53, PD1, CCR4
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
SP
Z-0
30
SP
Z-0
14
SP
Z-0
36
SP
Z-0
20
SP
Z-0
12
SP
Z-0
13
SP
Z-0
31
SP
Z-0
25
§
SP
Z-0
01
SP
Z-0
10
SP
Z-0
32
SP
Z-0
34
SP
Z-0
33
SP
Z-0
16
SP
Z-0
23
§
SP
Z-0
21
SP
Z-0
06
SP
Z-0
19
SP
Z-0
02
SP
Z-0
18
SP
Z-0
27
SP
Z-0
17
SP
Z-0
07
SP
Z-0
03
SP
Z-0
29
SP
Z-0
05
SP
Z-0
26
§
SP
Z-0
09
SP
Z-0
28
SP
Z-0
22
SP
Z-0
15
SP
Z-0
11
SP
Z-0
24
§
SP
Z-0
04
¶
SP
Z-0
08
SP
Z-0
37
SP
Z-0
38
Histopathological data
Age <60 ≥60 ≥70 ≥80
Race W B H AI
Stage IVA IVB IB
Gender Male Female
SS origin de novo Pre-MF
LCT Without With
Vital status Alive Dead
� � � �
� � �
� �
Somatic mutationsCCR4
CARD11
FAS
Nonsense
Splicing siteRPS6KA1
ZEB1
Frame-shift
TP53
ARID1A
RHOA
0
5
10
15 M
uta
tio
n p
er
Mb
Silent
Nonsilent
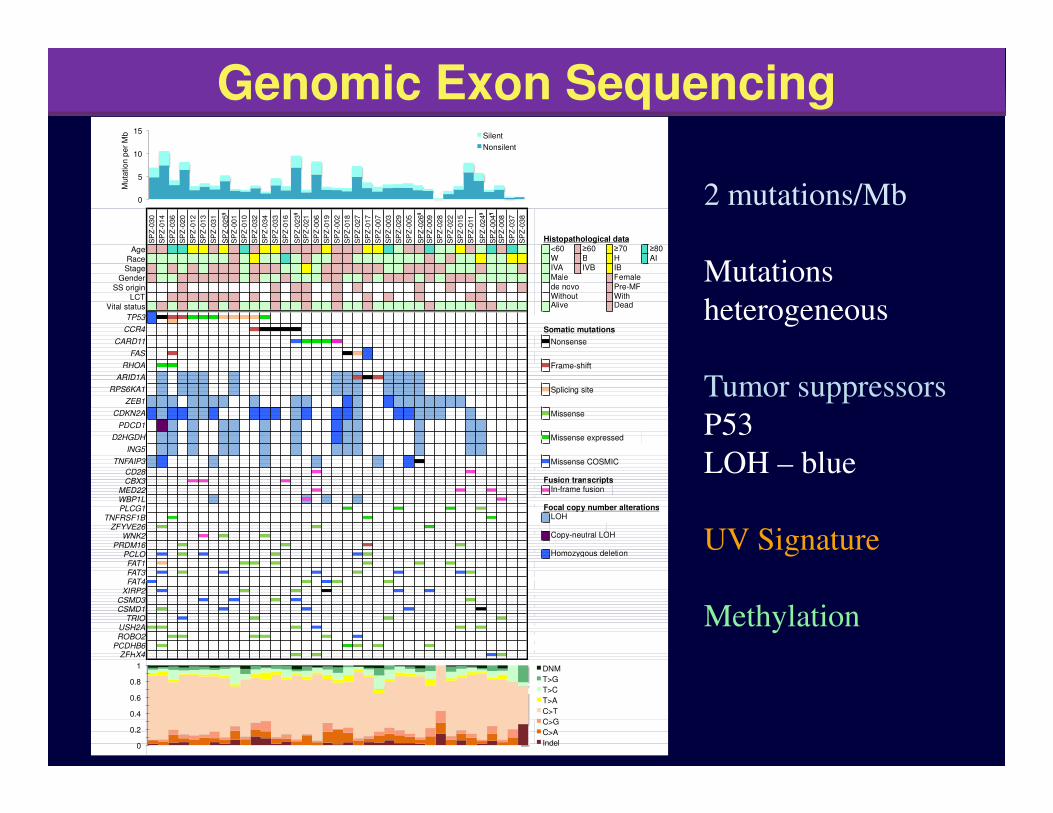
Genomic Exon Sequencing
2 mutations/Mb
Mutations
heterogeneous
Tumor suppressors
P53 �
� � �
� � �
�
�PCDHB6
PLCG1TNFRSF1B
ZFYVE26
CD28
USH2AROBO2
CSMD1
ZFHX4
FAT4
D2HGDH
ING5
XIRP2
FAT1FAT3
PCLOPRDM16
CBX3MED22WBP1L
WNK2
TNFAIP3
CSMD3
Copy-neutral LOH
Missense
Missense expressed
TRIO
Homozygous deletion
Focal copy number alterationsLOH
Missense COSMIC
Fusion transcriptsIn-frame fusion
CDKN2A
PDCD1
0
0.2
0.4
0.6
0.8
1 DNM
T>G
T>C
T>A
C>T
C>G
C>A
Indel
P53
LOH – blue
UV Signature
Methylation
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
1p
36
.1
2q
37
.3
7p
14
.1
7q
34
14
q1
1.2
9p
21
.3
MYC STAT5A/5B
ARID1
A
PDCD1
D2HGD
H
ING5
CDKN2A
CDKN2BTRG TRB
TCF3
19
p1
3.3
TP53
17
p1
3.1
10
p1
1.2
3
10
q2
3.3
1
FAS
ZNF438
ZEB1
100%
50%
0%
0%
50%
100%
TRA
DLEU1
DLEU2
13
q1
4.2
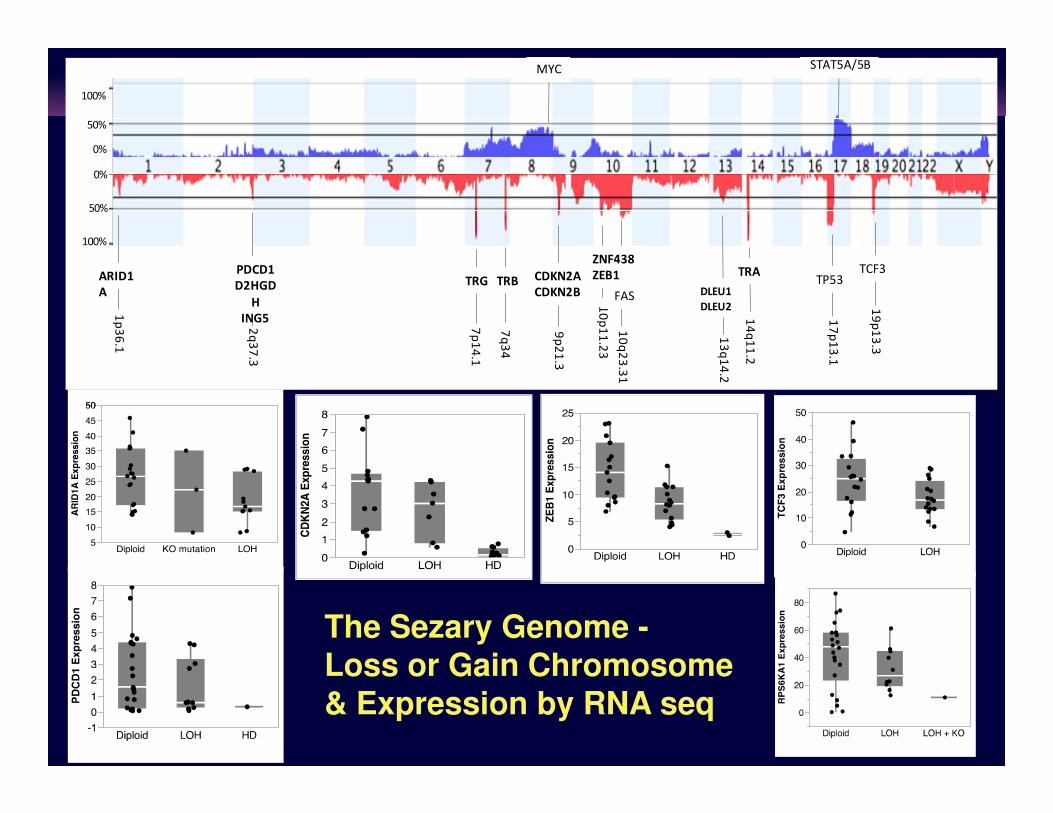
The Sezary Genome -Loss or Gain Chromosome& Expression by RNA seq

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
G1
S G2
M
G0
G1/S Checkpoint
G2/M Checkpoint CDK2
CCNE1
RB1 E2F
CCND1
CCND3
CDK4
MYC
CDKN2A
FD-58%
