sonographic evaluation
TRANSCRIPT
Sonographic Evaluation ofVascular Injuries
Diana Gaitini, MD, Nira Beck Razi, MD, Eduard Ghersin, MD,Amos Ofer, MD, Michalle Soudack, MD
Objective. The purpose of this presentation is to highlight the color Doppler duplex sonographicfeatures of procedure-related and blunt or penetrating trauma-related vascular injuries. Methods.Different kinds of vascular complications such as pseudoaneurysms, arteriovenous fistulas, dissection,and thrombosis are discussed. Cases of vascular injuries in the extremities, neck, and abdomen are pre-sented to illustrate the spectrum of sonographic appearances. Results. Color Doppler duplex sonog-raphy is valuable in the diagnosis and monitoring of most vessel injuries and in the treatment ofpseudoaneurysms. It is useful for flow analysis and for follow-up after treatment. However, because oflimitations inherent to sonography, such as bones, air, casts, skin burns, and relatively slow perfor-mance of the test, magnetic resonance imaging, computed tomography, and angiography are neces-sary for further evaluation in selected cases. Conclusions. Color Doppler duplex sonography is a widelyavailable, noninvasive, and accurate technique for evaluating vascular injuries and should be the first-line imaging modality in most patients. Key words: arteriovenous fistula; diagnosis; false aneurysm;sonography; vascular injuries.
Received June 21, 2007, from the Department ofMedical Imaging, Rambam Medical Center, Haifa,Israel. Revision requested July 18, 2007. Revisedmanuscript accepted for publication August 1, 2007.
Address correspondence to Diana Gaitini, MD,Unit of Ultrasound, Department of Medical Imaging,Rambam Medical Center, Ha’aliya 8, PO Box 9602,31096 Haifa, Israel.
E-mail: [email protected]
AbbreviationsAVF, arteriovenous fistula; CDDS, color Doppler duplexsonography; CTA, computed tomographic angiography;DSA, digital subtraction angiography. MRA, magneticresonance angiography
he prevalence of vessel injuries is on the risebecause of increasing rates of invasive proceduresand traumatic events. At a level I trauma center,iatrogenic injuries were the causes of one third of
arterial damage.1 The complication rate in complex coro-nary procedures reaches 6%. Fibrinolytic therapy, antico-agulants, large-diameter vascular sheaths, and poorpuncture or compression techniques increase the rate ofvascular complications.2 Partial or complete thrombosis,intimal flaps, dissection, arteriovenous fistulas (AVFs), andpseudoaneurysms are the main vascular complications.
The neck, extremities, and abdominal organs areanatomic sites amenable to investigation with colorDoppler duplex sonography (CDDS). Subcutaneous air,large hematomas, casts, and large skin wounds mayimpede CDDS performance. Aberrant vessels andanatomic areas difficult to scan, such as the thoracic inletand the pelvis, lessen the accuracy of CDDS. Further lim-itations are derived from operator dependence andlengthy examinations, which may be inappropriate in theacute care setting.3 Despite these limitations, CDDS is
© 2008 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 2008; 27:95–107 • 0278-4297/08/$3.50
T
Image Presentation

presently considered the first-line examinationfor evaluation of vascular injuries, withreported sensitivity of 95% to 97% and accu-racy of 95% to 98%.3–5 Magnetic resonanceangiography (MRA) and computed tomo-graphic angiography (CTA) are useful comple-mentary examinations. Digital subtractionangiography (DSA) is shifting to a more thera-peutic role for endovascular management.
Procedure-Related Vascular Injuries
Vascular injuries may follow percutaneous pro-cedures. Puncture site vascular injuries includeperivascular hematomas, pseudoaneurysms,and AVFs. A perivascular hematoma is the mostfrequent complication at the puncture site.Clinically, it is a nonpulsatile focal swelling withecchymosed skin. It appears as a complex solidand cystic soft tissue mass adjacent to the injuredvessel, without blood flow on Doppler interroga-tion (Figure 1). A diffuse hematoma, even obvi-ous clinically, may be unrecognizable on CDDSbecause of poorly defined infiltration of bloodinto the soft tissues. An AVF is a false vascularchannel between an artery and the adjacent vein.A palpable thrill and a bruit on auscultation areoften present. Color Doppler duplex sonographyshows a mosaic color pattern due to high turbu-lent flow in the fistula, low-resistance arterial flowin the feeding artery, and a high-velocity, chaotic
waveform in the draining vein. Extravascularcolor signals represent perivascular tissue vibra-tion due to transmitted pulsation of turbulentcontinuous blood flow between the artery andthe vein (Figure 2). A pseudoaneurysm or falseaneurysm is a pulsatile hematoma that commu-nicates through a channel (neck) with the injuredartery. It follows total disruption in the arterialwall and continuous extravascular flow, con-tained by the surrounding tissues. It complicates0.1% to 0.2% of diagnostic and 3.5% to 5.5% ofinterventional procedures, representing morethan 60% of interventional vascular complica-tions.6 Clinically, a pulsatile mass with a palpablethrill and an audible to-and-fro murmur isdetected. Color Doppler duplex sonography isthe diagnostic imaging modality of choice: it candelineate the cavity, the degree of clotting, thecommunication with the artery, and the bloodflow pattern. The lumen has bidirectional,swirling, or “yin-yang” color flow and turbulent orpulsatile flow on a spectral display. The neck typi-cally has a to-and-fro waveform due to flow enter-ing during systole and exiting during diastole(Figure 3). Pseudoaneurysms vary in size and mayhave multiple compartments (Figure 4). A fluid-fluid level due to hematocrit layering may be seenin large pseudoaneurysms (Figure 5). They mayinvolve surgical sites, most often bypass graftanastomosis (Figure 6). Sonographically guidedthrombin injection is the treatment of choicefor large pseudoaneurysms that do not clotspontaneously, converting them into thrombosedhematomas within seconds, with a 93% to 100%success rate.7,8 A flow void after injection confirmsthrombosis (Figure 7). The neck width of the pseu-doaneurysm is of prognostic value because a wideand short neck may carry a higher risk of failureand embolic complications during thrombininjection. Hypoechoic hypervascular lymphnodes, dilated varicose veins with slow swirlingflow (Figure 8), and fluid containing femoral oringuinal hernias, with fluid movement due to res-piratory motion, may mimic pseudoaneurysms.
