sinusitis
TRANSCRIPT
Postgraduate course presentation
Sinusitis
Eugene 6. Kern, M.D. Rochester, Minn.
Sinusitis broadly means any inflammatory process that involves the sinuses. The most common in- flammation of the sinuses is the common cold. This paper will discuss the various aspects of acute, sub- acute, and chronic suppurative (bacterial) sinusitis, including predisposing factors, differential diagnosis, management, and complications.
PATHOPHYSIOLOGY
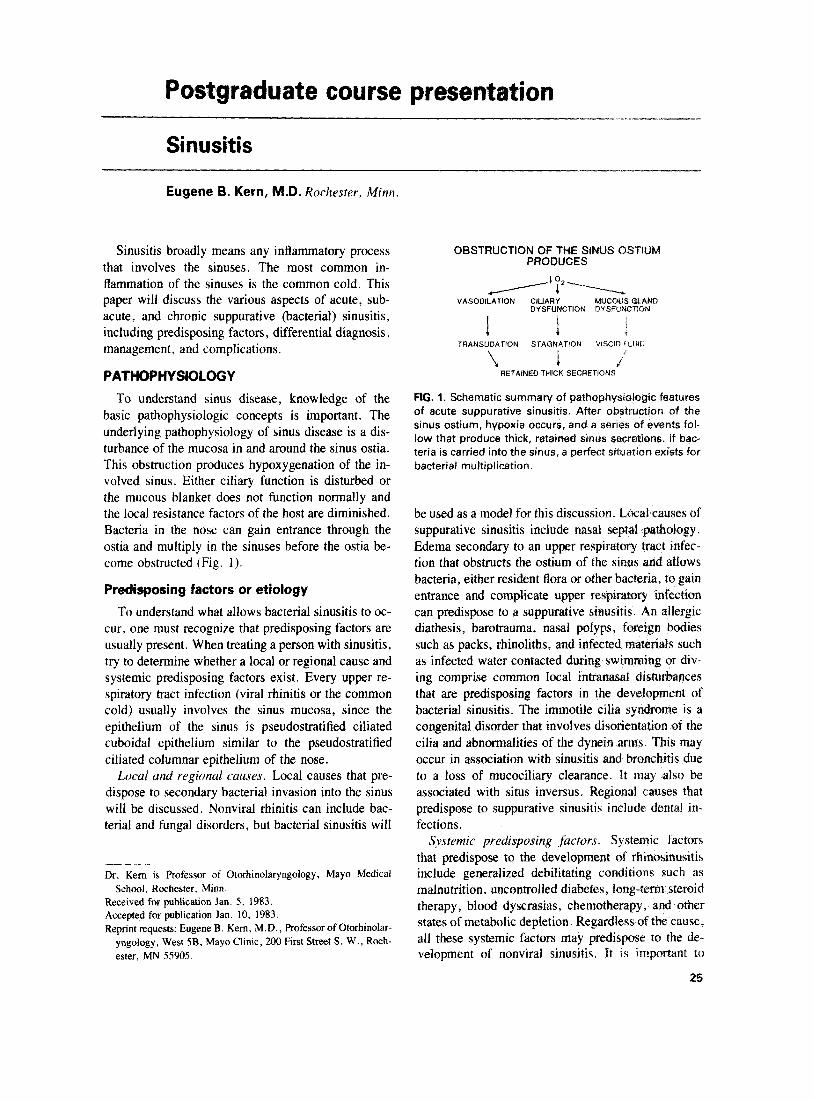
To understand sinus disease, knowledge of the basic pathophysiologic concepts is important. The underlying pathophysiology of sinus disease is a dis- turbance of the mucosa in and around the sinus ostia. This obstruction produces hypoxygenation of the in- volved sinus. Either ciliary function is disturbed or the mucous blanket does not function normally and the local resistance factors of the host are diminished. Bacteria in the nose can gain entrance through the ostia and multiply in the sinuses before the ostia be- come obstructed (Fig. I).
