south african neurodevelopmental therapy association ... · south african neurodevelopmental...
TRANSCRIPT
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION
SANDTA
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER
Newsletter NOVEMBER 2013SANDTA NEC
Chairperson:Dorothy Russell083 375 [email protected]
Vice Chairperson:Shelagh Hughes084 6864571s [email protected]
Treasurer:Carol Brenner 083 [email protected]
Secretary:Elisabeth Barry 083 [email protected]
CPD Co-ordinator:Dorothy Russell083 375 [email protected]
Education Representative:Karien [email protected]
Branch Liaison:Andrea [email protected]
Newsletter:Shelagh Hughes084 6864571s [email protected]
Website:Shelley Broughton082 [email protected]
SANDTA OFFICE CONTACT DETAILSLalique SmitTel 051 436 8145Fax 086 275 2869Email [email protected] www.sandta.org.za
CONTENTS
SANDTA CONGRESS 2014......................................2- CALL FOR PAPERS................................................3- CALL FOR ABSTRACTS.........................................4
INTERNATIONAL SANDTA MEMBER NEWS- Submitted by Paul Nuwagaba (OT).........................5
PHYSIOTHERAPY AND THE ORTHOPAEDICMANAGEMENT OF CHILDREN WITH CEREBRAL PALSY AT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL- Submitted by Linda Wood........................................6
CP RESEARCH LINKS..............................................8
FEEDBACK FROM THE 2013 BASIC PAEDIATRIC NDT COURSE.....................................9
SANDTA NEC-BRANCHES MEETING 2013..........11
SANDTA NATIONAL AGM 2013.............................12
CORRECT DISABILITY TERMINOLOGY...............13
REMINDERS:- FINANCIAL ASSISTANCE - ADVERTISING VIA SANDTA- ADVERTISING SECOND HANDTHERAPY EQUIPMENT..........................................14
ONLINE CPD ARTICLES........................................15
BRANCH CONTACTS & GENERAL INFORMATION..................................16
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 2
Theme: Merging Science and PracticeDEADLINE FOR SUBMISSION OF ABSTRACTS: 28 February 2014
The South African Neurodevelopmental Therapy Association is now awaiting submission of abstracts for oral and poster presentations plus short workshops for the above congress. The theme of the Congress is Merging Science and Practice. The objective of the Congress is to provide practical and scientific content that stimulates the interest of all disciplines involved in the rehabilitation of babies, children, adolescents and adults with central motor disturbances.
Abstracts will be reviewed for acceptance on their scientific merit and should therefore be of a high standard and relevant to the theme of the congress. Abstracts must be submitted by e-mail, in English and per the instructions below, to the following email address: [email protected]. Faxed abstracts will not be accepted. Abstracts that do not conform to the instructions below will not be considered.
In your email, please indicate a) your profession; b) your place of work; c) comprehensive contact details; and d) what type of presentation you would like to do (oral or poster presentation). If you would like to present a workshop, please indicate the proposed length of the workshop in hours. Workshops will be offered in the afternoon on two of the congress days.
Invited presenters are welcome to join the Congress on the day of their presentation. Should they wish to attend the entire Congress they need to register.Authors will be informed by 11 April 2014 whether their abstracts have been accepted.
INSTRUCTIONS FOR THE PREPARATION OF ABSTRACTS (as per separate form)The form can be downloaded from http://www.sandta.org.za
– Title should be typed in capital letters, bold and left aligned– If submitting more than one abstract, each abstract must be sent as a separate email and the
title should indicate that these are separate abstracts, i.e. JOE WEST ABSTRACT 1; JOE WEST ABSTRACT 2; etc.
– No references, end–notes, diagrams or frames should be included in the abstract.– Audio-visual and other equipment requirements should NOT be included in the abstract.– Please advise us of the duration of your presentation/workshop
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 3
SOUTH AFRICAN NEURODEVELOPMENTAL
THERAPY ASSOCIATION CONGRESSCall for Papers
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 4
Main/First Author: Presenting author's name should be underlined and bolded.
