snapshot. perfect image. so simple. a magazine...
TRANSCRIPT

TechnologyTalking Cone Beam
Wealth ManagementAdvanced Tax Planning
The Woodlands Dental GroupThe Power of a Group
A MAGAZINE DEDICATED TO THE SUCCESS OF DENTISTRY ISSUE 4 2009A MAGAZINE DEDICATED TO THE SUCCESS OF DENTISTRY ISSUE 4 2008
Call your local Burkhart store for more information
Or contact Instrumentarium at:
Toll free: (800) 558-6120
Email: [email protected]
www.instrumentariumdental.com/usa/
SSnapshot. Perfect image. So simple.
Plug & Play sensor with a zero footprint
Scale 1:1
Film size 241 x 31 mm1.66 x 1.22 inches
Snapshot Sensor size 244 x 31 mm1.73 x 1.22 inches
Snapshot Sensor size 137 x 26 mm1.46 x 1.02 inches
Set it and forget it
Take almost every intraoral image at just one exposure setting. Snapshot’s wide dynamic range provides superior images of all segments of the dentition without altering the settings on your x-ray device.
Just press one button.
The Snapshot sensor has intelligent, integrated electronics.
There are no separate boxes lying around in limited workspace
environments.
Snapshot is ready for use just by plugging the USB cable into any
computer having a Windows XP or Vista operating system. The sensor is detected
automatically and all needed drivers are copied directly from the sensor.
This, combined with the absence of a tabletop electronics unit, make sharing the sensor between
operatories particularly convenient.
Contact your Burkhart Account Manager for more information.
Catalyst M
agazine B
urkhart Dental —
Issue 4 2
00
9
Intelligent MagneticSensor Connector
The NEW
GREEN TO GOPLANMECA® ProSensor
• Magnetic connector from sensor tocontrol box allowing one-handed useattaches quickly and easily releasesfrom interface box under tension(unique to ProSensor)
• Exclusive LED light provides instantaneousfeedback by displaying different colorsto indicate current status of sensorensuring proper image acquisition
• Kevlar reinforced cable has only 2 wiresenhancing durability
• Sensors are hermetically sealed to allowimmersion to prevent infection topatient (unique to PLANMECA)
Sensors available in threesizes 0, 1, and 2
Size 2 Image
Size 0 Connector
PLANMECA®
ProSensorNEW 5 YEAR
Warranty Program!
PLANMECA USA INC. • 100 N. Gary Ave., Suite A, Roselle, IL 60172 • Phone: (630) 529-2300 • Fax: (630) 529-1929 • www.planmecausa.com
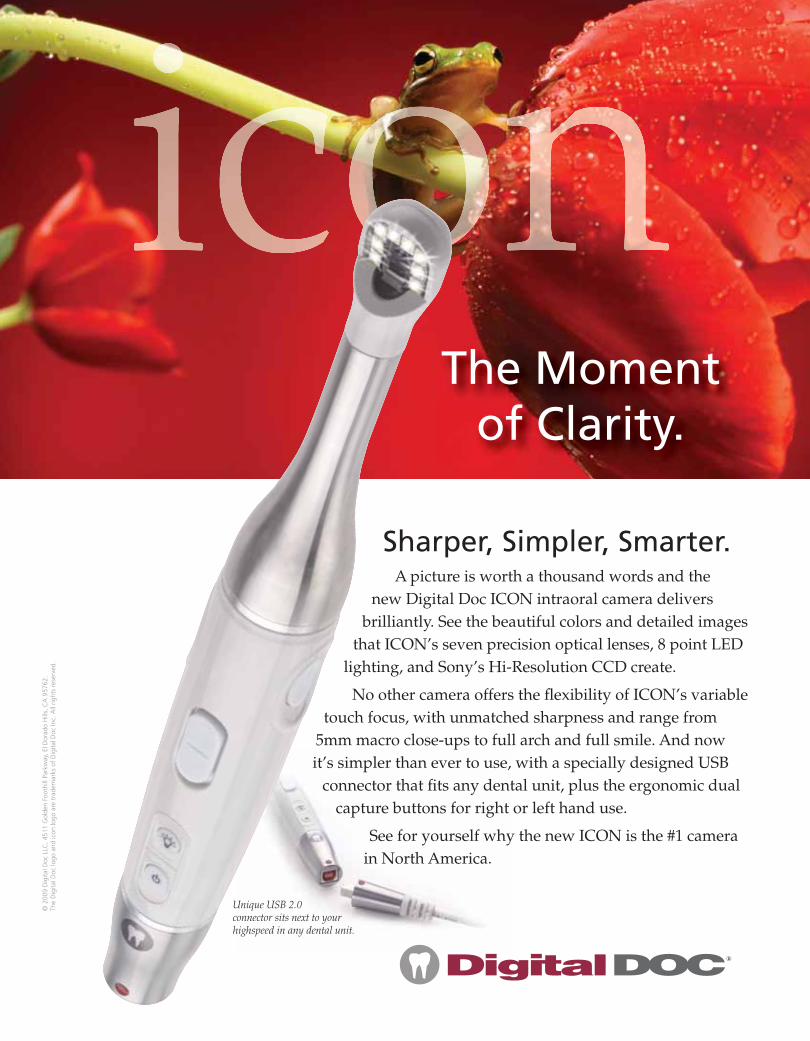
A picture is worth a thousand words and the new Digital Doc ICON intraoral camera delivers
brilliantly. See the beautiful colors and detailed images that ICON’s seven precision optical lenses, 8 point LED
lighting, and Sony’s Hi-Resolution CCD create.
No other camera offers the fl exibility of ICON’s variable touch focus, with unmatched sharpness and range from
5mm macro close-ups to full arch and full smile. And now it’s simpler than ever to use, with a specially designed USB
connector that fi ts any dental unit, plus the ergonomic dual capture buttons for right or left hand use.
See for yourself why the new ICON is the #1 camera in North America.
®
The Moment of Clarity.
Sharper, Simpler, Smarter.
© 2
009
Dig
ital D
oc L
LC, 4
511
Gol
den
Foot
hill
Park
way
, El D
orad
o H
ills,
CA
957
62.
The
Dig
ital D
oc lo
go a
nd ic
on lo
go a
re t
rade
mar
ks o
f D
igita
l Doc
Inc.
All
right
s re
serv
ed.
Unique USB 2.0 connector sits next to your highspeed in any dental unit.
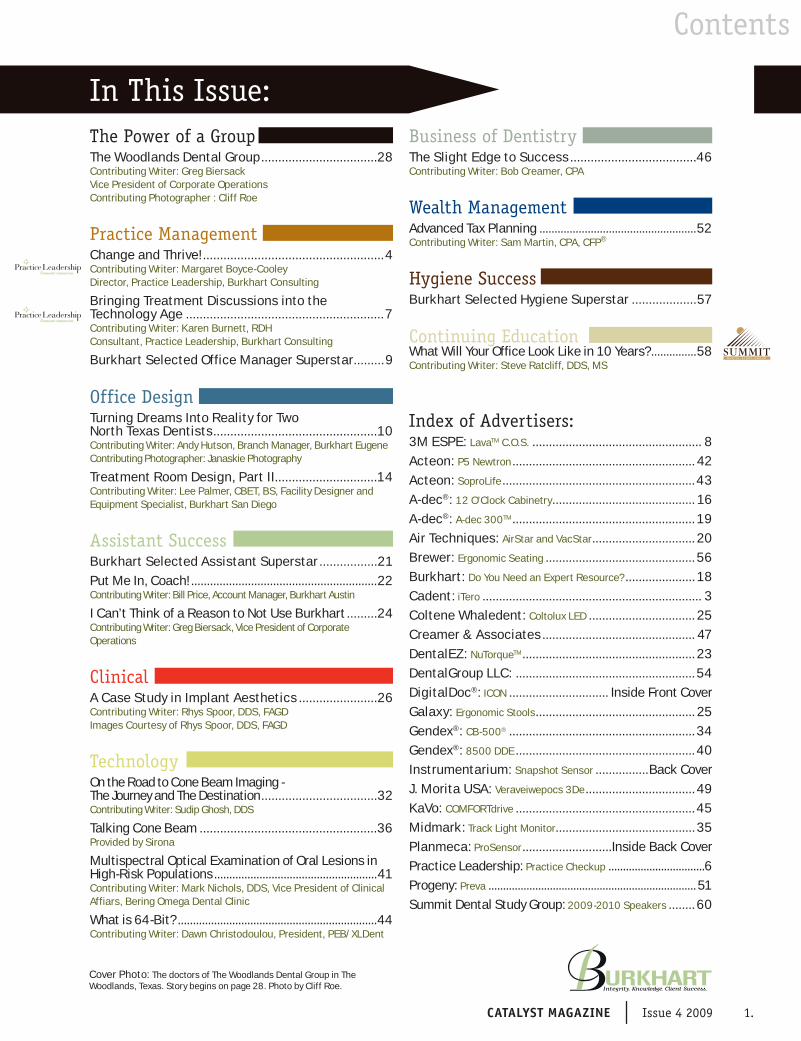
Contents
The Power of a GroupThe Woodlands Dental Group ..................................28Contributing Writer: Greg BiersackVice President of Corporate OperationsContributing Photographer : Cliff Roe
Practice ManagementChange and Thrive! .....................................................4Contributing Writer: Margaret Boyce-Cooley Director, Practice Leadership, Burkhart Consulting
Bringing Treatment Discussions into the Technology Age ..........................................................7Contributing Writer: Karen Burnett, RDH Consultant, Practice Leadership, Burkhart Consulting
Burkhart Selected Office Manager Superstar .........9
Office DesignTurning Dreams Into Reality for TwoNorth Texas Dentists ................................................10Contributing Writer: Andy Hutson, Branch Manager, Burkhart EugeneContributing Photographer: Janaskie Photography
Treatment Room Design, Part II..............................14Contributing Writer: Lee Palmer, CBET, BS, Facility Designer and Equipment Specialist, Burkhart San Diego
Assistant SuccessBurkhart Selected Assistant Superstar .................21Put Me In, Coach! ...........................................................22Contributing Writer: Bill Price, Account Manager, Burkhart Austin
I Can’t Think of a Reason to Not Use Burkhart .........24Contributing Writer: Greg Biersack, Vice President of Corporate Operations
ClinicalA Case Study in Implant Aesthetics .......................26Contributing Writer: Rhys Spoor, DDS, FAGDImages Courtesy of Rhys Spoor, DDS, FAGD
TechnologyOn the Road to Cone Beam Imaging -The Journey and The Destination ..................................32Contributing Writer: Sudip Ghosh, DDS
Talking Cone Beam ....................................................36Provided by Sirona
Multispectral Optical Examination of Oral Lesions in High-Risk Populations ......................................................41Contributing Writer: Mark Nichols, DDS, Vice President of Clinical Affiars, Bering Omega Dental Clinic
What is 64-Bit? ..................................................................44Contributing Writer: Dawn Christodoulou, President, PEB/XLDent
Business of DentistryThe Slight Edge to Success .....................................46Contributing Writer: Bob Creamer, CPA
Wealth ManagementAdvanced Tax Planning ....................................................52Contributing Writer: Sam Martin, CPA, CFP®
Hygiene SuccessBurkhart Selected Hygiene Superstar ...................57
Continuing EducationWhat Will Your Office Look Like in 10 Years? ...............58Contributing Writer: Steve Ratcliff, DDS, MS
Index of Advertisers: 3M ESPE: LavaTM C.O.S. ................................................... 8Acteon: P5 Newtron ....................................................... 42Acteon: SoproLife ..........................................................43A-dec®: 12 O’Clock Cabinetry ........................................... 16A-dec®: A-dec 300TM ....................................................... 19Air Techniques: AirStar and VacStar ............................... 20Brewer: Ergonomic Seating ............................................. 56Burkhart: Do You Need an Expert Resource? .....................18Cadent: iTero .................................................................. 3Coltene Whaledent: Coltolux LED ................................ 25Creamer & Associates .............................................. 47DentalEZ: NuTorqueTM .................................................... 23DentalGroup LLC: ......................................................54DigitalDoc®: ICON .............................. Inside Front CoverGalaxy: Ergonomic Stools ................................................ 25Gendex®: CB-500® ........................................................34Gendex®: 8500 DDE ......................................................40Instrumentarium: Snapshot Sensor ................Back CoverJ. Morita USA: Veraveiwepocs 3De ................................. 49KaVo: COMFORTdrive ......................................................45Midmark: Track Light Monitor ..........................................35Planmeca: ProSensor ...........................Inside Back CoverPractice Leadership: Practice Checkup .................................6Progeny: Preva .......................................................................51Summit Dental Study Group: 2009-2010 Speakers ........60
Cover Photo: The doctors of The Woodlands Dental Group in The Woodlands, Texas. Story begins on page 28. Photo by Cliff Roe.
CATALYST MAGAZINE Issue 4 2009 1.
In This Issue:
InTouch
Greg Biersack, Vice President of Corporate Operations.
During my travels to visit dental of f ices, I am of ten asked what makes Burkhart unique.
Although there are many answers, three capture the greatest benefits our clients receive:
1. Burkhar t account managers understand the importance of learning about their clients’ business and needs before presenting anything. Nobody likes a pushy salesperson whose exclusive focus is on sales and commission. In contrast, everybody likes working with someone whose goal it is to help others succeed. This is where we excel.
2. Burkhar t is a privately held company, the long-term focus of which is on helping dental offices succeed. This focus guides our determination to elevate consistently the level of service we provide. Contrast this with a publicly traded company whose short-term requirement is to satisfy shareholders’ need for profitability.
3. Burkhart is the only company that provides a written guarantee to lower supply costs for dental offices. We take responsibility, and are held accountable for this aspect of the expenses faced by offices.
Our unique offerings and approach to serving our clients has resulted in their success and the continual growth of our business.
Greg Biersack,Burkhart Vice President of
Corporate Operations
Contact your Burkhart AccountManager today to find out how to
lower your office’s supply overhead.
Responsible forthe ClinicalSupplies in
Your Office?
800.562.8176www.burkhartdental.com
2. Issue 4 2009 CATALYST MAGAZINE
At Burkhart we realize that our clients are both dental professionals and business owners. It is our goal to help them be successful at both aspects of their careers. Catalyst is fully dedicated to that success. The articles in this publication vary from product use and selection to business management topics and provide information and guidance
that can lead to a more successful practice. Throughout the publication
are stories of Burkhart clients who have succeeded in the areas that are highlighted. We hope that you enjoy.
If you have a request for a topic that you would like for us to cover in Catalyst,
please contact Greg Biersack at:
LOCATED IN:Anchorage, Alaska
Phoenix, ArizonaSan Diego, California
Bay Area, CaliforniaSacramento, California
Denver, ColoradoBoise, Idaho
Las Vegas, NevadaTulsa, Oklahoma
Oklahoma City, OklahomaEugene, Oregon
Portland, OregonAustin, Texas
Houston, TexasDallas, Texas
Salt Lake City, UtahSpokane, WashingtonTacoma, WashingtonYakima, Washington
Serving the DentalProfession since 1888...
Catalyst Magazine is published byBurkhart Dental Supply
2502 South 78th St.Tacoma, WA 98409Tel. (253) 474-7761Fax (253) 472-4773
Principal EditorGreg Biersack
Managing EditorHolly Kean
All rights reserved. Reproduction of any part of this publication without written permission
from the Publisher is strictly forbidden. Images are not necessarily to scale.
Customer Service:
800.562.8176
In Touch – From the Editor
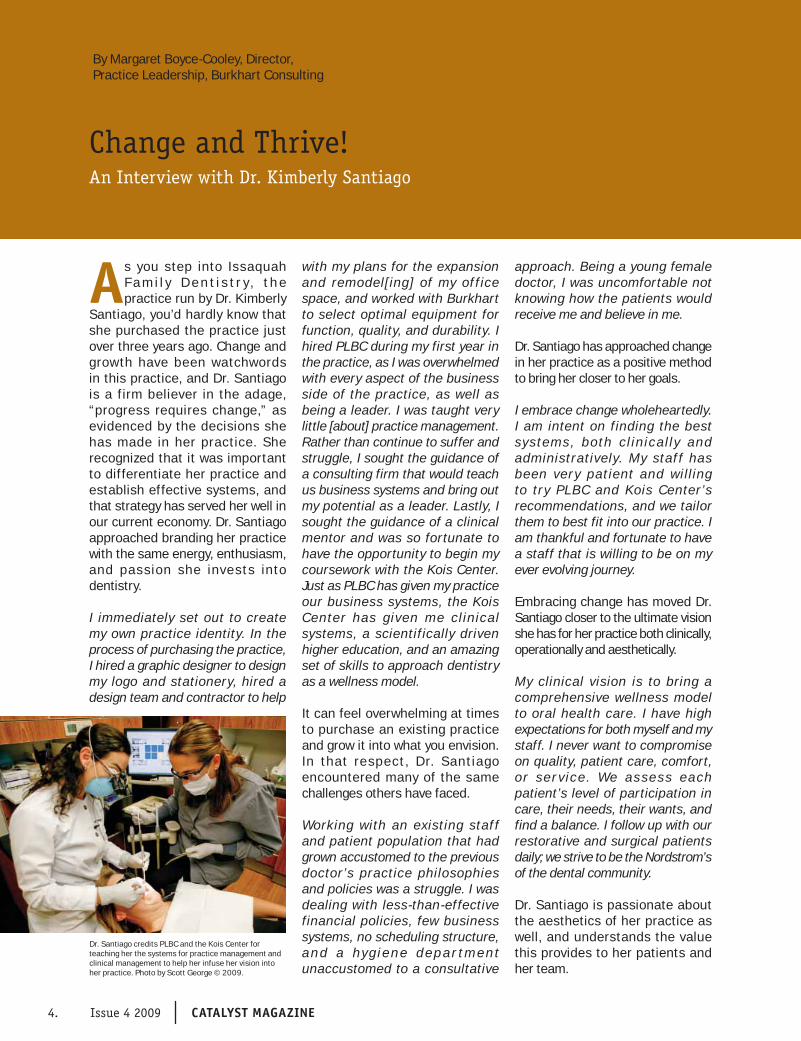
As you step into Issaquah F a m i l y D e n t i s t r y , t h e practice run by Dr. Kimberly
Santiago, you’d hardly know that she purchased the practice just over three years ago. Change and growth have been watchwords in this practice, and Dr. Santiago is a firm believer in the adage, “progress requires change,” as evidenced by the decisions she has made in her practice. She recognized that it was important to differentiate her practice and establish effective systems, and that strategy has served her well in our current economy. Dr. Santiago approached branding her practice with the same energy, enthusiasm, and passion she invests into dentistry.
I immediately set out to create my own practice identity. In the process of purchasing the practice, I hired a graphic designer to design my logo and stationery, hired a design team and contractor to help
with my plans for the expansion and remodel[ing] of my of f ice space, and worked with Burkhart to select optimal equipment for function, quality, and durability. I hired PLBC during my first year in the practice, as I was overwhelmed with every aspect of the business side of the practice, as well as being a leader. I was taught very little [about] practice management. Rather than continue to suffer and struggle, I sought the guidance of a consulting firm that would teach us business systems and bring out my potential as a leader. Lastly, I sought the guidance of a clinical mentor and was so fortunate to have the opportunity to begin my coursework with the Kois Center. Just as PLBC has given my practice our business systems, the Kois Center has given me cl inical systems, a scientifically driven higher education, and an amazing set of skills to approach dentistry as a wellness model.
It can feel overwhelming at times to purchase an existing practice and grow it into what you envision. In that respect , Dr. Santiago encountered many of the same challenges others have faced.
Working with an existing staf f and patient population that had grown accustomed to the previous doctor’s practice philosophies and policies was a struggle. I was dealing with less-than-effective financial policies, few business systems, no scheduling structure, a n d a hy g i e n e d e p a r t m e n t unaccustomed to a consultative
approach. Being a young female doctor, I was uncomfortable not knowing how the patients would receive me and believe in me.
Dr. Santiago has approached change in her practice as a positive method to bring her closer to her goals.
I embrace change wholeheartedly. I am intent on finding the best systems, both c l inical l y and administratively. My staf f has been very patient and will ing to try PLBC and Kois Center’s recommendations, and we tailor them to best fit into our practice. I am thankful and fortunate to have a staff that is willing to be on my ever evolving journey.
Embracing change has moved Dr. Santiago closer to the ultimate vision she has for her practice both clinically, operationally and aesthetically.
My clinical vision is to bring a comprehensive wellness model to oral health care. I have high expectations for both myself and my staff. I never want to compromise on quality, patient care, comfort, or ser v ice . We as ses s each patient’s level of participation in care, their needs, their wants, and find a balance. I follow up with our restorative and surgical patients daily; we strive to be the Nordstrom’s of the dental community.
Dr. Santiago is passionate about the aesthetics of her practice as well, and understands the value this provides to her patients and her team.
Dr. Santiago credits PLBC and the Kois Center for teaching her the systems for practice management and clinical management to help her infuse her vision into her practice. Photo by Scott George © 2009.
4. Issue 4 2009 CATALYST MAGAZINE
By Margaret Boyce-Cooley, Director,Practice Leadership, Burkhart Consulting
Change and Thrive!An Interview with Dr. Kimberly Santiago

Practice Management
Issaquah Family Dentistry (left to right) Irina Brunets, Kara Prew, Jenn Peschel, Dr. Kimberly Santiago, Linda Carlton,Cori Frandsen and Kim Swofford. Photo by Scott George © 2009.
Patients take note of every detail when they step into the practice and hopefully interpret them to be a reflection of the care and quality they are to encounter here at Issaquah Family Dentistry. This helps … the patients and the team realize a sense of organization, standardization, and consistency.
Dr. Santiago’s desire for stability and growth initially caused some instability in the practice. Change can be difficult, however, and Dr. Santiago learned that the quicker you can let go of inefficient systems and embrace new, more effective ones, the closer you move toward your goal.
The practice has evolved into a patient-centered experience. Each team member is attentive, caring, motivated, and truly enjoys patient care. We went from business chaos to vir tually ordered systems. If there is not a system in place, we create a new one. Systems are the foundation for practice stability and future growth.
While you are in the midst of change and are striving to make the practice your own, it can often feel as though the transformation isn’t happening fast enough—while for your team, it can feel like it is happening all too quickly! Fear can begin to play a role, and it’s at these times that it is best to heed Churchill’s wisdom, “There is nothing wrong with change if it is in the right direction.” Change can help practices thrive, even in this economy, and Dr. Santiago’s practice is a case in point. When situations change, these practices change with them. Envision what you want in your practice, and take the steps—make the changes—to do just that.
Our efficiencies have improved, which has led to better production. As a result, I’ve been able to invest in amazing CE courses as well as dabbling in additional technology.
With greater implementation of systems, we have been able to bring in more clinical systems, treatments, and technologies.
Dr. Santiago has also learned along the way that one of the greatest inhibitors to change can reside within you.
It can be quite difficult to lead a group of contemporaries. I do my best to be the leader and minimize my role as friend/equal. I attempt to give everyone real-time feedback as objectively as possible, sticking to fact-fact rather than emotion-driven conversation. Again, it is a challenge I work at constantly.
Dr. Santiago is not alone in this area. All of the preparation and training you received in school has been centered on creating healthy mouths and not healthy practices. Dr. Santiago welcomed change, and brought PLBC in to help her reach the dreams and goals she had for her practice.
PLBC is one of the best investments I’ve made. It will rock your business foundations and transform your
leadership skill set. Be prepared to make changes—some you may struggle with—[but] the benefits will come, in time. Be committed to the advice they offer, implement [it], and follow up with employees. Holding everyone, including you, accountable for the changes is the key to success.
Practice Leadership, Burkhart Consulting,
is a full-service consulting firm specializing
in developing leaders and teams in
dent is t r y. For more than a decade,
Practice Leadership has helped hundreds
o f p rac t ice s achieve new leve ls o f
success. Contact your Burkhart Account
Manager or Practice Leadership directly at
800.665.5323 for more information.
CATALYST MAGAZINE Issue 4 2009 5.
Routine maintenance
means fewer emergencies!
Practice Leadership can:
• Analyze overhead and growth strategies to improve profi tability.
• Analyze your business to discover strengths and identify areas that may need more focus.
• Help clarify practice vision and expectations to give direction to your practice and improve team performance.
• Show you ways to achieve your practice goals.
• Increase profi tability while decreasing stress.
Contact Your Burkhart Account Manageror Call Practice Leadership at 800.665.5323
Or contact us by email at: [email protected]
Is it Time for a PRACTICE CHECKUP?
www.practiceleadership.com

Practice Management
Bringing Treatment Discussions into the Technology AgeDoes it matter how up-to-date your method of presenting treatment is?By Karen Burnett, RDH, Consultant, Practice Leadership, Burkhart Consulting
CATALYST MAGAZINE Issue 4 2009 7.
Everybody’s Got TechEvery day, almost every man, woman, and child uses a cell phone, DVD, iPod, or some other form of technology. Technology is even going to the dogs with GPS collars! You might be one of these high-tech consumers personally, but has it carried over into your practice? Health care marketing often focuses on technology competitiveness. This type of marketing capitalizes on the consumer’s expectation that medical and dental providers wi l l invest in the equipment necessary to provide increased comfort, decreased number of appointments, increased treatment quality, and even convey critical details to other practitioners, labs, and specialists when indicated.
How “technology competitive” your practice is can determine whether you attract new patients, quality staff, prospective associates, or buyers when it is time to transition. So are you asking patients to see a tiny crack in an amalgam and accept treatment by coordinating a mouth mirror and hand mirror? Do you expect a patient to invest time and money in a dental implant
based on a t ypodont model example? Is your staff less efficient because they are working with and maintaining older equipment? Is your lack of technology costing you leading-edge candidates for your team? The businesses that thrive despite this economy are those that attract both clients and employees, and continue to be proactive in creating a better experience within that business.
Communication ToolVisuals are used to communicate and market because they produce results! Why does your favorite coffee place have a display case of baked goods? Why do clothing stores have display windows? A visual image, whether it is a digital panoramic radiograph, intraoral camera view, or digital ex traoral photo, ser ves as a pat ient c ommunic at ion too l that complements your verbal p r e s e n t a t i o n . P a t i e n t s c an appreciate that you’ve invested in technolog y when i t he lps them make informed decisions about their t reatment . When the method you use to present treatment improves your patients’ understanding of their treatment o p t i o n s , g r e a t e r t r e a t m e n t acceptance is sure to follow.
You have probably learned that providing quasi-dental school level knowledge to a patient about a procedure does not always result in a scheduled appointment—patients tend to accept treatment when they are able to understand the benefit of the screening or visualize the treatment recommended. Digital frames that display before and after
photos and imaging can be one way to convey your treatment outcomes. Cone beam technology can help a patient understand if he or she is a candidate for an implant or to have a third molar extracted. The benefit of early detection can be provided by oral cancer screening systems. All technology specializes in providing more immediate and concise information for you and your patients, to ensure that better treatment decisions are made.
To use your technology effectively, don’t keep those new toys all to yourself. Training your team so that they are comfortable using the latest equipment means that your patients will have greater exposure to that technology as well. The key to introducing your team to a new piece of technology is to develop a protocol for its use. Clinical and even front office team members’ knowledge of technology can contribute to case acceptance and new patient referrals. Notably, technology beyond the clinical area can contribute to case acceptance
Technology like the Trimira identifi 3000 is one of the more recent early cancer detetion systems to enter the market and can really make a difference in what patients see and understand about the health of their own mouths.
Models may not offer a lot of valuable infomation to a client who is considering substantial dental treatment. Technology is key in showing the severity of the problem and show areas of treatment for each patient as it relates to them specifically.