Predisposing factors or etiology
To understand what allows bacterial sinusitis to oc- cur, one must recognize that predisposing factors are usually present. When treating a person with sinusitis, try to determine whether a local or regional cause and systemic predisposing factors exist. Every upper re- spiratory tract infection (viral rhinitis or the common cold) usually involves the sinus mucosa, since the epithelium of the sinus is pseudostratified ciliated cuboidal epithelium similar to the pseudostratified ciliated columnar epithelium of the nose.
Local and regional causes. Local causes that pre- dispose to secondary bacterial invasion into the sinus will be discussed. Nonviral rhinitis can include bac- terial and fungal disorders, but bacterial sinusitis will
Dr. Kern is Professor of Otorhinolaryngology, Mayo Medical School, Rochester, Minn.
Received for publication Jan. 5, 1983. Accepted for publication Jan. 10, 1983. Reprint requests: Eugene B. Kern, M.D., professor of Otorhinolar-
yngology , West 5B, Mayo Clinic, 200 First Street S. W , Roch- ester. MN 55905.
OBSTRUCTION OF THE SINUS QSTIUM PRODUCES
VASODILATION MUCOLIS GLAND DYSFUNCTION DYSFUNCTION
TRANSUDATION STAGNATION VISCIO i LlllU
\, i A’ RETAINED THICK SECRETIONS
FIG. 1. Schematic summary of pathophysiologic features of acute suppurative sinusitis. After obstruction of the sinus ostium, hypoxia occurs, and a series of events fol- low that produce thick, retained sinus secretions. If bac- teria is carried into the sinus, a perfect situ&ion exists for bacterial multiplication.
be used as a model for this discussion. Local causes of suppurative sinusitis include nasal septal pathology. Edema secondary to an upper respiratory tract infec- tion that obstructs the ostium of the sinus and allows bacteria, either resident flora or other bacteria, to gain entrance and complicate upper respiratory infection can predispose to a suppurative sinusitis. An allergic diathesis, barotrauma, nasal polyps, foreign bodies such as packs, rhinoliths, and infected materiab <such as infected water contacted during swimming or div- ing comprise common local intranasai disturbances that are predisposing factors in the development of bacterial sinusitis. The immotile cilia syndrome is a congenital disorder that involves disorientation of the cilia and abnormalities of the dynein arms. This may occur in association with sinusitis and bronchitis due to a loss of mucociliary clearance. tt may also be associated with situs inversus. Regional causes that predispose to suppurative sinusitis include dental in-
fections. Systemic predisposing factors. Systemic factors
that predispose to the development of rhinosinusitis include generalized debilitating conditions such as malnutrition, uncontrolled diabetes, long-term steroid therapy, blood dyscrasias , chemotherapy, and other states of metabolic depletion. Regardless of the cause, all these systemic factors may predispose to &he de- velopment of nonviral sinusitis. It is important to
25

J. ALLERGY CLIN. IMMUNOL. JANUARY 1984
26 Kern
TABLE 1. Suppurative sinusitis
Acute Chronic
Pain +4 -
Nasal obstruction +4 +2 Nasal discharge +4 +2 Systemic symptoms +4 -
+4 = severe; +2 = mild or moderate; - = not present.
identify the predisposing factor not only to effect proper management but also to remove the cause, especially when it is local or regional. Controlling the underlying predisposing factor is important in the long-term management of recurrent rhinosinusitis.
CLASSIFICATION A classification of sinusitis based on pathology is
useful in patient management. In addition to naming the involved sinus, the classification should contain some concept as to the duration of the sinus infection.
Acute suppurative sinusitis
Arbitrarily, acute suppurative sinusitis is any in- fectious process in the sinus lasting from 1 day to 3 wk.
Subacute suppurative sinusitis
Subacute suppurative sinusitis is a sinus infection that lingers from 3 wk to approximately 3 mo. The epithelial changes in the sinuses are usually reversible in the acute and subacute phases. Irreversible changes usually occur after 3 mo of subacute sinusitis, leading into the next or chronic phase.
