sport related concussion pathology (patients with mtbi who died of other causes) • microscopic...
TRANSCRIPT

Sport Related Concussion
Andy Peterson MD MSPH FAAP

Disclosures
• I have no financial or personal interests in
products discussed today
• I may briefly discuss off-label use of
medications for the treatment of post-
concussion symptoms.
• I will discuss only 1 brand of NCT. Several
others are available on the market.

• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• (Concussion Clinic Protocol and Evidence Base)
• Recognition / Evaluation / Return to Play
Covered Today
boring
not boring

471 concussion review articles in past 5 years!



• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today

Concussion definitions:
• 1966 Congress of Neurological Surgeons
– Concussion is a clinical syndrome
characterized by immediate and transient
impairment of neural functions, such as
alteration of consciousness, disturbance of
vision, equilibrium, etc, due to mechanical
forces

Concussion definitions:
• American Academy of Neurology:
– Trauma-induced alteration in mental status that
may or may not involve loss of consciousness.
Concussion definitions:
• Zurich Statement – Concussion is defined as a complex pathophysiological process affecting the
brain, induced by traumatic biomechanical forces. Several common features that
incorporate clinical, pathologic and biomechanical injury constructs that may be
utilized in defining the nature of a concussive head injury include:
• Concussion may be caused either by a direct blow to the head, face, neck or elsewhere
on the body with an “impulsive” force transmitted to the head.
• Concussion typically results in the rapid onset of short-lived impairment of neurologic
function that resolves spontaneously.
• Concussion may result in neuropathological changes, but the acute clinical symptoms
largely reflect a functional disturbance rather than a structural injury.
• Concussion results in a graded set of clinical symptoms that may or may not involve loss
of consciousness. Resolution of the clinical and cognitive symptoms typically follows a
sequential course; however, it is important to note that, in a small percentage of cases,
post-concussive symptoms may be prolonged.
• No abnormality on standard structural neuroimaging studies is seen in concussion.

Common features: • May be caused by direct blow or transmitted blow to the head.
• Rapid onset of short-lived neurologic impairment that resolves
spontaneously.
• May cause neuropathological changes but symptoms usually
due to functional rather than structural injury.
• Typically follows a graded and sequential course.
• Usually does not involve loss of consciousness.
• Normal structural neuroimaging studies

Common symptoms
• Headache or head pressure
• Balance disturbance or dizziness
• Nausea
• Felling “dinged,” “foggy” or “stunned”
• Visual problems
• Hearing problems
• Irritibility or emotionality

Common cognitive features
• Unaware of score of game, period,
opposition
• Confusion
• Amnesia
• Loss of consciousness

Common physical signs • Transient impaired consciousness (GCS < 15)
• Poor coordination or balance
• Seizure
• Slow to answer questions or follow directions
• Easily distracted, poor concentration
• Inappropriate emotions
• Vomiting
• Vacant stare/glassy eyed
• Slurred speech
• Personality changes
• Inappropriate behavior
• Decreased playing ability

• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today

Gross/micro pathology (patients with MTBI who died of other causes)
• Microscopic axonal injury
• Axon retraction bulbs
• Microglial clusters
• (Tau deposition)

Pathophysiology • Cortical contusions
• Axonal rupture/stretch/shear
• Cell membrane permeability
• Release of excitatory neurotransmitters from injured axons impairs function of nearby cells – Acetylcholine
– Glutamate
– Aspartate
• ENERGETICS!


Farkas O, Lifshitz J, Povlishock JT. J Neurosci. 2006 Mar
A-C Neurons flooded with both dextrans revealing cellular injury with irregular distorted profiles
and vacuolization (arrows) Most severe show uptake in nucleus (double arrow)
D – Other double labeled axons demonstrate little or no pathologic damage


