son espases hospital experience - sborl...
TRANSCRIPT

OlfactoryOlfactory Dysfunction & Dysfunction & Neurological Disorders Neurological Disorders
Son Espases Hospital Experience Son Espases Hospital Experience
Fernanda A MuFernanda A Muññoz Protooz Proto
ENT Resident ENT Resident
20152015

Introduction
““Olfactory dysfunction is a common and early symptom of many Olfactory dysfunction is a common and early symptom of many neurodegenerative diseases, particularly of Parkinson's disease neurodegenerative diseases, particularly of Parkinson's disease
Alzheimer's disease (AD), and mild cognitive impairment Alzheimer's disease (AD), and mild cognitive impairment heralding its progression to dementiaheralding its progression to dementia””

The aim of the study The aim of the study
To describe:
Prevalence
Spectrum of neurological diseases
Patients that consulted for loss of smell
Clinical findings
Risk factors

Materials and Methods
Retrospective study
All olfatometry between 2008 and 2015
Barcelona Smell Test-24 BAST-24

Barcelona Smell Test - 24 (BAST-24)

Materials and Methods

Materials and Methods

ResultsResults
From 2008 to 2015: 497 olfatometry
Mean age: 53 years
Mean age: 60 years

ResultsResults

ResultsResults

Summary of CasesSummary of Cases
Table 1. Summary of Results. Epidemiological results (Sex: 1:Male, 2: Female) , age, Olfactometry results, Smoke, Department of first visit, Neurological diagnosis, comorbilities. HT: Hypertension, HLP: Hyperlipidemia, DM: Diabetes Mellitus, BPH: Benign Prostatic Hyperplasia, MI: Myocardial infarction, OSA: Obstructive Sleep Apnea, OP: Osteoporosis, AR: Alergic Rhinitis.

Neurological Diagnosis

Cognitive Impairment and Cognitive Impairment and DementiaDementia

Cognitive Impairment and Cognitive Impairment and DementiaDementia
65% (15) 65% (15)
Diagnosis:Diagnosis:Cognitive Impairment 13
Mild amnesic cognitive impairment / incipient AD: 2: 2
Mild amnesic cognitive impairment 11
Mild cognitive impairment: 5: 5
Mild no-amnesic cognitive impairment 55
Vascular Mild cognitive impairment 11
Prodromic Alzheimer Disease: 1

Olfactory DysfunctionOlfactory DysfunctionCognitive Impairment/ DementiaCognitive Impairment/ Dementia
OlfactometryOlfactometry ResultsResults

Olfactory Olfactory DysfuctionDysfuction & Stroke& Stroke
Sex Age Det I Iden I Det V Iden V Smoke 1st visit Diagnosis Comorbidities
2 67 40 5 100 0 ? NRL
Stroke, Mild no-amnesic cognitive
impairment
HLP, HT, DM, 3 Strokes
1 44 85 20 100 0 NO NRL Stroke HT, MI
1 70 0 0 50 0 ? NRL StrokeHT, HLP,
Cerebrovascular disease
1 61 100 25 100 0 NO NRL Stroke
HLP, DM, Cerebrovascular
disease, Auricular Flutter

Olfactometry Results: StrokeOlfactometry Results: Stroke

ComorbiditiesComorbidities
Dyslipidemia 43%
Hypertension 29%
Cerebrovascular disease: 29%
Acute myocardial infarction: 2 patients
Depression: 38%

Olfactory Dysfunction & Depression
Case Gender Age Diagnosis Comorbidities
1 2 86 Mild amnesic cognitive impairment / incipient AD HT, Depression, Glaucoma
3 2 58 Mild no-amnesic cognitive impairment HLP, Depression, Hyperthyrodism, GERD
4 2 62 Mild amnesic cognitive impairment / incipient AD Depression, Hypothyroid, Fibromyalgia, Parotid carcinoma
5 2 65 Mild cognitive impairment HLP, Depression, MI
7 1 64 Tremor (Incipient Parkinson) HLP, Depression,
8 2 61 Vascular Mild cognitive impairment Cerebrovascular disease, Depression
12 2 68 Mild no-amnesic cognitive impairment HLP, HT, OP, OSA, Fibromyalgia, Depression
16 1 55 Compressive cervical myelopathy, Hydrocephalus Depression
21 2 49 Mild cognitive impairment Cerebrovascular disease, Depression, Migraine, Alergic Rhinitis
Table 2. Summary of Results of patients diagnosed of depression and neurological disorder. Epidemiological results (Sex: 1:Male, 2: Female), age, neurological diagnosis, comorbidities HT: Hypertension, HLP: Hyperlipidemia, DM: Diabetes Mellitus, BPH: Benign Prostatic Hyperplasia, MI: Myocardial infarction, OSA: Obstructive Sleep Apnea, OP: Osteoporosis

