somatosensory sensation & motor functions
DESCRIPTION
Somatosensory Sensation & Motor Functions. Interdisciplinary Program in Neuroscience Eye Movement & Vision Research LAB Hwang, Jae Won. Somatosensory Sensation. Somatosensory Sensation Modalities Receptors Somatosensory Pathways Somatosensory Cortex Motor Functions Disorders. - PowerPoint PPT PresentationTRANSCRIPT
Interdisciplinary Program in NeuroscienceEye Movement & Vision Research LAB
Hwang, Jae Won
Somatosensory Sensation & Motor Functions
Somatosensory Sensation
Somatosensory Sensation– Modalities– Receptors– Somatosensory Pathways– Somatosensory Cortex
Motor Functions Disorders

Somatosensory Modalities
Touch Proprioception Nociception Temperature Sense
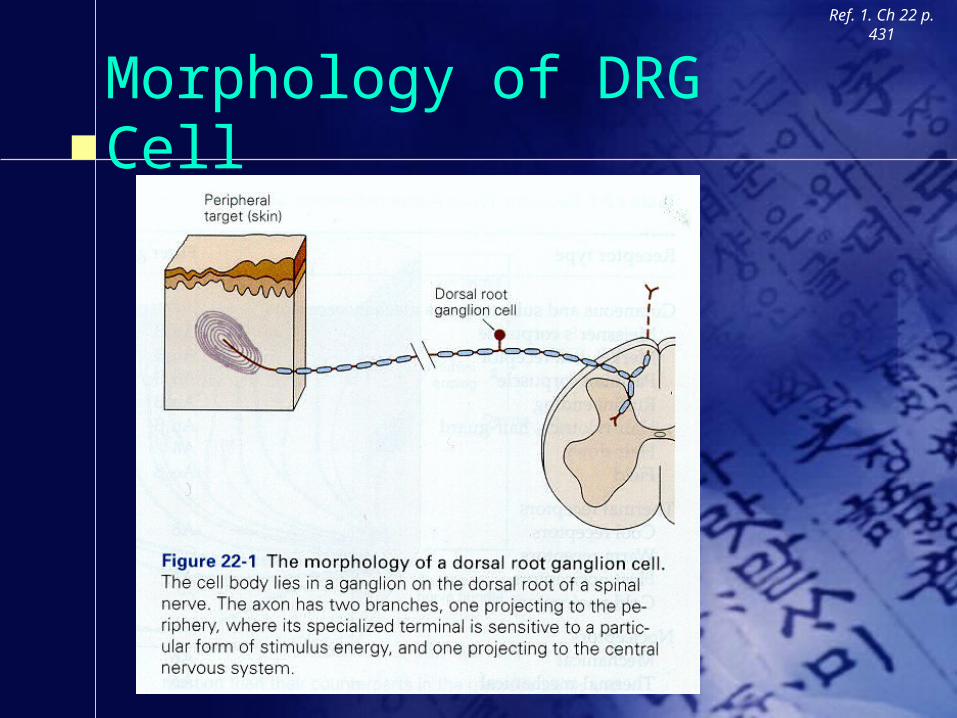
Morphology of DRG Cell
Ref. 1. Ch 22 p. 431
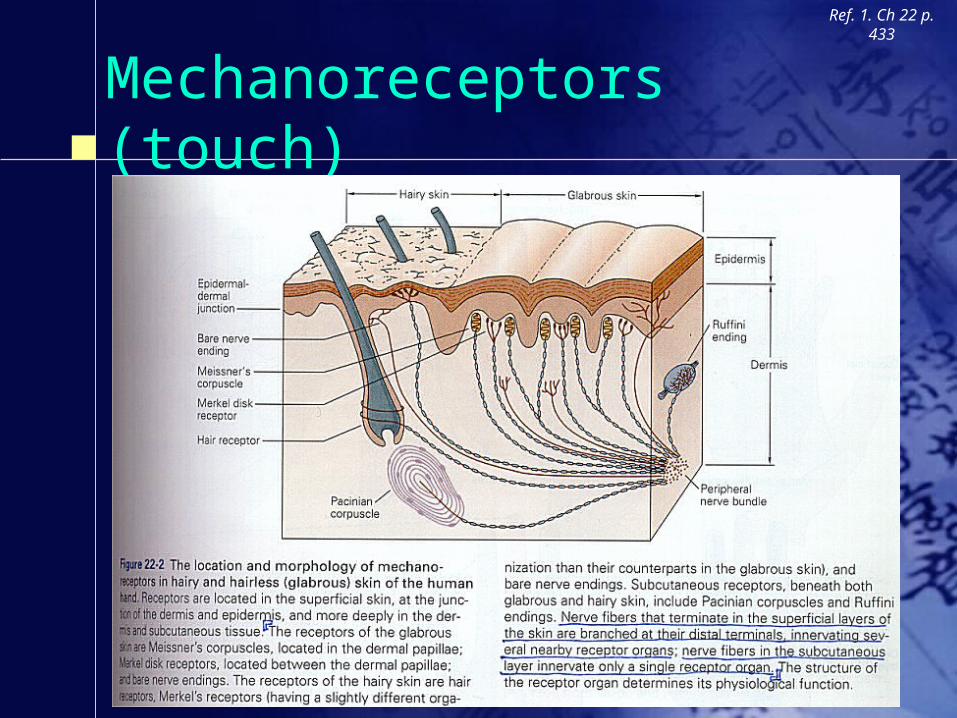
Mechanoreceptors (touch)
Ref. 1. Ch 22 p. 433

Mechanoreceptors (proprioception)
Ref. 1. Ch 21 p. 415

Receptor Types
Ref. 1. Ch 22 p. 432

Receptive Field (touch)
Ref. 1. Ch 22 p. 434

Two Point Discrimination
Ref. 1. Ch 22 p. 436

Distribution of DermatomesRef. 1. Ch 22 p.
445
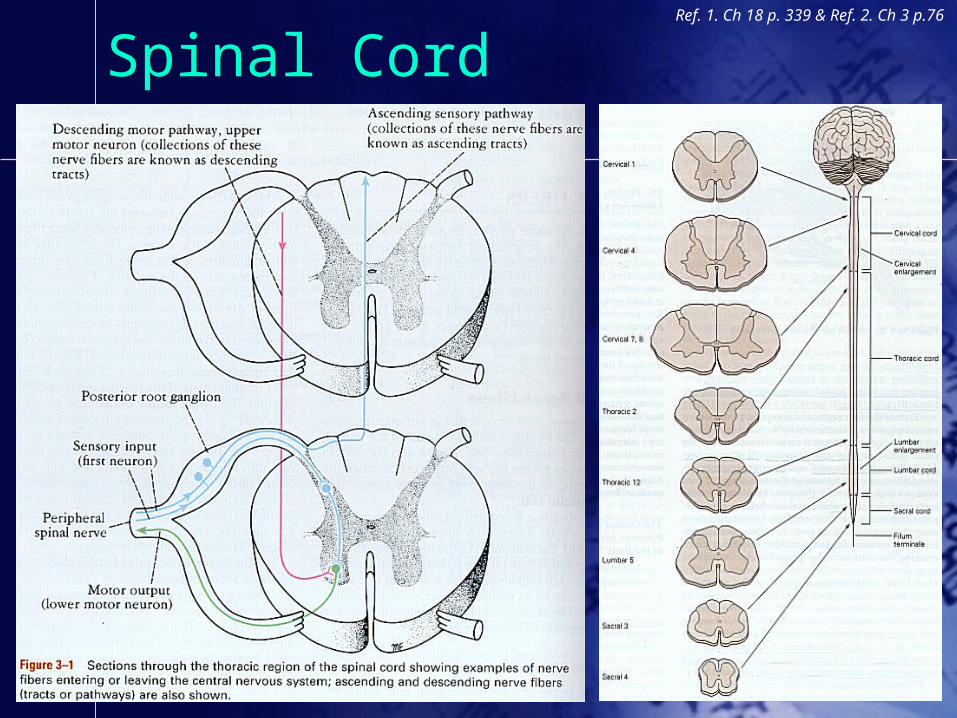
Spinal CordRef. 1. Ch 18 p. 339 & Ref. 2. Ch 3
p.76

