središnja medicinska knjižnica - connecting repositoriescore.ac.uk/download/pdf/11699751.pdf ·...
TRANSCRIPT

1
Središnja medicinska knjižnica
Čuković-Bagić I., Macan D., Dumančić J., Manojlović S., Hat J. (2010) Dilated
odontome in the mandibular third molar region. Oral Surgery, Oral Medicine,
Oral Pathology, Oral Radiology, and Endodontics, 109 (2). pp. e109-13. ISSN
1079-2104
http://www.elsevier.com/locate/issn/10792104
http://www.sciencedirect.com/science/journal/10792104
http://dx.doi.org/10.1016/j.tripleo.2009.10.003
http://medlib.mef.hr/712
University of Zagreb Medical School Repository
http://medlib.mef.hr/
2
Dilated odontome in the mandibular third molar region
Ivana Čuković-Bagić, DMD, PhD,a Darko Macan, DMD, DDS, PhD,b Jelena Dumančić, DMD,
PhD,c Spomenka Manojlović, MD, PhD,d and Josip Hat, MD, MSce
a Professor, Department of Paediatric and Preventive Dentistry, School of Dental Medicine,
University of Zagreb, Croatia
b Professor, Head, Department of Oral Surgery, School of Dental Medicine, University of
Zagreb, Department of Oral and Maxillofacial Surgery, University Hospital Dubrava, Zagreb,
Croatia
c Teaching Assistent, Department of Dental Anthropology, School of Dental Medicine,
University of Zagreb, Croatia
d Professor, Department of Pathology, University Hospital Dubrava, School of Medicine,
University of Zagreb, Croatia
e Attending Radiologist, Department of Radiology, University Hospital „Sisters of Mercy“,
Zagreb, Croatia
Corresponding Author: Darko Macan, University Hospital Dubrava, Av. G. Suska 6, 10000
Zagreb, Croatia. Tel: +385914664075, Fax: +3852864250, E-mail: [email protected]

3
ABSTRACT
The dilated odontome is the most severe form of the dens invaginatus (dens in dente),
which is extremely rare in the mandible, especially in the molar region. We report a 28-year-old
female with an odd appearance of the mandibular third right molar on panoramic X-ray. CT scan
findings were suggestive that the intraosseous circular radiopaque formation was a dilated
odontome. The alveotomy of the “tooth” was performed, and histopathological analysis of the
inner and surrounding soft tissue revealed a diagnosis consistent with a dilated odontome. To the
best of our knowledge, this paper for the first time presents a CT scan of a dilated odontome.
INTRODUCTION
Dens invaginatus (dens in dente, “tooth within a tooth”, dilated odontome) is the tooth
anomaly that results from an infolding of the outer surface into the interior of a tooth. It most
frequently affects the permanent maxillary lateral incisors, followed by the maxillary central
incisors, premolars and canines, and less often the posterior teeth. It is rare in the mandible,
especially in the molars, and occurs symmetrically in about half of the cases.1 The most
commonly-used classification is that proposed by Oehlers2, who described the anomaly as
occurring in three forms. In Type 1, which is a minor form, the enamel-lined invagination is
confined within the crown of the tooth, not extending beyond the amelocemental junction. In
Type 2, the enamel-lined invagination extends apically beyond the cementoenamel junction, but
remains within the root. In Type 3, the enamel-lined invagination extends apically beyond the
cementoenamel junction and perforates apically to create an apical or periodontal foramen. In the
most severe form, named dilated odontome, the tooth has a circular or oval shape with a
radiolucent interior and presents a single structure, often with a central soft tissue mass.3,4 A