Chronic suppurative sinusitis
The chronic phase begins somewhere around 3 mo and lasts indefinitely. Thus, if a sinus infection has persisted for longer than 3 mo, the condition is known as chronic suppurative sinusitis. In general, chronic sinusitis is either inadequately treated or untreated acute sinusitis and must be surgically treated, since the irreversibly diseased mucosa must be removed and sinus ventilation and drainage must be accom- plished for resolution.
An example of the terms used in describing the diagnosis of sinusitis for a bacterial infection is “acute suppurative right maxillary sinusitis. ” It is important to identify (1) the sinus involved, (2) the involved side, and (3) how long the process has been present.
SYMPTOMS Symptoms of nonviral sinusitis relate to the loca-
tion of the sinus involved and whether the individual is suffering from acute, subacute, or chronic sinusitis.
In general, Table I will be useful in a consideration of acute and chronic sinusitis. The most frequent symp- toms of acute suppurative sinusitis include pain, nasal obstruction, nasal discharge, and systemic symptoms that include febrile reactions and other constitutional phenomena such as malaise and lethargy.
Pain In acute sinusitis, the patient usually has pain over
the infected sinus; if it is frontal sinusitis, the pain is frontal pain; if it is ethmoid sinusitis, it is ethmoid pain, which includes pain in the medial portion of the nose, or retro-orbital pain; if it is sphenoid sinusitis, the patient usually has vertex headaches; and if it is maxillary sinusitis, the patient will have pain in the cheek or face.
Nasal discharge and systemic symptoms In acute suppurative sinusitis, the patient usually
has a mucopurulent yellow to green nasal discharge that is either unilateral or bilateral. With the history of a previous upper respiratory tract infection, a predis- posing factor, usually both sides become involved and systemic findings are frequent. Laboratory findings of an elevated erythrocyte sedimentation rate and in- creased white blood cell count (leukocytosis), asso- ciated with a febrile course and constitutional symp- toms of lethargy and malaise may occur. In chronic sinusitis, the patient usually has a mucopurulent dis- charge and symptoms of mild nasal obstruction, but pain and the systemic symptoms are conspicuously absent. The patient usually is not febrile and does not complain of headache or facial pain.
Nasal obstruction and other symptoms
Remember that acute sinusitis can be superimposed on an already chronically infected sinus! With maxil- lary rhinosinusitis, the patient may also complain of dental pain, nasal airway obstruction, and much puru- lent discharge. Not infrequently the sinus inflamma- tion begins in one sinus and, because the ostia of the maxillary, ethmoid, and frontal sinuses drain into the middle meatus, the inflammation spreads to the other sinuses. Involvement of all the sinuses is called pan- sinusitis. The patient therefore may have symptoms related to inflammation of all the sinuses.
Periorbital edema may also be present when the ethmoid or frontal sinuses are involved, because of their close proximity to the eye. It should also be noted that both sphenoid and ethmoid sinusitis can produce occipital, vertex, or parietal pain, pain at the root of the nose, retro-orbital pain, or pain radiating down into the neck.
With exacerbations of acute suppurative sinusitis (recurrent rhinosinusitis), predisposing factors should

TABLE II. Relation of antibiotic dosage to serum concentration --
Route and dose
Antibiotic Intravenous Intramuscular
I_ .-.-..._ ._“._ -. -- ._.. --.- ___
Peak serum -I _I -_ concentration
Oral bglmll --mm. --
Crystalline PCN G 1-5 million units q. 4-6 h.
-
- -
Procaine PCN G 0.3-1.2 million unitb q. 6-12 h.
-
-
Phenoxymethyl PCN V - Benzathine PCN -
Methicillin Oxacillin Dicloxacillin Ampicillin Amoxicillin Carbenicillin
Cephalothin Cefazolin Cephalexin Erythromycin Clindamycin
Vancomycin Streptomycin Kanamycin
Gentamicin Tobramycin Tetracycline Chloramphenicol Colistin
1-2 gm q. 4-6 h. 0.5 gm q. 4-6 h.
-
I .2 million units q. 2-4 wk
1-2 gm q. 4-6 h. 0.5-2 gm q. 6 h.