Touch & Proprioception(joint) PathwayRef. 3. http://thalamus.wustl.edu/course/
bassens.html

Decussation of Medial Lemnisci
Ref. 2. Ch 5 p. 195

Proprioception(muscle & tendon) Pathway
Ref. 3. http://thalamus.wustl.edu/course/body.html

Nociceptive Afferent Fibers
Ref. 1. Ch 24 p. 473-474

Pain & Temperature Pathway
Ref. 3. http://thalamus.wustl.edu/course/body.html
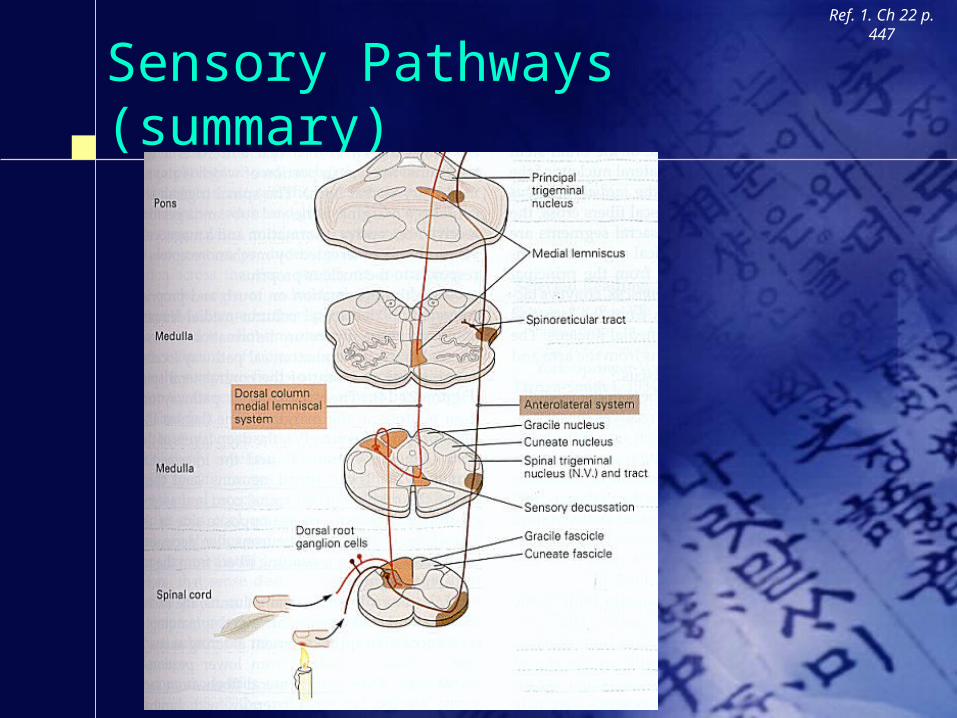
Sensory Pathways (summary)
Ref. 1. Ch 22 p. 447
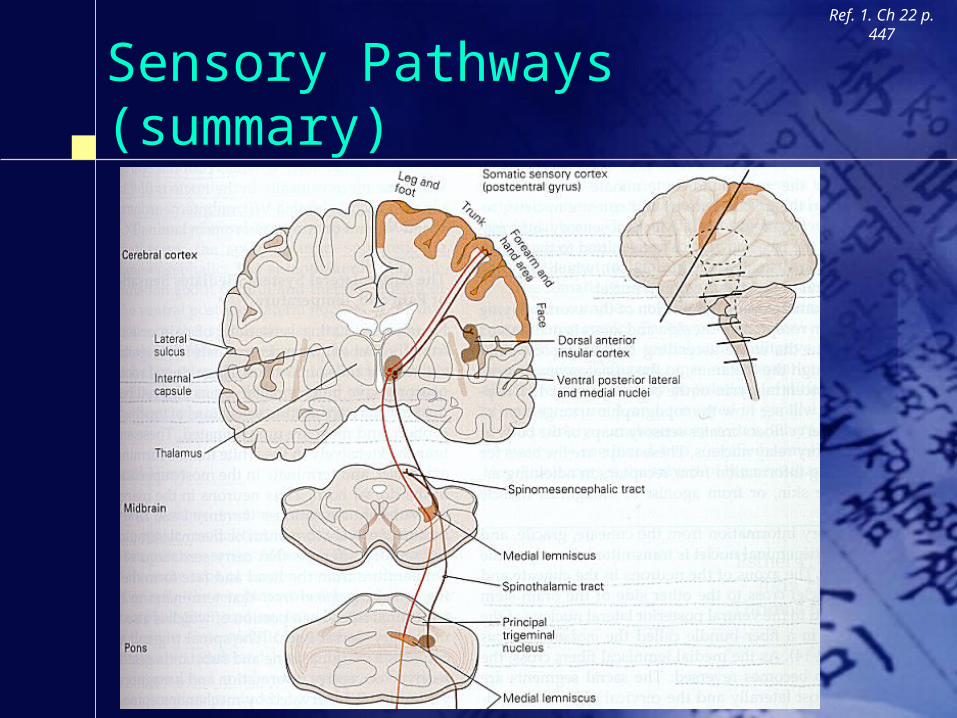
Sensory Pathways (summary)
Ref. 1. Ch 22 p. 447
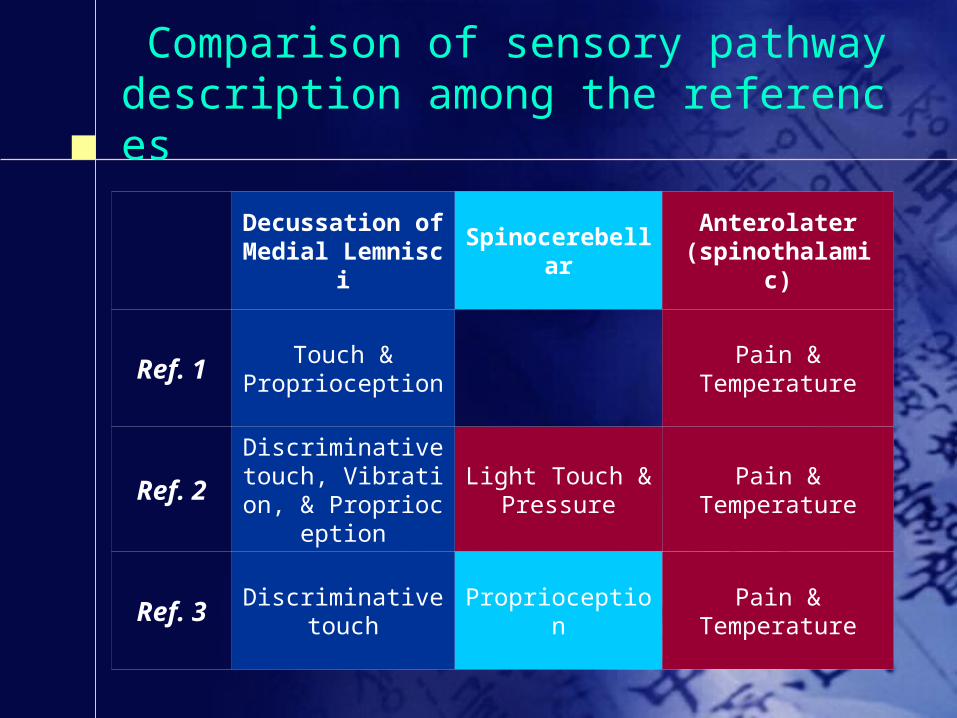
Comparison of sensory pathway description among the references
Decussation of Medial Lemnisci Spinocerebellar Anterolater
(spinothalamic)
Ref. 1 Touch &Proprioception
Pain &Temperature
Ref. 2Discriminative touch, Vibration, & Prop
rioception
Light Touch &Pressure
Pain &Temperature
Ref. 3 Discriminative touch
Proprioception Pain &Temperature

