srmc 2017 employee benefit guide - sampsonrmc.org · short-term disability ... the benefits...
TRANSCRIPT

Investment Group strategic planning & marketing services
Providing you with the very best in care
2017 Employee Benefit Guide
2
Sampson Regional Medical Center (SRMC) is proud to offer our employees a full range of benefit plans from which to choose. This guide is designed to provide you with an overview of the benefits available to you and your family. We encourage you to use this guide when planning your Open Enrollment benefit elections. As a Sampson Regional Medical Center (SRMC) employee you will have the opportunity to participate in a variety of available insurance plans, including: Medical Insurance
Dental Insurance
Vision Insurance
Basic Life/Accidental Death & Dismemberment (AD&D)
Voluntary Life/Accidental Death & Dismemberment (AD&D)
Short-term Disability
Long-term Disability
Employee Assistance Program (EAP)
Flexible Spending Account (FSA)
Universal Life and Accidental Death & Dismemberment (AD&D)
Accident Insurance
Critical Illness
What’s new for 2017:
We will be changing our medical carrier from BCBSNC to UMR (United Healthcare TPA) You will be required to me with an enrollment counselor in order to make your 2017
benefit elections.
3
Who is Eligible... If you are a Sampson Regional Medical Center full-time employee (working on average 30 or more hours per week) you and your dependents are eligible to enroll in the benefits described in this guide.
How to Enroll...
The first step is to review this benefit guide. You are required to make an appointment with an onsite enrollment counselor to complete your elections. You will be
responsible for notifying the counselor on whether you and/or your spouse are participating in the wellness program as well as attest to being a tobacco or non- tobacco user. Employees wishing to cover their eligible spouses will need to complete the “Spousal Eligibility” form, as well as enroll them for the 2017 plan year.
After your meeting, you can log in to HR In-touch (www.SRMC.HRintouch.com) to view your elections and print a confirmation statement. You are required to complete enrollment for all benefits. Employees must only enroll legal dependents. Proof of dependency may be required.
When to Enroll... Open enrollment for your 2017 benefits will be Tuesday, November 15th through Tuesday, November 22nd. The benefits you elect during open enrollment will be effective from January 1, 2017 through December 31, 2017.
Open Enrollment Reminder... This is an important time of year to add, delete or make changes to your current benefit elections. Unless you have a qualified change in status, you cannot make changes to your current benefits until the next open enrollment period. Qualified changes in status include: marriage divorce legal separation birth or adoption of a child change in child’s dependent status death of spouse, child or other qualified dependent change in residence due to an employment transfer for you or your spouse commencement or termination of adoption proceedings change in spouse’s benefits or employment status. You have 30 days from your qualifying event date to contact your Human Resources Department and make updates to your current benefit elections. Your Human Resources Department will need to verify the qualifying event and update your benefits accordingly.
4
MEDICAL INSURANCEMEDICAL INSURANCE
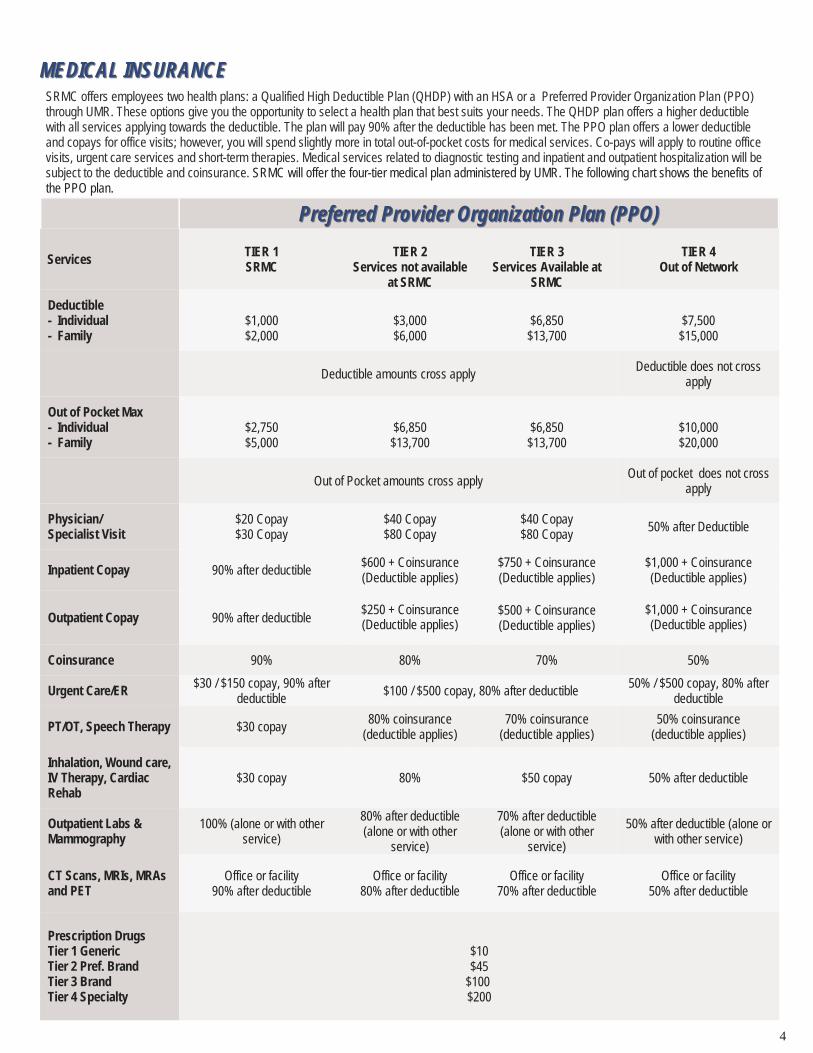
Preferred Provider Organization Plan (PPO)Preferred Provider Organization Plan (PPO)
Services TIER 1 SRMC
TIER 2
Services not available at SRMC
TIER 3
Services Available at SRMC
TIER 4 Out of Network
Deductible - Individual - Family
$1,000 $2,000
$3,000 $6,000
$6,850 $13,700
$7,500 $15,000
Deductible amounts cross apply Deductible does not cross
apply
Out of Pocket Max - Individual - Family
$2,750 $5,000
$6,850 $13,700
$6,850 $13,700
$10,000 $20,000
Out of pocket does not cross apply
Physician/ Specialist Visit
$20 Copay $30 Copay
$40 Copay $80 Copay
$40 Copay $80 Copay 50% after Deductible
Inpatient Copay 90% after deductible $600 + Coinsurance (Deductible applies)
$750 + Coinsurance (Deductible applies)
$1,000 + Coinsurance (Deductible applies)
Outpatient Copay 90% after deductible $250 + Coinsurance (Deductible applies)
$500 + Coinsurance (Deductible applies)
$1,000 + Coinsurance (Deductible applies)
Coinsurance 90% 80% 70% 50%
Urgent Care/ER $30 / $150 copay, 90% after deductible
$100 / $500 copay, 80% after deductible 50% / $500 copay, 80% after
deductible
PT/OT, Speech Therapy $30 copay 80% coinsurance
(deductible applies) 70% coinsurance
(deductible applies) 50% coinsurance
(deductible applies)
Inhalation, Wound care, IV Therapy, Cardiac Rehab
$30 copay 80% $50 copay 50% after deductible
Outpatient Labs & Mammography
100% (alone or with other service)
80% after deductible (alone or with other
service)
70% after deductible (alone or with other
service)
50% after deductible (alone or with other service)
CT Scans, MRIs, MRAs and PET
Office or facility 90% after deductible
Office or facility 80% after deductible
Office or facility 70% after deductible
Office or facility 50% after deductible
Prescription Drugs Tier 1 Generic Tier 2 Pref. Brand Tier 3 Brand Tier 4 Specialty
$10 $45
$100 $200
Out of Pocket amounts cross apply
SRMC offers employees two health plans: a Qualified High Deductible Plan (QHDP) with an HSA or a Preferred Provider Organization Plan (PPO) through UMR. These options give you the opportunity to select a health plan that best suits your needs. The QHDP plan offers a higher deductible with all services applying towards the deductible. The plan will pay 90% after the deductible has been met. The PPO plan offers a lower deductible and copays for office visits; however, you will spend slightly more in total out-of-pocket costs for medical services. Co-pays will apply to routine office visits, urgent care services and short-term therapies. Medical services related to diagnostic testing and inpatient and outpatient hospitalization will be subject to the deductible and coinsurance. SRMC will offer the four-tier medical plan administered by UMR. The following chart shows the benefits of the PPO plan.
