skeletal metastases in malignant tumors prof. dr. nazem shams professor of general surgery &...
TRANSCRIPT

Post-graduate Course
Skeletal Metastases in Malignant Tumors
Prof. Dr. Nazem ShamsProfessor of General Surgery & Surgical
OncologyFaculty of Medicine
Mansoura University

Post-graduate Course
Introduction
Importance of dealing with this subject originating from recent methods of management –even in late terminal cases- for better quality of life rather than aiming for cure.
Post-graduate Course
Metastatic Potential of Tumors
The development of metastasis is a complex and highly selective process that is dependant upon the interplay of host and intrinsic characteristics of tumor cells, adhesive capacities, cell motility, enzyme secretion and others.

Post-graduate Course
Routes of Metastasis
The routes by which cancer cell emboli ordinarily reach the skeleton is the blood stream (venous or arterial).
The role taken by lymphatic is not important due to apparent absence of lymph channels in bone marrow,
There is also a minute role for perineural spread.

Post-graduate Course
Routes of Metastasis
1. Venous Route.
Vertebral venous system which is a network of valveless veins around the spinal dura mater and the vertebrae.
This system has cranial and body wall connection and even connections with the veins in the wall of the vessels of extermities.
When the intrathoracic or intra-abdominal pressure rises, as in coughing or sneezing, a reversed flow in the venous vertebral system can occur.

Post-graduate Course
Routes of Metastasis
2. Arterial Spread:
Cancer cell emboli reaching the lungs by way of caval circulation sometimes pass through the lungs instead of being arrested in them.
Post-graduate Course
Routes of Metastasis
3. Perineural Spread:
Perineural space via the fifth cranial nerve have been speculated.
Post-graduate Course
Theories of Metastasis
1. Anatomical2. Soil & seed3. Surface properties.

Post-graduate Course
Incidence of Bone Metastasis
The overall incidence of skeletal metastasis rates 70% or more.