-
0.5-2 gm q. 4-6 h. -
0.5-2 gm q. 6 h. -
20-40 gm/day in 6 doses
0.5-l gm q. 6 h
0.25-l gm q. 4-6 h. 0.125- 1 gm q. 4-6 h. 0.25-l gm q. 6 h. 0.25-1 gm q. 8 h. 0.5-I gm q. 6 h.
1-2 gm q. 4-6 h. 0.5-I gm q. 4-8 h.
-
0.5-l gm q. 6 h. 0.6-2.7 gm/day in 2-4
doses 0.5 gm q. 6 h.
-
15 mg/kg/day in 2
-
1 gm q. 4-6 h. 0.25-I gm q. 6-12 h
-
0.2 gm q. 4-6 h. 300 mg q. 6-X h.
0.25-l gm q. 6 h.
0.25-l gm q. 6 h. 150-300 mg q. 6 h.
doses 1-2 mg/kg q. 8 h. 1-2 mg/kg q. 8 h. 0.25 gm q. 6 h. 0.5-I gm q. 6 h.
- 0.5-l gm q. 12 h. 15 mg/kg/day in 2
doses 1-2 mg/kg q. 8 h. 1-2 mg/kg q. 8 h.
- -
2.5-5 mg/kg/day in 2-4
0.25-l gm q. 6 h. 0.25-l gm q. 6 h.
- -
- - -
- -
-
0.25-l gm q. 6 h. -
-
Amphoteticin B doses
0.25-l mg/kg/day in 1 - -
dose
PCN = penicillin.
be sought and complete cultures (general bacterial, acid-fast bacillus, fungi, and anaerobes) should be obtained from the involved sinus directly by puncture and lavage or surgical drainage. In chronic suppura- tive sinusitis, the only complaints may be nasal air- way obstruction and postnasal discharge.
DlFFEREMTIAL DIAGNOSIS The differential diagnosis is usually not difficult.
For acute suppurative sinusitis, the patient must have upper airway obstruction and mucopumlent nasal or postnasal discharge. Visualization of mucopus in the nose or in the nasopharynx, pus adherent to the posterior pharyngeal wall, erythema or edema of the turbinates, and pain over the affected sinus with as- sociated headache and systemic findings of fever in the range of 38.3 to 39.4 C make the diagnosis.
The differential diagnosis of suppurative sinusitis,
depending on whether it is acute or chronic, inctwdes
upper respiratory tract infections (viral rhfnitis), al- lergic rhinitis (seasonal and/or perennial 1, vasomotor reactions, or any other cause of nasal disturbance that produces nasal airway obstruction, which may in- clude benign or malignant tumors of the nose and maxilla (upper jaw). These conditions must be con- sidered and usually can be ruled out easily by merely looking into the patient’s nose.
SINUS ROENTGEN~AMS Sinus x-ray films are taken to help can&m the di-
agnosis of suppurative (bacterial) sinusitis. The stan- dard anteroposterior view or Caldwell’s view, Wa- ter’s view, and the lateral view are routinely taken. The submental vertex view is taken only occasionally. When an invading organism spreads to a sinus, the mucosa and submucosa react with the classic inflam-

28 Kern J. ALLERGY CLIN. IMMUNOL.
JANUARY 1984
matory response: vascular dilation, increase in vascu- lar permeability, and transudation of fluid producing interstitial edema. Clinically this produces edema or swelling of the submucosa of the septum, turbinates, and sinuses. These structures have an increased vas- cularity with associated erythema. When an exudate occurs owing to the bacterial interreaction with the polymorphonuclear leukocytes, a purulent discharge is found. This produces nasal obstruction and muco- purulent-secretions that can drain anteriorly or poste- riorly down the throat or remain in the sinuses.
