specialising in disability - compliant learning resources · 2019-05-03 · 1.2 supporting...
TRANSCRIPT

CHC33015 Certificate III in Individual Support
Specialising in Disability
Support and Empowerment
of People with Disability
Version 1.0 Produced 15 July 2016
Copyright © 2016 Compliant Learning Resources. All rights reserved. No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database or retrieval system other than
pursuant to the terms of the Copyright Act 1968 (Commonwealth), without the prior written permission of Compliant Learning Resources.
Le
ar
ne
r G
uid
e 4
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 2 © Compliant Learning Resources
Version control & document history
Date Summary of modifications made Version
15 July 2016 Version 1.0 final produced following
validation v1.0
SA
MPL
E
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 3
TABLE OF CONTENTS
This is an interactive table of contents. If you are viewing this document in Acrobat,
clicking on a heading will transfer you to that page. If you have this document open
in Word, you will need to hold down the Control key while clicking for this to work.
LEARNER GUIDE......................................................................... 5
I. CONTRIBUTING TO ONGOING SKILLS DEVELOPMENT .................... 13
1. Contributing to Skills Assessment ................................................ 18 1.1 Observing the Person’s Skills and Competencies ....................................... 19 1.2 Supporting Engagement of Family and Carers in Skills Assessment......... 20 1.3 Recording Observations Accurately and Objectively.................................. 20 1.4 Working with Your Supervisor.................................................................... 21
2. Assisting with Ongoing Skills Development .................................. 22 2.1 Encouraging the Person with Disability to Engage as Actively as Possible in All Activities ........................................................................................ 22 2.2 Interpreting and Following Skills Development Strategies in the Individualised Plans .............................................................................................. 25 2.3 Encouraging and Assisting the Person to Identify Personal Strengths and Personal Goals ................................................................................................ 30 2.4 Providing Support to Identify Resources to Complement Strengths ............ 30 2.5 Providing Positive Support and Constructive Feedback ................................ 32 2.6 Monitoring Strategies and Discussing Difficulties to Determine Effectiveness of Skills Development Activities ..................................................... 36
3. Supporting Incidental Learning Opportunities ............................. 38 3.1 Providing Encouragement in Real-Life Situations ..................................... 39 3.2 Positive Approaches and Strategies in Promoting Enjoyment and Maximising Engagement ....................................................................................... 39 3.3 Withdrawing Support to Encourage Experiential Learning ......................40
II. FOLLOWING PERSON-CENTRED BEHAVIOUR SUPPORTS .............. 41
1. Applying a Person-Centred Approach ........................................... 42 1.1 Supporting the Person in Maintaining their Activities for Daily Living (ADLs) ........................................................................................................ 44 1.2 The Person’s Individual Needs, Strengths, Capabilities, and Preferences ............................................................................................................ 49 1.3 Potential Problems with Engaging or Motivating the Person .................... 50 1.4 Providing a Safe Environment for the Person ............................................ 51
2. Behaviours of Concern and their Contexts .................................... 52 2.1 Recognising Behaviours of Concern ........................................................... 53 2.2 Consider the Context of the Behaviour of Concern .................................... 57 2.3 Recording All Observations Accurately and Objectively ............................ 59
3. Providing Positive Behaviour Support .......................................... 63 3.1 Recognising Appropriate and Inappropriate Interventions to Behaviours of Concern .......................................................................................... 64 3.2 Responding to Critical Incidents Accordingly ............................................ 70 3.3 Monitoring Strategies and Reporting the Person’s Changing Needs and Behaviours ...................................................................................................... 71 3.4 Following Referral Procedures .................................................................... 72 SA
MPL
E
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 4 © Compliant Learning Resources
III. SUPPORTING COMMUNITY PARTICIPATION AND SOCIAL INCLUSION
............................................................................................... 73
1. Opportunities for Community Participation and Social Inclusion . 77 1.1 Assisting in Identifying the Interests, Abilities, and Requirements of the Person with Disability to Engage in a Social Network .................................... 77 1.2 Providing Information on and Accessing Community Participation Options, Networks, Services and Other Resources to Meet the Person’s Needs and Wants ................................................................................................... 78 1.3 The Cultural and Religious Needs of the Person with Disability ............... 79
2. Strategies for Community Participation and Social Inclusion ...... 80 2.1 Strategies for Strengthening Options, Networks, and Services ................. 81 2.2 Continuous Improvement in Support Services .......................................... 82
3. Addressing Barriers to Community Participation and Social Inclusion ............................................................................................ 83
3.1 Recognising Physical, Skill, and Other Barriers to Community Participation and Social Inclusion ........................................................................ 83 3.2 Collaborating with the Person with Disability to Identify and Implement Solutions in Overcoming Barriers ...................................................... 85 3.3 Monitoring the Success of Strategies Used in Overcoming Barriers ......... 86 3.4 Recognising Own Limitations in Addressing Issues .................................. 86
IV. FACILITATING EMPOWERMENT OF PEOPLE WITH DISABILITY .... 88
1. Demonstrating Your Commitment in Empowering People with Disability ........................................................................................... 92
1.1 Changes in the Legal, Political, and Social Frameworks ............................ 93 1.2 Your Own Personal Values and Attitudes Regarding Disability ................ 95
2. Fostering Human Rights ............................................................... 97 2.1 Assisting the Person with Disability to Understand their Rights ............... 97 2.2 Indications of Possible Abuse and Neglect ................................................. 98
3. Facilitating Choice and Self Determination ................................. 102 3.1 Using the Person-Centred Approach in Empowering the Person with Disability .............................................................................................................. 102 3.2 Advocacy Services and Complaint Mechanisms ....................................... 105
CONCLUSION .......................................................................... 107
What have we learned? ........................................................................................... 107 What next? .............................................................................................................. 107
FEEDBACK ......................................................................... 108
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 5
LEARNER GUIDE
Unit Description
CHCDIS001 – Contribute to ongoing skills development using a strengths-based approach
This unit describes the skills and knowledge required to assist with supporting the ongoing skill development of a person with disability. It involves following and contributing to an established individual plan and using a positive, strengths-based approach.
CHCDIS002 – Follow established person-centred behaviour supports
This unit describes the skills and knowledge required to implement behaviour support strategies outlined in an individualised behaviour support plan for a person with disability.
CHCDIS003 – Support community participation and social inclusion
This unit describes the skills and knowledge required to assist with supporting people with disability in community participation and social inclusion using a person-centred approach. This involves enabling people to make choices to maximise their participation in various community settings, functions and activities to enhance psychosocial well-being and lifestyle in accordance with the person’s needs and preferences.
CHCDIS007 – Facilitate the empowerment of people with disability
This unit describes the skills and knowledge required to facilitate the empowerment of people with disability to deliver rights based services using a person-centred approach. It should be carried out in conjunction with individualised plans.
This unit applies to workers in varied disability contexts.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 6 © Compliant Learning Resources
About this Unit of Study Introduction
As a worker, a trainee, or a future worker you want to enjoy your work and become
known as a valuable team member. This unit of competency will help you acquire the
knowledge and skills to work effectively as an individual and in groups. It will give
you the basis to contribute to the goals of the organisation which employs you.
It is essential that you begin your training by becoming familiar with the industry
standards to which organisations must conform.
These units of competency introduce you to some of the key issues and
responsibilities of workers and organisations in this area. The unit also provides you
with opportunities to develop the competencies necessary for employees to operate
as team members.
This Learner Guide Covers
Contributing to Ongoing Skills Development
1. Contributing to Skills Assessment 2. Assisting with Ongoing Skills Development 3. Supporting Incidental Learning 4. Completing Workplace Documentation
Following Person-Centred Behaviour Supports
1. Applying a Person-Centred Approach 2. Behaviours of Concern and their Contexts 3. Providing Positive Behaviour Support
Supporting Community Participation and Social Inclusion
1. Opportunities for Community Participation and Social Inclusion 2. Strategies for Community Participation and Social Inclusion 3. Addressing Barriers to Community Participation and Social Inclusion
Facilitating the Empowerment of People with Disability
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 7
Learning Program
As you progress through this unit of study you will develop skills in locating and
understanding an organisation’s policies and procedures. You will build up a sound
knowledge of the industry standards within which organisations must operate. You
will become more aware of the effect that your own skills in dealing with people has
on your success or otherwise in the workplace. Knowledge of your skills and
capabilities will help you make informed choices about your further study and career
options.
Additional Learning Support
To obtain additional support you may:
Search for other resources. You may find books, journals, videos and other
materials which provide additional information about topics in this unit.
Search for other resources in your local library. Most libraries keep
information about government departments and other organisations, services
and programs. The librarian should be able to help you locate such resources.
