sports injuries: the role of imaging in diagnosis and ... · sports injury imaging page 4...
TRANSCRIPT

THE ESC NEWSLETTER
AUTUMN08
inside this issue:Page 2Sports injury imaging
Page 4Fundraising for Bowel Cancer UK
Page 6Statin therapy in diabetes
Page 8New photo competition - win a case of vintage Champagne
Sports Injuries: the Role of Imaging in Diagnosis and Treatment
continued on page 2
Injuries related to sport are an unfortunate complication of an active lifestyle. Such injuries may be acute – for instance, a sprained ankle ligament – or they may be chronic, such as shoulder impingement syndromes or tendinosis of the elbow. Whether suffered by a regular runner or an occasional skier, these injuries can impact significantly on an individual’s enjoyment of exercise.
Diagnostic imaging provides for accurate assessment of injuries, allows the clinician to make an informed evaluation of prognosis and may also be used
page 2
degeneration, are also sensitively demonstrated and multiplanar reformats and surface rendered images detect abnormal morphology, predisposing to conditions such as hip impingement.
What follows is a brief overview of examples of the enormous range of sports injuries, as demonstrated by diagnostic imaging.
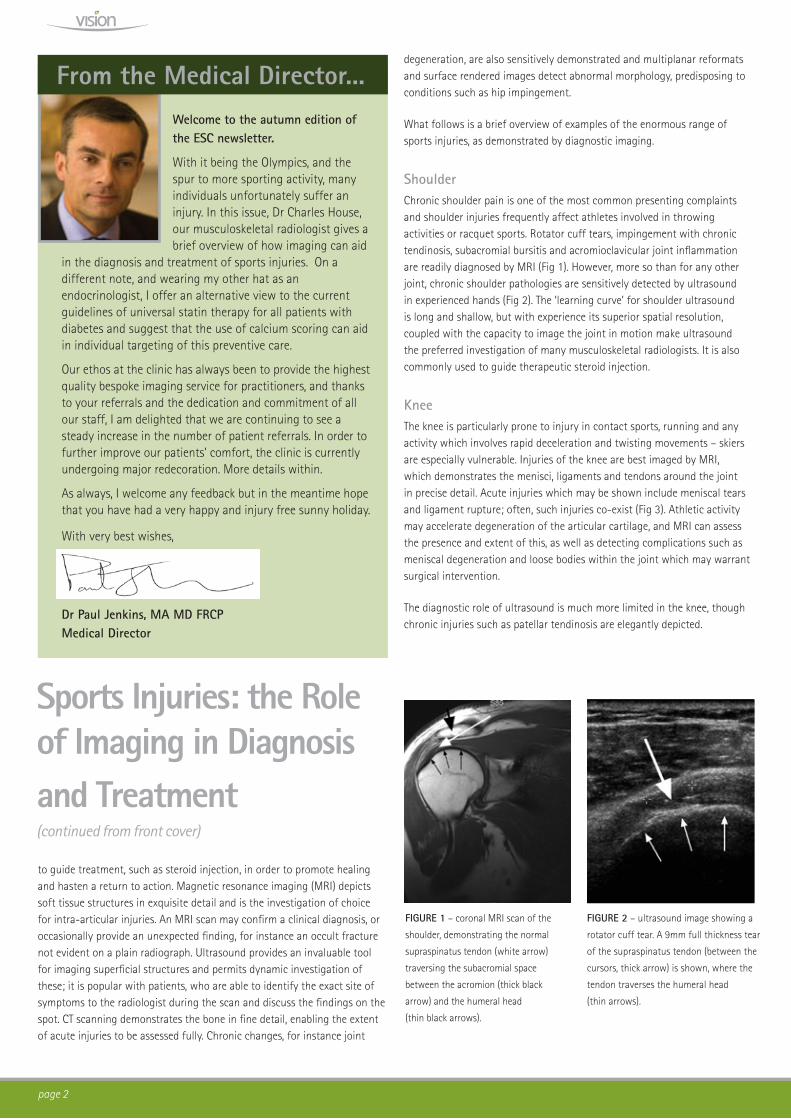
ShoulderChronic shoulder pain is one of the most common presenting complaints and shoulder injuries frequently affect athletes involved in throwing activities or racquet sports. Rotator cuff tears, impingement with chronic tendinosis, subacromial bursitis and acromioclavicular joint inflammation are readily diagnosed by MRI (Fig 1). However, more so than for any other joint, chronic shoulder pathologies are sensitively detected by ultrasound in experienced hands (Fig 2). The ‘learning curve’ for shoulder ultrasound is long and shallow, but with experience its superior spatial resolution, coupled with the capacity to image the joint in motion make ultrasound the preferred investigation of many musculoskeletal radiologists. It is also commonly used to guide therapeutic steroid injection.