Magnetic Resonance Magnetic Resonance
MRI study in 19/21 patients
Pathologic result: 16
Normal: 3
Finding:
4 cases of stoke: encefalomalacia in the 4 cases
Cortical atrophy in 9/16 cases
Microangiopathy lesions in 7/16
Hypoplastic olfactory tracts in in 3/16
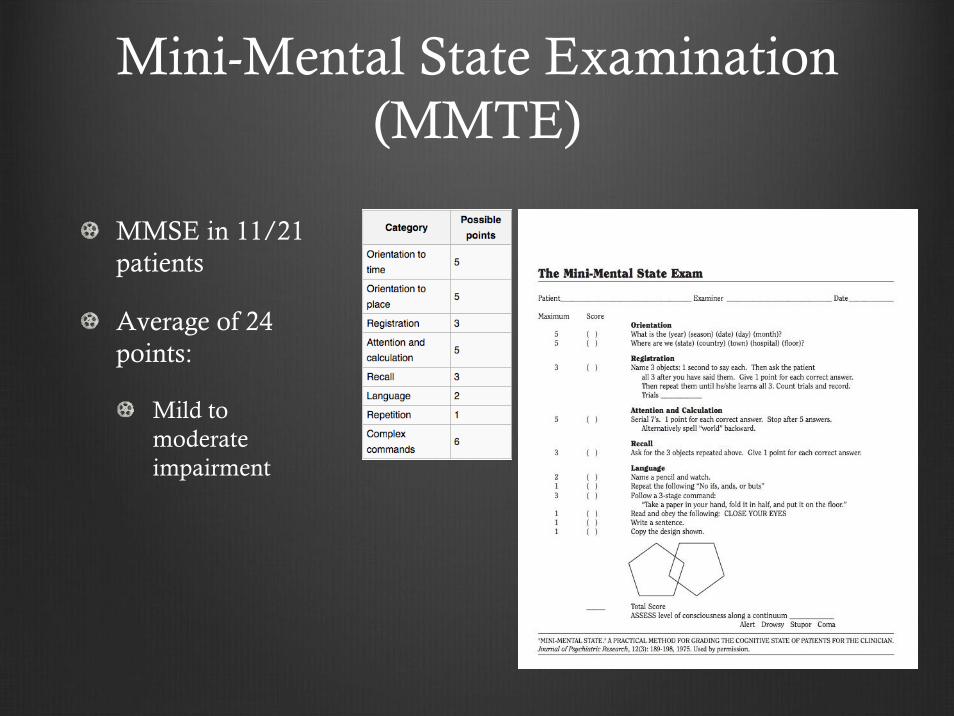
Mini-Mental State Examination (MMTE)
MMSE in 11/21 patients
Average of 24 points:
Mild to moderate impairment
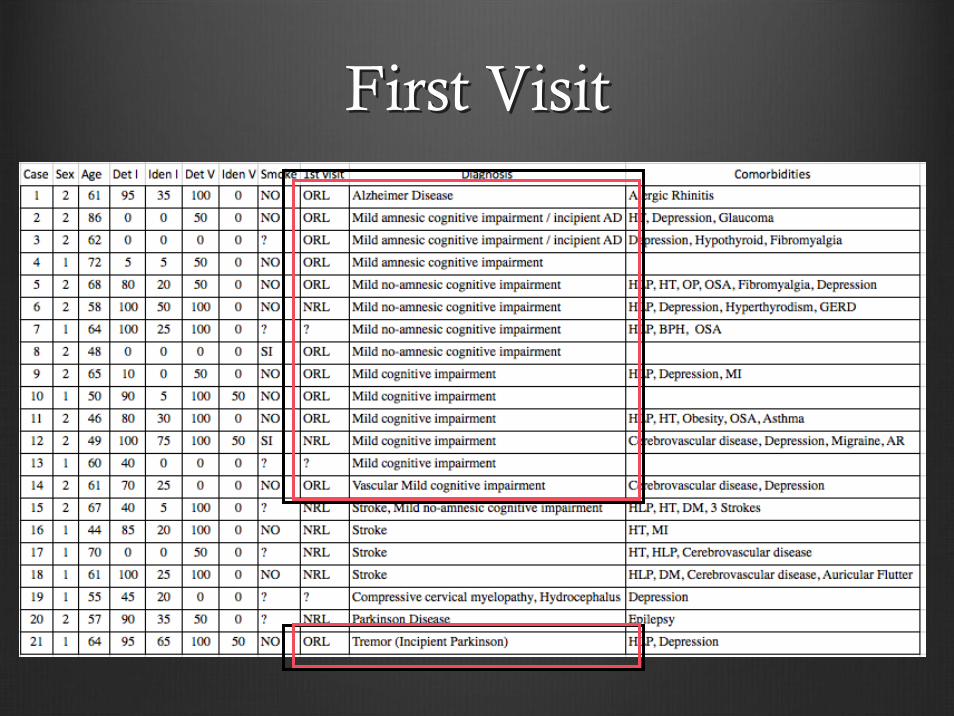
First Visit First Visit