Procedures such as angioplasty, thrombolysis,and stent placement may be complicated bythrombosis, intimal flaps, aneurysms, arterialruptures, and stent stenosis. Arterial thrombosisis the most frequent complication. Varyingdegrees of thrombus echogenicity may be
96 J Ultrasound Med 2008; 27:95–107
Sonographic Evaluation of Vascular Injuries
Figure 1. Image from a 70-year-old man with groin swellingafter femoral catheterization. Color Doppler sonography showsa large hypoechoic heterogeneous mass (arrow) surrounding thefemoral artery (fa) at the proximal thigh, consistent with ahematoma.
J Ultrasound Med 2008; 27:95–107 97
Gaitini et al
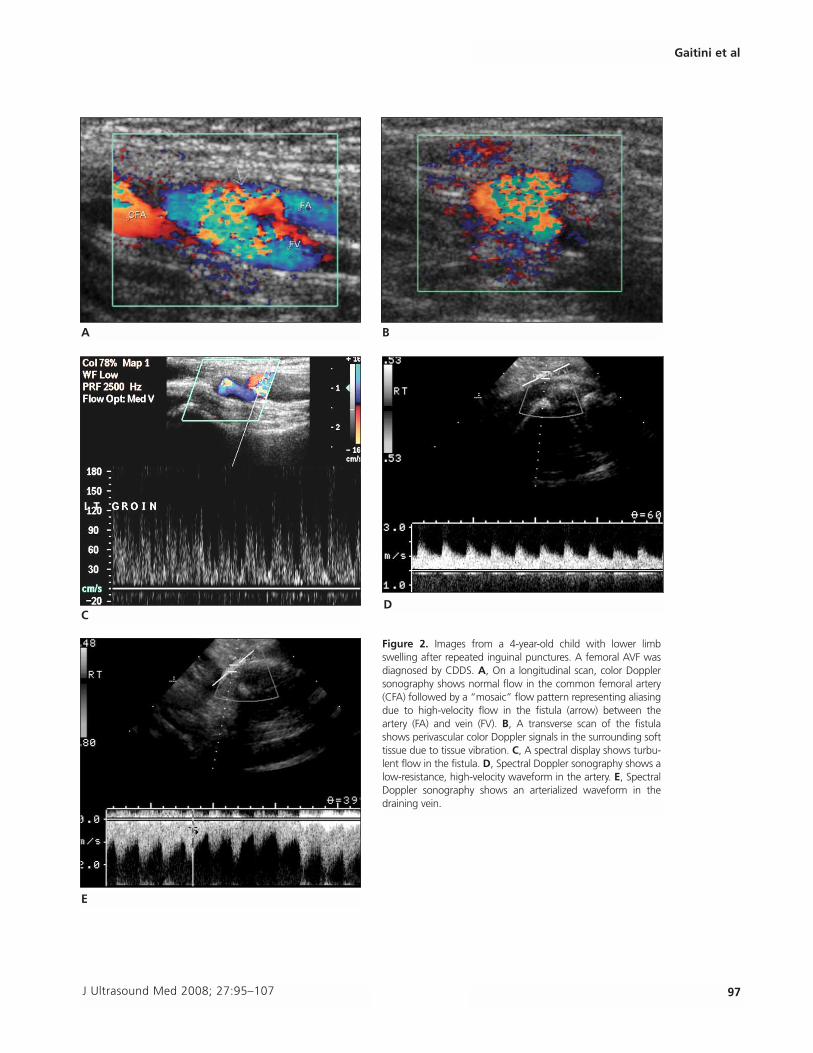
Figure 2. Images from a 4-year-old child with lower limbswelling after repeated inguinal punctures. A femoral AVF wasdiagnosed by CDDS. A, On a longitudinal scan, color Dopplersonography shows normal flow in the common femoral artery(CFA) followed by a “mosaic” flow pattern representing aliasingdue to high-velocity flow in the fistula (arrow) between theartery (FA) and vein (FV). B, A transverse scan of the fistulashows perivascular color Doppler signals in the surrounding softtissue due to tissue vibration. C, A spectral display shows turbu-lent flow in the fistula. D, Spectral Doppler sonography shows alow-resistance, high-velocity waveform in the artery. E, SpectralDoppler sonography shows an arterialized waveform in thedraining vein.
A B
C
E
D
detected depending on the thrombus age. A par-tially occluding thrombus causes alteration inthe color flow pattern, waveform, and velocities(Figure 9). A totally occluding thrombus causesan abrupt cutoff of color flow and retrograde flowin a collateral pathway. A vasospasm and exter-nal compression without evidence of an intrinsic
vessel injury may be correctly diagnosed byCDDS. Focal dissection resulting from guideinsertion may be seen in a severely atherosclerot-ic artery (Figure 10). Color Doppler duplexsonography, at times in combination with MRAand CTA, can noninvasively show most arterialinjuries.9 Vein thrombosis may complicate
98 J Ultrasound Med 2008; 27:95–107
Sonographic Evaluation of Vascular Injuries
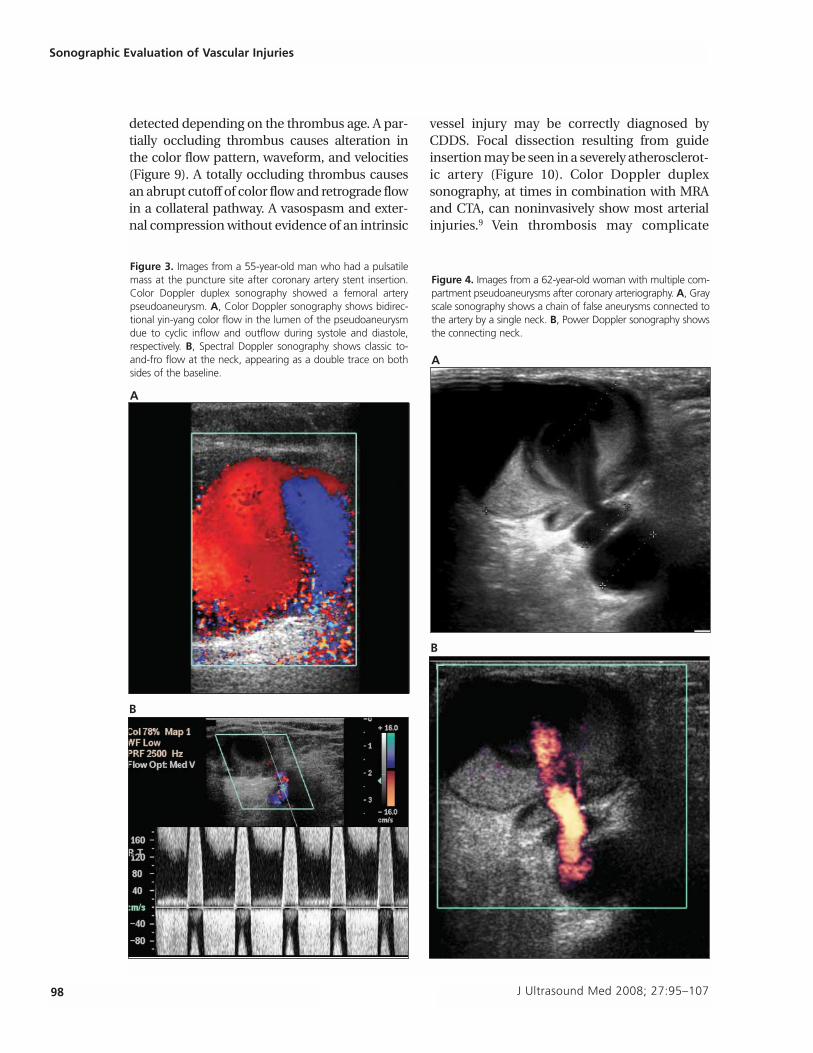
Figure 3. Images from a 55-year-old man who had a pulsatilemass at the puncture site after coronary artery stent insertion.Color Doppler duplex sonography showed a femoral arterypseudoaneurysm. A, Color Doppler sonography shows bidirec-tional yin-yang color flow in the lumen of the pseudoaneurysmdue to cyclic inflow and outflow during systole and diastole,respectively. B, Spectral Doppler sonography shows classic to-and-fro flow at the neck, appearing as a double trace on bothsides of the baseline.