Practice Management
Practice Leadership, Burkhart Consulting,
is a full-service consulting firm specializing
in developing leaders and teams in
dent is t r y. For more than a decade,
Practice Leadership has helped hundreds
o f p rac t ice s achieve new leve ls o f
success. Contact your Burkhart Account
Manager or Practice Leadership directly at
800.665.5323 for more information.
Register to attend a Lava™
Chairside Oral Scanner C.O.S. seminar in your area.
Earn CE credits.
Ask your Burkhart representative for more information.
The Lava C.O.S. provides the foundation for the dental practice of the future.
impressions1
1
Lava™ Restorations
continuous
1
Canada.
o
ProductivityPPPPPPP dddd i iImproved
Lava™
Chairside Oral Scanner C.O.S.
Digital ImpressionsPrecise
essions
as well. Many practices offer online applications for outside financing and have Web sites that feature patient testimonials as well as “after” photos to help establish conf idence in your treatment recommendations among your newest patients.
PaybackThe dent al oath re fer s to a responsibility to grow professional knowledge and improve skills to meet patients’ needs. The intention of dental equipment and technology is to help patients complete t reatment wi thin a reasonable amount of time and assist them in avoiding more extensive and expensive treatment in the future. With respect to the current economy, most patients appreciate this patient-centered approach. Both advanced and updated equipment can save appointment time for you and your patients, which contributes to prac t ice prof i t ab i l i t y and patient satisfaction. How many impressions do you not have to retake on patients who gag? Among patients with tori and small arches, how much more comfortable would they be using a digital impression system? How about the benefits of
a digital shade guide that avoids multiple visits to get just the right color for an anterior crown?
ConclusionOutdated technology can detract from treatment acceptance and the growth of new patients for the practice. Perception is everything, so it is essential that patients are introduced to the newest scans and screenings during medical appointments. Keeping up with technology advances the professionalism of dentistry. The “dinosaur” intraoral camera cart and Web site featuring long-gone staf f members today could be compared to the spittoon on the floor and the belt-driven handpiece found in a dentist’s office in the 1800s. They were the best of their time, but only for a time. Demonstrate that you are invested in the standard of care for your patients, and get those referrals from appreciative patients that will help carry the practice through to more profitable times. Given the number of us who continually upgrade our cell phones and computers, people clearly value technology and want the latest advances. What technology in your practice demonstrates your level of expertise and quality of care?
Above: Show your patients that your are actively invested in increasing the standard of care in your office by implmenting technology like charting software from XLDent.
Hobbies:
What I like about my job:
My Greatest challenge is:
Success at our office means:
What Burkhart means to me:
Office Manager, Chester T. Low, DDS - Richmond, California
Long walks along the bay with my daughter, playing with my grandchildren, and growing orchids.
Assisting Dr. Low and his dedicated staff to achieve our mission statement “to give back to the community”.
Working with over 20 employees and helping everyone stay on target so that we deliver excellent dental care and keep the office running smoothly.
Encouraging our patients to choose excellent dental care in an affordable, pleasant atmosphere.
I feel Joyce Nichelini gives us complete personal service. She takes care of our buying choices, providing us with options that save us time and money. I never have to worry about anything as long as she is here. The service technicians are great, friendly, and they are here as soon as we call. The associates at Burkhart are all a pleasure to work with and talk to.
Nancy Lincoln
CATALYST MAGAZINE Issue 4 2009 9.

Office Design
Turning
Dreams into
Reality for
Two North
Texas DentistsBy Andy Hutson, Branch Manager, Burkhart Eugene
Start with an infectious smile and a zest for life, add a welcoming, unique interior, and the desire
to offer only the very best dental technology currently available, and what you’ll see is Dr. Stacey Harris and her new office, Star Creek Dental. Upon entering Star Creek Dental, it is hard to imagine that only 14 weeks elapsed between its conception and Dr. Harris’ first patient. Once Dr. Stacey Harris decided to leave her associateship position to pursue ownership, she knew exactly where
she wanted to open her own practice – a thriving new active lifestyle community in Allen, Texas. Visibility and quick access to one of the area’s main highways, State Highway 121, were bonuses to this location. “The fact that I grew up here, beginning with the first grade, allowed Allen to be the natural choice, especially with friends and family nearby.”
Dr. Harris isn’t the only one who grew up in Allen. Her husband, Dr. Chad Fendley, did too. Dr. Harris and Dr. Fendley form a unique team. The two began dating in high school, attended their senior prom together, and have shared three graduations. The first was from Allen High School, the next at Texas Tech University, and finally the University of Texas Health Science Center at Houston Dental Branch in 2001. “During dental school, our professors quickly learned that we were a couple and began referring to us as “the team,” and we have never steered away from that.”
“By suppor t ing each other ’s professional growth, maximum potential, and dreams, and always
offering advice and insight, the two doctors complement each other well.”
“A l thoug h we own s ep ar a te practices, we keep up with each other during the day and get instant feedback from each other. When I decided to take the risk and begin my own start-up practice, Chad was there pushing me and supporting me the entire time.”
In fact, Dr. Harris is lucky enough to have her husband, who became a Fellow of the Internat ional Congress of Oral Implantology in 2007, provide her patients with bone augmentation procedures and surgical implant placement. “It is a luxury to provide my patients with those services without them having to go to another office.”
To get the ball rolling on Dr. Harris’ project, a phone call was made to Burkhart Account Manager, Karen Glessner-Aston, with whom Dr. Fendley had worked for five years at his practice. A meeting was coordinated between Dr. Harris, the then-current Equipment Specialist for the Dallas area, and MedTech Construction.
Above Left: The waiting area modern and relaxing and fits Dr. Stacey Harris’ desire to have an office that didn’t look like a “typical” dental office. Above right: Dr. Harris’ water filtration system is the first of it’s kind in Allen, Texas removing 99% of all bacteria for her patients. Photos by Janaskie Photography © 2009.
10. Issue 4 2009 CATALYST MAGAZINE
Office Design“I was impressed from the very beginning with the professionalism of Burkhart and MedTech. I arrived at this initial meeting with a primitive floor plan and watched it evolve before my very eyes while changes were made on the spot. I left that meeting with the final plan!”
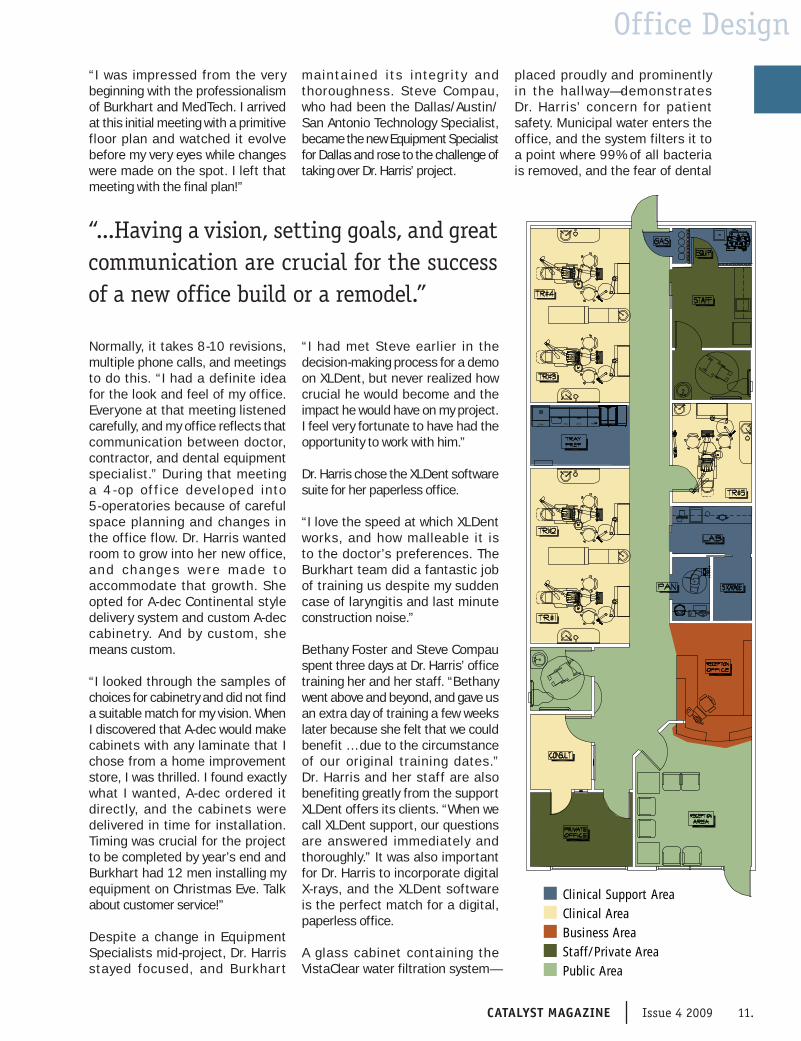
Normally, it takes 8-10 revisions, multiple phone calls, and meetings to do this. “I had a definite idea for the look and feel of my office. Everyone at that meeting listened carefully, and my office reflects that communication between doctor, contractor, and dental equipment specialist.” During that meeting a 4 - op of f ice developed into 5-operatories because of careful space planning and changes in the office flow. Dr. Harris wanted room to grow into her new office, and change s were made to accommodate that growth. She opted for A-dec Continental style delivery system and custom A-dec cabinetry. And by custom, she means custom.
“I looked through the samples of choices for cabinetry and did not find a suitable match for my vision. When I discovered that A-dec would make cabinets with any laminate that I chose from a home improvement store, I was thrilled. I found exactly what I wanted, A-dec ordered it directly, and the cabinets were delivered in time for installation. Timing was crucial for the project to be completed by year’s end and Burkhart had 12 men installing my equipment on Christmas Eve. Talk about customer service!”
Despite a change in Equipment Specialists mid-project, Dr. Harris stayed focused, and Burkhar t
maintained i t s integr i t y and thoroughness. Steve Compau, who had been the Dallas/Austin/San Antonio Technology Specialist, became the new Equipment Specialist for Dallas and rose to the challenge of taking over Dr. Harris’ project.
“I had met Steve earlier in the decision-making process for a demo on XLDent, but never realized how crucial he would become and the impact he would have on my project. I feel very fortunate to have had the opportunity to work with him.”
Dr. Harris chose the XLDent software suite for her paperless office.
“I love the speed at which XLDent works, and how malleable it is to the doctor’s preferences. The Burkhart team did a fantastic job of training us despite my sudden case of laryngitis and last minute construction noise.”
Bethany Foster and Steve Compau spent three days at Dr. Harris’ office training her and her staff. “Bethany went above and beyond, and gave us an extra day of training a few weeks later because she felt that we could benefit … due to the circumstance of our original training dates.” Dr. Harris and her staff are also benefiting greatly from the support XLDent offers its clients. “When we call XLDent support, our questions are answered immediately and thoroughly.” It was also important for Dr. Harris to incorporate digital X-rays, and the XLDent software is the perfect match for a digital, paperless office.
A glass cabinet containing the VistaClear water filtration system—
placed proudly and prominently in the hallway— demonstrates Dr. Harris’ concern for patient safety. Municipal water enters the office, and the system filters it to a point where 99% of all bacteria is removed, and the fear of dental
“...Having a vision, setting goals, and great communication are crucial for the success of a new office build or a remodel.”
Clinical Support AreaClinical Area
Clinical Support AreaClinical AreaBusiness AreaStaff/Private AreaPublic Area
CATALYST MAGAZINE Issue 4 2009 11.

Office Design
Top: The sterilization area complete with the VistaPure water purification system, an Assistina handpiece maintenance system and a Lisa sterilizer in A-dec cabinetry. Bottom: Functional and beautiful operatories relfect
the use of green and black throughout the office. Photos by Janaskie Photography © 2009.12. Issue 4 2009 CATALYST MAGAZINE12. Issue 4 2009 CATALYST MAGAZINE

Office Designwaterline biofilm is eliminated. Star Creek Dental is the only dental office in the city of Allen currently approved to offer this sophisticated water f i l t ra t ion sys tem. Her sterilization area utilizes A-dec cabinetry, Lisa sterilizer, VistaPure water filtration, and an Assistina for handpiece maintenance.
Dr. Harris wanted her office to reflect her personality and opted to paint the walls a shade of lime green with accents of black and red. “People kept trying to dissuade me from using such bright colors, but I knew it would work.” Custom artwork done by Dr. Harris’ brother, Bradley Harris, showcases not only his talents, but her desire to have an office that doesn’t look like a typical dental office. A wall of mirrors reflects the natural lighting, and a comfortable, lounge-like reception area welcomes the patient. A bright, large consultation room creates a non-threatening environment in which to discuss treatment options. “I had a great time with the construction phase and thoroughly enjoyed decorating my home away f rom home.” Patients have responded with great feedback on the amenities here, especially the ceiling mounted TVs and warm water from the syringes—even the color of the walls!
Dr. Harris and Dr. Fendley must have enjoyed the design and construction processes because during her project, Dr. Fendley purchased the practice where he had been associating for the previous five years. As soon as he purchased it, ideas were already in place to expand, remodel, and bring the necessary technology into that office. As before, Burkhart and MedTech were contacted, and the process began again with the same group of people. Dr. Fendley comments that “Steve has been instrumental in my decision-making process. He does what most salespeople these days forget to do: he listens. Steve has been mindful of my budget and my
likes/dislikes on delivery systems, cabinetry, and technology.” Trying to work around the schedule of a busy, two-doctor office has proven challenging, so Dr. Fendley’s project is being completed in two phases. Phase I included converting to digital X-rays and installing the Sirona Galileos 3-D panoramic X-ray, updating the mechanical room, and expanding the office by 500 square feet for personal office spaces. “One of the focuses of my office is implantology, and now with 3-D technology, there is zero guesswork in surgically placing implants, especially with the ability to map nerves and to have surgical guides fabricated.” Phase II of Dr. Fendley’s project begins soon and will include updating the reception area and installing new A-dec 12 o’clock delivery system and cabinetry in the operatories. “I can’t wait to see the finished product!” exclaims Dr. Fendley.
These dental projects have consumed Dr. Harris and Dr. Fendley for nearly a full year now, but ask them about it, and they say they would do it all over again, especially with the help they received from the professionals at Burkhart Dental Supply. Both doctors agree that having a vision, setting goals, and great communication are crucial for the success of a new office build or a remodel.
Dr. Harris remarks, “My greatest compliment is that many of the dental professionals who worked on my project are now my patients!”
Below Top: Star Creek Dental’s office door. Below Middle: Patient consultation area is bright and reflective of Dr. Harris’ vision for her practice. Below Bottom: Equipment Specialist Steve Campau and Burkhart Account Manager Karen Glessner helped to make the project a success for Drs. J. Chad Fendly and Stacey Harris. Photos by Janaskie Photography © 2009.
CATALYST MAGAZINE Issue 4 2009 13.
Office Design
Part 2:
Treatment
Room DesignBy Lee Palmer, CBET, BS, Facility Designer and Equipment Specialist, Burkhart San Diego
From Par t I, you may have decided whether you wanted closed rooms, modular rooms,
or even an open bay design. In this article, we will focus more on the delivery of both static and dynamic instrumentation and armamentarium to the oral cavity.
This breaks down primarily to where the dynamic instrumentation
for the doctor will come from, and where the dynamic and static instrumentation and work surfaces will come from for the assistant. Secondarily, we must decide the source of the operating light, intraoral X-ray, computer monitors, keyboard, and mouse, and other interrelated parts of the overall delivery scheme.
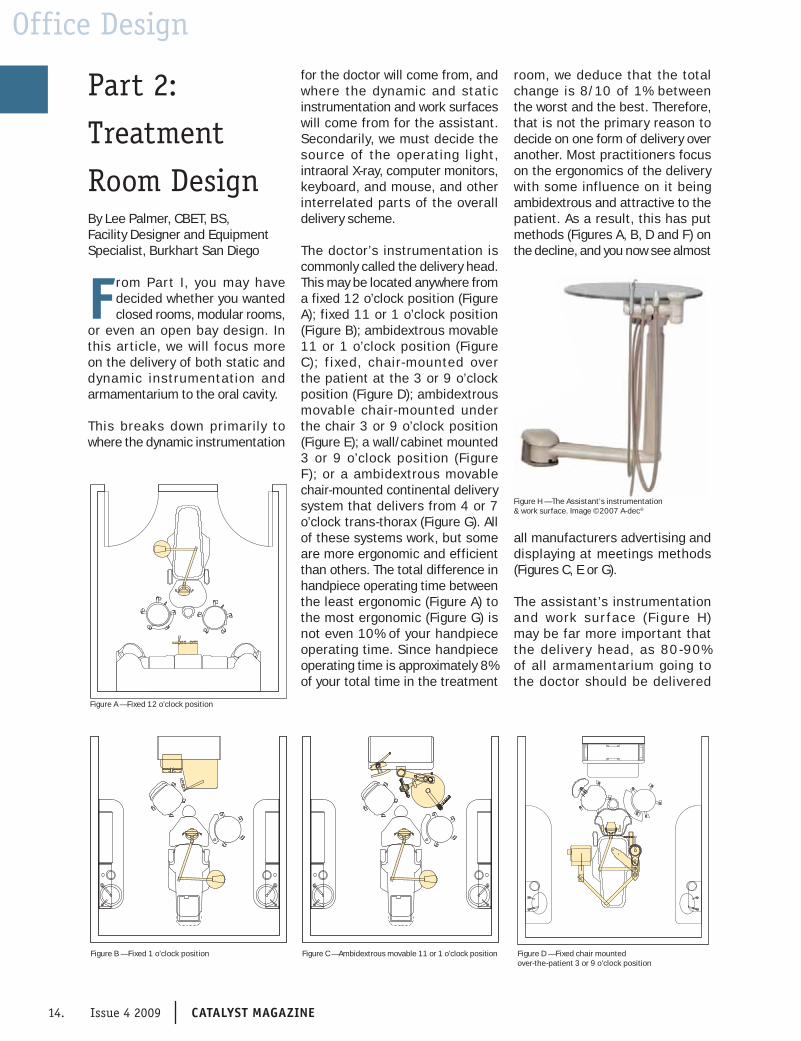
The doctor’s instrumentation is commonly called the delivery head. This may be located anywhere from a fixed 12 o’clock position (Figure A); fixed 11 or 1 o’clock position (Figure B); ambidextrous movable 11 or 1 o’clock position (Figure C); f ixed, chair-mounted over the patient at the 3 or 9 o’clock position (Figure D); ambidextrous movable chair-mounted under the chair 3 or 9 o’clock position (Figure E); a wall/cabinet mounted 3 or 9 o’clock position (Figure F); or a ambidextrous movable chair-mounted continental delivery system that delivers from 4 or 7 o’clock trans-thorax (Figure G). All of these systems work, but some are more ergonomic and efficient than others. The total difference in handpiece operating time between the least ergonomic (Figure A) to the most ergonomic (Figure G) is not even 10% of your handpiece operating time. Since handpiece operating time is approximately 8% of your total time in the treatment
room, we deduce that the total change is 8/10 of 1% between the worst and the best. Therefore, that is not the primary reason to decide on one form of delivery over another. Most practitioners focus on the ergonomics of the delivery with some influence on it being ambidextrous and attractive to the patient. As a result, this has put methods (Figures A, B, D and F) on the decline, and you now see almost
all manufacturers advertising and displaying at meetings methods (Figures C, E or G).
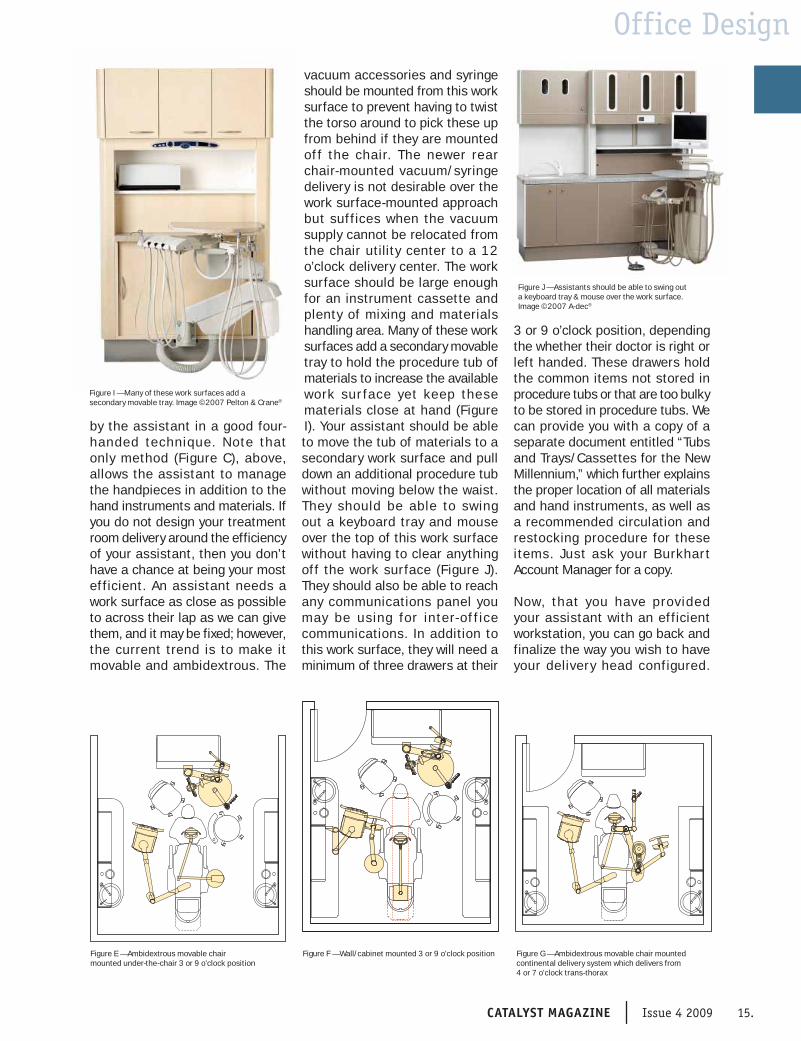
The assistant’s instrumentation and work sur face (F igure H) may be far more important that the delivery head, as 80 -90% of all armamentarium going to the doctor should be delivered
14. Issue 4 2009 CATALYST MAGAZINE
Figure A — Fixed 12 o’clock position
Figure B — Fixed 1 o’clock position Figure C — Ambidextrous movable 11 or 1 o’clock position Figure D — Fixed chair mounted over-the-patient 3 or 9 o’clock position
Figure H — The Assistant’s instrumentation & work surface. Image ©2007 A-dec®
Office Design
by the assistant in a good four-handed technique. Note that only method (Figure C), above, allows the assistant to manage the handpieces in addition to the hand instruments and materials. If you do not design your treatment room delivery around the efficiency of your assistant, then you don’t have a chance at being your most efficient. An assistant needs a work surface as close as possible to across their lap as we can give them, and it may be fixed; however, the current trend is to make it movable and ambidextrous. The
vacuum accessories and syringe should be mounted from this work surface to prevent having to twist the torso around to pick these up from behind if they are mounted of f the chair. The newer rear chair-mounted vacuum/syringe delivery is not desirable over the work surface-mounted approach but suffices when the vacuum supply cannot be relocated from the chair utility center to a 12 o’clock delivery center. The work surface should be large enough for an instrument cassette and plenty of mixing and materials handling area. Many of these work surfaces add a secondary movable tray to hold the procedure tub of materials to increase the available work sur face yet keep these materials close at hand (Figure I). Your assistant should be able to move the tub of materials to a secondary work surface and pull down an additional procedure tub without moving below the waist. They should be able to swing out a keyboard tray and mouse over the top of this work surface without having to clear anything off the work surface (Figure J). They should also be able to reach any communications panel you may be using for inter-of f ice communications. In addition to this work surface, they will need a minimum of three drawers at their
3 or 9 o’clock position, depending the whether their doctor is right or left handed. These drawers hold the common items not stored in procedure tubs or that are too bulky to be stored in procedure tubs. We can provide you with a copy of a separate document entitled “Tubs and Trays/Cassettes for the New Millennium,” which further explains the proper location of all materials and hand instruments, as well as a recommended circulation and restocking procedure for these items. Just ask your Burkhar t Account Manager for a copy.
Now, that you have provided your assistant with an efficient workstation, you can go back and finalize the way you wish to have your delivery head configured.
CATALYST MAGAZINE Issue 4 2009 15.
Figure E — Ambidextrous movable chair mounted under-the-chair 3 or 9 o’clock position
Figure F — Wall/cabinet mounted 3 or 9 o’clock position Figure G — Ambidextrous movable chair mounted continental delivery system which delivers from 4 or 7 o’clock trans-thorax
Figure I — Many of these work surfaces add a secondary movable tray. Image ©2007 Pelton & Crane®
Figure J — Assistants should be able to swing out a keyboard tray & mouse over the work surface. Image ©2007 A-dec®
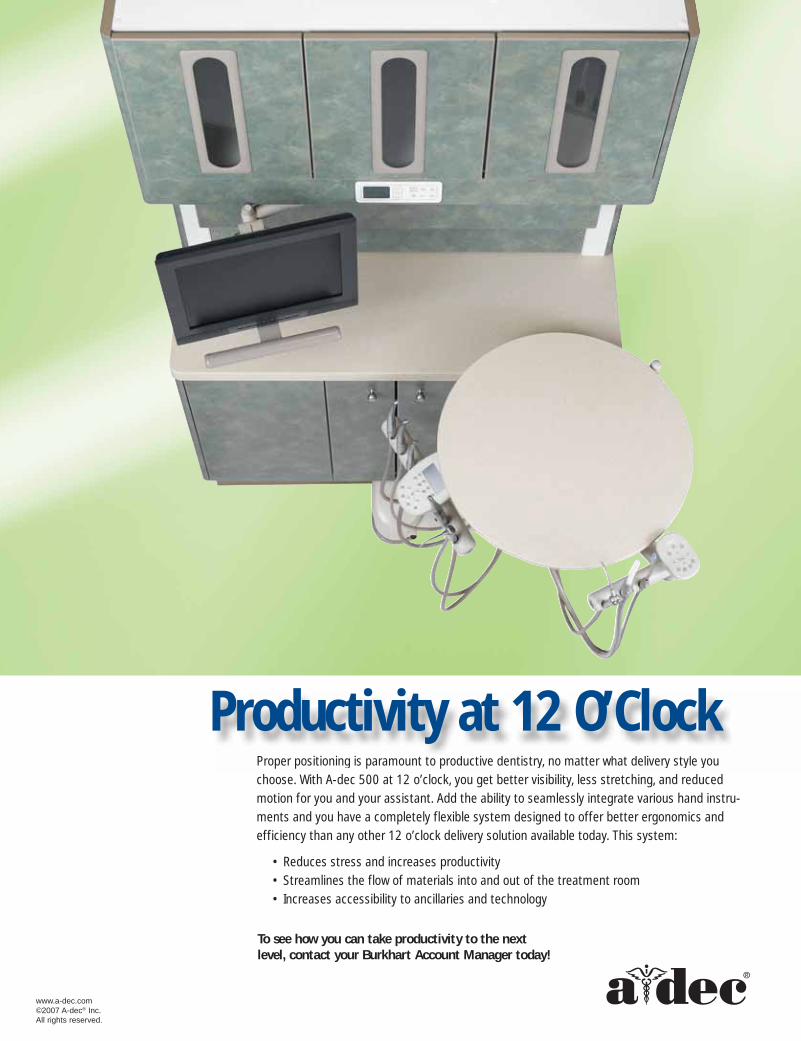
Proper positioning is paramount to productive dentistry, no matter what delivery style you
choose. With A-dec 500 at 12 o’clock, you get better visibility, less stretching, and reduced
motion for you and your assistant. Add the ability to seamlessly integrate various hand instru-
ments and you have a completely flexible system designed to offer better ergonomics and
efficiency than any other 12 o’clock delivery solution available today. This system:
• Reduces stress and increases productivity
• Streamlines the flow of materials into and out of the treatment room
• Increases accessibility to ancillaries and technology
5580
www.a-dec.com©2007 A-dec® Inc. All rights reserved.
Proper positioning is paramount to productive dentistry, no matter what delivery style you
Productivity at 12 O’Clock
To see how you can take productivity to the next level, contact your Burkhart Account Manager today!