KneeThe knee is particularly prone to injury in contact sports, running and any activity which involves rapid deceleration and twisting movements – skiers are especially vulnerable. Injuries of the knee are best imaged by MRI, which demonstrates the menisci, ligaments and tendons around the joint in precise detail. Acute injuries which may be shown include meniscal tears and ligament rupture; often, such injuries co-exist (Fig 3). Athletic activity may accelerate degeneration of the articular cartilage, and MRI can assess the presence and extent of this, as well as detecting complications such as meniscal degeneration and loose bodies within the joint which may warrant surgical intervention.
The diagnostic role of ultrasound is much more limited in the knee, though chronic injuries such as patellar tendinosis are elegantly depicted.
Sports Injuries: the Role of Imaging in Diagnosis and Treatment (continued from front cover)
to guide treatment, such as steroid injection, in order to promote healing and hasten a return to action. Magnetic resonance imaging (MRI) depicts soft tissue structures in exquisite detail and is the investigation of choice for intra-articular injuries. An MRI scan may confirm a clinical diagnosis, or occasionally provide an unexpected finding, for instance an occult fracture not evident on a plain radiograph. Ultrasound provides an invaluable tool for imaging superficial structures and permits dynamic investigation of these; it is popular with patients, who are able to identify the exact site of symptoms to the radiologist during the scan and discuss the findings on the spot. CT scanning demonstrates the bone in fine detail, enabling the extent of acute injuries to be assessed fully. Chronic changes, for instance joint
Welcome to the autumn edition of the ESC newsletter.
With it being the Olympics, and the spur to more sporting activity, many individuals unfortunately suffer an injury. In this issue, Dr Charles House, our musculoskeletal radiologist gives a brief overview of how imaging can aid
in the diagnosis and treatment of sports injuries. On a different note, and wearing my other hat as an endocrinologist, I offer an alternative view to the current guidelines of universal statin therapy for all patients with diabetes and suggest that the use of calcium scoring can aid in individual targeting of this preventive care.
Our ethos at the clinic has always been to provide the highest quality bespoke imaging service for practitioners, and thanks to your referrals and the dedication and commitment of all our staff, I am delighted that we are continuing to see a steady increase in the number of patient referrals. In order to further improve our patients’ comfort, the clinic is currently undergoing major redecoration. More details within.
As always, I welcome any feedback but in the meantime hope that you have had a very happy and injury free sunny holiday.
With very best wishes,
Dr Paul Jenkins, MA MD FRCPMedical Director
From the Medical Director...
FIGURE 1 – coronal MRI scan of the
shoulder, demonstrating the normal
supraspinatus tendon (white arrow)
traversing the subacromial space
between the acromion (thick black
arrow) and the humeral head
(thin black arrows).
FIGURE 2 – ultrasound image showing a
rotator cuff tear. A 9mm full thickness tear
of the supraspinatus tendon (between the
cursors, thick arrow) is shown, where the
tendon traverses the humeral head
(thin arrows).