DiscussionDiscussion

Mild cognitive impairment (MCI)Mild cognitive impairment (MCI)
Intermediate stage between the expected cognitive decline of Intermediate stage between the expected cognitive decline of normal aging and dementianormal aging and dementia
1010--15 % of MCI went on to develop dementia in each year that the 15 % of MCI went on to develop dementia in each year that the research results were followed up. research results were followed up.
Actually research has focused on identifying people with MCI whoActually research has focused on identifying people with MCI whowill go on to develop dementiawill go on to develop dementia
Patients could be offered a range of support at an early stage iPatients could be offered a range of support at an early stage in the n the illnessillness
Alzheimer Society. Mild cognitive impairment (MCI). Dr Alexander Kurz, Department of Psychiatry and Psychotherapy, Technische Universität München, Munich, and Dr Basil Ridha, Institute of Neurology, University College London

Systematic review.
Increased risk of later onset of AD in subjects with baseline hyposmia
Possible relationship between decreased olfaction in participants with MCI and conversion to AD but was inconclusive due to low follow-up rates.

AD is Incresing in prevalence AD is Incresing in prevalence
• The number of people with Alzheimer’s disease (AD) doubles for every 5-year interval past age 65
• Only 1-in-4 people with Alzheimer’s disease have been diagnosed.
• Alzheimer’s and dementia is most common in Western Europe.

The neuropathologic changes of olfactory dysfunction in neurodegenerative diseases may involve:•The olfactory epithelium•Olfactory bulb/tract•Primary olfactory cortices and their secondary targets.
Olfactory dysfunction is related to deposition of pathological proteins:α-synuclein, hyperphosphorylated tau protein neurofilament protein featured by neurofibrillary tangles, Lewy bodies and neurites
Inducing a complex cascade of molecular processes including oxidative damage, neuroinflammation, and cytosolic disruption of cellular processes
Leading to cell death

Recent studies of olfactory dysfunction have focused its potentiRecent studies of olfactory dysfunction have focused its potential as al as an an early biomarker for the diagnosis early biomarker for the diagnosis of neurodegenerative disorders of neurodegenerative disorders and their disease progression. and their disease progression.
We also present neuropathological findings in the olfactory bulbWe also present neuropathological findings in the olfactory bulband tract in a large autopsy cohort (n = 536, 57.8 % female, meaand tract in a large autopsy cohort (n = 536, 57.8 % female, mean n age 81.3 years). age 81.3 years). The severity of olfactory bulb HPThe severity of olfactory bulb HPττ, A, Aββ, and , and ααSynuclein pathology correlated and increased significantly Synuclein pathology correlated and increased significantly (P < (P < 0.001) with increasing neuritic Braak stages, Thal A0.001) with increasing neuritic Braak stages, Thal Aββ phases, and phases, and cerebral Lewy body pathology, respectively. cerebral Lewy body pathology, respectively.

• Longitudinal study: MCI outpatients, CA-SIT Smell Identification • 88 MCI v/s 46 healthy control patients
MCI subjects have been divided into two groups,• 40% MCI olfactory-normal• 60% MCI olfactory-impaired
At 2-year follow-up, the 47% of MCI olfactory-impaired subjects and the 11% of MCI olfactory-normal subjects progressed to dementia.
In a logistic regression model,• Lower score in MMSE (95%; p = .004) • Pathological smell identification at baseline (95%, p = .03) were independently associated with the progression to dementia within 2 years.