Office Design
Once you have decided on these two systems, then you can start to consider where the light and intraoral X-ray and patient viewing monitor might come from.
Let’s explore light delivery for a moment. Of course, you can deliver it from a post mount on your chair that is either fixed or movable (ambidextrous), but if you have eliminated the treatment system from your chair, then you will have the cost of a mounting system added to the cost of the light itself. You can mount the light
on the ceiling, which is relatively ambidextrous for the practitioner, but it should be mounted on the side opposite of patient entry. A ceiling light is a good choice, but it adds the cost of backing and power in the ceiling to the light itself. Another choice is the track mounted light, which is truly ambidextrous, but it also adds the cost of the support and electrical, and it is the most expensive of all dental lights. Finally, a new method called a cabinet or wall mount is available (Figure K). This is becoming much more popular, as it does not involve the ceiling of the treatment room. In addition, it is ambidextrous and offers more positioning flexibility than even a track light, while costing about the same as a ceiling light. It can come from either side of the treatment room, and the light head stores directly above the patient’s head when the chair is in the dismissal position. Since it never needs to be swung away from the chair to allow entry or exit and never has to be shoved all the way down the track for the same reason, it is available with minimal movement once the
patient is reclined into an operating position.
The computer monitor can be chair mounted (Figure L) on either a fixed or movable (ambidextrous) mount, or it can be mounted from the ceiling or the wall/cabinet. The chair mount seems to be more popular today due to its proximity to the patient and practitioner, which allows a more intimate discussion of what the camera has captured. M any o f t h e c h a i r - m o un t e d monitors are being mounted higher to permit viewing of the monitor while in the reclined position. Many offices are using a separate ceiling or wall-mounted monitor arm to allow use of the monitor for viewing in both the upright and reclined positions. We have found that the best combination is one configured at 12 o’clock for the assistant and doctor to display information not intended for the patient, a second that is mounted to the chair for the doctor’s use during intraoral camera use and consultation, and a fixed, ceiling-mounted third monitor, which the patient can view during the examination using an
Figure L - A chair-mounted computer monitor. Image © 2007 A-dec®
Figure M - A pass-through cabinet for your intra-oral x-ray. Image© 2007 Pelton & Crane.
CATALYST MAGAZINE Issue 4 2009 17.
Figure K — A cabinet-mounted light. Image ©2007 A-dec®

Office Design
intraoral camera and to watch TV during treatment. A final solution that has gained popularity is to mount a monitor to the track-mounted dental light, so that it can be used in both the upright and reclined positions.
Finally, we need to locate the int raoral X - ray. This may be mounted off the 12 o’clock wall, which makes them ambidextrous; however, the original reason for this mounting was due to the relatively shor t-reach arms on X-rays some 50 years ago! The 12 o’clock position also necessitates the purchase of one X-ray per treatment room. Since we have a lot of things we want to deliver from the 12 o’clock wall, we have taken advantage of the new longer reach delivery arms and have moved the X-ray to either side wall, at the 3 or 9 o’clock of the patient. Many of these are now being mounted in either a pass-through cabinet in a regular wall or in cabinetry that has a pass through feature (Figure M - page 17). One must also consider the new portable X- ray uni t from Ar ibex called the Nomad Pro, as it eliminates all mounting considerations. It weighs only 6 pounds and provides excellent radiographs, especially when paired with digital sensors. Several of the intraoral X-rays that you might want to mount in a pass
through on a central cabinet or pass-through cabinet for a fixed wall treatment room offer a place to plug in the X-ray sensor (Figure N). This makes it convenient to use the sensor, as it swings out with the X-ray to any room that needs to make a radiograph. These are the Progeny Preva and Gendex Expert with any USB sensor, and the Planmeca Intra with its ProSensor. The ProSensor also comes in an Ethernet variety for connection to your network, so there is no “A/B” switch to change when you take it from one room to the next from a pass-through.
We hope this ar ticle has been useful in explaining the process of locating and select ing the equipment that is appropriate for your treatment room and as always, your local Burkhart Equipment Special is t can of fer speci f ic guidance regarding the brands and models that are best suited to your needs.
Figure N - Intra oral x-rays like the PLANMECA Intra combined with sensors like the PLANMECA ProSensor provide excellent radiographs and should be considered when designing new treatment areas.
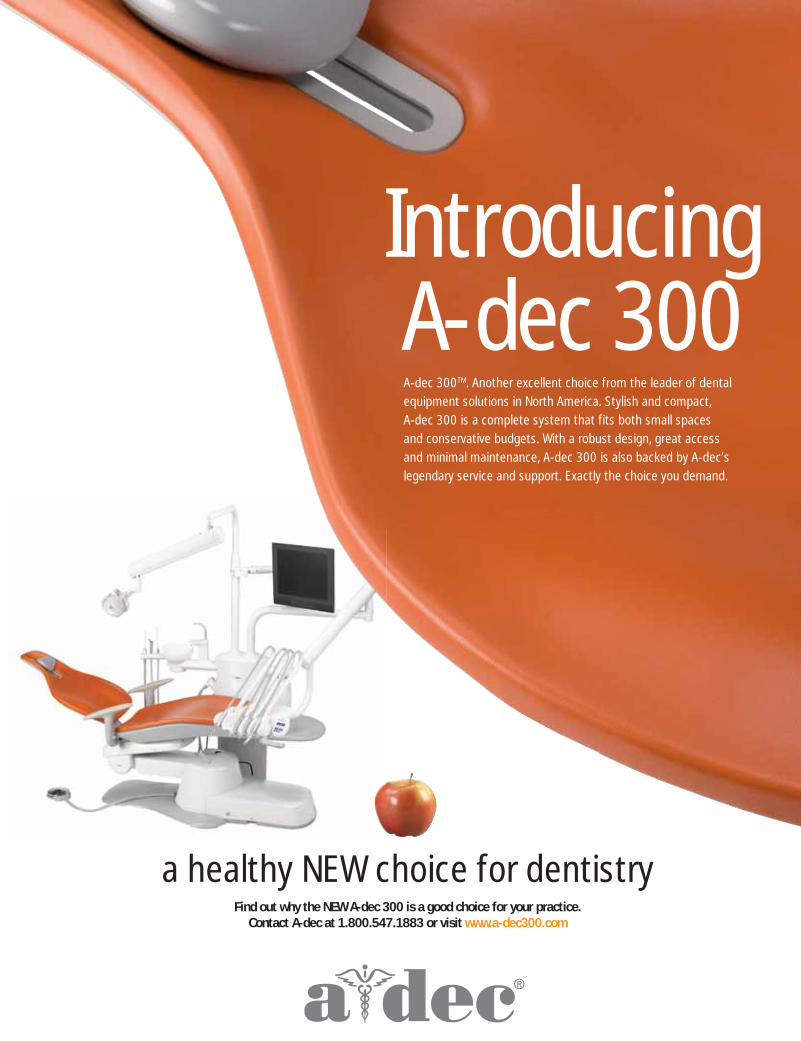
a healthy NEW choice for dentistryFind out why the NEW A-dec 300 is a good choice for your practice.
Contact A-dec at 1.800.547.1883 or visit www.a-dec300.com
Introducing A-dec 300A-dec 300TM. Another excellent choice from the leader of dental
equipment solutions in North America. Stylish and compact,
A-dec 300 is a complete system that fits both small spaces
and conservative budgets. With a robust design, great access
and minimal maintenance, A-dec 300 is also backed by A-dec’s
legendary service and support. Exactly the choice you demand.

HOW’S YOUR HEART?AIR TECHNIQUES
KEEPS YOUR PRACTICE PUMPING.
Make The Healthy Choice –– AirStar Compressors, STS And VacStar Vacuum Systems.Compressors and vacuum systems are at the very heart of your practice. In fact your success depends on them –– without them you simply could not treat your patients. So it is vital to choose the systems you know you can depend on, day after day, year after year. Which is exactly why so many dentists choose Air Techniques.
AirStar Compressors with NEW Membrane Dryer. Ultra-dry air, oil-free and virtually maintenance-free.STS Dry Vacuum Systems. High-performance, remarkably efficient and environmentally responsible.VacStar Wet Vacuum Systems. Save space and water, and they’re oil-free!
•
•
•
Count on Air Techniques compressors and vacuum systems…the heart of your healthy practice.
www.airtechniques.com
® ™
™
To order or for more information contact your local Burkhart Dental representative.
© 2
009
Air
Tech
niq
ues,
Inc.
Hobbies:
What I like about my job:
My Greatest challenge is:
Success at our office means:
What Burkhart means to me:
Dental Assistant, Premier Dental Care, PC - Colorado Springs, CO
Hiking, reading, spending time with family and friends and of course, watching sports especially baseball and college sports.
The satisfaction of knowing that I made a patient comfortable in an uncomfortable situation.
Letting a patient know that we are here to help them and educate them regarding their dental health and the importance of that knowledge.
Knowing that we have given our patients the utmost dental care in every aspect that our office offers.
Scott Plantenburg has been a great help to me just knowing that my ordering is being taken care of and if my office needs anything, he is there.
Lorie Jo Firestone, EDDA
CATALYST MAGAZINE Issue 4 2009 21.

Assistant Success
22. Issue 4 2009 CATALYST MAGAZINE
Put Me In, Coach!By Bill Price, Account Manager, Burkhart Austin
Imagine that you are the manager of a fictitious professional baseball team, and you have the option of using a designated hitter in your lineup. But your salary cap is maxed out, and you don’t have the money to pay a big-time slugger, so you make your pitcher bat in his place in the interest of saving money. The pitcher may not be produce anything offensively, and sure, there’s always the risk of injury or fatigue, but you really don’t have the money to pay an all-star to play only for offense.
Now imagine a modern day Babe Ruth approaches you and offers to play for the team free of charge. All he asks is that you make him the designated hitter. He’s had some education on pitching and fielding, but his only practical experience and training is at the plate—and he practices hitting all the time. He’s one of the most prolific hitters of all time, and in this imaginary league, he’s the designated hitter for several other teams, too. Since he’s not on any team’s payroll, the league commissioner has agreed to allow him to support all of you, and because his only goal is to make your team better, there is no risk that he will divulge any sensitive information to the other teams he works with[SF1]. His only goal is to make everyone more productive.
Such a player would not only give you more talent on the offense, but you would be able to allow your pitcher to do exactly what he does best – pitch! In addition to the obvious benefits, you could make use of the slugger’s experience in other clubhouses. This guy has played for the best and worst teams in the league, and he could
share strategies and ideas he’s gained from those organizations (without breaking confidentiality, of course), allowing you to apply that knowledge to your own team.
Can you imagine telling the slugger, “Thanks, but no thanks…?”
Every time I walk into a dental office and see the doctor scurry around a corner to avoid the dental sales rep who has just darkened her doorway, I feel like I should check to make sure I remembered deodorant that morning. Do I smell bad? Am I that unpleasant to look at or talk with? Do I need to trim some of those embarrassing nose hairs that make my face look like a party favor, or is Dr. Jones just afraid I will try to sell her something she doesn’t need or want?
While I realize there are plenty of Account Managers who have done a great deal to tarnish my profession’s reputation, the truth is, we represent a tremendous wealth of knowledge and training in topics
ranging from product knowledge to leadership within the practice. After all, our profession is handling dental merchandise, talking about dental equipment, and visiting dental offices that are doing many things to help themselves become more successful.
The most successful of f ices I visit are those that try to learn as much as they can, as often as they can. They want to know when I’m coming by, and they try to make themselves available at some point during my visit. They ask questions, and they give me homework. They actually look forward to my visits because I make it my mission to bring something of value to their offices every time I call on them.
Many offices would love to hire a consulting firm, but they don’t want to spend the money. I would argue that for offices that can’t go the consulting route, a good sales rep can offer the next best thing. Just like the slugger in my farfetched example, we reps visit scores of
“ They actually look forward to my visits because I make it my mission to bring something of value to their offices every time I call on them.”

Assistant Success
Integrated NuTorqueTM
The touchably intuitiveelectrichandpiece
www.DentalEZ.com
StarDental® NuTorque Electric:· Shortest, lighter-weight motorfor comfortable control
· Torque control - more power,more precision
· Easy-to-use touch screen· Endo and general memorypre-sets for all procedures
M A K E S Y O U R P R A C T I C E P E R F E C TTT TM
DentalEZ® Galaxy® Delivery System:· Flexibility and versatility to position instrumentsandmaterials wherever needed
· Improve overall operatory productivity· 100% seamless integration of intuitive NuTorqueelectric handpiece
dental offices every week, and we are able to observe the different ways those practices either succeed or fail. Most dentists will not visit 20 dental offices in their entire lives—I was in 20 offices last Tuesday.
In addition to the exposure I’ve had to the many dental practices in my territory, my employer, Burkhart Dental Supply, is vigilant about making sure we are the best trained sales force in the industry. My job is not only to learn everything I can about merchandise and equipment, bu t to learn about prac t ice management and how a dental practice works. Several times a year, I am sent to on-site training seminars that last several days. I don’t have any continuing education hours that some board requires of me, but I work for a company that is committed to transforming employees into resources for their customers.
By helping my offices become more productive businesses, I allow the doctors I serve to focus on what they do best – dentistry. Whether I am implementing inventory control systems or searching for coupons and free goods promotions that make sense for certain offices, everything I have been trained to do is designed to reduce the customer’s cost.
Maybe you’re reading this thinking, my rep has never really brought anything of value, or my rep never comes by, so when would I make use of him. Worse yet, I can’t stand my rep and his crazy nose hair! If that’s the case, I suggest you make a change in your representation, because you’re missing out on one of the least expensive, most effective resources available. If you don’t really know much about your rep, I would suggest you make
yourself available to him or her at some point to discuss your practice.
So the nex t t ime your dental sales representative drops by your office, don’t pass up on a golden opportunity to improve your business. It won’t cost you more than a couple of minutes, and it could get you a better return on your investment than any other resource available. In an uneasy economic environment, you’d be foolish to leave your potential MVP on the bench.
Bill Price is an Acccount
Manager in Austin, Texas.
Assistant Success
I Can’t Think of a Reason to Not Use BurkhartSupply Savings Guarantee Success Story
By Greg Biersack, Burkhart VP Corporate Operations
24. Issue 4 2009 CATALYST MAGAZINE
Dr. D av i d B r own r un s a thr iv ing prac t ice in the beautiful town of Yakima,
Wa sh ing ton . H e g rew up in Bremer ton, Washing ton and at tended Central Washing ton for his undergraduate degree. A positive experience in receiving dental treatment stimulated his interest in the dental profession. A f t e r g r a d u a t i n g f r o m t h e University of Washington Dental School in 1999, he decided to buy a practice in Yakima. He has built that practice into an extremely successful business, and he commented that he likes running the business almost as much as he does doing dentistry.
I had the chance to ask him a few questions about working with Burkhart and the Supply Savings Guarantee.
You have been on the Supply Savings program for 10 years. What was the appeal of the program?
The previous dentist purchased supplies from many dif ferent c omp anie s and c at a logue s . They had cards for the different products that told where they should call. This system was time consuming and cumbersome. The practice’s supply costs were 11% when I bought the practice. I am an avid supporter of strong systems and pay very close attention to the numbers. Jack Stewart (Burkhart Account Manager) presented the Supply Savings Guarantee program to me and it seemed like a “no-brainer.” The program controls
my costs, is efficient for my staff, and does not take my time. It only took me a very short time to figure out that this is what worked best for me.
What do you see as the best aspects of the Supply Savings Guarantee program?
It gives me piece of mind knowing that my supplies and cost controls are taken care of. I don’t have to shop around. This is a time savings for me so that I can focus on treating my patients and running the practice. It is one less thing to micromanage. I can focus on patient care and vision building for the practice.
What do you see as different about this program?
I really don’t pay attention to the other suppliers. I know they have programs to buy certain amounts, but Burkhart has controlled my costs and gives me great service. I am happy and loyal.
What do you l ike best about working with Jack Stewart?
I like having someone like Jack in my corner. I can ask him what is working in other offices, or I can ask him to research certain products for me. He always gets back to me with good information. He is part of our team. The program is great, but it is just the tip of the iceberg. The other intangibles that I get from Jack and the other Burkhart team members make my life easier.
Jim Waller (Burkhart Equipment Specialist) was instrumental in re-equipping my office when we did our remodel. He really took care of us. They all do so much more than just sell us supplies.
What are your thoughts about the service team that takes care of you?
They are fantastic! They are like team members. They always try to save me money and are looking out for my best interests. They suggest that we “try this” as a lowest cost solution. I have a great relationship with them.
Are there any additional thoughts that you would l ike to share with other doctors considering partnering with Burkhart?
Don’t think about it. Just do it! I can’t think of a reason not to use Burkhart.
Dr. Brown has been a Guarantee customer for 10 years. In his most recently completed Guarantee year, his supply percentage was 3.56%. This is a savings of $38,374 in comparison to his guaranteed percentage of 6.5%.
Thanks, Dr. Brown, for selecting Burkhar t to be your business partner.