page 3
Hip/PelvisHip pain in an older sportsman is often related to articular cartilage degeneration, and MRI can confirm this whilst also assessing damage to the acetabular cartilaginous labrum. Femoro-acetabular impingement is an increasingly recognised cause of labral injury in a younger age group and the bony abnormalities which pre-dispose to this are most accurately delineated by CT scanning (Fig 4). Inflammation of the tendon attachments around the hip and pelvis, including the hamstring origins and the gluteal muscle insertions, is a common cause of chronic symptoms, sensitively diagnosed by MRI and may be treated by ultrasound-guided injection (Fig 5).
Elbow and WristSporting injuries around the elbow are frequently related to the attachments of the common flexor tendon of the forearm or the common extensor tendon (‘tennis elbow’ or lateral epicondylitis). These injuries are often chronic and although self-limiting are slow to resolve and may respond well to the ultrasound-guided treatment of ‘dry-needling’, promoting scar formation in the tendon. Wrist pain is well-assessed with MRI, which may demonstrate ligament injury (including to the intracapsular scapholunate ligament), tears of the triangular fibrocartilage, tendonitis or occult fracture of the scaphoid (Fig 6). Ultrasound also clearly demonstrates inflammation around the tendon sheaths (teno-synovitis) or synovitis in the carpus and can accurately guide injection of steroid if appropriate in such cases.
Ankle and FootAcute injuries of the ankle often result from twisting mechanisms and involve ligament damage. Ligament sprains are sensitively demonstrated by MRI, which also detects synchronous bony bruising and other soft tissue injuries, for instance tendon tears. Both MRI and ultrasound may be of use in assessment of Achilles tendon injuries and will demonstrate chronic tendinosis as well as acute rupture (Fig 7). Other chronic conditions of the ankle joint include impingement syndromes, and joint degeneration, each of which may respond to guided steroid injection.
Pain in the forefoot in runners may relate to bony stress in the metatarsals or sesamoid bones, and these pathologies are best diagnosed by MRI. Inflamed bursae in the interspaces between the metatarsals must be distinguished from
neuromas of the digital nerves (Mortons neuroma) and ultrasound or MRI will allow this – ultrasound having the added advantage once again of enabling a targeted steroid injection once the diagnosis is confirmed.
SummaryDiagnostic imaging is an invaluable adjunct to clinical assessment in patients with sports-related injuries. MR imaging, ultrasound and CT imaging together provide the means to assess both soft tissue and bone injuries in exquisite detail. Whether in confirming the clinical diagnosis, fully characterising the extent of trauma or in uncovering an occult injury, imaging provides the next step in the return to sporting fitness.
Dr Charles House Consultant Musculoskeletal Radiologist UCLH NHS Trust
FIGURE 6 – the plain film appearances
were equivocal in this patient, but this
T1-weighted MR image of the wrist
clearly shows the fractured scaphoid
bone.
FIGURE 7 – axial plane contrast-
enhanced MR image in a patient with
chronic ankle pain shows a thickened and
partially torn tibialis posterior tendon
(arrow). Note the rim of enhancing
inflammation of the tendon sheath.
FIGURE 3 – coronal plane MRI image
diagnoses a tear of the medial meniscus
(long arrow), with a meniscal fragment
displaced within the joint (dotted arrow).
Note the normal lateral meniscus
(short arrow).
FIGURE 4 – surface rendered CT image shows in
3-dimensions the bony morphology in a case of anterior hip
impingement.
FIGURE 5 – MR scanning confirmed the clinical diagnosis of an
acute tear of the rectus femoris head of the right quadriceps
muscle in this young athlete.

page 4
In order to maintain our comfortable and relaxing ambience for our patients about to undergo a scan, the ESC centre is currently undergoing major redecoration. Interior designer Hugh Berry, whose team has worked on the transformation of many Harley Street properties and large London Hospitals sees great potential in our clinic.