5
MEDICALMEDICAL INSURANCEINSURANCE
Services TIER 1 SRMC
TIER 2
Services not available at SRMC
TIER 3
Services Available at SRMC
TIER 4 Out of Network
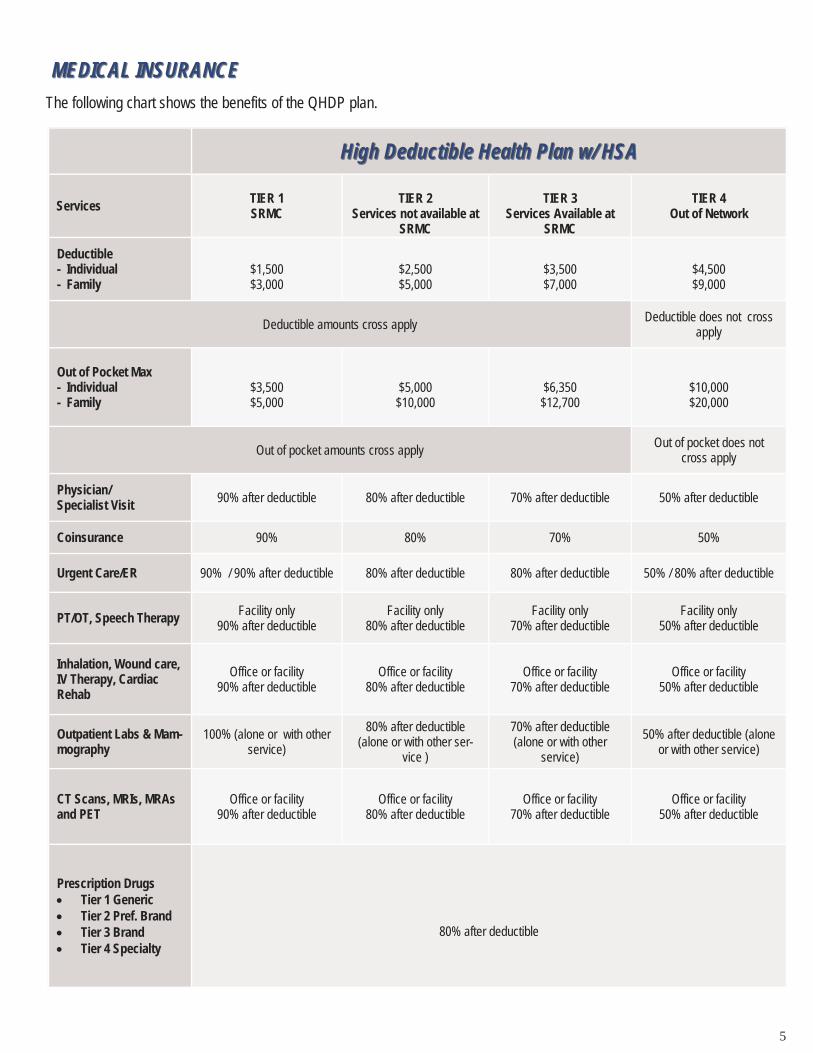
Deductible - Individual - Family
$1,500 $3,000
$2,500 $5,000
$3,500 $7,000
$4,500 $9,000
Deductible amounts cross apply Deductible does not cross
apply
Out of Pocket Max - Individual - Family
$3,500 $5,000
$5,000 $10,000
$6,350 $12,700
$10,000 $20,000
Out of pocket amounts cross apply Out of pocket does not
cross apply
Physician/ Specialist Visit 90% after deductible 80% after deductible 70% after deductible 50% after deductible
Coinsurance 90% 80% 70% 50%
Urgent Care/ER 90% / 90% after deductible 80% after deductible 80% after deductible 50% / 80% after deductible
PT/OT, Speech Therapy Facility only 90% after deductible
Facility only 80% after deductible
Facility only 70% after deductible
Facility only 50% after deductible
Inhalation, Wound care, IV Therapy, Cardiac Rehab
Office or facility 90% after deductible
Office or facility 80% after deductible
Office or facility 70% after deductible
Office or facility 50% after deductible
Outpatient Labs & Mam-mography
100% (alone or with other service)
80% after deductible (alone or with other ser-
vice )
70% after deductible (alone or with other
service)
50% after deductible (alone or with other service)
CT Scans, MRIs, MRAs and PET
Office or facility 90% after deductible
Office or facility 80% after deductible
Office or facility 70% after deductible
Office or facility 50% after deductible
Prescription Drugs Tier 1 Generic Tier 2 Pref. Brand Tier 3 Brand Tier 4 Specialty
80% after deductible
High Deductible Health Plan w/ HSA High Deductible Health Plan w/ HSA
The following chart shows the benefits of the QHDP plan.
6
Below are the 2017 monthly employer rates and the bi-weekly employee contribution amounts. These rates are based on you and your spouse both participating in the wellness program and you and your spouse both attesting to being a non-tobacco user.
QHDHP Plan PPO Plan
Tier SRMC Pays Monthly Employee Pays Bi-weekly
Tier SRMC Pays Monthly Employee Pays Bi-weekly
EE $544.45 $0.00 EE $577.75 $30.00
ES $603.77 $130.00 ES $696.75 $200.00
EC $478.03 $110.00 EC $611.37 $180.00
EF $762.87 $210.00 EF $869.08 $300.00
In the event you do not participate in the wellness program, your bi-weekly contribution will increase by $20. If you are enrolling your spouse in the medical plan, and he/she does not participate in the wellness program, your bi-weekly contributions will increase by another $20. If you are a tobacco user, your bi-weekly contribution will also increase by $20. And if enrolling your spouse in the medical plan and they are a tobacco user, your bi-weekly contribution will increase an additional $20. Below are a few examples:
Example 1:
Tom is enrolling as Employee Only in the HDHP. He is not a wellness participant and is not a tobacco user. His bi-weekly contribution would be $20.
Example 2:
Betty is enrolling as Employee + Spouse in the PPO plan. She is a wellness participant, but her husband is not. Betty and her spouse are both non-tobacco users. Her bi-weekly contribution would be $220.
Example 3:
Martha is enrolling as a Family in the HDHP. She is not a wellness participant, and her husband is not a wellness participant. Martha and her spouse are both tobacco users. Her bi-weekly contribution would be $290
Example 4:
Kyle is enrolling as a Employee + Child in the PPO. He is not a wellness participant, and is a tobacco users. His bi-weekly contribution would be $220.
Formula to help calculate your medical cost:
Base Rate: $ determined above
Employee is a Wellness Participant: add $0
Spouse is a Wellness Participant: add $0 Employee is not a Wellness Participant: add $20
Spouse is not a Wellness Participant: add $20
Employee is a Non-Tobacco User: add $0
Spouse is a Non-Tobacco User: add $0
Employee is a Tobacco User: add $20
Spouse is a Tobacco User: add $20
Your Bi-weekly Medical Contribution:
MEDICAL BIMEDICAL BI--WEEKLY CONTRIBUTIONSWEEKLY CONTRIBUTIONS
7
TAX ADVANTAGE ACCOUNTSTAX ADVANTAGE ACCOUNTS
Flexible Spending Account (FSA) A Healthcare FSA is an account that allows you to set aside a portion of your income each year on a pre-tax basis so you can pay for qualified health care expenses with tax-free dollars. Because the money you contribute is deducted from your paycheck before taxes and the withdrawals are tax-free, your FSA can mean significant savings. You can use the tax-free dollars in your FSA for any qualified medical expense, for example: Copayments for doctor visits Health plan deductibles and coinsurance Prescriptions Dental and orthodontic care Hearing aids Eyeglasses, contact lenses, laser eye surgery With your Healthcare FSA, your contribution is deducted from your paycheck in equal amounts over the course of the year, but your full year’s contribution is available to you from day one. You can set aside up to $2,600 annually. If enrolled in the High Deductible Health Plan, you are not eligible to contribute towards a Healthcare FSA. Dependent Care Flexible Spending Account You may elect to have a specified number of pre-tax dollars deducted from your paycheck each period for dependent care expenses. You can set aside up to $5,000 for the plan year. Your contribution is deducted from your paycheck in equal amounts over the course of the year. However, only the funds actually deposited are available for withdrawal. This account reimburses you for dependent care expenses for eligible children and qualified adults to allow you and your spouse to work. Dependent care expenses are covered if your child is under age 13 or is physically or mentally incapable of self-care. You will be required to provide the Tax ID number of your dependent care provider. Before and after school programs are also qualified expenses. Both of the Flexible Spending Accounts are considered to be “use it or loose it”. This means that any unused amounts in the accounts at the end of the plan year will be forfeited. Keep this in mind when planning how much money you will need to allocate for these accounts. Limited Flexible Spending Account (Limited FSA) If you enroll in the High Deductible Health Plan, you can participate in the Limited FSA which reimburses you for eligible dental and vision expenses. By establishing a Limited FSA, you can save money on taxes by using these dollars for your dental and vision expenses while preserving your HSA funds for other purposes. The maximum yearly contribution is $2,600. Health Spending Account (HSA) If you enroll in the High Deductible Health Plan, you can participate in the Health Savings Account. You can make deposits through payroll deductions up to the annual limits set by the IRS of $3,400 for single and $6,750 for family. You can use this account to pay for medical, dental and vision expenses. At age 55 and above, an additional $1,000 contribution is allowed annually.
