sky diving running a marathon swimming with snakes public speaking
TRANSCRIPT
• Sky diving
• Running a marathon
• Swimming with snakes
• Public speaking

VACUUM HISTORY
• Vacuum extraction was first described in 1705 by Dr. James Yonge, an English surgeon, several decades before the invention of the obstetric forceps. However, it did not gain widespread use until the 1950s, when it was popularized in a series of studies by the Swedish obstetrician Dr. Tage Malmström. By the 1970s, the vacuum extractor had almost completely replaced forceps in most northern European countries, but its popularity in many English-speaking countries, including the United States and the United Kingdom, was limited until the1980s
• The first instrumental deliveries were performed to extract fetuses from patients who were at high risk of maternal mortality due to prolonged and/or obstructed labor. In these cases, saving the mother's life took precedence over possible harm to the fetus.
• There is data that suggest a benefit to vacuum extraction over forceps.
• Successful vaginal delivery rates appear to be higher with vacuum extraction, and
• maternal and fetal trauma and the need for anesthesia are decreased.
• rectal incontinence and nonneurologic weakening of the sphincter are more common with forceps than vacuum deliveries. Increased hyperbilirubinemia and scalp trauma.
• How many people have had a forceps delivery in the past year?
• How many people have had a vacuum delivery in the past year?
• How many of you have had your baby go to the nursery because of that vacuum delivery?

• I don’t know about you guys but I have found out the hard way that I'm a little of an optimist. I’m like the guy with the severed limb calling it a flesh wound.
• One more pull it will come, ok one more pull it will come ,its coming, ok one more pull it will come …
• If its not coming after 3 pulls you need to abandon your plan.

ADVERSE OUTCOMES
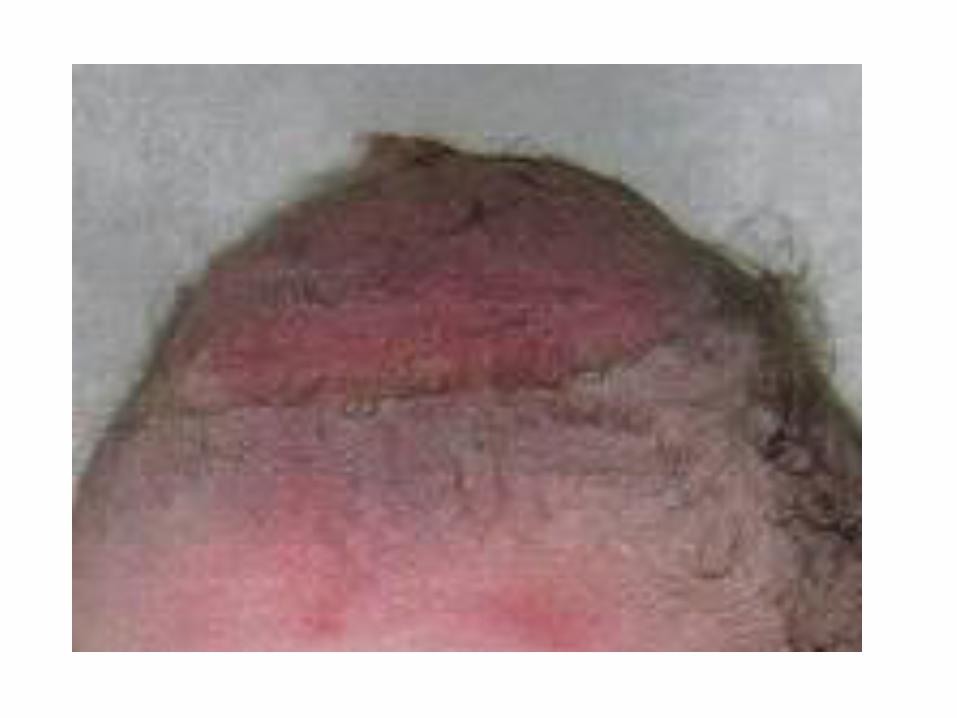
• Scalp laceration that may be painful and may interfere with breastfeeding
• Subgaleal Hemorrhage
• Intracranial Hemorrhage

VACUUM DELIVERY

Subgaleal hemorrhage
• diffuse swelling of the head and signs of hypovolemic shock (e.g., pallor, hypotension, tachycardia and increased respiration rate).
• The signs may be present at delivery or may not become clinically apparent until several hours or up to a few days following delivery.
• The swelling is usually diffuse, shifts dependently when the infant’s head is repositioned and indents easily on palpation.
• In some cases the swelling is difficult to distinguish from the edema of the scalp. On occasion, the hypotension and pallor are the dominant signs while the cranial findings are unremarkable.
VACUUMS ARE SERIOUS!
• So when your doc is talking about a vacuum I want to make sure that your brain kicks into overdrive. Think about the cause of this situation.
• Is it a big baby?
• Does mom have chorio and the uterus isn’t contracting efficiently?
• Is her bladder full?