Roentgenographic manifestations of this pathologic process in the mucosa and submucosa of the sinuses will appear as an increase in radiodensity. This “thickening’ ’ of the “sinus membranes” occurs in allergic rhinitis and vasomotor reactions, and the pri- mary care physician should not treat the roentgeno- graphic findings alone. Since air is normally present in sinuses when a bacterial infection occurs, patho- logic change will produce an increase or thickening of the membranes of the sinus that will be apparent on a roentgenogram, with secretions present in the si- nuses. Air-fluid levels may be found because the transudation of fluid from the submucosa partially fills the sinus cavity as the inflammatory response ensues. When there is polyplike (polypoid) material in the nose, it usually is found in the sinuses, too. Sinus x-ray films are helpful in confirming the diagnosis of acute or chronic suppurative sinusitis, but the major information comes from listening, looking, and feeling.
DIAGNOSIS
The diagnosis of sinusitis is made by history and physical examination and is supported by roentgeno- graphic findings. Roentgenograms may be ordered in cases of acute suppurative sinusitis to determine the extent of involvement, especially when pain and sys- temic features are prominent or when patients are ex- tremely ill or are failing to get well within 1 wk on antibiotic treatment. Transillumination of the sinuses can be used, although the procedure is not as accurate as roentgenography in diagnosing abnormalities in the sinuses. Sinuscopy is an advanced, sophisticated technique and probably should be done only by a rhinologist.
CULTURES Cultures obtained directly from the sinuses are
more accurate than cultures taken from the nose, but the only time such material can be obtained is during a sinus lavage or at the time of surgical exploration. Recognize that an intranasal culture does not always
reflect what is occurring in the sinuses. Cultures should be obtained when the patient is extremely ill (systemic findings and/or, experiencing severe pain) or when the patient is not responding to conventional management (including antibiotics for suppurative sinusitis). When the cultures are obtained, they should be studied for general bacteria, acid-fast bacil- lus, fungi, and anaerobes
MANAGEMENT Management of suppurative characteristic sinusitis
can be broken down into medical management and surgical management. Surgical management can be minor surgical management, office surgery, or operat- ing room intervention.
Medical management
Since most of the acute suppurative sinusitis in- fections are produced by gram-positive organisms, the majority of which are Streptococcus pneumoniae, Staphylococcus aureus, and streptococci (groups A, B, and C) and Haemophilus injluenzae (gram- negative) along with a host of anaerobic organisms, the treatment of choice is penicillin G. Penicillin G is also a good choice as initial and definitive therapy for gram-negative cocci and gram-positive and gram- negative bacilli. Antibiotics are the keystone of medi- cal management in acute suppurative sinusitis. For H. injluenzae, ampicillin or amoxacillin is indicated. For the commonly used antibiotics, see Table II for the relationship of dosage to serum concentration.
The antibiotic therapy should be continued for a minimum of 7 days after the symptoms have disap- peared. The average duration of treatment is 10 days. Because of the poor distribution to the involved sinuses, it is mandatory to maintain adequate antibi- otic levels; otherwise chronic suppurative sinusitis may occur. In addition to striking out against the or- ganism involved, it is important to facilitate drainage and decrease edema around the ostia. Oral deconges- tants and topical nasal decongestant sprays and/or drops are extremely important to facilitate drainage. This is one of the few instances in which use of de- congestant drops (1% phenylephrine) in the nose is beneficial.
Analgesics are important for control of pain, and humidification may be useful at bedtime. Another valuable part of the medical management is to discuss the disorder and the plan of management with the patient. The patient understands that medical man- agement is only a portion of the management and that a surgical procedure may be necessary, either in the office or in the operating room. The patient also

KLUME 73 NLsMPEP 1 Par! 1
should be told that an attempt will be made to deter- mine the predisposing etiologic factors; any such fac- tors will be controlled, and surgery may be necessary.
Surgical management
Surgical management should be considered to facilitate drainage of the involved sinus and to remove the diseased mucosa. This is necessary (1) when complications are threatening, (2) for relief of severe pain, and (3) when the patient is not responding to medical treatment.