Full Name: Phone: (incl. international dialling, country & area codes)
Work:Cell/Mobile:
Title: Email:
Organisation: Tick/check presentation type:
Poster:
Oral:
Job Title/Profession: Workshop:
Abstract (maximum 300 words) Times New Roman; 12 point; Single spacing
Speaker BiographyQualifications, recent publications & recent conference presentations should be included
SOUTH AFRICAN NEURODEVELOPMENTAL
THERAPY ASSOCIATION CONGRESSSubmission of Abstract
International SANDTA member news:
Paul Nuwagaba- Occupational Therapist
Having had regular contact with Paul since taking on the newsletter portfolio I became aware of the number of international SANDTA members and so made contact with them asking for feedback on their professional and NDT training and the work that they are currently doing.
Paul very kindly submitted the following article:
My name is Paul Nuwagaba, an Occupational Therapist trained from Uganda and Bobath/NDT trainee. I completed the Introductory and Basic courses at Bobath Center, London in 2008 and Johannesburg, South Africa in 2010 respectively.
I currently live in Riyadh in the Kingdom of Saudi Arabia and am working with the Sultan Bin Abdulaziz Humanitarian City, a Rehabilitation Hospital that is accredited by the Commission for Accreditation of Rehabilitation Facilities (CARF) and Joint Commission International (JCI).
I came to train in the Bobath/NDT treatment approach after identifying challenges with working with children with neurological disorders especially Cerebral palsy.
We have been able to apply NDT skills through interdisciplinary work as a professional team with family centred care approaches. In the family centred approach the parent/caregiver plays a key role in both participation and decision making in the treatment program. In addition we have started up internal monthly training of PTs, OTs, SLPs who are Bobath/NDT trainees to enable us to improve and maintain hands-on skills and we are looking forward to further collaboration with SANDTA for both internal and external training so as to enable us to strengthen our skills.
For the Cerebral Palsy intervention and services, the paediatric units follows the International Classification of Functioning Disability and Health (ICF) model to promote participation and inclusive development with schools and community to enhance participation levels.
As an accredited program, outcomes are measured monthly with an emphasis on participation levels of patients. For example the program monitors the educational activities and placement of children of school going age; mainly commencing school for new children and returning to school for children already in school. The interdisciplinary team discusses the potential outcomes during the admission in an initial team conference where parents attend and discuss their goals and expectations with the team. The team is equally involved in setting goals for therapy and educational intervention to maximize the potential for the child to participate in school, home and community activities.
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 5
Thanks for sharing the great work you do with us, Paul.
We wish you and your team all the very best!
From your SA colleagues in NDT
Physiotherapy and the Orthopaedic management of children with Cerebral Palsy at Chris Hani Baragwanath Academic Hospital
By Linda Wood
Three years ago, the paediatric physiotherapy team at Chris Hani Baragwanath Academic Hospital was approached by Dr Greg Firth, the newly appointed Head of Department of the Paediatric Orthopaedic Surgery Department at the hospital, with the aim of developing a more multidisciplinary approach when managing children with Cerebral Palsy (CP) who require surgical intervention. He had returned from his fellowship at the Royal Children’s Hospital in Ottawa, Canada and Melborne, Australia where he had trained under the guidance of the world renowned orthopaedic surgeon Professor Kerr Graham. The team at the Royal Children’s Hospital are leaders in the field of the surgical management of children with CP, and during his fellowship Dr Firth trained extensively in the orthopaedic management of children with CP and worked closely with the physiotherapists at the hospital. Historically, surgical intervention for children with CP did not hold high priority at CHBAH and the proposal from Dr Firth seemed very daunting, with few physiotherapists in the department having had any experience in this field. The next few months proved to be a very rapid learning process for us as we benchmarked other experienced therapists, sought articles and attended lectures in an effort to provide an effective post-operative rehabilitation. There have been some key changes over the past three years to the services offered to the children with CP who seek health care at CHBAH, one of which is the introduction of a hip surveillance program. It is internationally accepted practise to screen all children with CP for hip subluxation, with this program primarily run by the therapists at the hospital (Gordon, 2006). Hip dislocation in children with CP has been widely reported in the literature. The early identification of hip subluxation can assist in the prevention of hip dislocation and the resultant complications such as pain, poor hygiene and secondary musculoskeletal deformity such as scoliosis (Wynter, 2008). Once the hip has been dislocated for longer than six months it is often too late to intervene, which makes early identification of hip subluxation, essential in the management of these children.