Contact information services such as Infolink, Equal Opportunity
Commission, Commissioner of Workplace Agreements, Union organisations,
and public relations and information services provided by various government
departments. Many of these services are listed in the telephone directory.
Contact your facilitator.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 8 © Compliant Learning Resources
Facilitation
Your training organisation will provide you with a facilitator. Your facilitator will
play an active role in supporting your learning. Your facilitator will help you any time
during working hours to assist with:
How and when to make contact,
What you need to do to complete this unit of study, and
What support will be provided.
Here are some of the things your facilitator may do to make your study easier:
Give you a clear visual timetable of events for the semester or term in which
you are enrolled, including any deadlines for assessments.
Provide you with online webinar times and availability.
Use 'action sheets' to remind you about tasks you need to complete, and
updates on websites.
Make themselves available by telephone for support discussion and provide
you with industry updates by e-mail where applicable.
Keep in touch with you during your studies.
Flexible Learning
Studying to become a competent worker is an interesting and exciting thing to do.
You will learn about current issues in this area. You will establish relationships with
other students, fellow workers, and clients. You will learn about your own ideas,
attitudes, and values. You will also have fun. (Most of the time!)
At other times, studying can seem overwhelming and impossibly demanding,
particularly when you have an assignment to do and you aren't sure how to tackle it...
and your family and friends want you to spend time with them... and a movie you
want to see is on television....
Sometimes being a student can be hard.
Here are some ideas to help you through the hard times. To study effectively, you
need space, resources, and time.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 9
Space
Try to set up a place at home or at work where:
1. You can keep your study materials,
2. You can be reasonably quiet and free from interruptions, and
3. You can be reasonably comfortable, with good lighting, seating, and a flat
surface for writing.
If it is impossible for you to set up a study space, perhaps you could use your local
library. You will not be able to store your study materials there, but you will have
quiet, a desk and chair, and easy access to the other facilities.
Study Resources
The most basic resources you will need are:
1. A chair
2. A desk or table
3. A computer with internet access
4. A reading lamp or good light
5. A folder or file to keep your notes and study materials together
6. Materials to record information (pen and paper or notebooks, or a computer
and printer)
7. Reference materials, including a dictionary
Do not forget that other people can be valuable study resources. Your fellow workers, work supervisor, other students, your flexible learning facilitator, your local librarian, and workers in this area can also help you.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 10 © Compliant Learning Resources
Time
It is important to plan your study time. Work out a time that suits you and plan
around it. Most people find that studying in short, concentrated blocks of time (an
hour or two) at regular intervals (daily, every second day, once a week) is more
effective than trying to cram a lot of learning into a whole day. You need time to
'digest' the information in one section before you move on to the next, and everyone
needs regular breaks from study to avoid overload. Be realistic in allocating time for
study. Look at what is required for the unit and look at your other commitments.
Make up a study timetable and stick to it. Build in 'deadlines' and set yourself goals
for completing study tasks. Allow time for reading and completing activities.
Remember that it is the quality of the time you spend studying rather than the
quantity that is important.
Study Strategies
Different people have different learning
'styles'. Some people learn best by
listening or repeating things out loud.
Some learn best by 'doing', some by
reading and making notes. Assess your
own learning style, and try to identify any
barriers to learning which might affect
you. Are you easily distracted? Are you
afraid you will fail? Are you taking study
too seriously? Not seriously enough? Do
you have supportive friends and family? Here are some ideas for effective study
strategies:
Make notes. This often helps you to remember new or unfamiliar information. Do
not worry about spelling or neatness, as long as you can read your own notes. Keep
your notes with the rest of your study materials and add to them as you go. Use
pictures and diagrams if this helps.
Underline key words when you are reading the materials in this learner guide. (Do
not underline things in other people's books.) This also helps you to remember
important points.
Talk to other people (fellow workers, fellow students, friends, family, or your
facilitator) about what you are learning. As well as helping you to clarify and
understand new ideas, talking also gives you a chance to find out extra information
and to get fresh ideas and different points of view. SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 11
Using this Learner Guide
A learner guide is just that, a guide to help you learn. A learner guide is not a text
book. Your learner guide will:
1. Describe the skills you need to demonstrate to achieve competency for this
unit;
2. Provide information and knowledge to help you develop your skills;
3. Provide you with structured learning activities to help you absorb knowledge
and information and practice your skills;
4. Direct you to other sources of additional knowledge and information about
topics for this unit.
How to Get the Most Out of Your Learner Guide
Read through the information in the learner guide carefully. Make sure you
understand the material.
Some sections are quite long and cover complex ideas and information. If you come
across anything you do not understand:
1. Talk to your facilitator;
2. Research the area using the books and materials listed under Resources;
3. Discuss the issue with other people (your workplace supervisor, fellow
workers, fellow students);
4. Try to relate the information presented in this learner guide to your own
experience and to what you already know.
5. Ask yourself questions as you go. For example, 'Have I seen this happening
anywhere?' 'Could this apply to me?' 'What if....’ This will help you to 'make
sense' of new material, and to build on your existing knowledge.
6. Talk to people about your study.
7. Talking is a great way to reinforce what you are learning.
8. Make notes.
9. Work through the activities.
Even if you are tempted to skip some activities, do them anyway. They are there for a
reason, and even if you already have the knowledge or skills relating to a particular
activity, doing them will help to reinforce what you already know. If you do not
understand an activity, think carefully about the way the questions or instructions
are phrased. Read the section again to see if you can make sense of it. If you are still
confused, contact your facilitator or discuss the activity with other students, fellow
workers or with your workplace supervisor.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 12 © Compliant Learning Resources
Learning Checkpoints
This learner guide contains learning checkpoints which are represented by the
following icons:
Checkpoint! Let’s Review
Further Reading
Further Reading checkpoints direct you to external resources that are highly
recommended for you to read. They also contain additional questions to facilitate
supplementary learning and to guide you relate what you have read in real life.
Checkpoint! Let’s Review contain review questions for you to answer on your own
to ensure that you have learned key points from the relevant section. If you have a
hard time answering these questions, worry not. You can always revisit chapters and
take another shot at these review questions.
Additional Research, Reading, and Note-Taking
If you are using the additional references and resources suggested in the learner
guide to take your knowledge a step further, there are a few simple things to keep in
mind to make this kind of research easier.
Always make a note of the author's name, the title of the book or article, the edition,
when it was published, where it was published, and the name of the publisher. This
includes online articles. If you are taking notes about specific ideas or information,
you will need to put the page number as well. This is called the reference
information. You will need this for some assessment tasks, and it will help you to find
the book again if you need to.
Keep your notes short and to the point. Relate your notes to the material in your
learner guide. Put things into your own words. This will give you a better
understanding of the material.
Start off with a question you want answered when you are exploring additional
resource materials. This will structure your reading and save you time.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 13
I. CONTRIBUTING TO ONGOING SKILLS
DEVELOPMENT
In Learner Guide 1, 2, and 3, we focused on the many roles and responsibilities of the support worker in the provision of care and support to clients. These roles and responsibilities include supporting the client’s indepencence and well-being, working legally and ethically, and working in health and community services, including being able to work with diverse people and communicating effectively.
This Learner Guide will focus on the key knowlwedge and skills of the support worker in working in the disability support context, including:
Contributing to ongoing skills development of a person with disability using a strengths-based approach;
Following peron-centred behaviour supports; Supporting the person’s community participation and inclusion; Facilitating empowerment of people with disability.
This section of the Learner Guide will cover key knowledge and skills in contributing to ongoing skills development of a person with disability using a strengths-based approach.
Before proceeding, let’s try to understand more about some of the practices, philosophies, and theories behind disability and the provision of disability support.
What are the first few words, ideas, and thoughts that come in to your mind when you hear the word disability?
Let’s take a look at the World Health Organization’s definition of disability, and see if any of it is similar to your answers:
(Sourced from www.who.int)
Disability or disabilities
It is an umbrella term, covering impairments, activity limitations, and participation restrictions. An impairment is a problem in body function or structure; an activity limitation is a difficulty encountered by an individual in executing a task or action; while a participation restriction is a problem experienced by an individual in involvement in life situations. SA
MPL
E
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 14 © Compliant Learning Resources
Changing Attitudes Towards Disability
There are two models of disability – the medical and social model. These two models provide view disability differently, and each model provides a framework of how disability support services are designed and delivered.
Medical Model of Disability
Long ago, disability or disabities are seen as medical problems to be fixed or incapacities of the person – something that he can’t do or is not able to do. This views and attitudes towards disability fall under the Medical Model of Disability. This model says that people are disabled because of their impairments and must be fixed or treated through medical interventions. It focuses on what is ‘wrong’ with the person instead of what the person needs.
These views and attitudes have created low expectations on people with disability and has often led to people losing independence, choice, and control in their own lives. This traditional model of disability does not take into consideration the individual’s experience of living with a disablity nor does it help to develop more inclusive ways of living. Because of this, the social model of disability has been developed.