Neurodegenerative conditions with dementia have particular difficulties with the recognition and identification of odours rather than the detection, suggesting a link to impairment of higher cognitive function.
Olfactory impairment has been shown to be predictive of conversion from mild cognitive impairment to Alzheimer's disease with 85.2% sensitivity.
Sensory considerations are likely to play a greater role in dementia care in the future, with the development of purpose-built dementia care facilities and the focus on non-pharmacological management strategies

• Olfactory deficits precede clinical onset of cognitive and memory deficits and coincide with AD pathology preferentially in the central olfactory structures, suggesting a potential biomarker for AD early detection and progression.
RESULTS:• Prominent atrophy in the primary olfactory cortex (POC) and hippocampus was found in
both AD and MCI subjects.
CONCLUSIONS:• Decline in olfactory activity was correlated with the AD structural degeneration in the
POC.
• Olfactory fMRI may thus provide an earlier and more sensitive measure of functional neurodegeneration in AD and MCI patients.

ParkinsonParkinson

Parkinson Disease (PD) & Olfactory Parkinson Disease (PD) & Olfactory dysfuction (OD)dysfuction (OD)
1975 First report on olfactory dysfunction in Parkinson’s disease
The most common of neurodegenerative disorders manifesting hiposmia.
The prevalence of OD in PD ranges from 45% to 90%
Some authors argue that the diagnosis of PD should be reconsidered in patients with normal olfaction

Studies have revealed a reduced sense of smell in some individuals many years before they develop the classical motor signs of PD.
This implies that olfactory testing could be used as a preclinical marker
This finding is in line with an earlier TRODAT SPECT study which revealed that olfactory involvement occurs early in the disease process
Parkinson Disease (PD) & Olfactory Parkinson Disease (PD) & Olfactory dysfunction (OD)

• Hyposmia (typical non-motor features of PD)
• Volumetric magnetic resonance demonstrated close relationships between olfactory dysfunction and atrophy of amygdala and other limbic structures.
• Brain regions related to olfactory function are closely associated with cognitive decline
• Severe hyposmia is a prominent clinical feature that predicts the subsequent development of PDD. 18.7-fold increase in their risk of dementia
• Started a randomized, double-blind study using donepezil for the PD group with severe hyposmia.

How can we explain a relationship between depression and dementia?

Depression & Dementia

Depression may increase dementia risk, with a pooled estimate of1.97 (95% CI: 1.67-2.23).
It still does not distinguish between depression is a prodrome of dementia, or an independent causal risk factor.
There is a trend towards smaller effect sizes in studies with longer follow-up, which would be consistent with expectations if depression were part of the prodrome of dementia
Depression & Dementia

Conclusions Conclusions
OD is a common and early symptom of many neurodegenerative diseases, particularly of Parkinson’s, Alzheimer's disease (AD), and mild cognitive impairment heralding its progression to dementia.
OD is a predictive of conversion from MCI to AD with hifg sensitivity.
In AD, the deposition of pathological proteinsinvolve: olfactoryepithelium, olfactory bulb/tract, primary olfactory cortices andtheir secondary targets.

ConclusionsConclusions
OD in PD is a common finding and seems to be an early sign of PD and a predictive feature of Parkinson's disease with dementia (PDD)
Olfactory dysfunction and atrophy of amygdala and other limbic structures shows that severe hyposmia is a prominent clinical feature that predicts PDD.
It still does not distinguish clearly whether depression is a prodrome of dementia, or an independent causal risk factor.