M-3%
M-3%
BA-39%
M-3% BD-39%
TP53 M-30%
FD-3% BD-72%
E2F
HIC1 HOXA9
ARID1A FD-33% M-8%
CDKN1A
FD-11%
CDK1
CCNB1
ATR M-5%
ATM
CDC25C
CDC25A/B
M-3%
CHEK1/2
CREBBP M-3%
EP300 M-3%
M: Somatic mutation FD: Focal deletion BA: Broad amplification BD: Broad deletion F: Gene fusion
Up: Upregulated %: Percentage of cases altered
RPS6KA1
FD-33%
ARID3A
Up (56%, 5.5-fold)
a
PATHWAYS TO THE FUTURE
�
EP300 M-3% %: Percentage of cases altered BD-41%
α β
TCR/CD3
CD
4
PT
PR
C
CD
28
CT
LA
4
PD
CD
1
CA
CN
M-42% F-5% FD-36%
ICO
S
PI3K M-13% F-3%
Cell proliferation Survival
ZAP70
GRB2
RAS
M-5%
Ca2+
NFAT
M-8%
NFAT AP-1
Ca2+
Ca2+
ITPR1/3
M-13%
CAMK2
M-8%
CREB
LA
T
SOS1
PLCG1
M-3%
M-11%
LCP2
ITK PIP2
DAG
M-3%
PTPN11
PTPN6
LCK
CDC42
MAPK8
M-3%
JUN
M-5%
ATF2
PRKCQ
MAP3Ks
M-13% IKBKB
M-3%
CARD11
M-13%; F-3%
BCL10
MALT1
NF-κB
RAC
Up (88%, 8.6 fold)
Up (53%, 5.4 fold)
F-3% F-3%
Up (53%, 5 fold)
b
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Why is the SS cell nucleus cerebriform?
� Why are SS patients red? Staph toxins? AMPs?
� Why do they acquire keratoderma? 60% Tinea+
� Why are they cold? Vasodilation, VEGF, low TSH
� Why to they itch? opiate receptor mediated, IL-31
Questions Remaining
� Why to they itch? opiate receptor mediated, IL-31 from CCR4+ cells killed by HDAC-inhibitors
� What genes or epigenetic changes drive T cell proliferation? Making progress – T cell signalling
� Can we cure SS? 79% SS cured with TBSEB and non-ablative allogeneic transplant and target therapy for others.
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Spatz & Anderson Foundations, Blanche Bender Chair, NCI, Dermatology Foundation, companies for financial support for trials and translational research.
� Lab and Clinical Research: Xia Ni, Lisa Shuie, R Talpur, C-L Zhang, Clinical Research Fellows, Derm Residents, medical students.
Acknowledgments