8
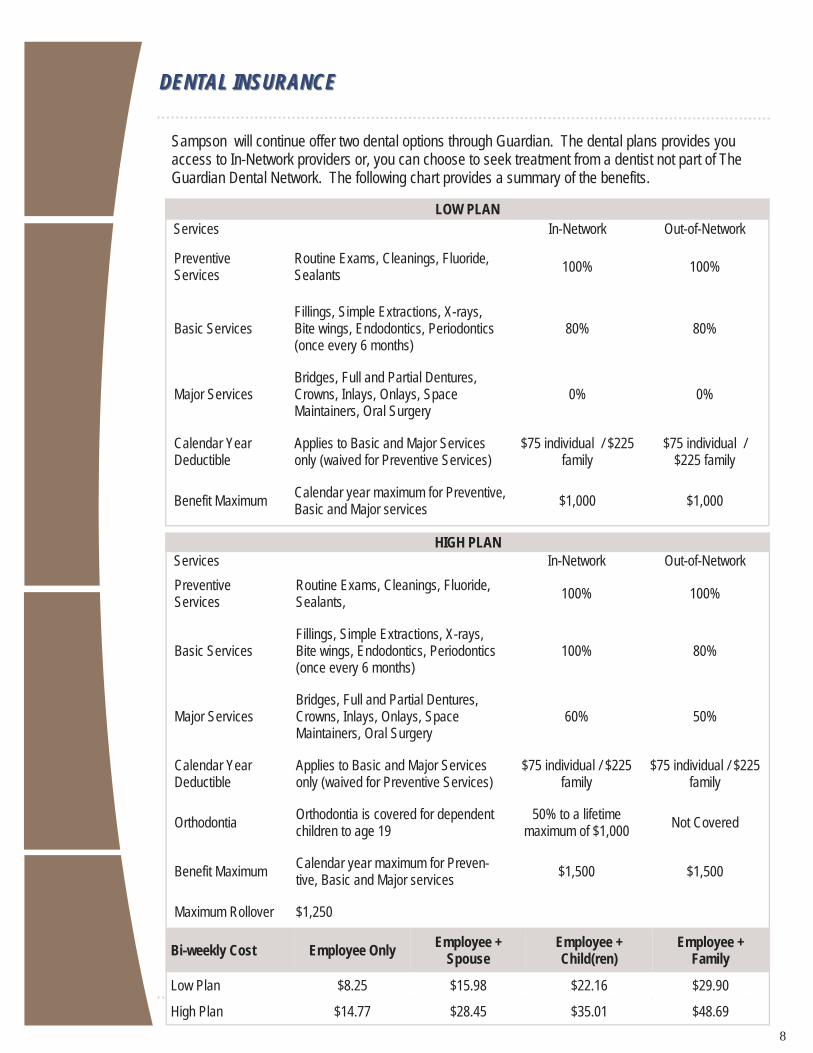
Sampson will continue offer two dental options through Guardian. The dental plans provides you access to In-Network providers or, you can choose to seek treatment from a dentist not part of The Guardian Dental Network. The following chart provides a summary of the benefits.
DENTAL INSURANCEDENTAL INSURANCE
LOW PLAN Services In-Network Out-of-Network
Preventive Services
Routine Exams, Cleanings, Fluoride, Sealants
100% 100%
Basic Services Fillings, Simple Extractions, X-rays, Bite wings, Endodontics, Periodontics (once every 6 months)
80% 80%
Major Services Bridges, Full and Partial Dentures, Crowns, Inlays, Onlays, Space Maintainers, Oral Surgery
0% 0%
Calendar Year Deductible
Applies to Basic and Major Services only (waived for Preventive Services)
$75 individual / $225 family
$75 individual / $225 family
Benefit Maximum Calendar year maximum for Preventive, Basic and Major services
$1,000 $1,000
Services In-Network Out-of-Network
Preventive Services
Routine Exams, Cleanings, Fluoride, Sealants,
100% 100%
Basic Services Fillings, Simple Extractions, X-rays, Bite wings, Endodontics, Periodontics (once every 6 months)
100% 80%
Major Services Bridges, Full and Partial Dentures, Crowns, Inlays, Onlays, Space Maintainers, Oral Surgery
60% 50%
Calendar Year Deductible
Applies to Basic and Major Services only (waived for Preventive Services)
$75 individual / $225 family
$75 individual / $225 family
Benefit Maximum Calendar year maximum for Preven-tive, Basic and Major services
$1,500 $1,500
HIGH PLAN
Orthodontia Orthodontia is covered for dependent children to age 19
50% to a lifetime maximum of $1,000
Not Covered
Maximum Rollover $1,250
Bi-weekly Cost
Low Plan $8.25 $15.98 $22.16 $29.90
High Plan $14.77 $28.45 $35.01 $48.69
Employee Only Employee +
Spouse Employee + Child(ren)
Employee + Family
9
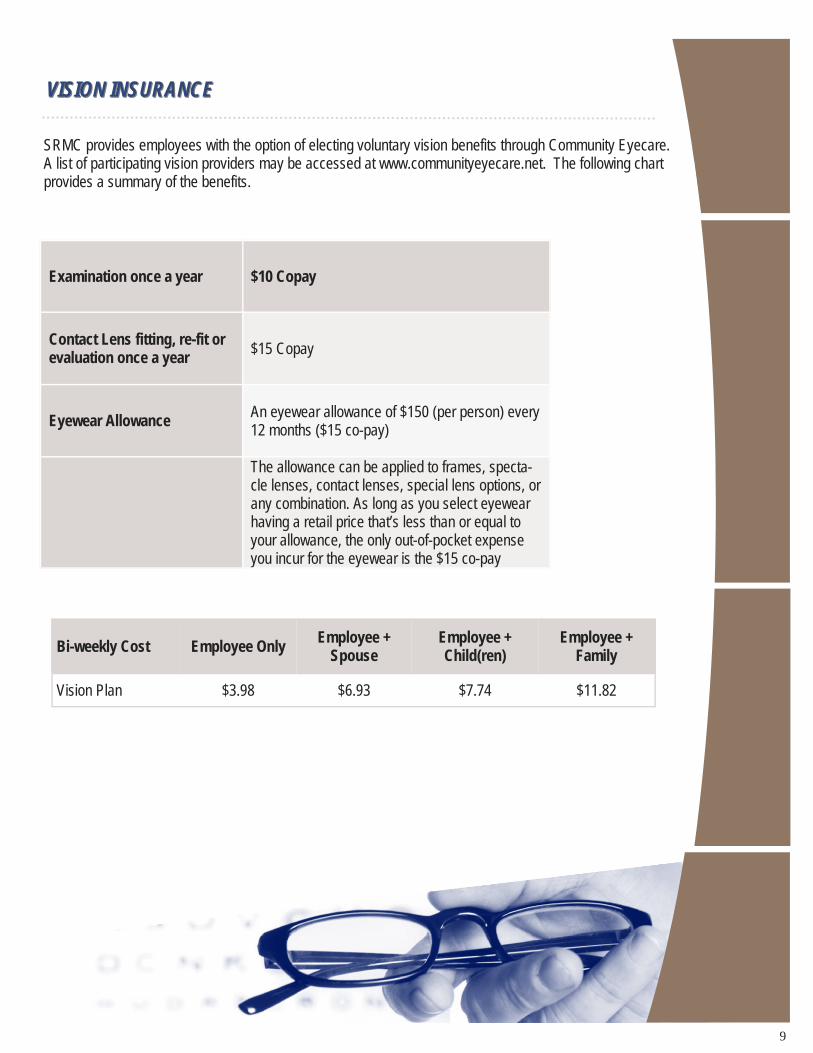
SRMC provides employees with the option of electing voluntary vision benefits through Community Eyecare. A list of participating vision providers may be accessed at www.communityeyecare.net. The following chart provides a summary of the benefits.
VISION INSURANCEVISION INSURANCE
Examination once a year $10 Copay
Contact Lens fitting, re-fit or evaluation once a year $15 Copay
Eyewear Allowance An eyewear allowance of $150 (per person) every 12 months ($15 co-pay)
The allowance can be applied to frames, specta-cle lenses, contact lenses, special lens options, or any combination. As long as you select eyewear having a retail price that’s less than or equal to your allowance, the only out-of-pocket expense you incur for the eyewear is the $15 co-pay
Bi-weekly Cost Employee Only Employee +
Spouse Employee + Child(ren)
Employee + Family
Vision Plan $3.98 $6.93 $7.74 $11.82
10
SRMC provides full-time employees with group life and accidental death and dismemberment (AD&D) through Lincoln Financial Group. The benefit is as follows: Class 1: One times base annual salary rounded to the next highest $1,000, to a maximum of $200,000 Class 2: One times base annual salary rounded to the next highest $1,000, to a maximum of $162,000
BASIC LIFE AND ACCIDENTAL DEATH AND DISMEMBERMENT INSURANCEBASIC LIFE AND ACCIDENTAL DEATH AND DISMEMBERMENT INSURANCE
VOLUNTARY LIFE AND ACCIDENTAL DEATH INSURANCEVOLUNTARY LIFE AND ACCIDENTAL DEATH INSURANCE
Benefit Guarantee Issue Amount
Employee Increments of $10,000 to a maximum of $300,000 $100,000 for new hire
Spouse Increments of $5,000 to a maximum of 2.5 times the employee’s salary
$25,000 for new hire
Child(ren) Increments of $2,000 to a maximum of $10,000 (depending on age)
Not applicable
SRMC provides full-time employees with the option of purchasing additional life insurance on a voluntary basis through Lincoln Financial Group.
