spmc 4: a case based discussion on tetrology of fallot
TRANSCRIPT

CASE PRESENTATIONINTERNAL MEDICINE
RAJKUMAR EUNICETHAKAR KRUPALI
GENERAL DATA
Name: A.C.Age:22
Sex: FemaleReligion: Roman Catholic
Address: Poblacion,Dominal.
CHIEF COMPLAINT
STOMACH PAIN
HISTORY OF PRESENT ILLNESS• a diagnosed case of a cyanotic dse since birth (blue baby
syndrome.)
• lethargic and low on energy since birth with DOB with exertion like walking or running.
1 month PTA
• a sudden onset of dull epigastric pain rated 5/10 which would be on and off with no relieving or aggravating factors. There was no associated diarrhea, vomiting,dysuria,oliguria,pyuria or fever associated with it.
1 week PTA
•The patient’s above mentioned epigastric pain continued with the same characteristics which was now rated as 8/10.

PERSONAL SOCIAL HISTORYLifestyle:
Wakes at 7:00 am Breakfast: 8 am Mostly stays at home
cooking,resting,sleeping. Dinner 8-9 pm Sleep 10-11 pm No known allergies
Diet: Rice, fruits, chicken and pork.
Habit:
• Non alcoholic non smoker.
Single, Has completed 4th yr high skl in 2013.

Past Medical HistoryDx case of a cyanotic heart dse since birth. Was a full term baby.No previous surgeries or hospitalizations. Non hypertensive, non asthmatic
Immunizations Cannot recall if he had taken any immunizations.
Family historyNo sibblings or parents have any heart dse. No HTN,diabetes,ashtma or other known illness in family.
REVIEW OF SYSTEMS
General: (+)syncope Eye: (+) Redness noted few months ago. Ears: no tinnitus, vertigo or infections Nose: no nasal catarrh or epistaxis Mouth: no fissures or sores or bleeding gums GI: no scars, no distended abdomen, no masses.

Pulmonary sys: Difficulty of breathing w/ exertion. No orthopnea.
Cardiac: Cyanotic hrt dse since birth. (+) dyspnea, (-)orthopnea, (-) chest pain and palpitations.
Skin: Cyanosis noted since birth Neurologic sys: (-) seizure, sensory
perversions or neurologic deficits. Hematopoetic: no history of abnormal bleeding.
(-) petechiae (-) purpura. Psychiatric: no hx of depression or treatment of
psychiatric disorders like anxiety, violence or illusions.
Physical examination
Temperature: 36.9⁰C Respiratory rate: 30 Cardiac rate: 83 Weight: 42 kg Height: 137.16 cm BMI: 22.6 Blood pressure: 130/80
Physical examination
General description:
The patient is quick to respond
Alert
Skin:
No rashes No petechiae or purpura clubbing of nails and
cyanosis noted
Lymph nodes• Lymph nodes not palpable
Skull:• No deformities• No signs of trauma
Physical examination
Eyes: Well distributed hair in
eyebrows Anicteric sclera Pink palpebral
conjunctiva with no exudates
Periorbital edema Presences of red orange
reflex, no hemorragic arteries noted
Ears:
Pinna appear normal Both ear canals are clear
with no exudates Tympanic membrane
with good cone of light Good acuity to whispered
voice
Physical examination
Nose:
Septum midline No nasal catarrh or
discharge No tenderness
Mouth and throat: Oral mucosa dusky blue Cyanotic lips Good dentition Tongue midline Pharynx with no
exudates Tonsils not inflamed
Physical examination
Neck:
Supple Thyroid lobes not felt No distended neck veins
Breast:
No ulcerations or discharge
Chest: • I-Thorax symetrical• Good excursion• P- equal tactile fremitus in
both lungs• P-Lungs resonant• A-Breath sounds vesicular
Cardiac:• I- adynamic precordium• P-No thrills or heaves felt• A-Apex beat: 5th ICS 8-9 cm from
midsternum; no S3 or S4 heard• grade II systolic murmur at the
llsb