If one considers the prostate, kidney and thyroid, the incidence of skeletal metastasis in cases which have run their full clinical course.
Sometimes the primary lesion is clinically silent and bone metastasis gives the first information about the presence of tumor as in kidney, lung and pancreas as well as lymphoma.

Post-graduate Course
Sites of Bone Metastasis
The vertebral column particularly in the lumbar area and the sacrum, the rib cage including the sternum, the femoral and humeral shafts, the pelvic bones and the calvarium are the general sites of predilection.
Post-graduate Course
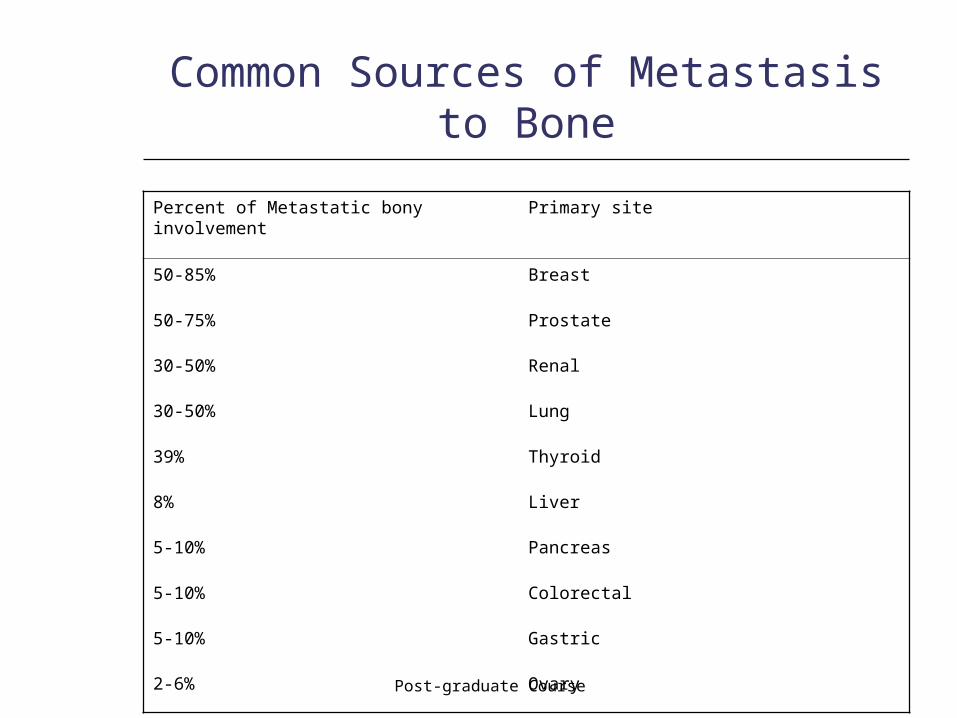
Common Sources of Metastasis to Bone
Primary sitePercent of Metastatic bony involvement
Breast50-85%
Prostate50-75%
Renal30-50%
Lung30-50%
Thyroid39%
Liver8%
Pancreas5-10%
Colorectal5-10%
Gastric5-10%
Ovary2-6%
Post-graduate Course
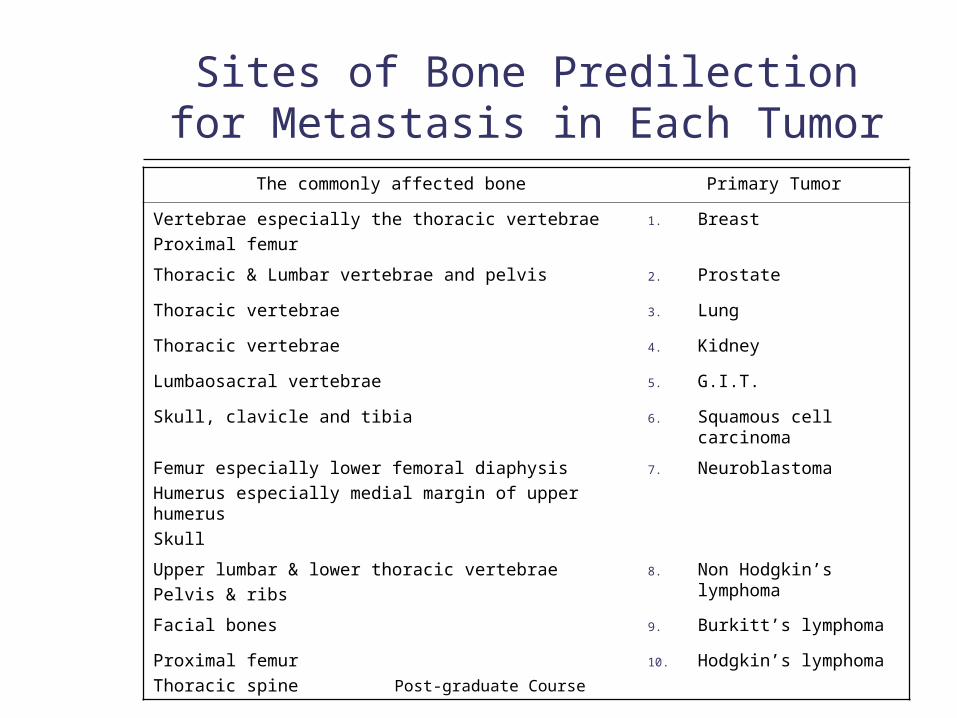
Sites of Bone Predilection for Metastasis in Each Tumor
Primary TumorThe commonly affected bone
1. BreastVertebrae especially the thoracic vertebraeProximal femur
2. ProstateThoracic & Lumbar vertebrae and pelvis
3. LungThoracic vertebrae
4. KidneyThoracic vertebrae
5. G.I.T.Lumbaosacral vertebrae
6. Squamous cell carcinoma
Skull, clavicle and tibia
7. NeuroblastomaFemur especially lower femoral diaphysisHumerus especially medial margin of upper humerusSkull
8. Non Hodgkin’s lymphoma
Upper lumbar & lower thoracic vertebraePelvis & ribs
9. Burkitt’s lymphomaFacial bones
10. Hodgkin’s lymphomaProximal femurThoracic spine
Post-graduate Course
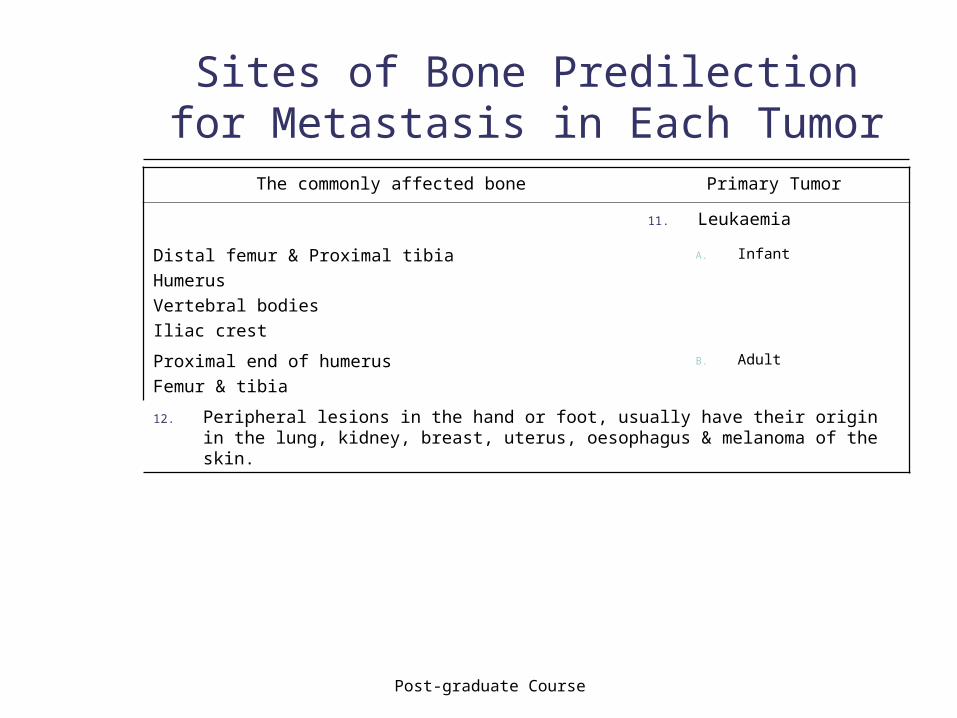
Sites of Bone Predilection for Metastasis in Each Tumor
Primary TumorThe commonly affected bone
11. Leukaemia
A. InfantDistal femur & Proximal tibiaHumerusVertebral bodiesIliac crest
B. AdultProximal end of humerusFemur & tibia
12. Peripheral lesions in the hand or foot, usually have their origin in the lung, kidney, breast, uterus, oesophagus & melanoma of the skin.
Post-graduate Course
Clinical Presentation
1. Pain2. Pathological Fracture3. Swelling4. Neurological Manifestations5. General symptoms6. Paraneoplastic syndrome