Note: If electing employee voluntary life after the initial enrollment, your guarantee issue amount is $10,000. If electing voluntary life for your spouse after the initial enrollment, the guarantee issue amount is $5,000. Any amount over the guaranteed issue amount is subject to evidence of insurability.
Age Monthly Life & AD&D rates per
$1,000 of coverage
<25 $0.10 25-29 $0.10 30-34 $0.10 35-39 $0.14 40-44 $0.21 45-49 $0.33 50-54 $0.54 55-59 $0.87 60-64 $1.15 65-69 $1.79 70-74 $3.11 75-79 $5.31
Employee AD&D $0.02
Spouse AD&D $0.02 Child Life & AD&D $0.08
Important Note: During Open Enrollment employees can elect up to two increments ($20,000) in additional life insurance without completing an Evidence of Insurability form. Spouses can also increase their voluntary life insurance election by two increments ($10,000) without completing an Evidence of Insurability form.
11
SRMC provides full-time employees with short and long-term disability income benefits on a voluntary basis. In the event you become disabled due to a non work-related injury or sickness, disability income benefits are provided as a source of income.
DISABILITY INCOME BENEFITSDISABILITY INCOME BENEFITS
Short-Term Disability Long-Term Disability
Benefits Begin
15th day of disability resulting from an Accident
15th day of disability resulting
from an Illness
After a 180 Day elimination period
Benefits Duration 24 Weeks 2 Year Own Occupation with
Benefit Duration of definition of SSNRA
Percentage of Income Replaced 60%
Class 1: 66.66% Class 2: 60%
Maximum Benefit $2,500 per week Class 1: $11,000 per month Class 2: $10,000 per month
Employee Cost $ 0.51 per $10 of weekly benefit Employees pay $3.00 per pay period
for the Long-term disability plan. SRMC pays majority of the cost.
Note: Short and Long term disability insurance have a pre-existing condition limitation. This means that if you were treated for a medical condition three months prior to the effective date that specific condition will be considered a pre-existing condition and will not be covered for twelve months after the effective date of coverage. Refer to the benefit plan summary for more details.
Employee Assistance Program (EAP)Employee Assistance Program (EAP)
SRMC provides full-time employees and their immediate family 24/7 access to resources on the following topics through Lincoln Financial Group: -Depression -Marital or family difficulties -Substance abuse -Stress management/anxiety -Legal or financial concerns -child or elder care Access Online: www.GuidanceResources.com Username: LFGSupport Password: LFGsupport1 Access by phone: 888-628-4824
12
Group Voluntary Accident Insurance, offered by Allstate Benefits, can help cover the unexpected costs related to accident expenses. Em-ployees, employee’s spouse and dependent children are eligible for this plan. This policy pays a specific benefit amount for: Initial care such as ambulance, emergency room, and initial
doctor visit Follow-up care such as outpatient doctor’s treatment, and
medical devices Injuries, including burns, dislocations and fractures Catastrophic accident Accidental death
ACCIDENT INSURANCEACCIDENT INSURANCE This benefit, offered through Aflac, pays a lump sum benefit when you are diagnosed with a critical illness. Cancer (internal or invasive), Stroke, Kidney Failure, Heart Attack, Major Organ Transplant, Carcinoma in situ, and Coronary Artery Bypass Surgery are all covered critical illnesses. Plan Features: Lump-sum benefits paid directly to the insured (unless
otherwise assigned) following the diagnosis of each covered critical illness
Spouse coverage available Each dependent child is covered at 25% of the primary
insured amount at no additional charge. Benefits amounts available for $5,000 up to $50,000 for
employees and $30,000 for spouse. Annual Health Screening Benefits included. The plan is portable with stipulations. Immediate effective date—coverage will be effective the date
the employee signs the application. After the waiting period, an insured may receive a Wellness Benefit of $100 for any one covered screening test per calendar year. Some of the covered health screening tests include the following:
Mammograms Colonoscopy Chest X-ray Stress test on a bicycle or treadmill Fasting blood glucose test Bone marrow testing Breast ultrasound CA 15-3 (blood test for breast cancer) CA 125 (blood test for colon cancer) CEA (blood test for colon cancer)
CRITICAL ILLNESS CRITICAL ILLNESS
Additional Features: Benefits are paid for accidents that occur on and off the job. Premiums are paid through convenient payroll deduction. The coverage is individually owned so you may be able to take
it with you if you leave your employer. Coverage is guaranteed at initial enrollment, there are no medi-
cal exams to take. 24 hour accident coverage for yourself or your entire family Benefits are paid directly to you unless you assign them to
someone else. The coverage is portable.
Group Universal Life and Accidental Death & Dismemberment , of-fered by Allstate Benefits, is designed to provide death benefits to your beneficiaries if you pass away, but it also allows you to build up cash value. As long as you have enough cash value to pay for your policy’s insurance charges, your coverage stays in force.
Family coverage options are available for your spouse, children and grandchildren.
Premium rates are based on age and tobacco usage You may take the coverage with you if employment ends
as long as premiums are paid to the insurance company The following riders are included with your plans:
Premium Waiver Accidental Death Benefit
This information is not intended to be a complete description of the insurance coverage available. Group Universal Life benefits provided by policy form GUL22P or state variation. The policies have exclusions and limitations, and may have reductions of benefits at specific ages.
GROUP UNIVERSAL LIFE AND GROUP UNIVERSAL LIFE AND ACCIDENTAL DEATH & DISMEMBERMENTACCIDENTAL DEATH & DISMEMBERMENT
OPTIONAL VOLUNTARY BENEFITSOPTIONAL VOLUNTARY BENEFITS
13
Benefit Carrier Phone Website
Medical Insurance UMR 800-826-9781 www.umr.com
Vision Insurance Community Eyecare 888-254-4290 www.communityeyecare.net
Basic Life and AD&D Voluntary Life and AD&D Long Term Disability Short Term Disability
Lincoln Financial Group 800-423-2765 www.lfg.com
Accident Insurance and Universal Life Insurance
Allstate 800-521-5353 www.allstateatwork.com
Flexible Spending Accounts Stanley Benefits 877-727-3539 www.stanleybenefits.com
Dental Insurance Guardian 800-541-7846 www.guardiananytime.com
Critical Illness Aflac 800-433-3036 www.aflacgroupinsurance.com
Health Savings Accounts Stanley Benefits 877-727-3539 www.stanleybenefits.com
The information in this guide is not a promise or guarantee of employment or benefit coverage. If there is a conflict between information in this guide and the actual plan documents or policies, the documents and policies will always govern. Complete details about all benefits can be obtained by reviewing current plan descriptions, contracts, certificates, policies, and plan documents available from the Human Resources Department.
SRMC Human Resources Department Open Monday-Friday 8:30am - 5:00pm
CONTACT INFORMATIONCONTACT INFORMATION

14
Special Enrollment Model Notice If you are declining enrollment for yourself or your dependents (including your spouse) because of other health in-surance or group health plan coverage, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage (or if the employer stops contributing towards your or your dependents' other coverage). However, you must request enrollment within 30 days after your or your dependents' other coverage ends (or after the employer stops contributing toward the other coverage). If you decline enrollment for yourself or for an eligible dependent (including your spouse) while Medicaid coverage or coverage under a state children's health insurance program is in effect, you may be able to enroll yourself and your dependents in this plan if you or your dependents lose eligibility for that other coverage. However, you must request enrollment within 60 days after your or your dependents' coverage ends under Medicaid or a state children's health insurance program. If you or your dependents (including your spouse) become eligible for a state premium assistance subsidy from Medicaid or through a state children's health insurance program with respect to coverage under this plan, you may be able to enroll yourself and your dependents in this plan. However, you must request enrollment within 60 days after your or your dependents' determination of eligibility for such assistance.