Social Model of Disability
As opposed to the medical model of disability, the social model of disability, a fairly recent development in the sector, says that disability is not caused by the impairment or difference but rather it is caused by the way the society is organised – that the society today contains barriers that restrict people with disabilities from fully enjoying their lives.
This model views ‘disability’ as the result of people living with impairments interacting in an environment with physical, attitudinal, communication and social barriers. An example of these barriers includes the lack of ramps to the entrance of buildings making it difficult for a wheelchair user to get inside these buildings.
The approach of this model is mainly on fixing these barriers in society, rather than trying to ‘fix’ the person’s disability.
Other examples or scenarios applying the social model of disability include:
A person who has an intellectual disability wants to live independently in his own home. Under the social model, the person will be given support and options to enable him to do this. While under the medical model, this person might be recommended to live in a communal home.
A girl who has a visual impairement would love to read a book. A solution using the social model approach would include making the full-texts audio recording version of the book. This way, regardless of this impairment, the girl can still enjoy the book she wanted to read.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 15
Other practices, philosophies, and theories behind disability and the provision of disability support include:
Social Devaluation This is the belief of society that a person or a group of people with disabilities cannot contribute to society as much as those with no disability. As a result, people living with disabilities are viewed as having less value than others. Below are some examples of how social devaluation impact the person’s quality of life:
Depression
Thinking that they are a burden to others
Low self-esteem and less confidence
Negative self-image
Strengths-Based Practice It focuses on what a person living with disability can do, rather than what he/she cannot do. Part 1 of the Learner Guide will discuss this practice further into detail as it is applied in the ongoing skills development of the person with disability.
Active Support Active support enables and empowers people with disabilities to participate in all aspects of their lives.
Person-Centred Practice It sees the person with a disability as an individual rather than a sick person. The person must also be valued and is worthy of respect no matter their disability.
Social Devaluation
Strengths-Based Practice
Active Support
Person-Centred Practice
Community Education
Capacity Building
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 16 © Compliant Learning Resources
Community Education This includes programs to promote learning and social development work with individuals and groups in their communities using formal and informal teaching and learning methods.
Capacity Building It is developing a person’s skills and capabilities to promote his/her independence. It is demonstrated through doing a task with the person rather than doing a task for that person.
Other Concepts in Disability Support
The following concepts are encountered in the provision of support to people with disability.
Vulnerability
This is the characteristic of being easily hurt or attacked by others. People with disability are oftentimes vulnerable to discrimination and bullying in different settings (e.g. education, corporate, community), and even abuse and neglect by others.
Power
In the context of disability support, this is the ability and capacity of the person with disability to decide on matters relevant to his/her support. This power enables the person to enjoy and gain control over his/her life.
Independence
Independence or inependent living is living, working, playing just like everyone else with minimum support from others. Independence of people with disability are promoted through the use of aids and equipment and through skills development.
Interdependence
This is the mutal reliance between the person with disability and others (e.g. family, carer, support worker). In this concept, the person with disability does not take a passive role in the provision of his/her support, but instead, he/she takes an active part which the family, carers, and support workers also depend on. SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 17
Principles of Access and Equity
Today, practices, legal and ethical considerations, and standards in the provision of disability support services align with the principles of acess and equity. Support workers and support service providers aim to provide services in accordance with these principles.
What is Access and Equity?
(Sourced from www.opendoors.net.au)
In detail,
Access means services should be available to everyone who is entitled to them and hsould be free of any form of discrimination regardless of the person’s country of birht, language, culture, race, religion or disability.
While Equity means services should be developed and delivered on the basis of fair treatment of clients who are eligible to receive them.
Checkpoint! Let’s Review 1. Think of examples of situations or scenarios in disability
support that demonstrates the following concepts: Vulnerability Interdependence
2. In your own words, briefly explain the following concepts,
for each concept: Person-Centred Practice Capacity Building Community Education
3. Explain the difference between the medical and social
model of disability.
Now that you have been introduced to the concepts, practices, theorires in disability and in the provision of disability support, let us proceed to discussing the key practical skills needed for a support worker to contribute to a client’s ongoing skills development.
Access and Equity
means ensuring all Australians, regardless of racial, religious, cultural or language backgrounds, or disability enjoy full access to services that they are entitled to.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 18 © Compliant Learning Resources
1. Contributing to Skills Assessment
All throughout this part, we have mentioned terminologies such as skills development and strenghts-based practice. Earlier, we said strenghts-based practice focuses of what the person with disability can do instead of what the person cannot do. This approach or practice is just one in many approaches used in developing the skills of people with disability. Why is ongoing skills development for people with disability important? Number 1, as we have discussed just earlier, the views and attitudes towards disability is shifting tremendously from the medical model towards the social model of disability; and Number 2, skills development is in line with a number of legal and ethical considerations, including dignity of risk, as well as the emerging practices in disability support, including person-centred practice and empowering the client’s. Ongoing skills development using a strengths-based approach may relate to the following depending on the needs, goals, and preferences of the person:
Skills development aims to empower the people with disability through strategies, techniques, and meaningful activities that focus on the person’s strengths, skills, and competencies.
Life skills
Vocational skills
Social skills
Personal support skills
Developing and maintaining relationships including
intimate relationships
Maintaining physical health including sexual health
Safety SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 19
Skills Assessment Processes
In order to determine in which strategies, techniques, and activities the person with disability can benefit the most, his/her existing skills and competencies are first assessed – what can he do? what are the areas for improvement? what does he enjoy doing?
In the skills assessment processes the following factors are considered:
The person’s dreams and aspirations Cultural values and expectations Holistic health needs (physical, social, emotional, psychological) The person’s preferred communication method The person’s strengths and capabilities The person’s learning style
This section of the Learner Guide will talk about practical skills in contributing to skills assessment of a person with disability.
1.1 Observing the Person’s Skills and Competencies
Everyone, including people with disability, have different skills and competencies. These skills and competencies can range from a complex skill to a simple one (such as having a friendly personality). Skills and competencies may include:
Communication Personal hygiene Meal preparation
Transport Money handling Dressing and
grooming
Eating Household tasks Recreational activities SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 20 © Compliant Learning Resources
In skills assessment, the skills and competencies, such as outlined above, are observed and documented in a manner that respects the rights of the person with disability. Protocols and processes for observation and documentation of these skills will vary across organisations, however, they must ensure that rights, including the privacy, confidentiality, and dignity of the person with disability is always upheld and respected.
1.2 Supporting Engagement of Family and Carers in Skills Assessment
In line with the views under the social model of disability views, family, friends, and carers are attributed as key contributors in assessment processes. They can provide valuable input and information to the skills assessment processes about the person with disability - as they most probably know the person better than the support staff.
The provision of support is a collaboritve effort among the multi-disciplinary staff (nurses, doctors, support worker, etc.), the person with disability, and his/her family and carers. Supporting the engagement of the client’s family and carers can be done through formal and informal meetings, consultation, questionning, and more.
1.3 Recording Observations Accurately and Objectively
Crucial to the skills assessment in the ongoing skills development is recording the observations on a person’s skills and competencies. Organisations will have specific workplace documents prescribed for this, however, it is required that you are able to record all observations accurately and objectively. This can be done through:
Recording facts rather than opinions
Recording enough detail to capture what exactly happened
Avoiding biases in your description
Use active verbs (action words)
Observing without interpreting (e.g. recording what you saw what the person is doing rather than the reasons why he is doing it)
Avoiding recording something that did not occur
Recording observations in the order they occur.
Considering the context of when and where the observation was made. SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 21
1.4 Working with Your Supervisor
As mentioned, skills assessment is a collaborative effort among you (support worker), the rest of the support staff team, the person with disability, and the person’s family and carers. Part of your contribution to skills assessment is being able to provide feedback to your supervisor in the organisation about any changes in the person’s demonstration of skills in different environments as well as any changes in the person’s status likely to impact on skills development. Processes and protocols for providing feedback relevant to the ongoing skills development of the person with disability will vary across organisations. Ensure that you work in consultation with your supervisor and colleagues, especially with matters that are unclear to you.
Further Reading
The following are some films that portray the lives of different people with disability:
The Theory of Everything (2014) Still Alice (2014) The Sessions (2012) Temple Grandin (2010)
Have you seen any of the films mentioned above? If not, take time to see at least one (1) of the films listed above, and identify three (3) skills and competencies of the person with disability in this movie.
Checkpoint! Let’s Review
1. In your own words, briefly explain skills assessment and its significance in the ongoing skills development of a person with disability.