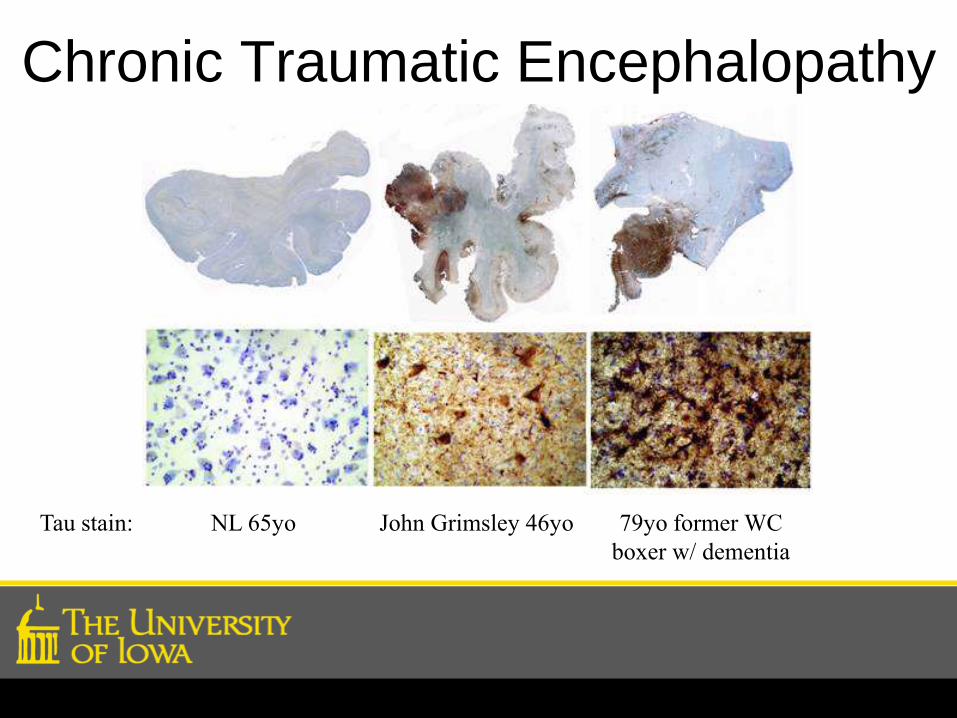
Chronic Traumatic Encephalopathy
Tau stain: NL 65yo John Grimsley 46yo 79yo former WC
boxer w/ dementia

Dave Duerson (and 153+ others)
Maroon et al. PLOS ONE. 2015.





• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today

Epidemiology
• Difficult due to underreporting
• Probably 1.6 to 3.8 million per year
• ~65% in 5-18yo
• Most do not come to clinical attention Nonfatal traumatic brain injuries from sports and recreation activities--United States, 2001-2005. MMWR Morb Mortal Wkly Rep.
Jul 27 2007;56(29):733-737.
McCrea M, Hammeke T, Olsen G, Leo P, Guskiewicz K. Unreported concussion in high school football players: implications for prevention.
Clin J Sport Med. Jan 2004;14(1):13-17.

Lincoln AJSM 2011

Lincoln AJSM 2011

Marar AJSM 2012

Zuckerman AJSM 2015

2.79%

What do these have in common?
Football
Boxing
Hockey
Wrestling
Soccer
Rugby
Baseball
McKee Acta Neuropathol (2014) 127:29-51


2015 NCAA Wrestling Rule Change
Rule 6.1.5 – Referee Timeout, Concussion Evaluation Timeout
In the case of a possible concussion, the referee shall stop the
match for a concussion evaluation. The medical staff shall have
unlimited and unimpeded time to evaluate the participants. In
cases of uncertainty, the medical staff shall be granted the ability
to remove the participant from the wrestling area to perform the
concussion evaluation. During the evaluation, the match will be
suspended until a decision is rendered. The referee, the coaches
of both participants and the non-injured wrestler are to remain on
the mat. A concussion evaluation timeout shall not count towards
the contestant’s injury timeout or recovery timeout. Coaching of
the contestant being evaluated is not permitted.

• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today


Iowa Concussion Law BE IT ENACTED BY THE GENERAL ASSEMBLY OF THE STATE OF IOWA:
Section 1. NEW SECTION. 280.13C Brain injury policies.
1. a. The Iowa high school athletic association and the
Iowa girls high school athletic union shall work together to
distribute the guidelines of the centers for disease control
and prevention of the United States department of health and
human services and other pertinent information to inform and
educate coaches, students, and the parents and guardians
of students of the risks, signs, symptoms, and behaviors
consistent with a concussion or brain injury, including
the danger of continuing to participate in extracurricular
interscholastic activities after suffering a concussion or
brain injury and their responsibility to report such signs,
symptoms, and behaviors if they occur.