Ascending & Descending Tracts
Ref. 2. Ch 4 p. 145
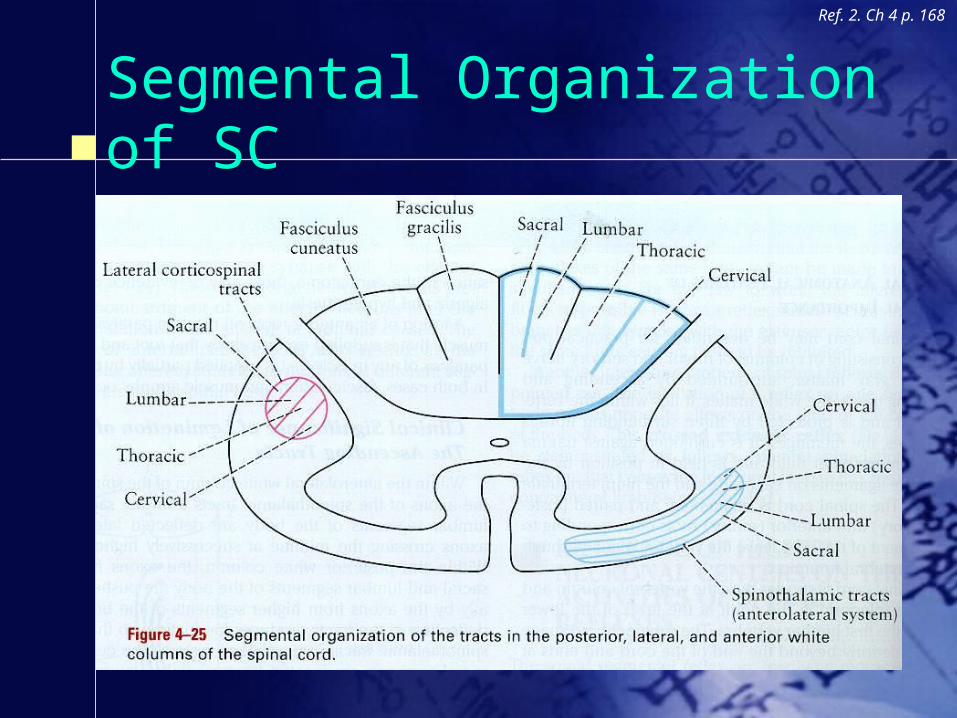
Segmental Organization of SC
Ref. 2. Ch 4 p. 168