A
B
Figure 4. Images from a 62-year-old woman with multiple com-partment pseudoaneurysms after coronary arteriography. A, Grayscale sonography shows a chain of false aneurysms connected tothe artery by a single neck. B, Power Doppler sonography showsthe connecting neck.
A
B
indwelling catheters, inferior vena cava filters,and venous stents and shunts. Thrombosedveins are typically noncompressible (Figure 11).When a thrombus is suspected in a central veinsuch as the brachiocephalic vein or the superi-or vena cava, both sides should be examined:bilateral dampening of the spectral waveform,converting the normal biphasic pattern into anonpulsatile pattern, indicates superior venacava thrombosis, whereas unilateral dampeningis a sign of ipsilateral brachiocephalic thrombo-sis.10 Complications of transjugular intrahepaticportosystemic shunts may occur early becauseof stent dislodgement and hemorrhage or latebecause of stenosis and occlusion.
Percutaneous nonvascular procedures such askidney and liver biopsies may cause vascularinjuries. Active hemorrhage may be detected dur-ing real-time examination as a jet from the biopsytract to the organ capsule. Pseudoaneurysms andAVFs (Figure 12), more common complications,may be detected in up to 10% to 15% of trans-plant kidney biopsies, and large AVFs may causerenal dysfunction.11
J Ultrasound Med 2008; 27:95–107 99
Gaitini et al
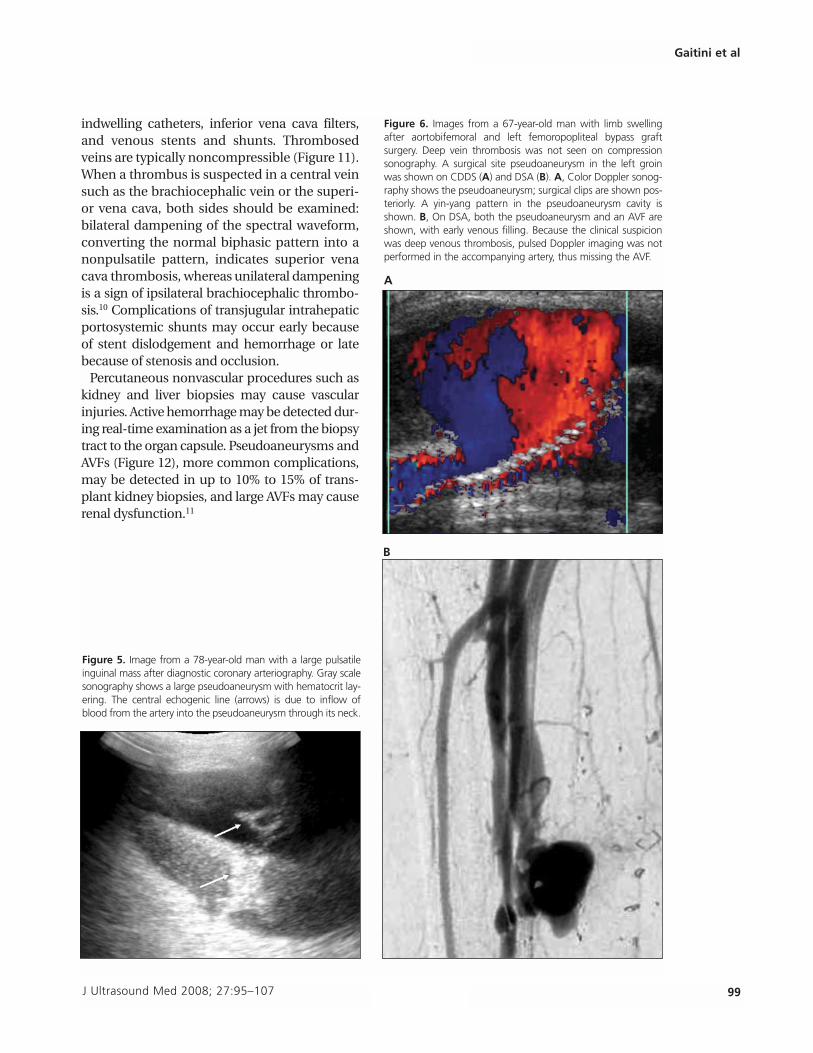
Figure 6. Images from a 67-year-old man with limb swellingafter aortobifemoral and left femoropopliteal bypass graftsurgery. Deep vein thrombosis was not seen on compressionsonography. A surgical site pseudoaneurysm in the left groinwas shown on CDDS (A) and DSA (B). A, Color Doppler sonog-raphy shows the pseudoaneurysm; surgical clips are shown pos-teriorly. A yin-yang pattern in the pseudoaneurysm cavity isshown. B, On DSA, both the pseudoaneurysm and an AVF areshown, with early venous filling. Because the clinical suspicionwas deep venous thrombosis, pulsed Doppler imaging was notperformed in the accompanying artery, thus missing the AVF.