Post-graduate Course
Diagnostic Approaches
I. Laboratory Investigations:
1. Blood picture2. Blood glucose3. Blood electrolytes4. Urine5. Enzymes6. Tumor markers
Post-graduate Course
Diagnostic Approaches
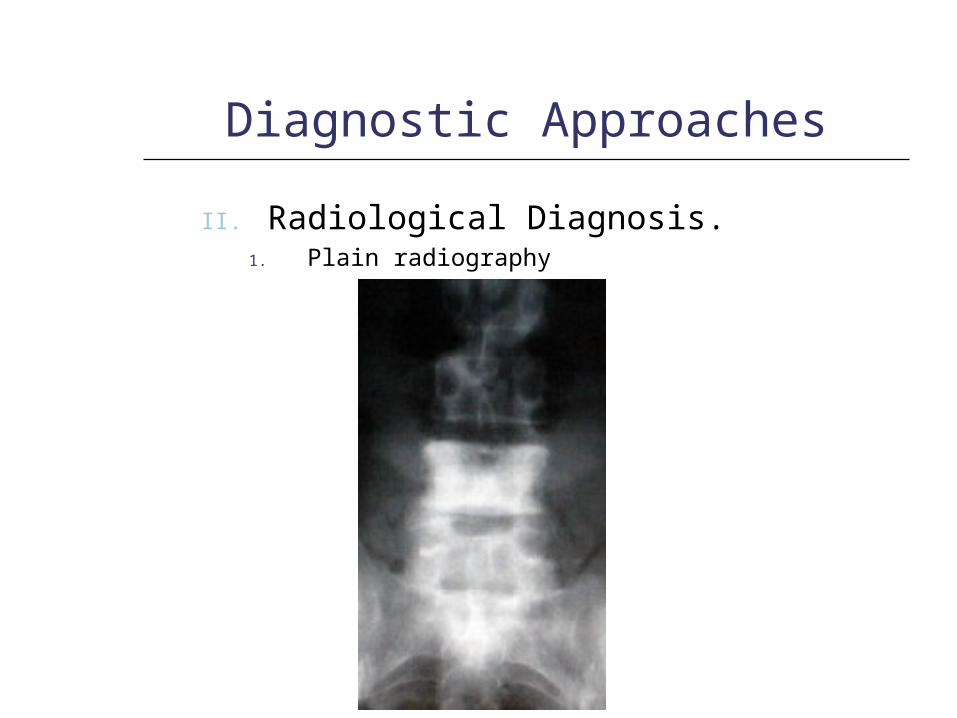
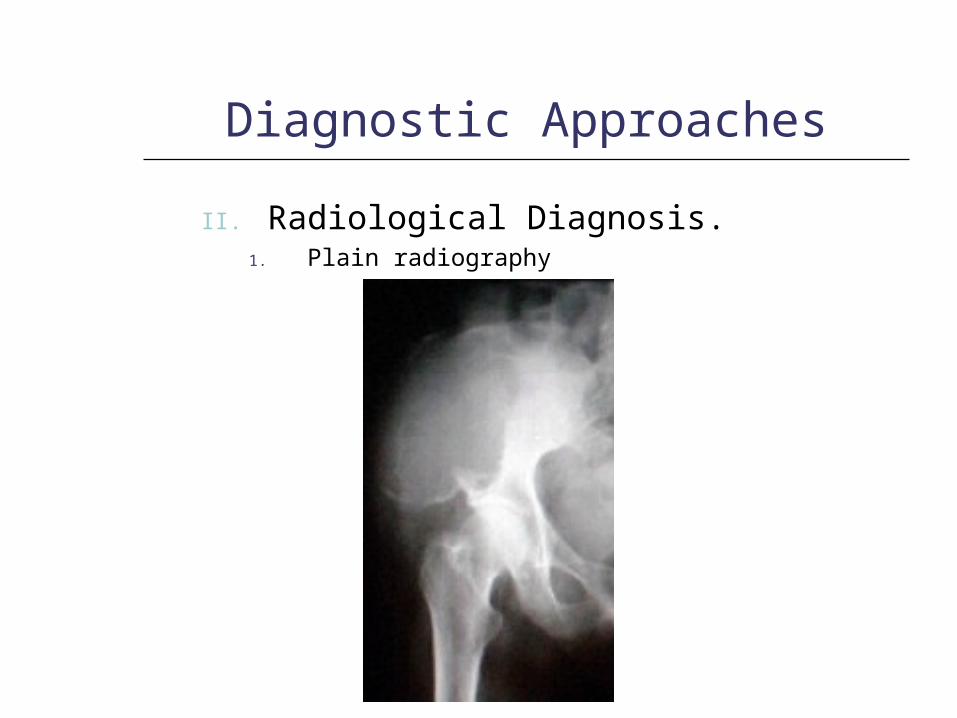
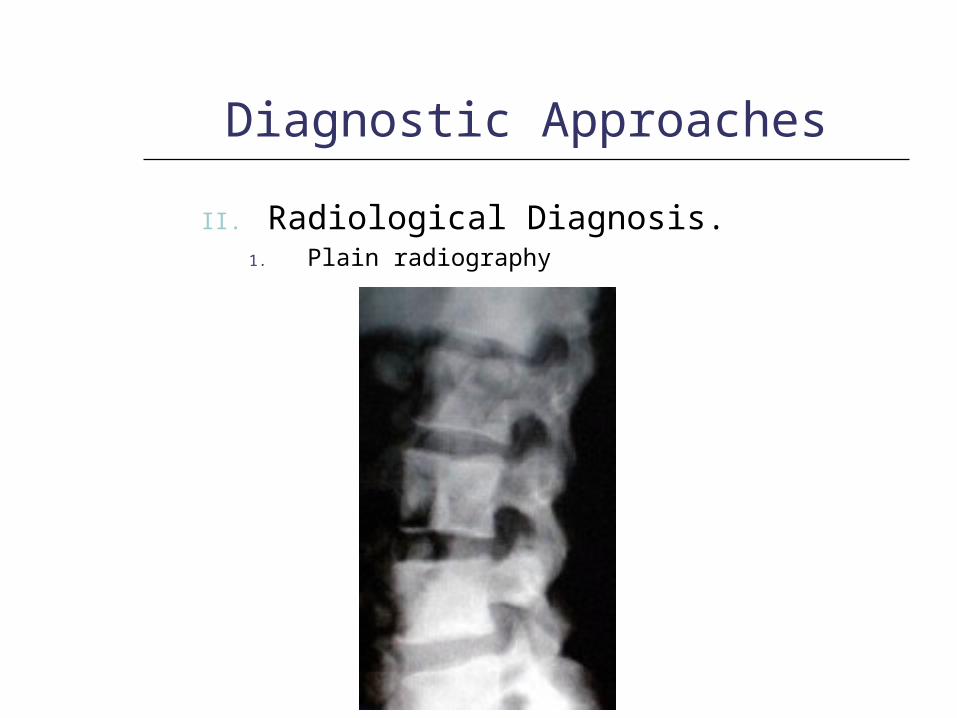
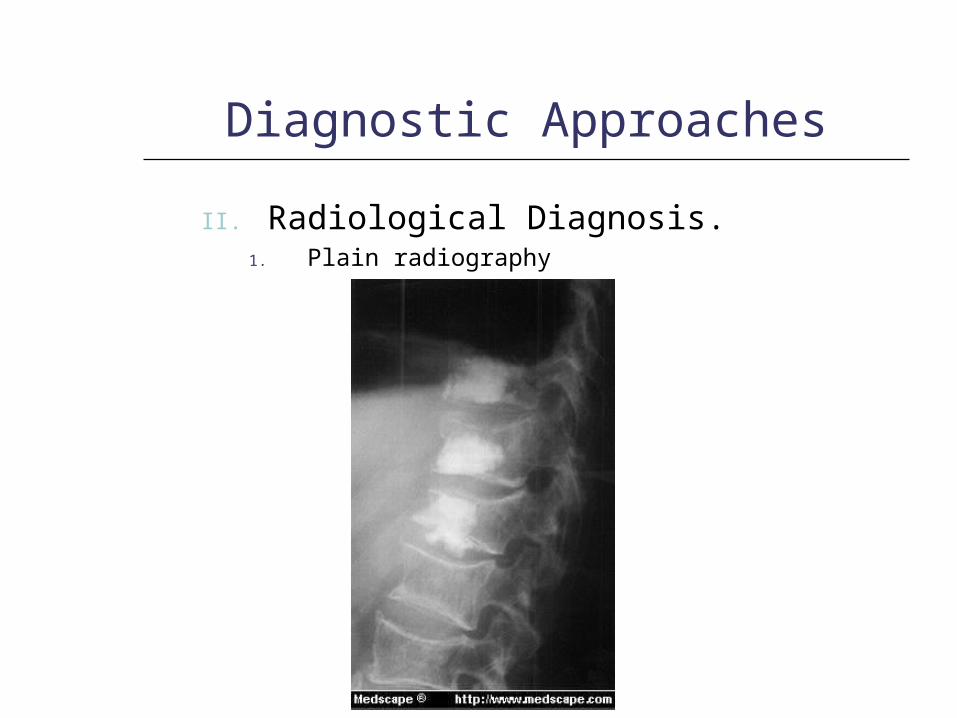
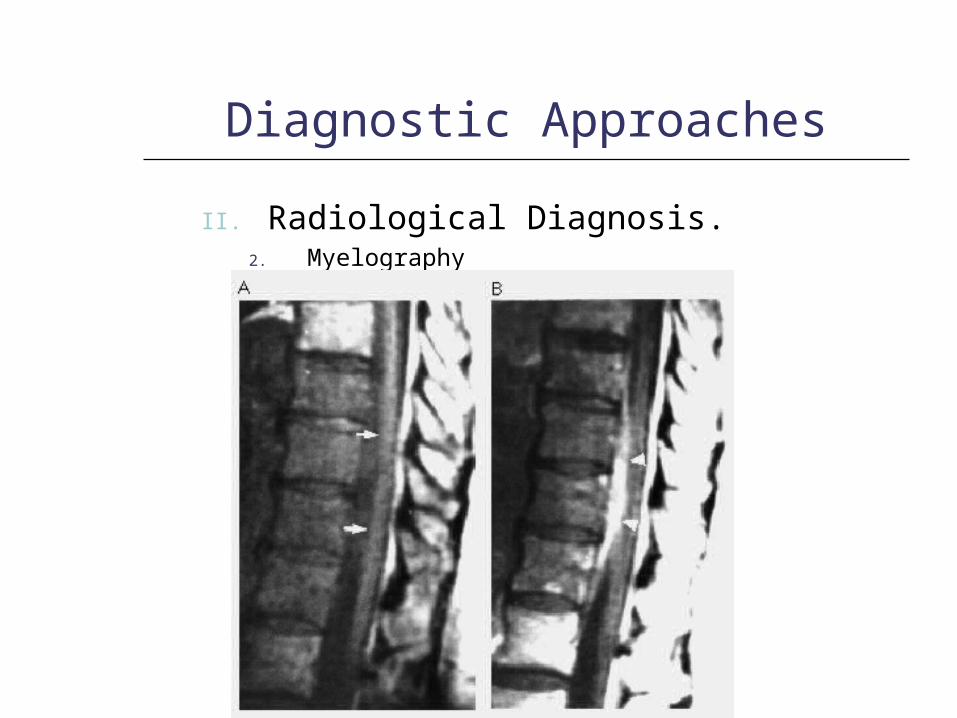