Physical examination
Abdomen:
I- not Protuberent No scars noted,
discolorations A- normoactive bowel
sounds P-Tympanic abdomen on
percussion P-Liver palpable 1 cm
below right costal margin
Extremities:
Not Edematous Presence of clubbing No varicosities but presence
of cyanosis No ulcerations, rashes or
lacerations noted

Physical examination
Musculoskeletal:
Can sit errect without support
No joint pain or deformity Spine curvature normal
with no scoliosis Good range of motion in ,
wrists, elbows, shoulders, hips, knees and ankle
Conscious level: The patient was not lethargic
or stuporous
Mental status:• Alert and cooperative• Thought coherent, oriented to
person, place and time

Physical examinationCranial nerves:I – Patient was able to smellII – Visual fields full to confrontation. Reactive pupils.III, IV & VI – Normal EOM movement and intact pupillary reflexesV – Facial sensation intact to pinprick. Corneal reflex is present.VII – Symmetrical facial movementVIII – Equal hearing on both sidesIX, X – No difficulty swallowing, no hoarsenessXI – Able to shrug both shoulders XII- No tongue deviation
Gait: Stable gait Can sit and walk without
support
Motor: • Good muscle bulk and tone• Strength 5/5
Sensory:
• Sensitive to pin prick, light touch and vibration senstive
Differential DiagnosisCyanosis,Clubbing,
polycythemia, epigastric pain, grade II systolic
murmurWhat could it be..??
Heart disease..? Lung disease..? What’s with the epigastric pain?

22 yrs old, female. non alcoholic, non smoker
Clubbing, Cyanosis, grade II systolic murmur llsb, epigastric pain(8/10) decrease in pain after food intake(2/10)
The pt is on furosemide, spironolatone
Epigastric pain, 8/10
Acutegastritis
GERD
• No nausea• No vomitting• No loss of
appetite
Cholelithiasis• no chest pain• No burning
sensation• No dry cough• No sore throat• No dysphagia• No regurgitation
• No loss of appetite• No clay colored stool• Pain relieved after food intake• No fever, chills• No nausea,vomiting• No jaundice
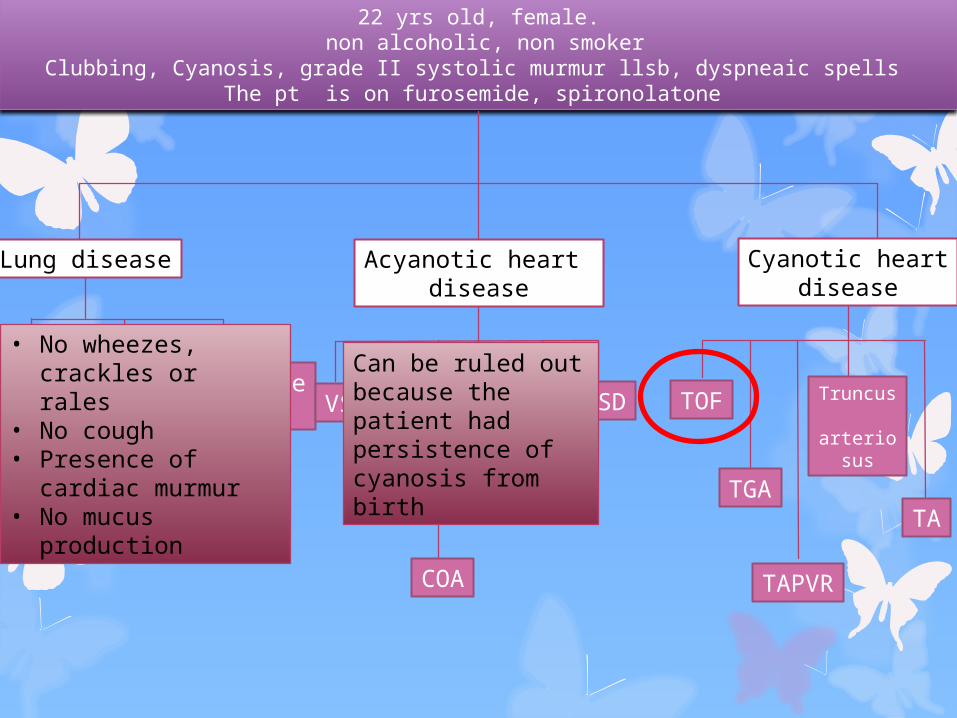
22 yrs old, female. non alcoholic, non smoker
Clubbing, Cyanosis, grade II systolic murmur llsb, dyspneaic spells The pt is on furosemide, spironolatone
Lung disease Acyanotic heart disease
Cyanotic heartdisease
COPD
Pulmonary embolism
Acute severeasthma
• No wheezes, crackles or rales
• No cough• Presence of cardiac
murmur• No mucus
production
VSD
COA
PDA
PS AS
AVSDCan be ruled out because the patient had persistence of cyanosis from birth
TOF
TGA
TAPVR
Truncus
arteriosus
TA
ADMITTING IMPRESSION
ACUTE GASTRITIS AND TETROLOGY OF FALLOT