“The many quirky Georgian features in this potentially beautiful building will be revealed and enhanced. This will be achieved through restoration of the original details, which will then be further improved with clever use of colour and design. The needs of a modern clinic can then sit harmoniously within this grand old building.”
We look forward to welcoming you and your patients to the new look centre when it is finished later this summer.
In recognition of Bowel Cancer Awareness month in April, the European Scanning Centre was pleased to work with the charity Bowel Cancer UK to promote the benefits of colorectal cancer screening. As well as offering a discount to patients undergoing a virtual colonoscopy during the promotion, the Centre pledged to donate a proportion of the scan costs to Bowel Cancer UK to help support the charity in its invaluable ongoing work in this area.
Ian Beaumont, Director of Communications was presented with a cheque during a recent visit to the Centre and said
‘Bowel Cancer UK is passionate about early colorectal cancer detection, because early detection saves lives. We are extremely grateful to companies who help patients get the early screening they need.‘During this promotion alone, 40% of patients screened were found to have polyps or cancerous tumours. An incidental finding of a 1.5cm gallstone accounted for another patient who came in for a scan suffering from extreme abdominal pain.
Centre refurbishment
Bowel Cancer UK
We are delighted to announce that Patricia, our
Head of Patient Services has had a baby girl,
Alicia. While Patricia is on maternity leave,
Nelia Cantinho is helping in the kitchen and will
continue to ensure our patients are well fed
and watered.
We also welcome Bezhad Mokri-Moayadd who
joins us as an Applications Specialist and
Radiographer. Bezhad has a tremendous
pedigree as not only is he a qualified
radiographer who will assist in our scanning,
but is also a professional sports man and is
currently studying for a PhD in medical research
at University of London, Birkbeck College.
Bezhad is looking forward to meeting many of
you over the coming months.
Staff newsRecent studies in molecular genetics have
begun to unravel the genetic causes of
coronary heart disease. However, such studies
have generally required large numbers of
patients to be sufficiently powered.
The use of calcium scores, a validated surrogate
end-point for CHD, will allow for fewer patients.
In collaboration with Professor Nilesh Samani, BHF
Chair of Cardiology at Leicester Medical School and
an international authority in CHD genetics, we have
recently initiated a pilot study into the association
between genetic polymorphisms and calcium scores,
with a view to applying for further funding from
research grant bodies to significantly expand on these
findings. The other collaborators in this exciting project
are cardiologists, Dr Laura Corr and Dr David Brull, and
Professor Stephen Bustin, Chair of Molecular Science at
Barts and The London Medical School.
Genetics of CHD
Nelia Cantinho
Bezhad Mokri-Moayadd
Inder Bull, Sales & Marketing Manager, ESC with Ian Beaumont, Director of Communications, Bowel Cancer UK

page 5
How long have you worked at the ESC?Lindsey
’’I have been with the Centre for just over three years. I work on reception two days a week’.
Emma
‘I have been here for about four years. I am the Centre’s receptionist for the other three days. When I am on reception, Lindsey works in the front office performing a variety of other admin tasks, including answering phones and booking appointments, and vice versa’.
Your role is a busy and diverse one. What happens in your typical working day?Lindsey
‘A typical day on reception will be busy from start to finish. We first check the diary on our patient record system and make sure we have all the referral forms and medical questionnaires before patients start arriving. We greet patients at reception, take them downstairs to the patient lounge and ensure they are offered a drink if they can have one. It is our job to inform the radiographers or radiologist that the patients are here and
to hand over all completed paperwork. Another part of our role is preparing the ultrasound room for the radiologists.’
Emma
‘We print out any medical questionnaires if patients have not remembered to bring them along to their appointment. We are also responsible for all the billing. We take payments from self-paying patients at reception after they have had their scan and had time to relax. We also call insurance companies to confirm cover for insured patients’.