High Power LED Curing Light
slim FASTCORDLESS
Slim Curing Probe Easier Posterior Access Better Visibility
Fast Cures 2mm cured in only 10 seconds
High Capacity Battery Hundreds of Cures Per Full Charge
Cordless Portable convenience
It’sPINK!
Buy 2, Get 1FREE!
Clinical
26. Issue 4 2009 CATALYST MAGAZINE
A Case Study in Implant AestheticsBy Rhys Spoor, DDS, FAGDAccredited Member of the American Academy of Cosmetic Dentistry
This case illustrates the creative use of restorat ive dental design and fixed prosthetics
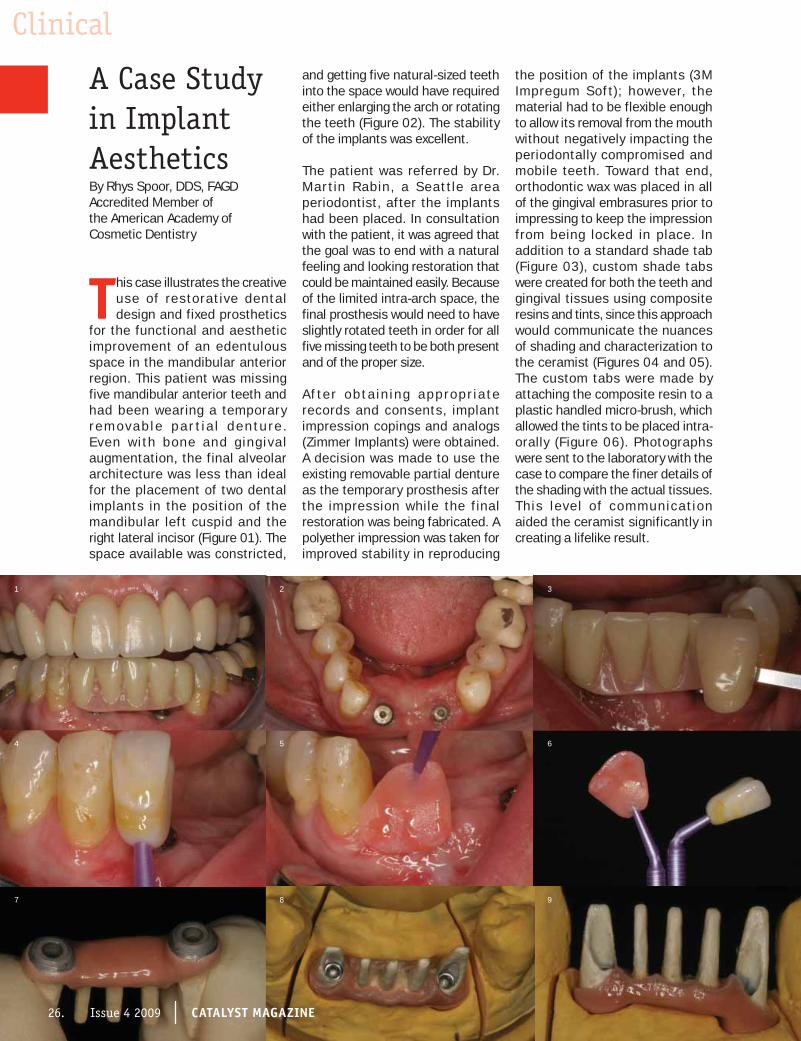
for the functional and aesthetic improvement of an edentulous space in the mandibular anterior region. This patient was missing five mandibular anterior teeth and had been wearing a temporary r e m ov ab l e p a r t i a l d e n t u r e . Even wi th bone and g ing ival augmentation, the final alveolar architecture was less than ideal for the placement of two dental implants in the position of the mandibular left cuspid and the right lateral incisor (Figure 01). The space available was constricted,
and getting five natural-sized teeth into the space would have required either enlarging the arch or rotating the teeth (Figure 02). The stability of the implants was excellent.
The patient was referred by Dr. Mar t in Rabin, a Seat tle area periodontist, after the implants had been placed. In consultation with the patient, it was agreed that the goal was to end with a natural feeling and looking restoration that could be maintained easily. Because of the limited intra-arch space, the final prosthesis would need to have slightly rotated teeth in order for all five missing teeth to be both present and of the proper size.
A f te r ob t a in ing appropr ia te records and consents, implant impression copings and analogs (Zimmer Implants) were obtained. A decision was made to use the existing removable partial denture as the temporary prosthesis after the impression while the f inal restoration was being fabricated. A polyether impression was taken for improved stability in reproducing
the position of the implants (3M Impregum Sof t); however, the material had to be flexible enough to allow its removal from the mouth without negatively impacting the periodontally compromised and mobile teeth. Toward that end, orthodontic wax was placed in all of the gingival embrasures prior to impressing to keep the impression from being locked in place. In addition to a standard shade tab (Figure 03), custom shade tabs were created for both the teeth and gingival tissues using composite resins and tints, since this approach would communicate the nuances of shading and characterization to the ceramist (Figures 04 and 05). The custom tabs were made by attaching the composite resin to a plastic handled micro-brush, which allowed the tints to be placed intra-orally (Figure 06). Photographs were sent to the laboratory with the case to compare the finer details of the shading with the actual tissues. This level of communicat ion aided the ceramist significantly in creating a lifelike result.
1
7
4
2
8
5
3
9
6
26. Issue 4 2009 CATALYST MAGAZINE

Clinical
CATALYST MAGAZINE Issue 4 2009 27.
ClinicalClinicalA metal framework was fabricated, and opaqued and pink gingival porcelain was placed with a flat contour, which interfaced tightly with the alveolar crest (Figure 07). This design had three major advantages: it allowed for easy oral hygiene, reduced the impaction of food during mastication, and made all subgingival margins screw retained, thus eliminating all subgingival cement margins as well as the need to remove subgingival cement. The final crowns were designed with the three center teeth as one unit that would ultimately be seated using a permanent resin cement (Kerr Maxcem Elite). The abutment crowns would be cemented with a temporary cement (Kerr Tempbond Clear), which would permit total retrievability of the restoration and allow for future repairs or modifications (Figures 08, 09 and 10).
The gingival tissues were cleared from the head of the implant fixtures with a tissue punch (Figure 11), and the restoration was tried and radiographed to ensure a precise
fit (Figure 12). The restoration was then removed, and the three “pontic” teeth were cemented with a resin cement (Figure 13). The abutment crowns were placed during this process to ensure the most precise alignment of all of the restorative pieces. It was important to check that the intraoral driver would fit between the seated pontic teeth and still align with the screw to full depth for torquing (Figure 14). The restoration was then reseated, and the final abutment screws were torqued to 25 N-cm according to the implant manufacturer’s recommendations (Figure 15). The abutment crowns were then seated with temporary cement, which gave the entire restoration retrievability, while the strength and retention of the restoration was screw retained.
The final photographs (Figures 16 and 17) show the restoration at three weeks after delivery, and indicate excellent gingival tissue blend and harmony with the adjacent dentition. By using creative design and technical precision, restorative
aesthetic dentistry can compensate for our lack of ability to completely rebuild supporting tissues to ideal contours. Clear communication between the patient, dentist, and the ceramist are integral to a successful outcome.
AcknowledgementsThe supportive tissue augmentation and implant placement was by Dr. Martin Rabin, periodontist, in Seat t le, WA. The exquisite ceramic art was created by Daniel Sorenson, CDT, Experience Dental Studio, and Provo, Utah.
Dr. Spoor maint a ins
a pr ivate pract ice in
aesthetic and restorative
dentistry in Seattle, WA
and can be contacted at
www.RhysSpoor.com.
Left Page: Figure 1 The patient after implant placement with removable temporary partial denture in place. Figure 2 The arch form showed a deficiency of space for properly sized and spaced missing teeth. Figure 3 Shade tab from Ivoclar Chromoscope shade guide showed the body shade to be 130. Figure 4 Custom shade tab made from Kerr Premise composite and Kerr Kolor Plus composite tints. Figure 5 Gingival custom shade tab made with Cosmodent gingival shaded composites and Kerr Kolor Plus tints. Figure 6 Microbrushes were used to hold the custom shade tabs. Figure 7 Gingival aspect of the restoration showing the flat interface with the alveolar crest. Figures 8, 9 and 10 (Figure 10 This Page) The final prosthesis on the laboratory model. Figure 11 Nobel Biocare gingival tissue punch
held in the fingers was used to clear excess tissue away from the implant fixture. Figure 12 The restoration being tried in and lightly torqued for radiographic verification of intimate seating. Figure 13 The three “pontic” teeth (Ivoclar e-Max) were seated with a light cured resin cement (Kerr MaxCem). Figure 14 The final restoration was checked to assure the torque driver had adequate clearance to seat the restoration intra-orally. Figure 15 The final restoration fully seated and torqued to 25Ncm (Zimmer implants). Note slight blanching of the gingival tissue. Figure 16 The abutment teeth have been cemented with Kerr Temp Bond Clear to allow for future retrieval of the restoration if the need arises. Figure 17 Adding slight rotations to the individual teeth while maintaining the proper tooth size attained the most natural appearance. Photos courtesy of Dr. Rhys Spoor.
10
15
12
11
16
13
3
17
14
CATALYST MAGAZINE Issue 4 2009 27.

The Power of a Group
The Woodlands Dental Group:The Power of a GroupBy Greg Biersack, Vice President of Corporate Operations
28. Issue 4 2009 CATALYST MAGAZINE
The year is 2009, and the country is experiencing its worst recession since WWII. A
group of friends in The Woodlands, Texas gathers for a photo. You can tell that they are professional and dedicated, but also that they are filled with the joy of friendship. They do not wear the signs of stress and anxiety; rather, they reflect the comfort associated with success and fun. The shoot is part Fortune magazine cover and part lit tle
league team photo. How did the group find this amazing comfort zone in their relationship? To understand the situation, we need to get into our time machine and return to the year 1981, the year of another big recession.
Getting TogetherIn 1981, two general dentists, Dr. Michael Freeman and Dr. David Ryder, started a discussion about
the possibility of working together in a group practice. They both had successful private practices but wondered about the benefits of g reater col laborat ion and economies of scale in sharing some of the expenses of a practice. They pulled into the discussion several other practicing dentists from The Woodlands to explore the possibility further. Among them were Dr. Calvin Jochetz (general dentist), Dr. Ron Rogers (orthodontist), Dr. Robert Dernick (general dentist), and Dr. Michael Dwyer (periodontist). “We knew nothing about how a group practice might work,” said Dr. Freeman. “So we decided to look for a seminar,” added Dr. Ryder. And off they went to Pocatello, Idaho to learn from Porter Sutton about how to put together a possible arrangement. Porter had helped to form several other dental groups and was excited about sharing this possibility. All of the doctors credit their experience in working with Porter to clear the path toward their association.
“For the next two years we met almost every week to plan how we would make this work,” Dr. Dernick said. “We had to buy the land, build a facility, and find a way to merge six practices.” To help them during that time, they also solicited the assistance of Don Clay, a corporate consultant. “Don taught us corporate thinking. We needed to get out of an individual way of thinking and learn to think as a group. We needed a common vision,” said Dr. Dernick. “We were lone wolves, and we needed to learn to get along and focus on the group,” added Dr. Jochetz. In addition to the change in how they were practicing, they all knew that The doctors of The Woodlands Dental Group show their lighter sides.Back (left to right): Dr. Wade Williams, Dr. Calvin Jochetz, Dr.
Robert Dernick, Dr. Judith Ragsdale, Dr. David Epstein & Dr. Michael Dwyer. Front (left and right): Dr. David Ryder & Dr. Michael Freeman. Photo by Cliff Roe © 2009

The Power of a Group
CATALYST MAGAZINE Issue 4 2009 29.
they would have to bite off a big expense; it was a big decision to make in the midst of a recession. “I knew that this would reduce my net to start out with. But it was with the belief that eventually, my net would be better off,” said Dr. Jochetz.
Valley of FireIn 1985, after years of planning, building, and countless meetings, the Woodlands Dental Group prepared to open its doors. They star ted of f in an arrangement that they described as a true group. By this, they meant that they would share all expenses, staff, patients, and profit. “Within the first six months, we learned that the true group idea was not going to work, and that we would have to do something differently,” said Dr. Freeman. They felt that it was difficult for the patients, who were accustomed to seeing “their dentist,” to see someone different. Moreover, it was difficult for the staff, the members of which constant ly found themselves working with a different dentist. Dr. Ryder added, “We determined that it was not a good concept for the pat ient . They did not like it. Additionally, we had an administrator handling the staff and they did not like it. We knew that we would have to morph.” This was a difficult time for the group. Revenue was down as a direct result of a major decline in oil field business profits. Additionally, they each carried the burden of substantial additional debt. “Houston was in the grip of an energy recession, so our growth f latlined. We needed to make
changes and turn things around quickly,” Dr. Ryder exclaimed.
Equipped with the belief that what they were doing was best for all of them, they continued to meet on a weekly basis to work through the challenges. They had an unshakable commitment to the group’s vision. “We had to go through the Valley of Fire. It required a lot of trial and error, but we were lucky in that we had compatible personalities, similar training, and a lot of things in common,” said Dr. Dernick. They made a change so that patients regularly saw the same dentist. They altered the personnel structure so that some staff members worked in teams for a single doctor while all shared a core business office team. They also revised their expense-sharing and income al loc at ion . “ We continued to meet and make a tweak here and there. It definitely involved some angst, but we just kept gnawing our way through it,” said Dr. Ryder. Additionally, to strengthen the services they offered, they added a seventh member to the group, Dr. Judith Ragsdale, a Pediatric Dentist. She recalls, “I was right out of school and had to build my practice from scratch. I felt connected to the others for mentorship.”
A Common VisionAlthough each doctor was very different in many ways, they all worked hard to cement a common vision for the group. Dr. Freeman put it this way, “Every dentist is dif ferent. We use dif ferent equipment , have a di f ferent approach to working with our staff, and want to work different hours. We needed to have leeway in doing things.” However, what bound them together despite these differences was a set of priorities that listed patient first, group second, and the individual third. “We all had a desire to give great service to the patients,” said Dr. Ragsdale. “We
Top Photo: Group Support Staff (left to right) Jill Hill, Linda Overcast, Marla Anderson & Nicole Purvis. Middle Photo (left to right) Back row - Sue Nadolski, Aimee Holleman, Andrea “Andie” Willis & Kathy King. Middle Row - Anita Gilbert & Chirstina Gonzales. Front - Dr. Michael Freedman. Bottom Photo (left to right) Back Row - Penni Biehl, Jennifer Mathena, Tina Aitken-Sanchez, Holly Abernathy & Marla Anderson. Second Row - Dr. David Ryder, Dr. David Epstein, Donna Yasoni & Cindy Ashley: Photos by Cliff Roe © 2009.
“We all had a desire to give great service to the patients.”- Dr. Judith Ragsdale

worked with a consultant who would always encourage us to put the patient first. It reminded us of what was most important.” This top priority was reflected in the comments each doctor made as they defined success. Dr. Freeman said that success is “patients feeling taken care of.” Dr. Ryder shared that patient retention and loyalty were the keys to their success. Dr. Jochetz felt that success was defined as doing fair, honest, quality oriented dentistry for the patient. Finally, Dr. Dwyer observed, “You have to treat the patient as you would a member of your family and be cognizant of what is best for them. We want to make dentistr y a pleasant experience.”
The second priority was the group. “We all recognized that we couldn’t have things our own way,” said Dr. Ragsdale. When differences came
up in the group, each member would have a vote. “Whatever the result, you would have to move on. You couldn’t let it fester. You would have to trust the wisdom and judgment of the others,” she said. Dr. Dernick added, “We had to agree on common things. We learned to share and be happy. We had to sacrifice and do what was best for the group.” This sharing included leadership within the group. “Every year, we would have a dif ferent managing par tner. This person was responsible for handling the day-to-day decisions for the group and bringing the group together for bigger decisions
monthly or quarterly,” said Dernick. Dr. Jochetz added, “We would get together and vote on issues; the majority would always win.” This shared leadership model, coupled with a willingness to put the group before the individual, has remained consistent over time.
23 Years ForwardFast forward 23 years to 2008, and we find these same dentists still working together in a successful and thriving group. Considering the changes that have happened naturally with each doctor and the shifts that have taken place around them, this is an amazing accomplishment. “Things have continually evolved with the group. We have learned what each doctor can and should be responsible for, and in what areas we should share,” said Dr. Dernick. They have worked together so closely and shared so
much that they have found ways to strengthen the group progressively. “We spend time together each day at lunch. It is here that we discuss issues that come up and work through those issues. We used to meet weekly, then monthly, then quarterly. Now we tackle issues as they arise,” Dr. Dernick added. Through these years of evolution, each doctor has benefited from their joint experience and from the group, and they are quick to share these benefits. “For me, the biggest benefit has been the fun that we have. I know that my net has been better, but it is the fun that I have that was missing
“...the best benefit is the fun that we have. You can’t put a dollar value on it.” -Dr. Michael Freeman
Photo 1 (left to right) Standing - Debbie Powers, Denise Clark, Maria Russell & Lorene Kubeczka. Seated - Rhonda Chenet & Dr. Michael Dwyer. Photo 2 (left to right) Back Row - Andrea Stokes, Amy Liczwek, Jeflyn Brocato, Cynthia Givens, Marcey Phillips, Heather Sauter & Kim McShan. Second Row - Beth Ann Nichols & Nancy Copley. Seated - Dr. Judith Ragsdale. Photo 3 (left to right) Back Row - Maria Ebert, Kara Hinkinbein, Michelle McGill & Suzanne Hebert. Seated - Nicole Crawford, Marty Alverez & Dr. Robert Dernick. Photo 4 (left to right) Back Row - Jan Smith, Cheri Ferguson & Patricia Etheridge. Seated - Lisa O’Neill, Pam Meyer, Dr. Calvin Jochetz & Kathie Boswell. Photo 5 (left to right) Back Row - Amy Bynum, Marcey Phillips & Laura Heckart. Second Row - Olga Lopez & Linda Dolyniuk. Front: Dr. Wade Williams. Photos by Cliff Roe © 2009
30. Issue 4 2009 CATALYST MAGAZINE
1
2
3
4
5

Successdefined for (and by) the group:
“Finding balance and happiness where I work, having the ability to attain financial goals, and maintaining a quality family life.” -Dr. Robert Dernick
“Doing the best dentistry for the patient, and staying together as friends.” -Dr. Calvin Jochetz
“Positive perception of patients, fulfillment of staff, good reputation in community.” -Dr. Michael Freeman
“The longevity and continuity of the staff – they feel at home, are happy, have fun, and care about each other. Of course, patient retention is
important as well.” -Dr. David Ryder
Advicethey would give to a group of dentists considering a group practice:
“Make sure that everyone owns equally, like whoyou are working with, be willing to compromise, and protect the group.” -Dr. David Ryder
“Ask why you’re doing it in the first place, organize and build around goals, look around at various group models, don’t be in a hurry, and meet oftento develop a structure and agreement.” -Dr. Michael Freeman
“Choose the right people, conduct your due diligence,get all of your agreements in writing, and then, JUST DO IT – it is a lot more fun!” -Dr. Calvin Jochetz
“Ensure the doctors are compatible. Get to know each other as well as possible, get someone to help you think as a group, and be willing to give up selfish behavior.” -Dr. Robert Dernick
Workingwith Burkhart:
“We are all very pro-Burkhart. They are committedto seeing us succeed, and that shines through. Shirley does a great job, and we have nothing but praise for Burkhart. It has been a tremendous company for us.” -Dr. Michael Freeman
“Burkhart is the best. They live up to theirpromises. We have a very good relationship with allof the people at Burkhart. The people [at Burkhart]are quality people!” -Dr. Calvin Jochetz
“We have a great relationship with Burkhart and Shirley—You cannot put a value on a relationship. They treat us well, and we appreciate it.” -Dr. David Ryder
from my solo practice,” said Dr. Jochetz. Dr. Dernick noted, “The rewards have been worth 10 times what I gave up. We learn so much from each other every day talking at lunch about the cases we are working on. The shared knowledge is so valuable.” Dr. Freeman added, “[By] practicing with other dentists, I can always bounce things off my friends. I have someone to cover for me when I am out of town, and I do not have to worry; I have staff backup, I have lower overhead because of economies of scale, and I get to work with happy people. But the best benefit is the fun that we have. You can’t put a dollar value on it.”
Preparing for TransitionIn 2008, Dr. Rogers retired, and the orthodontic part of the group was moved under the care of Dr. Wade Williams. It was the first step in what will be a series of transitions for a number of dentists at The Woodlands Dental group. Dr. Williams is excited to work for the group and have an opportunity to become a partner. He said, “The other dentists provide high quality treatment, and that made me feel very comfortable. I have been able to find people with the same vision that I have for a practice. The group has been patient and willing to share advice.” When asked what advice he would give others considering joining the group, he shared, “Build your relationships. Be willing to compromise. Take into consideration other factors and people.” Just one month ago, a second transition took place as Dr. Ryder brought Dr. Epstein in as an associate in the group. Dr. Epstein noted, “I liked how the practice was run. They have great patients. I can ask the other doctors’ opinions and learn from them.”
Dr. Ragsdale shared her excitement about the transitions to the next group of dent ists , especially because of the new blood and ideas being infused into the
group. But they all recognize the importance of selecting the right doctors to join the practice for the transitions. The new dentists must be willing to buy into the vision of the group, be willing to share, and consistently place the group before themselves. Dr. Jochetz shared, “It is like a marriage. They need to be prepared for give and take.” This will be the most critical component for the transit ions within the practice as well as for the long-term success of The Woodlands Dental Group.
A Picture Tells a Thousand WordsWhat started out as an idea many years ago has since turned into a long-running success story. The connections and bonds are apparent in everyone’s faces as the photographer snaps away. Through the tireless efforts of the dentists and their teams, a commitment to their patients, and a belief in the power of the group, the doctors of The Woodlands Dental Group have experienced amazing success and have accomplished so much—together. Congratulations and smile wide; there is so much to be happy about.
The Woodlands Dental Group has been a client of Burkhart since 1998, and the practice has been on the Supply Savings Guarantee program since that time. Over this 10-year period, Burkhart has remained been below the office’s guaranteed percentage each year, and has saved the group $397,356. The Woodlands Dental Group is happy to share their very positive feelings about the Burkhart service department and their technician, Alan Aultman. Shirley Lusk is the Burkhart Account Manager that takes care of the Woodlands Dental Group.
CATALYST MAGAZINE Issue 4 2009 31.
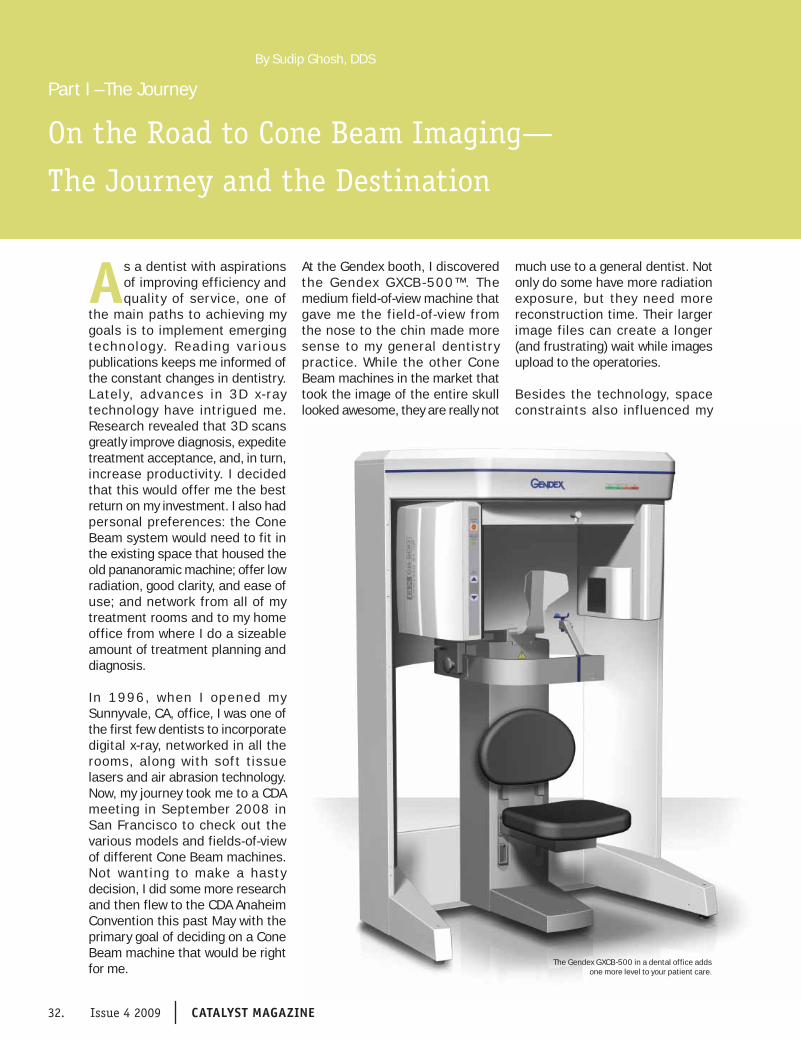
Technology
Part I –The Journey
On the Road to Cone Beam Imaging—
The Journey and the Destination
By Sudip Ghosh, DDS
32. Issue 4 2009 CATALYST MAGAZINE
As a dentist with aspirations of improving efficiency and quality of service, one of
the main paths to achieving my goals is to implement emerging technolog y. Reading var ious publications keeps me informed of the constant changes in dentistry. Lately, advances in 3D x- ray technology have intrigued me. Research revealed that 3D scans greatly improve diagnosis, expedite treatment acceptance, and, in turn, increase productivity. I decided that this would offer me the best return on my investment. I also had personal preferences: the Cone Beam system would need to fit in the existing space that housed the old pananoramic machine; offer low radiation, good clarity, and ease of use; and network from all of my treatment rooms and to my home office from where I do a sizeable amount of treatment planning and diagnosis.
In 1996, when I opened my Sunnyvale, CA, office, I was one of the first few dentists to incorporate digital x-ray, networked in all the rooms, along with sof t t issue lasers and air abrasion technology. Now, my journey took me to a CDA meeting in September 2008 in San Francisco to check out the various models and fields-of-view of different Cone Beam machines. Not wanting to make a hasty decision, I did some more research and then flew to the CDA Anaheim Convention this past May with the primary goal of deciding on a Cone Beam machine that would be right for me.
At the Gendex booth, I discovered the Gendex GXCB -500™. The medium field-of-view machine that gave me the field-of-view from the nose to the chin made more sense to my general dentistry practice. While the other Cone Beam machines in the market that took the image of the entire skull looked awesome, they are really not
much use to a general dentist. Not only do some have more radiation exposure, but they need more reconstruction time. Their larger image files can create a longer (and frustrating) wait while images upload to the operatories.
Besides the technology, space constraints also influenced my
The Gendex GXCB-500 in a dental office adds one more level to your patient care.

