st. mary’s general hospital · st. mary’s general hospital will be the ... patient and family...
TRANSCRIPT

St. Mary’s General Hospital 1 911 Queen’s Blvd. Kitchener, ON N2M 1B2
St. Mary’s General Hospital
April 1, 2012

St. Mary’s General Hospital 2 911 Queen’s Blvd. Kitchener, ON N2M 1B2
Part A:
Overview of St. Mary’s Quality Improvement Plan 1. Overview of our quality improvement plan for 2012-13 St. Mary’s mission is “To continue the healing ministry of Christ consistent with our Catholic traditions and values”. In November 2010, we developed a new vision, strategic directions, and strategic goals that are in keeping with our mission. All of our strategic goals are in some way, related to improving quality of care for our patients and ultimately will support achieving our vision:
St. Mary’s General Hospital will be the safest and most effective hospital in Canada
characterized by innovation, compassion, and respect. Over the past year, we have engaged staff, volunteers and physicians in continuous improvement using Lean principles as our framework. In December 2010, St. Mary’s launched a campaign “1,000 Better Ways” to inspire our staff, physicians and volunteers to achieve our goals and ultimately our vision. In December 2011, we celebrated achievement of this goal with staff, physicians, volunteers, and two former patients. Click on the following link to hear some of our staff talk about their experience with continuous improvement and how it has helped St. Mary’s patients St. Mary's 1000 Better Ways Video. 2. What we will be focusing on and how these objectives will be achieved Our strategic goals and Quality Improvement Plans were developed with reference to our patient satisfaction survey results, incident report aggregate data, quality of care reviews, informal patient feedback, and other relevant quality indicators that are being tracked on our corporate balanced scorecard and Quality Report (shared quarterly with the Board Quality Committee and the Board of Trustees). St. Mary’s does exceptionally well in many areas of quality and safety. The following are some examples where we have demonstrated exceptional performance:
Hospital Standardized Mortality Ratio (HSMR) - Our HSMR continues to decrease and is well below the benchmark of 100.
Central Line Infections- Zero cases since December 2009. Ventilator Associated Pneumonia (VAP) - St. Mary’s has had 1 patient develop VAP from
August 2010 to end of February 2012.

St. Mary’s General Hospital 3 911 Queen’s Blvd. Kitchener, ON N2M 1B2
Surgical Safety Checklist- Our compliance rate with the surgical safety checklist is 99.8%. Patient and Family engagement- we engaged 432 patients and families through focus
groups, senior team patient rounds, and by including patients/families in quality of care reviews and improvement events. This will continue to be an expectation at St. Mary’s.
Another success we have had over the past year was with respect to the reduction of unnecessary time spent in acute care. Through a “Home First” St. Mary’s refresh initiated in August 2011, the number of patients that are alternate level of care at St. Mary’s has been reduced significantly. Many more patients are now making important decisions about their future from home, where judgment is not being affected by being in the acute care setting. The number of alternative level of care patients in the hospital per day has decreased from 20 to 12 (at the median). Also, the average length of stay for patients that require alternative level of care has decreased from 22 to 14 days. Please see the report on progress for the Quality Improvement Plan for last fiscal year 2011/12.