Which other departments do you work closely with in the ESC and how important is it for you all to work as a team?Emma
‘As we are the middle person between the patient and the radiographer or on duty radiologist, we interact mostly with the imaging department. Our job is to ensure that everything runs smoothly. We need to know what patients are having done and where they are in the Centre at all times so we can keep everyone informed. Lindsey and I work extremely well together. We know when the other needs help so will jump in and lend a hand’.
Lindsey
‘We also work closely with the medical secretaries Julie, Maria and Suzanne as we can get doctors phoning in about their reports. It is very important to be a good team player and get to know each other’s personalities in order to communicate effectively.’
What challenges do you face?Lindsey
‘We are a very busy Centre and the phones are constantly ringing. In this job you need to be able to talk in detail about lots of different scans in order to explain what’s involved. You also need to find out as much information about the patient at the time of booking, particularly if they have any allergies or are asthmatic, as this is crucial for the scanning process. In the beginning, I found this a little challenging but once you’ve been here a while, it all becomes automatic.’
Emma
‘When it’s very busy and patients are coming and going all day it can be tricky to keep an eye on who is here. You also have to get so much done when dealing with large numbers of patients and in a such short space of time that you really do need to be organised. This job really keeps you on your toes!’
You are the front line and a patient’s first contact with the ESC – how important is it to make a good first impression?Emma
‘Very important! We plan ahead and ensure that we are at the reception desk for when a patient arrives. We prepare all the paperwork beforehand or will know if patients are bringing the questionnaires or referral forms with them. We ensure patients are offered a drink on arrival and that they are as comfortable as they can be while they are with us. We get everything ready for them in advance so that the process is as quick and as smooth as possible once they are here’.
Lindsey
‘Smile! We always say good morning or good afternoon and are courteous and professional. It’s very important to be at the reception desk when a patient arrives and not downstairs, for example, with another patient. As we are becoming steadily busier, Emma and I will both be sitting on the reception desk after the current centre refurbishment to help with this’.
How do you help reassure patients and keep them calm if they are feeling anxious about their scan?Emma
‘We try to reassure patients as much as possible and make them feel comfortable and not rushed. We always make sure they have had enough refreshments and feel okay before they leave the Centre’.
Lindsey
‘The caring side just comes out and you try to reassure them as much as possible. You get to know which patients want to talk and which want to be left alone to sit quietly or read. We always offer patients a drink providing they can have one and point out that our radiographers will be happy to answer any questions they may have about the scan’.
People like to see a familiar face/hear a familiar voice. Have you developed any good working relationships with referring doctors and/or their secretaries since you’ve been working here? Lindsey
‘‘I have developed professional relationships with numerous doctors and secretaries in the Harley Street area. I think it definitely helps for them to speak to someone they know and to hear a familiar voice. It builds up a level
of trust, as they can be confident they are speaking to someone who knows what they are doing and who will deliver what they promise’.
Emma
‘Yes, definitely! The benefit of working on Harley Street for so many years is that I already knew many of the local referring doctors and their secretaries before I started here. I definitely think it is a bonus that they can call up or drop in and speak to someone familiar. It gives us that personal touch’.
What do you enjoy the most about working at the ESC?Emma
‘That’s simple - the people! We are a small, friendly team and we all get on really well. Working on reception is also a great way to meet new people, which I enjoy.’
Lindsey
‘I like the buzz I get when the Centre is busy and I enjoy helping people. I also like working in a small team and we all get on so well. We have some great social events such as our recent Summer Sports Day, which was a really good laugh.’
What makes a good receptionist? What qualities do you need?Lindsey
‘You need to have a bright and cheerful nature and be used to dealing with many different people with different personalities and of different cultures and religions.’
Emma
‘You also need to be a friendly, calm and organised person who can work well under pressure.’