4
case of a dilated composite odontome in the maxilla was reported at the F.D.I. meeting in Paris
in 1931.5 Rushton6 used the term “dilated composite odontoma” and proposed that what
differentiates dens invaginatus from the former is the time when the disturbance occurs. Dens
invaginatus occurs later in odontogenesis and thus forms a recognizable tooth. Thoma and
Goldman7 in 1946 formulated that in dilated odontomes the crown or root part of the tooth shows
marked enlargement.
We report a 28-year-old female with a dilated odontome originating in the right third
molar region of the mandible, discovered incidentally on a routine panoramic radiograph.
CASE REPORT
A 28-year-old female had an excision of Naevus verrucosus dorsi at the Department of
Plastic, Reconstructive and Aesthetic Surgery. Her past medical history included a tonsillectomy
at 8 years of age but was otherwise unremarkable. The patient complained to the plastic surgeon
of discomfort and crowding of the mandibular anterior teeth, so he referred her to our
Department of Oral and Maxillofacial Surgery for evaluation of the development of the
mandibular third molar.
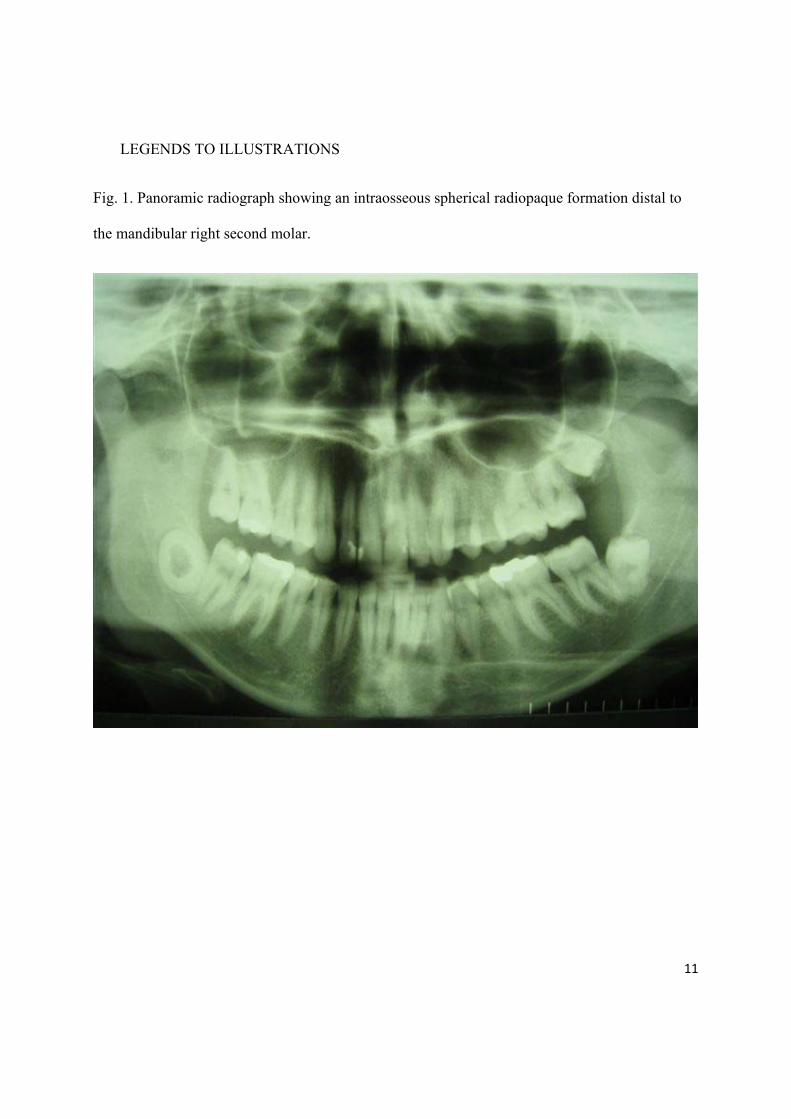
A panoramic radiograph showed an agenesis of the right third molar and a retained left
third molar in the maxilla with an impacted left third molar in the mandible. In the region distal
to the mandibular right second molar, an intraosseous spherical radiopaque formation with a
radiolucent interior was observed.
Because the radiopaque formation did not resemble the regular appearance of a molar, the
patient was referred for a micro-slice computerized tomography (MSCT)scan in order to exclude