b. Annually, each school district and nonpublic school shall
provide to the parent or guardian of each student a concussion
and brain injury information sheet, as provided by the Iowa
high school athletic association and the Iowa girls high
school athletic union. The student and the student’s parent
or guardian shall sign and return the concussion and brain
injury information sheet to the student’s school prior to the
student’s participation in any extracurricular interscholastic
activity for grades seven through twelve.
Iowa Concussion Law

2. If a student’s coach or contest official observes signs,
symptoms, or behaviors consistent with a concussion or brain
injury in an extracurricular interscholastic activity, the
student shall be immediately removed from participation.
Iowa Concussion Law

3. a. A student who has been removed from participation
shall not recommence such participation until the student has
been evaluated by a licensed health care provider trained in
the evaluation and management of concussions and other brain
injuries and the student has received written clearance to
return to participation from the health care provider.
b. For the purposes of this section, a “licensed health care
provider” means a physician, physician assistant, chiropractor,
advanced registered nurse practitioner, nurse, physical
therapist, or athletic trainer licensed by a board designated
under section 147.13.
c. For the purposes of this section, an “extracurricular
interscholastic activity” means any extracurricular
interscholastic activity, contest, or practice, including
sports, dance, or cheerleading.
Iowa Concussion Law

Unintended Consequences?? (so far there is no evidence on either side)
• Incentive to under-report
• False sense of security
– Untrained coaches/officials
– Uncertainty about who can clear
• Bypass ATC?
• Transfer of liability
• Cost
• Second guessing officials

• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today


Johnny doesn’t have a concussion.
He didn’t get knocked out and had
a normal CT scan

Berrington et al. Projected Cancer Risk from Computed Tomographic Scans Performed in the United States in 2007. Arch Intern Med.
2009;169(22).

OK, when should I image? • In the hours after an injury if:
– Worsening symptoms
– Declining level of consciousness
– Worsening amnesia
– Progressive balance disturbance
– Focal neurologic deficits
• Later if:
– Seizures
– Declining mental status

What’s coming
• PET
• SPECT
• (fMRI)
• DTI with Tractography

Fractional Anisotropy
Wilde EA et al. Neurology. 2008 Mar
Free diffusion Diffusion in one direction

Singh Met al. Magn Reson Imaging. 2010 Jan


Qualities for an ideal biomarker?
1. Sample source (CSF, serum, saliva, urine)
2. Sensitivity and specificity
3. Signal vs background

Biomarkers of Brain Injury Biochemical
Marker
Physiologic Role Location Comment
Neuron Specific
Enolase
(NSE)
Involved in
increasing neuronal
chloride levels
Cytoplasm of
neurons, platelets,
RBC’s
Detectable within 6
hours, serum half
life of 24 hours
S100B
Calcium binding
protein, may inhibit
synaptic plasticity
Astroglia, bone
marrow, fat, skeletal
muscle
Detectable almost
immediately after
injury, ½ life 60 min
Myelin Basic Protein
(MBP)
Abundant protein in
myelin
Myelin Increased only after
severe TBI, peaks
48-72 hours
Cleaved Tau
(c-tau)
Microtubule
associated protein in
axons
Axons in the CNS Poor marker in
pediatric population
Glial Fibrillary Acidic
Protein
(GFAP)
Intermediate protein
of astroglial skeleton
Astroglial skeleton Peaks in 24-48
hours found only in
CNS

The more I rest now, the quicker I
will recover.


Moser, Glatts and Schatz. Jpeds. 2012.
49 high school and college athletes. Rest for 1 or 2 weeks
when concussed. Measured ImPACT.

Moser, Glatts and Schatz. Jpeds. 2012.

Thomas, et al. Pediatrics. 2015.

Thomas, et al. Pediatrics. 2015.