ReferencesReferences
Behrman S1, Chouliaras L1, Ebmeier KP2. Considering the senses in the diagnosis and management of dementia. Maturitas. 2014 Apr;77(4):305-10. doi: 10.1016/j.maturitas.2014.01.003. Epub 2014 Jan 18.
Attems J1, Walker L, Jellinger KA. Olfactory bulb involvement in neurodegenerative diseases. Acta Neuropathol. 2014 Apr;127(4):459-75. doi: 10.1007/s00401-014-1261-7. Epub 2014 Feb 20.
Sun GH1, Raji CA, Maceachern MP, Burke JF. Olfactory identification testing as a predictor of the development of Alzheimer's dementia: a systematic review. Laryngoscope. 2012 Jul;122(7):1455-62. doi: 10.1002/lary.23365. Epub 2012 May 2.
Alda Cardesin1, Isam Alobid1,2, Pedro Benitez4, Erika Sierra2, Josep de Haro4, Manuel Bernal-Sprekelsen1, Cesar Picado3, Joaquim Mullol1,2. Barcelona Smell Test - 24 (BAST-24): validation and smell characteristics in the healthy Spanish population*. Rhinology, 44, 83-89, 2006
Jennifer J. Stamps a,�, Linda M. Bartoshuk b, Kenneth M. Heilman c . A brief olfactory test for Alzheimer's disease. Journal of the Neurological Sciences 333 (2013) 19–24
K. K. Johansen1,2, B. J. Warø2, J. O. Aasly1,2. Olfactory dysfunction in sporadic Parkinson’s Disease and LRRK2 carriers. Acta Neurol Scand 2014: 129: 300–306 DOI: 10.1111/ane.12172
Graves AB, Bowen JD, Rajaram L, McCormick WC, McCurry SM, Schellenberg GD, et al. Impaired olfaction as a marker for cognitive decline: interaction with apolipoprotein E epsilon4 status. Neurology Oct 1999;53(7):1480–7.
Tabert MH, Liu X, Doty RL, Serby M, Zamora D, Pelton GH, et al. A 10-item smell iden- tification scale related to risk for Alzheimer's disease. Ann Neurol Jul 2005;58(1): 155–60.

ReferencesReferences
Hidalgo1,3, G. Chopard1,3,4, J. Galmiche3,4, L. Jacquot1, G. Brand1,2. Just noticeable difference in olfaction: a discrimi- native tool between healthy elderly and patients with cognitive disorders associated with dementia*. Rhinology 49: 513-518, 2011
VasavadaVasavada MM1, Wang J1, MM1, Wang J1, EslingerEslinger PJ2, Gill DJ3, Sun X1, PJ2, Gill DJ3, Sun X1, KarunanayakaKarunanayaka P1, Yang QX4. Olfactory cortex degeneration in P1, Yang QX4. Olfactory cortex degeneration in Alzheimer's disease and mild cognitive impairment. J Alzheimer's disease and mild cognitive impairment. J AlzheimersAlzheimers Dis. 2015 Jan 1;45(3):947Dis. 2015 Jan 1;45(3):947--58. 58.
VyhnalekVyhnalek M1, M1, MagerovaMagerova H2, H2, AndelAndel R3, Nikolai T4, R3, Nikolai T4, KadlecovaKadlecova A4, A4, LaczoLaczo J4, J4, HortHort J4.Olfactory identification in J4.Olfactory identification in amnesticamnestic and nonand non--amnesticamnestic mild cognitive impairment and its neuropsychological correlatesmild cognitive impairment and its neuropsychological correlates. J . J NeurolNeurol Sci. 2015 Feb 15;349(1Sci. 2015 Feb 15;349(1--2):1792):179--84. 84.
VelayudhanVelayudhan L1. Smell identification function and Alzheimer's disease: a seL1. Smell identification function and Alzheimer's disease: a selective review. lective review. CurrCurr OpinOpin Psychiatry. 2015 Mar;28(2):173Psychiatry. 2015 Mar;28(2):173--9. 9.
Conti MZ1, Conti MZ1, ViciniVicini--ChiloviChilovi B, Riva M, B, Riva M, ZanettiZanetti M, M, LiberiniLiberini P, P, PadovaniPadovani A, A, RozziniRozzini L. Odor identification deficit predicts clinical L. Odor identification deficit predicts clinical conversion from mild cognitive impairment to dementia due to Alzconversion from mild cognitive impairment to dementia due to Alzheimer's disease. Arch heimer's disease. Arch ClinClin NeuropsycholNeuropsychol. 2013 Aug;28(5):391. 2013 Aug;28(5):391--9. 9.
Carmichael ST, Clugnet MC, Price JL. Central olfactory connections in the macaque monkey. J Comp Neurol Aug 1994;346(3):403–34.
Ferreyra-Moyano H, Barragan E. The olfactory system and Alzheimer's disease. Int J Neurosci Dec 1989;49(3–4):157–97.
[Price JL, Davis PB, Morris JC, White DL. The distribution of tangles, plaques and re- lated immunohistochemical markers in healthy aging and Alzheimer's disease. Neurobiol Aging Jul–Aug 1991;12(4):295–312.