SPOTLIGHT...on our two Receptionists, Lindsey Davis and Emma Barry
Lindsey Davis
Emma Barry
Staff Sports Day

page 6
Patients with diabetes are at particular high risk of cardiovascular disease
(CVD) with a prevalence 2-3 fold that of the general population. Indeed
CVD accounts for the majority of deaths of these patients. The number of
people with diabetes in the UK is currently more than a million but with
the obesity epidemic is expected to increase to at least 3 million within
a few years and possibly up to 6 million, or 1 in 10 of the population.
Therefore, it is important to develop an effective strategy for prevention
of CVD in these patients.
Statin therapy in diabetes
In recent years ‘statins’ have been increasingly promoted in the fight
against CVD both in patients with and without diabetes and the
recommendations for their use have been ever broadening. The American
Heart Association (AHA) recommends that patients with diabetes belong
in the same high-risk category as patients with known CVD i.e. ‘coronary
heart disease equivalents’ and as such should be subject to the same
recommendations for lipid lowering therapy. The recent Joint British
Cardiac Societies’ guidelines for the prevention of CVD have echoed this
and state that patients with diabetes should be routinely considered for
statin treatment regardless of cholesterol levels. However, careful analysis
of the data from the relevant epidemiological trials suggests that such
a policy may not be appropriate for all diabetic patients encountered in
clinical practice and that a more focussed approach to statin prescribing
would be preferable. Importantly, in many studies the relative risk
reductions did not translate into similarly impressive reductions in absolute
risk (Table 1).
In the MRC/British Heart Foundation study, 5 years of statin administration
to diabetic patients, half of whom had previous CVD, resulted in a 1.5%
reduction in actual mortality. This equates to 1000 patients needing
treatment with a statin over a 5 year period to prevent 15 deaths, or just
over 3 per year. Beneficial results were also reported in the Collaborative
Atorvastatin Risk Reduction Study (CARDS). However, several studies have
failed to demonstrate any beneficial effects of statins in diabetic subjects.
In the Antihypertensive and Lipid Lowering Treatment to Prevent Heart
Attack Trial (ALLHAT), 40mg pravastatin was compared to usual care in
3638 subjects. Despite these subjects also being hypertensive and many
with a previous history of coronary or other occlusive arterial disease, there
was no significant reduction in coronary event rate. A similar lack of any
significant benefit was also reported in both the lipid lowering arm of the
Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT), despite all patients
being hypertensive and having at least one other cardiovascular risk factor,
and the recent Atorvastatin Study for Prevention of coronary heart disease
Endpoints in NIDDM (ASPEN) study.
Cost and compliance with statin therapy
In addition to questioning their universal efficacy, two other reasons
as to why adopting a scattergun approach to statin prescribing might
not be optimal for clinical practice are first, the cost implication of this
wholesale approach and second, and frequently ignored is the issue of
non-compliance. Many study authors forget that diabetes is largely an
asymptomatic condition and it is unrealistic to expect patients to adhere to
their prescriptions on an indefinite basis. Most are already required to take
a combination of tablets (often with every meal) for glycaemic control, in
addition to combinations of anti-hypertensive agents, and aspirin.
Is universal statin therapy in diabetes best practice?
Table 1: Absolute risk reductions in CVD mortality from the major large primary prevention trials of statins in patients with diabetes. MRC/BHF = Medical Research Council/ British Heart Foundation study; CARDS = Collaborative Atorvastatin Risk reduction in Diabetes Study; ASCOT = Anglo-Scandinavian Cardiac Outcomes Trial – Lipid Lowering Arm; ALLHAT = Antihypertensive and Lipid-Lowering treatment to prevent Heart Attack Trial; ASPEN = Atorvastatin Study for Prevention of coronary heart disease Endpoints in NIDDM. n.s. = non-significant
Study No. of subjects Statin dose Years of Follow Up Absolute risk reduction in CVD mortality, %, (p value)
MRC/BHF 5963 Simvastatin 40mg 5 1.5 (0.02) (2003)
CARDS 2838 Atorvastatin 10 mg 3.9 0.8 (0.06) (2003)
ASCOT 5032 Atorvastatin 10mg 3.3 0.55 (n.s.) (2002)
ALLHAT 3638 Pravastatin 40 mg 6 0.4 (n.s.) (2002)
ASPEN 2410 Atorvastatin 10mg 4.25 0.0 (n.s.) (2006)

page 7
Fig 1: Cox proportional hazards cumulative survival for 10,377 subjects with and without diabetes according to CAC scores: (a) non-diabetic subjects; (b) lower survival in diabetic subjects with equivalent CAC scores; (c) normal survival in diabetic subjects with zero CAC score. Adapted from Raggi et al 2004 J Am Coll Cardiol, 43(9), 1663-1669.
