spine deformities
DESCRIPTION
deformitas sipnal, textbook reading orthoTRANSCRIPT
DEFORMITIES OF SPINE
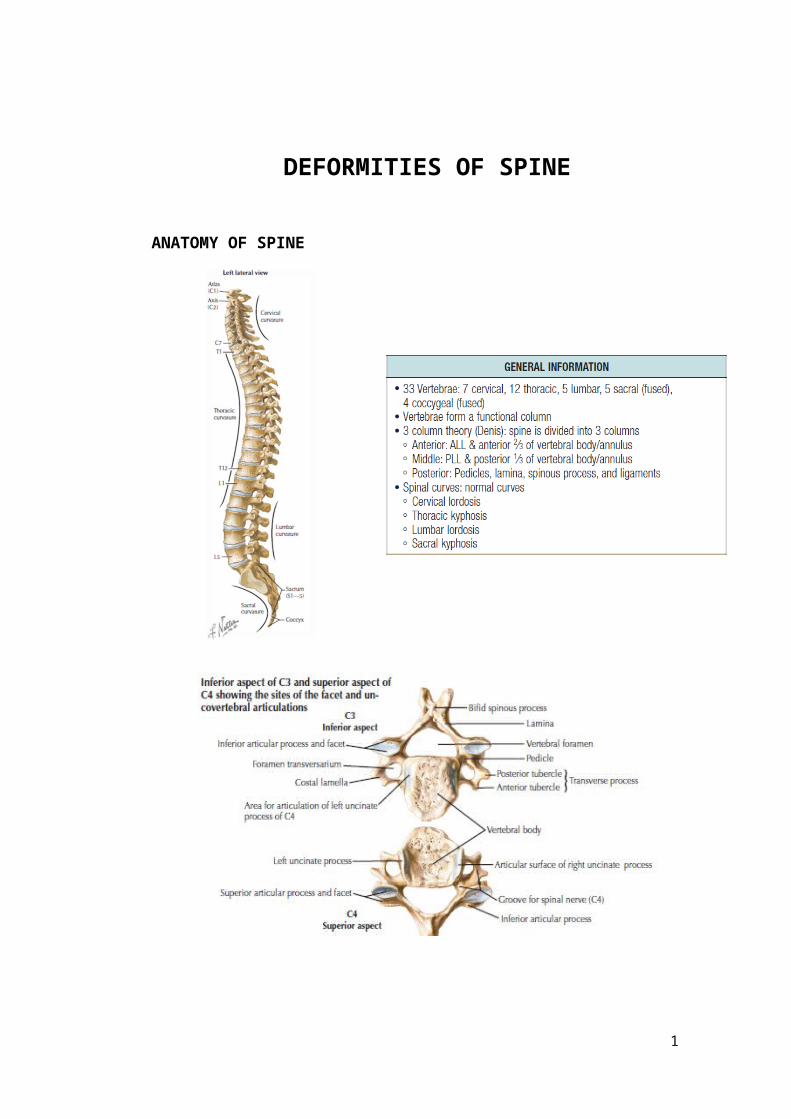
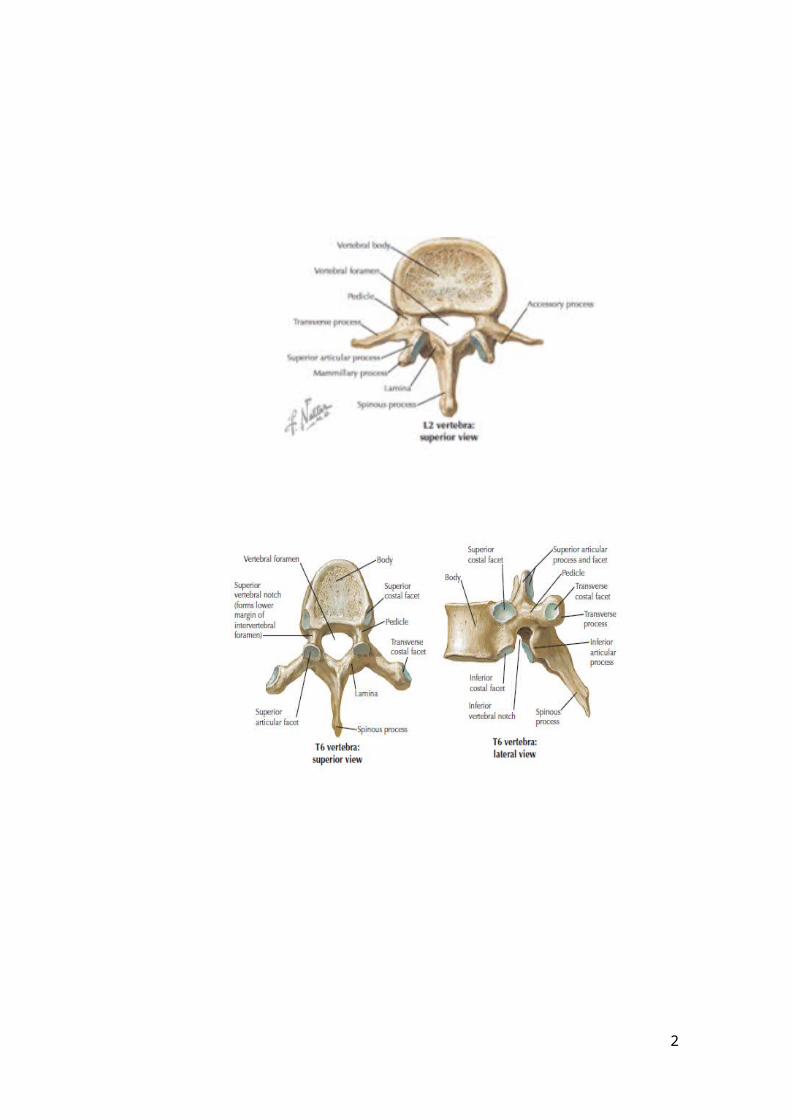
ANATOMY OF SPINE
1
2
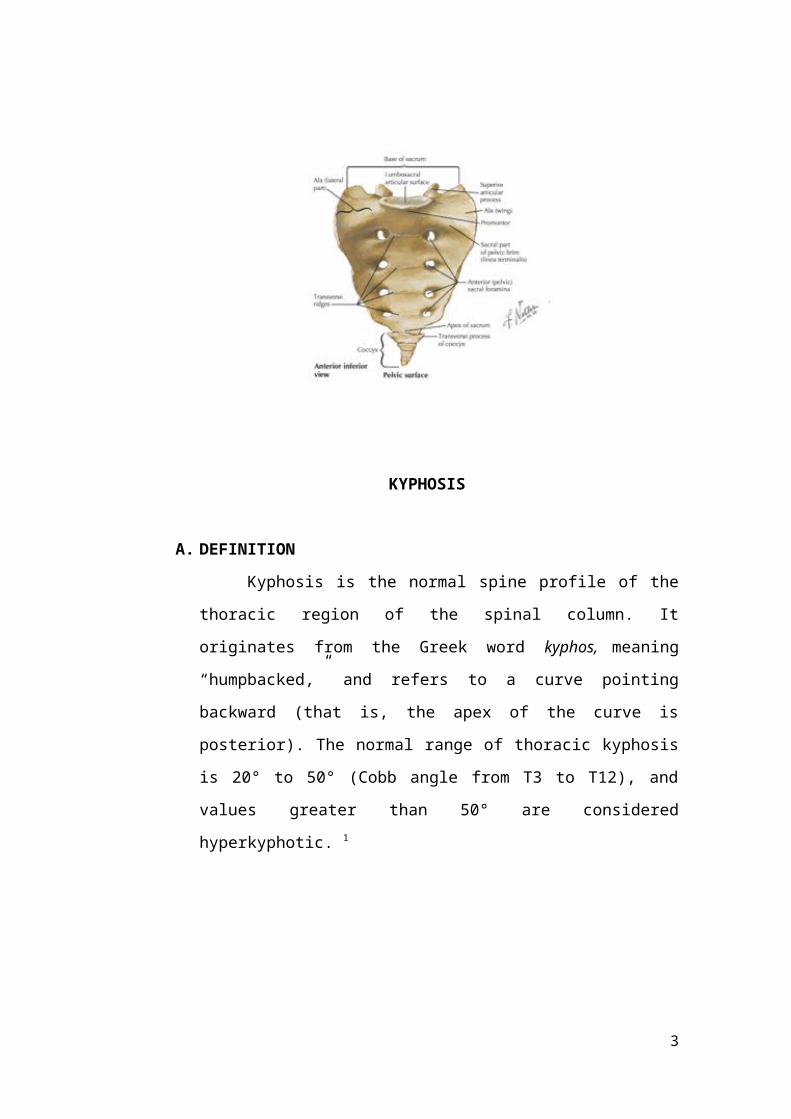
KYPHOSIS
A. DEFINITION
Kyphosis is the normal spine profile of the thoracic region of the
spinal column. It originates from the Greek word kyphos, meaning
“humpbacked,” and refers to a curve pointing backward (that is, the apex
of the curve is posterior). The normal range of thoracic kyphosis is 20° to
50° (Cobb angle from T3 to T12), and values greater than 50° are
considered hyperkyphotic. 1
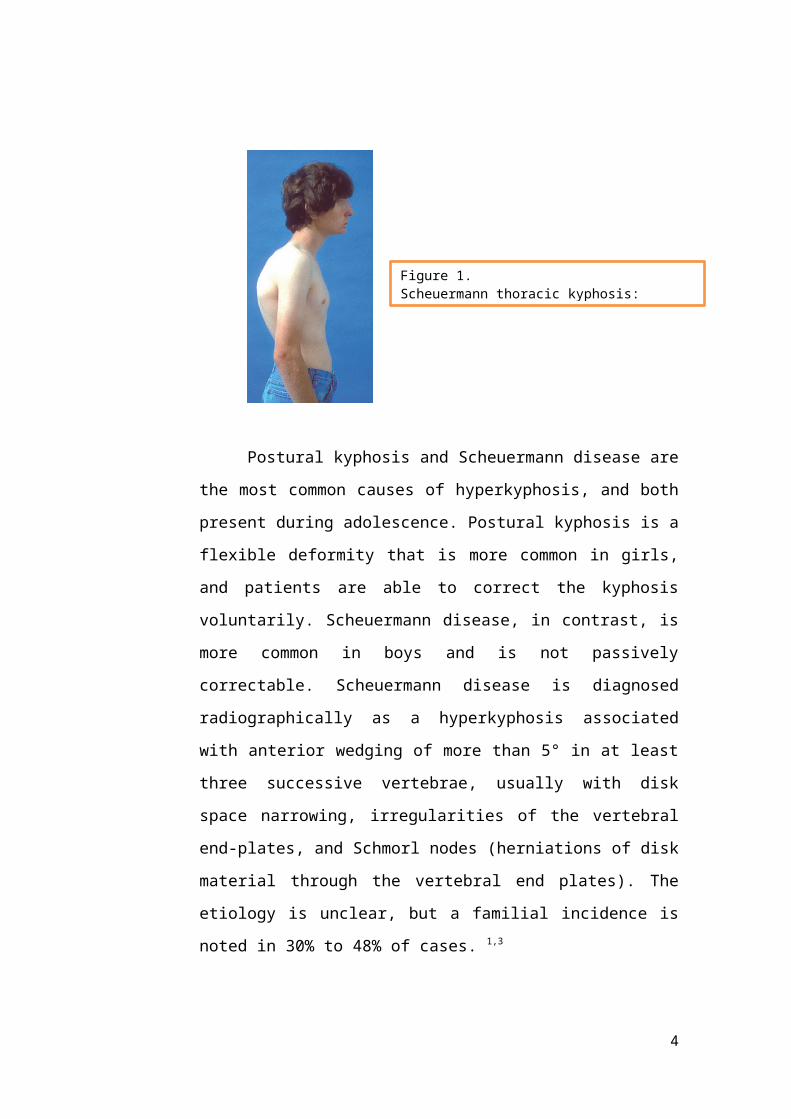
Postural kyphosis and Scheuermann disease are the most common
causes of hyperkyphosis, and both present during adolescence. Postural
kyphosis is a flexible deformity that is more common in girls, and patients
are able to correct the kyphosis voluntarily. Scheuermann disease, in
contrast, is more common in boys and is not passively correctable.