Minor .surgical procedures Srrvus IRRIGATION (LAVAGE). The main indication
for maxillary sinus irrigation (lavage) is the presence of mucopurulent material in subacute or chronic max- illary sinusitis, as suggested by history and abnormal x-ray films for fluid levels or the presence of an opaque sinus. The main purpose for maxillary sinus irrigation is to remove mucopumlent material from the involved sinus. Occasionally a unilateral maxil- lary sinus opacity may be seen on a film. This maxil- lary sinus should be irrigated, and the aspirate should be sent for cytologic studies to rule out malignancy. If this study is negative and a tumor is suspected, a surgical exploration of the sinus is indicated. Thus a sinus wash may also be helpful in diagnosis.
ARCYROL PACKS. Argyrol packs may be introduced into the nose after the nose has been decongested with 1% phenylephrine. Argyrol is an astrigent and helps promote drainage of the sinuses.
Major surgicul procedures. The general goals and principles of sinus surgery are to remove diseased mucosa and establish drainage into the nose. This is accomplished by removing obstructions and creating direct continuity from the involved sinus into the in- tranasal space. Adequate sinus ventilation (oxygena- tion) is important. Surgery should be carried out by physicians who are experienced in rhinologic surgery.
MAXII-LARY SINUS SURGERY (OPENING INTO THE INFERIOR MEATUS). A nasoantral window procedure is usually indicated for patients with recurrent rhinosi- nusitis and persistent or chronic suppurative sinusitis with or without polypoid or hypertrophic changes. The purpose of the nasoantral window is to allow or facilitate drainage from the maxillary sinus into the nose. This window is created in the nose under the inferior turbinate in the inferior meatus. The nasoan- tral window also allows access at the time of surgery for the removal of diseased mucosa.
The Caldwell-Luc procedure is usually indicated in cases that fail to improve after the nasoantral window operation. The procedure has a slightly higher mor- bidity consisting mainly of paresthesias or recurrent
intermittent pain if the front wali ~1‘ rhe maxillary sinus has been removed. An incision i\ made in the buccogingival fold under the lip above the gum. A nasoantral window is also included as part of the op- eration. Aggressive removal o!‘ norm4 iurbinate tis- sue of the lateral wall of the nose musl be avoided or serious atrophic changes can occur thar can make the patient miserable.
The advantage that the Caldwell-Luc procedure has over the nasoantral window procedure IS better access and visualization. The Caldwell-Luc operation is es- pecially indicated for patients with a uninasal maxil- lary sinus problem (opaque antrumj that does not re.- spond to sinus irrigation. The possibiltty of a tumor must be ruled out, and this approach t’acilitates ade- quate exposure and biopsy.
ETHMOID SINUS SURGERY. An ethmosdectomy is usually carried out in cases of recurrenr nasal polyps with ethmoid sinusitis. Ethmoids are usually involved, since the polyps seem to originate from the ethmoid labyrinth in most instances. The intranasal approach is generally advocated in experienced hands, and the complication rate is low (less than .3’+t. although blindness and cerebrospinal fluid leak. can (xcur. Bleeding is the most frequent complication. The pro- cedure is used to remove the polypoid obstruction to breathing and to provide adequate drainage of the ethmoid sinuses. An intranasal ethmoidectomy may also be performed as a prelude to frontal smus surgery.
The external ethmoid approach may he necessary for patients with suspected malignancy or as a drain- age or decompression procedure for patients with acute suppurative ethmoiditis with threarened orbital complications. The incision is made in she region 01‘ the brow, usually heals quite well. ar;d i\ rarely noticeable.
FRONTAL SINUS SURGERY, Frontal sinus surgery 1s usually less common than maxillary or ethmoid sinus surgery. The surgery is performed for the same rea- sons as maxillary or ethmoid sinus surgery. Patients are usually seen for evaluation of suppurative disease in the frontal sinus. Not infrequently, patients with intranasal disease or nasal polyps will have change:\ evident on sinus x-ray films and do not require frontal sinus surgery because removal of the obsrructinn of the nasofrontal duct region usually allows the frontal sinus to return to normal. The major reason for frontal sinus surgery is persistent recurrent infection, espe- cially with pain and/or recurrent swelling over the frontal sinus, in patients who have had ;I previous frontal sinus disease.