A
B
Figure 5. Image from a 78-year-old man with a large pulsatileinguinal mass after diagnostic coronary arteriography. Gray scalesonography shows a large pseudoaneurysm with hematocrit lay-ering. The central echogenic line (arrows) is due to inflow ofblood from the artery into the pseudoaneurysm through its neck.
Trauma-Related Vascular Injuries
Vascular injuries following blunt or penetratingtrauma are illustrated according to different bodylevels accessible to CDDS: the neck, extremities,and abdomen. Penetrating neck trauma leads tovascular injuries in 25% of casualties. Carotidartery injuries constitute 80% of penetratingtrauma incidents, whereas vertebral arteryinjuries are more common in blunt trauma.12,13
Thrombosis is the most common injury. Otherinjuries include mild intimal irregularities, inti-mal flaps, pseudoaneurysms, and AVFs (Figure13).14–16 Although CDDS was sensitive in evalua-tion of stable patients with neck zone II penetrat-ing injuries (Figure 14)17,18 and accuratelyshowed arterial injuries in 86% of examina-tions,16 CTA with multiplanar reformation is thefirst-line examination.19 Magnetic resonanceangiography in the acute setting is restrictedbecause of limited availability and lack of com-patibility with life support devices.20,21 In limbartery injuries, CDDS is less sensitive than arteri-ography for detection of small intimal defects orsmall-vessel occlusions but is successful indetecting more substantial lesions such as pseu-doaneurysms, AVFs, and major vessel occlusions(Figure 15), with reported specificity of 99%, sen-sitivity of 50%, and accuracy of 96% comparedwith arteriography.3,22,23 Blunt or penetratingabdominal trauma may result in visceral pseu-doaneurysms and AVFs, which are increasinglydetected because of the widespread use of diag-nostic computed tomography for blunt trauma(Figures 16 and 17).24,25
In conclusion, CDDS is considered the imagingtechnique of choice for most vascular injuries.Computed tomographic angiography, MRA andDSA are reserved for selected cases or directedtherapy.
100 J Ultrasound Med 2008; 27:95–107
Sonographic Evaluation of Vascular Injuries
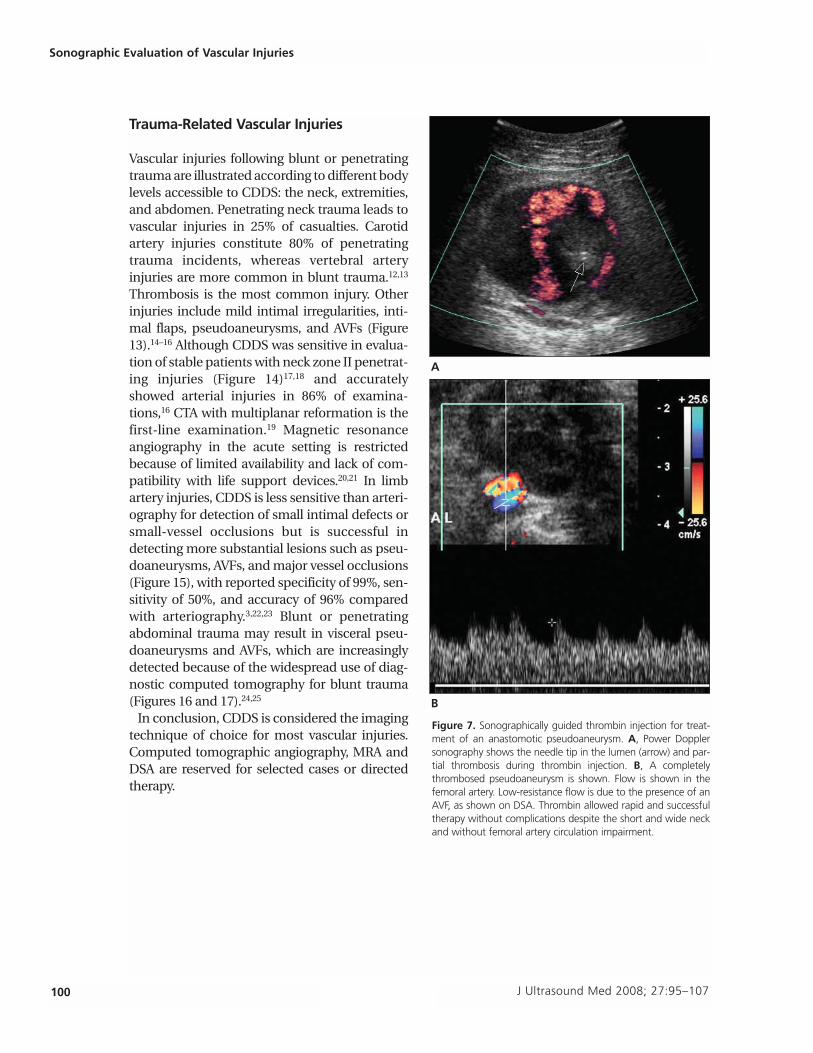
Figure 7. Sonographically guided thrombin injection for treat-ment of an anastomotic pseudoaneurysm. A, Power Dopplersonography shows the needle tip in the lumen (arrow) and par-tial thrombosis during thrombin injection. B, A completelythrombosed pseudoaneurysm is shown. Flow is shown in thefemoral artery. Low-resistance flow is due to the presence of anAVF, as shown on DSA. Thrombin allowed rapid and successfultherapy without complications despite the short and wide neckand without femoral artery circulation impairment.