Newborns’ and Mothers Health Protection Act Enrollment Notice Group health plans and health insurance issuers generally may not, under federal law, restrict benefits for any hospi-tal length of stay in connection with childbirth for the mother or newborn child to less than 48 hours following a vaginal delivery, or less than 96 hours following a cesarean section. However, federal law generally does not prohib-it the mother's or newborn's attending provider, after consulting with the mother, from discharging the mother or her newborn earlier than 48 hours (or 96 hours as applicable). In any case, plans and issuers may not, under federal law, require that a provider obtain authorization from the plan or the issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
Women’s Health and Cancer Rights Act Enrollment Notice
If you have had or are going to have a mastectomy, you may be entitled to certain benefits under the Women’s Health and Cancer Rights Act of 1998 (WHCRA). For individuals receiving mastectomy-related benefits, coverage will be provided in a manner determined in consultation with the attending physician and the patient, for: all stages of reconstruction of the breast on which the mastectomy was performed; surgery and reconstruction of the other breast to produce a symmetrical appearance; prostheses; and treatment of physical complications of the mastectomy, including lymphedema. These benefits will be provided subject to the same deductibles and coinsurance applicable to other medical and sur-gical benefits provided under this plan. Therefore, the following deductibles and coinsurance apply: UMR PPO Deductible: In Network: $1,000 individual; $2,000 family Out of Network: $7,500 individual; $15.000 family Out-of-Pocket: In Network: $2,750 individual; $5,000 family Out of Network: $10,000 individual; $20,000 family UMR HSA: Deductible: In Network: $1,500 individual; $3,000 family Out of Network: $4,500 individual; $9,000 family Out-of-Pocket: In Network: $3,500 individual; $5,000 family Out of Network: $10,000 individual; $20,000 family
15
Lifetime Limits Model Notice
The lifetime limit on the dollar value of benefits under the UMR Medical Plans no longer applies. Individuals whose coverage ended by reason of reaching a lifetime limit under the plan are eligible to enroll in the plan. In-dividuals have 30 days from the date of this notice to request enrollment.
Important Notice from SRMC About Your Prescription Drug Coverage and Medicare
Please read this notice carefully and keep it where you can find it. This notice has information about your current prescription drug coverage with SRMC and about your options under Medicare’s prescription drug coverage. This information can help you decide whether or not you want to join a Medicare drug plan. If you are consider-ing joining, you should compare your current coverage, including which drugs are covered at what cost, with the coverage and costs of the plans offering Medicare prescription drug coverage in your area. Information about where you can get help to make decisions about your prescription drug coverage is at the end of this notice. There are two important things you need to know about your current coverage and Medicare’s prescription drug coverage: 1. Medicare prescription drug coverage became available in 2006 to everyone with Medicare. You can get this coverage if you join a Medicare Prescription Drug Plan or join a Medicare Advantage Plan (like an HMO or PPO) that offers prescription drug coverage. All Medicare drug plans provide at least a standard level of cover-age set by Medicare. Some plans may also offer more coverage for a higher monthly premium. 2. SRMC has determined that the prescription drug coverage offered by the UMR plans are, on average for all plan participants, expected to pay out as much as standard Medicare prescription drug coverage pays and is therefore considered Creditable Coverage. Because your existing coverage is Creditable Coverage, you can keep this coverage and not pay a higher premium (a penalty) if you later decide to join a Medicare drug plan. When Can You Join A Medicare Drug Plan? You can join a Medicare drug plan when you first become eligible for Medicare and each year from October 15th to December 7th. However, if you lose your current creditable prescription drug coverage, through no fault of your own, you will also be eligible for a two (2) month Special Enrollment Period (SEP) to join a Medicare drug plan. What Happens To Your Current Coverage If You Decide to Join A Medicare Drug Plan? If you decide to join a Medicare drug plan, your current SRMC coverage will be affected. See pages 7- 9 of the CMS Disclosure of Creditable Coverage To Medicare Part D Eligible Individuals Guidance (available at http://www.cms.hhs.gov/CreditableCoverage/), which outlines the prescription drug plan provisions/options that Medi-care eligible individuals may have available to them when they become eligible for Medicare Part D. If you do decide to join a Medicare drug plan and drop your current SRMC coverage, be aware that you and your dependents will not be able to get this coverage back. When Will You Pay A Higher Premium (Penalty) To Join A Medicare Drug Plan? You should also know that if you drop or lose your current coverage with SRMC and don’t join a Medicare drug plan within 63 continuous days after your current coverage ends, you may pay a higher premium (a penalty) to join a Medicare drug plan later. If you go 63 continuous days or longer without creditable prescription drug coverage, your monthly premium may go up by at least 1% of the Medicare base beneficiary premium per month for every month that you did not have that coverage. For example, if you go nineteen months without creditable coverage, your premium may consistently be at least 19% higher than the Medicare base beneficiary premium. You may have to pay this high-er premium (a penalty) as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to join.

16
For More Information About Your Options Under Medicare Prescription Drug Coverage… More detailed information about Medicare plans that offer prescription drug coverage is in the “Medicare & You” handbook. You’ll get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare drug plans. For more information about Medicare prescription drug coverage: Visit www.medicare.gov Call your State Health Insurance Assistance Program (see the inside back cover of your copy of the “Medicare & You” handbook for their telephone number) for personalized help Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048. If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available. For information about this extra help, visit Social Security on the web at www.socialsecurity.gov, or call them at 1-800-772-1213 (TTY 1-800-325-0778). Remember: Keep this Creditable Coverage notice. If you decide to join one of the Medicare drug plans, you may be required to provide a copy of this notice when you join to show whether or not you have maintained creditable coverage and, therefore, whether or not you are required to pay a higher premium (a penalty). Date: January 1, 2017 Name of Entity/Sender: Sampson Regional Medical Center Contact--Position/Office: Bradley Jackson, Controller Address: 607 Beaman Street, Clinton, NC 28329-0260 Phone Number: (910) 592-8511
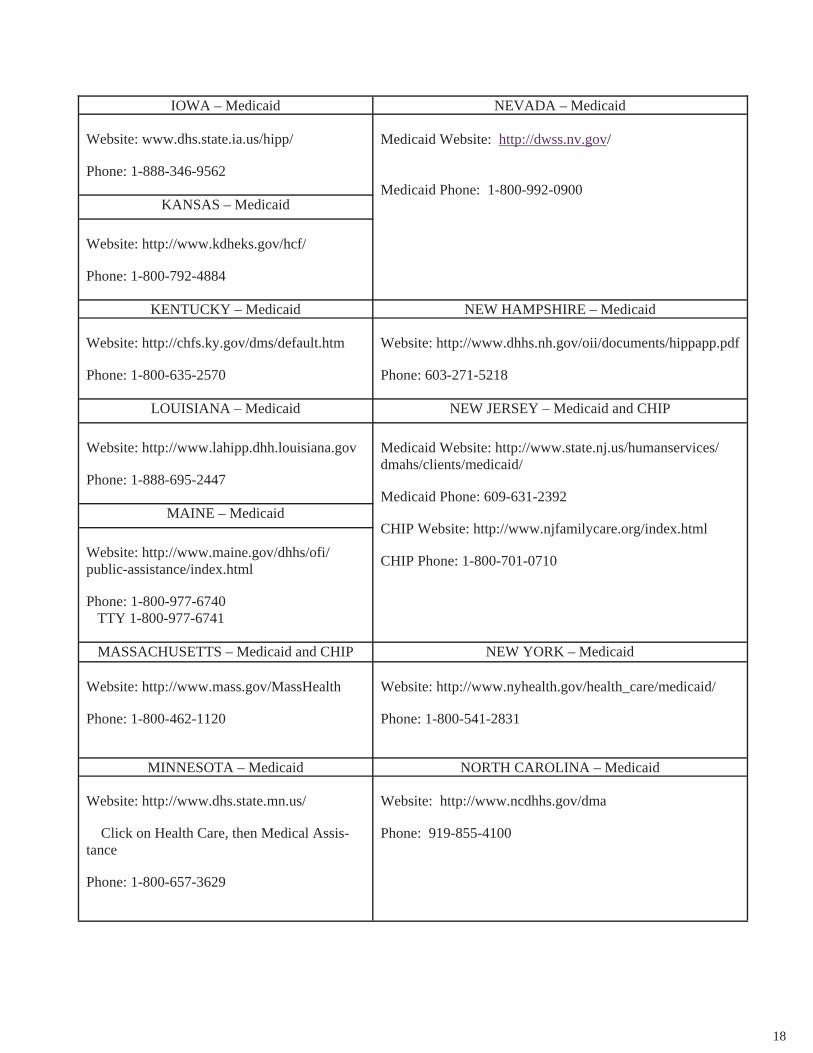
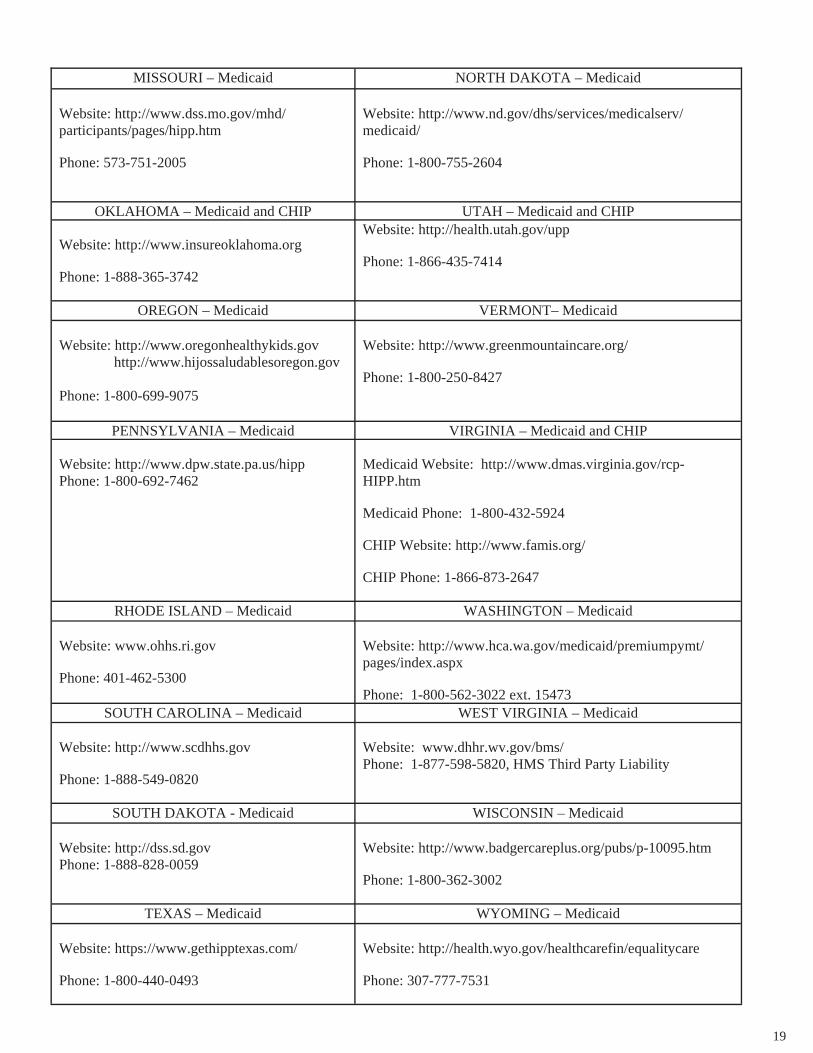