2. List at least three (3) skills and competencies that a person may have.
3. List three (3) ways you can ensure accuracy and objectivity in recording observations.
SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 22 © Compliant Learning Resources
2. Assisting with Ongoing Skills Development
Earlier, we have learned that skills development can relate to the development of the person’s life skills (e.g. using the public transport), vocational skills, social skills, or personal support skills – depending on the person’s individualised plan.
Can you recall what an individualised plan is from the previous learner guides?
Individualised plans (care plans or support plans) are documentation of client’s information relevant to the provision of his/her own care and support.
Individualised plans across organisations vary greatly, but they usually contain:
the client’s basic information (name, history, condition, allergies if any); the client’s holistic needs (physical, emotional, psychological, and spiritual) the client’s goals in terms of their holistic needs, strategies in supporting and empowering the client to meet their holistic
needs
Skills development must be based on the person’s individualised plan, as part of the strenghts-based and person-centred approach (What are the person’s goals, needs, and preferences? What can he/she do?), in order to plan and implement strategies and activities that are most suited to the person, and at the same time strategies and activities that the person will find most meaningful.
This section of the Learner Guide will discuss about practical skills needed for the disability support worker to contribute and assist with the person’s ongoing skills development.
2.1 Encouraging the Person with Disability to Engage as Actively as
Possible in All Activities
Earlier, we introduced the term Active Support – which is enabling and empowering people with disabilities to participate in all aspects of their lives. In detail, Active support promotes optimum participation in everyday activities of the person’s own life. Active support builds on the person’s strengths and promotes participation, choice, and self-esteem.
Active support is about supporting the person to engage in their life based on their abilities rather than disabilities. It can be used with other support approaches such as person-centred planning, communication planning, and positive behaviour support planning. SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 23
The benefits of active support for people are:
Promotes independence and autonomy
Support choice and control over own life
Supports active participation in physical and mental activities
Supports active participation in relationships
Promotes health and wellbeing
There are three main components to active support and they are:
In line with the provision of active support to people with disability, your role in assisting with their ongoing skills development is to encourage them to engage as actively as possible in all activities.
Found in the next page is a case study that demonstrates application of active support:
Providing the right level of assistance for the person to participate in activities of daily living.
Active Support Plans that outline and organise the tasks that the person is encouraged to complete.
Opportunities include personal care, household duties, participation in social activities of choice and hobbies.
Recording so participation in tasks can be monitored and reviewed for improvements and to inform other
members of the team.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 24 © Compliant Learning Resources
Lulu
Lulu is a thirty-five year old woman with physical and intellectual disability. Lulu loves cooking shows but has never cooked a meal. When meals are cooked, Lulu always watches the staff prepare them. One day, Lulu expressed an interest in cooking; she can make sandwiches and she is very creative at making the sandwiches look attractive and appetising.
To support Lulu to actively participate in cooking, picture cards of different meals are shown to Lulu and from which she can choose from. The pictures cards were developed with input from Lulu, her mother, the support team and Lulu’s Speech and Language Pathologist. The cards are located in a place where Lulu can easily access them.
Due to Lulu’s physical disability she is unable to hold a spoon and bowl when mixing ingredients. Lulu was referred to the physiotherapist. The therapist recommended that she use a spoon with an oversized handle and a non-slip mat to mix ingredients. Lulu now uses these.
The staff provided the right amount of support, ‘not too much and not too little’, and the correct guidance (e.g. verbal prompts, gestures and positive feedback) to meet Lulu’s needs. Lulu has now developed skills in cooking and has developed her strength of making food look attractive.
Lulu now makes cupcakes for family and friends, and everyone comments on how wonderful they look. This has greatly improved her self-esteem and confidence.
Checkpoint! Let’s Review
1. What is an individualised plan? List three (3) details or information contained in an individualised plan.
2. What is the use of individualised plan in the ongoing skills development of the person with disability?
3. List three (3) benefits of active support.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 25
2.2 Interpreting and Following Skills Development Strategies in the
Individualised Plans
When assisting with a person’s skills development, ensure that strategies used are in line with the person’s individualised plan. This is done by aligning strategies and actitivities with the person’s individual goals, needs, preferences, strengths, and requirements.
There are a number of strategies used in skills development. These include teaching and learning strategies, strategies to promote the person’s independence, reinforcing techniques, and prompting and fading. This section of the Learner Guide will discuss each of these strategies.
Teaching and Learning Strategies
The following are different teaching and learning strategies used in skills development:
Role modelling – a strategy for passing knowledge, skills, and values through leading by example rather than verbally talking about these knowledge, skills, and values.
Demonstration – involves showing someone how a particular task or activity is done or how something is used.
Skills component mastery – a strategy that aims to ‘master’ or achieve a level of performance for a particular skill component usually before moving onto another skill component.
For example, the task is baking a cake. Baking a cake is composed of subtasks, such as preparing ingredients, preheating oven, putting the cake batter into the oven, and decorating the cake. The skills component mastery approach to this would be to focus on one subtask first (e.g. preparing ingredientsuntil the learner gains the ‘master’ level of performance for this subtask before moving to the next subtask (e.g. preheating the oven and putting the cake batter into the oven).
Role modelling Demonstration Skills component
mastery
Contextualisation Drama and role
plays Peer education
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 50 © Compliant Learning Resources
1.3 Potential Problems with Engaging or Motivating the Person
The provision of disability support is not an easy and smooth process. There will
always be potential issues, problems, and conflicts along the way including when
engaging with and or motivating the person. These may range from:
personal issues with the person (e.g. client may be too down to engage in any
activity),
communication issues (e.g. language barriers and misunderstanding in
communication)
cultural and religious issues and concerns (e.g. disagreeing beliefs and values
between support worker and client)
legal and ethical concerns (e.g. occurrence of WHS incidents)
issues of non-adherence to organisational policies and procedures (e.g. WHS
procedures not being followed)
When you encounter these issues and concerns while engaging and motivating the
person, it is important that you consult your organisation’s policies and procedures
and act in accordance with the policies and procedures and with your role in the
organisation. Where problems are beyond scope of role ensure that you seek support
from relevant personnel, including supervisor and trusted and experienced co-
workers.
Important! Always work in consultation with supervisors and trusted and experienced co-workers especially about matters unclear to you.
Always act in accordance with legal and ethical requirements as well as with your organisation’s policies and procedures when problems with engaging or motivating the person.
Checkpoint! Let’s Review
Think of at least two (2) problems that you might encounter while engaging and motivating your client.
What possible actions can you take, in line with your role as a support worker, to address these problems?
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 51
1.4 Providing a Safe Environment for the Person
In the person-centred approach to providing behaviour support, it is essential to
provide a safe environment for the person conducive to positive and adaptive
responses. What constitutes a safe environment primarily depends on the person,
his/her needs, preferences, goals, and wants, which can be found in his/her support
plan.
For example, some people’s condition such
as Autism greatly benefit from routines.
When the routine is changed it can cause a
disturbance to the person’s wellbeing. A
safe environment for this person includes
maintaining routines, and when changes
to routines are unavoidable, ensuring that
the person can transition smoothly –
introducing a new task slowly rather than
abruptly.
Other ways to provide and maintain a safe environment for your clients may include
but not limited to:
Controlling stimuli that the person may find unpleasant, e.g. noise.
Respecting the client’s personal space as his/her personal preference
Providing the person with meaningful activities outlined in his/her support
plan.
Enhancing the person’s visual access, making sure that they can see what they
need to see.
Providing and maintaining a safe environment is very important, as the environment
can act as carer and support of the person. It plays a critical role in ensuring that
people’s quality of life is maximised.
Another way of determining what the ‘ideal’ or what the most conducive
environment is for the person, is through consulting with the person’s family and
carers, as they have more knowledge and first-hand experience in supporting the
person. This is usually done in person-centred planning where the support staff
meets with the person and the family and carers of the person to discuss matters
relevant to the provision of support.
Whatever approach or strategy you use in providing and maintaining a safe
environment for the person, always ensure that they align with your client’s support
plan, organisational policies and procedures, and legal and ethical requirements.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 52 © Compliant Learning Resources
Further Reading
Dementia is a chronic or persistent disorder of the mental processes caused by brain disease or injury and marked by memory disorders, personality changes, and impaired reasoning. It not only affects older people but it also affects people under 60 years old. This type of dementia is called young onset dementia and is considered a disability.
The following link will direct you to a resource about reducing behaviours of concern of people living with dementia.
ReBOC Reducing Behaviours of Concern
The link includes information about providing a safe environment for people living with dementia (See page 18, Environment).
Checkpoint! Let’s Review
1. Briefly discuss what is meant by ‘safe environment’ for a person with disability.
2. In what ways can you provide a safe environment for the person?
Now that you are acquainted with the use of the person-centred approach in providing behaviour support, we will delve further into behaviours of concern.