5
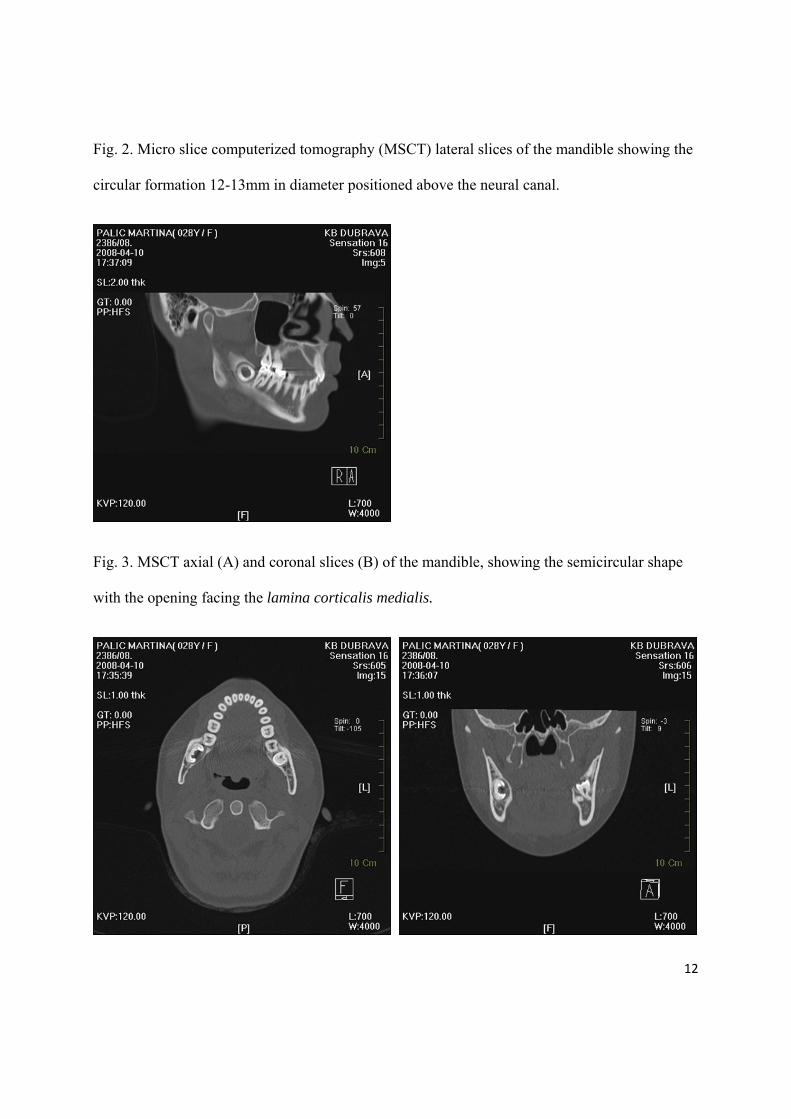
an odontogenic tumor. The MSCT lateral slice of the mandible showed a circular formation of
12-13 mm in diameter positioned above the neural canal.
In the horizontal and frontal projections, the formation was of semicircular shape, with
the opening facing the lamina corticalis medialis of the mandible.
In these projections the enamel was easily distinguished, as it was covering the inner
portion of the formation, while the outer portion was of dentine density with a very thin laminar
radiolucent area, which was presumably pulp space. The surrounding bone was of normal
structure, and there was neither a perforation of the lamina corticalis nor one of the neural canal.
This formation was presumed to represent the dilated odontome.
Under general anesthesia, a mucoperiosteal flap was raised posterior to the mandibular
second molar. The buccal cortical plate was removed, exposing the ovoid mass, which was
removed. The surgical flap was repositioned and sutured. Healing was uneventful.
Macroscopically, the extirpated formation was a spherical flattened tooth, 17.2 mm in
diameter with the diminutive crown (max. height 4.2 mm). Figure 5 shows deep central
invagination of the occlusal surface, delineated with irregular pitted enamel. The invagination
extended beyond the cementoenamel junction, corresponding to the Type II of dens invaginatus
according to the Oehlers2 classification. It occupied the center of the expanded short root (max.
length 4.9 mm). A part of the radicular portion was slightly damaged during the operation,
revealing a thin, compressed pulp space between the inner and outer dentinal wall.
Two specimens of soft tissue surrounding the anomalous tooth were sent for
histopathological examination. The soft tissue surrounding the impacted tooth-like mass was