Thomas, et al. Pediatrics. 2015.
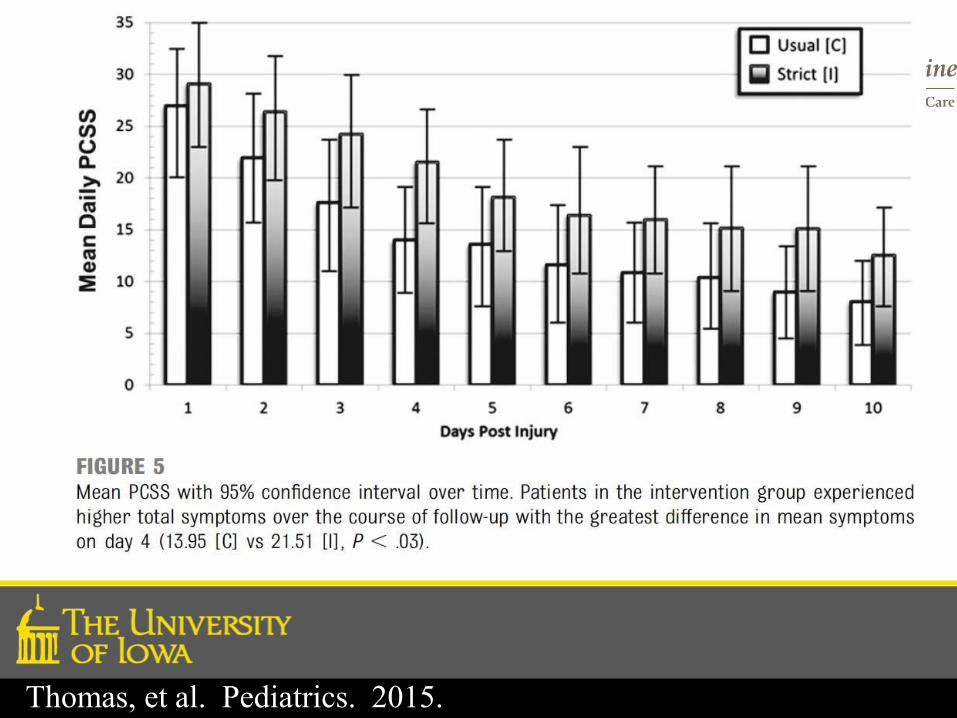
Thomas, et al. Pediatrics. 2015.

Silverberg, et al. JAMA Pediatrics. 2016.

Silverberg, et al. JAMA Pediatrics. 2016.

Silverberg, et al. JAMA Pediatrics. 2016.

I just got Johnny this sweet
mouthguard. It will protect him from
concussions.

John Stenger DDS
Notre Dame dentist
1964
5 case reports of players
who were concussion
prone before mouthguard
but not after


Wisniewski DDS
Guskiewicz PhD
2004
large NCAA dataset
506,297 exposures
369 concussions


McGuine PhD
Brooks MD
2014
large high school dataset
2287 players
134,437 exposures
211 concussions








“Unfortunately, no helmet can prevent a concussion”

“Unfortunately, no helmet can prevent acconcussion”













What does work?
• Limit hitting
• Limit hitting
• Limit hitting
• Limit hitting
• Maybe changing the way people hit





Pellman et al. Neurosurgery. 2004





Broglio, et al. JAT. 2016
Followed rule change – unlimited tackling to tackling 2x per week.

Broglio, et al. JAT. 2016

Johnny just got his third
concussion. I already told him that
this means he has to quit sports.

Number of Concussions
Am
ount
of
Bad
nes
s

When to consider disqualification
• Multiple lifetime concussions
• Persistent diminished performance
• Persistent post concussive symptoms
• Progressively prolonged recoveries
• Easy concussability

I sure am glad little Suzy doesn’t play such dangerous sports.

Marar AJSM 2012

I’m going to make
sure Billy doesn’t
start playing
football too early.
Gotta protect his
brain

OR 1.93 (1.74-2.15)
1.7% concussion 3.3% concussion
Increased risk PCS with mTBI2 1. Nation et al. Football-Related Injuries Among 6- to 17-Year-Olds Treated in US Emergency Departments 1990-2007. Clin Pediatr. 2011
Mar;50(3):200-7.
2. Falk et al. The specificity of post-concussive symptoms in the pediatric population. J Child Health Care. 2009 Sept;13(3):227-38.

Peterson et al. In press. OJSM. 2016.


• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today
My doctor told me that I have a
grade 2 concussion and can return
to play in a week.


What about LOC?
Does not predict severity,
neuropsychological test results,
duration of symptoms or balance test
results.