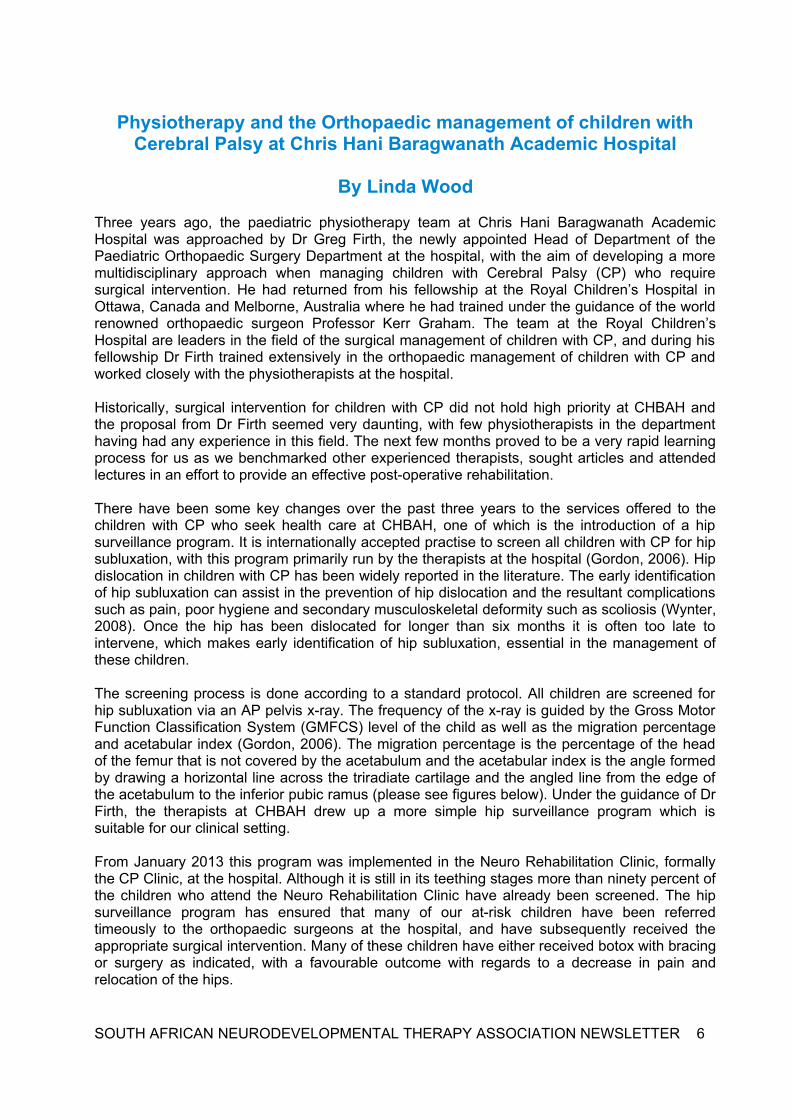
The screening process is done according to a standard protocol. All children are screened for hip subluxation via an AP pelvis x-ray. The frequency of the x-ray is guided by the Gross Motor Function Classification System (GMFCS) level of the child as well as the migration percentage and acetabular index (Gordon, 2006). The migration percentage is the percentage of the head of the femur that is not covered by the acetabulum and the acetabular index is the angle formed by drawing a horizontal line across the triradiate cartilage and the angled line from the edge of the acetabulum to the inferior pubic ramus (please see figures below). Under the guidance of Dr Firth, the therapists at CHBAH drew up a more simple hip surveillance program which is suitable for our clinical setting.
From January 2013 this program was implemented in the Neuro Rehabilitation Clinic, formally the CP Clinic, at the hospital. Although it is still in its teething stages more than ninety percent of the children who attend the Neuro Rehabilitation Clinic have already been screened. The hip surveillance program has ensured that many of our at-risk children have been referred timeously to the orthopaedic surgeons at the hospital, and have subsequently received the appropriate surgical intervention. Many of these children have either received botox with bracing or surgery as indicated, with a favourable outcome with regards to a decrease in pain and relocation of the hips.