6
composed of loose connective tissue containing capillaries and few islands of regular
odontogenic epithelium, consistent with a dental follicle. The tiny fragments taken from the
occlusal lining of the mass were composed of amorphous, partly calcified eosinophilic material.
The diagnosis was consistent with a dilated odontome.
DISCUSSION
Dilated odontoma originates during the morphodifferentiation stage of dental
development, but its exact etiology and genesis are unknown. Proposed theories include focal
growth retardation, focal growth stimulation, and localized external pressure in certain areas of
the tooth bud.8
Most cases of dens invaginatus are usually diagnosed incidentally on routine radiographs.
A radiological study by Thomas9 has revealed an incidence of 7.74%. Another radiographic
study reported that the incidence in maxillary lateral incisors, the most frequently-affected teeth,
is 9.66%.10 Some cases at the mandibular arch have also been reported, where the affected teeth
were predominantly premolars.11-13 Hamasha and Alomari14 investigated the prevalence of dens
invaginatus in Jordanian adults, and that study revealed no cases in the mandibular arch.
Our case, as far as we know, is the only one presented by MEDLINE search of the last
ten years where the most severe form of dens invaginatus, named a dilated odontome,
unilaterally affects a mandibular third molar. The molar region is an unusual location for dens
invaginatus, though it is a typical location for odontogenic tumors. The differential diagnosis
regarding an unusual appearance and localization of the radiopacity in our case included
odontoma, cemento-ossifying fibroma, osteoma, and osteoblastoma/osteoid osteoma.15 Complex
odontomas present as amorphous conglomerations of dentin and enamel and are more common

7
in the posterior mandible, presenting as a well-defined radiopacity surrounded by a radiolucent
rim. Compound odontomas present multiple rudimentary tooth-like structures and are more
common in the anterior maxilla. Both are often associated with an unerupted tooth. The shape is
usually irregular, but the dilated varieties are often well-defined, corticated, round or oval masses
with radiolucent centers.4 As in our case, Yamamoto et al.16 also found small root formation.
Surgical curettage or enucleation is recommended. Cemento-ossifying fibroma is a benign bone
neoplasm more frequently found in the posterior mandible. Its radiographic appearance varies
from a unilocular radiolucency to a radiopaque mass surrounded by a well-defined radiolucent
rim. Surgical curettage or enucleation is recommended.17
The osteoma is also a benign bone neoplasm, but it is more frequently found in the
mandibular body and the condyle. The endosteal type presents as a small, asymptomatic
radiopacity with no radiolucent rim. The peripheral type of osteoid osteoma presents as a
radiopacity without a radiolucent rim, and is not associated with root resorption. Superimposition
of an osteoma over the tooth roots is a common radiological finding. The osteoblastoma/osteoid
osteoma is a larger benign bone neoplasm that typically involves the posterior mandible. Its
excision or curettage is recommended.
Teeth with invaginations are prone to caries, pulp infection, and periapical pathosis if
present in the oral cavity.18-21 In our case, the unerupted dilated odontome was related to
crowding of the mandibular frontal teeth.
In case of erupted teeth, various treatment strategies could include preventive and
restorative treatment, but in teeth with severe anatomical irregularities, an alveotomy is the only
solution.

8
REFERENCES
1. White SC, Pharoah MJ. Oral Radiology: Principles and Interpretation, 5th ed. St. Louis:
Mosby; 2004.
2. Oehlers FAC. Dens invaginatus (Dilated composite odontome). I. Variations of the
invagination process and associated anterior crown forms. Oral Surg Oral Med Oral
Pathol 1957;10:1204-18.
3. Oehlers FAC. Dens invaginatus (Dilated composite odontome).II. Associated Posterior
Crown Forms and Pathogenesis. Oral Surg Oral Med Oral Pathol 1957;10:1302-16.
4. Pharoah M. Dental Imaging. http://imaging.consult.com/chapter/S1933-0332(07)76002-
0)
5. Anonymus. Dilated composite odontome. Proc R Soc Med 1937;30:1250.
6. Rushton MA. A collection of dilated composite odontomes. Br Dent J 1937;63:65-86.
7. Thoma KM, Goldman HM. Oral Pathology, 5th ed. St. Louis: C.V. Mosby; 1960, p. 1221-
2.
8. Tsurumachi T, Hayashi M, Takeichi O. Non-surgical root canal treatment of dens
invaginatus type 2 in a maxillary lateral incisor. Int Endod J 2002;35:310-4.
9. Thomas JG. A study of dens in dente. Oral Surg Oral Med Oral Pathol 1974;38:653-5.
10. Gotoh T, Kawahara K, Imai K, Kishi K, Fujiki Y. Clinical and radiographic study of
dents invaginatus. Oral Surg Oral Med Oral Pathol 1979;48:88-91.
9
11. Conklin WW. Bilateral dens invaginatus in the mandibular incisor region. Oral Surg Oral
Med Oral Pathol 1978;45:905-8.
12. El Deeb ME. Nonsurgical endodontic therapy of a dens invaginatus. J Endodont
1984;10:107-9.
13. Banner H. Bilateral dens in dente in mandibular premolars. Oral Surg Oral Med Oral
Pathol 1978;45:827-8.
14. Hamasha AA, Alomari QD. Prevalence of dens invaginatus in Jordanian adults. Int
Endodont J 2004;37:307-10.
15. Stavrou E, Tosios KI, Stavrou IE. Globular radiopacity around the apex of an impacted
maxillary third molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;103:594-
8.
16. Yamamoto K, Morimoto Y, Kawakami T, Shiotani H, Sugimura M. A case of dilated
odontoma arising in buccal region of 3rd molar tooth of mandible. Journal of the Japanese
Stomatological Society 1999;48:395-9.
17. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology, 2nd
ed. Philadelphia: Saunders; 2002, p. 553-71.
18. Murphy JB, Doku HC. Dens in dente: An unusual sequela. Abbreviated case report. Oral
Surg Oral Med Oral Pathol 1977;43:530-1.
19. Samimy B. Dens invaginatus: A potential hazard to the pulp. Quintessence Int
1977;11:91-2.