Scheuermann disease is diagnosed radiographically as a hyperkyphosis
associated with anterior wedging of more than 5° in at least three
successive vertebrae, usually with disk space narrowing, irregularities of
the vertebral end-plates, and Schmorl nodes (herniations of disk material
through the vertebral end plates). The etiology is unclear, but a familial
incidence is noted in 30% to 48% of cases. 1,3
3
Figure 1. Scheuermann thoracic kyphosis: clinical photograph.2
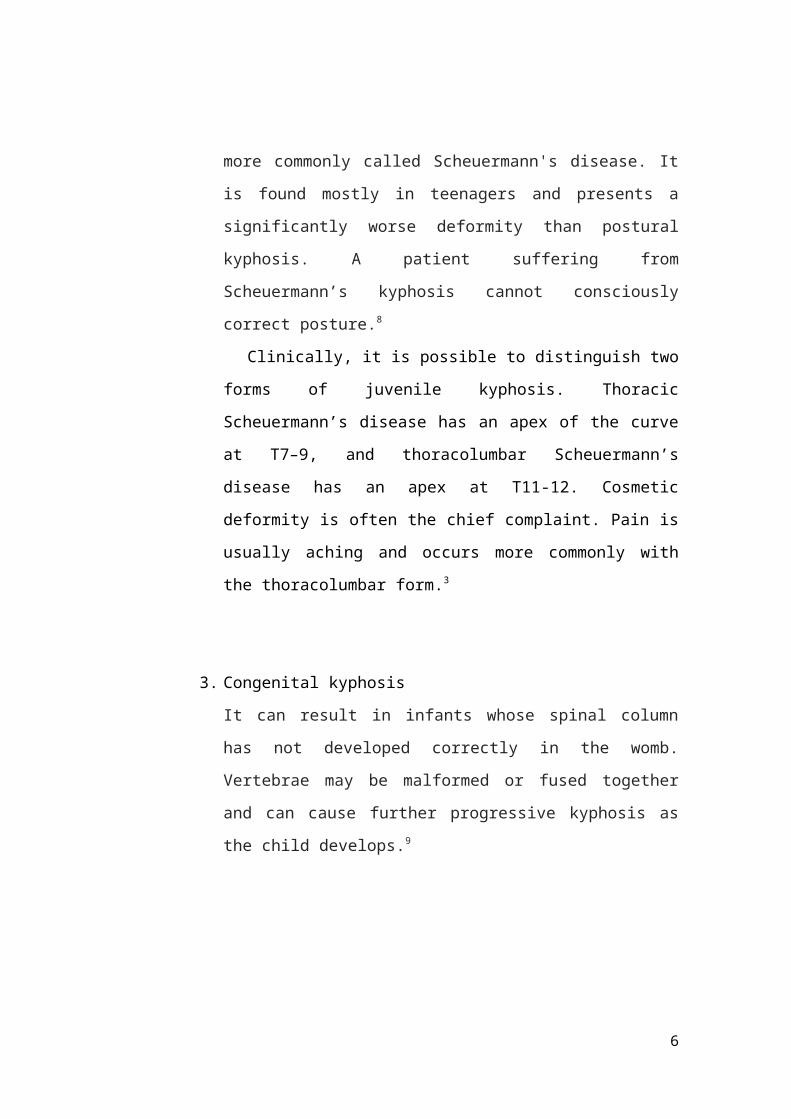
Congenital kyphosis implies a structural defect in vertebral
formation, and may become apparent in infants and toddlers; the other
forms of kyphosis may be diagnosed throughout childhood and
adolescence.1
B. CLASSIFICATION
1. Postural kyphosis
The most common type, normally attributed to slouching, can
occur in both the old4 and the young. In the young, it can be called
'slouching' and is reversible by correcting muscular imbalances. In the
old, it may be a case of hyperkyphosis and called 'dowager’s hump'.
About one third of the most severe hyperkyphosis cases in older
people have vertebral fractures.5 Otherwise, the aging body does tend
towards a loss of musculoskeletal integrity,6 and hyperkyphosis can
develop due to aging alone.
2. Scheuermann's kyphosis
Significantly worse cosmetically and can cause varying degrees of
pain, and can also affect different areas of the spine (the most common
being the midthoracic area). Scheuermann's kyphosis is considered a
form of juvenile osteochondrosis of the spine, and is more commonly
called Scheuermann's disease. It is found mostly in teenagers and
presents a significantly worse deformity than postural kyphosis. A
patient suffering from Scheuermann’s kyphosis cannot consciously
correct posture.8
Clinically, it is possible to distinguish two forms of juvenile
kyphosis. Thoracic Scheuermann’s disease has an apex of the curve at
T7–9, and thoracolumbar Scheuermann’s disease has an apex at T11-
12. Cosmetic deformity is often the chief complaint. Pain is usually
aching and occurs more commonly with the thoracolumbar form.3
3. Congenital kyphosis
4
It can result in infants whose spinal column has not developed
correctly in the womb. Vertebrae may be malformed or fused together
and can cause further progressive kyphosis as the child develops.9
C. PATHOPHYSIOLOGY
The pathophysiology of kyphosis depends on the etiologic factor.
The exact cause of Scheuermann disease is still imprecisely defined.
Scheuermann postulated that the condition resulted from avascular
necrosis of the apophyseal ring. Other theories include histologic
abnormalities at the endplate, osteoporosis,10 and mechanical factors that
affect spinal growth.11 A Danish study demonstrated an important genetic
component to the entity.12
D. DIAGNOSIS
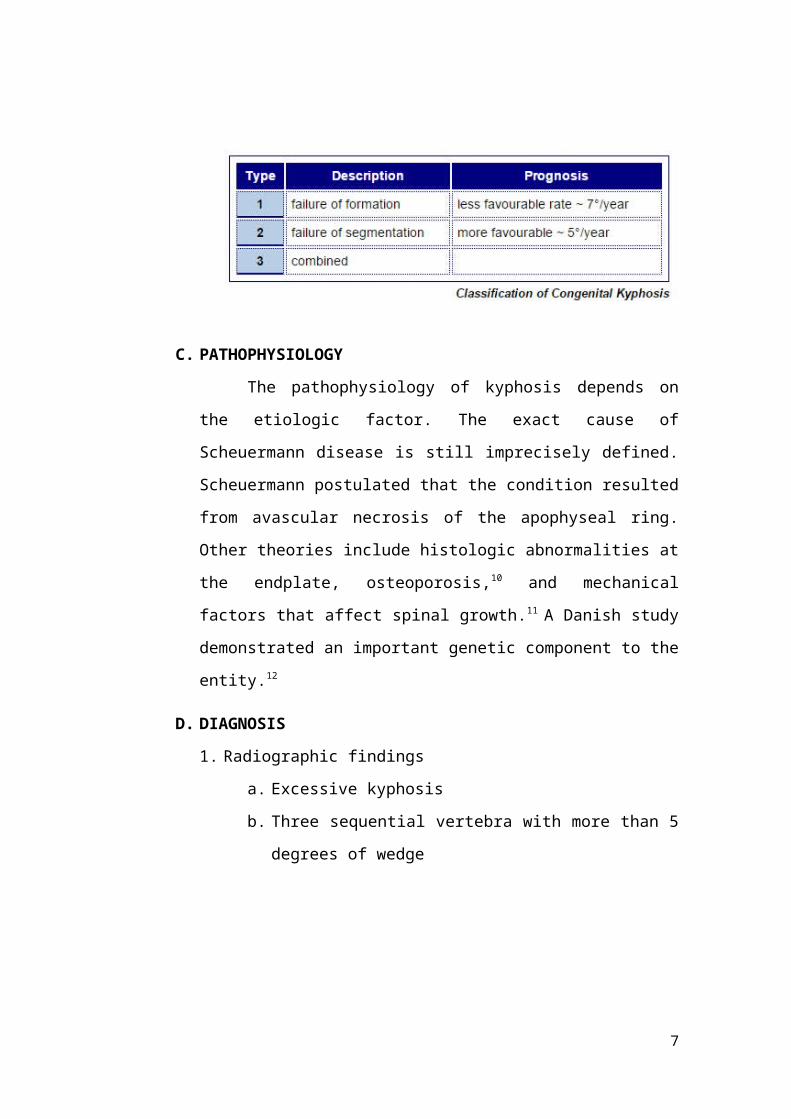
1. Radiographic findings
a. Excessive kyphosis
b. Three sequential vertebra with more than 5 degrees of wedge
5
Anterior wedging of thoracic spine in a 15-year-old boy withScheuermann kyphosis
2. Clinical characteristics
a. More common in boys
b. Affected patients usually overweight
c. Kyphosis is not postural: does not complete correct with
hyperextension
d. Neurologic changes are rare: MRI indicated if they are
present13
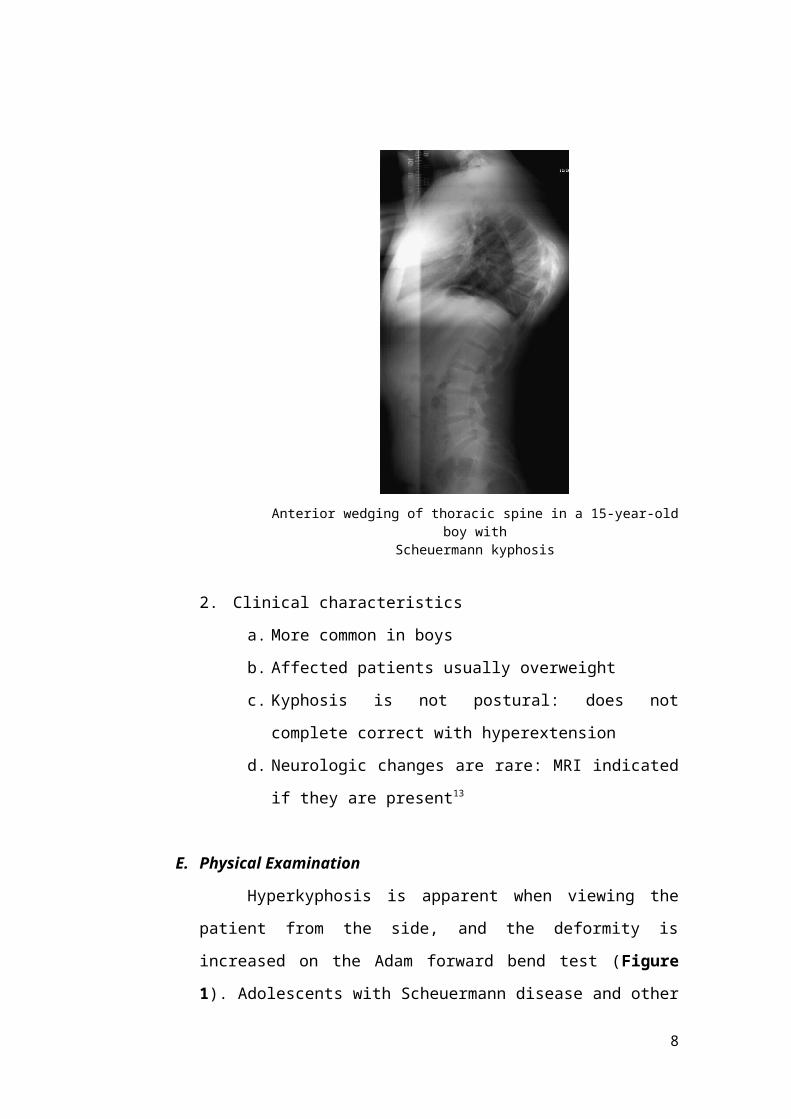
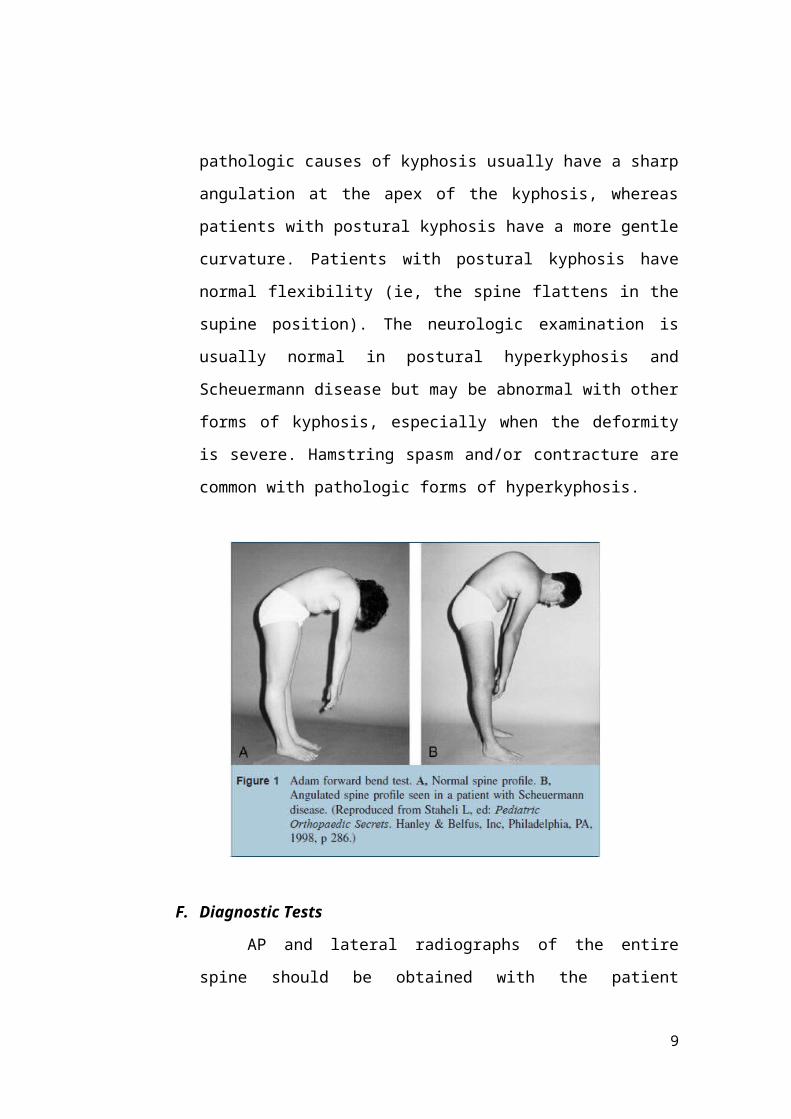
E. Physical Examination
Hyperkyphosis is apparent when viewing the patient from the side,
and the deformity is increased on the Adam forward bend test (Figure 1).
Adolescents with Scheuermann disease and other pathologic causes of
kyphosis usually have a sharp angulation at the apex of the kyphosis,
whereas patients with postural kyphosis have a more gentle curvature.
Patients with postural kyphosis have normal flexibility (ie, the spine
flattens in the supine position). The neurologic examination is usually
6
normal in postural hyperkyphosis and Scheuermann disease but may be
abnormal with other forms of kyphosis, especially when the deformity is
severe. Hamstring spasm and/or contracture are common with pathologic
forms of hyperkyphosis.
F. Diagnostic Tests
AP and lateral radiographs of the entire spine should be obtained
with the patient standing. The reviewer should look for congenital
abnormalities as well as irregularities of the vertebrae, disk spaces, and the
end plates. The curve magnitude is measured on the lateral radiograph
using the Cobb method. When the upper thoracic vertebrae cannot be well
visualized, kyphosis should be measured from T5 to T12. The angle is
formed by the intersection of a line drawn along the superior end plate of
T5 and a line drawn on the inferior end plate of T12. Any curvature
exceeding 50° is considered abnormal.
7
G. Complication
The natural history of flexible or postural hyperkyphosis is benign,