The intranasal approach is usually designed to es- tablish drainage by removing disease in the region of

30 Kern J. ALLERGY CLIN. IMMUNOL. JANUARY 1984
the frontal sinus duct in the middle meatus and remov- ing any pathologic obstruction.
There are two major reasons for external frontal sinus surgery: (1) an acute frontal sinusitis that does not resolve and (2) complications threaten to occur. When apatient with acute suppurative frontal sinusitis does no6 improve with medical management, then a frontal sinus trephine operation is indicated. An ex- ternal frontal sinus operation is also indicated for pa- tients who have pain and mucopyoceles or recurrent suppurative disease of the frontal sinus. The external incision is in the brow and is usually combined with intranasal surgery in an attempt to reconstitute a nor- mal nasal frontal duct, so that recurrent infections now have a drainage site through the normal nasal frontal duct into the nose.
The so-called osteoplastic flap operation is rarely necessary. The stated indication for the procedure is to obliterate the frontal sinus if the frontal sinus is extremely small. With a large frontal sinus, a com- bined intranasal and external approach, with re- establishment of a normal frontal sinus duct, is pref- erable. Surgery, of course, should be carried out by physicians who are familiar with frontal sinus disease and who know the art of intranasal surgery.
SPHENOID SINUS SURGERY. The same principles apply to sphenoid sinus surgery as apply to the other sinuses. Surgery is indicated for removal of disease, for establishment of drainage, and for biopsy. Patients who have pain (vertex and/or retro-orbital), involve- ment of the cavernous sinus with a cranial nerve palsy (III, IV, or VI), or other impending central nervous system complications should have sinus roentgenog- raphy and sphenoid sinus surgery if such is indicated.
COMPLICATIONS
Complications can occur in patients who have acute or chronic sinusitis. Fortunately, the rate of sig- nificant complications is low, although precise figures are not available. Complications are generally local and related to the involved sinus. However, compli- cations may be more distant from the sinus but are usually regional in location.
Since the eye is a structure essentially surrounded on three sides by sinuses (the frontal above, the ethmoid medially, and the maxillary below), condi- tions affecting these sinuses can by extension involve the orbital contents. Usually acute ethmoid disease, especially in children, and frontal sinus infections, especially in adults, produce the eye findings. The sphenoid may also produce eye findings, but only because of its relationship to the cavernous sinus through which course the third (occulomotor), fourth (trochlear), and sixth (abducens) cranial nerves.
Cellulitis
Cellulitis can occur in response to any one of the inflammatory disorders of the maxillary, ethmoid, or frontal sinuses. Especially with the ethmoid sinus, cellulitis with edema involving the lid is not uncom- mon, especially with young children. Treatment should be aggressive. Cultures should be taken. If antibiotics have been started, then increasing the dos- age should be considered along with hospitalization and ophthalmologic consultation. Penicillin G and amoxacillin are probably the best initial antibiotic choices while cultures are growing.
Abscess The maxillary, ethmoid, frontal, and sphenoid
sinuses can all produce inflammatory reactions that can result in an abscess. For example, the frontal can produce a periorbital or orbital apex abscess; the fron- tal sinus may also produce periorbital abscess with proptosis. Patients must be actively and aggressively treated if an abscess formation is beginning. Appro- priate incision and drainage must be carried out. The orbital apex, in particular, may become involved with an ethmoid or sphenoid abscess and permanent loss of vision may occur. Thus these inflammatory reactions must be treated vigorously. Ophthalmologic and/or neurosurgical consultants should be called in when complications are likely.
Meningitis and cavernous sinus thrombosis
The cavernous sinus may become infected with an inflammatory reaction in the sphenoid sinus. Any one of the sinuses has connections to the ophthalmic circu- lation through the pterygoid vessels. These connect to the cavernous sinus and may produce meningitis and/or cavernous sinus thrombosis. Fortunately, this is an uncommon complication for all of the cases of sinusitis that have affected the human race. Classic findings include changes in sensorium, delirium, spik- ing fever, chemosis, and proptosis. These symptoms and signs lead one to suspect a significant impending complication. Neurologic evaluation must be carried out immediately, and appropriate diagnostic studies should be instituted aggressively. The culprit sinus may have to be drained, and antibiotic therapy must be initiated to avoid the progression of these devastat- ing complications.