• Maroon JC, Lovell MR, Norwig J, Podell K, Powell JW, Hartl R. Cerebral concussion
in athletes: evaluation and neuropsychological testing. Neurosurgery. Sep
2000;47(3):659-669; discussion 669-672.
• Jennett B, Bond M. Assessment of outcome after severe brain damage. Lancet. Mar
1 1975;1(7905):480-484.
• Lovell MR, Iverson GL, Collins MW, McKeag D, Maroon JC. Does loss of
consciousness predict neuropsychological decrements after concussion? Clin J
Sport Med. Oct 1999;9(4):193-198.
• Leininger BE, Gramling SE, Farrell AD, Kreutzer JS, Peck EA, 3rd.
Neuropsychological deficits in symptomatic minor head injury patients after
concussion and mild concussion. J Neurol Neurosurg Psychiatry. Apr
1990;53(4):293-296.
• Erlanger D, Saliba E, Barth J, Almquist J, Webright W, Freeman J. Monitoring
Resolution of Postconcussion Symptoms in Athletes: Preliminary Results of a Web-
Based Neuropsychological Test Protocol. J Athl Train. Sep 2001;36(3):280-287.
• McCrory PR, Ariens T, Berkovic SF. The nature and duration of acute concussive
symptoms in Australian football. Clin J Sport Med. Oct 2000;10(4):235-238.

Zemek et al. JAMA. 2016.
• 9 large peds ER (PERC)
• 2 years
• 46 item derivation
• 2006 participants
• 9 item validation
• 1057
Low cut point
• Sensitivity 95%
• Specificity 18.1%
• NPV 85%
• PPV 36%
High cut point
• Sensitivity 20%
• Specificity 93%
• NPV 70%
• PPV 60%

Prague subtypes:
• Simple concussion
• Complex concussion
McCrory P, Johnston K, Meeuwisse W, et al. Summary and agreement statement of the 2nd International Conference on Concussion in Sport,
Prague 2004. Br J Sports Med. Apr 2005;39(4):196-204.

Zurich subtypes:
McCrory P, Meeuwisse W, Johnston K, et al. Consensus Statement on Concussion in Sport: the 3rd International Conference on Concussion in
Sport held in Zurich, November 2008. Br J Sports Med. May 2009;43 Suppl 1:i76-90.
McCrory P, et al. Consensus Statement on Concussion in Sport: the 4th International Conference on Concussion in Sport held in Zurich,
November 2012. Br J Sports Med 2013;47:250–258


1. Harmon KG, et al. American Medical Society for Sports Medicine Position Statement:
Concussion in Sport. Br J Sports Med. Jan 2013;47:15-26.
2. McCrory P, et al. Consensus Statement on Concussion in Sport: the 4th International
Conference on Concussion in Sport held in Zurich, November 2012. Br J Sports Med
2013;47:250–258
3. Herring S, et al. Concussion (Mild Traumatic Brain Injury) and the Team Physician: A
Consensus Statement – 2011 Update. Med Sci Sports Exerc. Dec 2011;43(12):2412-22.
4. McCrory P, Meeuwisse W, Johnston K, et al. Consensus Statement on Concussion in
Sport: the 3rd International Conference on Concussion in Sport held in Zurich, November
2008. Br J Sports Med. May 2009;43 Suppl 1:i76-90.
5. McCrory P, Johnston K, Meeuwisse W, et al. Summary and agreement statement of the
2nd International Conference on Concussion in Sport, Prague 2004. Br J Sports Med. Apr
2005;39(4):196-204.
6. Aubry M, Cantu R, Dvorak J, et al. Summary and agreement statement of the First
International Conference on Concussion in Sport, Vienna 2001. Recommendations for the
improvement of safety and health of athletes who may suffer concussive injuries. Br J
Sports Med. Feb 2002;36(1):6-10.
7. Guskiewicz KM, Bruce SL, Cantu RC, et al. National Athletic Trainers' Association
Position Statement: Management of Sport-Related Concussion. J Athl Train. Sep
2004;39(3):280-297.
8. Concussion (mild traumatic brain injury) and the team physician: a consensus statement.
Med Sci Sports Exerc. Nov 2005;37(11):2012-2016.

Second Impact Syndrome
• By 1998, there had been 17 published cases. A review (McCrory 1998) demonstrated that only 5 of these were likely to be second impact syndrome
• Numerous case reports published in late 1990’s/early 2000’s. Validity of claims not rigorously reviewed.


17/138 had recent concussion!