and these curves are unlikely to progress, but other forms of kyphosis
present a significant risk for progression. The consequences of a
progressive kyphosis may include back pain; rarely, neurologic symptoms,
usually seen with congenital kyphosis; and a decrease in pulmonary
function, seen with curvatures greater than 90° to 100° (restrictive
pattern).
H. Treatment
Postural kyphosis can be observed or treated with an exercise
program. Progressive curvatures due to Scheuermann disease may be
treated by a bracing program in patients who are skeletally immature (full-
time wear, Milwaukee brace or equivalent), and a subset of patients with
progressive and symptomatic curvatures greater than 70° are candidates
for a posterior or an anterior/posterior spinal fusion with instrumentation.
Congenital kyphosis is much more likely to require surgical intervention,
sometimes in the first few years of life. Bracing is not effective in patients
with congenital deformities, and progressive deformities often require
surgical stabilization.
8
SCOLIOSIS
A. Introduction
Spinal deformity may affect the sagittal, coronal, and axial planes. Sagittal
plane deformity or kyphotic deformities of the spine are best seen on physical
examination from the side with
the patient bending forward. Sagittal plane malalignment of the spine may
involve any region of the spine but is most common in the thoracic and
thoracolumbar spine and is common with aging. Scoliosis is defined by
coronal plane deformity, but there is a concordant rotational deformity that is
apparent on examination. Shoulder asymmetry, pelvic tilt, and asymmetric
abdominal or flank creases are signs of deformity in the coronal plane. Trunk
rotation or rib prominence on forward bending (Adam forward bend test) is a
critical measure of axial plane deformity and may be apparent earlier than
coronal deformity in patients with scoliosis. In younger patients, scoliosis is
usually idiopathic, but in older patients it also may occur as a result of
degenerative changes. Patients with a new onset of scoliosis or rapid
progression of deformity should be evaluated for syndromes or diseases that
may be a cause of spinal deformity such as neurofibromatosis, spinal cord
lesions, or a tethered spinal cord. Spondylolisthesis (isthmic) usually occurs at
the lumbosacral joint and is accompanied by tight hamstring muscles (inability
to toe-touch). Onset of a spinal deformity in adulthood, or de novo
degenerative scoliosis, is common and may be associated with aging,
segmental instability, and osteoporosis. A rapid progression of deformity in
the adult may be an indication of neoplasm or infection. These conditions may
be accompanied by compromise of the spinal nerve roots and/or the spinal
cord.
Scoliosis is primarily a lateral curvature of the spine, but there is often a
degree of associated kyphosis. Mathematical analysis of the curves has
revealed several distinct patterns, which are dependent on the relative
contributions of these two deformities. In the management of any case, the
9
first and most important decision to make is whether there is any deformity of
the vertebrae (structural scoliosis). If the vertebrae are normal (non-structural
scoliosis) the deformity is usuall due to one of the following conditions: it
may be compensatory, resulting from tilting of the pelvis from real or apparent
shortening of one leg. It may be sciatic and due to unilateral protective muscle
spasm, especially that accompanying a prolapsed intervertebral disc. Postural
scoliosis occurs most commonly in adolescent girls and generally resolves
spontaneously.
B. Defenition
Scoliosis is a lateral curvature of the spine. In adults, the condition is
classified as either a deformity that developed during childhood or a deformity
that developed after skeletal maturity, usually secondary to degenerative
spondylosis and/or degenerative spondylolisthesis. Changes that occur with
aging, including osteoporosis, degenerative disk disease, spinal stenosis, and
degenerative spondylolisthesis, may contribute to and/or confound the
symptoms and progression of either condition.
C. Epidemiology
Scoliosis is present in 2 to 4 percent of children between 10 and 16 years
of age. The ratio of girls to boys with small curves of 10 degrees is equal but
increases to a ratio of 10 girls for every one boy with curves greater than 30
degrees. Scoliosis in girls tends to progress more often and, therefore, girls
more commonly need treatment than boys. The prevalence of curves greater
than 30 degrees is approximately 0.2 percent, and the prevalence for curves
greater than 40 degrees is approximately 0.1 percent. Improved understanding
of the natural history and prognosis of this disease can help the physician
predict the patients with scoliosis who need treatment.