� Baylor Genome Center- D. Wheeler, Linghua Zhang
� CTCL family – colleagues/friends throughout the world who take care of CTCL patients and support each other: USCLC, EORTC, ISCL, CLIC

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice

clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
Naomi Kanof Lecture75th SID Meeting May 8, 2015
Silencing the Sézary cellPast, Present, & Future
Madeleine Duvic, MD
Prof of Dermatology &
Internal Medicine
Blanche Bender Chair in
Cancer Research
Dept of Dermatology
MD Anderson Cancer Center
Houston, Texas
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Attended NYU medical school, mentored by DrSulzberger and became editor of the Journal of Investigative Dermatology x 17 years. She married a lawyer, had two children in Washington DC.
� Dedicated to her patients, Chief of Pediatric
Who was Naomi Kanof?
� Dedicated to her patients, Chief of Pediatric Dermatology at Washington Hosp Center
� She knew political figures – Wilber Mills’ Fanny Fox. She and Scoop Jackson raised funds for Sulzberger chair & start the Military Dermatology Program- John Stanley first job.
� (S. Katz, unpublished data)
clinicaloptions.com/oncology
Current Concepts in T-Cell Lymphoma: Applying Evidence to Practice
� Duke Medical School - Duke Triple Threats: Lowell
Goldsmith, Gerald Lazarus, S. Pinnell & Brian
Jegasothy. Master clinicians: J Lamar Callaway, Robert
Gilgor, Mike Tharp, Janet Hickman.
� Elizabeth Kanoff (Naomi’s cousin) taught “how to run an
office and divert curbside consults.”
Pathway Analysis
office and divert curbside consults.”
� NIH immunology 3rd year elective- Fauci, Anderson,
Waldmann. First scientific paper – improved the lives
of NZB/W mice w estrogen inhibitor. Saw first SS pt.
� Clinical Research can help more people than a private
practice and collaborate with interesting people.