Technology
CATALYST MAGAZINE Issue 4 2009 33.
CATALYST MAGAZINE Issue 4 2008 33.
choice. My panoramic machine was situated in a small 4 foot by 4 foot space along the main hallway. With no desire to remodel and the need to use the existing 110V electrical outlet, I was able to check that aspect off of my list of requirements.
In Anaheim, I approached the Gendex booth and started asking questions. Taking a no-nonsense approach, I was looking for answers and had no time to waste. Gendex representative, Larry Gioffre was extremely helpful and answered all my queries precisely. Since I had some previous challenging experiences with other dealers, he walked me over to Burkhart Dental. I met with John Arauzo, the Bay Area Equipment Specialist and then with Lisa Wells, the Bay Area Branch Manager, who sat with me and completed the purchase agreement in about 15 minutes with no ‘ifs, ands, or buts.’ She even agreed to move this equipment at a later date at no charge if I decided to move my practice to another location in the future. The price was great, the service offerings were great—I had no reason to say ‘no.’ I finished my work at the CDA Convention way before lunch and had the whole day to myself.
Larry Gioffre came to my office the very next working day, re-measured the space and completed the plan for the installation. Three weeks later, the entire team from Gendex and Burkhart came to the install. The team included Alan Young, Gendex Western Regional Field Services Manager, Edgar Sanchez, Gendex Applications Trainer, Larry Martel, Burkhart Service Technician, and Neil Johnson, Burkhart Service Technician. This was on a Thursday, and three dentists were working in the office. Apart from moving this machine through the waiting room, there was very little disruption. When the installers encountered a problem in positioning this machine into this space, they quickly dismantled and reassembled it in the space.
Alan Young worked with my Network Adminis t rator to seamle s s ly integrate the software to all my rooms and the home office. He also helped to install the photographic printer that day. During this time, my patients were walking in and out of the main hallway with very little disruption. All the work was done ver y professionally and with no noise at all. The service from Gendex and Burkhart was remarkable. Lisa continued to check in during the process to ask if everything was going well. When a small glitch arose, they listened and fixed it promptly.
The next day was the only day we kept the office closed. Three people from Gendex flew in, along with Burkhart’s Larry Martel, to train my entire staff. We learned how to calibrate the unit, and to take and view images. We were excited and a bit apprehensive. In all honesty, this is complex technology—it provides a lot of vital information. We learned so much on that day, but still wanted time to explore the machine ourselves to discover all of its capabilities. Alan returned for an additional training session later. Although we are already using our system, we are still in the learning process for certain applications, which is normal.
After installation and training, it was ‘business as usual’—but even better, now that we had the Cone Beam. There were no boxes, no clutter; everything was networked and backed up from the very first day. The best part is that patients were impressed that they didn’t have to travel to a hospital setting or x-ray lab. I was proud to show them clearly the location of their infection or the nerve. I can visually show the patients their problems, possible complications, and the post-treatment results. All of those details are clearly visible on the 3-D scan.
Even in the shor t t ime since my C one B e am sy s tem was
installed, efficiency has increased tremendously. Lisa from Burkhart still calls and she and our account manager, Dennis McSweeney, visit personally to see how we are progressing. That’s a nice touch. Even though I just made a big investment, I’m already thinking that since the process went so smoothly, I will return to them for my next new equipment purchase.
So, this was my journey, and I have happily arrived at my destination, encountering very few bumps along the road. In part 2, I will share my destination—how my GXCB-500 is helping me to reach my goals of greater efficiency, increased treatment acceptance, and above all, better patient care. Next time, it’s all about the smiles.
A f t e r g r a d u a t i n g
dental school from The
University of Bombay
i n I n d i a i n 1 9 8 3 ,
D r. Gho sh e arne d a
M a s t e r o f S c i e n c e
(MS) in Endodontics &
Restorative in 1987. In
1999, he completed a Master of Science
(MS) program and a Certificate degree in
Operative Dentistry from the University
of Iowa. Since 1996, he is in private
practice with his wife, Manisha Ghosh, who
graduated from Dental School in 1985
from the University of Bombay, India. She
also has Masters Degree in Health Care
Administration (MHA) and a MBA from the
University of Houston, Texas. Both dentists
are members of the ADA, CDA, and Santa
Clara Dental Society.
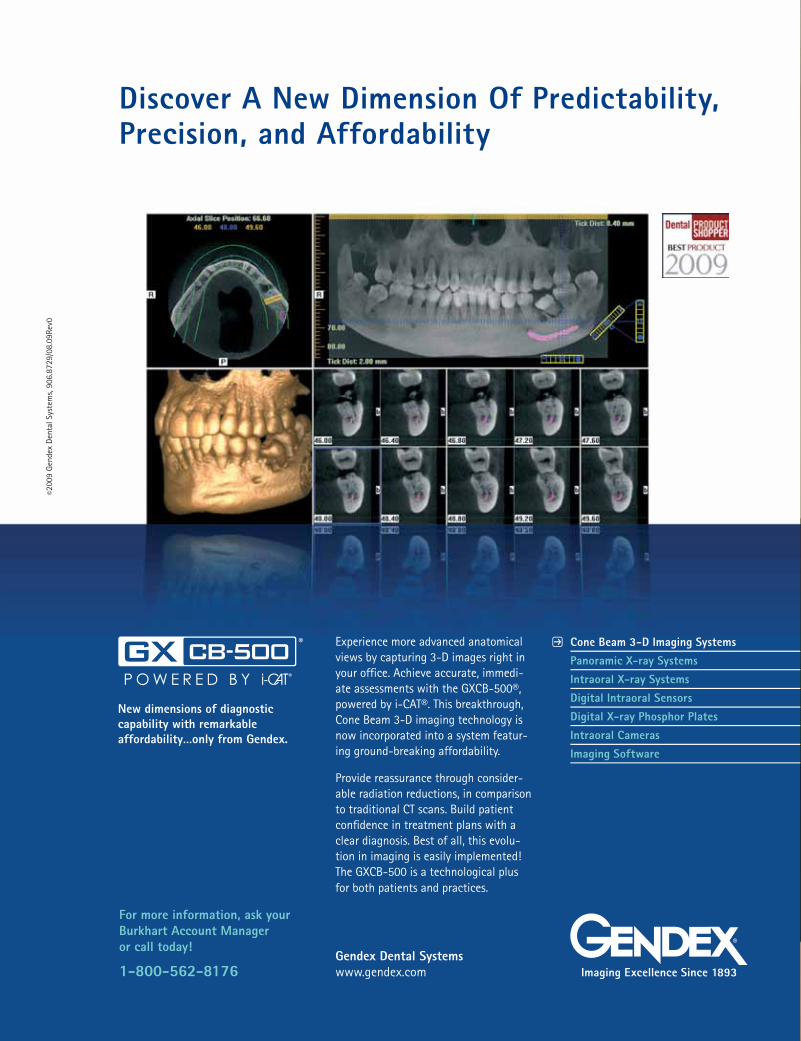
34. Issue 4 2008 CATALYST MAGAZINE
Discover A New Dimension Of Predictability, Precision, and Affordability
New dimensions of diagnostic capability with remarkable affordability…only from Gendex.
Experience more advanced anatomical views by capturing 3-D images right in your office. Achieve accurate, immedi-ate assessments with the GXCB-500®, powered by i-CAT®. This breakthrough, Cone Beam 3-D imaging technology is now incorporated into a system featur-ing ground-breaking affordability.
Provide reassurance through consider-able radiation reductions, in comparison to traditional CT scans. Build patient confidence in treatment plans with a clear diagnosis. Best of all, this evolu-tion in imaging is easily implemented! The GXCB-500 is a technological plus for both patients and practices.
Gendex Dental Systemswww.gendex.com
Cone Beam 3-D Imaging SystemsPanoramic X-ray SystemsIntraoral X-ray SystemsDigital Intraoral SensorsDigital X-ray Phosphor PlatesIntraoral CamerasImaging Software
P
Imaging Excellence Since 1893
©200
9 G
ende
x De
ntal
Sys
tem
s, 90
6.87
29/0
8.09
Rev0
For more information, ask your Burkhart Account Manager or call today!
1-800-562-8176
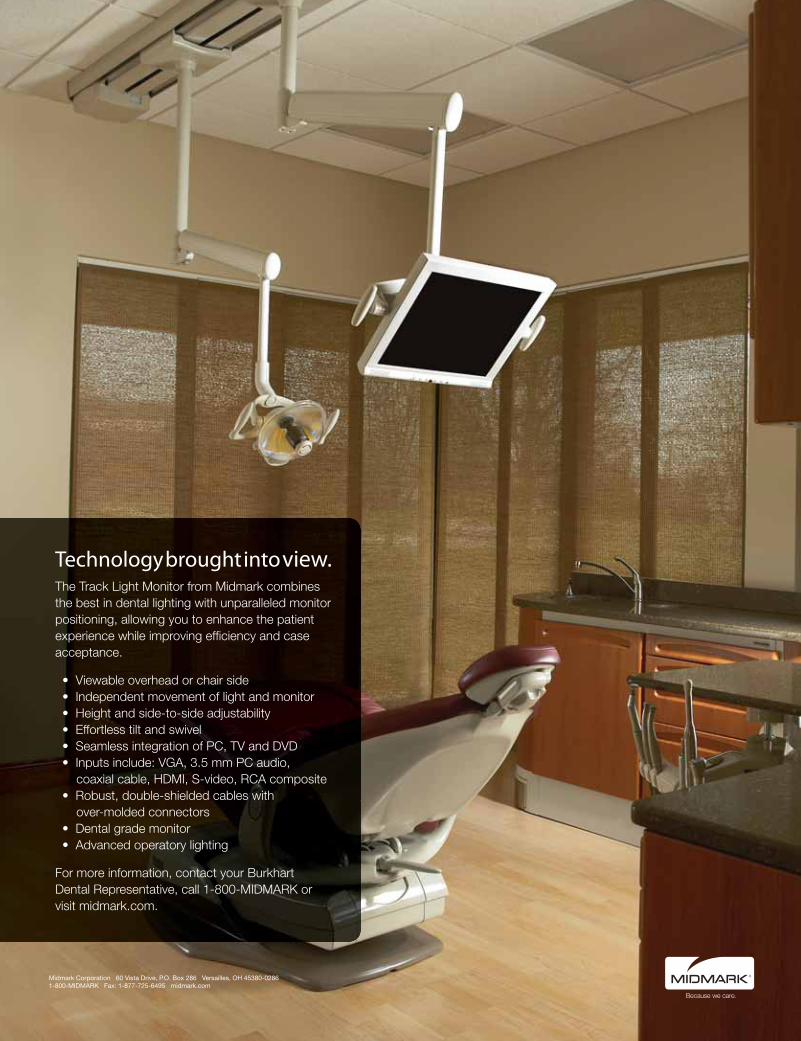

TechnologyTechnology
36. Issue 4 2009 CATALYST MAGAZINE
Q
Q
Q
Q
Q
Talking Cone BeamDr. Reznick & Dr. Patel discuss 3-D cone beam imaging in the practice, and how it can help doctors work together to provide better care for their patients.
Tell us about yourself and your practices:
Dr. Reznick (hereafter, Dr. R): I went to dental school at Tufts University, trained in Oral and Maxillofacial Surgery at the University of Southern California, then went back to obtain my medical degree. I have practiced in suburban Los Angeles for 18 years. My practice is in a middle to upper middle income area, and my patients vary from blue-collar workers, to soccer moms and their kids, to the CEOs of major corporations, and a number of well-known Hollywood celebrities. My patients come from the local area, from throughout California, and occasionally from outside the state—even internationally.
Dr. Patel (hereaf ter, Dr. P): I graduated from Ohio State University in 2006. Most candidates are required to complete a specialty in Prosthodontics, but I was fortunate enough to be admitted into the Implant Prosthodontics Program under Professor Edwin A. McGlumphy directly from dental school. I now have a private practice that focuses on General, Cosmetic, and Implant Prosthodontic Dentistry. I enjoy treating complex reconstructive cases and plan to focus my practice entirely on these cases in the near future. I rely on my specialists (Oral Surgeons, Periodontists, Orthodontists, etc.) for comprehensive and inter-disciplinary care.
What do you look for when referring to specialists?
Dr. P: Without the cone beam in my office, I never really had defined
criteria for referring patients. It was almost like I used to pick a surgeon out of a hat. With cone beam in my office, I can clearly see everything I need in order to formulate and develop an ideal treatment plan. I have the ability to refer with confidence, knowing that I am providing my specialists with what they need to achieve optimal results. I can make decisions quickly and efficiently because with 3-D imaging, what you see is what you get! Because of this technology, my office receives as many referrals as we refer out. We see a wide range of patients, and often receive referrals from our specialists for 3-D imaging and treatment planning.
What are the sources of your referrals?
Dr. R: In my practice, the majority of patients referred to me are from GPs in the local area. I also see a number of patients referred from GPs and specialists throughout Southern Cal i fornia. Another referral source is from the Internet. I was one of the first oral surgeons to have a Web site for my practice. Many patients come to me after reading about the practice on my Web site. If you Google my name, you get at least ten pages [of results][SF5], and I suspect many patients come to my office as a result.
What types of cases do you see, and what about general practitioner referrals? Do they involve a certain type of case?
Dr. R: I see the full variety of situations, from simple single implant cases, to multiple implant reconstruction, to complicated cases that may require multiple procedures over a 1 to 2-year period. What I’ve found in teaching oral surgery is that there are varying levels of training and expertise with GPs as well as with specialists. There are some very
competent and well-trained GPs doing their own implant surgery. There are also those who have taken a couple of courses, but only do a few implant placements each year, so their experience remains limited. What I’ve found, is that the general dentist who is very well versed in implant dentistry is more apt to think about implants as an option when planning their patients’ treatment. I actually see more complicated cases … from those GPs who are comfortable with implant dentistry and actually place their own implants and do the restorations on simpler cases. Those dentists who do their own implants understand what goes into the treatment planning. They’re great to work with. They see the limitations [and] the difficulties, and they appreciate all of the factors that lead to good treatment outcomes.
What sort of impact does cone beam have on guided implant surgery?
Dr. R: This is the prime use of cone beam imaging in dental practices. Guided Implant Surgery is the latest quantum leap in implant surgery. We used to use a panoramic radiograph and study models to evaluate potential implant sites. From there, clinical experience, surgical art, and guesswork were used to perform implant surgery. Many factors could adversely affect implant placement. I’ve seen articles and textbook chapters where even the “exper ts” had implants coming out off-angle or poorly-positioned. Guided Implant Surgery allows us to diagnose, treatment plan, and work from 3-dimensional CT images of the bone. Because we can see all the important anatomy without distor t ion, and take accurate measurements, we can place implants with much more precision. Many times, smaller incisions can be made, and using custom-made surgical guides, the implant placement is more accurate. This

Technology
CATALYST MAGAZINE Issue 4 2009 37.
Q
Q
Q
Q
saves significant time in surgery. As a result, I can schedule more patients in my day, increasing my daily productivity. This is one of the unexpected benefits we enjoy that I alluded to earlier.
What effect does cone beam have on the communication process?
Dr. P: For me, things have changed very rapidly, and it’s all due to cone beam imaging being integrated into my office. Prior to cone beam imaging, communication with a referral was difficult and cumbersome. Communication is something we all strive to improve upon, along with continuity of care. We need to have everyone, the GP, the specialist, and the patient all on the same page. I think having cone beam has revolutionized the way we work together. This allows us to communicate digitally. With the system we employ, we can pull up the very treatment plan we work on, change it, and send it back and forth for review until we come to an agreement. This streamlines the whole process and ends up satisfying all parties, including the patient, much more quickly than the typical methods. Communication is now less of an issue because it’s so much easier to do with cone beam and its tools. It’s a great benefit to our patients.
Dr. R: Communication is absolutely essential. The general dentist is the captain of the ship when dealing with multidisciplinary treatments. As a specialist, [since] I rely very heavily on referrals, it’s essential that I have good communication channels with my referring dentists, because if I don’t, they will be out of the loop and feel like they would need to refer elsewhere. Having the cone beam in the office has improved the communication with the general dentist. They can see implant treatment plans before they are placed, through e-mails or on interactive 3-D viewer CDs. They can give their feedback to me, and the final result will be the most ideal treatment plan from both the surgical and prosthetic standpoints.
What about using cone beam images for patient education?
Dr. R: That’s been really important. I’m a strong advocate of patient education. I have used models and audiovisual representations of our oral surgery procedures for many years. Nothing has had as profound or dramatic an effect as when I bring up a 3-D image of the patient to demonstrate their anatomy and show them their treatment options. I show them exactly where the implants will be placed, and show them various anatomical landmarks, such as nerves and sinuses, and how we will avoid problems with those areas. The patients have a greater understanding of their situation and the proposed treatment for it, and this increases case acceptance.
Dr. P: As a GP, cone beam has opened my eyes to all aspects of surgical treatment. The fact of the matter is that it took the majority of dentists a long time to learn to read 2-D X-Ray images, and we were working from those 2-D images to show patients pathology and propose treatment plans. We all have to admit that some patients do not easily see what we see in a 2-D X-ray film or image. How could they? With cone beam, we are able to show more realistic and specific 3-D images. When we show them an area in need of dental treatment, patients can see it clearly. It’s almost tactile, and when a patient sees an image or a model of his or her own skull, it brings it all home. When we look at a cone beam image, the patients see exactly the same thing we are seeing. It’s no longer a case of asking them if they see what we see, it’s a case [where] both of us [see] the same image at the same time. It provides clarity for both the dentist and the patient, and it takes much less time to explain the treatment proposal.
Do you use cone beam with all patients, or just for the complex cases?
Dr. P: For me, it ’s my primary diagnostic tool. I generally scan all of my patients except for pediatric patients. I am able to diagnose the health of every single tooth in the mouth, and I can isolate problems quickly. I honestly couldn’t work without cone beam anymore. With incidental findings as high as 25%, I find myself justifying CBCT scans as a routine diagnostic procedure. If I have any questions, I readily refer my scans for review by an Oral Maxillofacial Radiologist, and I follow their guidelines for limiting unnecessary radiation exposure.
Dr. R: I don’t know how I lived without cone beam either. Cone beam has revolutionized how we look at (and through) our patients. You can see more in 3-D than you could possibly imagine in 2-D. Although I don’t scan everyone, if there is any question of larger problems, then a scan is almost mandatory. Cone beam CT imaging is essential for [the] evaluation of patients with impacted teeth to [learn] exactly where the teeth are located. During surgery, I know what to expect; it makes it so much easier, and it helps save time. You see things that you never saw or appreciated before.
How is the current economic climate affecting your business? Have you made any changes to the way you are practicing?
Dr. P: I haven’t changed anything major to try to adapt to this economic climate. In compromising, you may find that you offer something less than the best. Patients know when this occurs and [they] are very astute. What I am finding is that no matter the economic conditions, patients are more inclined to go for the quicker outcome. For those patients who understand the intricacies of implant dentistry, or any interdisciplinary treatment, I am finding the length of treatment time does affect the treatment they choose. Fortunately, CBCT

Technology
38. Issue 4 2009 CATALYST MAGAZINE
imaging allows us to achieve more predictable results in less time!
Dr. R: I think [that] in this economy, I’m happy to be taking on any cases, whether they are complex or simple. The number of my patient referrals has def ini tely been affected. Patients are putting off whatever they can until they are more [confident about] what the future holds. I have had patients that do not move forward with treatment because of their financial situation, and others who I saw two years ago surprise me by calling to say they are ready start. I think patients in general, in any economic climate, are always trying to be as cost efficient as possible. If it’s possible, they would always prefer that I treat them without bone grafting and a prolonged treatment time. Sometimes, though, it’s not possible, so we work to offer the patients the best treatment options at a fair cost.
How do you justify the financial commitment to purchase the 3-D imaging unit in your practice?
Dr. R: I’m often asked if it’s worth spending almost $200,000 on a piece of equipment when, in the present economic climate, doctors are wondering if they will have patients in their chair next week. Looking at cone beam CT as just another piece of equipment is not the right way to look at it. The cost of the machine—my monthly payment—is really insignificant when c ompared to what we can do with the technology. The money is more than covered by the increase in productivity and patient acceptance. Patients come to us because of the technology we incorporate, and how well we use it to provide them with better care. It has to be seen as a way of elevating the level of service you provide and setting yourself apart from the others. Having the treatment information that cone beam gives you, puts you in a better situation
to treat your patients much less invasively and more efficiently.
Dr. P: I’m a GP, and I am like all the other GPs. We are all concerned about the f inancial impact of owning a cone beam scanner. I learned very quickly that the business of cone beam is not in charging for scans. It’s for the quality of service it helps me provide to my patients. With cone beam, I’ve seen a direct increase in patient case acceptance. I’m not concerned about whether the patient will do it; inevitably, the patients appreciate it, and they are prepared to come back for that service. Everyone’s thinking about cone beam—they’re all questioning the cost— but that is sue wi l l become smaller and smaller as more companies improve it, and the standard of care increases. There will come a day when cone beam will be readily available for all patients. It’s all about being a better dentist.
Why is the uptake and integration of cone beam technology slow in some practices?
Dr. P: I think it’s because they’re not educated regarding all of its potential uses. Some articles on the subject have merit and others don’t. Cone beam is so new that doctors, such as Dr. Reznick and I, feel that it is very important [to] help our colleagues … understand the various uses of cone beam imaging, and how it is applied in our practices every single day. Although integrating a unit into your practice can be challenging, the rewards are great, and I don’t think anyone ever looks backward to working only in two dimensions.
Dr. R: I agree with everything Dr. Patel said. There are a number of factors, and the major one is simply a lack of understanding. There are some doctors who really embrace technology and others who shy away. Some think
of it as only a tool for treatment planning implants, as opposed to a tool to aid in everything from patient education to full-scope treatment planning. The negative experience has generally come from implant planning software that utilized images from a medical CT scan. The doctors that have used medical CT have experienced implant treatment planning as labor intensive, and having a steep learning curve. Speaking from experience, obtaining the scan and getting the images into our computers was frequently an obstacle for us and our patients. We had to refer the patient out to an imag ing center, which may take up to a week to get an appointment. They would charge them a minimum of $350 for a scan. We would then have to get the study back on a CD, send it out to convert it to a proprietary format—which might take a few more days—and then we’d have to load that onto our computers to start to treatment plan. So you can see that it was a very cumbersome way of doing things. It was a very long, involved process that might even get more involved and costly if the scan was taken incorrectly by the hospital technician. This is the sort of experience many dentists have had with CT scanning and implant planning in general, so they think of cone beam as really only something to utilize with the more complicated implant cases. They don’t realize all the other ways that specialists, such as me, and general dentists, such as Dr. Patel, can integrate this technology into our practices on a daily basis to enhance the level of patient care we provide. One of the things Dr. Patel and I have benefited from is that the system we use has very intuitive software. It makes the whole process extremely efficient. Within 30 seconds of the scan coming up on the screen, we can already begin to treatment plan, and we can do this with the patient chairside. This is very powerful.