A
B
J Ultrasound Med 2008; 27:95–107 101
Gaitini et al
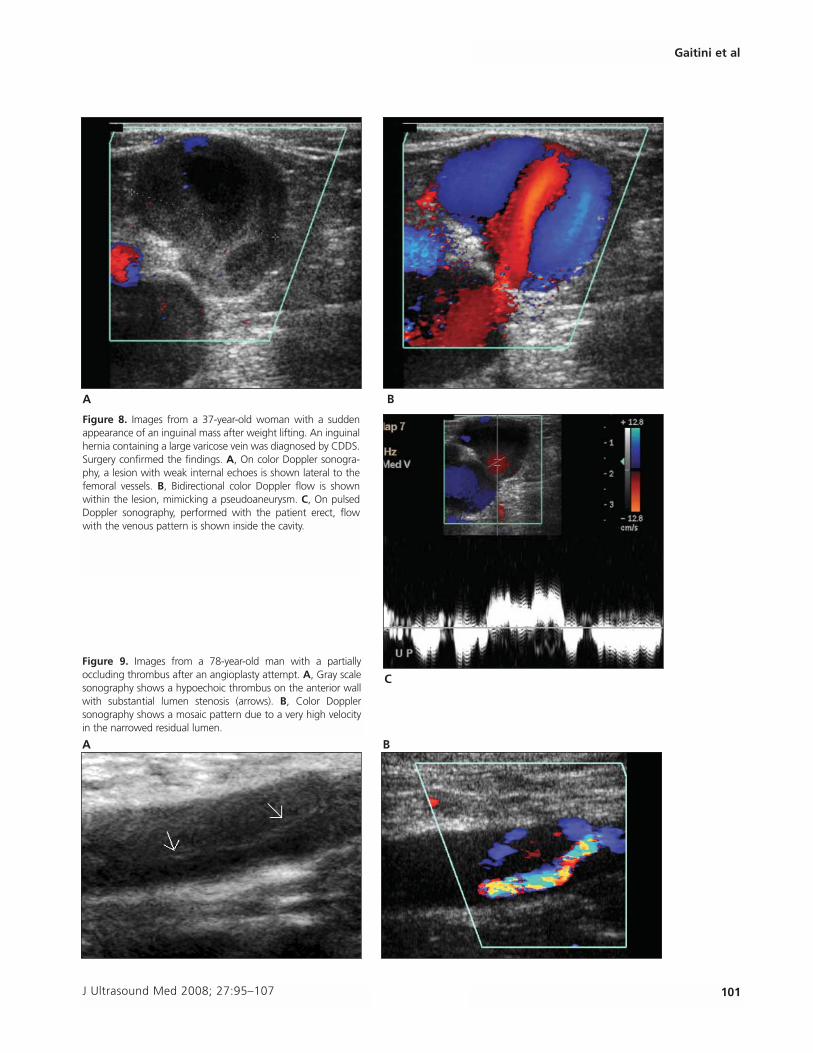
Figure 8. Images from a 37-year-old woman with a suddenappearance of an inguinal mass after weight lifting. An inguinalhernia containing a large varicose vein was diagnosed by CDDS.Surgery confirmed the findings. A, On color Doppler sonogra-phy, a lesion with weak internal echoes is shown lateral to thefemoral vessels. B, Bidirectional color Doppler flow is shownwithin the lesion, mimicking a pseudoaneurysm. C, On pulsedDoppler sonography, performed with the patient erect, flowwith the venous pattern is shown inside the cavity.
A B
C
Figure 9. Images from a 78-year-old man with a partiallyoccluding thrombus after an angioplasty attempt. A, Gray scalesonography shows a hypoechoic thrombus on the anterior wallwith substantial lumen stenosis (arrows). B, Color Dopplersonography shows a mosaic pattern due to a very high velocityin the narrowed residual lumen.
A B
102 J Ultrasound Med 2008; 27:95–107
Sonographic Evaluation of Vascular Injuries
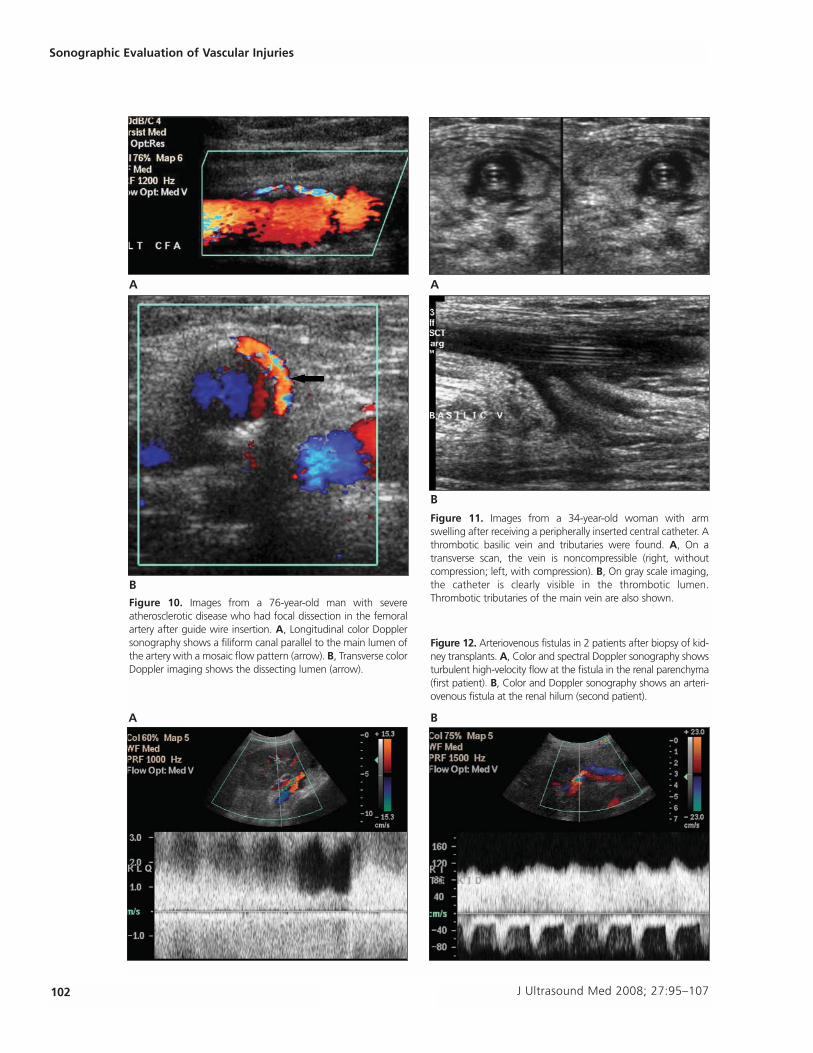
Figure 10. Images from a 76-year-old man with severeatherosclerotic disease who had focal dissection in the femoralartery after guide wire insertion. A, Longitudinal color Dopplersonography shows a filiform canal parallel to the main lumen ofthe artery with a mosaic flow pattern (arrow). B, Transverse colorDoppler imaging shows the dissecting lumen (arrow).
A
B
Figure 11. Images from a 34-year-old woman with armswelling after receiving a peripherally inserted central catheter. Athrombotic basilic vein and tributaries were found. A, On atransverse scan, the vein is noncompressible (right, withoutcompression; left, with compression). B, On gray scale imaging,the catheter is clearly visible in the thrombotic lumen.Thrombotic tributaries of the main vein are also shown.