10
D. Pathogenesis
Many studies have attempted to uncover the pathophysiologic process
underlying idiopathic scoliosis. Multiple abnormalities have been found, yet
none has been conclusively linked to all cases. Studies of twins have given the
firmest indication that the most significant factor is genetic. Indeed, a recent
meta-analysis showed that not only is the risk for scoliosis greater in
monozygotic twins than in dizygotic twins, the rate of curve progression is
nearly identical among twins subjected to a variety of environmental
influences. Current theorists believe that scoliosis is a multigene dominant
condition with variable phenotypic expression. Therefore, even though
scoliosis is typically present in most members of the same family, its severity
can vary widely from parent to child and sibling to sibling. When both parents
have scoliosis, the risk that their children will require treatment is 50 times
that in the general population
E. Clinical Findings
The most common presenting symptom is pain localized to the region of
the deformity. The most common overlapping syndrome is degenerative
spondylosis, which may also cause lower lumbar pain. Because age-related
changes in the spine are present in nearly everyone, a thorough evaluation is
required to identify the most likely source of pain. Radicular pain is most
commonly associated with compression of the L4 or L5 nerve root due to
asymmetric hypertrophy of the facet joints, asymmetric disk degeneration, and
mild rotatory subluxation.
Neurologic changes are infrequent but most commonly involve the
extensor hallucis longus muscle. In some patients, the chief presenting
symptom is a progressive spinal deformity Some report that they are “getting
shorter.” These patients may also report that the “hump” on their back is
getting bigger, or that they are leaning to the side more. Cardiopulmonary
decompensation rarely is evident in adultonset scoliosis. Symptoms related to
11
pulmonary compromise are associated with more severe thoracic curves,
including both idiopathic and neuromuscular curves.
F. Classification
Congenital Scoliosis
A. Defenition
Congenital scoliosis is a progressive three-dimensional deformity of the
spine caused by congenital anomalies of the vertebrae that result in an
imbalance of the longitudinal growth of the spine. To understand their natural
history and their treatment, it is important to understand the embryologic
development of vertebrae.
B. Classification
Two types of basic vertebral anomalies can occur: failures of formation
and failures of segmentation.
a) Failure of vertebral formation
Failure of vertebral formation (type I deformity) can be partial, causing
a wedged vertebra with intact pedicles (Fig. 22–2), or complete, causing a
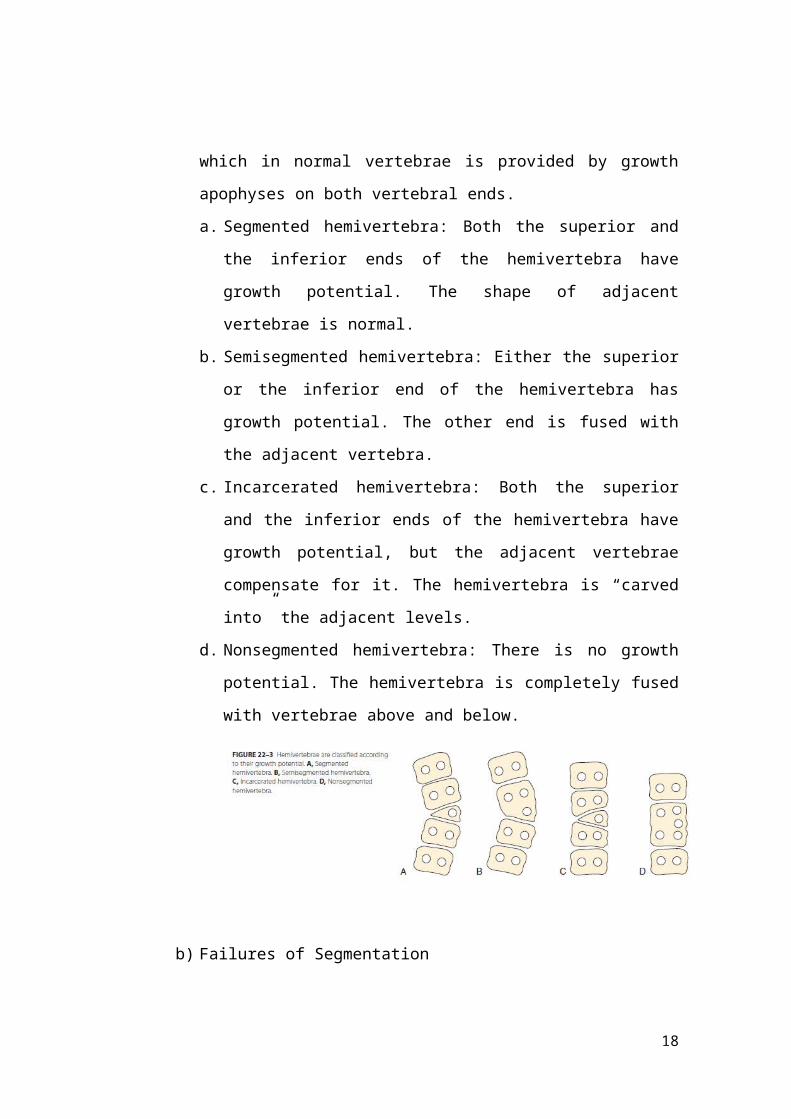
hemivertebra with a unilateral pedicle (Fig. 22–3). Hemivertebrae are
classified according to their longitudinal growth potential, which in normal
vertebrae is provided by growth apophyses on both vertebral ends.
a. Segmented hemivertebra: Both the superior and the inferior ends of the
hemivertebra have growth potential. The shape of adjacent vertebrae is
normal.
b. Semisegmented hemivertebra: Either the superior or the inferior end of
the hemivertebra has growth potential. The other end is fused with the
adjacent vertebra.
c. Incarcerated hemivertebra: Both the superior and the inferior ends of
the hemivertebra have growth potential, but the adjacent vertebrae
12
compensate for it. The hemivertebra is “carved into” the adjacent
levels.
d. Nonsegmented hemivertebra: There is no growth potential. The
hemivertebra is completely fused with vertebrae above and below.
b) Failures of Segmentation
Failure of segmentation (type II deformity) can be partial, causing
a bar (Fig. 22–4), or complete, causing a block vertebra. A congenital bar
can be anterior, posterior, lateral, or mixed. In many cases, vertebral
anomalies owing to failures of formation and failures of segmentation
coexist, occasionally on several levels, and form a mixed deformity (type
III deformity).
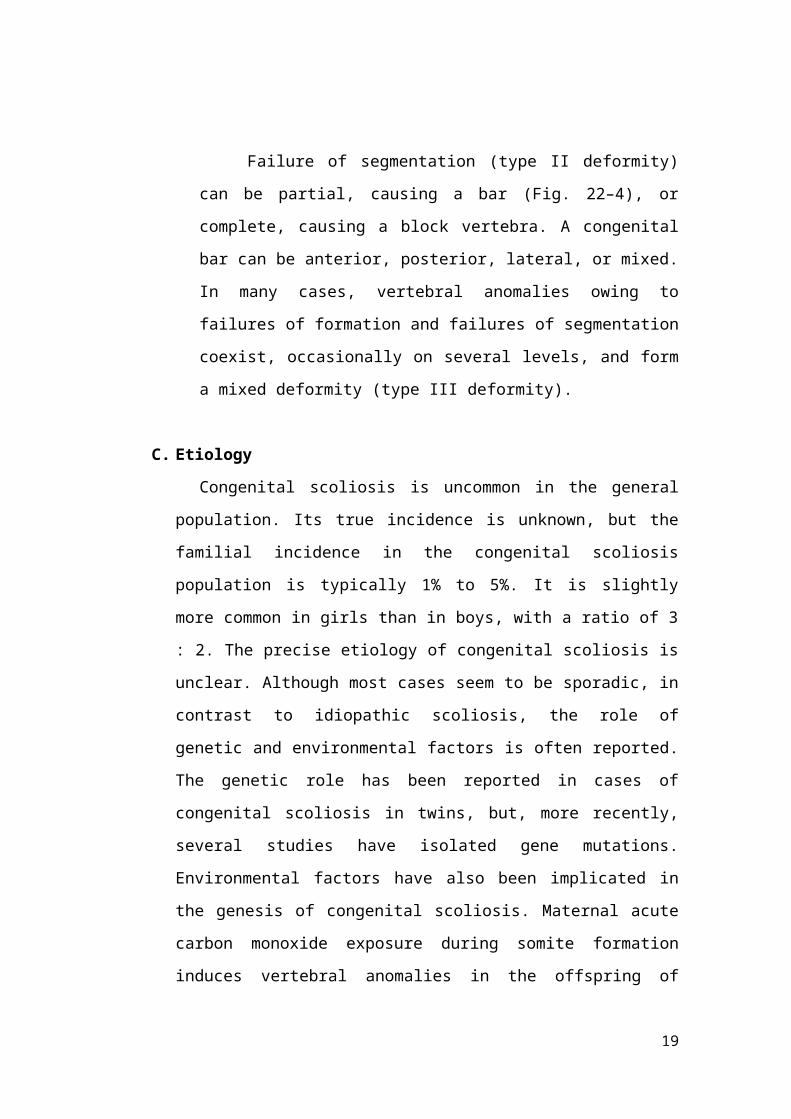
C. Etiology
Congenital scoliosis is uncommon in the general population. Its true
incidence is unknown, but the familial incidence in the congenital scoliosis
population is typically 1% to 5%. It is slightly more common in girls than in
boys, with a ratio of 3 : 2. The precise etiology of congenital scoliosis is
unclear. Although most cases seem to be sporadic, in contrast to idiopathic
scoliosis, the role of genetic and environmental factors is often reported. The
genetic role has been reported in cases of congenital scoliosis in twins, but,
more recently, several studies have isolated gene mutations. Environmental
factors have also been implicated in the genesis of congenital scoliosis.
Maternal acute carbon monoxide exposure during somite formation induces
vertebral anomalies in the offspring of mouse and rabbit models. The
13
mechanism of carbon monoxide action remains vague, however. Carbon
monoxide could act directly on the cartilaginous spine via resulting hypoxia or
a gene mutation. The etiologic theories are clouded further by the finding of
an increased incidence of idiopathic scoliosis in families with congenital
scoliosis.