What to know about Zurich 1. Don’t grade concussions
2. Symptoms are key (signs are less helpful)
3. LOC does not predict outcome
4. Amnesia poorly predicts outcome
5. Seizures do not predict outcome
6. Repeat concussions are probably bad
7. Kids aren’t just little adults
8. Elite athletes should not be treated differently
9. Use a graduated return to play McCrory P, et al. Consensus Statement on Concussion in Sport: the 4th International Conference on Concussion in Sport held in Zurich,
November 2012. Br J Sports Med 2013;47:250–258

• Definitions
• Basic Pathophysiology (and CTE)
• Basic Epidemiology
• Iowa Concussion Law
• Common Misconceptions
• Review of Recent Concussion Guidelines
• Concussion Clinic Protocol and Evidence Base
• Recognition / Evaluation / Return to Play
Covered Today

Concussion Clinic Protocol • Preseason Preparation
• Concussion Recognition
• Initial Concussion Evaluation
• Initial Rest
• Monitor Symptoms
• +/- Neurocognitive testing
• +/- All sorts of rehabilitation techniques
• Graduated return to play


Graduated RTP 1. Complete physical and cognitive rest.
2. Aerobic exercise (e.g. walking, swimming, stationary bike,
etc.) First easy, then harder.
3. Sport-specific exercise (e.g. skating, running, etc.)
4. Non-contact training drills (e.g. passing drills in football or
hockey)
5. Full contact practice
6. Normal game play
McCrory P, et al. Consensus Statement on Concussion in Sport: the 4th International Conference on Concussion in Sport held in Zurich,
November 2012. Br J Sports Med 2013;47:250–258


Preseason Assessment
• Concussion predicts concussion
• Girls are at higher risk
• Sport, position and style of play are strongest
predictors of risk
• Genetics - ???
• Mood, Learning and Attention Disorders
• Migraine headaches


Marar AJSM 2012

Pellman et al. Neurosurgery. 2004

Pellman et al. Neurosurgery. 2004

Genetics • ApoE promoter (g-219T) homo
• OR 2.7 (1.1-6.8)1,2
• Tau ser53pro homo
• OR 8.4 (1.03-68.79)1
• Apo E2 + E4 + promoter
• OR 9.8 (1-96.6)1
• Previous concussion
• OR 1.75 (1.11-2.76)3
• Family History?
• Largest prospective cohort shows no association (Terrell,
unpublished ongoing research)
1. Terrell et al. APOE, APOE Promoter, and Tau Genotypes and Risk for Concussion in College Athletes. Clin J Sport Med. Jan 2008;18(1):10-17.
2. Tierney et al. Apolipoprotein E Genotype and Concussion in College Athletes. Clin J Sports Med. Nov 2010;20(6):464-468.
3. Hollis et al. Incidence, risk and protective factors of mild traumatic brain injury in a cohort of Australian nonprofessional male rugby players. Am J Sports Med. Dec
2009;37(12):2328-33.

Migraine
Gordon et al. BJSM. 2006

Concussion Clinic Protocol • Preseason Preparation
• Concussion Recognition
• Initial Concussion Evaluation
• Initial Rest
• Monitor Symptoms
• +/- Neurocognitive testing
• +/- All sorts of rehabilitation techniques
• Graduated return to play

Concussion Recognition (47.3% of concussions in HS football players unreported)
McCrea et al. CJSM. 2004.

Initial Evaluation
(most use SCAT3)

BJSM 2013

1. GCS
2. Maddocks sideline assessment score
3. Concussion Symptom Severity Score
4. Cognitive assessment
5. Neck Examination
6. Balance examination (Double, Single, Tandem
stance)
7. Coordination examination (FNF)
8. Delayed recall



Symptom Score Checklists
Lots of different scales and different items
Research still being conducted on usefulness
How many items?
Which questions?
Sensitivity/Specificity?
Predictability?
How to administer?
Clusters of scores?

17 64
X X

Time
Sym
pto
ms


0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29
To
tal S
co
re
Day
a2605F
Peterson, et al. CJSM 2014

-70
-60
-50
-40
-30
-20
-10
0
10
20
30
40
50
60
70
0 10 20 30 40 50 60 70 80 90 100
Sc
ore
Dif
fere
nc
e
Mean Day Score
Within Day score SD: 11.4 (95%CI: 9.9, 13.4 Repeatability coefficient: +/- 31.5 (two scores on the same day will differ within this limit 95% of the time.
Peterson, et al. CJSM 2014