Thalamus
Ref. 1. Ch 18 p. 343

Somatosensory Cortex
Ref. 1. Ch 23 p. 453

RF of Cell in a Column in SSC
Ref. 1. Ch 23 p. 456
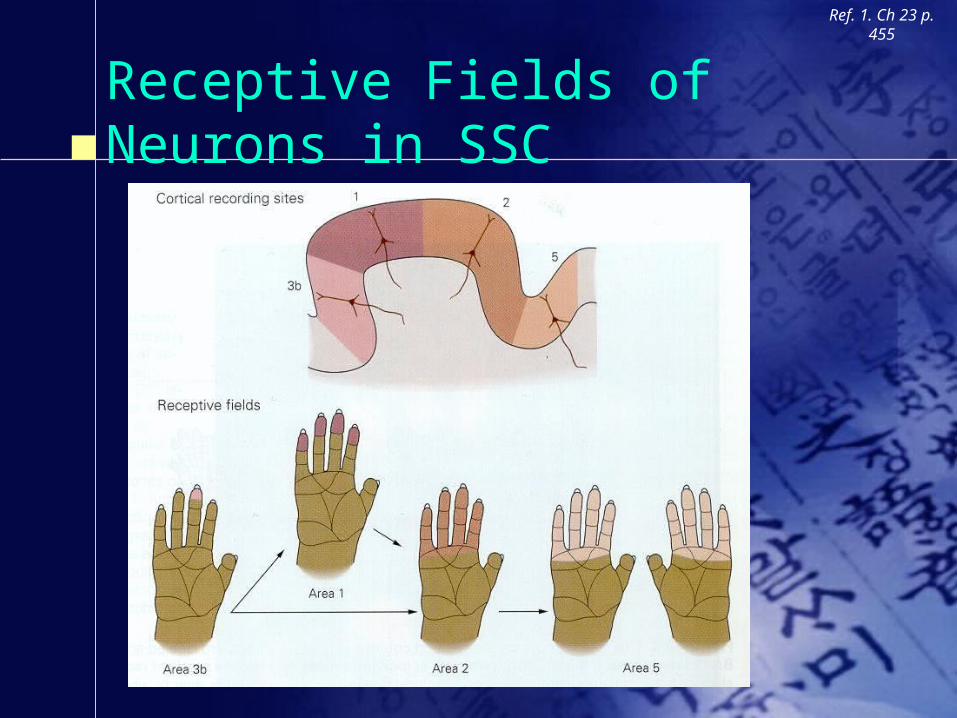
Receptive Fields of Neurons in SSC
Ref. 1. Ch 23 p. 455
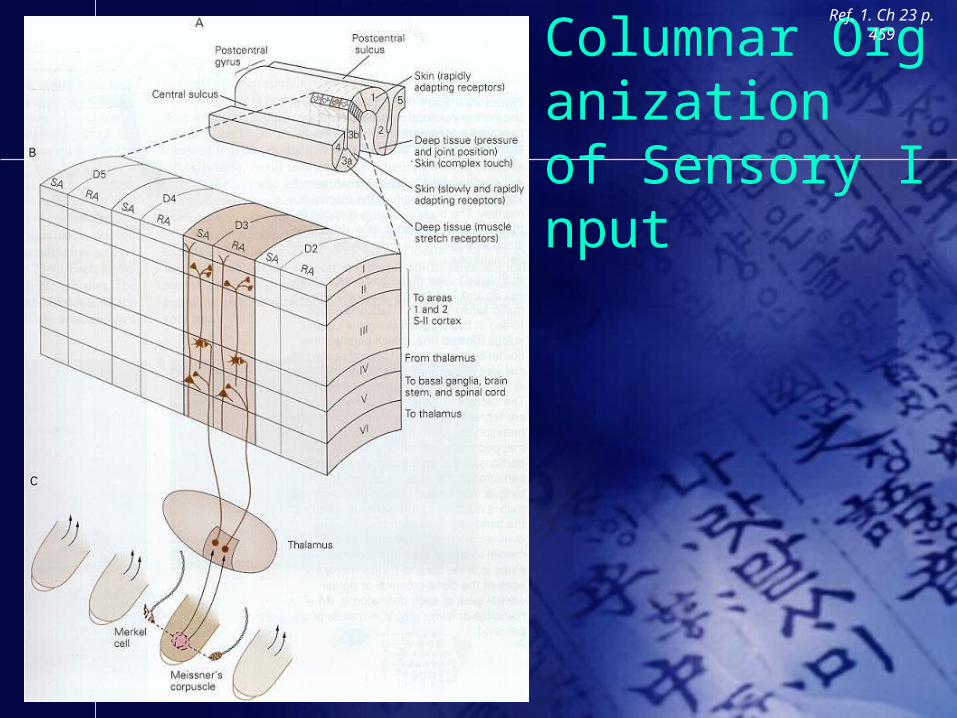
Columnar Organization of Sensory Input
Ref. 1. Ch 23 p. 459
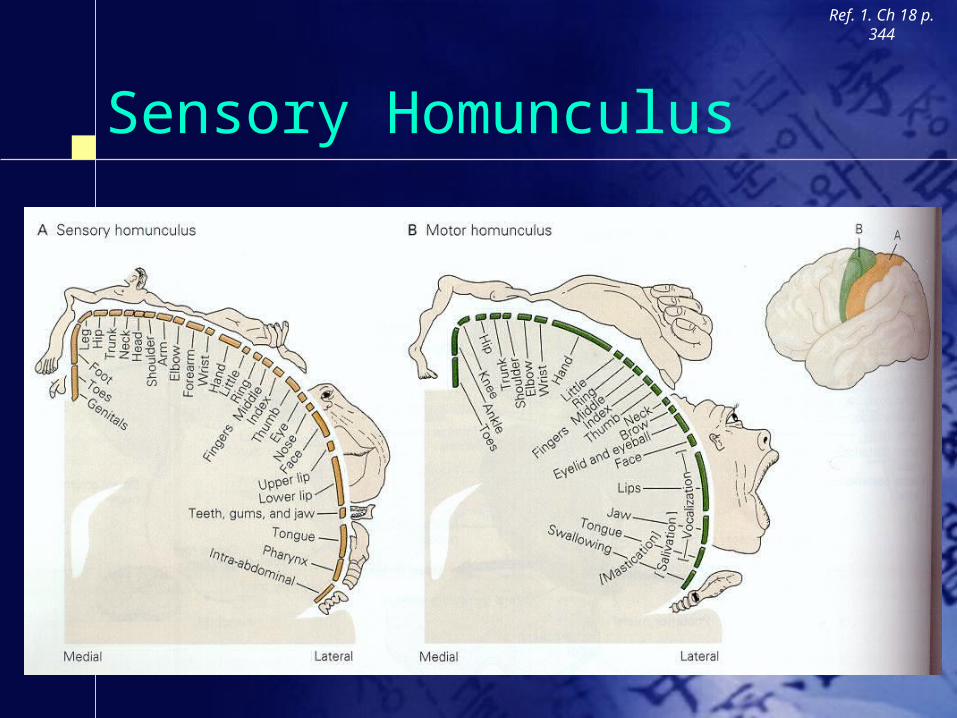
Sensory Homunculus
Ref. 1. Ch 18 p. 344
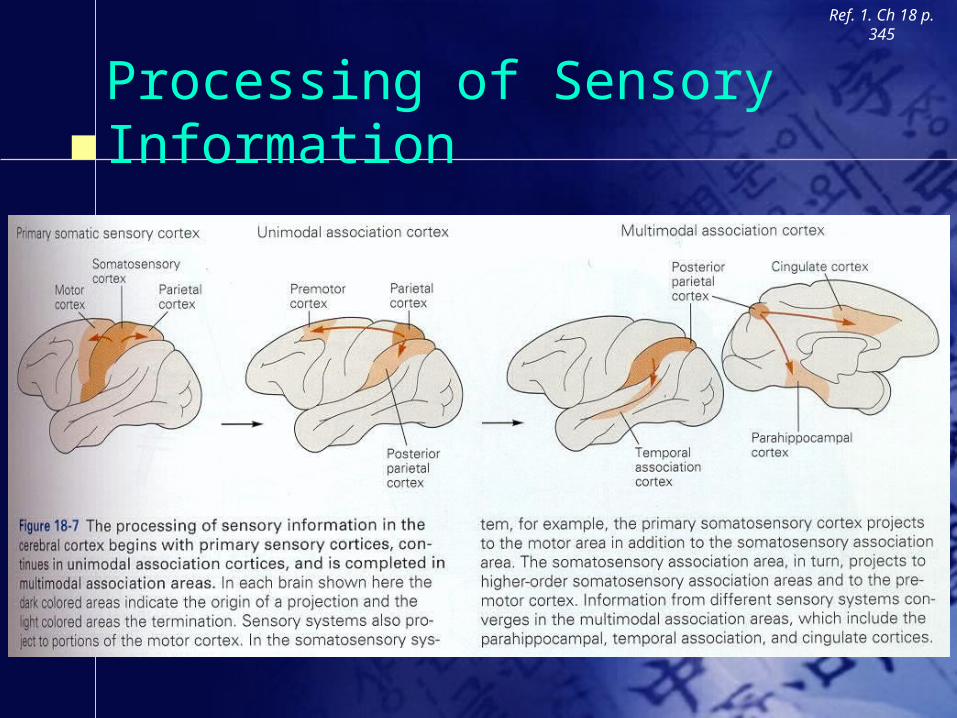
Processing of Sensory Information
Ref. 1. Ch 18 p. 345