2. Behaviours of Concern and their Contexts
Earlier we briefly explained what behaviour is and what behaviours of concern are.
As a recap, behaviours of concern (BOC) are those behaviours that are considered to
be those behaviours that are challenging, harmful, and or disruptive.
In detail, behaviour of concern is defined as:
(Sourced from www.dbmas.org.au)
... is any behaviour which causes stress, worry, risk of actual harm to the person or their carers, staff, family members, and others around them... SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 53
There are models used to explain and understand why these behaviours of concern
occur. One of these is the model regarding the person’s unmet needs. In this model, a
person is explained to exhibit behaviours of concern when their needs are not met,
such as hunger, thirst, pain, social and environmental needs, and other’s needs.
Behaviours of concerns, therefore, can be considered as indicators that a person has
needs unmet.
Below are examples of behaviours of concern as indicators of unmet needs for people
with disability.
A person with disability hurting himself/herself (e.g. hitting, or scratching).
A person with disability refusing to do things – eating or taking medication.
A person with disability shouting and screaming for no apparent or observable
reason.
A person with disability hiding from or avoiding other people.
Further Reading
Read further about behaviours of concern and the four (4) models used to explain and understand them through this link: ReBOC Reducing Behaviours of Concern (See pages 6 – 9)
2.1 Recognising Behaviours of Concern
In disability support, behaviours of concern are typically identified in the person’s
behaviour support plan.
What is a behaviour support plan?
According to www.communities.qld.gov.au, a behaviour support plan
summarises the three elements of positive behaviour approach:
Understanding why the person engages in challenging behaviour
Finding environmental causes for challenging behaviour, and then modifying
them so that the behaviour is unnecessary.
Teaching the person new skills to meet their needs without having to resort to
challenging behaviour.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 54 © Compliant Learning Resources
The behaviour support plan is used to describe the practical ways of effectively
supporting the person who engages in behaviours of concern.
Specifically, the behaviour support plan must clearly describe:
why the person uses challenging behaviour;
how the environment must be modified to make this behaviour unnecessary;
specific approaches to teaching the person new skills so that they do not have
to rely on challenging behaviour to have their needs met;
what the objectives of the plan are; and
How all people in the person's life (i.e. their ‘team’), will contribute to
implementing the plan.
Important! Where behaviour of person with disability is
encountered and considered to be harmful and puts others at
risk and this behaviour is not identified or documented in the
support plan, the support worker must notify the supervisor
immediately. Ways of reducing this behaviour of concern should
be identified in consultation with supervisor, other specialists,
and the person’s family members and carers.
Found below is a sample of a behaviour support plan:
Positive Behaviour Support Plan
Name of service provider who will use this plan:
Lotus Compassionate Care
First Name: Lester Surname: Dorne
Date of Birth: 19 May 1967
Date Plan Written: September 2016 Gender: Male Female
Behaviours of Concern
Hiding away from people
Locking self in a room
Refusing to do things, refusing to eat and take medication
Property damage, breaking things
Statement of Hypotheses
Lester becomes anxious when there are too many people present in the room, when people come too
close to his personal space, when he hears too much noise, specifically when a lot of people are
talking at the same time. He does not like it when he hears people screaming and shouting and SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 55
talking aggressively. As a result, he walks out and locks himself in his room for hours, refusing to eat
and take medication for long periods of time.
He gets nervous and angry when he hears people screaming and shouting, and at times like these, the
resolves to throwing and breaking things.
This is hypothesised to be the result of past experiences of abuse from his stepfather.
Positive Strategies
Strategy 1: Maintaining and respecting personal space.
Lester is uncomfortable with crowds.
Where this cannot be avoided, assist Lester build rapport with one person first.
Allow a minute for Lester to know the person and be comfortable with the person.
Ensure that when Lester is with another person maintain supervision at a safe distance that is
not too close to his personal space.
He becomes anxious when people come too close to his personal space. He considers this as an
“invasion” of his personal space.
Staff should maintain a distance about 1 meter from Lester.
Where staff need to come closer (e.g. hygiene and shaving) staff should make eye contact
with Lester and tell him what you need to do, slowly and calmly. E.g. “Can I help you with
your shave” or “Would you like me to help you with that?”
Give about 5 – 10 seconds for Lester to process this information.
When Lester agrees, use positive expressions such as smiling and begin the task slowly and
gradually.
Strategy 2: Provide meaningful and engaging activities for Lester
Where it cannot be avoided to have people in the room,
Redirect Lester’s attention by providing him with meaningful and engaging activities. This
includes giving him a book to read – he likes re-reading the novel True History of the Kelly
Gang by Peter Carey and listening to instrumental jazz through his mp3 player and
earphones.
Lester reacts positively to the following reinforces: smiling and verbal praise.
Provide reassurance to Lester when interacting with people. Introduce Lester first to the
person and assist Lester build rapport with the other person. Maintain supervision at a safe
distance that is not too close to his personal space.
Strategy 3: Provide meaningful and engaging activities for Lester
Lester will be provided with regular community access support to join in with community activities and
explore interest such as walking to the local park and visiting the local library (Cascade Peak Library)
Staff to organise outings with Lester where possible taking into consideration co-tenants and
staffing arrangements.
Staff to be aware of Lester’s outing schedule and remind him if he is going out later that day
as well as prior to activity.
Strategy 3: Awareness of cues of distress
Lester prefers routines and appears to become distressed when there are too many people present in
the room (more than ten (10) people) and when he hears people talking loudly at the same time or
screaming, shouting, and talking aggressively. SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 56 © Compliant Learning Resources
Maintain daily routines
Monitor the room, Lester is comfortable with just one to five other people in the room.
Prepare Lester for a new activity. Ensure he is reminded at least twice of the activity within an
hour prior to the activity.
Monitor Lester for signs of distress, expressions of panic and anxiety and trying to avoid the
crowd.
If you notice Lester becoming distressed, redirect others away from Lester.
From a respectable distance, ask Lester if he is okay.
Redirect Lester to a calming activity, such as flicking through magazines or sitting on the
veranda watching birds.
Strategy 4: Regular health professional review
Lester requires support to attend scheduled appointments with the social worker and with Dr Manu
Karhu (psychiatrist).
Strategy 5: Communication Strategies
An Assessment process to be completed including trial of low and Hi-tech Alternative Augmentative
Communication (AAC) aides scheduled October 2016.
In the above example, the behaviours of concern are identified as well as strategies
that can be used to reduce these behaviours of concern.
Important! As a support worker, it is crucial that you
familiarise yourself with your client’s individualised plans –
these may include the care plan or support plan, behaviour
support plan, health support plan, communication plan, and
others.
Ensure that you complete client’s routines such as assisting with
activities with daily living (ADLs) in accordance with these plans.
If there are matters in the plan that are unclear to you, it is best
to consult with your supervisor and trusted and experienced co-
workers.
It is also important to report any changes relevant to the client’
needs. These may include behaviours of concern not identified in
the plan.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 57
2.2 Consider the Context of the Behaviour of Concern
Behaviours of concern mostly do not happen for no reason. As we’ve discussed
earlier, one model of behaviour of concern explains that these behaviours are often
the result of unmet needs. Apart from these needs, behaviours of concern also
happen because of one factor or a combination of factors:
In addition, when behaviours do occur, the following have to be considered:
what happened before, during and after the behaviour of concern
These are the events and details of these events that led for the behaviour of
concern to happen.
Was the person alone? Was he/she with another person(s)? What were they
talking about and what were they doing? Where was the person when the
behaviour of concern happened?
the type, frequency and triggers of the behaviour
These include a description of the behaviour...
What exactly did the person do? Was it disruptive? Did it pose harm to
others? How many times did the behaviour happen?
...and anything that triggered or prompted the behaviour.
What caused the behaviour? Was there anything in the environment that
caused the behaviour? Where did the behaviour of concern happen?
Physical Emotional
Environmental Medication
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 58 © Compliant Learning Resources
environmental factors in the context of the behaviour
These include the location, the people, the time, the elements present in the
environment (e.g. noise)
Where was the person when the behaviour occurred?
person’s emotional well-being in the context of the behaviour
This is the state of how the person is feeling at the time of the behaviour.
How was the person feeling at the time when the behaviour of concern
happened? Was he calm and collected? Was he sad or happy? Was the
person showing any anger or irritability at that time?
the person’s health status in the context of the behaviour
This is the physical state of the person at the time when the behaviour
occurred.
Was the person experiencing any physical discomfort? Was he in pain? Was
he sick at the time of the behaviour?
the person’s medication in the context of the behaviour
This includes all the factors relating to the medication of the person.
Was he taking any medication at that time? Did he miss any medication? Is
he taking more than his regular dosage? Does the medication include any
side effects? Has the person had any significant changes in their medication
regimen during the last three months?