Premium Assistance Under Medicaid and the Children’s Health Insurance Program (CHIP) If you or your children are eligible for Medicaid or CHIP and you’re eligible for health coverage from your employer, your state may have a premium assistance program that can help pay for coverage, using funds from their Medicaid or CHIP programs. If you or your children aren’t eligible for Medicaid or CHIP, you won’t be eligible for these premium assistance programs but you may be able to buy individual insurance coverage through the Health Insurance Marketplace. For more information, visit www.healthcare.gov. If you or your dependents are already enrolled in Medicaid or CHIP and you live in a State listed below, contact your State Medicaid or CHIP office to find out if premium assistance is available. If you or your dependents are NOT currently enrolled in Medicaid or CHIP, and you think you or any of your dependents might be eligible for either of these programs, contact your State Medicaid or CHIP office or dial 1-877-KIDS NOW or www.insurekidsnow.gov to find out how to apply. If you qualify, ask your state if it has a program that might help you pay the premiums for an employer-sponsored plan. If you or your dependents are eligible for premium assistance under Medicaid or CHIP, as well as eligible under your employer plan, your employer must allow you to enroll in your employer plan if you aren’t already enrolled. This is called a “special enrollment” opportunity, and you must request coverage within 60 days of being determined eligible for premium assistance. If you have questions about enrolling in your employer plan, contact the Department of Labor at www.askebsa.dol.gov or call 1-866-444-EBSA (3272).

17
ALABAMA – Medicaid COLORADO – Medicaid
Website: http://www.medicaid.alabama.gov Phone: 1-855-692-5447
Medicaid Website: http://www.colorado.gov/ Medicaid Phone (In state): 1-800-866-3513 Medicaid Phone (Out of state): 1-800-221-3943
ALASKA – Medicaid
Website: http://health.hss.state.ak.us/dpa/programs/medicaid/ Phone (Outside of Anchorage): 1-888-318-8890 Phone (Anchorage): 907-269-6529
ARIZONA – CHIP FLORIDA – Medicaid
Website: http://www.azahcccs.gov/applicants Phone (Outside of Maricopa County): 1-877-764-5437 Phone (Maricopa County): 602-417-5437
Website: https://www.flmedicaidtplrecovery.com/ Phone: 1-877-357-3268
GEORGIA – Medicaid
Website: http://dch.georgia.gov/ - Click on Programs, then Medicaid, then Health Insurance Premium Pay-ment (HIPP) Phone: 1-800-869-1150
IDAHO – Medicaid MONTANA – Medicaid
Medicaid Website: http://healthandwelfare.idaho.gov/Medical/Medicaid/PremiumAssistance/tabid/1510/Default.aspx Medicaid Phone: 1-800-926-2588
Website: http://medicaidprovider.hhs.mt.gov/clientpages/ clientindex.shtml Phone: 1-800-694-3084
INDIANA – Medicaid NEBRASKA – Medicaid
Website: http://www.in.gov/fssa Phone: 1-800-889-9949
Website: www.ACCESSNebraska.ne.gov
Phone: 1-800-383-4278
If you live in one of the following states, you may be eligible for assistance paying your employer health plan premiums. The following list of states is current as of January 31, 2014. Contact your State for more infor-mation on eligibility.
18
IOWA – Medicaid NEVADA – Medicaid Website: www.dhs.state.ia.us/hipp/ Phone: 1-888-346-9562
Medicaid Website: http://dwss.nv.gov/
Medicaid Phone: 1-800-992-0900
KANSAS – Medicaid
Website: http://www.kdheks.gov/hcf/ Phone: 1-800-792-4884
KENTUCKY – Medicaid NEW HAMPSHIRE – Medicaid Website: http://chfs.ky.gov/dms/default.htm Phone: 1-800-635-2570
Website: http://www.dhhs.nh.gov/oii/documents/hippapp.pdf Phone: 603-271-5218
LOUISIANA – Medicaid NEW JERSEY – Medicaid and CHIP
Website: http://www.lahipp.dhh.louisiana.gov Phone: 1-888-695-2447
Medicaid Website: http://www.state.nj.us/humanservices/ dmahs/clients/medicaid/ Medicaid Phone: 609-631-2392 CHIP Website: http://www.njfamilycare.org/index.html CHIP Phone: 1-800-701-0710
MAINE – Medicaid
Website: http://www.maine.gov/dhhs/ofi/public-assistance/index.html Phone: 1-800-977-6740 TTY 1-800-977-6741
MASSACHUSETTS – Medicaid and CHIP NEW YORK – Medicaid Website: http://www.mass.gov/MassHealth Phone: 1-800-462-1120
Website: http://www.nyhealth.gov/health_care/medicaid/ Phone: 1-800-541-2831
MINNESOTA – Medicaid NORTH CAROLINA – Medicaid Website: http://www.dhs.state.mn.us/ Click on Health Care, then Medical Assis-tance Phone: 1-800-657-3629
Website: http://www.ncdhhs.gov/dma Phone: 919-855-4100
19
MISSOURI – Medicaid NORTH DAKOTA – Medicaid
Website: http://www.dss.mo.gov/mhd/participants/pages/hipp.htm Phone: 573-751-2005
Website: http://www.nd.gov/dhs/services/medicalserv/medicaid/ Phone: 1-800-755-2604
OKLAHOMA – Medicaid and CHIP UTAH – Medicaid and CHIP Website: http://www.insureoklahoma.org Phone: 1-888-365-3742
Website: http://health.utah.gov/upp Phone: 1-866-435-7414
OREGON – Medicaid VERMONT– Medicaid Website: http://www.oregonhealthykids.gov http://www.hijossaludablesoregon.gov Phone: 1-800-699-9075
Website: http://www.greenmountaincare.org/ Phone: 1-800-250-8427
PENNSYLVANIA – Medicaid VIRGINIA – Medicaid and CHIP Website: http://www.dpw.state.pa.us/hipp Phone: 1-800-692-7462
Medicaid Website: http://www.dmas.virginia.gov/rcp-HIPP.htm Medicaid Phone: 1-800-432-5924 CHIP Website: http://www.famis.org/ CHIP Phone: 1-866-873-2647
RHODE ISLAND – Medicaid WASHINGTON – Medicaid Website: www.ohhs.ri.gov Phone: 401-462-5300
Website: http://www.hca.wa.gov/medicaid/premiumpymt/pages/index.aspx Phone: 1-800-562-3022 ext. 15473
SOUTH CAROLINA – Medicaid WEST VIRGINIA – Medicaid Website: http://www.scdhhs.gov Phone: 1-888-549-0820
Website: www.dhhr.wv.gov/bms/ Phone: 1-877-598-5820, HMS Third Party Liability
SOUTH DAKOTA - Medicaid WISCONSIN – Medicaid
Website: http://dss.sd.gov Phone: 1-888-828-0059
Website: http://www.badgercareplus.org/pubs/p-10095.htm Phone: 1-800-362-3002
TEXAS – Medicaid WYOMING – Medicaid Website: https://www.gethipptexas.com/ Phone: 1-800-440-0493
Website: http://health.wyo.gov/healthcarefin/equalitycare Phone: 307-777-7531
20
To see if any other states have added a premium assistance program since January 31, 2014, or for more information on special enrollment rights, contact either: U.S. Department of Labor U.S. Department of Health and Health Services Employee Benefits Security Administration Centers for Medicare & Medicaid Services www.dol.gov/ebsa www.cms.hhs.gov 1-866-444-EBSA (3272) 1-877-267-2323, Menu Option 4, Ext. 61565 OMB Control Number 1210-0137 (expires 10/31/2016)
SRMC
HIPAA NOTICE OF PRIVACY PRACTICES THIS NOTICE DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DIS-CLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CARE-FULLY. This Notice of Privacy Practices describes how SRMC may use or disclosed protected health information to carry out treatment, payment, healthcare operations, and for other purposes that are permitted or required by law. This Notice also sets out our legal obligations concerning your protected health information, and describes your rights to access and control your protected health information. Protected health information (or "PHI") is individually identifiable health information, including demographic infor-mation, collected from you or created or received by a healthcare provider, a health plan, your employer (when func-tioning on behalf of SRMC or a healthcare clearinghouse and that relates to: (i) your past, present, or future physical or mental health or condition; (ii) the provision of health care to you; or (iii) the past, present, or future payment for the provision of health care to you. This Notice of Privacy Practices has been drafted to be consistent with what is known as the "HIPAA Privacy Rule," and any of the terms not defined in this Notice should have the same meaning as they have in the HIPAA Privacy Rule.