A
B
Figure 12. Arteriovenous fistulas in 2 patients after biopsy of kid-ney transplants. A, Color and spectral Doppler sonography showsturbulent high-velocity flow at the fistula in the renal parenchyma(first patient). B, Color and Doppler sonography shows an arteri-ovenous fistula at the renal hilum (second patient).
A B
J Ultrasound Med 2008; 27:95–107 103
Gaitini et al
A
B
C
E
D
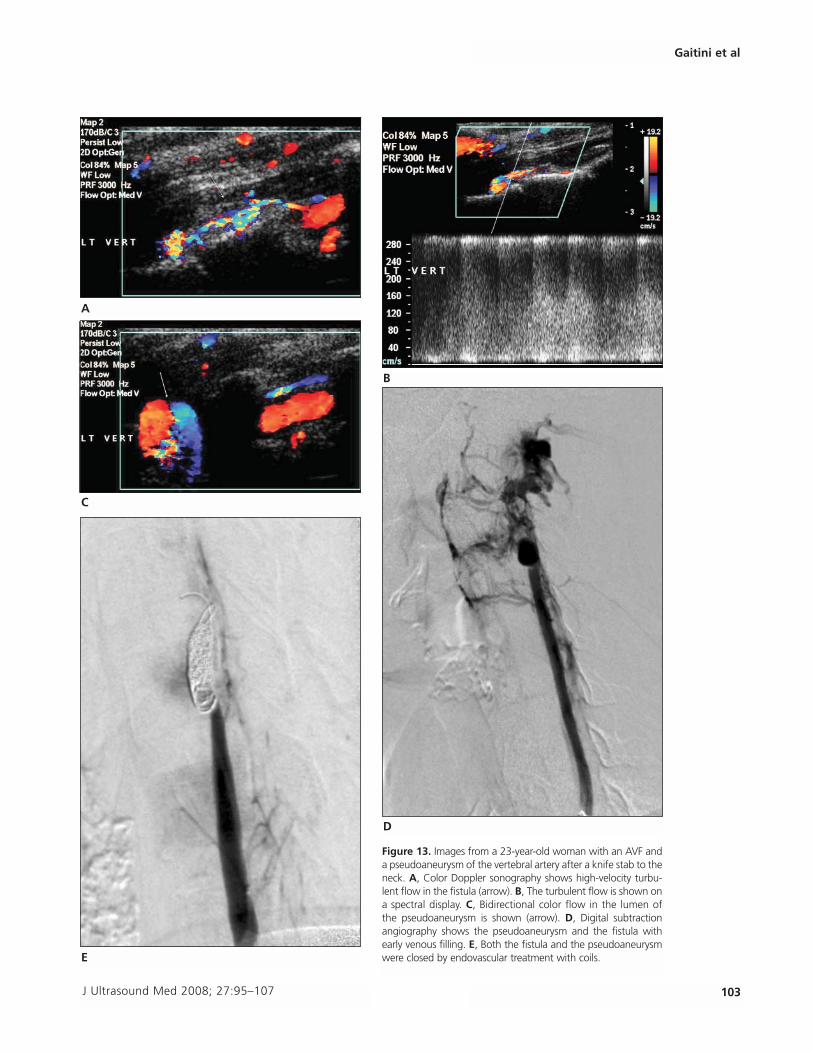
Figure 13. Images from a 23-year-old woman with an AVF anda pseudoaneurysm of the vertebral artery after a knife stab to theneck. A, Color Doppler sonography shows high-velocity turbu-lent flow in the fistula (arrow). B, The turbulent flow is shown ona spectral display. C, Bidirectional color flow in the lumen ofthe pseudoaneurysm is shown (arrow). D, Digital subtractionangiography shows the pseudoaneurysm and the fistula withearly venous filling. E, Both the fistula and the pseudoaneurysmwere closed by endovascular treatment with coils.
104 J Ultrasound Med 2008; 27:95–107
Sonographic Evaluation of Vascular Injuries
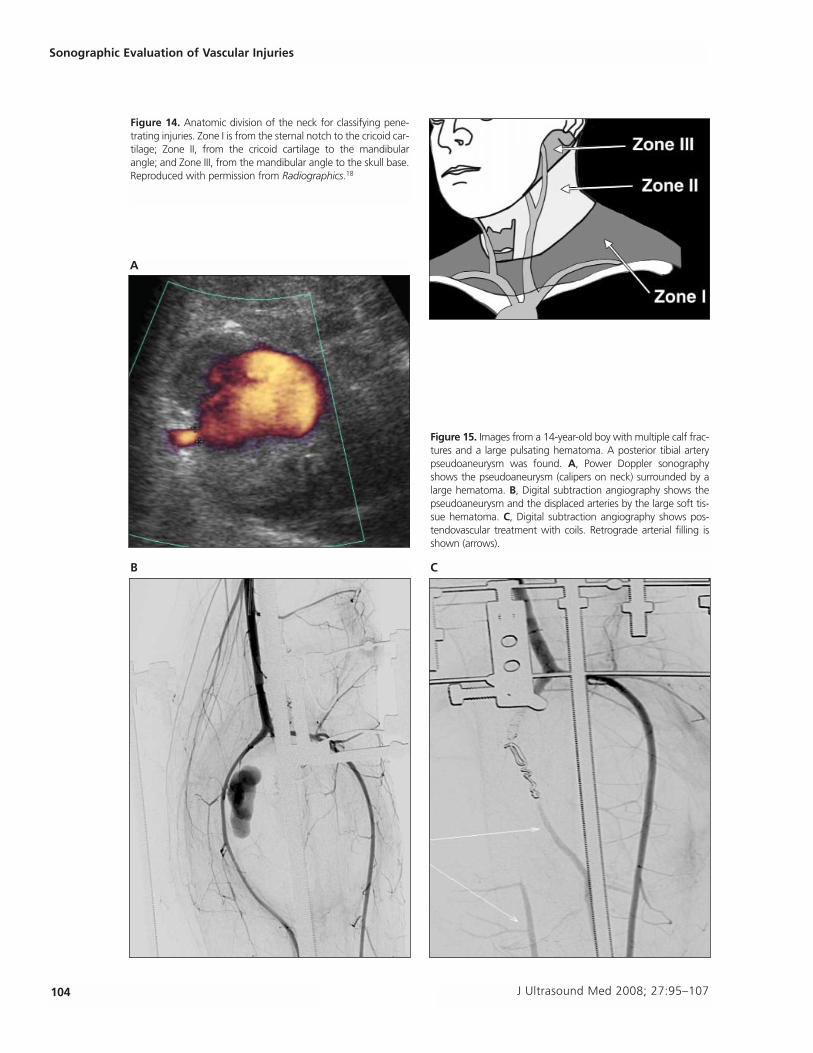
Figure 14. Anatomic division of the neck for classifying pene-trating injuries. Zone I is from the sternal notch to the cricoid car-tilage; Zone II, from the cricoid cartilage to the mandibularangle; and Zone III, from the mandibular angle to the skull base.Reproduced with permission from Radiographics.18
Figure 15. Images from a 14-year-old boy with multiple calf frac-tures and a large pulsating hematoma. A posterior tibial arterypseudoaneurysm was found. A, Power Doppler sonographyshows the pseudoaneurysm (calipers on neck) surrounded by alarge hematoma. B, Digital subtraction angiography shows thepseudoaneurysm and the displaced arteries by the large soft tis-sue hematoma. C, Digital subtraction angiography shows pos-tendovascular treatment with coils. Retrograde arterial filling isshown (arrows).