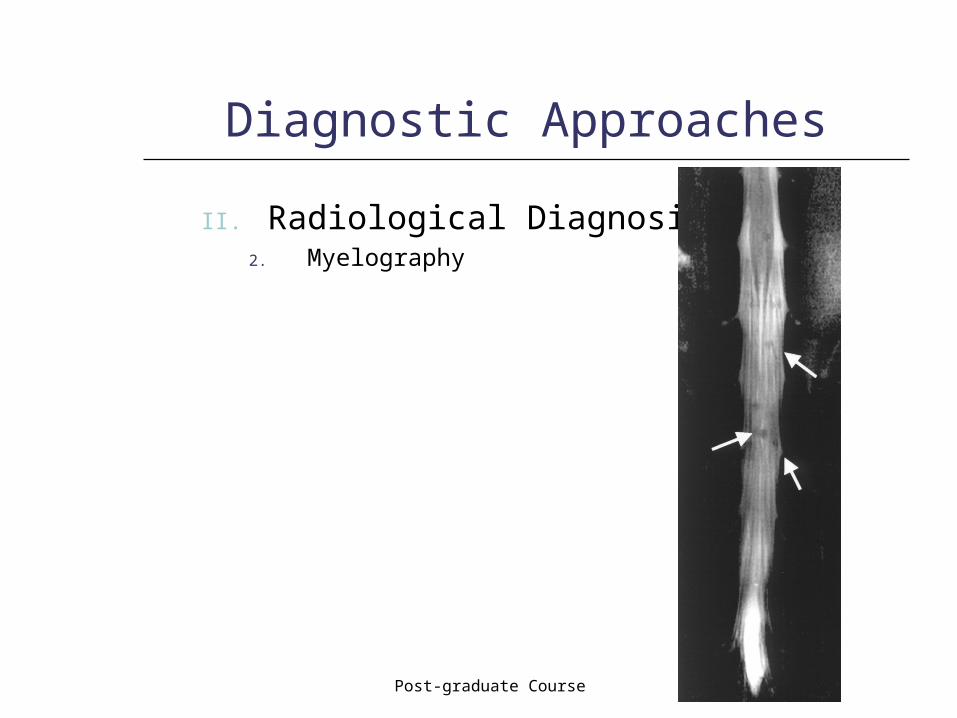
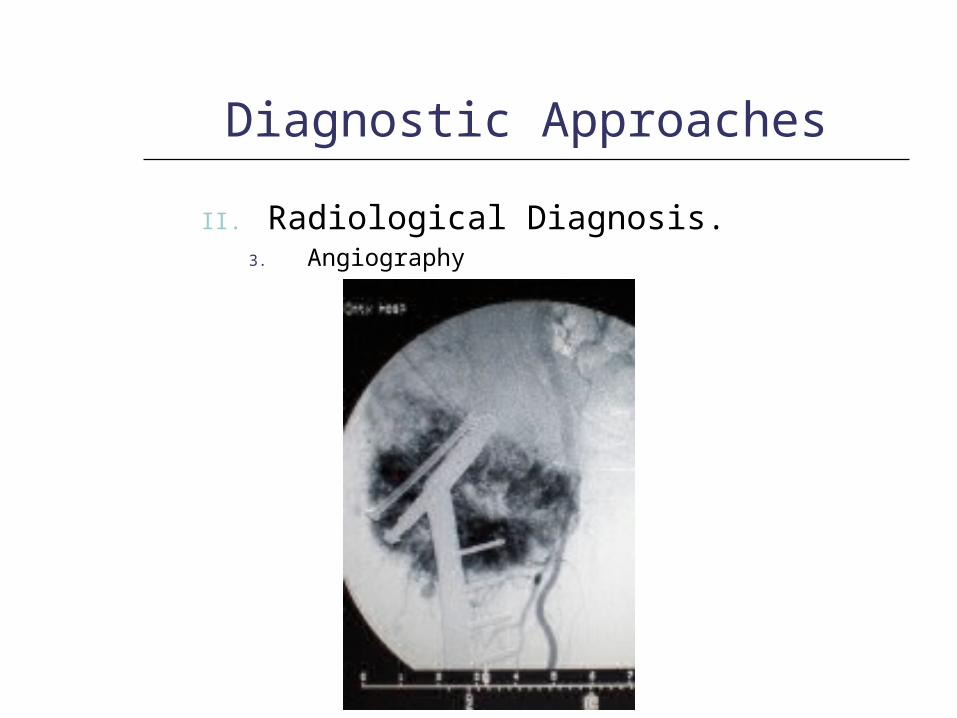
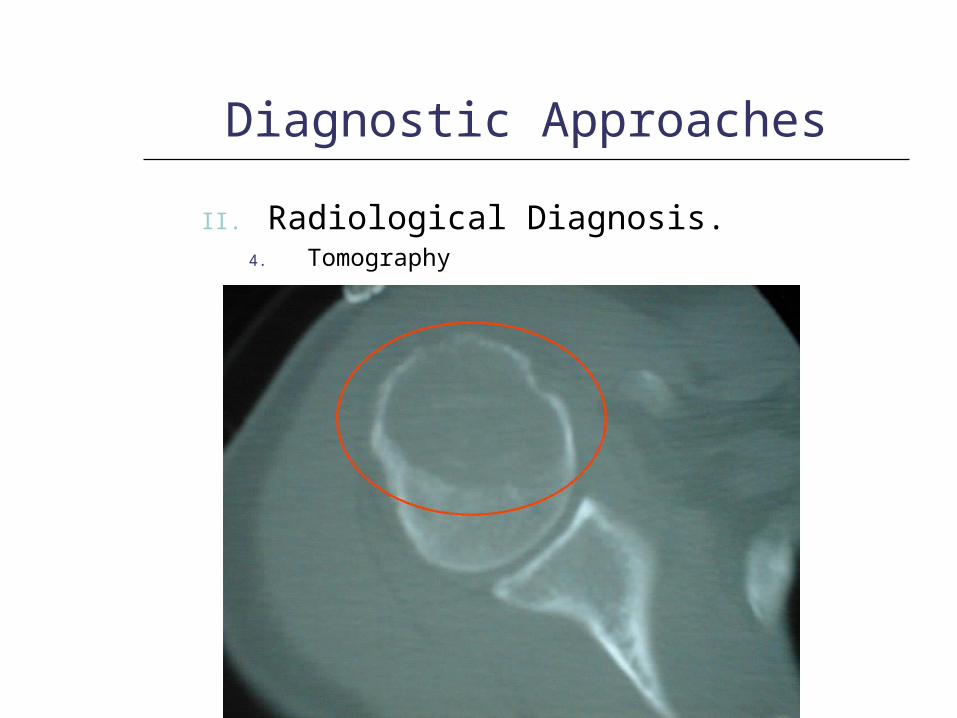
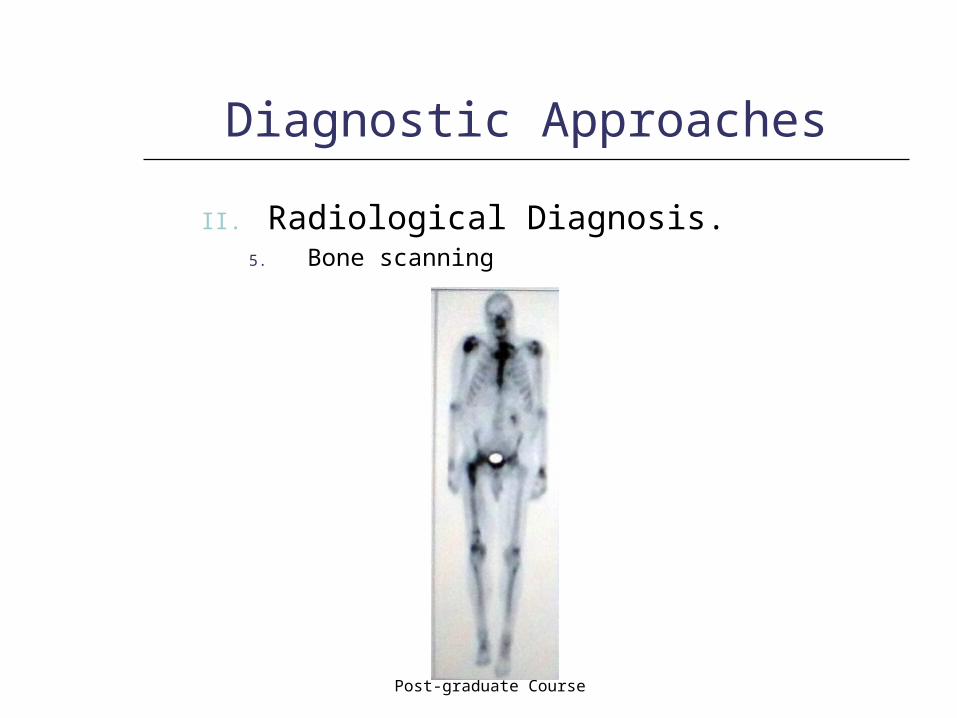
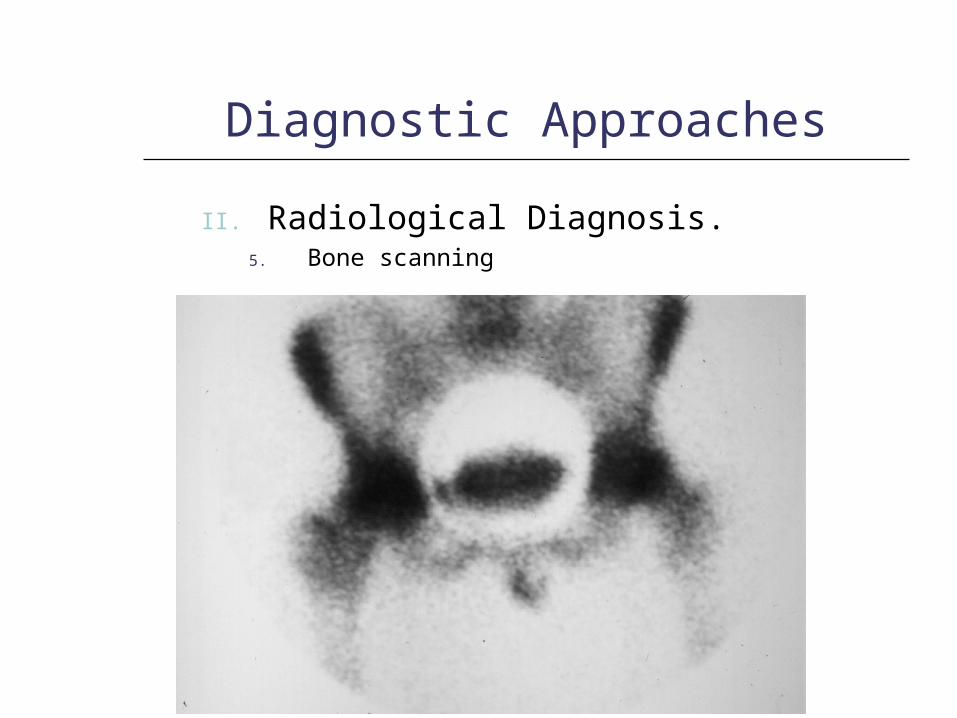