Motor Functions
Somatosensory Sensation Motor Functions
– Brain Structures Involved in Motor Control– Motor Pathways– Motor Neurons– Neuromuscular Junction
Disorders
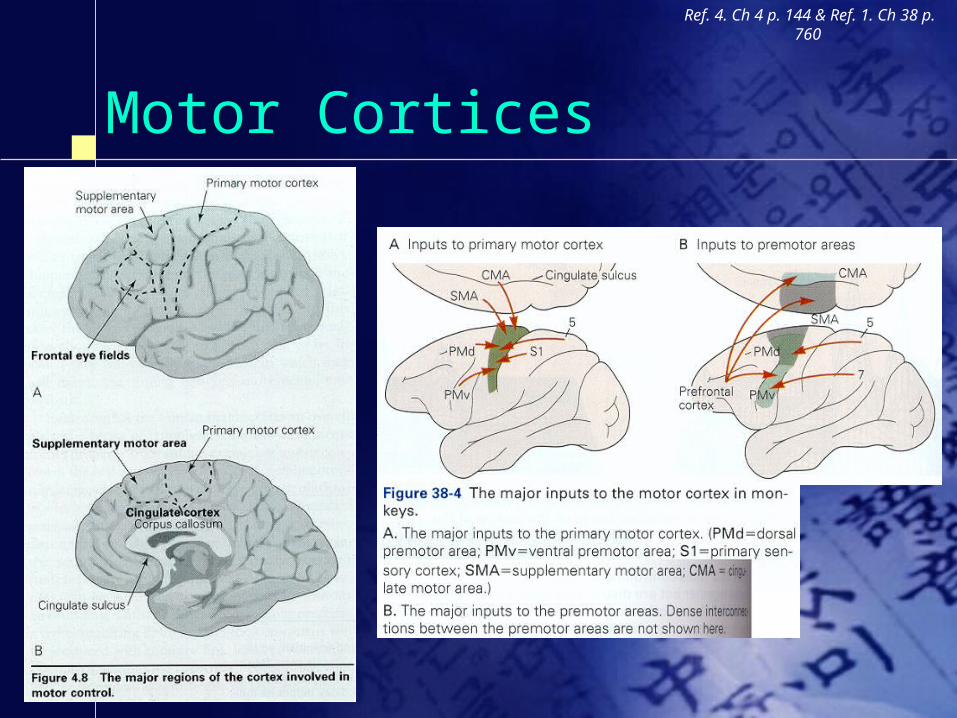
Motor Cortices
Ref. 4. Ch 4 p. 144 & Ref. 1. Ch 38 p. 760

Flow of Motor Information
Ref. 1. Ch 19 p. 356

Supplementary & Premotor Areas
Ref. 1. Ch 38 p. 773

Parietal Cortex
Ref. 4. Ch 4 p.148 & Ref. 1. Ch 28 p. 567
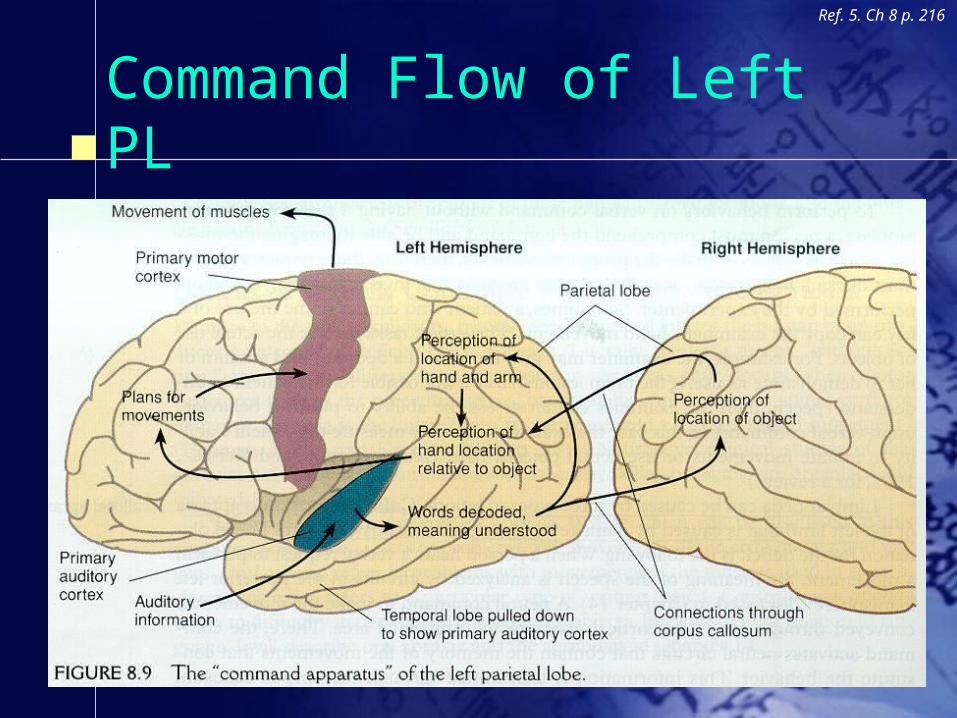
Command Flow of Left PL
Ref. 5. Ch 8 p. 216
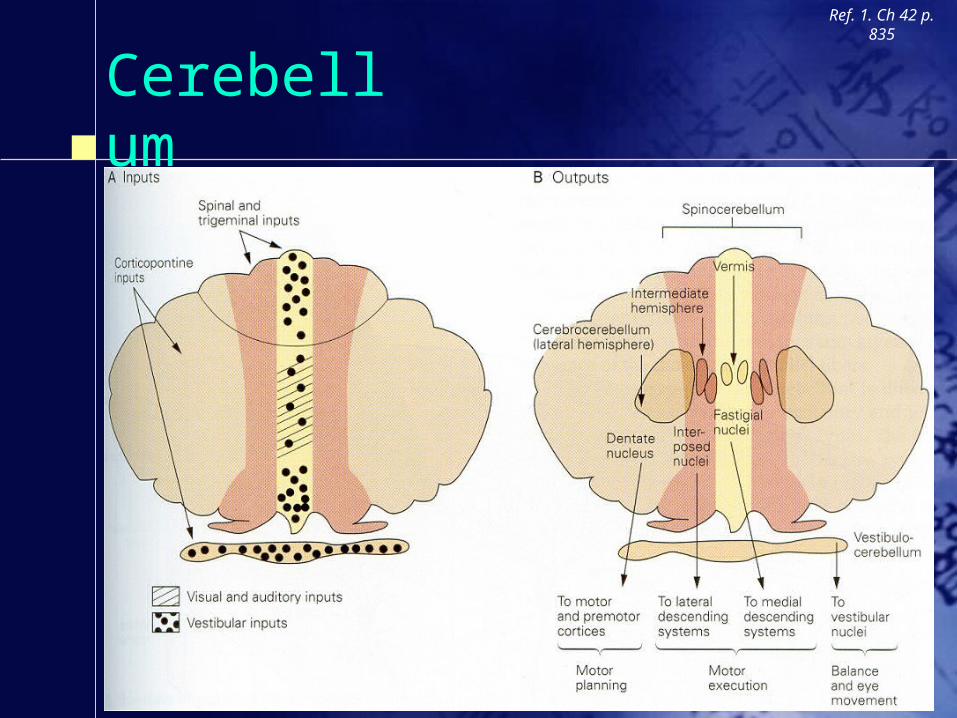
Cerebellum
Ref. 1. Ch 42 p. 835