The addition of lifelong statin therapy with their frequent associated
adverse effects is unlikely to result in long-term compliance. The recent
studies reflected this with less than half of patients still taking the statin
treatment after 4 years.
EBCT Assessment of CVD Risk
Taking these factors into account, there is a need for better targeting
of statin treatment of diabetic patients, by accurately identifying those
with a high risk of future CVD. Electron beam CT (EBCT) scanning for
coronary artery calcification (CAC) can fulfil these requirements. EBCT is
fundamentally different to conventional CT scanners in that the x-rays
are generated by a beam of electrons deflected onto fixed tungsten target
rings, rather than an x-ray emitting rotating gantry. This enables the
images to be obtained 5-10 times faster, which allows for more accurate
imaging of the moving heart. This superior speed also results in a very
significantly reduced radiation dose, an important consideration when
scanning asymptomatic individuals. EBCT scanning is extremely sensitive in
detecting calcium, and as deposition of coronary artery calcium only occurs
in atherosclerotic arteries, with its extent correlating strongly with the
severity of disease, quantification of CAC allows an accurate assessment
to be made of an individual’s CVD risk. The power and clinical utility of
calcium scoring is that it reflects the overall impact of all risk factors, both
known and unknown, on the end organ, the arterial wall.
Long-term large follow-up studies of asymptomatic individuals have
demonstrated that a high calcium score is associated with up to a 40-fold
increased risk of future coronary events, while conversely the American
Heart Association states that a zero calcium score is associated with a
0.05% chance of an event. This risk stratification has also been confirmed
in numerous studies of patients with diabetes and allows them to be
classified into two groups (Fig 1). First, those with a significant CAC score
have a worse prognosis than non-diabetic subjects with equivalent calcium
scores, and thus require more aggressive preventive therapy. However,
conversely approximately 30-50% of diabetic patients have no CAC
deposition and have been shown to have the same survival outcome as
non-diabetic subjects i.e. an extremely low CVD risk. Given this, it would
seem logical to conclude that these patients do not require routine primary
preventive statin therapy.
Conclusions
There is now compelling evidence to support EBCT coronary artery calcium
measurement as an effective means of screening diabetic individuals for
CVD. A high score indicates significant atheromatous disease and thus the
need for aggressive treatment with a statin that may arrest or even reverse
disease progression. Conversely, a zero or low score indicates none or
minimal coronary atheroma and thus no need for preventive medication or
further testing.
Dr Paul Jenkins MD FRCP
Reader in Endocrinology, Barts and The London School of Medicine
Medical Director, The European Scanning Centre
(a)
(b)
(c)No diabetes and diabetes with zero CAC score
Diabetes (n=903)
No Diabetes (n=9,474)
Follow-up (Years)
Follow-up (Years)
Follow-up (Years)
1.00
.98
.96
.94
.92
.90
.88
.86
.84
.82
.80
1.000
.990
.980
.970
.960
.950
.940
.930
.920
.910
.900
1.00
.98
.96
.94
.92
.90
.88
.86
.84
.82
.80
Cu
mu
lati
ve S
urv
ival
Cu
mu
lati
ve S
urv
ival
Cu
mu
lati
ve S
urv
ival
0 1 2 3 4 5
0 1 2 3 4 5
0 1 2 3 4 5
0 - 10 (n=351)
No diabetes (n=4,800)
x2=0.5, p=0.49
Diabetes (n=267)
0 - 10 (n=5,600)
11 - 100 (n=189)
11 - 100 (n=1,854)
101 - 400 (n=182)
101 - 400 (n=1,251)
401 - 1000 (n=110)
401 - 1000 (n=508)
>1000 (n=71)
>1000 (n=261)

page 8
Best CaptionCan you think of a caption for the photo below?It’s just a bit of fun! Entries will be judged on their humour and originality. Please only one entry per person.