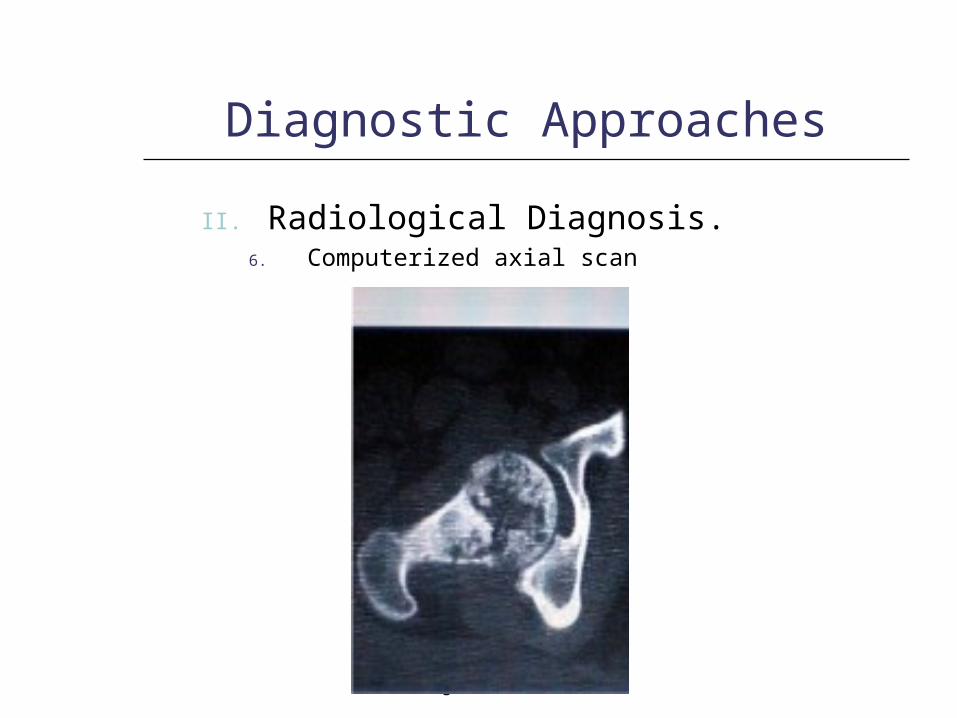
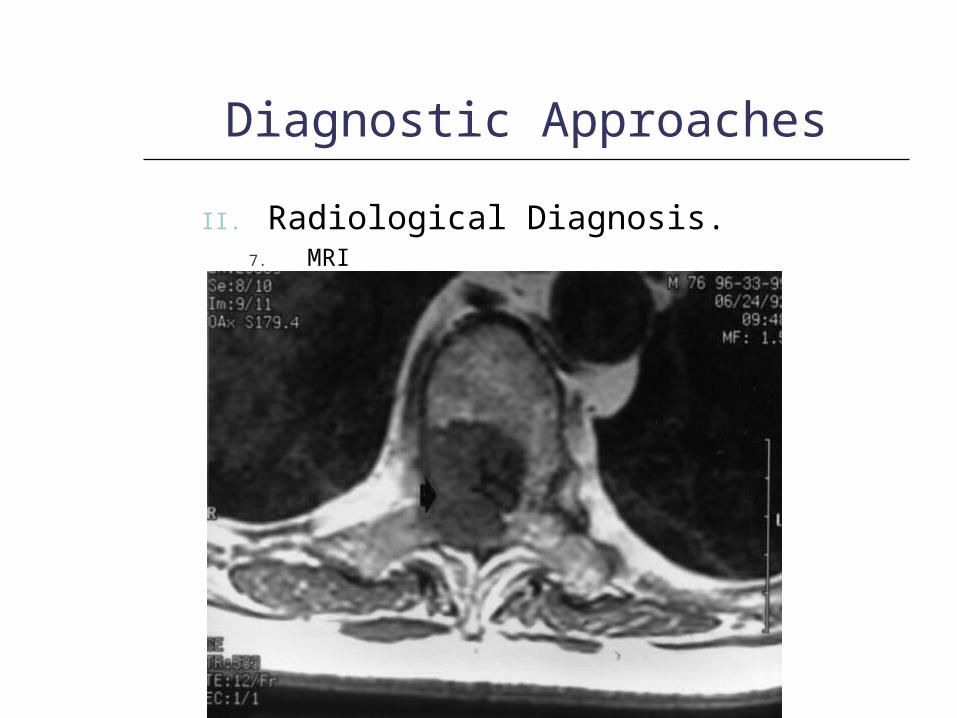
II. Radiological Diagnosis.
1. Plain radiography2. Myelography3. Angiography4. Tomography5. Bone scanning6. Computerized axial scan7. MRI8. PET