This is the context of the behaviour. The context needs to be considered and these
questions need to be asked so we steer away from immediately making the wrong
assumptions about people when they engage in behaviours of concern.
When we see someone with a disability engaging in behaviours of concern, we tend
to automatically label that person as ‘irritable’, ‘hot-tempered’, or sometimes ‘crazy’.
Which shouldn’t be, after all the ultimate aim of person-centred behaviour, is to
understand better the person including the behaviour of concern and reasons for
these behaviours of concern, and by understanding the person and the behaviour
better, more effective strategies can be developed in attempts to reduce these SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 59
behaviours. Remember, the behaviour does not automatically make the person; there
might be more reasons to it than meets the eye.
Checkpoint! Let’s Review
1. Identify four (4) factors that contribute to behaviours of concern, and provide at least one (1) example for each.
2. Identify two (2) things that need to be considered when we review the context of the behaviour.
2.3 Recording All Observations Accurately and Objectively
Part of providing person-centred behaviour support is to be able to consider the context of the behaviour of concern – before, during, and after, as well as to be able to record and document the behaviour of concern, in line organisational protocols. A support worker who was present at the time of the behaviour must complete the documentation. He/she does this recording all
of his/her observations when the behaviour of concern occurred – as accurately and objectively as possible. The following are ways on how we can record observations accurately and objectively:
Avoid words that are inherently subjective. Record facts rather than opinions Use active verbs (action words) Observe without interpreting Record only what you see or hear. Avoid recording something that did not
occur. Use words that describe but do not judge Record the behaviour in the order they occur And as what we’ve just discussed, consider the context.
Recording observations in the provision of behaviour support to people with disability may be completed in the client’s progress notes or behaviour chart.
How you will record and document your observations in relation to documenting behaviours of concern will depend on your organisational procedures and protocols. SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 60 © Compliant Learning Resources
These may include the templates or style guides to followed, privacy procedures, or how the records are to be maintained.
Important! In completing documentation in the provision of
behaviour support, you are required, as set within the scope of
your role as a support worker, to adhere to your organisation’s
policies, protocols, and procedures, as well as to legal and ethical
requirements. These include reporting notifiable incidents to
your WHS state/territory regulators, your duty of care, and
privacy and confidentiality considerations.
For example, a support is considered to have failed his/her duty
of care when he/she absentmindedly left a client’s behaviour
chart in a public location where anyone can see the document.
Do note that behaviour charts and any other documents relevant
to the client’s care and support contain private, confidential, and
sensitive information. When a support worker has done this,
he/she failed to fulfil his duty of care because he/she has
compromised his/her client’s privacy, confidentiality, and
dignity.
Found in the following pages are samples of progress notes and behaviour chart.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 61
Progress Notes
Name of service provider who will use this plan:
Lotus Compassionate Care
First Name: Lester Surname: Dorne
Date of Birth: 19 May 1967
Date
and Time Location Notes
Initial
Name and
Title
22 Jul
16
10:15
AM
Lounge
Room
Support worker was preparing the kitchen so
Lester, together with the support worker, can
prepare lunch. Lester was in the lounge room with
Matthew (another client residing at the group
home). Lester was seated on the couch, reading a
new book, while Matthew was watching the
television. Matthew has fallen asleep and his show
ended already. The television was still on and a
movie was about to come up next. The movie
which came up next was a violent one and had
actors shouting in argument, the next scene played
loud gunshots and explosions. The sounds from
the violent movie alarmed Lester and panicked.
Matthew has a hearing impairment and could not
here the movie. The remote control was far from
Lester’s reach and Lester wanted to turn the movie
off. It was stressing him so much. In response,
Lester threw the book he was reading to the
television but missed, he hit a vase instead and
broke it.
The support workers who heard the commotion
rushed to the room and found Lester in great
distress. He was about to throw another object – a
paperweight, to the television, but a support
worker was able to turn the television off using the
remote control. Lester calmed down. The support
worker, while maintaining safe distance, asked
calmly if he was okay and reassured him.
J.A.
(support
worker)
SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 62 © Compliant Learning Resources
Progress Notes
Name of service provider who will use this plan:
Lotus Compassionate Care
First Name: Lester Surname: Dorne
Date of Birth: 19 May 1967
Date
and
Time
Location Description of
Behaviour
Describe what happened
before Intervention(s)
Describe what happened
after the intervention(s)
Communication
method(s) used
Initial
Name
and
Title
22 Jul 16
10:15
AM
Lounge
Room
Throwing objects
(book and
paperweight)
towards the
television.
Support worker was preparing the
kitchen so Lester, together with the
support worker, can prepare lunch.
Lester was in the lounge room with
Matthew (another client residing at
the group home). Lester was seated
on the couch, reading a new book,
while Matthew was watching the
television. Matthew has fallen asleep
and his show ended already. The
television was still on and a movie
was about to come up next. The
movie which came up next was a
violent one and had actors shouting
in argument, the next scene played
loud gunshots and explosions. The
sounds from the violent movie
alarmed Lester and panicked.
Matthew has a hearing impairment
and could not here the movie. The
remote control was far from Lester’s
reach and Lester wanted to turn the
movie off. It was stressing him so
much.
Removed the noise from
the television / turned
the television off.
Maintained safe distance
from Lester
Lester calmed down. Non-verbal communication:
proximity, maintaining safe
distance while asking Lester
if he was okay in a calm
voice.
J.A.
(support
worker)
SA
MPL
E

Learner Guide 4 Version No. 1.0 Produced 13 July 2016 Page 63 © Compliant Learning Resources
Further Reading
Read more about recording observations and completing documentation in the individual support sector through the following link: www.qcal.org.au
3. Providing Positive Behaviour Support
Now that you’ve learned about person-centred approach and behaviour support, let’s
now apply this knowledge in providing positive behaviour supports.
Earlier we defined positive behaviour support as:
(Sourced from www.behavioursolutions.net)
Positive behaviour support, from the definition above is about focusing on the person
rather than the disability or the behaviour of concern. It focuses on the needs of the
person by trying to understand the person and the behaviour better – it attempts to
explain why the reason and the factors that have contributed to the behaviour –
rather than labelling the person as ‘irritable’, ‘hot-tempered’, or ‘just sick’.
A positive behaviour support therefore means applying a person-centred approach in
providing behaviour support. In the succeeding sections we will talk about how
positive behaviour supports are delivered as well as other factors that impact and
surrounds the provision of the support, such as communication factors and
strategies, interventions, strategies for behavioural supports, and many more.
Positive behaviour support's primary goal is to increase quality of life and its secondary goal is
decreasing behaviours of concern.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 64 © Compliant Learning Resources
Checkpoint! Let’s Review 1. Recall from previous sections of this Learner Guide, the
three (3) elements of the person-centred behaviour support.
2. In your own words, explain how the person-centred approach is relevant in the provision of positive behaviour support.
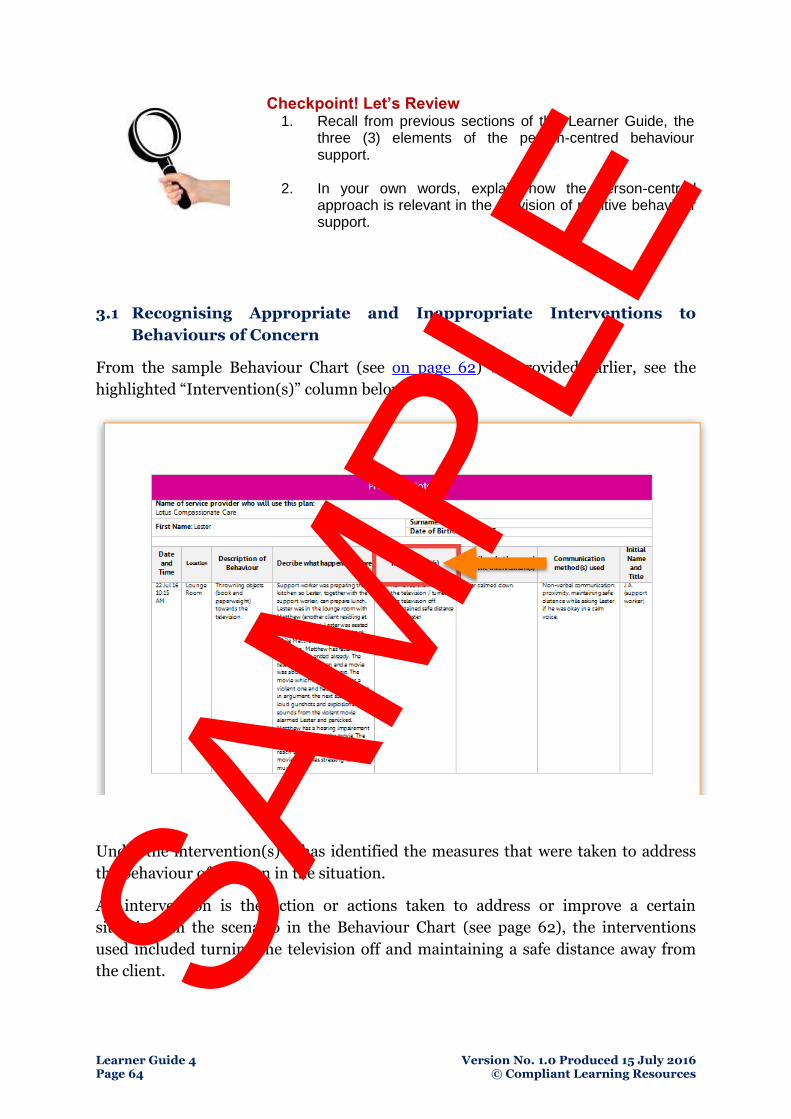
3.1 Recognising Appropriate and Inappropriate Interventions to
Behaviours of Concern
From the sample Behaviour Chart (see on page 62) we provided earlier, see the
highlighted “Intervention(s)” column below:
Under the intervention(s) it has identified the measures that were taken to address
the behaviour of concern in the situation.