D. Diagnosis
Anamnesis
As with scoliosis of any etiology, congenital scoliosis progresses in 70%
of patients during growth. The potential for increase in curvature is related to
imbalances in the number of growth apophyses and the location of vertebral
anomalies. Without any treatment, about 85% of patients with congenital
scoliosis have a curve greater than 41 degrees by maturity. Curves with
segmented hemivertebrae are at risk for progression during growth because
segmented hemivertebrae act as enlarging wedges (Fig. 22–6). The most
progressive anomaly is a convex segmented hemivertebra associated with a
concave unilateral bar because there is absolutely no growth potential on the
side of the bar. Conversely, a wedge vertebra has only a slight risk of
14
worsening, whereas a complete block or an incarcerated hemivertebra does
not cause any progressive scoliosis. The location of the anomaly also plays a
part in the evolution of scoliosis. The most severe anomalies are those located
at the thoracolumbar region, whereas the least severe are located at the upper
thoracic spine. The natural history of congenital scoliosis has to take several
factors into account:
Type of anomaly
Location
Number of anomalies
Initial severity of the scoliosis
Global growth potential balance between each side of the Spine
Physical Examination
The physical examination of a patient with congenital scoliosis is guided
by the knowledge of a heightened incidence of other structural and neural
anomalies. The examination should begin with an assessment of a patient’s
existing balance: sagittal plane balance and coronal balance, shoulder
malalignment, and any deviation of head and trunk from the center of the
pelvis. In addition, it is crucial to assess and document the neurologic status,
including strength, reflexes, and presence of any atrophy. Flexibility of the
deformity, gait, and limb-length inequality should be checked. Pain, if present,
should be localized and quantified. The presence of a dimple or any cutaneous
mark on the back should be noted. The examiner should search for other
anomalies of the extremities (particularly radial malformation) and range of
neck motion.
Radiology
CT Scan
MRI
15
A and B, It is easier to analyze segmented hemivertebra (A) or unilateral bar (B) when films are taken before 4 years of age than after.
C, Lumbar segmented hemivertebra in a 9-year-old child
FIGURE 22–5 Congenital scoliosis with VACTERL association managed by observation since birth. A and B, Right thoracic curve and compensatory lumbar curve remain relatively unchanged from birth at
1 year of age (A) and at 8 years of age (B).
E. Treatment
16
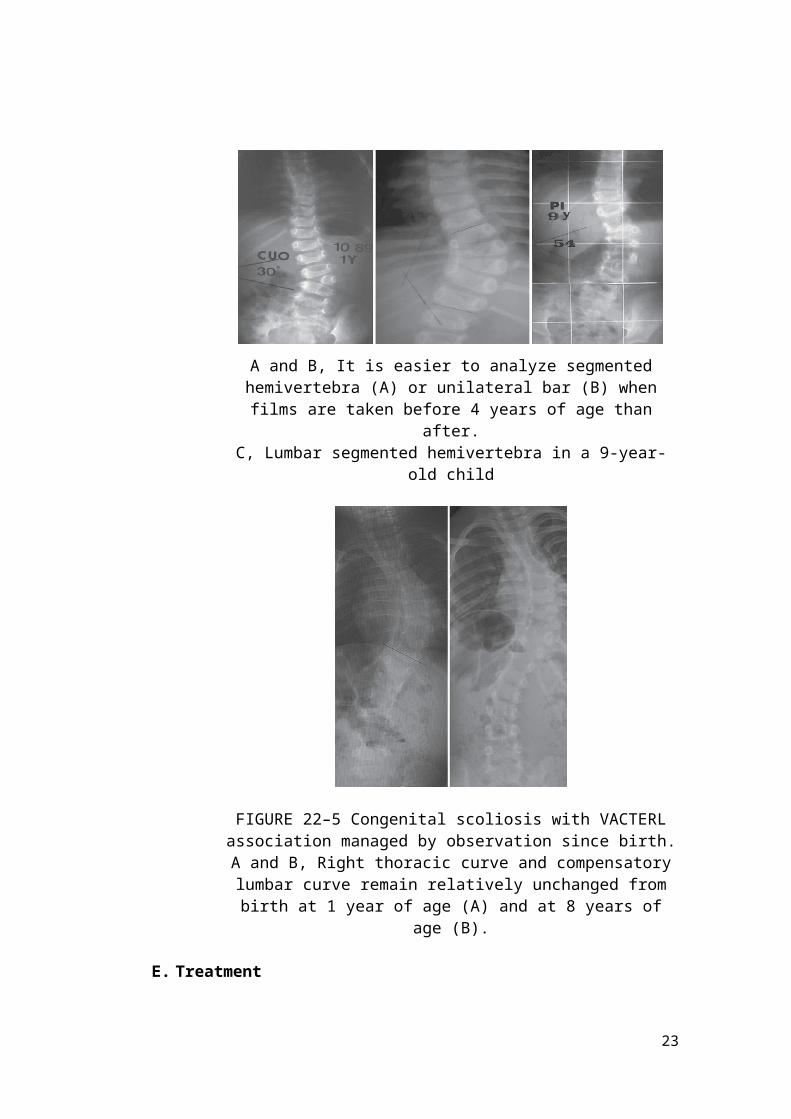
Non Operative
Congenital vertebral anomalies require close clinical monitoring at
periodic intervals during growth. Consistent observation allows for assessment
of the evolution of spinal curves. In complex malformations, early treatment is
often more straight forward and safer.
In contrast to idiopathic scoliosis, nonoperative treatment has little value
in congenital scoliosis. The only potentially useful treatment is bracing of the
noncongenital components of a flexible curve. For a few cases with long and
flexible curves, progression of scoliosis can be slowed by bracing. Spinal
curves in congenital scoliosis are often short and rigid, however Given the
significant time period remaining before skeletal maturity, bracing is rarely, if
ever, more than a temporizing solution. Treatment of congenital scoliosis
consists of two options: (1) clinical monitoring of static vertebral anomaly and
(2) operative treatment of worsening scoliosis.
Operative
Congenital scoliosis develops because one side of the spine is growing
faster than the other. The main principle of operative treatment is to balance
growth, with or without deformity reduction. Five major operations have been
described: posterior spine fusion, combined anterior and posterior spine
fusion, convex hemiepiphysiodesis, hemivertebra excision, and guided growth
by vertical expandable prosthetic titanium rib (VEPTR) or growing rods.
Idiopathic Scoliosis
A. Defenition
Idiopathic scoliosis is the most common cause of spinal deformity 80% of
all scoliosis cases are due to idiopathic scoliosis. Before arriving at the
diagnosis of idiopathic scoliosis in a patient, other causes, such as congenital,
neuromuscular (developmental or acquired), functional, inflammatory or
infectious, pathologic, and intraspinal, have to be discounted. Ponseti and
Friedman1 first described early-onset scoliosis in 1950. Dickson expounded
17
further on that concept and proposed that idiopathic scoliosis be divided into
early (0 to 5 years old) and late onset (>5 years old), based on spinal growth
velocity noted in these two age groups. Presently, idiopathic scoliosis is
divided into three categories based on chronologic age: infantile (birth to 2
years + 11 months), juvenile (3 years to 9 years + 11 months), and adolescent
(10 years to 17 years + 11 months). The radiographic diagnosis necessitates
measuring the coronal plane angle, using the Cobb method, as equal to or
greater than 10 degrees. Patients with curves less than 10 degrees are
considered to have spinal asymmetry.
B. Epidemiology
Infantile and juvenile scoliosis are less prevalent than adolescent
idiopathic scoliosis. Infantile idiopathic scoliosis is more common in Europe,
constituting less than 1% of idiopathic scoliosis cases in the United States, and
tends to comprise leftsided thoracic curves, typically occurring in boys. More
recent reviews suggest that there might be a decline in its incidence. Juvenile
cases are typically diagnosed at age 7 years in girls and 5 years in boys and
account for about 10% to 20% of idiopathic scoliosis cases.3 In contrast to
infantile idiopathic scoliosis, juvenile cases tend to occur predominantly in
girls and tend to comprise right-sided curves. Between the ages of 3 and 6
years, there seems to be a similar distribution between boys and girls,
however, again becoming predominant in girls after age 6 years.
Adolescent idiopathic scoliosis is more prevalent than other types of
idiopathic scoliosis. Among adolescents, the prevalence of 10-degree curves is
less than 3%, with about 5% of curves showing progression of greater than 30
degrees.
This prevalence decreases as a function of curve magnitude, however, to
about 0.3% to 0.5% and 0.1% in curves measuring 20 degrees and 40 degrees.
The prevalence of curves greater than 10 degrees is higher among girls, with a
4 : 1 ratio of girls to boys.
18
C. Etiology
Infantile scoliosis occurs roughly in 1 of 10,000 births. Possible causes are
thought to occur from intrauterine molding or postnatal pressure on the spinal
column from supine positioning
while sleeping. Other etiologic factors that have been considered in idiopathic
scoliosis include dysfunction in proprioception to maldevelopment in central
pattern generators in the spinal cord9-11 and connective tissue, hormonal, and
muscle structural changes.12 More recent reports in the literature strongly
suggest a genetic link. The growth spurt noted among adolescents seems to
play a role in progression, as a critical buckling load is reached on the existing
curve as the spine grows. In a review of the literature, Kouwenhoven and
Castelein13 concluded many factors may play a role in the initiation and
progression of adolescent idiopathic scoliosis at a certain age. The literature
suggests, however, that in the observed deformation of the spine, genetics and
the unique mechanics of the fully erect posture, which is exclusive to humans,
play an important role.
D. Diagnosis
Anamnesis and Physical Exam
A complete history and physical examination is completed, and any family
history of scoliosis is noted. With infantile and juvenile cases in particular, a
thorough prenatal and birth and developmental history is obtained. In
adolescent cases, growth spurt history, if any at the time of presentation, is
noted. This information is imperative in determining peak growth velocity and
its implications on curve progression. Symptoms of or weakness and how the
patient perceives his or her appearance relative to the deformity are especially
important with adolescent idiopathic scoliosis. Age at onset of menarche and
voice changes in boys are noted as well because they are likely predictors of
growth potential and possible curve progression.
During the examination, height, weight, and age (years plus months since
last birthday) are recorded. The head is examined with special attention to
19
torticollis and plagiocephaly because the latter has been associated with higher
incidence in infantile scoliosis. Possible conditions and anomalies that might
be present are buccal and palatal anomalies; café au lait spots; and midline
dimples or hair patches or both over the lumbodorsal spine, which can be
important clinical clues that an intraspinal pathologic process might be
present. Limb laxity is also checked, and genetic counseling and testing is
requested when laxity is present. Trunk shift is evaluated with the patient
standing and the hips and knees fully extended. The relationship of the
patient’s head to the pelvis is also noted in evaluating the overall coronal and
sagittal balance. Any shoulder, breast, or pelvic asymmetry is noted. Curve
rotation is assessed by performing an Adams forward-bend test and is
quantified with a scoliometer. This assessment is modified in infants by laying
the patient on the examiner’s knee. This test also helps assess the rigidity of
the curve, which is an important factor in terms of prognostication. Leg-length
discrepancy and pelvic obliquity are evaluated. Alternatively, a sitting forward
test can be performed. The latter maneuver can also help rule out
plagiocephaly and developmental hip dysplasia, especially in infants. When
leglength discrepancy is the likely cause of the deformity, a shoe lift is used to
reevaluate the patient to determine if the curve corrects.