Increase your SITUATIONAL AWARENESS
• What’s her history? Primip, multip.
• Think about if you have to go back to the OR. Where is anesthesia? Does mom have an IV?
• Think about If there is a shoulder dystocia, do you have a stool ready
• Always get a second nurse in the room and a NICU nurse
INSTRUCTIONS
• How many of you have ever read the instructions on the vacuum?
• We just casually take it out of the package and plop it on the docs table…..
Lets go back to that tired women that has been pushing for 3 hrs
• It is at this time that you and the doctor and the patient will have a quick conversation about the plan of the vacuum.
• I know the docs aren’t great at this but they are going to get better and we will help them. So the conversation will go something like this….

• The doctor must verbally consent the patient to use the vacuum
• Ask doctor if they want the team called in or shall we just be ready to call in the team. On nights, have crash sheet filled out!
• The nurse will verbally go over procedure with pt. saying:
• “The doctor is going to place a vacuum on the baby’s head. With each contraction you must push as hard as you can and the MD will assist you with the vacuum. She can only pull for 3 contractions; then you must push the baby out on your own or we will need to perform a C/S.”

DOCUMENTATION
• RN’s responsibility to note the start time of the application of the vacuum, number of pulls and pop offs. Tell MD which number pull, which number pop off, how many minutes since start time and fetal status.
• Document station of head before application of vacuum and before each pull. This was a question asked multiple times at a RCA.
• Refer to your vacuum checklist to make sure you are remembering everything.

New vacuum policy
• PURPOSE: Provide consistent selection and care management for a patient related to vacuum assisted delivery. To facilitate delivery of the fetal head during a vaginal delivery or cesarean section.
• DEFINITION : • Pop-off: Sudden complete detachment of the vacuum
from the head.• Pull: Use of traction during each contraction.• Situational Awareness: Perception of environmental
elements, including information, events, and actions, comprehension of their meaning, and the projection of how their status will impact outcomes, both immediately and in the near future.

• POLICY : • Contraindication to the use of the vacuum are:
– Fetal Demise– Face, brow or breach presentation
• Relative contraindication to the use of the vacuum are:– Less than 36 weeks gestation
• The MD will determine if the patient is a candidate for vacuum by patient history, dilation and need for anesthesia, as well as, estimated fetal weight, fetal position station, and amount of molding present.
• The MD will determine that a indication for vacuum is present, which include, but are not limited to:
– Maternal exhaustion– Prolonged second stage– Suspicion of potential maternal/fetal compromise
• The MD will examine alternative labor management strategies.• The MD will determine there is a high probability of success.• The MD will ensure the patient is prepared and has been given informed consent.

• There will be a time out/team discussion regarding – Maximum number of pulls that should occur– Maximum number of pop-off that should be allowed– Exit strategy has been established
• The exit strategies will be in action/place prior to the procedure beginning. This includes:
– Ability to perform a cesarean section– Available anesthesia– A newborn resuscitation team available
• Attempt at vacuum assisted delivery should be abandon if any of the flowing occur:
– More than three pulls.– More than 20 minutes have elapsed since the initiation of the procedure– Three pop-offs– No significant descent with each pull
• Team communication should occur though out the procedure to maintain situational awareness related to:
– Accrued time since initiation of procedure– Number of pulls– Number of pop-offs– Progress with each pull– Fetal and maternal status– Willingness to abandon procedure and enact exit strategy– Readiness of cesarean and infant resuscitation team

• Any use of vacuum during a cesarean section will follow the same policy and procedure as use during a vaginal delivery.
• No Multimodal delivery will be used.
• PROCEDURE: • Obtain the following equipment and open onto delivery table using sterile • 1. technique.• a. Specific vacuum extractor requested by MD• b. Straight urinary catheter, if requested by physician.• 2. For vacuums which require the nurse to manually pump up the
pressure, pump only into the green shaded area on the pressure gauge.• 3. Assist the physician to identify onset of contraction. • Traction should be coordinated with uterine contractions and
maternal • pushing efforts.• 4. Reduce the pressure between contractions if requested by
physician; this is now considered optional.• When contraction is no longer effective, the physician should
discontinue traction. • 5. Once head is delivered, release all pressure.