Basal Ganglia
Ref. 1. Ch 43 p. 856
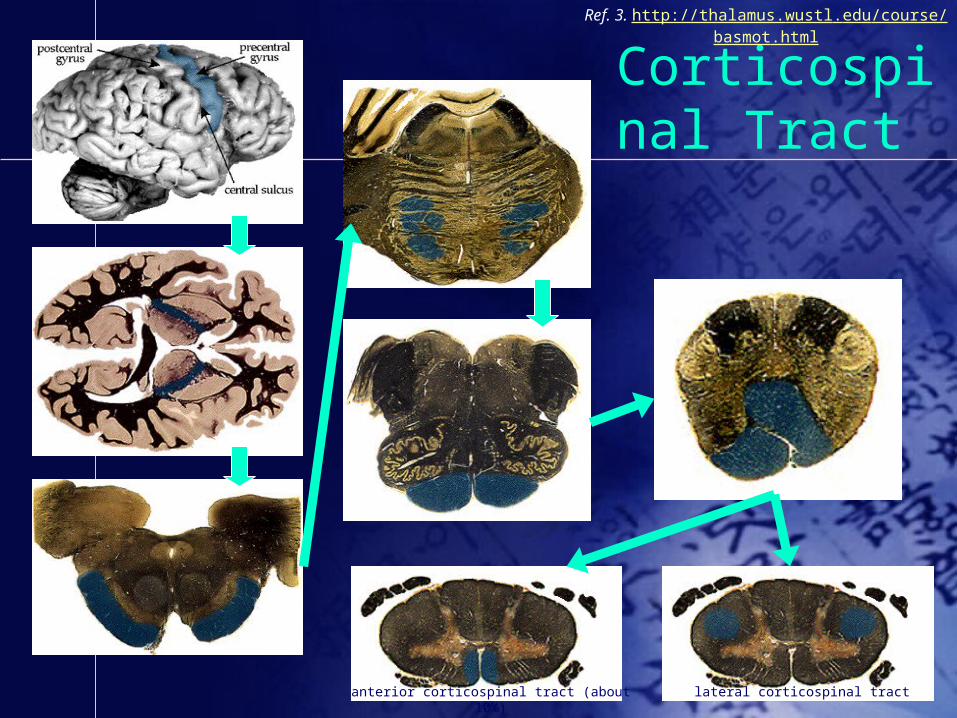
Corticospinal Tract
Ref. 3. http://thalamus.wustl.edu/course/basmot.html
anterior corticospinal tract (about 10%) lateral corticospinal tract
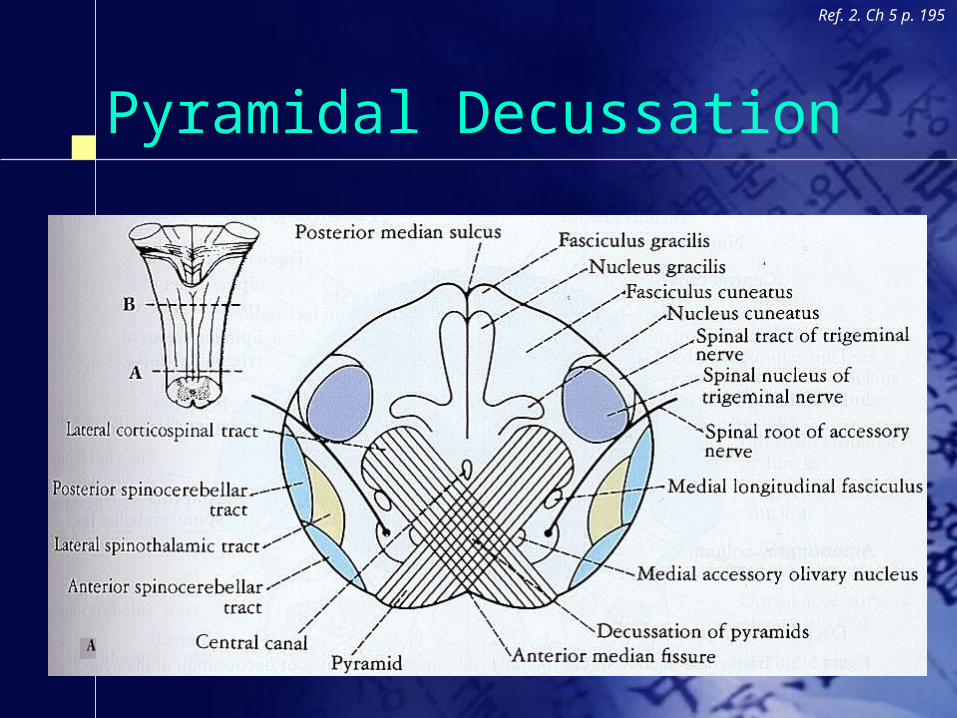
Pyramidal Decussation
Ref. 2. Ch 5 p. 195

Corticospinal Tract
Ref. 1. Ch 18 p. 346

Corticospinal Tract
Ref. 1. Ch 18 p. 346

Corticobulbar & Rubrospinal Tracts
Ref. 5. Ch 8 p. 212
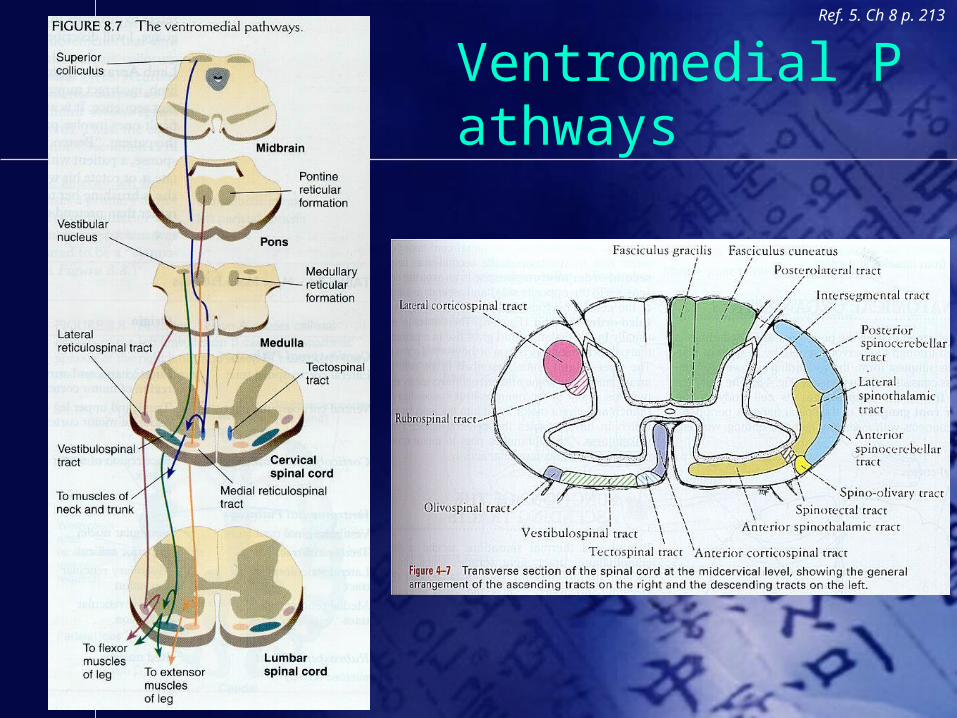
Ventromedial Pathways
Ref. 5. Ch 8 p. 213
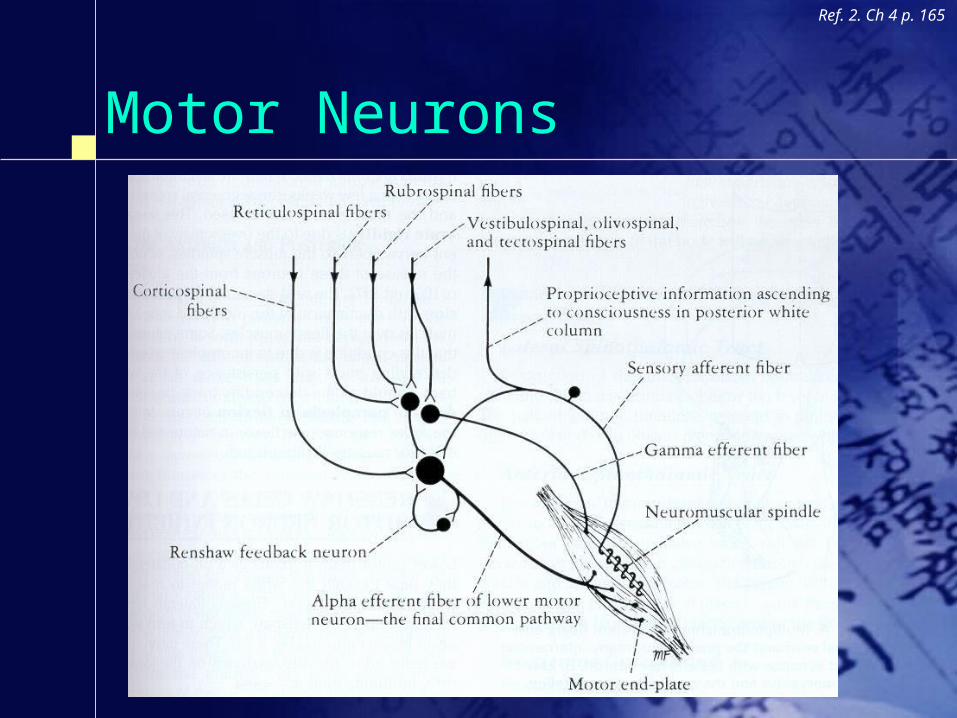
Motor Neurons
Ref. 2. Ch 4 p. 165