A thorough neurologic examination is performed. The neurologic
examination includes all cranial nerves; motor strength; reflexes (including
abdominal reflexes), often associated with Chiari malformations; sensory
modalities; and gait.27 Finally, other possible causes of scoliosis, such as
congenital, neuromuscular, and syndromic types, must be ruled out. Infection,
neoplasms, and spondylolisthesis also must be discounted.
20
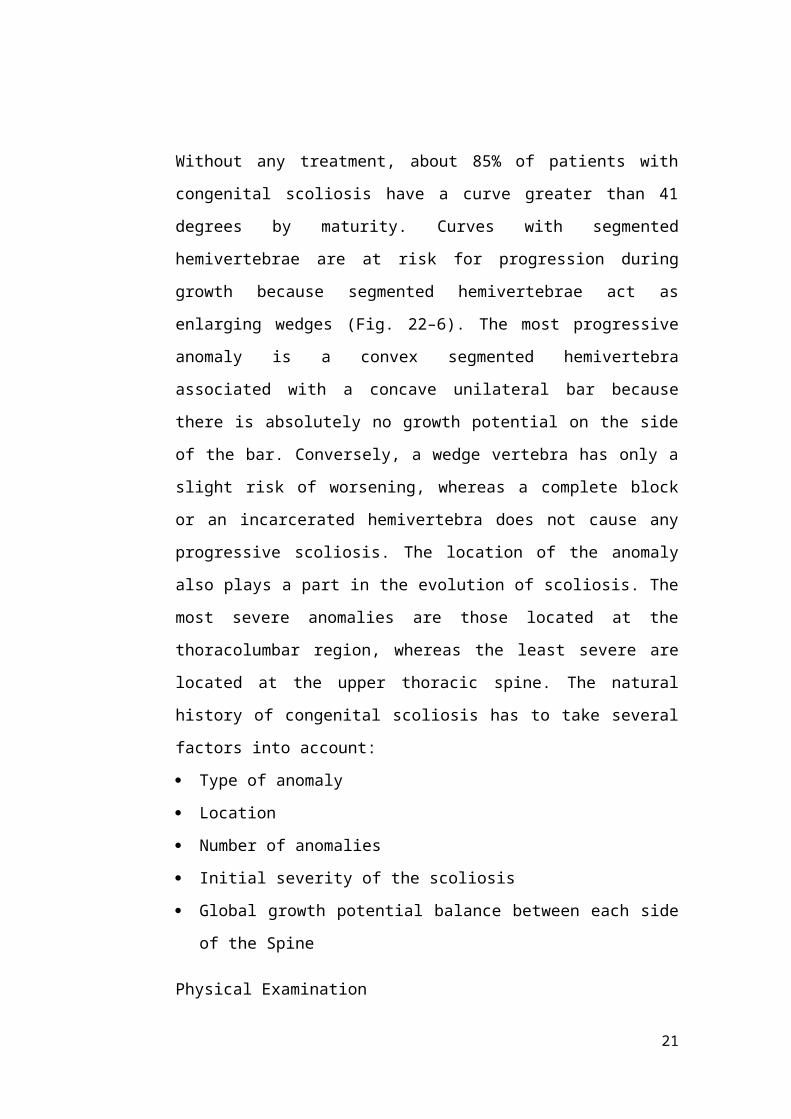
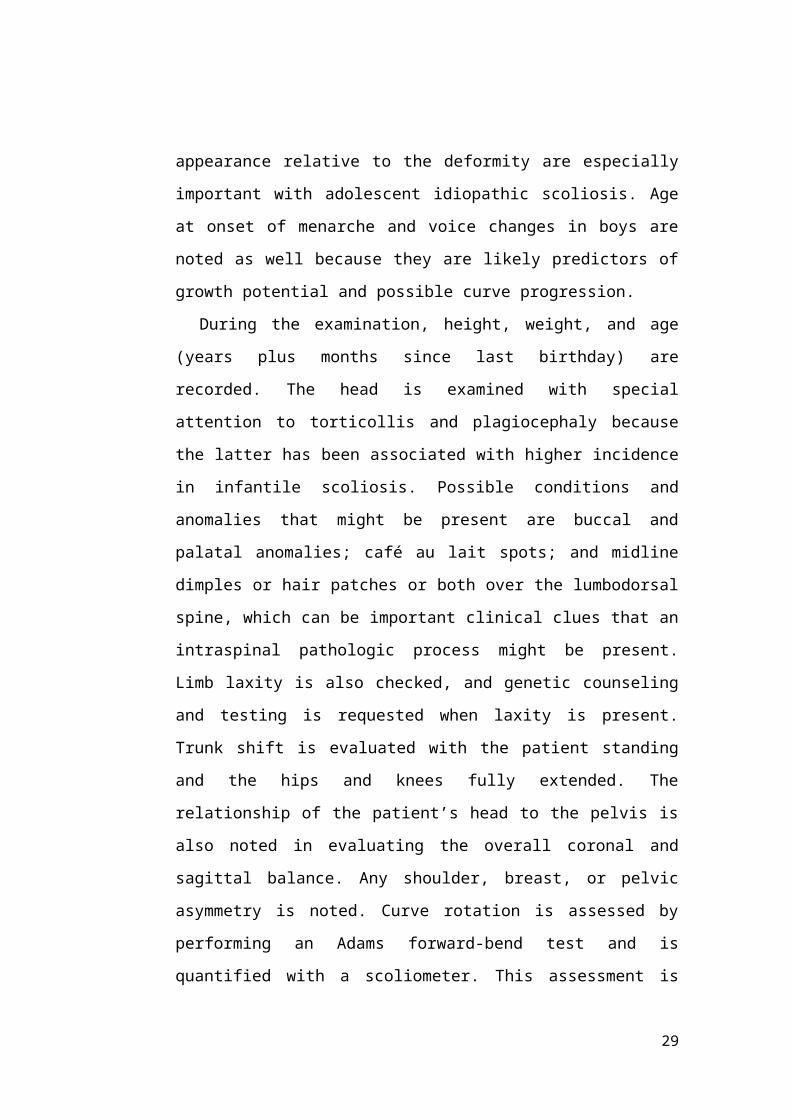
FIGURE 3. Adam’s forward bend test. (Left) As the patient bends over, the examiner looks from behind and from the side, horizontally along the contour of the back.
(Right) A rotational deformity known as a rib hump (arrow) can be easily identified.
Radiographic
Posteroanterior and lateral 36- × 14-inch long cassette views including
bending films with appropriately placed bolsters for further curve
classification and planning bracing or surgical intervention are obtained, and
the Cobb angles are measured. Curves greater than 20 degrees in infants and
children, neurologic symptoms in all patients with idiopathic scoliosis, and
left-sided, sharp angular or irregular curve patterns require further
investigation, including screening total spine magnetic resonance imaging
(MRI). When anomalies of the nervous system are present on MRI, a
neurosurgical consultation is indicated.
21
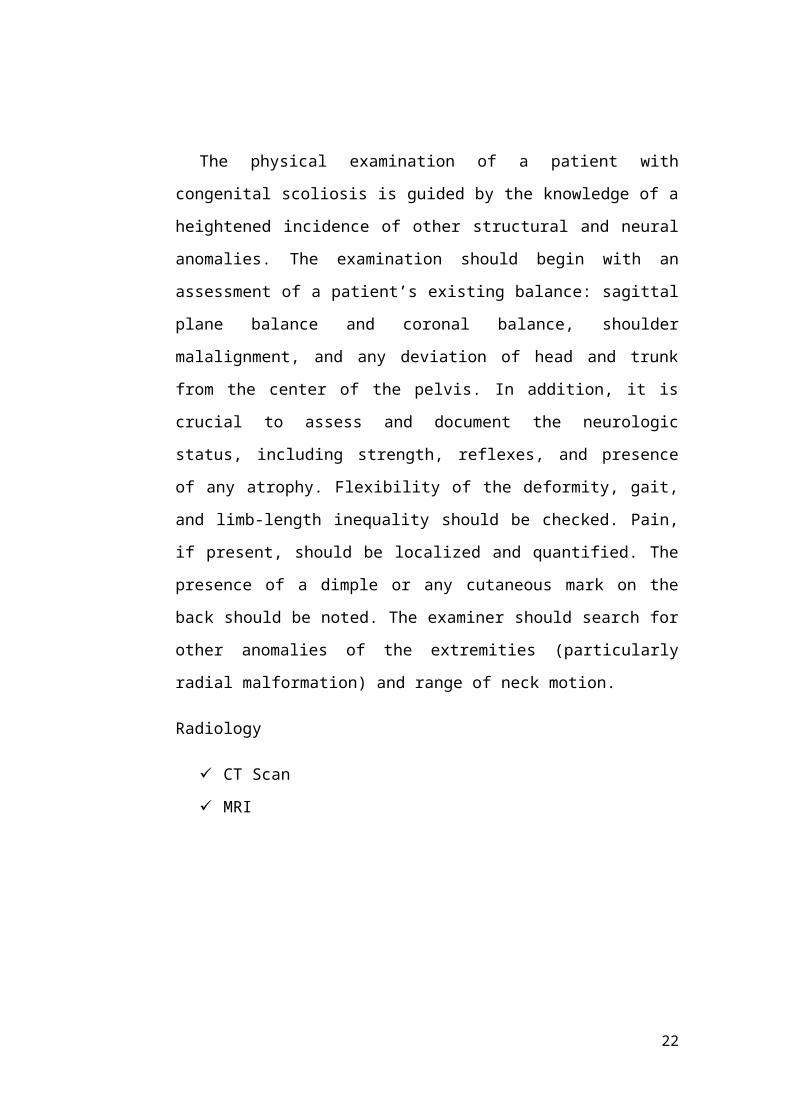
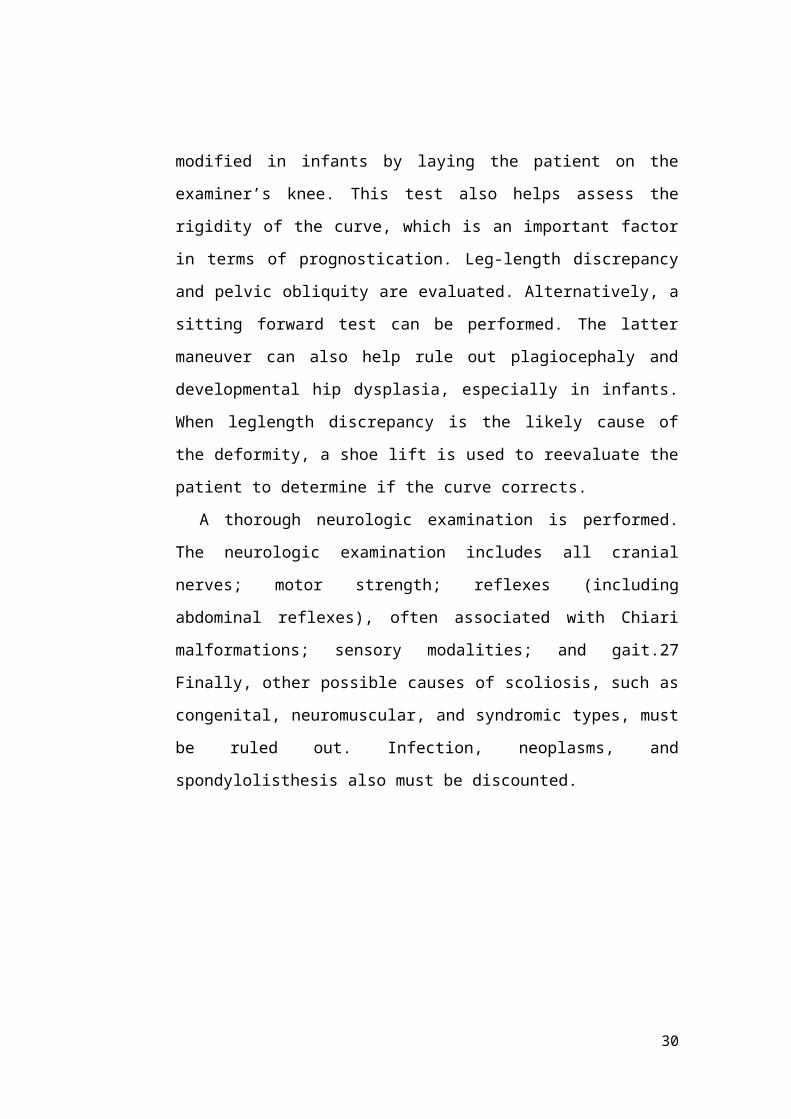
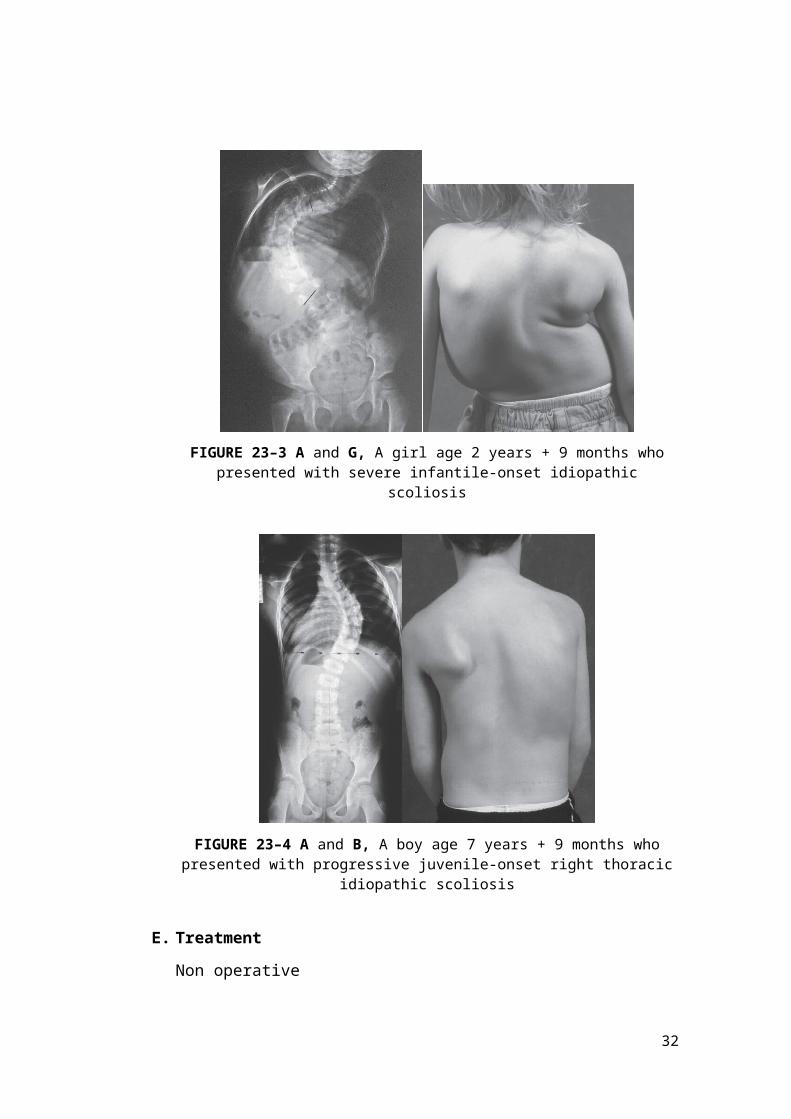
FIGURE 23–3 A and G, A girl age 2 years + 9 months who presented with severe infantile-onset idiopathic scoliosis
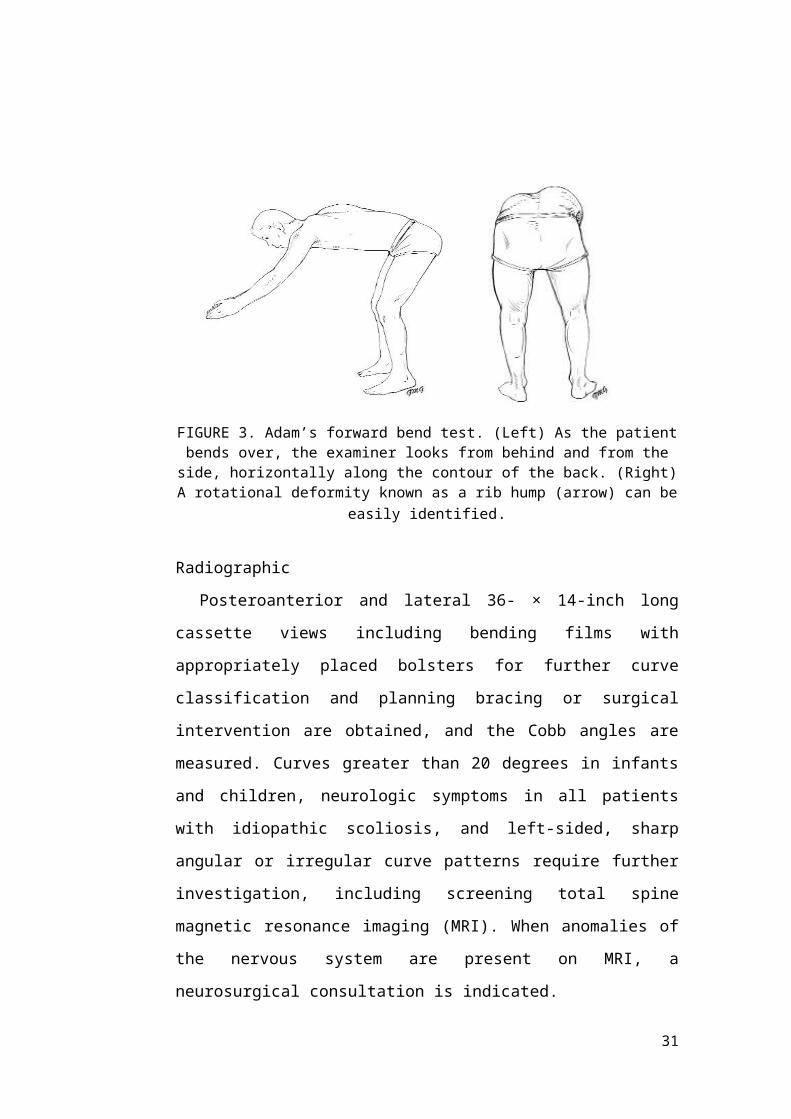
FIGURE 23–4 A and B, A boy age 7 years + 9 months who presented with progressive juvenile-onset right thoracic idiopathic scoliosis
E. Treatment
Non operative
Observation
Most infantile curves are left-sided; these curves have been known to
resolve spontaneously up to 90% of the time, but they can progress.41
22
Deciphering which curves will progress can be guided by the RVAD and the
relationship of the apical rib head to the vertebral body (i.e., phase I or II).22
Typically, curves less than 20 degrees are expectantly followed every 6 to 8
months. Infants with curves less than 25 degrees and RVAD less than 20
degrees and children with curves less than 25 degrees should be followed
clinically and radiographically every 6 months. Treatment is instituted for
curves greater than 25 degrees. Treatment is also started for a progression of 5
degrees or greater in two consecutive visits or 10 degrees or greater in one
follow-up visit. Juvenile curves more often require operative intervention,