If you have any questions or want additional information about the Notice or the policies and procedures described in the Notice, please contact: Privacy Officer, Michael Gilpin, SRMC, (910) 592-8511 This Notice of Privacy Practices becomes effective on October 1, 2014. Our Responsibilities The SRMC HEALTH PLAN is required by law to maintain the privacy of your protected health information. We are obligated to provide you with a copy of this Notice of our legal duties and of our privacy practices with respect to pro-tected health information and we must abide by the terms of this Notice. We reserve the right to change the provisions of our Notice and make the new provisions effective for all protected health information that we maintain. If we make a material change to our Notice, we will mail a revised Notice by First Class U.S. Mail to you at the address that we have on record for you. Primary Uses and Disclosures of Protected Health Information The following is a description of how we are most likely to use and/or disclose your protected health information. Payment and Health Care Operations We have the right to use and disclose your protected health information for all activities that are included within the definitions of “treatment,” “payment," and "health care operations" as set out in 45 C.F.R. § 164.501 (this provision is a part of the HIPAA Privacy Rule). We have not listed in this Notice all of the activities included within these definitions, so please refer to 45 C.F.R. § 164.501 for a complete list.
21
Treatment We may disclose your PHI to a healthcare provider for the healthcare provider’s treatment purposes, although it is more likely that a healthcare provider would receive your PHI from another healthcare provider, rather than from the SRMC HEALTH PLAN. For example, if your Primary Care Physician (PCP) or your treating medical provider refers you to a specialist for treatment, the SRMC HEALTH PLAN can disclose your PHI to the specialist to whom you have been referred so that they can become familiar with your medical condition, prior diagnoses and treatment, and prognosis. Payment We will use or disclose your PHI to pay claims for services provided to you and to obtain stop-loss reimburse-ments, or to otherwise fulfill our responsibilities for coverage and providing benefits. For example, we may disclose your protected health information when a provider requests information regarding your eligibility for coverage under the SRMC HEALTH PLAN, or we may use your information to determine if a treatment that you received was medically necessary. Healthcare Operations We will use or disclose your protected health information to support our business functions. These functions include, but are not limited to: underwriting; premium rating; conducting quality assessment and improvement activities; licensing; submitting claims for stop-loss coverage; conducting or arranging for medical review, legal services, audit services; business planning and business development. For example, we may use or dis-close your protected health information: (i) to provide you with information about one of our disease manage-ment programs; (ii) to respond to a customer service inquiry from you; or (iii) in connection with fraud and abuse detection and compliance programs. Business Associates The SRMC HEALTH PLAN contracts with individuals and entities (Business Associates) to perform various functions on our behalf or to provide certain types of services, such as legal, actuarial, accounting, consulting, or administrative services. To perform these functions or to provide the services, our Business Associates will receive, create, maintain, use, or disclose protected health information, but only after we require the Business Associates to agree in writing to contract terms designed to appropriately safeguard your information. For ex-ample, we may disclose your protected health information to a Business Associate to administer claims or to provide member service support, utilization management, or pharmacy benefit management. Examples of Business Associates include Interactive Medical Systems, the SRMC HEALTH PLAN’s Third-Party Admin-istrator, which handles many of the functions in connection with the operation of SRMC HEALTH PLAN. Other Covered Entities The SRMC HEALTH PLAN may use or disclose your protected health information to assist healthcare pro-viders in connection with their treatment or payment activities, or to assist other covered entities in connection with payment activities and certain healthcare operations. For example, we may disclose your protected health information to a healthcare provider when needed by the provider to render treatment to you, and we may dis-close protected health information to another covered entity to conduct healthcare operations in the areas of quality assurance and improvement activities, or accreditation, certification, licensing, or credentialing. This also means that we may disclose or share your protected health information with other insurance carriers in order to coordinate benefits, if you or your family members have coverage through another carrier. Plan Sponsor The SRMC HEALTH PLAN may disclose PHI to SRMC HEALTH PLAN sponsor, but only if the sponsor has amended its plan document as required by the Privacy Rule, certified to the SRMC HEALTH PLAN as required by the Privacy Rule, and established certain safeguards and firewalls to limit the classes of employees who will have access to PHI and to limit the use of PHI to plan purposes and not for non-permissible purposes. Any disclosures to SRMC HEALTH PLAN sponsor must be for purposes of administering the SRMC HEALTH PLAN, or pursuant to an authorization request signed by you. Examples would include disclosing “summary health information” (as defined under the HIPAA medical privacy regulations) to SRMC HEALTH PLAN sponsor for the purpose of obtaining premium bids or modifying, amending, or terminating SRMC HEALTH PLAN.

22
Potential Impact of State Law The HIPAA Privacy Regulations generally do not "preempt" (or take precedence over) state privacy or other applicable laws that provide individuals greater privacy protections. As a result, to the extent state law applies, the privacy laws of a particular state, or other federal laws, rather than the HIPAA Privacy Regulations, might impose a privacy standard under which the SRMC HEALTH PLAN will be required to operate. For example, where such laws have been enacted, we will follow more stringent state privacy laws that relate to uses and disclosures of protected health information concerning HIV or AIDS, mental health, substance abuse/chemical dependency, genetic testing, reproductive rights, etc. Other Possible Uses and Disclosures of Protected Health Information The following is a description of other possible ways in which the SRMC HEALTH PLAN may (and is permitted to) use and/or disclose your protected health information. Required by Law We may use or disclose your protected health information to the extent that federal law requires the use or disclosure. When used in this Notice, "required by law" is defined as it is in the HIPAA Privacy Rule. For example, we may disclose your protected health information when required by national security laws or public health disclosure laws. Public Health Activities We may use or disclose your protected health information for public health activities that are permitted or required by law. For example, we may use or disclose information for the purpose of preventing or controlling disease, injury, or disability, or we may disclose such information to a public health authority authorized to receive reports of child abuse or neglect. We also may dis-close protected health information, if directed by a public health authority, to a foreign government agency that is collaborating with the public health authority. Health Oversight Activities We may disclose your protected health information to a health oversight agency for activities authorized by law, such as audits, investigations, inspections, licensure or disciplinary actions, or civil, administrative, or criminal proceedings or actions. Over-sight agencies seeking this information include government agencies that oversee: (i) the healthcare system; (ii) government ben-efit programs; (iii) other government regulatory programs; and (iv) compliance with civil rights laws. Abuse or Neglect We may disclose your protected health information to a government authority that is authorized by law to receive reports of abuse, neglect, or domestic violence. Additionally, as required by law, we may disclose to a governmental entity authorized to receive such information your information if we believe that you have been a victim of abuse, neglect, or domestic violence. Legal Proceedings We may disclose your protected health information: (1) in the course of any judicial or administrative proceeding; (2) in re-sponse to an order of a court or administrative tribunal (to the extent such disclosure is expressly authorized); and (3) in response to a subpoena, a discovery request, or other lawful process, once we have met all administrative requirements of the HIPAA Pri-vacy Rule. For example, we may disclose your protected health information in response to a subpoena for such information, but only after we first meet certain conditions required by the HIPAA Privacy Rule. Law Enforcement Under certain conditions, we also may disclose your protected health information to law enforcement officials. Some of the rea-sons for such a disclosure may include, but not be limited to: (1) it is required by law or some other legal process; (2) it is neces-sary to locate or identify a suspect, fugitive, material witness, or missing person; and (3) it is necessary to provide evidence of a crime that occurred on our premises. Coroners, Medical Examiners, Funeral Directors, and Organ Donation We may disclose protected health information to a coroner or medical examiner for purposes of identifying a deceased person, determining a cause of death, or for the coroner or medical examiner to perform other duties authorized by law. We also may disclose, as authorized by law, information to funeral directors so that they may carry out their duties. Further, we may disclose protected health information to organizations that handle organ, eye, or tissue donation and transplantation. Research We may disclose your protected health information to researchers when an institutional review board or privacy board has: (1) reviewed the research proposal and established protocols to ensure the privacy of the information; and (2) approved the research.