Neuromuscular Junction
Ref. 1. Ch 11 p. 188

Disorders
Somatosensory Sensation Motor Functions Disorders
– Spinal Cord Syndromes– Phantom Limb– Agnosia & Apraxia– Subcortical Motor Disorders– Neurogenic Diseases of Motor Unit

Spinal Cord Syndromes
Ref. 2. Ch 4 p. 173
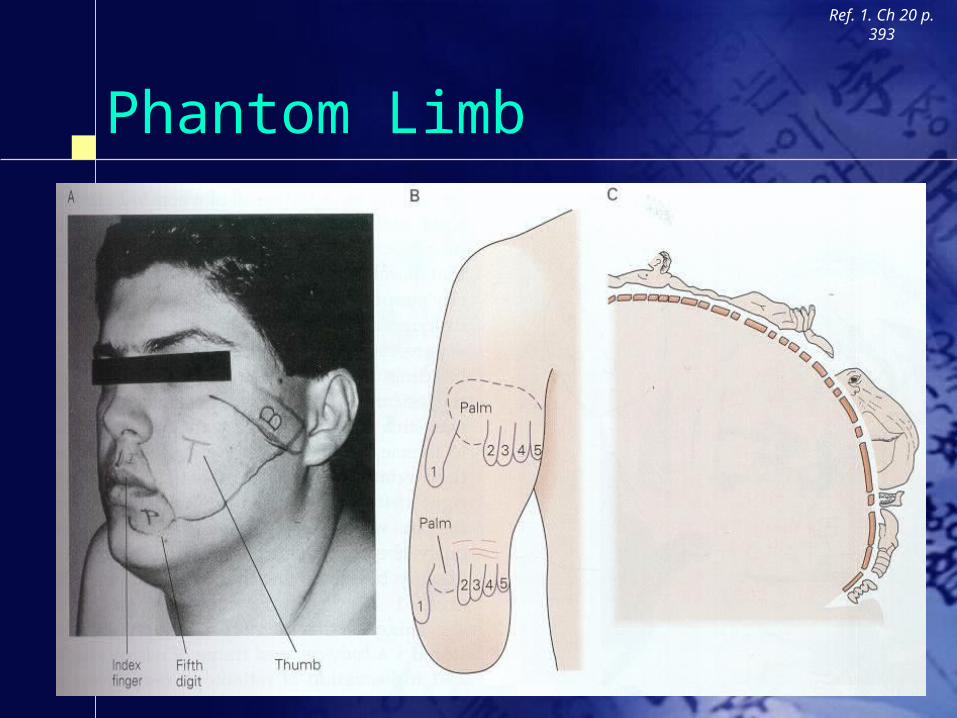
Phantom Limb
Ref. 1. Ch 20 p. 393

MEG of Amputee
Ref. 6. Ch 2 p. 32 & Ref. 7. p. 1610
Agnosia
The Inability to perceive or identify a stimulus by means of a particular sensory modality, even though its details can be detected by means of that modality and the person retains relatively normal intellectual capacity– Apperceptive visual agnosia
People with apperceptive visual agnosia may have normal visual acuity, but they cannot successfully recognize objects visually by their shape.
Prosopagnosia (Prosopon means “face”)– Associative visual agnosia
People with associative visual agnosia appear to be able to perceive normally but cannot name what they have seen.