B C
A
J Ultrasound Med 2008; 27:95–107 105
Gaitini et al
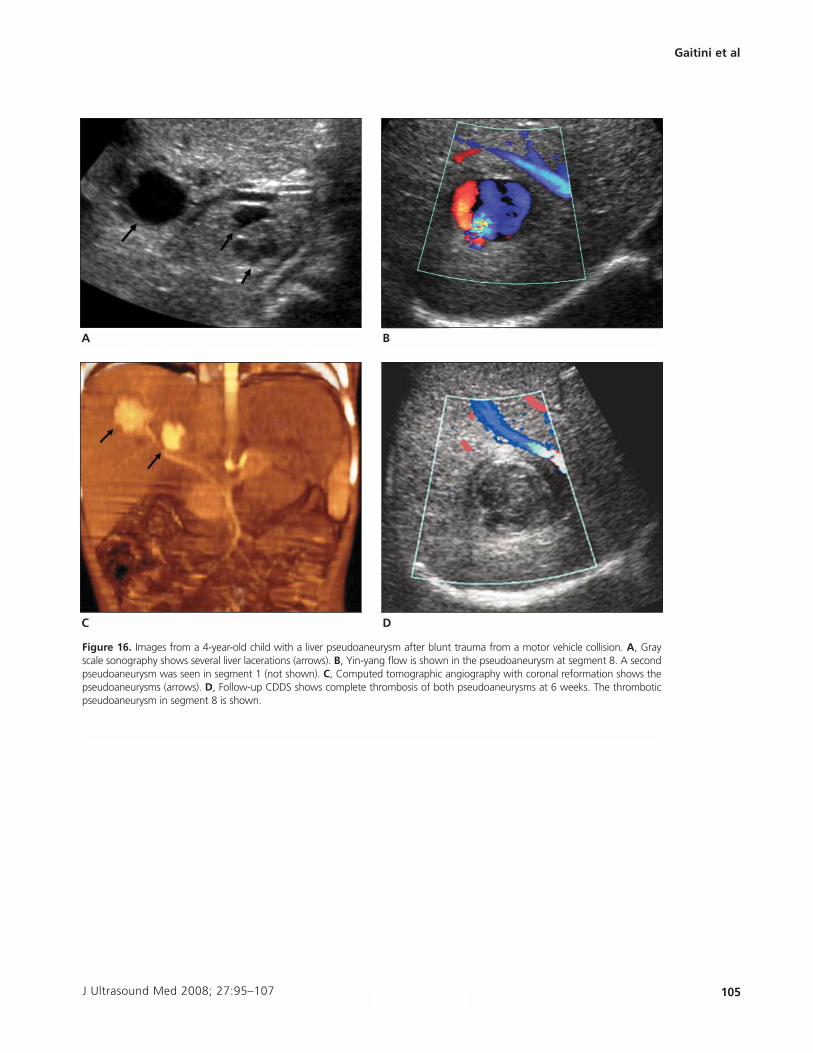
Figure 16. Images from a 4-year-old child with a liver pseudoaneurysm after blunt trauma from a motor vehicle collision. A, Grayscale sonography shows several liver lacerations (arrows). B, Yin-yang flow is shown in the pseudoaneurysm at segment 8. A secondpseudoaneurysm was seen in segment 1 (not shown). C, Computed tomographic angiography with coronal reformation shows thepseudoaneurysms (arrows). D, Follow-up CDDS shows complete thrombosis of both pseudoaneurysms at 6 weeks. The thromboticpseudoaneurysm in segment 8 is shown.
A B
C D
References
1. Giswold ME, Laundry GJ, Taylor LM, Moneta GL. Iatrogenicarterial injury is an increasingly important cause of arterialtrauma. Am J Surg 2004; 187:590–593.
2. Katzenschlager R, Ugurluoglu A, Ahmadi A, et al. Incidenceof pseudoaneurysm after diagnostic and therapeuticangiography. Radiology 1995; 195:463–466.
3. Bergstein JM, Blair JF, Edwards J, et al. Pitfalls in the use ofcolor-flow duplex ultrasound for screening of suspectedarterial injuries in penetrated extremities. J Trauma 1992;33:395–402.
4. Bynoe RP, Miles WS, Bell RM, et al. Noninvasive diagnosisof vascular trauma by duplex ultrasonography. J Vasc Surg1991; 14:346–352.
5. Panetta TF, Sales CM, Marin ML, et al. Natural history,duplex characteristics, and histopathologic correlation of
arterial injuries in a canine model. J Vasc Surg 1992; 16:867–876.
6. Kronzon I. Diagnosis and treatment of iatrogenic femoralartery pseudoaneurysm: a review. J Am Soc Echocardiogr1997; 10:236–245.
7. Morgan R, Belli A. Current treatment methods for post-catheterization pseudoaneurysms. J Vasc Interv Radiol2003; 14:697–710.
8. Brophy DP, Sheiman RG, Amatulle P, Akbari CM. Iatrogenicfemoral pseudoaneurysms: thrombin injection after failedUS-guided compression. Radiology 2000; 214:278–282.
9. Davison BD, Polak JF. Arterial injuries: a sonographicapproach. Radiol Clin North Am 2004; 42:383–396.
10. Patel MC, Berman LH, Moss HA, McPherson SJ. Subclavianand internal jugular veins at Doppler US: abnormal cardiacpulsatility and respiratory phasicity as a predictor of com-plete central occlusion. Radiology 1999; 211:579–583.