10
20. Taylor GN, Ill M, McDaniel R. Extraradicular communicating dens invaginatus. Oral
Surg 1977;44:931-7.
21. Šutalo J, Knežević A, Negovetić-Mandić V. Endodontic treatment of dens invaginatus-
case report. Acta Stomatol Croat 2004;38:215-8.
11
LEGENDS TO ILLUSTRATIONS
Fig. 1. Panoramic radiograph showing an intraosseous spherical radiopaque formation distal to
the mandibular right second molar.
12
Fig. 2. Micro slice computerized tomography (MSCT) lateral slices of the mandible showing the
circular formation 12-13mm in diameter positioned above the neural canal.
Fig. 3. MSCT axial (A) and coronal slices (B) of the mandible, showing the semicircular shape
with the opening facing the lamina corticalis medialis.

13
Fig. 4. Occlusal (A) and lateral (B) view of the extirpated spherical flattened tooth.

14
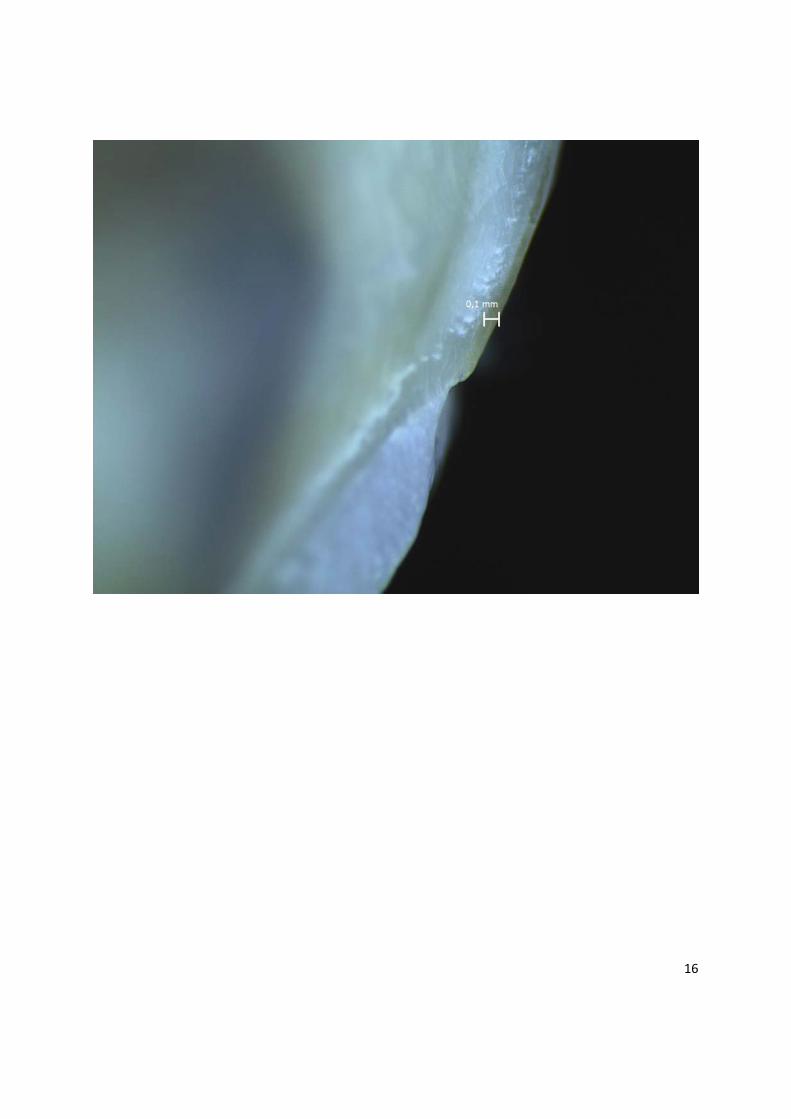
Fig. 5. Stereomicroscopic examination of the tooth. Central invagination of the occlusal surface
delineated with irregular pitted enamel (A). Compressed pulp space between the inner and outer
dentinal wall (B). Cementoenamel junction (C) with the invagination extending beyond it (D).