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 6
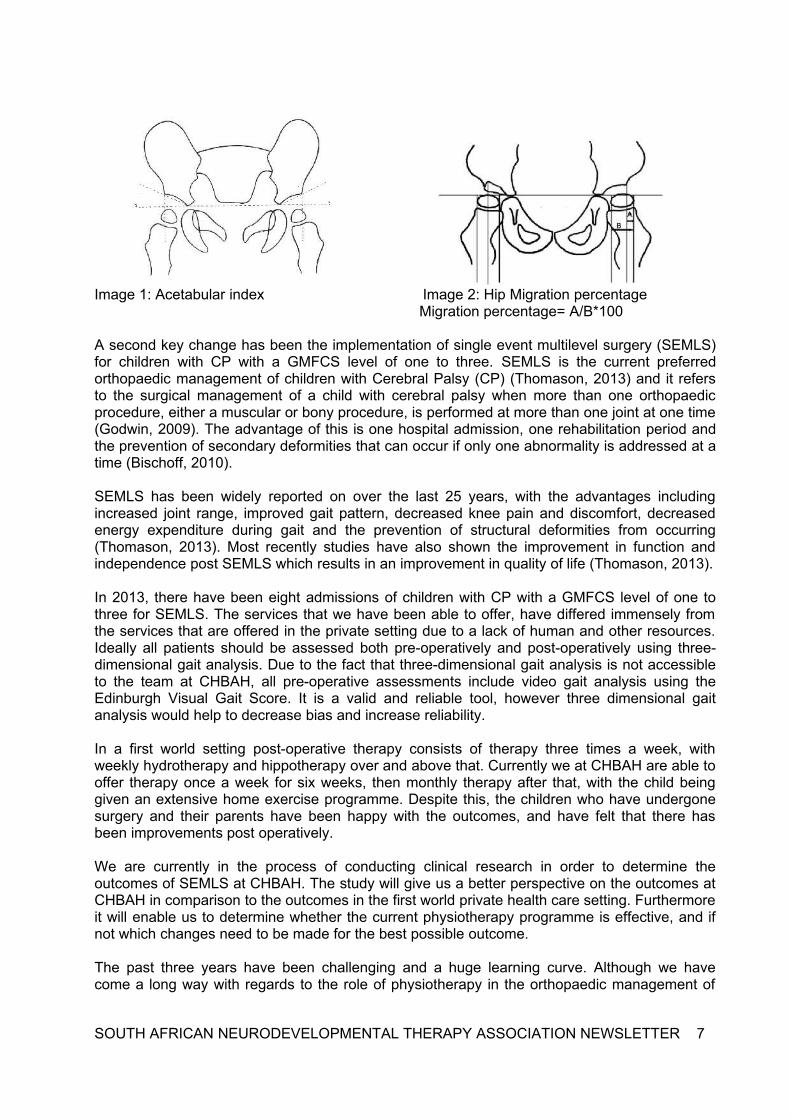
Image 1: Acetabular index Image 2: Hip Migration percentage Migration percentage= A/B*100
A second key change has been the implementation of single event multilevel surgery (SEMLS) for children with CP with a GMFCS level of one to three. SEMLS is the current preferred orthopaedic management of children with Cerebral Palsy (CP) (Thomason, 2013) and it refers to the surgical management of a child with cerebral palsy when more than one orthopaedic procedure, either a muscular or bony procedure, is performed at more than one joint at one time (Godwin, 2009). The advantage of this is one hospital admission, one rehabilitation period and the prevention of secondary deformities that can occur if only one abnormality is addressed at a time (Bischoff, 2010).
SEMLS has been widely reported on over the last 25 years, with the advantages including increased joint range, improved gait pattern, decreased knee pain and discomfort, decreased energy expenditure during gait and the prevention of structural deformities from occurring (Thomason, 2013). Most recently studies have also shown the improvement in function and independence post SEMLS which results in an improvement in quality of life (Thomason, 2013).