Example of Agnosia
Ref. 1. Ch 62 p. 1235

Apraxia
The inability to properly execute a learned skilled movement– Limb apraxia– Constructional apraxia– Oral apraxia– Apraxic agraphia
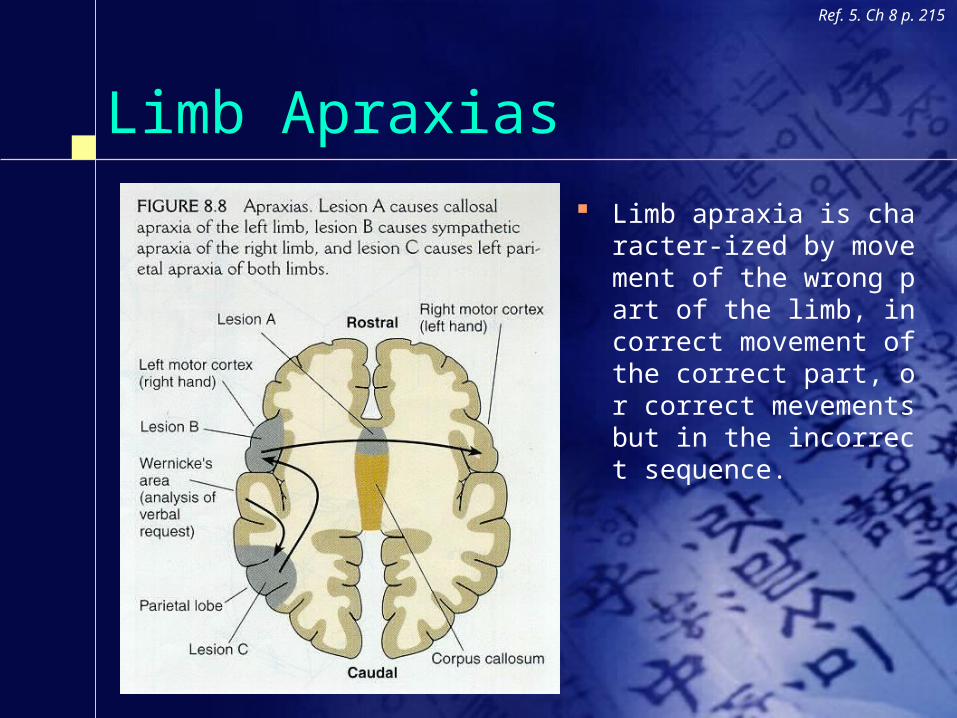
Limb Apraxias Limb apraxia is character-i
zed by movement of the wrong part of the limb, incorrect movement of the correct part, or correct mevements but in the incorrect sequence.
Ref. 5. Ch 8 p. 215
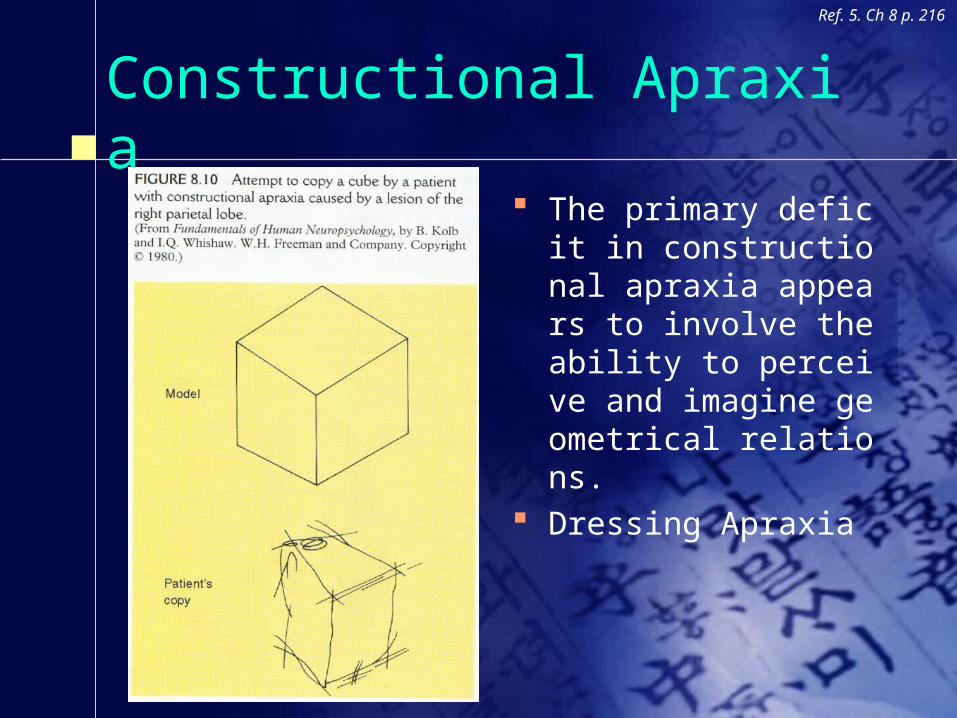
Constructional Apraxia The primary deficit in c
onstructional apraxia appears to involve the ability to perceive and imagine geometrical relations.
Dressing Apraxia
Ref. 5. Ch 8 p. 216

Balint’s syndrome
Balint’s syndrome occurs in people with bilateral damage to posterior parietal and prestriate cortex.
Balint’s syndrome consists of three major symptoms.– Optic ataxia (ataxia comes from the Greek word for “disorderly”)
A person with BS might be able to perceive and recognize a particular object, but when he or she tries to reach for it, the movement is often misdirected.
– Ocular apraxia (“without visual action”) If an object moves, or if a light flashes, the person with BS may report se
eing something but will not be able to make an eye movement that directs the gaze toward the target.
– Simultanagnosia If the gaze of a person with BS happens to fall on an object, he or she wil
l perceive it. But only one object will be perceived at a time.
Ref. 5. Ch 6 p. 163

Hemineglect
Ref. 1. Ch 20 p. 394-396

Parkinson’s Disease
Ref. 1. Ch 43 p. 860

Huntington’s DiseaseRef. 1. Ch 43 p.
860

Diseases of the Motor Unit
Ref. 1. Ch 35 p. 697
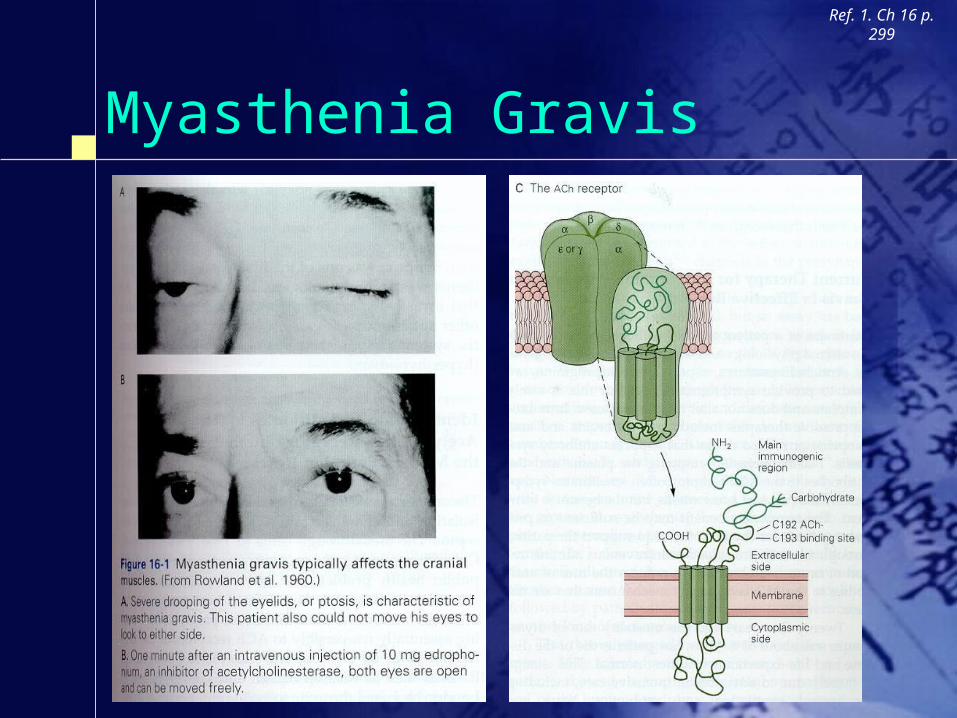
Myasthenia Gravis
Ref. 1. Ch 16 p. 299

References1. Eric R. Kandel, James H. Schwartz, Thomas M. Jessell (2000) Principles of Neural Science, 4th ed. New York, NY: McGraw-Hill
2. Richard S. Snell (2001) Clinical neuroanatomy for medical students, 5th ed. Baltimore, MD: Lippincott Williams & Wilkins
3. Diani W. Molavi (1997) Neuroscience tutorial Retrieved from WWW April 19, 2003. http://thalamus.wustl.edu/course/
4. Marie T. Banich (1997) Neuropsychology Boston, MA: Houghton Miffin
5. Neil R. Carson (1995) Foundations of physiological psychology, 3rd ed. Needham, MA: Allyn & Bacon
6. V.S. Ramachandran, Sandra Blakeslee (1998) Phantoms in the brain New York, NY: HarperCollins
7. Ramachandran VS, Hirstein W. (1998) The perception of phantom limbs. The D. O. Hebb lecture Brain, 121, 1603-1630