Technology
CATALYST MAGAZINE Issue 4 2009 39.
Q
Q
Dr. P: I was fortunate enough to be a consultant before opening my private practice. I was hired by specialists to help them integrate cone beam into their practices. I have had extensive experience with many of the machines available in the USA. Of all the equipment you can buy, integrating a cone beam system into your practice is one of the most challenging, but the payoff is extremely high.
The company we purchased our CBCT unit from designed a solution with the doctor, assistant, and the patient in mind. The designers thought about how their technology can be integrated clinically with maximum efficiency. What would take other CBCT units hours to achieve in diagnostic and treatment planning, is done in five minutes in my practice.
How does it affect your case acceptance rates?
Dr. P: Across the US, we have around a 50 -70% t reatment ac c ep t anc e r a te in gener a l dentistry. In terms of my case acceptance rate, and I attribute this figure to the integration of cone beam into my practice; I went from around 60% to 90%. I think it’s because: 1) Patients see exactly what their needs are. 2) The intuitive software tools allow us to measure and increase accuracy. 3) We can show patients the steps we will take and their options for treatment. 4) Our patients value our technology and the way we use it to provide better care. Some patients seek second and third opinions, but if the other dentist doesn’t have the technology and capabilities that I do, the patient invariably comes back.
Dr. R: I see a lot of patients for second and third opinions, and much of the time, patients choose to go with me. Maybe not only for me, but for the technology I employ in their treatment for their benefit. Patients are generally very sophisticated with regards to the
use of the Internet, so they often go “doctor shopping” because they want the best. I used to work with a partner who didn’t want to use cone beam the same way I did. From my former partner’s point of view computer guided implant treatment was an unnecessary added expense, but to the patients, i t was about having the best treatment—and the technology reflected that. It is a testament to my philosophy to provide the best care I can to my patients.
What would you l ike to see developed in the future?
Dr. R: We know a little of what’s coming down the road, and it is very exciting. One day, we will be able to do all our treatment planning in virtual reality and show patients their treatment options at each step along the way. Comprehensive 3-D digital dentistry is coming soon. We will be able to treatment plan for implants using digital impressions, digital wax-ups, and then create surgical guides off of these images. We can only imagine what is possible in the future using this incredible technology; many applications are yet to be invented, as their genesis will be in future innovations.
Dr. P: I think as dentists, we always dream to be able to comprehensively and completely treatment plan in 3-D. Imagine how in a short period of time we’ll be able to scan a patient and superimpose periodontal charting, endodontic treatment, restorative treatment, (veneers, crowns, bridges, etc.) and superimpose those onto a 3-D view of the patient’s skull. Imagine not ever having to take an impression … again—endless possibilities!
Dr. R: When we think about the future, we get really excited. 3-D digital dentistry and the associated information is easily portable and transferable between practitioners, so real-time collaboration across town or across the world will
become commonplace. Digital information can also be stored in much less space, and more easily retrieved than stone models and film radiographs. Technologies that are just in their infancy today will become the standard of care for dentistry in the future.
Jay B. Reznick, DMD, MD is a Diplomate of the American Board of Oral and Maxillofacial Surgery. He received his Dental degree from Tufts University, and his M.D. degree from the University of Southern California. He trained in Oral and Maxillofacial Surgery at LA County-USC Medical Center. His special clinical interests are in the areas of facial trauma, jaw and oral pathology, dental implantology, sleep disorder medicine, laser surgery, and jaw deformities. He also has expertise in the integration of digital photography, 3-D imaging, and CT-guided implant surgery in clinical practice.
He frequently lectures at continuing education meetings and has published articles in JADA, Journal of the California Dental Association, Oral Surgery-Oral Medicine-Oral Pathology, Compendium of Continuing Education in Dentistry, DentalTown Magazine, CE Digest, and Gastroenterology. Dr. Reznick is one of the Founders of the Web site OnlineOralSurgery.com, which educates practicing dentists in basic and advanced oral surgery techniques. He is the Director of the Southern California Center for Oral and Facial Surgery (www.sccofs.com) in Tarzana, California, and a consultant for many dental and surgical manufacturers. He can be reached at [email protected].
Neal S. Patel, DDS Dr. Patel is a General Dentist with Implant Prosthodontic Training from The Ohio State University, and he received a degree in Molecular Genetics from OSU as well. He maintains a private practice in Powell, Ohio, where he applies his special clinical interests in the areas of cosmetics, dental implantology, CAD/CAM dentistry, laser surgery, and complex reconstructions. He also has expertise in the integration of complete digital dentistry, 3-D imaging, dental materials, and CT-guided implant prosthetics.
He lectures frequently at continuing education meetings, and has published numerous clinical articles on advanced treatment techniques and procedures. He is a consultant for a number of dental manufacturers and works closely with R&D for product development and enhancement. He can be reached at [email protected].


Technology
CATALYST MAGAZINE Issue 4 2009 41.
Multispectral Optical Examination of Oral Lesions in High-Risk PopulationsBy Mark Nichols, DDS, Vice President of Clinical Affairs, Bering Omega Dental Clinic
Since 1987, the Bering Omega Dental Clinic in Houston, Texas, has been providing
compassionate health care and social services to people living with HIV/AIDS. The dental clinic is the only free and full service HIV/AIDS dedicated dental clinic in Texas, serving more than 2,000 individuals and accommodating over 15,000 patient visits annually. Our clinic serves approximately one in three HIV-positive people in the Houston/Harris county area.
Caring for a high volume of patients whose immune systems have been compromised places extraordinary demands on my clinical staf f, and as Vice President of Clinical Affairs, on me as well. We need clinical tools that are effective and efficient in identifying and diagnosing abnormalities in the oral cavity, especially those that could be precursors to oral cancer. Since mid-June of this year, I have been using the Trimira Identafi™ 3000 handheld multispectral device for examination of patients in my regular practice. As many as 5% of our patient population presents with HPV lesions, and a significant number of them are FEH (focal epithelial hyperplasia, HPV types 13 and 32), also known as Heck’s disease. Since I have used the unit in my practice, I have found it to be especially useful for examination of patients with disseminated disease, such as HPV. The convenient device helps me identify suspicious oral lesions and, if necessary, select a site for biopsy.
In preparation for an indentafi™ 3000 exam, a protective disposable cover is placed over the distal half of the device. This is meant to prevent cross-contamination between
patients and … shorten the down time between examinations that would be needed to sterilize an unprotected device completely. Identafi 3000 disposable covers in the form of dental #4 mirrors are commercially available at this time. We are also evaluating protective covers without mirrors at the Bering Omega Dental Clinic. Trimira expects to add these to its product line. After snapping the disposable cover in place, the provider puts on special filtering goggles. These allow unobstructed white and green-amber light examination with the identaf i 3000, while blocking the violet light that is used to excite autofluorescence. The final preparatory step is to dim the room lights to minimize their impact on the visualization of autofluorescence.
The identafi 3000 exam consists of visual evaluation of the oral cavity under the three different lighting conditions provided by the instrument. The first is a white-light evaluation. This view of the oral cavity provides information similar to that gained with a regular dental chair lamp. Often, the ability to place the light source inside the oral cavity will provide better illumination of areas that may be obscured by shadows, such as the areas of the tonsils and [the] base of the tongue.
The second view is with a violet-spectrum light, around 405 nm, which causes autofluorescence in certain tissue types, and is easily visible under the dimmed room light conditions in which the exam is performed. The size and shape of the device make it convenient for examination of the entire oral cavity, including the tongue,
buccal mucosa, gingival, hard and soft palate, and the floor of the mouth. Having identified a region of interest or an abnormality, I use the degree of loss of fluorescence to pick out biopsy sites that may be required. That is, I have biopsied the area that looks darkest in the region of interest (largest loss of fluorescence). The third view of the oral cavity, using green-amber illumination, allows fine visualization of vasculature at and near the tissue surface. To date, I have found the violet autofluorescence view to provide the most additional information to my regular examination.
A Hispanic adult male in his forties presented recently at the Bering Omega clinic with generalized HPV lesions on the labial and buccal mucosa. The lesions were sessile, slightly elevated, and stippled with normal color. Lesions were asymptomatic, but were beginning to increase in size and become of cosmetic and functional concern due to biting. In addition to a conventional oral exam, the patient was evaluated with a Tr imira identafi 3000.
Whi te l ight showed papule s characterist ic of FEH (Figure 1 - page 42). I lluminating the affected area with the identafi 3000 violet light caused the labial epithelium to appear bright blue, showing darker, red-tinted areas corresponding to the location of HPV lesions (Figure 2 - page 42). The green-amber image showing the vasculature present in the field of interest was also acquired (Figure 3 - page 42). For patients who show suspicious lesions under white-light examination but no loss of fluorescence, I have chosen a
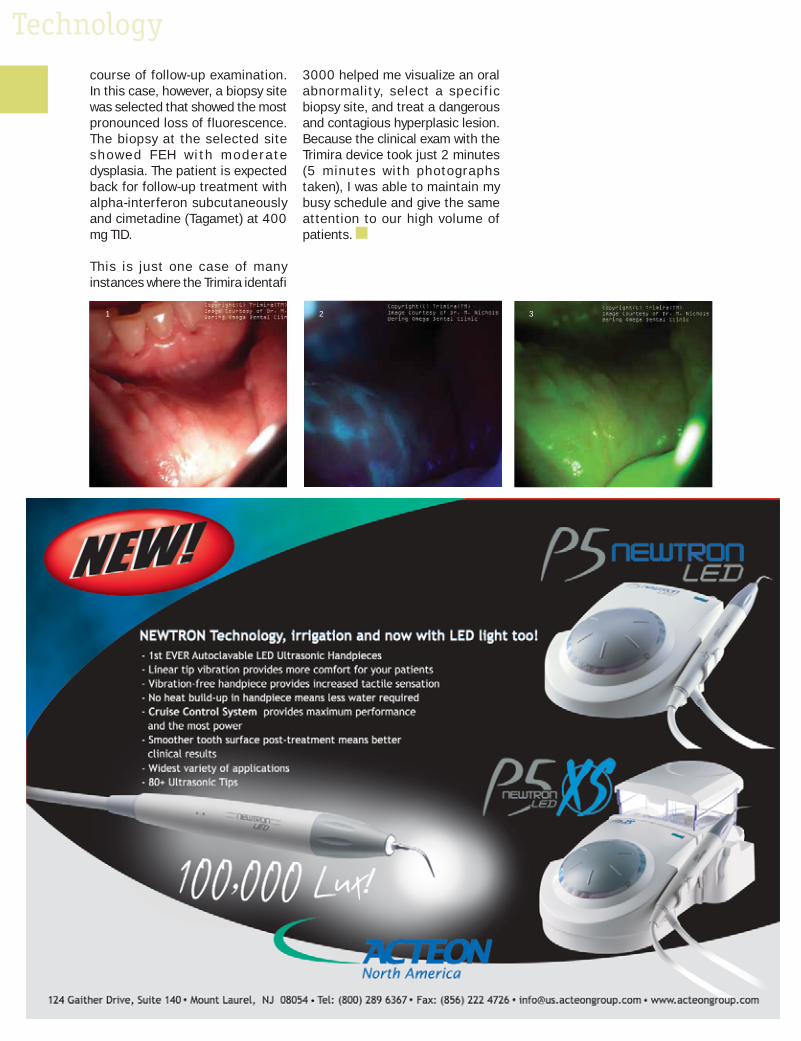
Technologycourse of follow-up examination. In this case, however, a biopsy site was selected that showed the most pronounced loss of fluorescence. The biopsy at the selected site showe d FEH w i th mo der a te dysplasia. The patient is expected back for follow-up treatment with alpha-interferon subcutaneously and cimetadine (Tagamet) at 400 mg TID.
This is just one case of many instances where the Trimira identafi
3000 helped me visualize an oral abnormality, select a specif ic biopsy site, and treat a dangerous and contagious hyperplasic lesion. Because the clinical exam with the Trimira device took just 2 minutes (5 minutes with photographs taken), I was able to maintain my busy schedule and give the same attention to our high volume of patients.
1 2 3
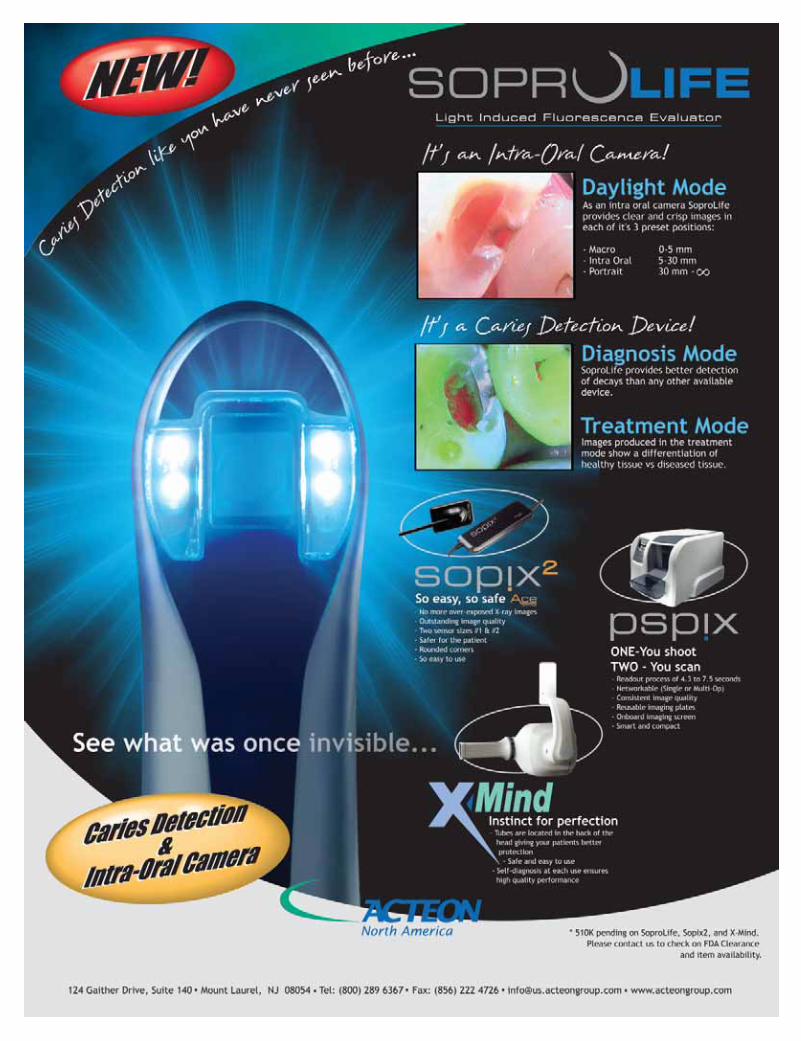

Technology
44. Issue 4 2009 CATALYST MAGAZINE
What is What is 64-Bit?64-Bit?By Dawn Christodoulou, President, PEB/XLDent
We are just over a year away from the close of the first decade in the 21st
century. It seems like yesterday that I was writing articles about Y2K and preparing our user base for this big, potentially cataclysmic event in the modern digital world. And now, just 10 years later, I’m writing another article on a significant transition in the unstoppable evolution of computing progress. This time, however, the article’s focus is not so much about an event that could threaten our digital infrastructure, b u t r a t h e r a b o u t a 6 4 - b i t evolutionary transition that will inevitably bring about progressive change.
Since the year 2000, I’ve cycled through 4 laptops, 3 computer operating systems (OS), and 6 mobile phones. I ’ve seen our children grow from toddlers to teenagers, and I’m less than a year away from another “please don’t remind me how old I am” birthday. According to our youngest son, my quick adaptation to new technology makes me young and hip. However, my inability to improve upon my PlayStation scores, and the fact that I still don’t have my Wall set up on Facebook, makes me ancient…not just old, ancient. It seems that my age really becomes apparent when I pick up a gaming controller. I don’t feel that old, but in terms of technology life cycles, his concept of ancient is quite correct. When Microsoft releases Windows 7 this October, I plan to go computer shopping again because the laptop I currently own is ancient. I’ve got my eye on a J3400 Motion Tablet PC with 4GB of memor y, hot swappable batteries and of course, a 64-bit native Windows 7 OS. I’d
get more memory, but for now that’s the limit on the J3400.
If you’ve gone computer shopping lately, you’ve probably noticed more advertisements touting 64-bit architecture with 64-bit operating systems. If you’re not sure what this means, simply put, a 64-bit native PC can handle larger amounts of information than a 32-bit system. Since it can use more RAM—4GB and up—a 64-bit computer will be more responsive when you’re running lots of programs at once or running applications that take advantage of the hardware’s full performance potential. When we entered the 21st century, it was a 32-bit world. Configuring your computer with 512MB of RAM was considered overkill, and the notion of ever reaching the 4GB resource limit was unthinkable. Then, we were in 32-bit childhood; now, we are now in 32-bit maturity, and just as 16-bit programs died, so will 32-bit programs or they will migrate to the 64-bit world.
Sixty-four bit computer architecture is not something new. In fact, it’s been commonplace for many years. It’s only recently that OEMs started shipping with 64-bit native Vista and this trend will continue with the release of Windows 7 in October. We are witnessing the start of yet another cycle that heralds the birth of every new computing generation. These cycles move the market on to the next technological plane, stimulate the need for upgrades, and feed our addiction for more computing power and speed. It happened with every major platform improvement since 8088 processors and DOS. Unfortunately, our industry, the dental industry, is slow to adapt to new standards, and this will likely be the case with Windows 7 64 as well.
Tw o e l e m e n t s i n t h e n e x t generation will factor into whether you can order your next computer with a 64-bit OS. The first is device
drivers, and the second is 64-bit deployable practice management applications. Device drivers are the programs that run the hardware that connects to your computer, such as printers, USB card swipers, scanners, digital X-ray sensors, and intraoral cameras. Notably, it’s not the printers or document scanners you need to worry about, as 64-bit drivers for these pieces of equipment have been out for some time. Instead, at least for the short term, it’s the digital sensors and panoramic units that will hold you back. At the writing of this article, 64-bit drivers were not yet available for dig i tal dental equipment, and in my research, only a few manufacturers identified that they were working on them. So it may be another year or two before you can order your operatory computers with a 64-bit OS load.
The second element that factors into the 64-bit equation is the application software. This is where it gets confusing, and this is where the software manufacturers that are not positioned to deploy 64-bit applications will either downplay the advantages of this new generation or work their advertising campaigns to confound your understanding of what a true 64-bit computing environment means. Most of the programs designed for a computer running a 32-bit version of Windows will work on one running a 64-bit version of Windows. This, of course, assumes that the software vendor has qualified its program and will support it in this environment. However, as we move further into the next decade, there will be no stopping the 64-bit evolution, and advanced applications software will become a desired necessity.
What does all of this mean to you? It means that you need to choose your technology solutions wisely.
At last, smooth contouring and precision handlingin a high-speed compact.
Featuring patented, micro-motor technology, KaVo has once again revolutionalized dental
handpieces. COMFORTdrive® features optimal cutting performance in a lighter, shorter and
quieter design making it the most innovative high-speed ever.
Test drive the new COMFORTdrive® today and embrace performance.Contact your local Burkhart sales consultant at 1-800-562-8176 today!
www.kavocomfortdrive.com
Business of Dentistry
The Slight Edge to Success
46. Issue 4 2009 CATALYST MAGAZINE
By Bob Creamer, CPA
Our sluggish economy has impacted businesses to the point where many have shut
their doors; even whole industries no longer exist . Yet dentistr y appears to be an industry which is much more resistant to the perils of a big recession. However, this resilience does not come without effort and investment. Dentists and their teams are creative and diligent in their efforts to maintain their production and achieve practice goals. But what makes one practice more successful than another? Why does one practice struggle to fill the schedule, while another practice is having its best year ever?
As our firm completes mid-year p lanning meet ing s w i th our c l ients , we are proud of the accomplishments and financial success they are experiencing. This success is evident despite the fact that the ADA is reporting the average practice is down during this current recession. Our clients are no different than any other practice in that the economy has affected all of them. Patients are cancelling appointments, and treatment plan acceptance is down in almost every office. Yet most of our practices have been able to work through these difficult times, reporting numbers comparable to, if not better than in any previous year. Each is finding success in various ways, but what makes them successful is the fact that they are applying the Slight Edge Principle.
The Slight Edge Principle is the
concept in which a prac t ice implements the things that will give it a competitive advantage. Generally, this is not one big thing; rather, it is a collection of small things, which applied consistently, result in a positive impact on the practice. When combining multiple slight edge principles, they snowball into a competitive advantage over all other practices in the community.
I will share with you 10 Slight Edge Principles I have seen utilized in our most successful practices, many of which are having their best year ever.
1. Dynamic and Positive Leader: All great teams have a great leader. As the dentist, you are that leader. Your dental team will inevitably become a reflection of you and your attitude. It’s up to you to establish the expectations and positive steps that will be taken to achieve the goals of your practice. You can never afford to have a bad day. If you come to work late or with a sour attitude, you run the risk of tainting the entire day. You give the rest of the team an excuse to complain about what is ailing them and why today is going to be a hard day.
While it is okay to acknowledge that our economy has presented you with some difficult challenges, you must demonstrate the leadership and p o s i t i ve d i re c t ion your practice will take to overcome any difficulties that arise. You and your team need to become doers and accomplishers, rather than victims with all the excuses necessary
to fail. When I talk with a dentist whose practice is struggling, I am not surprised that his or her attitude is often negative, and the excuses are those of a victim. On the other hand, in our best practices, the dentists are always optimistic, as they seek oppor tunities to improve and overcome. Attitudes are contagious. I f ever yone’s attitude is focused positively on accomplishing the goals, half the battle is already won.
2 . Te a m C o m m u n i c a t i o n : Communication within the dental team is vital if a practice is to maintain or increase prof i ts . Communications starts with the morning huddle. Morning huddles are when expectations and daily goals are discussed. Schedules are outlined, along with the duties of each team member. The whole team needs to anticipate and prepare for any problems that may arise. When the whole team is focused on working together, i t s members are much more likely to achieve the daily goals and maintain an enjoyable work environment.
I t i s also impor tant to have addit ional weekly or monthly meetings to discuss larger goals or issues facing the practice. In these meetings, ideas can be shared and plans developed to attack the things that are keeping the practice from achieving its goals. The doctor is the leader, but of ten, those doing the job are best suited to discover and solve the issues that exist within certain areas of the