ACUTE GASTRITIS
DISRUPTION OF MUCUS LAYER
INCREASED ACID PRODUCTIONDECREASED BICARBONATE
DIRECT DAMAGE TO EPITHELIUM
ULCERATIONS BLEEDING

TETROLOGY OF FALLOTALSO CALLED
BLUE BABY SYNDROME
Pulmonary stenosisVSD
Overriding AortaRV hypertrophy

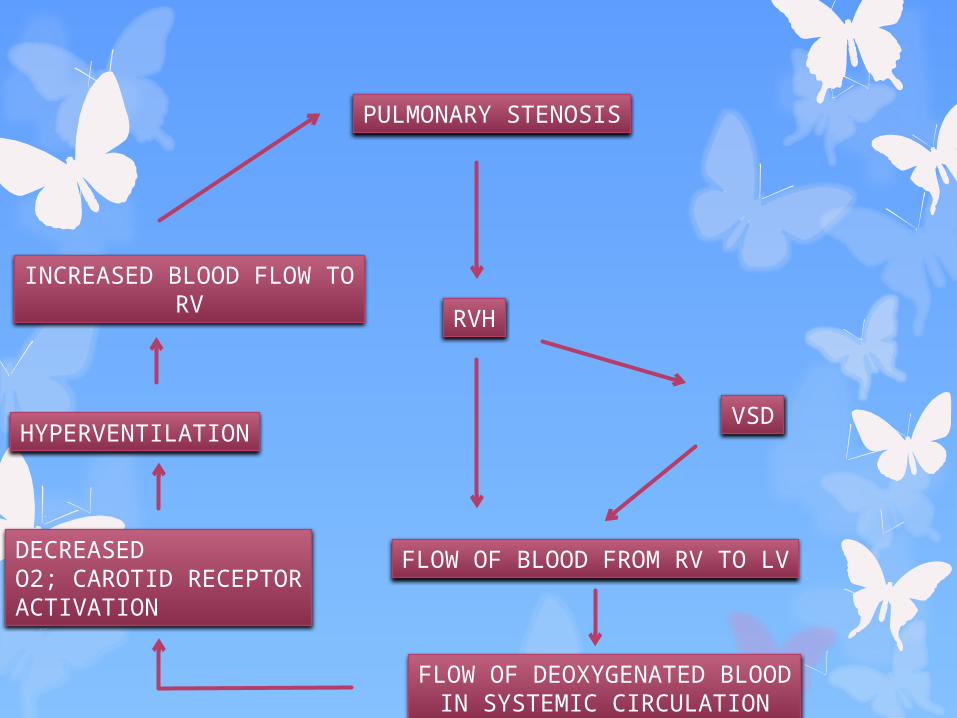
PULMONARY STENOSIS
RVH
VSD
FLOW OF BLOOD FROM RV TO LV
FLOW OF DEOXYGENATED BLOODIN SYSTEMIC CIRCULATION
DECREASEDO2; CAROTID RECEPTORACTIVATION
HYPERVENTILATION
INCREASED BLOOD FLOW TORV