An intervention is the action or actions taken to address or improve a certain
situation. In the scenario in the Behaviour Chart (see page 62), the interventions
used included turning the television off and maintaining a safe distance away from
the client. SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 65
Interventions used when addressing behaviours of concern must always be:
In line with legal and ethical requirements, include Work Health and
Safety legislation, UN Convention on the Rights of Persons with
Disabilities, and requirements.
In line with your organisation’s policies and procedures, these are usually
found in your organisation’s staff handbook, manuals, instructional
materials, and other resources.
In line with the person’s behaviour support plan. Read the sample Positive
Behaviour Support Plan (see on page 54) from the previous section and
you will find there strategies that have been identified and prescribed for
use in case the person’s behaviour of concern occurs again.
Always ensure the safety of the person engaging in behaviours of concern,
and the people around him/her, this includes you (the support worker),
other support staff, and other people in the area.
Always maintain, respect, and uphold the client’s dignity.
Note that not all interventions are appropriate. There are appropriate interventions
and others are inappropriate. The above guidelines describe the features of
appropriate interventions used in addressing behaviours of concern. On the other
hand, interventions that violate or do not follow the guidelines outlined above are
inappropriate, and may be considered illegal, unethical, and have legal implications
on the staff or the people using inappropriate interventions. These include abuse in
many forms, physical, verbal, emotional, sexual, psychological, and other forms.
Restrictive Practices
In implementing a behaviour support plan, it may be necessary to use what are called
“restrictive practices”. They are known as this because they would restrict the person
from carrying out their daily life in the way that it is normally conducted and
sometimes taking away the option of choice if that option may cause harm to
themselves or others.
Restrictive Practices are identified as the following examples:
Containment
Seclusion
Chemical restraint
Mechanical restraint
Physical restraint
Restricting access to objects SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 66 © Compliant Learning Resources
In general, a restrictive practice would only be used for the period of time that the
person was at risk of harm either to themselves or others and it would be ceased once
these criteria had passed.
The document that approves the practice and outlines how, when, where and why it
is used is called a Positive Behaviour Support Plan-Restrictive Practice. Plans that
are used to address other behaviours that do not require a restrictive practice are
called Positive Behaviour Support Plans-Non Restrictive. Support workers should
familiarise themselves with these plans and seek clarification from a supervisor if
required.
As a support worker it is your role and responsibility to follow the support plan. If
you have difficulty with implementing a support plan consult with the person and
seek advice from the supervisor, colleagues and professional staff e.g. Speech and
language Pathologist and/or Psychologist.
Important! It is important to note that these restrictive practices have to be authorised and approved. To use a restrictive practice without documented approval could result in a breach of legislation and legal consequences for the organization or the individual support worker.
Restrictive Practices are broken down into the following categories and require
different levels of approval to implement:
Seclusion
this practice means that the person is required to stay in an area without the
ability to leave that area if they are displaying behaviours outlined in the PBSP
that warrant the use of seclusion. It is considered seclusion if the person is in
this area with no other people (including support workers). The area would be
predetermined and documented in the plan to ensure that there was access to
water, toilet, shade etc. There will also be requirements on how long the
person is to remain in seclusion and what checks are to be made while they
are in this area.
An example of this practice may be when a person is agitated and may strike
out at others. They can access an area of the yard where they have the chance
to avoid stimuli that may be disturbing them and others are free from the risk
of harm.
Approval for this practice requires a formally appointed guardian and
generally this would be the Office of the Adult Guardian. SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 67
Containment
This practice means that the person is limited to a certain area and doesn’t
have the option of leaving that area if they are displaying behaviour outlined
in the PBSP that warrants the use of containment. This differs from seclusion
in that the person has other people in the same area.
An example of this may be when a person is agitated and can calm themselves
by watching a TV program of their choice in the common living area but may
continue to be agitated if they were to be in other parts of the home.
Approval for this practice requires a formally appointed guardian and often
this would be the Office of the Adult Guardian
Chemical Restraint
This generally means that the person requires prescribed medication to
alleviate the feelings of agitation that they are experiencing. The medication
can either be long term (part of their daily medication regime) or PRN (Pro re
nata or ‘as needed’).
An example of this may be a person who occasionally becomes agitated and
would be assisted to overcome that agitation with a medication designed for
that purpose and administered when the documented signs of agitation were
present.
Approval for this strategy in a PBSP may be authorised by a close family
member or advocate.
Mechanical Restraint – this practice means that some form of equipment has
been approved for use if the situation meets the criteria in the PBSP.
An example of this practice is if a person is showing agitation and hitting their
head against hard objects, a helmet can be fitted to protect them from harm.
Approval for this strategy in a PBSP may be authorised by a close family
member or advocate.
Physical Restraint
This practice means that there has been approval given for a physical response
to behaviour of concern. This is of short duration and applied only in the
situations described in the PBSP. It can take many forms including guiding a
hand away from an object, gently turning the person in a direction away from
where they were headed or holding a person to prevent them harming SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 68 © Compliant Learning Resources
themselves or others. Physical restraint that is not approved can be
determined to be abuse so ensure all practices used are approved in the PBSP.
An example of this practice is when a person is agitated and showing that they
may be going to strike at a person where they are headed. The PBSP would
approve that you hold their shoulders gently and turn them in another (safer)
direction.
Approval for this strategy in a PBSP may be authorised by a close family
member or advocate.
Restricted access to objects
This practice means that some objects may be withheld form the person either
continually or at certain times. A person should normally have access to items
either wholly or partially owned by them. Restricting access to those objects
must be approved in a plan and the reasons for doing so documented.
Restricted access to objects can cover a range of items that have been regarded
as potentially able to cause harm to the individual or others. It may only be at
certain specific times that these objects should be unavailable.
An example of this practice may be that scissors are only available when the
person can be closely supervised as there have been documented instances
when the individual has used them for self-harm.
Approval for this strategy in a PBSP may be authorised by a close family
member or advocate.
The primary purpose of a PBSP is to ensure that the person is free from the
potential to cause harm and that there are strategies in place to gradually
diminish the need for restrictive practices. When the audit was undertaken
for restrictive practices after the legislation was passed, over 75% of those
practices were deemed to be unnecessary and were then ceased.
As a support worker, you should be continually checking that no unapproved
restrictive practices are in place and report any observations to your
supervisor.
It is important you have a working knowledge and awareness of the
organisations policy and procedures in restrictive practices that will outline
the requirements for your state
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 69
In using interventions the following legal and ethical considerations are taken into
account:
Constraint - This involves restraining a person with disability for reasons
other than medical necessity or the absence of a less restrictive alternative to
prevent self-harm.
Imprisonment - This involves isolating a person with disability for reasons
other than medical necessity or the absence of a less restrictive alternative to
prevent self-harm.
Practice Standards - To ensure that everyone receive the same high-quality
and safe support services, disability support workers and service providers
must adhere to these.
Abuse - This can be physical, sexual, or psychological or emotional harm
inflicted to people with disability, and can also include neglect. This is a
violation of the human rights of people with disability.
Checkpoint! Let’s Review
1. Describe appropriate interventions. Discuss how they are different from inappropriate interventions.
2. What are restrictive practices?
Further Reading
Review the following samples provided in this Learner Guide and answer the question that follows:
Sample Behaviour Support Plan (see on page 54) Sample Behaviour Chart (see on page 62)
Is it necessary to use restrictive practices in the scenario provided in the Behaviour Chart? If yes, explain your reasoning, and if no, discuss why it is not necessary.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 70 © Compliant Learning Resources
Effective Communication as Part of Minimising Behaviours of Concern
Appropriate interventions also include effective communication strategies that are in
line with the person’s individualised plan.