Business of Dentistry
CATALYST MAGAZINE Issue 4 2009 47.
practice. Team members should be challenged to accept responsibility for solving these issues without being told. When we acknowledge issues within our own circle of control and endeavor to find the solution, it becomes a personal challenge, and therefore much more gratifying once achieved.
3. Controlling Expenses: During a monthly meeting, one of my clients addressed the issue of profitability with her team. Although they were maintaining collections, their expenses had increased and profitability was suffering. She challenged her team to come up with ideas that could decrease expenses without compromising the quality of care.
The front desk manager suggested that they change the brand of bottled water they offer to patients from an expensive boutique brand to a quality store brand. This cut their costs by more than 50%, yet it did not impact the patients’ experience adversely.
They also stopped their office plant maintenance contract. They now water and care for the office plants themselves. The dentist said this cost savings actually turned out to be enjoyable, as they learned who had the best “green thumb.” The team has bonded with the office décor, and they now appreciate sincerely the many favorable comments they receive from patients.
Although reducing the cost of bot t led water and car ing for their own plants won’t cover the building rent, it did strengthen the working relationship between team members and has raised their level of consciousness regarding cutting costs. The overall financial result of these and other cost-saving steps was enough to stabilize profits in a practice that was simply maintaining collections.
4. Facility Upgrades: In a similar team meeting at another practice, a hygienist suggested that rather than simply cut expenses, the practice actually needed to spend
money on improving the facility. Based on that idea, they repainted the inside of the office and replaced some floor coverings. The doctor also invested in some additional décor changes to enhance the aesthetic image of the practice. Now, the doctor and team feel like they are walking into a whole new office. Better yet, they believe the facility corresponds better to the high quality care they provide.
The impac t on pat ient s has been posi t ive, as they have acknowledged the change and compl imented the improved appearance of the practice. The doctor has even received additional pat ient referrals from happy patients who tell their friends and family about the wonderful facility. Their standard of care has always been high, yet patient comments and the ensuing referrals indicate that patients believe the quality of care has improved somehow. Right or wrong, many patients judge a practice on almost everything e x c e p t t h e q u a l i t y o f y o u r
POWERFUL TAX & BUSINESS SOLUTIONS FOR THE DENTAL COMMUNITY
SINCE 1977
We know the dental business and the issues you face.
Our services are industry driven and client specific.
[email protected](800) 248-1120
Phone: 503-585-1040Fax: 503-371-1640
Currently Accepting Clients in:OREGON, WASHINGTON, ALASKA, NEVADA, IDAHO, UTAH & MONTANA
Our member firms represent dentists in all
50 states!
The Academy of Dental CPAs (ADCPA) is a national association of accounting firms which specialize in delivering creative solutions that meet the unique
needs of the dental profession.
www.ADCPA.org
Business of Dentistry
48. Issue 4 2009 CATALYST MAGAZINE
restorations. The key is to provide optimal care, while appealing to what patients believe makes you better than your competition.
5. Marketing: While some practices have been cutting their marketing budgets in response to decreased collections, it is our best practices that have increased their marketing. Marketing can take many forms, with some options being more expensive than others. The previous example of investing in the image of the practice facility was fairly expensive, but the patient referrals and positive effects were numerous.
I t is commonly accepted that the best form of marketing is internal marketing. However, in our current recession, it is more impor tant than ever to focus some effort on external or direct marketing as well. Most practices are experiencing cancellations in their hygiene department and have found their patients’ purse strings have tightened. Patients are less likely to accept current treatment plans, or at least are more likely to delay or extend treatment. There has never been a greater need to grow the practice and expand the hygiene department by acquiring new patients.
I f pat ients are less l ikely to accept comprehensive care, the practice must do more diagnostic, preventive, and hygiene treatments to maintain similar figures. In many of our most successful practices, not only was hygiene maintaining production through new patient visits, but they actually added days of hygiene or even hired additional hygienists. In these situations, most of the growth in the practice resul ted from the expansion
in hygiene rather than through the complet ion of addi t ional comprehensive treatment. I expect even greater growth from these practices in the future. As our economy improves, these practices will be prepared to complete the treatment that the members of their newly enlarged patient base have delayed.
6. Patient Messaging Software: It requires a lot of team time and effort to make personal calls to confirm patient appointments. Even more time is spent with reminder calls advising that the appointment is within 48 or 24 hours. The majority of those phone calls end with messages being left on patients’ answering machines. Notably, those messages are notorious for getting lost or being missed.
Many dental offices are turning to automated e-mails and text messaging software to reduce team t ime and increase the effectiveness of patient contacts. According to recent surveys, 80% of mobile phone owners use text messaging. While text messaging is used more widely by individuals aged 13 to 22, use by older adults is rapidly increasing.
One of my 41-year-old dentists told me that she uses text messaging every day to stay in touch with family and friends. She introduced a text messaging software/service into her office a year ago. Patients are texted to remind them within 48 hours of their scheduled appointment . The pat ient i s reminded again at 24 hours. One hour prior to the appointment, the patient is sent an additional message to drive safely and to let them know the doctor and team
are looking forward to their visit. Patients also get birthday greetings and best wishes for selected holidays. They have also begun utilizing the texting software in their reactivation of patients. The doctor says that the feedback from her patients is generally very positive. The patient messaging service she utilizes was referred to her by our office; however, a number of these types of services exist. Her monthly fee is minimal, especially when considering the convenience and the fact that the team now has more time to concentrate on taking care of patients once they are in the office.
7. Patient Education: I have already acknowledged that treatment plan acceptance logically declines as a consequence of our economy. However, I have spoken to a number of practices that are still growing and attribute their growth to combating this trend successfully. The key to their success is patient education. They are taking the time necessary to make sure that patients truly understand the severity of their oral needs and the various treatment options. They are also explaining the benefits of each option, as well as the possible consequences of delaying treatment. Patients are better educated, as the doctor and team try harder to include patients in the decision-making process.
When asked why they did not do this previously, all said that they did, but acknowledged quickly that it was not to the extent of their current commitment to the process. They have found that the extra time they now spend with patients is being rewarded with greater patient acceptance and
“Patients will find a way to pay for things they value, and the key to getting good case acceptance is helping the patient identify and understand that value.”
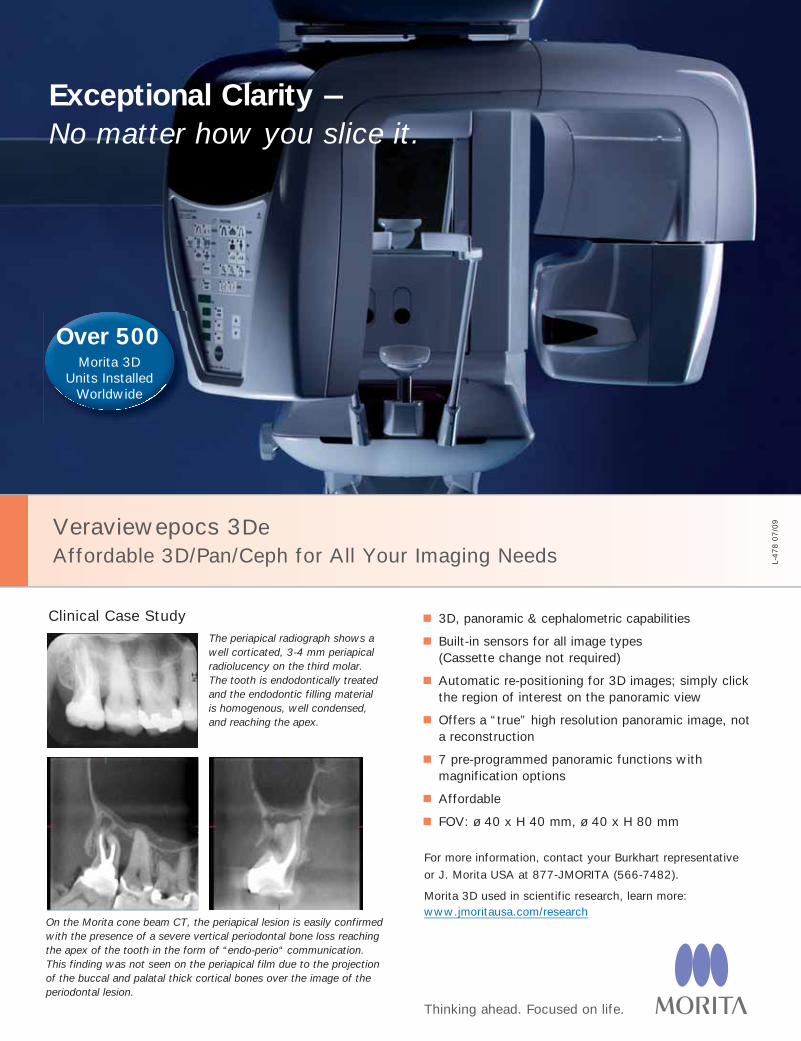
Veraviewepocs 3De Affordable 3D/Pan/Ceph for All Your Imaging Needs
3D, panoramic & cephalometric capabilities
Built-in sensors for all image types(Cassette change not required)
Automatic re-positioning for 3D images; simply click the region of interest on the panoramic view
Offers a “true” high resolution panoramic image, not a reconstruction
7 pre-programmed panoramic functions with magnification options
Affordable
FOV: ø 40 x H 40 mm, ø 40 x H 80 mm
Thinking ahead. Focused on life.
For more information, contact your Burkhart representative
or J. Morita USA at 877-JMORITA (566-7482).
Morita 3D used in scientific research, learn more: www.jmoritausa.com/research
L-478 0
7/0
9
Exceptional Clarity –No matter how you slice it.
On the Morita cone beam CT, the periapical lesion is easily confirmed with the presence of a severe vertical periodontal bone loss reaching the apex of the tooth in the form of “endo-perio“ communication. This finding was not seen on the periapical film due to the projection of the buccal and palatal thick cortical bones over the image of the periodontal lesion.
Over 500Morita 3D
Units Installed Worldwide
The periapical radiograph shows a well corticated, 3-4 mm periapical radiolucency on the third molar. The tooth is endodontically treated and the endodontic filling material is homogenous, well condensed, and reaching the apex.
Clinical Case Study

Business of Dentistry
50. Issue 4 2009 CATALYST MAGAZINE
B o b C r e a m e r i s a CPA and President of Creamer & Associates, P C , a n a c c o u n t i n g f irm. For the past 30 ye ar s , h i s f i r m ha s emphasized f inancial and retirement planning, d e n t a l t r a n s i t i o n s , practice enhancement,
wealth creation, tax savings and related accounting and consulting services for maintaining an efficient and profitable dental practice. He is also a member in the financial advising and investment company of Salem Asset Management, LLC. He is a founding member of the Academy of Dental CPA’s (www.adcpa.org).
Bob can be reached at: 800-248-1120 or [email protected]
a stronger relationship of trust. Patients have even complimented them on the difference. Some went as far as to say that in the past—and in previous practices—they had delayed or declined treatment because they didn’t understand completely either the need or the benefit. Patients will find a way to pay for things they value, and the key to getting good case acceptance is helping the patient identify and understand that value.
8. Technology: As I have pointed out in previous Catalyst articles, our surveys have once again confirmed that those practices which are up-to-date in technology and equipment continue to be among our most successful and profitable practices. Technology represents their slight edge advantage. It allows them to deliver the highest standard of care efficiently and effectively.
Digital radiography and intraoral cameras are excellent examples of technology that benefit doctor,
team, and patient. The increased ef f iciencies and an improved quality of life for the doctor and the team are obvious; however, the real enhancement lies with the patient. When used as part of the education process, patients can visualize their dental needs clearly on the monitor in the operatory or consultation room. The technology enhances their understanding and improves treatment acceptance dramatically. I have already said that patients will pay for what they value. I would take that a step further and say they value what they can see. Technology is the slight edge needed to improve patient acceptance.
9. Charge the Appropriate Fee: One of the best things you can do to maintain your practice during a recession is to balance and set your fees properly. Doctors need to maintain a market-relevant and balanced fee schedule, through which they pass along increased expenses to the patient. The worst thing a doctor can do is lower fees, thinking that it will somehow improve our economy and increase treatment acceptance—the approach simply does not work. In fact, I have often seen practices that have suffered greatly as a result of a poorly managed fee schedule. Practices should seek the assistance of a fee-setting professional. A properly established fee schedule can be the slight edge advantage the doctor needs to be fair to both the patient and the practice.
10. Follow-up Calls: One of the simplest, yet most effective slight edge principles a dentist and team can apply is to place follow-up calls to their patients consistently. During these post-visit calls, you should thank them for coming in and check on how they are recovering. Also, take the oppor tunity to reassure them of the quality of the restoration and the fact that you were very pleased with how well it turned out. If a doctor consistently
places just two follow-up calls each evening to patients treated that day, and if they see patients just 180 days per year, that’s 1,800 additional patient contacts in just 5 years. That is enough calls to make an additional positive impression on most of the active patients in a typical practice. Think about the additional goodwill gained if the hygienist also placed just two follow-up calls per day. It is a small, yet very powerful tool that can be used to gain a significant advantage over the competition. Sure, most practitioners occasionally place a random call, but it is the consistency and dedication to the calls that will endear you to your patients. It really costs you nothing other than your sincerity and your time.
Some Slight Edge Principles only require the dedicated expenditure of time over an extended period while others require a onetime financial expenditure to upgrade a facility or invest in equipment. Successfully applying the correct principle to your practice will yield big rewards. After all, it is just good business.
Investments in digital radiography like the new Instrumentraium Snapshot sensor can give dentists an edge that patients and staff alike can appreciate.
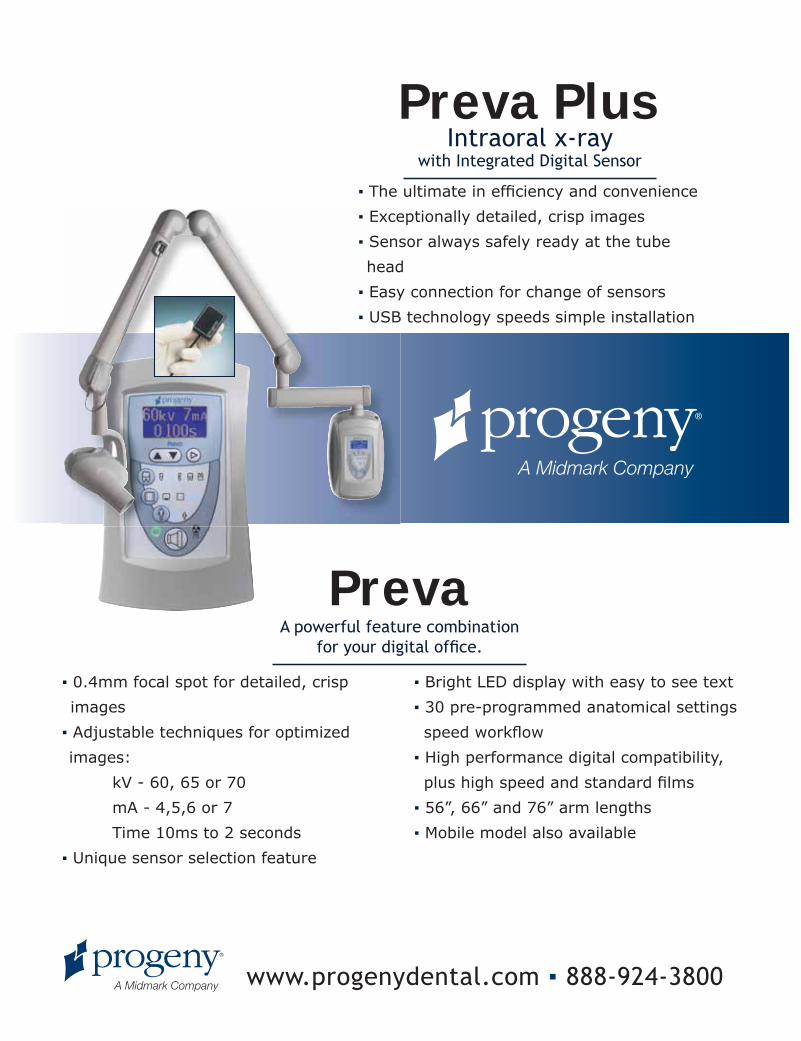
Intraoral x-raywith Integrated Digital Sensor
▪ The ultimate in efficiency and convenience
▪ Exceptionally detailed, crisp images
▪ Sensor always safely ready at the tube
head
▪ Easy connection for change of sensors
▪ USB technology speeds simple installation
Preva Plus
A powerful feature combination for your digital office.
▪ 0.4mm focal spot for detailed, crisp
images
▪ Adjustable techniques for optimized
images:
kV - 60, 65 or 70
mA - 4,5,6 or 7
Time 10ms to 2 seconds
▪ Unique sensor selection feature
▪ Bright LED display with easy to see text
▪ 30 pre-programmed anatomical settings
speed workflow
▪ High performance digital compatibility,
plus high speed and standard films
▪ 56”, 66” and 76” arm lengths
▪ Mobile model also available
Preva
www.progenydental.com ▪ 888-924-3800

Wealth Management
52. Issue 4 2009 CATALYST MAGAZINE
Advanced Tax PlanningBy Sam Martin, MBA, CFP®, CPA
If you make it but have to send it to the government, did you really earn it? By the very nature
of how you earn your living as a professional, successful dentists will pay plenty of federal income and FICA as well as state income tax, if applicable. Consequently, you wi l l want to employ two disciplines designed to address this crucial element of practice and personal financial management. First, you’ll want to manage this substantial cash flow obligation, and secondly, you’ll want optimize your after-tax income, which is not always the same, while paying the least amount of tax possible.
Tax Management For a successful general dentist, federal taxes alone may make up 30-33% of total taxable income. Assuming direct practice overhead is 60%, federal taxes can easily represent 12-14% of practice receipts . For lower overhead specialists, federal tax could represent 18-20% of practice revenues. The point is, this is a major aspect of your overall practice, and personal cash flow and should be addressed in a formal manner.
The f i r s t s tep in proper t ax management is to project taxes at least a year in advance. In our office, we will begin putting together cash flow plans for 2010 starting mid-fall this year. This will take into account any expected changes in the practice, staffing, fees, and productivity increases or decreases. Once the basic cash flow plan is produced, the tax projection can follow.
With estimated practice operating cash flow, we can then make tax
adjustments for items such as depreciation and amortization, as well as back out the non-deductible principal payments of any loan payments. We then combine the estimated taxable income of the practice with the balance of the personal tax transactions, which may be as simple as itemized deductions (such as mortgage interest, taxes, or charitable donations) and/or involve portfolio investments, real estate activities, and in some cases, other business activities.
Once this “baseline” tax projection is in place, the tax payment plan can be constructed. For incorporated dentists and specialists, part or all of the coming year’s tax payments will be through salary withholding. Salary has the advantage of lending itself to nice, even, and automated payments over the course of the year. In some years, salary withholding is all that is required; in other years, however, there may be an expectation of additional taxes due – perhaps because of growth in the practice, or perhaps a decline in depreciation expense from fixed assets (equipment, etc.) purchased in previous years, and/or declining interest expense on loans. Your tax can jump suddenly, even if your “income” does not change much; therefore, projecting taxes in advance and planning accordingly is highly recommended. For unincorporated dentists, (quasi) quarterly estimated payments are the primary means of federal tax payment. Since these payments come every 2, 3, or 4 months (April, June, September and January), creating a semi-automated savings plan is very helpful. Start by opening a separate savings or money market account to accumulate tax savings. Determine if you are a disciplined monthly saver or like many of our clients, you may find putting a smaller amount into the tax savings account on a weekly basis easier to manage. If you make periodic lump sum payments to your retirement plan, you can
use this account and spreadsheet for this purpose as well. Since the estimated payment dates are not spread out equally, we recommend utilizing a spreadsheet that shows the required weekly savings going into the account and the year’s schedule of estimated payments coming out of the account. This helps make sure you will have an adequate balance at each payment date.
For incorporated or unincorporated dentists, utilizing a tax savings account prov ide s c ash f low discipline and allows you to earn a little interest on your money before sending it off to the government. In some cases, where it is known that a large amount of tax will be due next April, it may be beneficial to utilize higher returning certificates of deposit (CDs) timed to come due prior to the tax deadline. We recommend that you schedule these a few weeks prior to the due date on the odd chance that your institution is involved in an FDIC action that could delay access to funds.
Monitoring: Once the cash flow and tax savings/payment plan is in place, most of the hard work is done. The projection should be reviewed at mid-year and in mid to late fall, and be adjusted as necessary. This prepares you to take the appropriate year-end tax planning steps.
So far, we have talked about tax management, which is important, but far from exciting. But if tax management is drudgery, then proactive tax planning is excitement. We just want to ensure that we restrict our excitement within the boundaries of what the tax law allows—but in our favor, of course.
Shifting Pockets – Tax Qualified Retirement Plans The f i r s t s top along the tax planning process is to determine the most effective tax-advantaged

Wealth Management
CATALYST MAGAZINE Issue 4 2009 53.
retirement plan for you and your practice. It is important to note that the “best plan” will change over time due to changes in your age, the configuration of your practice, tax and pension law, and what you can afford to fund. This latter criterion, what you can afford to fund, is key in terms of the type of plan that is likely to be the best fit at this time.
Note: Selection of the most beneficial tax-advantaged retirement plan should be tied into your overall personal financial or wealth management plan rather than being evaluated exclusively on cost (staff participation) versus benefit (tax savings). The various funding vehicles you utilize, both tax advantaged and otherwise, should serve your comprehensive plan to optimize the likelihood that you will achieve your long-term goals. Although a major focus of the qualified retirement plan is optimizing your tax deduction, the plan is also an important employee benefit and therefore should not be overlooked.
Plan Types: A wide variety of plan types and features are available. Starting at the “low” end, there is the SIMPLE-IRA, the SEP, and the (grandfathered) SARSEP. In the middle, we have 401(k) plans, including the popular “Safe Harbor” 401(k) plan, which is often coupled with a profit-sharing plan. Finally, at the high end, we have Defined Benefit plans, which may allow much larger tax-deductible contributions.
SIMPLE plans may allow the doctor to fund as much as $23,000 per year, and adding a spouse to the plan could put doctor funding as high as $35,000, with maximum
staff costs of 3% (matching).
A Safe Harbor 401(k) plan could allow the doctor to fund as much as $26,000 (or $31,800 if aged 50 or older) at a maximum staff cost of 4% (matching). Adding a spouse (caution advised) could increase funding another $16,500 (or $22,000 if aged 50 or older). Utilizing a profit-sharing plan either in conjunction with a 401(k) or in the form of an age-weighted plan (or other similar options) could achieve maximum plan funding of as much as $49,000 (not including spouse). However, maximizing this funding is often accompanied by significantly increased staff funding.
A defined benefit plan could allow a dentist or specialist to fund $100,000 or more. These plans are quite complicated but can provide outstanding deductions for those who can and will fund at this level or higher.
The key point is that there are a great number of retirement plan types and features. In this regard,
your chief tasks are to ensure that (1) you are utilizing the plan and features that provide the best fit for your comprehensive financial plan; (2) that the cost benefit relationship of staff participation versus tax savings makes sense for your situation; and (3) that each year, you review your plan to make certain it is the best type and includes the features appropriate for the coming year(s).
Deduct What You Already Spend This categor y addresses the expenses that all of us incur in our lives, but which we may be able to qualify in part or whole for tax
deduction. This includes: A u t o m o b i l e s : T h e r e a r e a variety of ways to optimize your business related driving, and there are slightly different rules for incorporated dentists and specialists versus unincorporated doctors. The starting point is to capture all of your business driving in a log – either throughout the year or perhaps two months out of the year as a valid “sample.” Most dentists would be surprised at the amount of business miles they actually drive.
Some dentists, particularly those who have long commutes (generally not deductible), might benefit by taking the steps needed to qualify for a home office deduction. Done correctly, this could convert non-deductible driving into deductible business miles.
Fully understanding what are and are not business miles, and utilizing other household vehicles primarily for non-business driving, can result in a significant tax benefit.
Alternatively, deducting business driving at the standard mileage reimbursement rate is easy and can still provide some benefit.
M e a l s a n d E n t e r t a i n m e n t : By knowing these rules and the documentat ion required, dent is ts and special is ts can optimize their tax deductions. We understand generally that meals and entertainment are only 50% deductible; however, you might be surprised at the number of exceptions that exist.
Any time legitimate business is discussed (and documented)
“Right now would be a great time to sit down with your dental CPA and your Burkhart Equipment and Technology Managers to hash out the next 3 to 5 years of practice investment.”
Wealth Managementyou likely have a tax-deductible expenditure; for example, periodic quiet dinners with one’s spouse can be a very legitimate deduction if business (the future of your practice for example) is discussed and documented.
Travel: Here is an area where if you really know the rules, you can exploit them to maximize business deductions. Although much too complicated for this ar ticle, I believe that any dentist who likes to travel, or who travels frequently for the purpose of continuing education or similar endeavors might be surprised at how the rules can be made to work in your favor.
T he p ro c e e d ing i s f a r f rom exhaustive, but it of fers some worthwhile examples. Here, the key point is to educate yourself and work with your dental CPA to understand how to utilize the various expense rules to your advantage. Your CPA can be of
substantial help at tax preparation time but if you really want to optimize your deductions, you’ll need to set up the game board ahead of time!
Strategic Office Investment Plan As we are move into the fall, dentists start thinking about what they should hurry up and buy in order to secure a tax deduction before the end of the year. Of course, we are all in favor of income tax deductions, but we would rather see this as part of a well considered 3 to 5-five year plan for office improvement or modernization. By planning ahead, you not only take advantage of income tax deductions, but you also benefit by maximizing your return on investment through plotting out the right timing, scheduling training, and as appropriate, and promoting your new technology.
Right now would be a great time
to sit down with your dental CPA and your Burkhar t Equipment and Technolog y Managers to hash out the next 3 to 5 years of practice investment. Coordinate this with your tax planning and your comprehensive f inancial or wealth management plan. In doing so, you’re likely to find that this approach makes you a much more profitable dentist while at the same time, it helps you reduce taxes by taking advantage of the significant tax benefits currently available, such as the $250,000 Internal Revenue Code Section 179 deduction or the 50% first-year bonus depreciation allowance.
Tax Management Of Investments In the early parts of their careers, most dentists and specialists tend to have most, if not all of their portfolio investment dollars in tax deferred vehicles, such as a 401(k) plan or SIMPLE-IRA (see above).
(425) 216-1612
The Dentist’s CPASM
SM
Dental Practice Advisors
DentalGroupLLC
Integrated Financial Services to Enhance Your Income and
Quality of Life
There Is No Substitute For Dental Experience and Financial Expertise...
Members
www.adcpa.org