In 2013, there have been eight admissions of children with CP with a GMFCS level of one to three for SEMLS. The services that we have been able to offer, have differed immensely from the services that are offered in the private setting due to a lack of human and other resources. Ideally all patients should be assessed both pre-operatively and post-operatively using three-dimensional gait analysis. Due to the fact that three-dimensional gait analysis is not accessible to the team at CHBAH, all pre-operative assessments include video gait analysis using the Edinburgh Visual Gait Score. It is a valid and reliable tool, however three dimensional gait analysis would help to decrease bias and increase reliability.
In a first world setting post-operative therapy consists of therapy three times a week, with weekly hydrotherapy and hippotherapy over and above that. Currently we at CHBAH are able to offer therapy once a week for six weeks, then monthly therapy after that, with the child being given an extensive home exercise programme. Despite this, the children who have undergone surgery and their parents have been happy with the outcomes, and have felt that there has been improvements post operatively.
We are currently in the process of conducting clinical research in order to determine the outcomes of SEMLS at CHBAH. The study will give us a better perspective on the outcomes at CHBAH in comparison to the outcomes in the first world private health care setting. Furthermore it will enable us to determine whether the current physiotherapy programme is effective, and if not which changes need to be made for the best possible outcome.
The past three years have been challenging and a huge learning curve. Although we have come a long way with regards to the role of physiotherapy in the orthopaedic management of
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 7
children with CP, there is still a lot to learn and develop at CHBAH to ensure that the services offered meet international standards.
Written by Linda Wood, with thanks to Tracey Bulmer and Dr Greg Firth
Bibliography
Bischof, F. (2010). Single event multilevel surgery in cerebral palsy: a review of the literature. South African Orthopaedic Journal, 30-33.
Godwin, E. (2009). Cerebral palsy and single-event multilevel sugery; Is there a relationship between level of function and intervention over time? Journal of Paediatric Orthopaedics, 29, 910-915.
Gordon, G. (2006). A systematic review for evidence for hip surveillance in children with cerebral palsy. The Bone and Joint Journal, 1492-1496.
Graham, K. (2005). Classifying Cerebral Palsy. Journal of Paediatric Orthopaedics, 25(1), 127-128.
Thomason, P. (2013). Single event multilevel surgery in children with bilateral spastic cerebral palsy: A 5 year prospective cohort study. Gait and posture, 37, 23-38.
Wynter, M. (2008). Consensus Statement on Hip Surveillance for Children with Cerebral Palsy: Australian Standards of care 2008. Melborne: Government of Western Australia Department of Health.
Keeping up to date with CPD research and news
EUROPEAN BOBATH TUTORS ASSOCIATION (EBTA)
The EBTA would like to encourage NDT/Bobath therapists from all countries to access their website for up to date NDT/Bobath information. The general public is able to access all areas of the website, except the members page.
www.bobath-ndt.com
CEREBRAL PALSY ALLIANCE NEWSLETTER
Cerebral Palsy Alliance is delighted to bring you this free weekly bulletin of published research into cerebral palsy, as indexed in the NCBI PubMed (Medline) and Entrez (GenBank) databases.
Please note: To subscribe, please complete the online form at www.cpresearch.org/subscribe/researchnews. You can also bookmark this form on your smart phone or email the link to a friend.
If you would like to unsubscribe from this bulletin, please email CP Research News, with the word 'Unsubscribe' in the subject line of the email.
Our organisation is committed to supporting cerebral palsy research worldwide - through information, education, collaboration and funding. Find out more at www.cpresearch.org.au
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 8
Feedback from the 2013 Basic Paediatric NDT Course- Johannesburg
We were a group of 24 participants embarking on the Basic 8 week NDT course in Johannesburg, February 2013. Our first introduction to the course was through the distance based learning assignments from November 2012 up until the course started in Feb 2013. This allowed for the course to be 7 weeks and the distance based learning accounting for 1 week. It was hard work and stressful at times, for us and the tutors, but the distance based learning modules gave us a good theoretical background for the course to come.
We all arrived on Monday morning, 4th Feb 2013, at the TMI with feelings of excitement. The Johannesburg traffic was a way to wake you up in the morning and a few of the therapists also made good use of the Gautrain. Our course leader was Doris Mbuyu who immediately made us feel welcome and at home. We had an opportunity to get to know all the participants that came from all over the world; Poland, Ghana, Germany. It was a wonderful group of people.