Effective communication means...:
Effective communication involves not just choosing the correct words but also
involves many other skills.
Effective communication depends on a number of factors, including but not
limited to the relationship between the sender and receiver, cultural norms,
how the person is feeling at that time, etc.
Effective communication is a mixture of effective verbal and non-verbal
communication techniques.
.... and it can be applied through:
Showing respect
Ensuring the environment does not create barriers
Being aware of cultural norms
Listening to the other person to hear the full message without interrupting
them
Paraphrasing what the person has said to enhance your understanding.
Understanding non-verbal communication.
Listen effectively
Use the clients preferred communication method e.g. picture book
3.2 Responding to Critical Incidents Accordingly
Responding to critical incidents accordingly include using appropriate interventions
to address a behaviour of concern in line with the person’s behaviour support plan
and other legal and ethical requirements.
Critical incidents in the provision of behaviour support also include near-misses,
accidents, and injuries that may have resulted from the behaviour of concern. For
example, a person who throws objects at others is likely to injure others the support
staff and other people around the person. Critical incidents also include abuse,
neglect and exploitation.
SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 71
Important! When dealing with critical incidents such as these, ensure that you:
Adhere to legal requirements, including notifying your supervisor and WHS regulator in the state/territory about notifiable incidents.
Adhere to ethical requirements, including respecting the person’s rights and dignity.
Act in accordance with your role as a support worker, e.g. promptly reporting to supervisor, and seeking support from other relevant personnel.
Adhere to your organisation’s policies and procedures, including WHS procedures.
3.3 Monitoring Strategies and Reporting the Person’s Changing Needs
and Behaviours
Part of providing positive behaviour support also includes monitoring strategies to
determine their effectiveness and reporting the person’s changing needs and
behaviours.
This is done to ensure that behaviour support plans are always updated. Can you
determine if the Sample Behaviour Support Plan (see on page 54) provided in this
Learner Guide needs updating. To determine this, look again at the details in Sample
Behaviour Chart (see on page 62). Take a good look and let’s see if you got it right.
The answer would be... YES! The behaviour support plan needs to be updated. Why?
Because there is no information in the current plan that is about television noise,
specifically violent noises (people arguing and talking aggressively and gunshot
sounds), triggering the client’s behaviour of concern. As you can recall, in the
description of what happened, these noises have triggered the person to engage in
the behaviour support plan.
Why do we need to update the client’s behaviour support plan in this situation? So
that the support staff and the family and carers of the client can think of strategies to
prevent this from happening again. If this trigger has been identified and strategies
have been outlined in addressing this trigger, the support staff would know to do –
this may include maintaining close supervision when the person is in a room with a
television turned on. Other strategies may also include, minimising the volume first
before switching channels, if the person wants to watch television. SAM
PLE
Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 72 © Compliant Learning Resources
3.4 Following Referral Procedures
In providing behaviour support, there are instances when you will be required to
seek support from others – including your supervisor and trusted and experienced
co-workers. In some cases, specialists are also required, as we’ve mentioned in the
section about Restrictive Practices. The type of referrals will also mainly depend on
what the client requires. For example, a client with speech impairment may be
referred to a speech pathologist. A client who has a physical disability may require
the referral to a physical therapist, and clients experiencing emotional and
psychological stress may need the help of a psychologist.
Referral procedures will depend on the organisation’s policies and procedures. It is
important that you fully familiarised yourself with the scope of your role – what your
responsibilities and limitations. So you will have a good idea on what to do in
different situations and you will know if there is a need to consult your supervisor or
refer the concern to specialists. Specialist services may include the following:
Psychologist
Case manager (disability specialty)
Specialist nurse
Speech and language pathologist
Occupational therapist
Social worker SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 73
III. SUPPORTING COMMUNITY PARTICIPATION
AND SOCIAL INCLUSION
In the first two parts of the Learner Guide we have covered on how you, the support
worker, can contribute to the ongoing skills development of using a strengths-based
approach and following person-centred behaviour support.
As a recap, can you recall what strengths-based and person-centred practices are?
Strengths-based approach focuses on what the person living with disability can
do rather than the disability itself. It looks past at the person’s disability and focuses
more on the strengths of the person, what he/she is capable of doing, areas of
improvement, and other potential capabilities. It also involves in organising skills
development activities that empower the person and make best use of the person’s
abilities. This approach can be best illustrated with “doing activities TOGETHER
WITH the person rather than doing activities FOR the person.”
On the other hand, the person-centred based approach is a holistic approach to
providing support to the person with disability. It addresses not only the person’s
physical needs, but other needs as well as well as social, psychological, emotional,
and other needs. It addresses these needs while maintaining and promoting the
person’s dignity, independence, and sense of empowerment.
In line with these approaches to the provision of support to people with disability,
the support staff and other people surrounding the person with disability all have
roles and responsibilities to play in supporting the person’s community inclusion.
This is part of providing support to meet the holistic needs of the person, specifically
the social and at times, spiritual and cultural needs as well.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 74 © Compliant Learning Resources
What does community inclusion mean for people with disability?
How community inclusion is best practised? It can be practised through the
following ways:
Allowing the person to engage in activities that he/she wishes to participate
in. (Engage in meaningful activities)
Recognising and respecting the person’s dignity of risk. (Autonomy)
Upholding the person’s rights while delivering services (Access and equity)
Treating the person with dignity and respect (Person-centred planning)
Taking into consideration the person’s individual wants, needs, goals, and
preferences in planning for his / her support. (Person-centred planning)
Providing sufficient information to person to enable him/her to make
informed decisions about his/her support (Access and equity)
Support and maintain regular contact with friends/groups
Person-centered e.g. person may need a referral to the dentist because of
pain and poor fitting dentures, a speech and language pathologist for
communication aids (other resources that will help the client communicate
and interact better with others).
Community inclusion for people with disability means:
being a part of a community and being accepted by others in this community.
a collaborative effort among the person and the current members of the community.
playing an active part in the activities and processes in the community.
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 75
Notice in the best practice examples above that there are similarities among them.
These similarities are the elements of best practice for community inclusion – in
other words, what makes up a best practice example for community inclusion.
As we’ve mentioned, the people around the person with disability all have roles and
responsibilities to play in supporting community inclusion for the person. These are
very important because the environment which includes you (the support worker),
the support staff, and the family and carers act as the secondary or a passive carer or
support worker for the person with disability. Just imagine what a difference can a
group of supportive and friendly staff and family and carers can do to impact the
quality of life of the person with disability.
Moreover, family, carers and other informal supporters play a central role in caring
for, and supporting, people with disability in Australia. Their involvement affects the
ability of people with disability to access and engage with a range of systems and
services, as well as more broadly, their ability to exercise legal capacity.
(Sourced from Equality, Capacity and Disability in Commonwealth Laws)
Person-centred planning
Strength based practice
Empowerment
Self-determination
Autonomy
Removing barriers
Engage in meaningful activities
Risk management
Skill development and maintenance
Support participation as a member of the community
Access and equity
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 © Compliant Learning Resources Page 107
CONCLUSION
What have we learned?
Congratulations, you’re reached the end of the second learner guide! To summarise
what you have learnt in this subject:
I. Contributing to Ongoing Skills Development
1. Contributing to Skills Assessment
2. Assisting with Ongoing Skills Development
3. Supporting Incidental Learning Opportunities
II. Following Person-Centred Behaviour Supports
1. Applying a Person-Centred Approach
2. Behaviours of Concern and their Context
3. Providing Positive Behaviour Support
III. Supporting Community Participation and Social Inclusion
1. Opportunities for Community Participation and Social Inclusion
2. Strategies for Community Participation and Social Inclusion
3. Addressing Barriers to Community Participation and Social Inclusion
IV. Facilitating Empowerment of People with Disability
1. Demonstrating Your Commitment in Empowering People with Disability
2. Fostering Human Rights
3. Facilitating Choices and Self-Determination
Please review any of the above areas that you are still not familiar with.
What next?
Now that you have completed the Learner Guide 4, you are now ready to commence working through Assessment Workbook 4.
Good luck with your Assessment!
SAM
PLE

Learner Guide 4 Version No. 1.0 Produced 15 July 2016 Page 108 © Compliant Learning Resources
FEEDBACK
Well done for finishing this learner guide. We hope that what you learn will open up new path ways for success in your life. At Compliant Learning Resources we continually strive to improve our resources and heighten the learning experience for you. One way of doing this is seeking your feedback. Your experience is important to us and we are very keen to hear any suggestions or complaints you may have. Click on the button below to let us know what you think of us and our learning resources.
End of Document
CLICK HERE
SAM
PLE