however.
Bracing and Casting
Bracing is the nonoperative treatment of choice in small but progressive
scoliosis in growing children and teens. In about 75% of cases, bracing can
control the curve and avoid progression, rendering the curve small enough so
that the risk of progression after growth is unlikely. In a younger child, whose
growth potential remains a significant issue, bracing allows for continued
growth until the patient requires eventual operative treatment because of curve
progression. With infantile cases, molded casting followed by bracing used to
be the mainstay in nonoperative management. Bracing and casting of these
patients comes with potential consequences, however, that include pulmonary
restriction, which can have future ramifications. Sanders and colleagues found
serial casting to be beneficial in the treatment of infantile scoliosis. They
reported that curves less than 60 degrees often fully corrected in infants if
casting was started before age 20 months.
Adolescents with curves less than 20 degrees at presentation are observed
and followed at 4-month and 6-month intervals. For curves between 20
degrees and 30 degrees, bracing is started if a curve progresses 5 degrees or
more in two consecutive visits or 10 degrees or more in one visit.
Bracing is usually started the first office visit when the patient is skeletally
immature (Risser ≤2) and presents with a 25- to 40-degree curve. Several
23
brace options exist, and deciding which brace to use depends on the apex of
the curve and physician preference. Curves with an apex above T6 would
likely require the use of a Milwaukee (cervicothoracolumbosacralorthosis)
brace. Conversely, curves with apices at T7 or below and above L2 do well in
a Boston underarm thoracolumbosacral orthosis brace, and these braces are
more socially acceptable because of the lack of a cervical extension. The
Charleston bending brace is an option if the child is noncompliant to brace-
wear. This brace is typically worn at night, and some studies have shown its
efficacy.49,50 The efficacy of a brace seems to depend on the length of time
the brace is worn. When bracing is initiated and pad placement is deemed
appropriate, patient follow-up occurs every 4 to 6 months, with in-brace
radiographic evaluation and appropriate fitting adjustments made when
necessary.
Operative
Operative intervention is usually recommended for patients whose curves
progress despite nonoperative management. In infants, operative intervention
is controversial; it is occasionally performed in infants with curves greater
than 45 degrees or thoracolumbar/lumbar curves greater than 40 degrees.