The first 4 weeks of the course kicked off with a bang. We were ready to learn more about the treatment approach that has been developing. During this first block, our practicals consisted of seeing CP children at TMI (Malamulele onward) as well as Forest town school. The Occupational Therapy week was part of this first block. We had several tutors and guest speakers that gave input in different areas.
The second part of the course was 3 weeks, the break in between gave us the opportunity to practise what we’d learned and to implement it into our practises. We did a community week in the Soweto area, at Mthimkulu stimulation school; here we made assistive devices by using low cost materials. During this block we also saw teenagers at Hope School. The different population and social environments of the CP children gave us the opportunity to expand our knowledge base and understanding of the treatment as well as management of the different groups of children. We had a wonderful lunch at “Wandie’s Restaurant”, in Soweto; were we were entertained with local music. This gave us a chance to socialize as colleagues and friends before departing the next day.
Throughout the course we were privileged to have guest lecturers in all different fields of expertise. Our outlook on the treatment and management of the child with cerebral palsy has changed. We have more confidence in the handling of children and their families. We will work in a more goal directed way and our treatment will be specific and a holistic approach will be followed. Our knowledge of neuroscience will assist in working in a more evidence based manner. We will try to work together as a team, the Physiotherapist, Occupational Therapist and Speech Therapist to establish a comprehensive treatment plan. This is together with the individual, the parents, caregiver as well as the medical team present.
This course has been so enriching on a personal as well as professional level and we thank every tutor, lecturer, child, parent and participant for their contribution!!
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 9
Participants of the 2013 Basic Bobath/NDT Paediatric course.
Dalene JoubertNaina Modi-PatelMariaan TeubesAgnieszka MasioAnna LisNatalie ToyJudith ArthurCharene HymanRozanne du ToitTasneem EssopjeeShannon MorganKirsten HuntleyKristina JoselowitzMaria van ZylLiesel Schoeman (Els)Lauren DaviesSumaya BabamiaSelmari PotgieterAnke WiplingerKristyl WeatherheadSarah MortonJeanne TaylorVallery MukwevhoJennifer Lau
OTSTOTPTPTSTAPTSTAOTOTOTPTPTOTPTOTSTAOTPTOTPTOTOTSTA
A heartfelt and sincere thank you to Christa Scholtz, Karien Marais, Dr Gillian Saloojee, Dianne Zeller, Annie Recordon (New Zealand), Estelle Brown, all the clinical supervisors, all lecturers, the children and their parents, the staff and colleagues at Malamulele Onwards, Forest Town School, Hope School, Mthimkulu Centre and anyone who contributed to the success of this course.
A special thank you to Estie du Plessis for her time and valuable experience.
Yogolelo Mbuyu (Course leader- SANDTA PT Tutor)
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 10
SANDTA NEC & Branches Face to Face Meeting- 11 October, Pretoria
The North Gauteng SANDTA Branch hosted this year's face to face meeting in Pretoria. The day ran smoothly with the NEC and branch representatives taking time to share their annual reports, discuss any issues from the past year and plan for the coming year. After a day long meeting the gathering moved to a local restaurant, Tribeca, for supper.
Thank you to the organisers- Esedra Strasheim and Bridget Herselman!
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 11
Christa & Karien- Ed Comm RepsBridget & Esedra- NG branch Andrea- Branch liason and SG branch Dorothy- CPD and Vice Chairperson
Marieta- FS branchElisabeth- Secretary and EC branch
Nina Strydom- Chairperson Vanessa- KZN branchBronwen- WC branch
SANDTA National AGM and Workshops
On Saturday 12 October 2013 the National SANDTA AGM was held in Pretoria with a full day of workshops titled- New Trends in the Management of People with Disabilities.
Despite a small response from SANDTA members the event went ahead smoothly and was enjoyed by all who attended. Thank you again to the North Gauteng branch who organised the event.