106 J Ultrasound Med 2008; 27:95–107
Sonographic Evaluation of Vascular Injuries
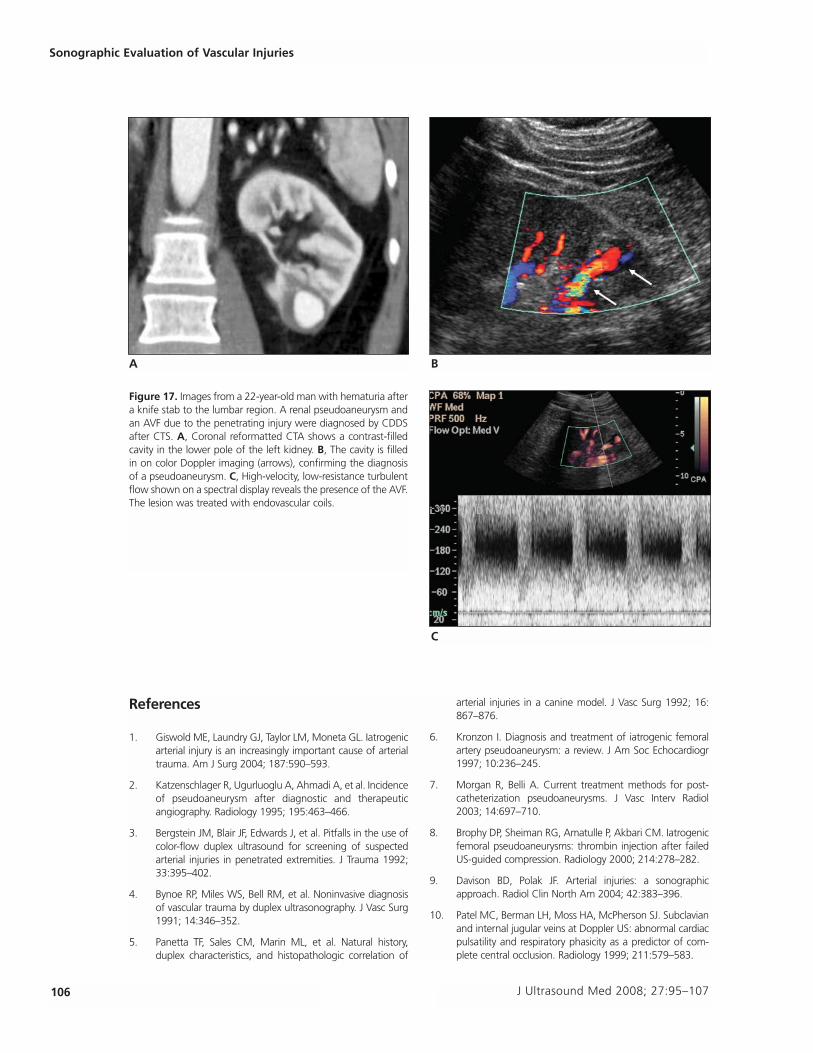
Figure 17. Images from a 22-year-old man with hematuria aftera knife stab to the lumbar region. A renal pseudoaneurysm andan AVF due to the penetrating injury were diagnosed by CDDSafter CTS. A, Coronal reformatted CTA shows a contrast-filledcavity in the lower pole of the left kidney. B, The cavity is filledin on color Doppler imaging (arrows), confirming the diagnosisof a pseudoaneurysm. C, High-velocity, low-resistance turbulentflow shown on a spectral display reveals the presence of the AVF.The lesion was treated with endovascular coils.
A B
C
11. Merkus JW, Zeebregts CJ, Hoitsma AJ, van Asten WN,Koene RA, Skotnicki SH. High incidence of arteriovenousfistula after biopsy of kidney allografts. Br J Surg 1993;80:310–312.
12. Kuehne JP, Weaver FA, Papanicolau G, Yellin AE.Penetrating trauma of the internal carotid artery. Arch Surg1996; 131:942–948.
13. Willis BK, Greiner F, Orrison WW, Benzel EC. The incidenceof vertebral artery injury after midcervical spine fracture orsubluxation. Neurosurgery 1994; 34:435–442.
14. Singh RR, Barry MC, Ireland A, Bouchier Hayes D. Currentdiagnosis and management of blunt internal carotid arteryinjury. Eur J Vasc Endovasc Surg 2004; 27:577–584.
15. Larsen DW. Traumatic vascular injuries and their manage-ment. Neuroimaging Clin North Am 2002; 12:249–269.
16. Cogbill TH, Moore EE, Meissner M, et al. The spectrum ofblunt injury to the carotid artery: a multicenter perspective.J Trauma 1994; 37:473–479.
17. Montalvo BM, LeBlang SD, Núñez DB Jr, et al. ColorDoppler sonography in penetrating injuries of the neck.AJNR Am J Neuroradiol 1996; 17:943–951.
18. Núñez DB Jr, Torres-León M, Múnera F. Vascular injuries ofthe neck and thoracic inlet: helical CT-angiographic corre-lation. Radiographics 2004; 24:1087–1100.
19. Eastman AL, Chason DP, Perez CL, McAnultyAL, Minei JP.Computed tomographic angiography for the diagnosis ofblunt cervical vascular injury: is it ready for primetime? J Trauma 2006; 60:925–929.
20. Miller PR, Fabian TC, Croce MA, et al. Prospective screen-ing for blunt cerebrovascular injuries: analysis of diagnosticmodalities and outcomes. Ann Surg 2002; 236:386–393.
21. Ofer A, Nitecki SS, Braun J, et al. CT angiography of thecarotid arteries in trauma to the neck. Eur J Vasc EndovascSurg 2001; 21:401–407.
22. Schoder M, Prokof M, Lammer J. Traumatic injuries: imag-ing and intervention of large arterial trauma. Eur Radiol2002; 12:1617–1631.
23. Schwartz M, Weaver F, Yellin A, Ralls P. The utility of colorflow Doppler examination in penetrating extremity arterialtrauma. Am Surg 1993; 59:375–378.
24. Soudack M, Epelman M, Gaitini D. Spontaneous thrombo-sis of hepatic post traumatic pseudoaneurysms: sono-graphic and computed tomographic features. J UltrasoundMed 2003; 22:99–103.
25. Basile KE, Sivit CJ, Sachs PB, Stallion A. Hepatic arterialpseudoaneurysm: a rare complication of blunt abdominaltrauma in children. Pediatr Radiol 1999; 29:306–308.
J Ultrasound Med 2008; 27:95–107 107
Gaitini et al