BESS – Our best validated test??
Sensitivity 34-64%
Specificity 91%
Assuming 2/10000 concussion rate
99.8% of positive screening will be false
positive
McCrea. J Int Neuropsychological Soc. 2005
McCrea. JAMA. 2003
Guskiewicz. AJSM. 2000
Barr. J Int Neuropsychological Soc. 2001

BESS
Video 23 football athletes
7 scorers
18.9 15.4
-3.5 (“meaningful
difference” is 4)
95%CI -6.2 - 0.67
IRR 0.745, 0.653
Mathiasen et al. CJSM 2013

All Players
1st Test Mean (Std)
(n = 48)
2nd Test Mean (Std)
(n=48)
Mean ∆ (95% CI)
p-value
Cumulative BESS Score 20.3 (6.1)
16.8 (6.4)
-3.55 (-5.27 – -1.82)
0.0001
Cumulative Firm Score 5.0
(4.0) 3.6
(3.2) -1.36
(-2.35 – 0.38) 0.0079
Cumulative Foam Score 15.4 (4.0)
13.2 (4.4)
-2.18 (-3.66 – -0.71)
0.0047
Peterson and Slayman, CJSM 2014

King-Devick Test

King-Devick Test

King Devick
Lots of small recent studies
Methods can be questioned in many of the studies with conclusions being made No description of how unwitnessed concussions are being diagnosed
Unsure if there is applicability over time
Questions on confounding variables to performance Fatigue, learning effect, effort on test
Big PR machine for this test currently
“King-Devick Test in association with Mayo Clinic” Website says can be used for concussions, learning and reading
disabilities, dyslexia, sleep deprivation, ALS, Parkinson’s, MS, hypoxia
May have utility as one of the TOOLS in the toolbox but not conclusive evidence at this point that it can be a sole determinant for sideline evaluation of concussion
Not immune from sandbagging

Clinical Reaction Time Test
May be a ‘poor man’s’ neurocognitive
alterative to assessing reaction time
Good correlation with computerized reaction
times

Vestibular/Ocular Motor Screen (VOMS)
Worse symptoms?
Smooth Pursuit
Horizontal Saccade
Vertical Saccade
Convergence
Horizontal VOR
Visual Motion
Distance
Near Point Convergence

Mucha. AJSM 2015


Kontos. AJSM 2015
264 unconcussed college athletes
Similar test-retest reliability as Mucha
11% false positive rate men
33% false positive rate women
77% false positive rate if history of motion
sickness

Other
C3 Logix
BrainScope
Pupilometer
Eye tracking / saccade tools
Balance tools (iPad, Wii, biosway)
Visual evoked potential tools
Abnormal speech recognition tools

Who should perform the concussion
evaluation in competition?

Should coaches be present?

Concussion Clinic Protocol • Preseason Preparation
• Concussion Recognition
• Initial Concussion Evaluation
• Initial Rest
• Monitor Symptoms
• +/- Neurocognitive testing
• +/- All sorts of rehabilitation techniques
• Graduated return to play

Rest/Monitor
• Mood
• Meds
• Activity

Concussion Clinic Protocol • Preseason Preparation
• Concussion Recognition
• Initial Concussion Evaluation
• Initial Rest
• Monitor Symptoms
• +/- Neurocognitive testing
• +/- All sorts of rehabilitation techniques
• Graduated return to play

ImPACT Immediate Postconcussion Assessment and Cognitive Testing
• Computer based NCT
• 30-45 minutes (compared to 3h)
• Increases sensitivity for persistent
concussion symptoms (VanKampen
2006)

ImPACT
• Concussion Symptom Severity Score
• Word memory = learning and retention
• Design memory = learning and retention
• X&O’s = visual working memory and cognitive speed
• Symbol match = memory and visual motor speed
• Color match = impulse inhibition and visual motor speed
• Three letter memory = verbal working memory and cognitive speed




1. Schatz et al. Sensitivity and Specificity of the ImPACT Test Battery for Concussion in Athletes. Arch Clin Neuropsychol. 2006
Jan;21(1):91-9.
2. McCrea et al. Standard Regression-Based Methods for Measuring Recovery After Sport-Related Concussion. J Inter Neuropsychol Soc.
2005 Jan;11(1):58-69.
Remember, cNCT only improves sensitivity!