The programme included the following excellent presentations:
– Eye movements and postural alignment in children with cerebral palsy: Christa Scholtz
– A sequential methods study describing the perceptions of environmental barriers and the employment of persons with disabilities in a private healthcare company: Nina Strydom
– Intensive blocks of therapy: do they work? A review of 60 children seen by the Malamulele Onward team: Nicole Whitehead
– Evaluating the evidence of our CP interventions: Prof. Faith Bischoff
– An informal introduction to the PROMPT speech treatment method and its use in conjunction with NDT: Karien Marais
AGM
At the AGM Nina Strydom stepped down as NEC chairperson and she was thanked for her outstanding leadership over the past two years. Her particular focus on good governance and further developing transparent processes has strengthened the organisation. Her hard work and dedication was much appreciated.
Dorothy Russell was voted in as the next Chairperson and Shelagh Hughes will take on the Vice Chairperson position.
The National Executive Committee, Education Committee and Treasurer annual reports will be available on the SANDTA website.
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 12
Elriza Janse van Vuuren, Maryanne van der Velde, Bridget Herselman & Theresa Marias
Dorothy thanking Nina Pam Gibbs & Faith Bischoff
Correct disability terminologyThe following information was sent as an email from Disability Rights at the Department of Women, Children and People with Disabilities ([email protected]). We thought it might serve as a useful reminder to therapists:
“The Promotion of Equality and Prevention of Unfair Discrimination Act (PEPUDA), 2000, outlaws hate speech on, among others, the basis of disability. Section 10, dealing with Prohibition of hate speech, states that
“10. (1)Subject to the proviso in section 12, no person may publish, propagate, advocate or communicate words based on one or more of the prohibited grounds, against any person, that could reasonably be construed to demonstrate a clear intention to
(a) be hurtful; (b) be harmful or to incite harm; (c) promote or propagate hatred.
(2) Without prejudice to any remedies of a civil nature under this Act, the court may, in accordance with section 2 (1)(2)(n) and where appropriate, refer any case dealing with the publication, advocacy, propagation or communication of hate speech as contemplated in subsection (1), to the Director of Public Prosecutions having jurisdiction for the institution of criminal proceedings in terms of the common law or relevant legislation.”
The Deaf Federation of South Africa (DeafSA), recommends that the following terminology be AVOIDED, as it is deemed as derogatory and harmful to Deaf persons: Deaf and Dumb, Mute, Person with a hearing loss, Non hearing person, Hearing Impaired, Hearing handicap.
CORRECT TERMINOLOGY: DeafSA notes that Deaf persons do not want to be primarily defined by their lack of (or poor) hearing. Deaf persons prefer to be called Deaf, Hard of Hearing or deaf when the need arises to refer to their hearing status, but not as a primary way to identify them as people.
This is in line with the guidelines provided by the UN Convention on the Rights of Persons with Disabilities, which notes that it is not the impairment per se which disables an individual, but the interaction between the person with an impairment and the environment which causes disability when this interaction is negative.
It is also not acceptable to refer to persons with disabilities as PWD in documents, just as it is not acceptable to call black persons BP and white persons WP.
Persons with disabilities likewise do not live with a disability, which would imply it is something they can choose to put on or not in the morning, rather simply use the term persons with disabilities.
The DWCPD is working with government departments to correct harmful and negative terminology contained in legislation and policy documents through a legislative audit and the finalisation of the National Disability Rights Policy. The DWCPD has also embarked on a participatory exercise in identifying harmful disability-related terminology in all the country’s official languages with the aim of developing positive disability-related language.
We similarly call on the media, the private sector, as well as civil society (including disability organisations) to liaise with organisations of persons with disabilities in correcting their use of terminology in order (a) afford persons with disabilities the respect and dignity guaranteed in the Constitution, and (b) not to fall foul of the PEPUDA.
Working together we can do more to build a fully inclusive society free from unfair discrimination, inequality, abuse and exploitation!
Your DisabilityRights Team in the DWCPD”
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 13
Reminders:
Financial assistance offered to SANDTA members
SANDTA offers members the opportunity to apply for financial assistance for attending continuing professional development events (such as congresses and other national or international events associated with Bobath/NDT) or for funding towards research projects as a part of postgraduate degrees.
Deadlines for applications are the last Friday of February, May, August and November.The financial assistance application process can be found on www.sandta.org.za- 'Member's section'- 'Protocols and procedures'.
Advertising via SANDTA
For details of advertising via SANDTA please see www.sandta.org.za- 'Member's section'- 'Protocols and procedures' or contact [email protected].