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.1. Plain radiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.2. Myelography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.3. Angiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.3. Angiography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.3. Angiography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.4. Tomography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.4. Tomography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.4. Tomography
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.4. Tomography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.4. Tomography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.4. Tomography

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.5. Bone scanning

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.6. Computerized axial scan
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.6. Computerized axial scan

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.7. MRI

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.7. MRI

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.7. MRI
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.7. MRI

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.7. MRI

Post-graduate Course
Diagnostic Approaches
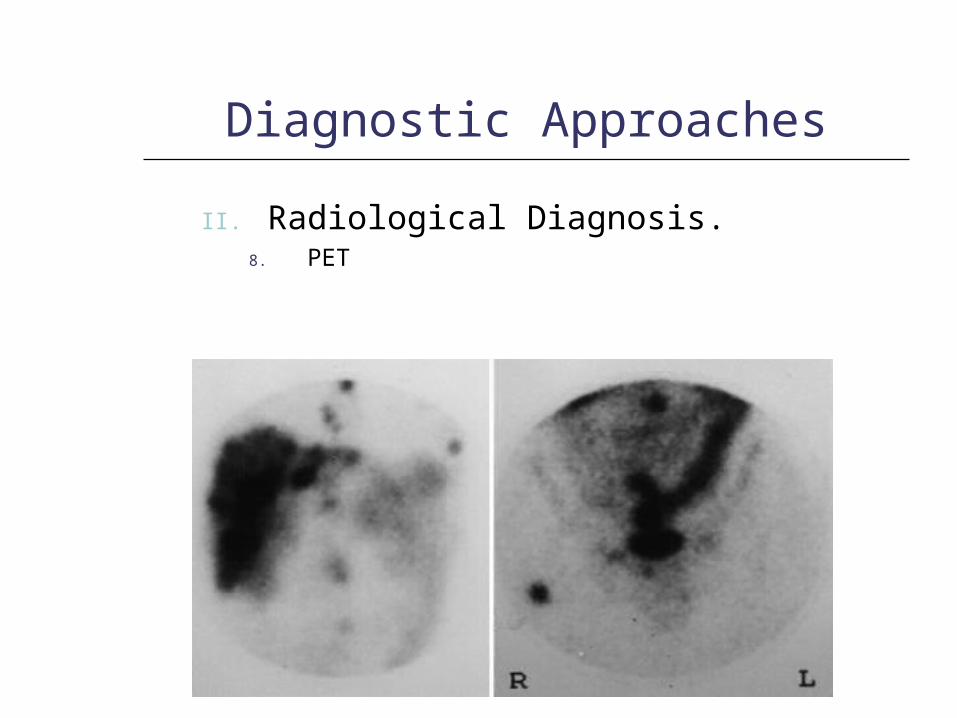
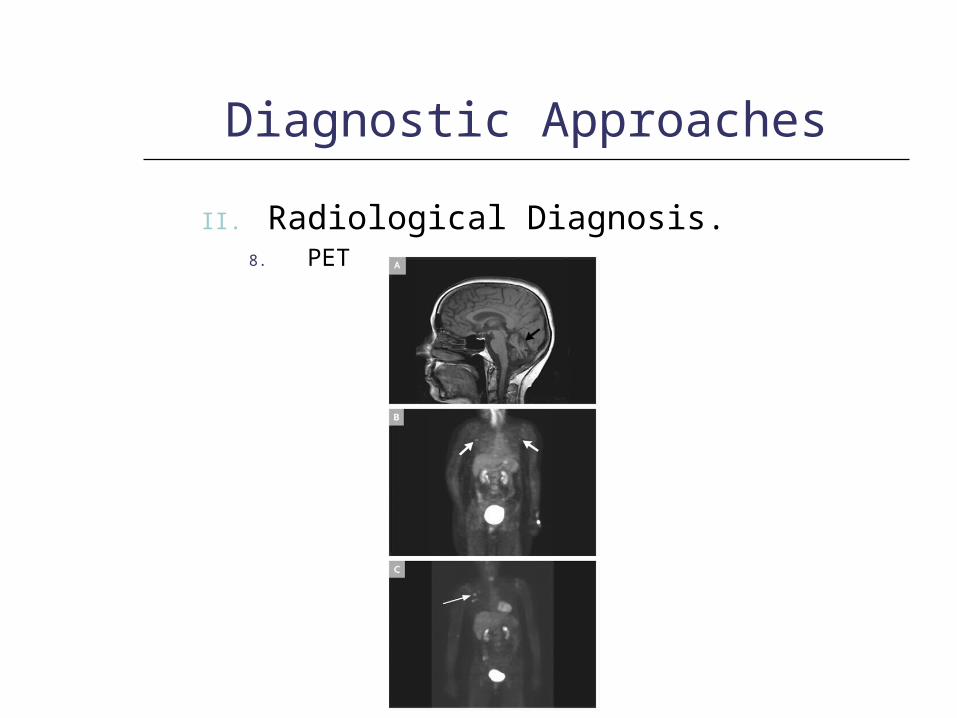
II. Radiological Diagnosis.8. PET

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.8. PET
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.8. PET
Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.8. PET

Post-graduate Course
Diagnostic Approaches
II. Radiological Diagnosis.8. PET

Post-graduate Course
Diagnostic Approaches
III. Biopsy
1. Needle biopsy2. Open biopsy

Post-graduate Course
Types of Skeletal Metastasis
Primary focusUsual type of
skeletal Metastasis
Relative Frequency
Very commonCommonInfrequentRare
BreastLytic and mixedx
Lung
CarcinomaPredominantly lytic
x
CarcinoidPredominantly blastic
x
ProstatePredominantly blastic, lytic in older age group
x
KidneyLytic-expandingX
ThyroidLytic-expandingX
Post-graduate Course
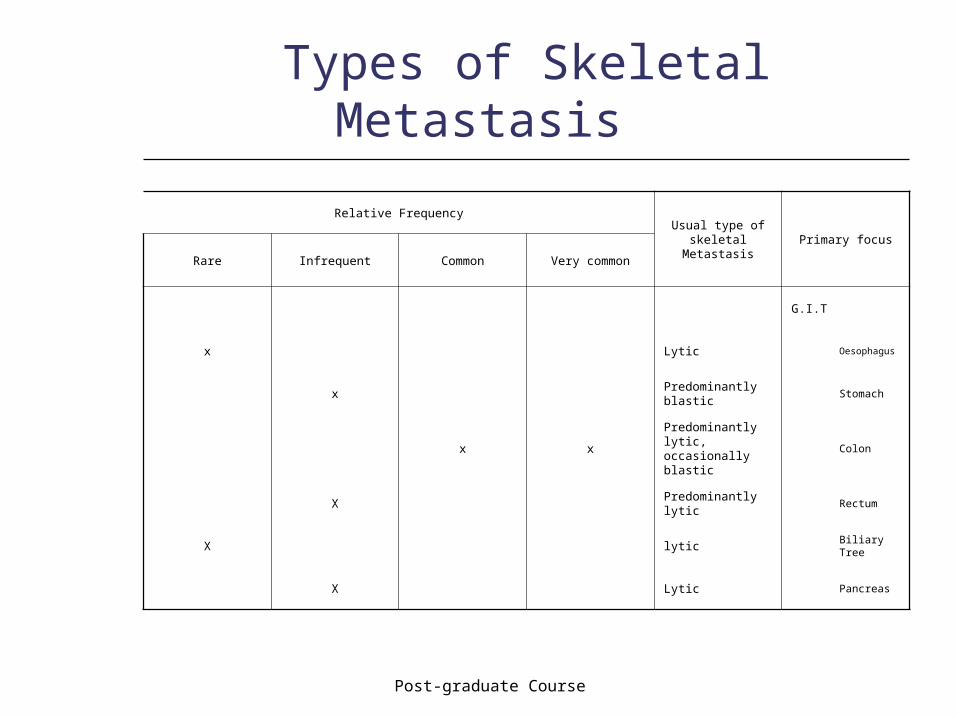
Types of Skeletal Metastasis
Primary focusUsual type of
skeletal Metastasis
Relative Frequency
Very commonCommonInfrequentRare
G.I.T
OesophagusLyticx
StomachPredominantly blastic
x
ColonPredominantly lytic, occasionally blastic
xx
RectumPredominantly lytic
X
Biliary TreelyticX
PancreasLyticX