• NURSING DOCUMENTATION: Document all information related to vacuum in the medical record and in the birth log.
• What happens if things don’t quite go as planned and we need help?

WHAT IS CREW RESOURCE MANAGEMENT?
• BETTER TEAMWORK
• NEWLY ACQUIRED COMMUNICATION AND PROBLEM SOLVING SKILLS
• AN OPERATING PHILOSOPHY THAT PROMOTES TEAM MEMBER IINPUT WHILE PRESERVING LEGAL AUTHORITY
• PROACTIVE ACCIDENT PREVENTION

COMMUNICATION
• COMMUNICATION IS THE KEY TO SUCCESS IN ANY ENDEAVOR. WE ALL HAVE EXPERIENCED MISUNDERSTANDINGS THAT HAVE LED TO ERRORS AND MISTAKES. CRM TEACHES PEOPLE TO FOCUS ON THE COMMUNICATION MODEL (SENDER-MESSAGE-MEDIUM-RECEIVER-FEEDBACK), SPEAKING DIRECTLY AND RESPECTFULLY AND COMMUNICATION RESPONSIBILITY


SITUATIONAL AWARENESS
• SITUATIONAL AWARENESS IS A CONCEPT THAT DISCUSSES THE NEED TO MAINTAIN ATTENTIVENESS TO EVERYTHING HAPPENING IN THE ROOM.
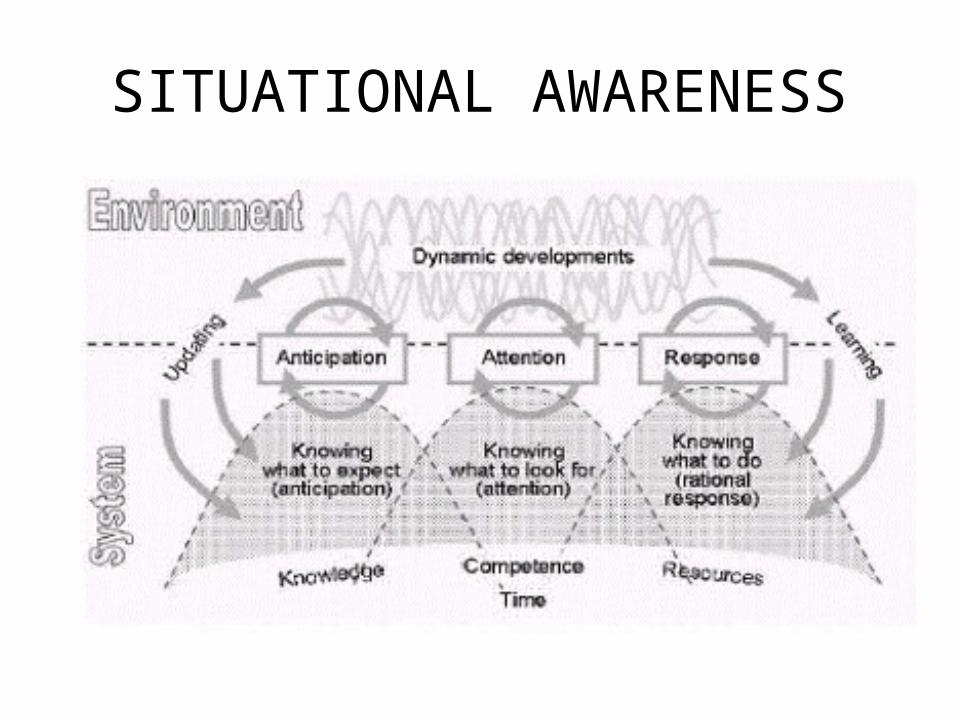
SITUATIONAL AWARENESS

DECISION MAKING
• DECISION MAKING IS BASED ON INFORMATION.TOO LITTLE INFORMATION RESULTS IN POOR RISK ASSESSMENT BY DECISION MAKER AND RESULTS IN ERRORS. TOO MUCH INFORMATION OVERLOADS THE DECISION MAKER AND MAKES IT DIFFICULT TO MAKE EFFECTIVE DECISIONS.