Concussion Clinic Protocol • Preseason Preparation
• Concussion Recognition
• Initial Concussion Evaluation
• Initial Rest
• Monitor Symptoms
• +/- Neurocognitive testing
• +/- All sorts of rehabilitation techniques
• Graduated return to play

• NSAID for headache?2
• Triptans for migraines3
• Melatonin for sleep4,5
• TCA for somatic symptoms6,7
• SSRI or TCA for depression8-10
• Stimulants for distractability11
• Psychology for coping12-14
No medications really fix the problem1
1. Beauchamp et al. Pharmacology of traumatic brain injury: where is the “golden bullet”.
Mol Med 2008;14:731–40.
2. Lenaerts ME, Couch JR. Posttraumatic headache. Curr Treat Options Neurol 2004;6:507–
17.
3. Haas DC. Chronic post-traumatic headaches classified and compared with natural
headaches. Cephalalgia 1996;16:486–93.
4. Samantaray et al. Therapeutic potential of melatonin intraumatic central nervous system
injury. J Pineal Res 2009;47:134–42.
5. Maldonado et al. The potential of melatonin in reducing morbidity-mortality after
craniocerebral trauma. J Pineal Res 2007;42:1–11.
6. Tyler et al. Treatment of post-traumatic headache with amitriptyline. Headache
1980;20:213–6.
7. Dinan TG, Mobayed M. Treatment resistance of depression after head injury:
8. a preliminary study of amitriptyline response. Acta Psychiatr Scand 1992;85:292–4.
9. Fann et al. Cognitive improvement with treatment of depression following mild
traumatic brain injury. Psychosomatics 2001;42:48–54.
10. Silver JM, McAllister TW, Arciniegas DB. Depression and cognitive complaints
following mild traumatic brain injury. Am J Psychiatry 2009;166:653–61.
11. Whyte et al. Effects of methylphenidate on attention deficits after traumatic brain injury:
a multidimensional, randomized, controlled trial. Am J Phys Med Rehabil 2004;83:401–
20.
12. Tsaousides T, Gordon WA. Cognitive rehabilitation following traumatic brain injury:
assessment to treatment. Mt Sinai J Med 2009;76:173–81.
13. Cicerone KD. Remediation of “working attention” in mild traumatic brain injury. Brain
Inj 2002;16:185–95.
14. Ho MR, Bennett TL. Efficacy of neuropsychological rehabilitation for mildmoderate
traumatic brain injury. Arch Clin Neuropsychol 1997;12:1–11.

Leddy and Willer. Use of graded exercise testing in concussion and return to activity management. Curr Sports Med
Reports. 2013;12(6):370-6.

Concussion Clinic Protocol • Preseason Preparation
• Concussion Recognition
• Initial Concussion Evaluation
• Initial Rest
• Monitor Symptoms
• +/- Neurocognitive testing
• +/- All sorts of rehabilitation techniques
• Graduated return to play

Graduated RTP 1. Complete physical and cognitive rest.
2. Aerobic exercise (e.g. walking, swimming, stationary bike,
etc.) First easy, then harder.
3. Sport-specific exercise (e.g. skating, running, etc.)
4. Non-contact training drills (e.g. passing drills in football or
hockey)
5. Full contact practice
6. Normal game play
McCrory P, et al. Consensus Statement on Concussion in Sport: the 4th International Conference on Concussion in Sport held in Zurich,
November 2012. Br J Sports Med 2013;47:250–258


OR, to frame as
covered, not-
covered

Covered
Things we all agree on
Things we kind of agree on
Areas of controversy / disagreement
Most common sideline tests
Guided discussion:
Sideline evaluation
Graduated RTP
Disqualification / retirement

Things we agree on
Concussions are probably bad.
Injured athletes should be removed from play
No same day RTP
Symptomatic athletes should not RTP
Graduated RTP
There is little to no role for protective equipment
If you are going to do testing, having a baseline
makes it more useful

Things we kind of agree on
All sideline concussion tests have significant limitations
Biomarkers, imaging and physiologic tests might be the
future, but aren’t ready for prime time
Sub-symptom aerobic exercise can safely be used when
the athlete is still symptomatic
Rest doesn’t really help that much.
Rules and legislation make a difference
No number of concussions threshold

Number of Concussions
Am
ount
of
Bad
nes
s

Things we disagree on / don’t know
cNCT
Role of sensors
Natural history
Risk stratification
Role of coincident mood disorder on persistent symptoms
Sport vs Blast vs MVA
Independent evaluators
Disqualification / retirement
Athletes who have ever had ICH