Come up with the winning caption and you will win 6 bottles of vintage champagne.
Entries to be submitted by 1st December 2008 via email to: [email protected]
A 49 year old man attended his GP with an
18 month history of intermittent blood in
his stools. He was referred locally to a
surgeon who performed a sigmoidoscopy.
This revealed mild diverticular disease. There
was no family history of colorectal cancer.
The surgeon recommended a colonoscopy
but the patient wished for a non-invasive
virtual CT colonoscopy. This demonstrated a
single 1.5 x 2 cm enhancing pedunculated
polyp within the mid-sigmoid colon with a
long enhancing stalk (Fig 1a and 1b). The
patient was subsequently referred for
conventional colonoscopic excision.
Histology revealed it to be a mildly dysplastic
tubular adenoma with complete excision.
Dr Peter Fairclough, Consultant Gastroenterologist, comments: Any person with unexplained rectal bleeding should be carefully examined and I congratulate this man on persisting until the cause was found and treated. It is not clear why the polyp was not seen on the first examination as it was only at 40cm from the anus. With modern equipment and good endoscopic skills, most patients can have visual colonoscopy comfortably without sedation if they wish, and with almost no risk. Removing polyps at colonoscopy is painless; indeed there is no sensation of the polypectomy. However, as with virtual colonoscopy, it is crucial to select the operator carefully.
Electron Beam Computed Tomography (EBCT)
Abdominal & Pelvic Scan
Angiography (carotid artery, coronary and
peripheral)
Bone Mineral Density
Brain
Heart Scan (coronary artery calcium)
Lung Scan
Renal Tract
Sinuses
Virtual Colonoscopy
UltrasoundAbdominal Aorta
Abdomen & Pelvis
Carotid Doppler
Echocardiography
FNA Thyroid
Gallbladder (static and dynamic)
Leg Veins
Prostate (trans-abdominal)
Prostate (trans-rectal)
Renal Tract
Testes
Thyroid Gland
X-rayWe offer a complete
X-ray service
MRIBrain
Carotid Arteries
Elbows
Feet
Fingers
Musculo-skeletal
Neck
Shoulder
Spine
European Scanning Centre68 Harley StreetLondon W1G 7HE
Tel: 020 7436 5755Fax: 020 7436 5756
www.europeanscanning.com
European Scanning Centre
Scans
Answer to Ross’s Riddle 3A surgeon returned from work every day by train, arriving at the station at exactly 7.30 pm. His wife drove to meet him at the station and she took him home in the car. She always drove at a steady 20mph and they always arrived home at the same time each day. One day he caught an earlier train but did not get a chance to tell his wife, so he started to walk home at a steady 3 mph. His wife set out at her usual time and saw him as she was driving to the station. She picked him up and returned home. They reached home 20 minutes earlier than normal. At what time did she pick him up? They met at 7.20 p.m. In this puzzle, the distances and speeds are irrelevant. The important thing is that the car travels at a steady speed. It takes 20 minutes less time than it normally would. This must mean that the journey was shorter by 10 minutes each way, so they met 10 minutes earlier than usual.
The first correct answer drawn out of the hat was that from Mr Michael Falter, a patient at the ESC.
Many congratulations from everyone at the ESC to our lucky winner!
Fig 1a
Fig 1b
Case Study: A polyp too far?