Osteomyelitis
Osteomyelitis may occur secondary to a maxillary sinus (antral) puncture or puncture of any sinus during an acute suppurative sinusitis. In general, the only sinus that should be considered for lavage or puncture is the frontal sinus during the acute inflammatory

VCLUME 73 NI!MBER 1, Part ’
stage. The frontal sinus has diploic vessels that may become infected, and osteomyelitis of the frontal sinus may ensue. This must be treated forcefully with high doses of antibiotics to avoid intracranial compli- cations or osteomyelitis. Surgical debridement should be considered by a surgeon interested in sinusology.
Oroantral fistulas
Oroantral fistulas may occur secondary to maxillary sinus complications, with erosion of a maxillary pre- molar or molar tooth. These infections need to be drained. Various flaps can be used to close the fistula; however, an intranasal antrostomy in the inferior meatus must be carried out to drain the maxillary sinus contents into the nose while the fistula is closed with an oral flap.
DISCUSSION WITH THE PATIENT
The patient must be informed that there are various steps in the management of acute and chronic sinusitis. Medical management is mainly indicated for acute sinusitis and is successful in most instances. In the subacute phase, medical management and minor surgical treatment are appropriate and curative in
instances. In the chronic phase of irreversible sal disease, surgical treatment is indicated. A
I-Luc operation is usually indicated in those maxillary sinus disease that are not controlled
an intranasal antrostomy. If there is a unilateral llary sinus involvement and a suspicion of pos- malignancy, then it is important that adequate
ualization be obtained; therefore a Caldwell-Luc pcedure is indicated. The Caldwell portion of the -ration is the sublabial incision above the buc- agingival fold; the Luc portion is the intranasal an- ltrostomy .
Surgery for acute maxillary sinusitis is indicated if &e pain persists for more than 24 to 48 hr (unrespon-
sive to antibiotics) or if there is a threat tri‘ impending complications. Lavage and/or an antral window pm-
cedure is indicated as a way of reliellrrg pressure. In acute ethmoiditis, surgical interventicrn xs indicated if pain persists and/or ophthalmologic complications are imminent. Either an intranasal ethrn~~ldect~~rn~ or an external ethmoidectomy should be I onsidered. The difficulty with an intranasal ethmoidect;,my is persis- tent bleeding. With acute frontal or sphcnold sinusitis in which the pain does not abate within 24 to 48 hr or in which a threat of complication is ltnpending, an external frontal sinus trephination !h indicated. A transnasal sphenoidectomy is indicated for persistent pain and/or threatened complications.
For chronic maxillary sinusitis. an inrranasal antral window is usually the first choice in surgery The concept is to establish drainage and remove the dis- eased mucosa. In addition, removal of obstruction to the ostium is valuable. For chronic ethmoidiris, an intranasal ethmoidectomy to remove nasal airway obstruction, obstruction to the sinus ostfa. and dis- eased mucosa to establish drainage is the surgical treatment of choice. For chronic frontal sinusitis, usually an intranasat ethmoidectomy and frontal sinus surgery with reconstitution of the frontal duct by use of Silastic sheeting are accomplished at the same time. For chronic sphenoid sinusitis. transseptal sphenoidectomy with removal of diseased mucosa and intranasal removal of the face of the sphenoid and enlarging of the sphenoid ostia surgicail\ will usually cure the problem.
REFERENCES
1. Costrini NV, Thomson WM, editors: Manual uf medical rhera-
peutics, ed. 22. Boston, 1977, Little. Brown & Co.
2. van Cauwenberge P, Ekedahl C: Advances in Gnusiris: micro- biological aspects and treatment. Gent, Belgium, i982, Scien-
tific Society for Medical Information