Children are typically more prone to curve progression and are more likely to
require operative intervention. Other patients who are likely to benefit from
operative intervention are skeletally immature patients with adolescent
idiopathic scoliosis with a greater than 40- to 45-degree curve and mature
patients with curves greater than 50 degrees.
Neuromuscular Scoliosis
A. Introduction
Neuromuscular disorders commonly lead to spinal deformities that are
some of the most challenging treatment dilemmas addressed by spine
surgeons. Despite the various conditions that fall in this category,
neuromuscular disorders involve neurologic or muscular deficiencies that
24
produce progressive multiplanar skeletal deformities. Common features of
neuromuscular scoliosis include the following:
Large curves early in life: Early neuromuscular insult predisposes patients
to rapidly progressive scoliosis.
Stiff curves: These patients are more likely to develop stiff curves because
of the early onset of neuromuscular deficiency resulting in limited
mobility and secondary contractures.
Progressive curves: As in idiopathic scoliosis, the potential for curve
progression is greatest during rapid growth and with loss of ambulation.
Increasing weakness or persistent muscle imbalance around the spine in
patients with neuromuscular disorders can cause progression of scoliosis
independent of growth, however.
Long curves: Less severely affected individuals may have an S-shaped
curve with well-balanced double curves. Long C-shaped curves are more
likely in severely affected patients with resultant sitting imbalance.
Pelvic obliquity: Lower extremity contractures and imbalanced spinal
deformity cause pelvic obliquity, which may impair comfortable sitting for
these patients.
Sagittal plane deformity: Gravity and muscular deficiency can also lead to
sagittal plane deformity, including thoracic or lumbar hyperkyphosis or
lumbar hyperlordosis. Patients with neuromuscular disorders are
challenging because of the complexity of their deformity and fragility of
their overall health and are best treated by an experienced surgeon with
support from a multidisciplinary team.
B. Classification
The classification of neuromuscular scoliosis can be based on the
underlying disorder: neurologic (e.g., cerebral palsy) or muscular (e.g.,
muscular dystrophy). Neurologic deficiencies can be broken down further into
upper motor neuron dysfunction, as seen in myelomeningocele, or lower
motor neuron dysfunction, as seen in spinal muscular atrophy (SMA).
25
C. Natural History
Neuromuscular scoliosis generally begins early in life, is rapidly
progressive, and causes significant morbidity. Some patients are capable of
ambulation, although many lose their ability to walk early in life or never
achieve ambulatory status at all. The use of a wheelchair affords these patients
educational and social opportunities that enrich their lives. Spinal deformity
can impair comfortable sitting and dramatically reduce the individual’s quality
of life. Unbalanced curves and significant pelvic obliquity make wheelchair
positioning difficult and may cause uneven distribution of weight that may
lead to pressure sores. Prominences created by the convexity of a curve may
result in skin breakdown; creases within the concavity of the trunk deformity
are susceptible to skin maceration and infection. Majd and colleagues showed
a correlation between deformity size, functional decline, and decubitus. Large
rigid curves restrict lung volume and impair respiration in patients who often
already have limited pulmonary capacity. Treatment of neuromuscular
scoliosis can also help the caretakers of these patients, improving the ease of
transfers, positioning, feeding, and hygiene. The ultimate goal of treatment of
patients with neuromuscular scoliosis is the maintenance of as much
independence and function as possible. When patients with neuromuscular
scoliosis lose the ability to sit comfortably, their quality of life is dramatically
decreased. The natural history for a given patient is largely determined by the
specific underlying neuromuscular condition and the degree of involvement.
D. Treatment
The basic principles of observing or bracing smaller, flexible curves and
surgically fusing larger, more rigid curves in adolescent idiopathic scoliosis
apply to the treatment of neuromuscular scoliosis, although with less
aggressive parameters.
Observation alone is employed until curves begin to cause functional
impairment. Bracing can be a temporizing measure, used primarily to provide
sitting support while the patient grows. Eventually, many of these patients
26
require surgical stabilization with a spinal instrumentation and fusion
procedure.
27
LORDOSIS
A. Definition
Lordosis is defined as an excessive inward curve of the spine. Some might
also called lordosis as swayback. The spine naturally curves at the neck, upper
back, and lower back to help absorb shock and support the weight of the head,
as well as the body itself. Lordosis occurs when the natural arch in the lower
back, or lumbar region, curves more than normal. This can lead to excess
pressure on the spine, causing pain.17
B. Etiology
Lordosis is found in all age group. It primarily affects the lumbar spine,
but can occur in the neck (cervical). When found in the lumbar spine, the
patient may appear swayback, with the buttocks more prominent and the
stomach seems to be sticking out, and in general an exaggerated posture.18
C. Cause
Up till now, the exact cause of lordosis in childhood remains unknown.
However, lordosis can affect people of any age. Other potential causes of
lordosis include:17,18,19
1. Obesity. Most researchers agree that obesity, especially central
(abdominal) obesity, with Body Mass Index (BMI) more than 24 kg/m2
might increase the lumbar lordosis angle. It is because some overweight
people lean backward to improve balance, and this leads to the change in
lumbar angle over time.
2. Discitis. An inflammation of intervertebral disc space that leads to
changing of lumbar curvature.
3. Osteoporosis. A decrease in bone density may affects the strength of the
bone, compromising the spine’s structural integrity.
4. Spondylolisthesis. This condition occurs when one vertebra slips forward
in relation an adjacent one, usually in the lumbar spine.
28
5. Poor posture. Some studies showed that a posture affects the angle or
vertebra over time. People who spend more time standing in excessive
straight position is said has more lordosis angle than people who are not.
It is hypothetically said that it is due to the prolong tilt of the pelvis by
abdominal muscles.
6. Kyphosis. Kyphosis is a condition where there is an excessive outward
curvature at the mid-back. Kyphosis may force the low back to
compensate for the imbalance created by a curve occurring at a higher
level of the soine.
7. Achondroplasia. A form of dwarfism that affects the alignment of the
vertebra.
D. Diagnosis
Apart from the complaints from patient, a thorough physical examination
needs to be performed in diagnosing a lordosis. The physician will want to
know when the curvature was first noticed, past progression, and other related
symptoms the patient experiences. A simplest way to check for lordosis is to
ask the patient to lie on his back on a hard surface. The physician should be
able to slide his hand under the patient’s back, with little space to spare. In
lordosis, there will be extra space between the hand and the back.17 Other than
that, the patient will be asked to bend forward and to the side to see whether
the curve is flexible or fixed, and to see for any asymmetrical appearance, also
the range of motion to measure the degree to which a patient can perform
movement of flexion, extension, lateral bending and spinal rotation.18 A
neurological evaluation for the symptoms of pain, tingling or numbness,
muscle spasm, weakness and bowel/bladder change will be evaluated to see
how much lordosis has affects the quality of life of the patient.18 Last but not
least, radiographic image will be taken to reveal the entire length of spine.
Radiographic examinations that were asked in lordosis are anterior/posterior
(AP) and lateral x-ray of lumbosacral. Side bending AP x-rays are sometimes
29
used to evaluate the flexibility of the spine, and MRI may be ordered if the
spinal cord has been compromised (or suspected).18
E. Treatment
Treatment for lordosis consists of non-surgical treatment and surgical
treatment. Non-surgical conservative treatment may include:17,18
Analgesics and anti-inflammatory medication.
Physical therapy to help build strength in core muscles, as well as to
enable the patient to build flexibility and increase range of motion.
Bracing maybe used to control curve progression in adolescents.
Reduction of body weight to ideal.
In severe cases, surgical intervention is needed. Surgical intervention is
considered if the lordotic curve is severe, when neurologic involvement exists,
or non-surgical conservative treatment has failed.18
DAFTAR PUSTAKA
1. Sarwark J, editor: Essential of Musculoskeletal care, ed 4, Rosemont, 2010,
AAOS;p.1118
2. Herring JA, editor: Tachdjian’s pediatric orthopaedics, ed 4, Philadelphia,
2008, WB Saunders
30
3. Taylor R, editor : Handbook of Musculoskeletal Problems and Injuries, New
York, 2006, Springer;p.175
4. Annals of Human Biology, Volume 1, Number 3 / July 1974.
5. Kado DM, Prenovost K, Crandall C (2007). "Narrative review: hyperkyphosis
in older persons". Ann. Intern. Med. 147 (5): 330–8. doi:10.7326/0003-4819-
147-5-200709040-00008. PMID 17785488.
6. Keller TS, Harrison DE, Colloca CJ, Harrison DD, Janik TJ (2003).
"Prediction of osteoporotic spinal deformity". Spine 28 (5): 455–62.
doi:10.1097/00007632-200303010-00009. PMID 12616157.
7. Osteopathy: A Complete Health Care System, by Leon Chaitow N.D., D.O.,
M.R.O.
8. http://www.back.com/back-pain/conditions/scoliosis/index.htm
9. Natural History of Congenital Kyphosis and Kyphoscoliosis. A Study of One
Hundred and Twelve Patients – MCMASTER and SINGH 81 (10): 1367 –
Journal of Bone no People and Joint Surgery
10. Bautmans I, Van Arken J, Van Mackelenberg M, Mets T. Rehabilitation using
manual mobilization for thoracic kyphosis in elderly postmenopausal patients
with osteoporosis. J Rehabil Med. Feb 2010;42(2):129-35. [Medline].
11. Tribus CB. Scheuermann's kyphosis in adolescents and adults: diagnosis and
management. J Am Acad Orthop Surg. Jan-Feb 1998;6(1):36-43. [Medline].
12. Damborg F, Engell V, Anderson M, et al. Prevalence, concordance, and
heritability of Scheuermann kyphosis based on a study of twins. J Bone Joint
Surg Am. 2006;88(10):2133-6. [Medline].
13. Miller MD, Thompson SR, Hart JA. Review of Orthopaedics, ed 6,
Philadelphia, 2012, Elsevier Saunders;p.253, miller's review 253
14. Sarwark, John F. Essentials of Muskuloskeletal Care. 4th Edition. P. 1118-
1121
15. Reamy Brian. Adolescent Idiopathic Scoliosis : Review and Current Concepts.
Volume 64. July 2001
16. Rothman-simeone The Spine. 6th edition. Volume 1. Chapter Scoliosis
31
17. Gabbey A.E., Krucik G. Lordosis. [online] Downloaded at: http://www.healthline.com/symptom/lordosis (13th January 2015)
18. Regan J.J., Herkowitz H.N. A Closer Look at Lordosis. Updated 9 th July 2012. [online] Downloaded at: http://www.spineuniverse.com/conditions/spinal-disorders/closer-look-lordosis (13th January 2015)
19. Been E., Kalichman L. Perspective: Lumbar Lordosis. The Spine Journal.
Elsevier Inc. 2013 [online] Downloaded at: https://lumbar%20lordosis1-s2.0-
S1529943013013855-main.pdf (13th January 2015)
32