15
16

17

18
Fig. 6. The soft tissue surrounding the "impacted tooth-like mass" was composed of loose
connective tissue containing capillaries and few islands of regular odontogenic epithelium,
consistent with a dental follicle (hematoxylin and eosin stain, original magnification x 40).
19
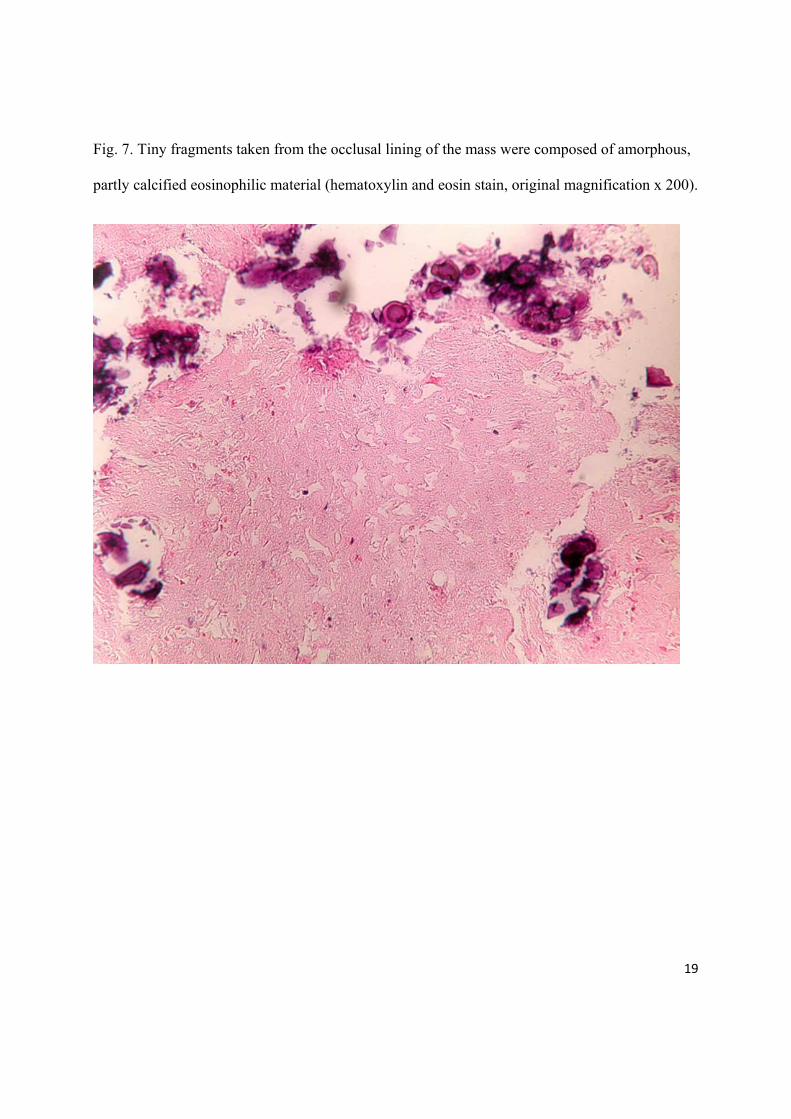
Fig. 7. Tiny fragments taken from the occlusal lining of the mass were composed of amorphous,
partly calcified eosinophilic material (hematoxylin and eosin stain, original magnification x 200).