Wealth Management
CATALYST MAGAZINE Issue 4 2009 55.
With all of your investment funds in tax deferred accounts, we have no (immediate) tax concerns.
However, successful dentists and specialists will typically find that their taxable investment accounts will eventually outpace their tax deferred accounts, consequently making income taxes your largest investment expense. Unfortunately, most individuals—and regrettably most investment professionals—do a very poor job of managing investment related taxes.
The f i r s t and perhap s mo s t important line of defense against investment related taxes is the use of proper asset location. Not to be confused with Asset Allocation, asset location is the process by which you locate, in a tax efficient manner, the var ious as se t s included in your Asset Allocation. Top wealth managers understand the importance of this – if your advisor does not, it might be time for a second opinion.
As a simple example, Dr. Long has $500,000 in his IRA and $500,000 in his taxable account. Let’s pretend it is all cash at this point. Af ter going through the planning process with his advisor and looking at each of the various dimensions of risk relative to his goals, Dr. Long and his advisor decide that his asset allocation should be 57% to equities (stocks or stock funds) 3% to commodities (index fund) and 40% to high credit fixed income (bonds or bond funds), including short-term bonds and a floating allocation to TIPS (Treasury Inflation Protected Securities). The advisor who fails to understand, or is perhaps unwilling to do the work, would then locate the assets in the two accounts as follows:
Ta x ab le Ac c ount : $28 5,0 0 0 (57%) in diversi f ied equit ies, $15,000 (3%) in commodities, and $200,000 (40%) in tax-free municipal bonds (Dr. Long is in a
high tax bracket (40%). However, his municipal bonds only pay about 70% of the rate comparable taxable bonds might pay. Nonetheless, the advisor points out that Dr. Long will still have a higher return after tax with the lower municipal bond rates versus paying tax on the higher paying taxable bonds.
Ta x - Defer red ( IR A) Ac c ount : $285,000 (57%) in diversif ied e q u i t i e s , $1 5 , 0 0 0 (3 %) i n commodities, and $200,000 (40%) in taxable bonds. Here, the taxable status does not matter due to the tax-deferred nature of the account. So what ’s wrong here? Well , both accounts are aimed at the same goal (Dr. Long’s retirement), but the advisor has treated the two accounts as i f they were two portfolios. In contrast, the enlightened (tax aware) advisor would have t reated the t wo accounts as a single portfolio. V iewing this as one por t folio comprised of multiple accounts with different tax attributes frees the advisor to take advantage of strategic tax location.
Asset class equities, particularly tax-managed asset class equities, can be very tax efficient. Taxable distributions are managed to be kept to a “dull roar,” and the income that is distributed is primarily long-term capital gains (taxed at a much lower rate than ordinary income) and qualified dividends. Alternatively, bonds (or bond funds) kick out taxable income taxed at ordinary rates, as do TIPS (which also kick out the “phantom” CPI adjustment as ordinary income). Commodities also tend to kick out ordinary income. Armed with this knowledge, then, the enlightened advisor locates the assets as follows:
Taxable Account: $500,000 in tax-managed diversified equities, including al l of the quali f ied in ternat ional equi t ie s . Such international equities have foreign income tax withheld on dividends
paid. This withholding represents nothing but a cost in a tax deferred account whereas in a taxable account, the foreign taxes withheld can qualify for a dollar-for-dollar credit against your US tax.
Tax-Deferred Account: $70,000 in diversified equities (the remaining equity allocation), $30,000 in commodities (index fund), and $400,000 in bonds, including TIPS. Interestingly, the overall portfolio has not changed a bit. However, the after-tax, long-term return on this configuration will be higher, which therefore adds real value to Dr. Long’s portfolio and improves the likelihood that he will indeed achieve his goals.
Another reason for s t rateg ic asset location is the conversion of capital gains into ordinary income, which is clearly not what we want to accomplish. However, by unnecessarily putting equities into tax-deferred accounts, that is exactly what you will accomplish. Over the long haul, we expect our equities to grow, and in a taxable account, we can access those assets by paying a long-term capital gains tax on the growth. However, if equities are placed in a tax-deferred account, all that growth will be taxed as ordinary income, either to the owner or the owner’s heirs.
Tax Loss Harvesting: When (in par t icular) equit ies are down (Lower than your cost—think 2008!) you have an opportunity to legally harvest the loss and deduct it on your federal income tax return. Losses can offset any capital gains as well as ordinary income up to $3,000 per year. The balance will carry over and can be used against future capital gains (perhaps generated from the por t folio, thereby making rebalanc ing efficient and/or other capital gains, such as the sale of real estate or your practice). Done correctly, tax loss harvesting has no economic

Wealth Management
Now You Can Help Your Back AND Your Wallet!
With Brewer’s Fall Ergonomic Seating PromotionValid 9/14/09 - 12/31/09
Visit us at:CDA Booth #620
GNYDM Booth #1614
$100Rebate*per stool
* $100 rebate with each 9000, 9100, 9200, 9400 Series stool purchased. Invoice and rebate form must be completed and returned to Brewer-Design by 1/31/10. No exceptions will be made. Rebate is in the form of a check. www.brewer-design.com
Clinically Researched Ergonomic Seating Specialists Since 1947
Please contact your Equipment Dealer for promotion details. Valid on orders received by Brewer-Design starting 9/14/09 through 12/31/09.
9200 Series
9100 Series
9000 SeriesDynaCore 9400 Series, a NEW Therapeutic Dynamic Seating System
9400 Series
Offer also valid on all Assistant Models (not shown).
impact on your portfolio, yet it provides a legal tax deduction.
Some adv isor s over look t ax loss harvesting oppor tunit ies altogether, while others tend to look only for oppor tunities as the end of the year approaches. Enlightened advisors monitor for tax loss harvesting opportunities throughout the year. Another benefit of strategic asset location (see above) is that it is much more likely for (volatile) equities to present tax loss harvesting oppor tunit ies. Therefore, this represents one more reason why you do not want equities locked up in your tax-deferred account.
Step-Up in Basis: If you have not already seen the light on asset location, here is yet another factor on strategic tax location. Despite the dismal equity markets in 2008, in the long run, we expect that
equities are much more likely to grow than bonds. Your equities will be taxed the same for Estate Tax purposes upon death, whether they are held in your taxable account or in your tax deferred account. However, assets held outside your tax deferred account (i.e., in your taxable account) will receive a step-up in income tax basis to your heirs. This can result in a very significant tax savings to your family.
Conclusion Income (and estate) taxes are one of your largest, yet controllable expenses. Income taxes permeate all of your financial activities – practice, personal, and investment. Educating yourself and/or working with a top dental CPA and Wealth Manager can add profound value to your long-term financial outcome.
Sam Martin is Director
of Wealth Management
Services and Advanced
Tax Planning for the
Dental Group, LLC /
Mar t in Boy le PLLC /
Dental Wealth Advisors,
LLC, a CPA , pract ice
advisory, financial planning and Wealth
Management services group exclusively
serving dentists and their practices. Sam
is a Certified Public Accountant (CPA), a
Certified Financial Planner (CFP®), and
holds a Masters Degree in Federal Income
Taxation. Located in Kirkland, WA – Sam
can be reached at 425.216.1612 or Sam@
cpa4dds.com.
Wealth Management
CATALYST MAGAZINE Issue 3 2009 57.
WWWWWWWWWWWWeeeeeeeeeeeaaaaaaaaaaallllllllllllltttttttttthhhhhhhhhhhhhh MMMMMMMMMMMMaaaaaaaaaannnnnnnnaaaagggggggggeeeeemmmmmmmeeeeeeeeeeennnnnnnnnnnnnnttttttttttttttttttttttttt
CACACACACACACACAAATATATATATATATATATATAALYLYLLYLYLYLYLLYLYLL STSTSTSTSTSTSTSTT M MM M M MMMMAGAGAGAGAGAGAGAGAA AZAZAZAZAZAZAZAZAAZINININININIININEEEEEEEEE IsIsIsIsIssususuuusue e eeee 33 3 3 2020202 090909099990909099 5757575557577......
Hobbies:
What I like about my job:
My Greatest challenge is:
Success at our office means:
What Burkhart means to me:
Dental Hygienist, Tom O’Brien, DDS - Houston, TX
Decorating, cooking, gardening, crafts like making Bible verse cards for my Honduras team.
I have to say that I really love everything about my job. I have to start with my boss, because he has been one of my biggest blessings and a huge inspiration in my life for more than 30 years. He allows me to be not only his hygienist, but also his "partner" in treating our patients. I also love our patients! They are my extended family.
Deep inside I am a very shy person. It's undetectable most of the time because I am also very talkative. But speaking in front of an audience terrifies me. But God has allowed me to do just that on occasion for the non-profit organization I am a part of. I can't say it is easy, but when you speak from the heart about something, it becomes easier.
Seeing a patient who has found themselves behind in their dental care and being able to restore their dental health and overall self-esteem. Being able to perform at the best of our abilities, comfortably and affordably, and most of all having our patients realize that we really are making a difference in our dental office.
Burkhart has been an amazing example of very hard working people, with integrity and fortitude.The service support is beyond compare. The office support team has made many complicated situations less complicated. They make my life, personally, a whole lot more simple, and it is a blessing to not have to worry about
anything. It is a privilege to be in partnership with all of the Houston Branch.
Kim Martin
CATALYST MAGAZINE Issue 4 2009 57.
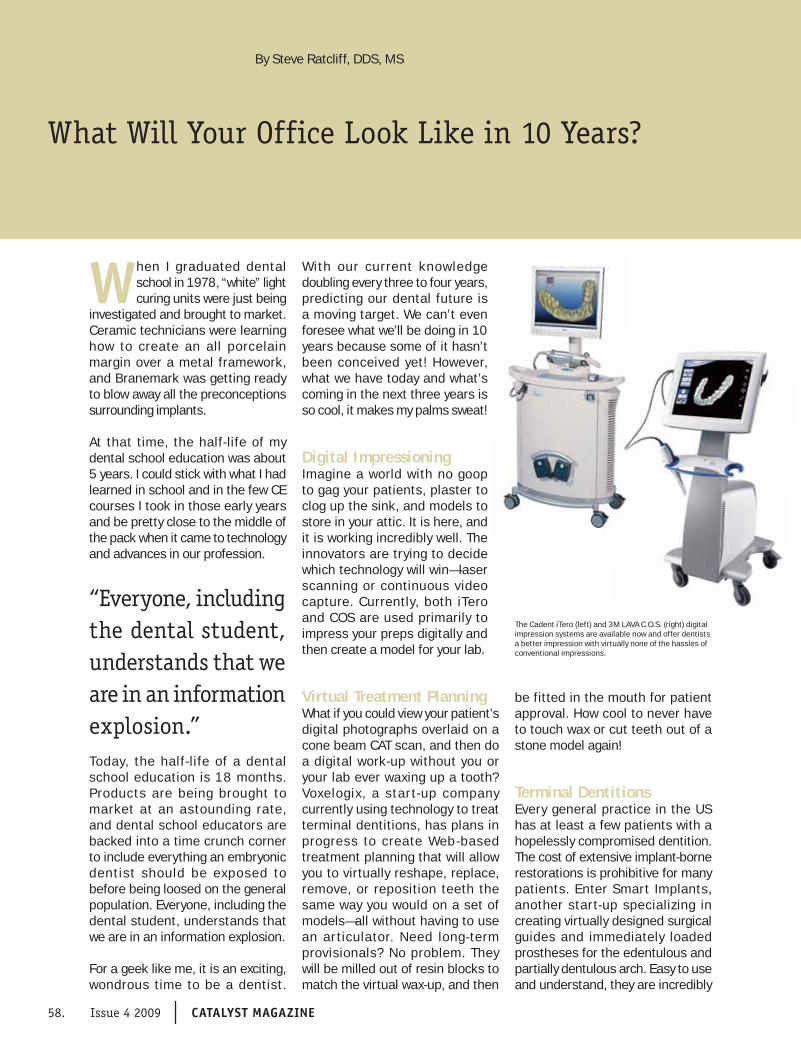
Continuing Education
58. Issue 4 2009 CATALYST MAGAZINE
What Will Your Office Look Like in 10 Years?
By Steve Ratcliff, DDS, MS
When I graduated dental school in 1978, “white” light curing units were just being
investigated and brought to market. Ceramic technicians were learning how to create an all porcelain margin over a metal framework, and Branemark was getting ready to blow away all the preconceptions surrounding implants.
At that time, the half-life of my dental school education was about 5 years. I could stick with what I had learned in school and in the few CE courses I took in those early years and be pretty close to the middle of the pack when it came to technology and advances in our profession.
Today, the half- life of a dental school education is 18 months. Products are being brought to market at an astounding rate, and dental school educators are backed into a time crunch corner to include everything an embryonic dentist should be exposed to before being loosed on the general population. Everyone, including the dental student, understands that we are in an information explosion.
For a geek like me, it is an exciting, wondrous time to be a dentist.
With our current knowledge doubling every three to four years, predicting our dental future is a moving target. We can’t even foresee what we’ll be doing in 10 years because some of it hasn’t been conceived yet! However, what we have today and what’s coming in the next three years is so cool, it makes my palms sweat!
Digital ImpressioningImagine a world with no goop to gag your patients, plaster to clog up the sink, and models to store in your attic. It is here, and it is working incredibly well. The innovators are trying to decide which technology will win—laser scanning or continuous video capture. Currently, both iTero and COS are used primarily to impress your preps digitally and then create a model for your lab.
Virtual Treatment PlanningWhat if you could view your patient’s digital photographs overlaid on a cone beam CAT scan, and then do a digital work-up without you or your lab ever waxing up a tooth? Voxelogix, a star t-up company currently using technology to treat terminal dentitions, has plans in progress to create Web-based treatment planning that will allow you to virtually reshape, replace, remove, or reposition teeth the same way you would on a set of models—all without having to use an ar ticulator. Need long-term provisionals? No problem. They will be milled out of resin blocks to match the virtual wax-up, and then
be fitted in the mouth for patient approval. How cool to never have to touch wax or cut teeth out of a stone model again!
Terminal DentitionsEvery general practice in the US has at least a few patients with a hopelessly compromised dentition. The cost of extensive implant-borne restorations is prohibitive for many patients. Enter Smart Implants, another start-up specializing in creating virtually designed surgical guides and immediately loaded prostheses for the edentulous and partially dentulous arch. Easy to use and understand, they are incredibly
“Everyone, including the dental student, understands that we are in an information explosion.”
The Cadent iTero (left) and 3M LAVA C.O.S. (right) digital impression systems are available now and offer dentists a better impression with virtually none of the hassles of conventional impressions.

Continuing Education
CATALYST MAGAZINE Issue 4 2009 59.
easy to deliver for both surgeon and GP, and at a much lower cost than traditional hybrid prostheses.
OrthodonticsRemember cephs from dental school? Our or tho colleagues spend hours tracing them to do a treatment plan. Anatamage, a software company focusing on CTCB applications, has a product which wraps your patients’ digital pictures around the volumized CT scan, and then moves teeth orthodontically in a movie format. This allows the patient to see how the movement progresses though treatment, and what the effects will be on the face.
Tooth BudsA group of Japanese researchers has successfully implanted a tooth bud derived from stem cells in a mouse. The tooth grew into the arch, occluded appropriately, and had a pulp that responded to stimuli. No report on how the mouse is doing after they extracted the newly grown tooth to see what it looked like from the inside out.
Ten years from now, we may no longer be doing implants. We may be replacing our hands with robotically performed procedures and using materials that haven’t even been invented yet. We won’t be reading paper journals, because they will be outdated by the time they get to our desks, and we will be connected to a worldwide “group” practice, with infinite resources to help us diagnose, plan treatment, and complete procedures we haven’t even seen yet.
Hang on! It is going be a wild ride!
Summit Dental Study Group is pleased to have Dr. Steve Ratcliff present “Living in a Virtual World and Other Ramblings through a Cluttered Mind.” Dr. Ratcliff will explore the vir tual ar ticulator, digital impressions, and how 3-D
cone beam technology is changing the way we practice.
For more information on this and other Summit lectures, please contact your loc al Burkhar t Account Manager, call Summit at (800)765-7277, or visit our Web site at www.summitdds.com
S teve Ratc l i f f , DD S,
MS is the Executive VP
of Specialty Education
at The Spear Institute
in Scottsdale, Arizona
w h e r e i s h e l p s
special is ts and their
restorative colleagues
embrace the gif ts and challenges of
interdisciplinary care.
Steve has been in the private general
practice for 30 years and for the last
15 year s has focused h i s work on
comprehensive adult restorative care.
Although he was nicknamed “the claw” by
several of his friends in dental school after
almost failing basic dental techniques he
has become regarded as one of the premier
clinicians in the US.
The former Chairman of Education at the
Pankey Institute, Steve is passionate about
helping dentists reach their preferred future
and is an engaging and down to earth
speaker. He presents and facilitates small
groups with a combination of excellent
clinical examples, interactive discussion
and well organized concepts.
The author of many journal articles and
the book, Digital Dental Photography: A
Clinician’s Guide; Steve is excited about
the uses of photography to bring clinical
examples to life, as well as how to use
images for interdisciplinary discussion and
patient understanding.
H e l e c t u r e s i n t e r n a t i o n a l l y o n
interdisciplinar y care, aesthetic and
restorative dentistry, occlusion and is well
known for his workshops on philosophy of
life and dental practice and he will always
speak at length about his experience as a
neophyte grandpa. (an exceptionally YOUNG
grandpa)
Living in a
Virtual World
and Other
Ramblings
Through a
Cluttered
Mind
Steve Ratcliff, DDS, MS
CONTINUING EDUCATION
Virtual dentistry, what is it? We know about cadcam and milled copings and abutments; yet really it is much more! In a few short years our lab benches and dental laboratories will look like video gaming centers. Did you hate articulators in dental school; you may never need one again! What about digital impressions, do they work? Can we really eliminate all that goo we put in people’s mouths? Even if all this works, why should I change? Digital advances have opened up a whole new dimension in our dentistry and for the benefi t of our patients. We can be more thorough and more accurate in our diagnoses and provide care that is more precise, easier to fabricate and deliver and ultimately takes less time and with less discomfort to our patients. Simply, we can’t aff ord to not stay current with technology!
We will explore:
• Th e virtual articulator
• How 3D cone beam technology is changing the way we practice
• Treating the terminal dentition-virtually
• Digital Impressions-beautiful dies
• What do I need in my offi ce?
Join us!November 19, 2009
Seattle, Washington
April 15, 2010San Diego, California
FOR MORE INFORMATION OR TO REGISTER, GO TO
WWW.SUMMITDDS.COM

the 2009-2010
Summit Speakers
Summit Dental Study Groupis an ADA CERP Recognized Provider
Programs Are
Supported By
Educational
Grants From:
What is Summit?
Summit Dental Study Group is dedicated to enhancing
and improving the practice of dentistry by offering quality
continuing education programs on pertinent and relevant
topics, delivered by recognized leaders in dental education. It is our goal to meet and exceed the needs and expectations of our participant by developing
courses that address their current clinical and business
concerns in practice, and provide a forum to network and share information with their colleagues in a relaxed,
constructive and positive environment.
Mr. Rolfe Carawan
“Tougher than the Times: How
to Prevent Practice Decay”
Seattle, WA – April 22, 2010
Dr. James Howard
“They are Common and They are
Treatable: Practical Guidelines
for Managing TMJ Disorders”
Seattle, WA – October 22, 2009
Dr. Peter Jacobsen
“Drugs, Bugs and Dentistry:
What to Prescribe!”
Richland, WA – October 30, 2009
Dr. Vince Kokich, Jr.
“Interdisciplinary Management
of Anterior Esthetic
Discrepancies”
San Diego, CA – November 19, 2009
Dr. John Kois
“Interdisciplinary Treatment
Planning: Diagnostically
Driven”
San Diego, CA – January 15, 2010
Dr. Mark Latta
“New Technologies Leading to
Better Clinical Performance in
Resin Systems”
Seattle, WA – February 4, 2010
Dr. Aldo Leopardi
“Top Down Approach to Dental
Implant Treatment Planning:
Parameters for Success in the
Aesthetic Zone”
Seattle, WA – March 18, 2010
Dr. Mark Murphy
“Profitable Behaviors to
Accelerate Your Practice NOW!”
Tulsa, OK – April 8, 2010
Dr. Steve Ratcliff
“Living in a Virtual World and
Other Ramblings Through a
Cluttered Mind”
Seattle, WA – November 19, 2009
San Diego, CA – April 15, 2010
Matt Roberts, CDT
& Dr. John Roberts
“Achieving Predictable
Aesthetics”
Seattle, WA – May 20, 2010
Dr. John West
“The Essence of Endodontic
Excellence: What Every
Clinician Should Know”
Seattle, WA – January 21, 2010
Ask Your Burkhart
Account Manager
about the Exciting
Continuing
Education
Opportunities Near
You!
www.summitdds.com1-800-765-7277

Intelligent MagneticSensor Connector
The NEW
GREEN TO GOPLANMECA® ProSensor
• Magnetic connector from sensor tocontrol box allowing one-handed useattaches quickly and easily releasesfrom interface box under tension(unique to ProSensor)
• Exclusive LED light provides instantaneousfeedback by displaying different colorsto indicate current status of sensorensuring proper image acquisition
• Kevlar reinforced cable has only 2 wiresenhancing durability
• Sensors are hermetically sealed to allowimmersion to prevent infection topatient (unique to PLANMECA)
Sensors available in threesizes 0, 1, and 2
Size 2 Image
Size 0 Connector
PLANMECA®
ProSensorNEW 5 YEAR
Warranty Program!
PLANMECA USA INC. • 100 N. Gary Ave., Suite A, Roselle, IL 60172 • Phone: (630) 529-2300 • Fax: (630) 529-1929 • www.planmecausa.com
A picture is worth a thousand words and the new Digital Doc ICON intraoral camera delivers
brilliantly. See the beautiful colors and detailed images that ICON’s seven precision optical lenses, 8 point LED
lighting, and Sony’s Hi-Resolution CCD create.
No other camera offers the fl exibility of ICON’s variable touch focus, with unmatched sharpness and range from
5mm macro close-ups to full arch and full smile. And now it’s simpler than ever to use, with a specially designed USB
connector that fi ts any dental unit, plus the ergonomic dual capture buttons for right or left hand use.
See for yourself why the new ICON is the #1 camera in North America.
®
The Moment of Clarity.
Sharper, Simpler, Smarter.
© 2
009
Dig
ital D
oc L
LC, 4
511
Gol
den
Foot
hill
Park
way
, El D
orad
o H
ills,
CA
957
62.
The
Dig
ital D
oc lo
go a
nd ic
on lo
go a
re t
rade
mar
ks o
f D
igita
l Doc
Inc.
All
right
s re
serv
ed.
Unique USB 2.0 connector sits next to your highspeed in any dental unit.
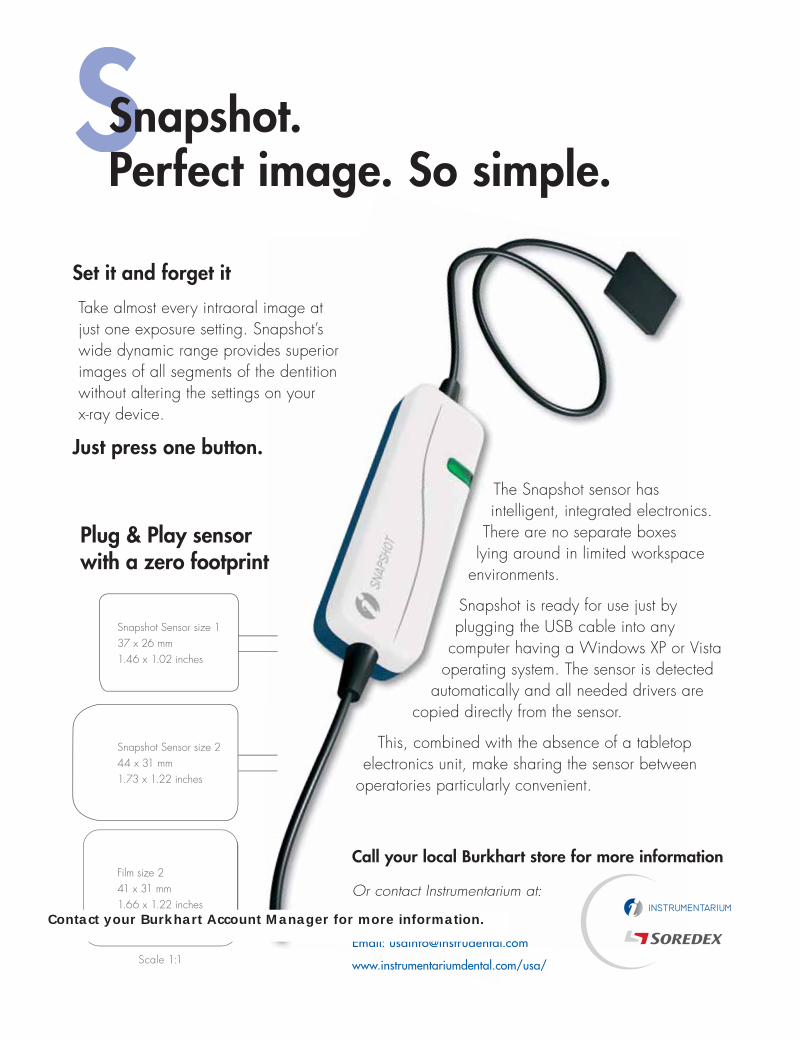
TechnologyTalking Cone Beam
Wealth ManagementAdvanced Tax Planning
The Woodlands Dental GroupThe Power of a Group
A MAGAZINE DEDICATED TO THE SUCCESS OF DENTISTRY ISSUE 4 2009A MAGAZINE DEDICATED TO THE SUCCESS OF DENTISTRY ISSUE 4 2008
Call your local Burkhart store for more information
Or contact Instrumentarium at:
Toll free: (800) 558-6120
Email: [email protected]
www.instrumentariumdental.com/usa/
SSnapshot. Perfect image. So simple.
Plug & Play sensor with a zero footprint
Scale 1:1
Film size 241 x 31 mm1.66 x 1.22 inches
Snapshot Sensor size 244 x 31 mm1.73 x 1.22 inches
Snapshot Sensor size 137 x 26 mm1.46 x 1.02 inches
Set it and forget it
Take almost every intraoral image at just one exposure setting. Snapshot’s wide dynamic range provides superior images of all segments of the dentition without altering the settings on your x-ray device.
Just press one button.
The Snapshot sensor has intelligent, integrated electronics.
There are no separate boxes lying around in limited workspace
environments.
Snapshot is ready for use just by plugging the USB cable into any
computer having a Windows XP or Vista operating system. The sensor is detected
automatically and all needed drivers are copied directly from the sensor.
This, combined with the absence of a tabletop electronics unit, make sharing the sensor between
operatories particularly convenient.
Contact your Burkhart Account Manager for more information.
Catalyst M
agazine B
urkhart Dental —
Issue 4 2
00
9