TEAMWORK
• WE HAVE A GREAT TEAM AND SHOULD CONTINUE TO WORK WELL TOGETHER. THE BETTER TEAMWORK WE HAVE THE BETTER OUR OUTCOMES WILL BE!

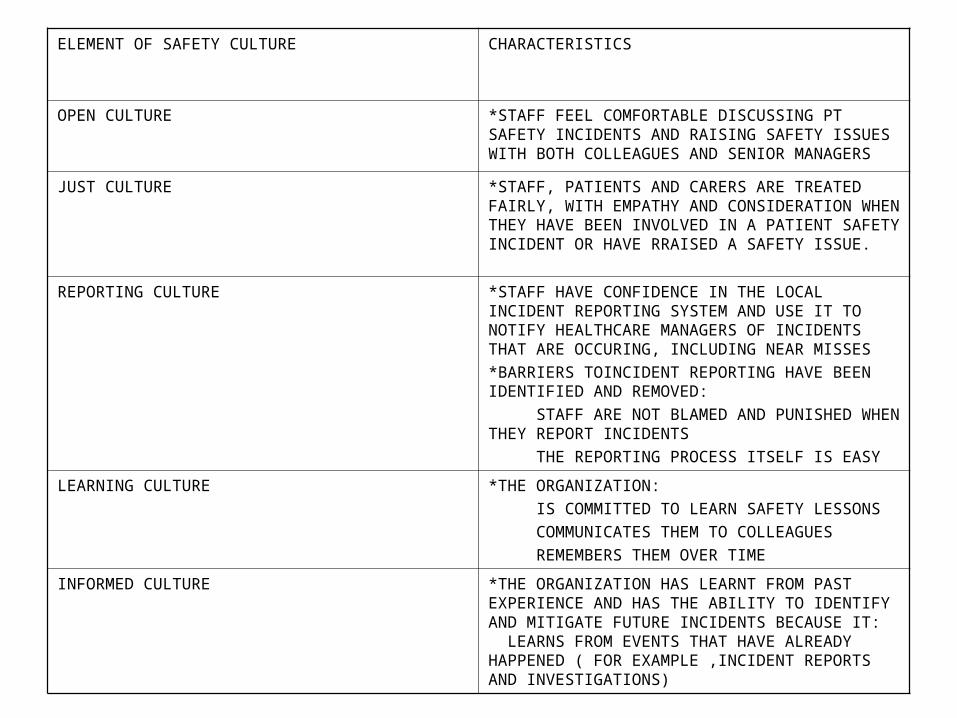
ELEMENT OF SAFETY CULTURE CHARACTERISTICS
OPEN CULTURE *STAFF FEEL COMFORTABLE DISCUSSING PT SAFETY INCIDENTS AND RAISING SAFETY ISSUES WITH BOTH COLLEAGUES AND SENIOR MANAGERS
JUST CULTURE *STAFF, PATIENTS AND CARERS ARE TREATED FAIRLY, WITH EMPATHY AND CONSIDERATION WHEN THEY HAVE BEEN INVOLVED IN A PATIENT SAFETY INCIDENT OR HAVE RRAISED A SAFETY ISSUE.
REPORTING CULTURE *STAFF HAVE CONFIDENCE IN THE LOCAL INCIDENT REPORTING SYSTEM AND USE IT TO NOTIFY HEALTHCARE MANAGERS OF INCIDENTS THAT ARE OCCURING, INCLUDING NEAR MISSES
*BARRIERS TOINCIDENT REPORTING HAVE BEEN IDENTIFIED AND REMOVED:
STAFF ARE NOT BLAMED AND PUNISHED WHEN THEY REPORT INCIDENTS
THE REPORTING PROCESS ITSELF IS EASY
LEARNING CULTURE *THE ORGANIZATION:
IS COMMITTED TO LEARN SAFETY LESSONS
COMMUNICATES THEM TO COLLEAGUES
REMEMBERS THEM OVER TIME
INFORMED CULTURE *THE ORGANIZATION HAS LEARNT FROM PAST EXPERIENCE AND HAS THE ABILITY TO IDENTIFY AND MITIGATE FUTURE INCIDENTS BECAUSE IT: LEARNS FROM EVENTS THAT HAVE ALREADY HAPPENED ( FOR EXAMPLE ,INCIDENT REPORTS AND INVESTIGATIONS)