Post-graduate Course
Types of Skeletal Metastasis
Primary focusUsual type of
skeletal Metastasis
Relative Frequency
Very commonCommonInfrequentRare
Female Reproductive System
Uterus:Corpus
lyticX
CervixLytic or mixedX
OvaryPredominantly lytic
Urinary Bladder
Predominantly lytic, blastic if prostate is involved
X
TestisPredominantly lytic, occasionally blastic
x

Post-graduate Course
Types of Skeletal Metastasis
Primary focusUsual type of
skeletal Metastasis
Relative Frequency
Very commonCommonInfrequentRare
Head, Neck and C.N.S.
BrainLytic or blasticX
Neuroblastoma
Lytic, mixed and blastic
X
Paranasal sinusesLyticX
NasopharynxLytic or blasticX
Skin
EpidermoidLyticx
MelanomaLytic-expandingx

Post-graduate Course
Schemes for Treatment of Skeletal Metastasis
I. Treatment policy of metastasisII. Treatment of skeletal metastasis
1) Surgical management2) Radiation therapy3) Hormonal therapy4) Chemotherapy5) Radioneuclide

Post-graduate Course
Schemes for Treatment of Skeletal Metastasis
III. Treatment of complications1) Pain2) Pathological fractures3) Spinal cord compression4) Hypercalcaemia

Post-graduate Course
Schemes for Treatment of Skeletal Metastasis
IV. Prophylactic treatment1) Adjuvant chemotherapy2) Adjuvant hormonal therapy

Post-graduate Course
Schemes for Treatment of Skeletal Metastasis
The treatment policy differs whether the metastasis is solitary or multiple and also differs according to the state of primary cancer and the general condition of the patient.

Post-graduate Course
Surgical Management of Skeletal Metastasis
1. Amputation:
Aims at palliation of pain if extensive cortical destruction around more distal fractures, fungation, intractable pain and vascular insufficiency.
Post-graduate Course
Surgical Management of Skeletal Metastasis
2. Prophylactic Internal Fixation:Indications:-1) Impending fracture.2) Pain3) Involvement of one-half of the cortex4) High risk femur
Pure lysis are seen on the roentgneogram The development of malignant lesion previously not
demonstrable in the bone Involvement of even a small portion of the cortex Increasing pain Carcinoma of the lung was the tumor type most likely to
be associated with one or more high risk factors Subtrochantric metastatic bone lesions secondary to
carcinoma of the lung
Post-graduate Course
Radiation Therapy
1. Localized irradiation2. Hemibody irradiation

Post-graduate Course
Hormonal Therapy
1) Casteration2) Oestrogenic hormones3) Androgenic hormones4) Progestins5) Antioestrogens6) Aminoglutethemide7) Bilateral adrenalectomy8) Hypophysectomy9) Thyroxin

Post-graduate Course
Cancer Patients Referred for Pain Relief in Pain-clinics
1. Traumatic: Pathological fractures Amputation stump and phantom limb pain
2. Skeletal: Osteolytic lesions Osteoprosis with consequent degenerative
and mechanical changes Hypercalcaemia

Post-graduate Course
Cancer Patients Referred for Pain Relief in Pain-clinics
3. Neurological: Nerve lesions due to compression or
invasion Central pain
4. Diagnostic and psychosomatic problems.

Post-graduate Course
Destructive Procedures in Treatment of Pain
1) Dorsal rhizotomy2) Commissural myelotomy3) Anterolateral cordotomy4) Trans-sphenoidal haypophysectomy5) Rhizotomy of the cranial nerves6) Subarachinoid injection of phenol7) Intrathecal & extradural opiates

Post-graduate Course
Management of Spinal Cord Compression
Spinal cord compression from malignant tumor metastatic to the epidural space will inevitably result in permanent neurological damage unless emergency measures are taken.
It should also be noted that epidural lesions below L1-2 region can result in compression on the cauda equina rather than the spinal cord itself.
Post-graduate Course
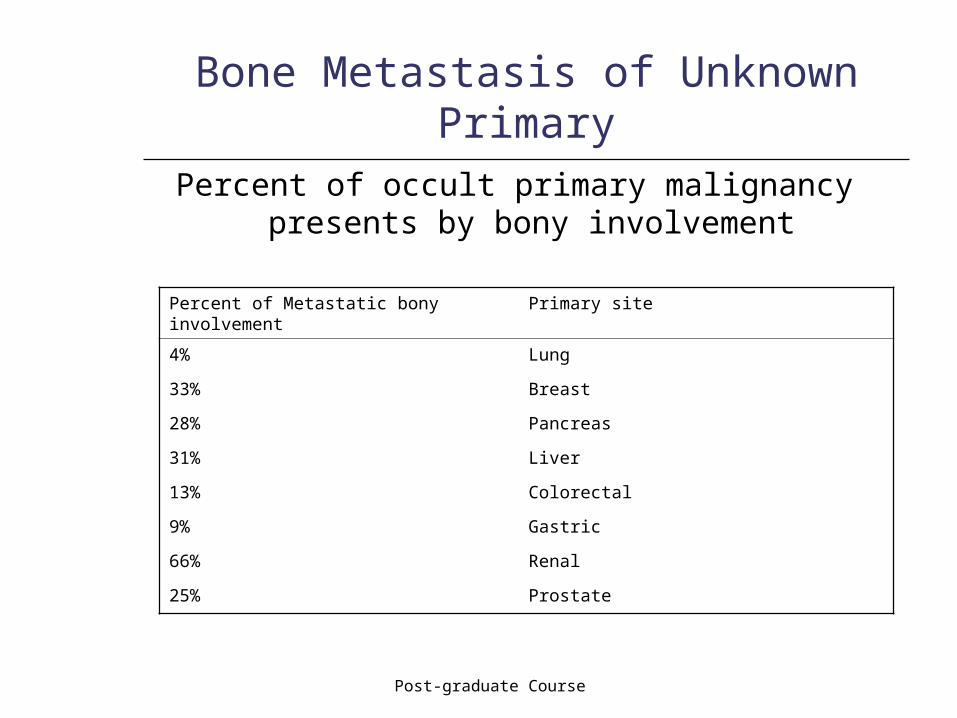
Bone Metastasis of Unknown Primary
Percent of occult primary malignancy presents by bony involvement
Primary sitePercent of Metastatic bony involvement
Lung4%
Breast33%
Pancreas28%
Liver31%
Colorectal13%
Gastric9%
Renal66%
Prostate25%

Post-graduate Course
Benign Tumors with Metastasis