There are the following options with the associated costs:
Advert Option Cost- Member Cost- Non-member NGOs & centres supporting CP
Advert posted on SANDTA website
R210 R315 R100
Advert as sms/email R265 R380 R155
Advert on website and sent as sms/email
R410 R620 R200
Advertising second hand therapy equipment
We would like to offer parents and therapists the opportunity to advertise second hand therapy equipment on our website. The idea is to create a platform for items for sale and items needed.
Therapy equipment should be in good working order and may not include AFOs and other items specifically fitted for an individual.
There will be no cost for this service. The adverts will be posted on the SANDTA website but SANDTA will not act as an agent in the transfer of goods or money.
Contact: [email protected] if you are interested.
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 14
CPD articles on the SANDTA website
We encourage you to access the CPD articles available to SANDTA members on the website (www.sandta.org.za). By reading an article and answering the multiple choice questions you can earn 3 CPD points. New articles have been loaded and can be accessed until the end of the year:
1) Efficacy of Constraint-Induced Movement Therapy for children with Cerebral Palsy with asymmetric motor impairmentAuthor: Taub, E et al (2004) Source: Pediatrics 2004; 113; 305
2) The EXCITE Stroke Trial, Comparing Early and Delayed Constraint-Induced Movement TherapyAuthor: Wolf, L et al (2010) Source: AHA Journals 101161
3) Self-efficacy and self-management after stroke: a systematic review Author: Jones F & Riazi A (2011) Source: Disability and Rehabilitation 33 (10) 797-810
4) The Rehabilitation Model of Care: When Old Becomes NewAuthor: Stolp K (2011) Source: American Academy of Physical Medicine &
Rehabilitation (3) 289-292
5) Virtual reality games for rehabilitation of people with stroke: perspective from usersAuthor: Lewis GN et al (2011) Source: Disability and Rehabilitation: Assistive
Technology 6(5) 453-463
6) Applying the ICF-CY to identify children’s everyday life situations: A step towards participation-focused code sets InternationalAuthor: Adolfsson M (2012) Source: Journal of Social Welfare ISSN 1369-6866 1012
7) Applying the International Classification of Functioning, Disability and Health (ICF) to measure childhood disabilityAuthor: Simeonsson RJ (2003) Source: Disability and Rehabilitation (25) 602-610
Online CPD ProcedureThe current set of seven academic articles are available until the end of December after which a new set will be loaded. The website features online submission of CPD article answers with instant scoring of your multiple choice answers. Each article is accredited with 3 CPD points.
Steps to follow:– Go to www.sandta.org.za – Go to the 'member's section' and log in with your SANDTA membership number and
password.– Select the CPD article by clicking the 'more' button associated with the article you wish
to access.– Download or open the article by clicking the 'view article' or 'download article' button. – Read the article. – Answer the articles questions displayed on that article's page and submit.Please ensure that your email address on your SANDTA website profile is correct.
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 15
SOUTH AFRICAN NEURODEVELOPMENTAL THERAPY ASSOCIATION NEWSLETTER 16
Newsletter deadline
Submissions for the newsletter must reach the editor by
30 January 2014
Please email submissions to [email protected]
Contact details for all National SANDTA administration queries:email- [email protected] 051 436 8145fax- 051 436636fax to email: 086 275 2869
Please let the office know of any changes to your contact details. Kindly also send a copy to your local branch.
Members are reminded to log on towww.sandta.org.za to update your profile. This is a useful way of contacting other NDT professionals and making referrals. It also allows the association to communicate regularly with members.
Submissions for the SANDTA newsletter
To simplify editing please use Word documents or plain text
Paper size – A4.Font: Arial
Font size: Titles 14 pt.Body of document: 11 pt.
Any photos/pictures to be sent separately from the text with a labelled text box in the document at insertion
point.
BRANCH CONTACTS
SOUTHERN GAUTENGPam [email protected]
NORTHERN GAUTENGEsedra [email protected]
KWAZULU-NATALVanessa [email protected]
WESTERN CAPEBronwen [email protected]
EASTERN CAPESarita [email protected]
FREE STATEMarieta [email protected]
FREE STATE GOLDFIELDS(interest group)Rina van [email protected]