23
To Prevent a Serious Threat to Health or Safety Consistent with applicable federal and state laws, we may disclose your protected health information if we believe that the dis-closure is necessary to prevent or lessen a serious and imminent threat to the health or safety of a person or the public. We also may disclose protected health information if it is necessary for law enforcement authorities to identify or apprehend an individu-al. Military Activity and National Security, Protective Services Under certain conditions, we may disclose your protected health information if you are, or were, Armed Forces personnel for activities deemed necessary by appropriate military command authorities. If you are a member of foreign military service, we may disclose, in certain circumstances, your information to the foreign military authority. We also may disclose your protected health information to authorized federal officials for conducting national security and intelligence activities, and for the protec-tion of the President, other authorized persons, or heads of state. Inmates If you are an inmate of a correctional institution, we may disclose your protected health information to the correctional institution or to a law enforcement official for: (1) the institution to provide health care to you; (2) your health and safety and the health and safety of others; or (3) the safety and security of the correctional institution. Workers’ Compensation We may disclose your protected health information to comply with workers’ compensation laws and other similar programs that provide benefits for work-related injuries or illnesses. Others Involved in Your Health Care We may make your protected health information known to a family member, other relative, close personal friend, or other per-sonal representative that you identify. Such a use will be based on how involved the person is in your care, or payment that re-lates to your care. We may release information to parents or guardians, if allowed by law. We also may disclose your information to an entity assisting in a disaster relief effort so that your family can be notified about your condition, status, and location. If you are not present or able to agree to these disclosures of your protected health information, then, using our professional judgment, we may determine whether the disclosure is in your best interest. Required Disclosures of Your Protected Health Information The following is a description of disclosures that we are required by law to make. Disclosures to the Secretary of the U.S. Department of Health and Human Services We are required to disclose your protected health information to the Secretary of the U.S. Department of Health and Human Ser-vices when the Secretary is investigating or determining our compliance with the HIPAA Privacy Rule. Disclosures to You We are required to disclose to you most of your protected health information in a "designated record set" when you request ac-cess to this information. Generally, a "designated record set" contains medical and billing records, as well as other records that are used to make decisions about your health care benefits. We also are required to provide, upon your request, an accounting of most disclosures of your protected health information that are for reasons other than treatment, payment, and health care opera-tions, and are not disclosed through a signed authorization. Personal Representatives We will disclose your protected health information to an individual who has been designated by you as your personal representa-tive and who has qualified for such designation in accordance with relevant state law. However, before we will disclose protect-ed health information to such a person, you must submit a written notice of his/her designation, along with the documentation that supports his/her qualification (such as a power of attorney). Even if you designate a personal representative, the HIPAA Pri-vacy Rule permits us to elect not to treat the person as your personal representative if we have a reasonable belief that: (i) you have been, or may be, subjected to domestic violence, abuse, or neglect by such person; (ii) treating such person as your personal representative could endanger you; or (iii) we determine, in the exercise of our professional judgment, that it is not in your best interest to treat the person as your personal representative. Spouse and Other Family Members With only limited exceptions, we will send all mail to the employee. This includes mail relating to the employee’s spouse and other family members who are covered under the Plan, and includes mail with information on the use of Plan benefits by the em-ployee’s spouse and other family members. If a person covered under the Plan has requested Restrictions or Confidential Com-
24
munications (see following “Your Rights”), and if we have agreed to the request, we will send mail as provided by the request for Restrictions or Confidential Communications. Other Uses and Disclosures of Your Protected Health Information Other uses and disclosures of your protected health information that are not described above will be made only with your written authorization. If you provide us with such an authorization, you may revoke the authorization in writing, and this revocation will be effective for future uses and disclosures of protected health information. However, the revo-cation will not be effective for information that we already have used or disclosed in reliance on your authorization. YOUR RIGHTS The following is a description of your rights with respect to your protected health information. Right to Request a Restriction You have the right to request a restriction on the protected health information we use or disclose about you for pay-ment or health care operations. Except as provided in the next paragraph, we are not required to agree to any re-striction that you may request. If we do agree to the restriction, we will comply with the restriction, unless the infor-mation is needed to provide emergency treatment to you. Effective February 17, 2010, we will comply with any restriction request if; (1) except as otherwise required by law, the disclosure is to the health plan for purposes of carrying out payment or health care operations (and is not for the purposes of carrying out treatment); and (2) the protected health information pertains solely to a health care item or service for which the health care provider involved has been paid out-of-pocket in full. You may request a restriction by writing to Privacy Officer, SRMC HEALTH PLAN. In your request, please tell us: (1) the information whose disclosure you want to limit; and (2) how you want to limit our use and/or disclosure of the information. Right to Request Confidential Communications If you believe that a disclosure of all or part of your protected health information may endanger you, you may request that we communicate with you regarding your information in an alternative manner or at an alternative location. For example, you may ask that we only contact you at your work address or via your work e-mail. You may request a restriction by writing to Privacy Officer, SRMC HEALTH PLAN, 607 Beaman Street, Clinton, NC 28329-0260. In your request, please tell us: (1) that you want us to communicate your protected health information with you in an alternative manner or at an alternative location; and (2) that the disclosure of all or part of the protected health information in a manner inconsistent with your instructions would put you in danger. Right to Inspect and Copy You have the right to inspect and copy your protected health information that is contained in a "designated record set." Generally, a "designated record set" contains medical and billing records, as well as other records that are used to make decisions about your healthcare benefits. However, you may not inspect or copy psychotherapy notes or certain other information that may be contained in a designated record set. To inspect and copy your protected health information that is contained in a designated record set, you must submit your request in writing to Privacy Officer, SRMC HEALTH PLAN, 607 Beaman Street, Clinton, NC 28329-0260. If you request a copy of the information, we may charge a fee for the costs of copying, mailing, or other supplies associated with your request. We may deny your request to inspect and copy your protected health information in certain limited circumstances. If you are denied access to your information, you may request that the denial be reviewed. To request a review, you must submit a written request to Privacy Officer, SRMC HEALTH PLAN, 607 Beaman Street, Clinton, NC 28329-0260. A licensed health care professional chosen by us will review your request and the denial. The person performing this review will not be the same one who denied your initial request. Under certain conditions, our denial will not be re-viewable. If this event occurs, we will inform you in our denial that the decision is not reviewable. In certain cases, we may deny your request for an amendment. For example, we may deny your request if the infor-mation you want to amend is not maintained by us, but by another entity. If we deny your request, you have the right to file a statement of disagreement with us. Your statement of disagreement will be linked with the disputed
25
Right to Amend If you believe that your protected health information is incorrect or incomplete, you may request that we amend your information. You may request that we amend your information by writing to Privacy Officer, SRMC HEALTH PLAN, 607 Beaman Street, Clinton, NC 28329-0260. Your request should include the reason the amendment is necessary. Right of an Accounting You have a right to an accounting of certain disclosures of your protected health information that are for reasons other than treatment, payment, or healthcare operations. No accounting of disclosures is required for disclosures made pursuant to a signed authorization by you or your personal representative. You should know that most disclosures of protected health information will be for purposes of treatment, payment, or healthcare operations, and, therefore, will not be subject to your right to an accounting. An accounting will include the date(s) of the disclosure, to whom we made the disclosure, a brief description of the information disclosed, and the purpose for the disclosure. You may request an accounting by submitting your request in writing to Privacy Officer, SRMC HEALTH PLAN, 607 Beaman Street, Clinton, NC 28329-0260. Your request may be for disclosures made up to 6 years before the date of your request, but not for disclosures made before April 14, 2004. The first list you request within a 12-month period will be free. For additional lists, we may charge you for the costs of providing the list. We will notify you of the cost involved, and you may choose to withdraw or modify your request at the time before any costs are incurred. Right to be Notified of a Breach You have the right to be notified in the event that we (or a Business Associate) discover a breach of unsecured protected health information. Right to a Paper Copy of This Notice You have the right to a paper copy of this Notice, even if you have agreed to accept this Notice electronically. COMPLAINTS You may complain to us if you believe that we have violated your privacy rights. You may file a complaint with us by writing to Privacy Officer, SRMC HEALTH PLAN, 607 Beaman Street, Clinton, NC 28329-0260. You also may file a complaint with the Secretary of the U.S. Department of Health and Human Services. Complaints filed directly with the Secretary must: (1) be in writing; (2) contain the name of the entity against which the complaint is lodged; (3) describe the relevant problems; and (4) be filed within 180 days of the time you became or should have become aware of the problem. We will not penalize or any other way retaliate against you for filing a complaint with the Secretary or with us.