St. Mary’s General Hospital 4 911 Queen’s Blvd. Kitchener, ON N2M 1B2
The key areas that our strategic goals and Quality Improvement Plan (QIP) will focus on for 2012/13 to further enhance quality and patient safety is shown in the following chart (* indicates strategic goals included in QIP).
Strategic Direction
Strategic Goal Measure Target (2012/2013)
Improvement Initiatives/Comments
Quality and Safety
“We will provide safe, kind, effective and timely care in an environment of inquiry and learning.”
*The wait time for admitted
patients in the Emergency Department (ER) will decrease by 10% at the 90
th percentile.
ER wait times: 90th
percentile ER length of stay for admitted patients.
≤ 20 hours • Improve physician consultation request response time.
• Improve diagnostic test turnaround time for diagnostic imaging.
• Implement new flow coordinator role.
• Implement physician practice metrics and feedback system.
*The number of adverse events
affecting patients will decrease by 25%, from 229 to 166: -Hospital acquired Infections -Medication errors -Mislabeled lab specimens/patient identification errors
The number of adverse events including hospital acquired infections, medication incidents (severity level 2, 3, 4), and lab specimen labeling errors/patient identification errors.
≤ 166 (Reduce by 25%)
• Hand Hygiene compliance
• Training/Education of environmental support persons and other health care providers
• Increase visibility of infection control team (increase 1 FTE).
• Implement pre-emptive isolation for MRSA.
• Implement chlorine based cleaning solutions for Clostridium Difficile.
• Improve medication transcription process.
• Implement bedside positive patient ID and labeling for lab specimen collection in the ER.
Patient and Family-Centred Care
“We will ensure that the patient and their family are at the centre of everything we do, every encounter, every day.”
*Patient satisfaction regarding
the discharge transition process will improve by 2%.
Patient satisfaction results for following questions: -Discussed danger signals to watch for -Discussed purpose of home medications -Discussed when to resume normal activities.
Increase by 2% • Review/revise discharge information content and approach.
• Identify high risk patients on admission and ensure transition planning.
Our People
“We will foster a positive and productive culture that engages our greates resource—our staff, physicians and Volunteers.”
Staff, Physician and volunteer engagement will improve by 2%.
Staff and physician satisfaction survey results. Number of voluntary departures.
Increase by 2% • Three areas of focus include communication, value and recognition for good work, reduce non-value add activity to increase time for direct patient care.
• Quality of work life working group established to assist with development of specific initiatives for each of these priority areas.
1,000 measurable improvements will be implemented.
Number of measurable improvements made across the organization in 2011/12.
≥ 1,000 per year • Improvements will be suggested and implemented by all units through daily unit based huddles.

St. Mary’s General Hospital 5 911 Queen’s Blvd. Kitchener, ON N2M 1B2
Strategic Direction
Strategic Goal Measure Target (2012/2013)
Improvement Initiatives/Comments
Financial Stewardship
“We will invest our resources to achieve this vision.”
*Our budget will be balanced by
the end of 2012/13. Total Margin (consolidated): percent by which total corporate (consolidated) revenues exceed or fall short of total corporate (consolidated) expense, excluding the impact of facility amortization, in a given year.
0.014% • Reduce non-value added activity and waste through daily continuous improvement system.
• Implement hospital improvement plan initiatives (41 initiatives).
Methods to measure value to the health system will be identified at the unit and corporate level.
Value = Quality/Cost To be determined.
• Methods to measure value to the health system will be explored at the corporate level as well as at the unit/department level.
The objectives, targets, and change improvement initiatives are shown in detail in Part B of this document.
St. Mary’s General Hospital 6 911 Queen’s Blvd. Kitchener, ON N2M 1B2
Some of the resources that have been dedicated to help drive the performance improvement process include:
• Development of a performance management/improvement team comprised of two facilitators.
• Implementation of a Lean Leadership Development program for formal and informal leaders in the organization.
• Awareness level training for all front line staff.
• Dedicated resources to replace staff while participating in improvement projects. • Purchase of a positive patient identification and bedside labeling system for obtaining
lab specimens.
• Increase in infection control staffing level of one full time equivalent. • Implementation of a new flow coordinator role to assist with patient flow from the ER to
inpatient units. 3. How the plan aligns with the other planning processes This quality improvement plan links with other planning initiatives within and external to St. Mary’s. Some examples of documents that are linked with this plan include the Hospital Services Accountability Agreement , Accreditation Canada Required Organization Practices, and St. Mary’s strategic directions and goals (which are aligned with the Waterloo Wellington Local Health Integration Network plans/priorities). Many of the initiatives that are part of the QIP involve working with external partners such as CCAC, other acute care hospitals, and other community agencies. Our quality improvement framework is supported by a Board Quality Committee, our Board of Trustees, an operational Patient Safety and Quality Monitoring Committee, and program/unit specific Quality Utilization and Risk Committees. A Quality Report and Corporate Balanced Scorecard are reviewed with the Board of Trustees and board Quality Committee quarterly. In addition, all departments/programs have a scorecard with indicators that are aligned with organizational and quality improvement priorities. All units/programs present on progress in achieving unit goals and improvement initiatives to the board Quality Committee annually. The annual progress reports are narrated presentations and are posted on St. Mary’s General Hospital’s web site (available to public). These presentations are also shared with the hospital management group. We share our progress in achieving our strategic goals with staff quarterly through town halls and through written communication. In addition, all departments have a visual display board to share their unit goals and metrics, which are aligned with organization goals. Daily unit huddles take place at visual display boards. A wall will be put up in our lobby to visually display our progress in achieving our organization strategic goals for 2012/13. 4. Challenges, risks and mitigation strategies The corporate risks that are relevant to St. Mary’s achieving the objectives in this QIP include:

St. Mary’s General Hospital 7 911 Queen’s Blvd. Kitchener, ON N2M 1B2
• An increase in the number of patients that have to be isolated for infection control purposes.
• Funding gaps. • Non-renovated inpatient areas of our 1960’s building lack space lending to
overcrowding of patients, compromising infection control and accessibility.
• The Sandoz medication shortage and impact on practice changes and Pharmacy human resources.
One of our goals is to reduce adverse events including hospital acquired infections by 25%. We plan to do this through initiatives described in Part B of this document. St. Mary’s plans to address limitations of non-renovated 1960’s inpatient care areas through submission of a master plan to the MOHLTC- capital branch for approval. We are currently using Lean principles/methodologies as part of our continuous improvement framework to increase the value added activity to maximize the quality of care we provide for our patients. We will implement our hospital improvement plan to balance our budget for 2012/13. We will also continue to benchmark ourselves against other best practice organizations to find opportunities to improve value to the health care system.
Part B: Our Improvement Targets and Initiatives
Please refer to Part B (next page).

St. Mary’s General Hospital 8 911 Queen’s Blvd. Kitchener, ON N2M 1B2
PART B: Improvement Targets and Initiatives 2012/13
Please do not edit or modify provided text in Columns A, B & C
AIM MEASURE CHANGE
Quality dimension Objective Measure/Indicator
Current
performance
Target for
2012/13 Target justification
Priority
level Planned improvement initiatives (Change Ideas) Methods and process measures
Goal for change ideas
(2012/13) Comments
Safety
Reduce incidence of Ventilator
Associated Pneumonia (VAP)
VAP rate per 1,000 ventilator days: the total number of newly diagnosed VAP cases in the ICU after
at least 48 hours of mechanical ventilation, divided by the number of ventilator days in that
reporting period, multiplied by 1,000 - Average for Jan-Dec. 2011, consistent with publicly reportable
0.36 0 Ideal Target 2 1) Continue safer healthcare now VAP prevention
strategies.
1) Emphasize hand hygiene in senior team and manager
staff rounds.
Question regarding hand hygiene
included in senior team rounding
guideline template.
Discussion regarding hand
hygiene occur with each staff
member during rounds 80% of
the time.2) Increase visibility of IPAC team. Increase staffing by 1
FTE.
Use of alcohol hand gel at unit
and corporate level.
Increase in usage of alcohol
hand gel of ≥ 5%
3) Emphasize hand hygiene in daily staff huddles. Observations by senior team
during huddles- include in
standard work/staff rounds
template.
% of huddle whereby hand
hygiene results posted.
4) Continue audits and share results with staff
immediately as part of audit process; share results
monthly by unit across hospital as part of monthly
huddle review.
Hand hygiene results are posted
on huddle boards monthly by unit
and includes results across
organization. Discussion
regarding results included in
monthly updates with staff.
100% of direct patient care
areas have hygiene results
posted on unit visual display
boards
5) Complete training of staff; 780 staff have been
trained, remainder of staff and physicians to be done.
Training of staff and physicians to
be completed.
90% of staff and physicians
completed training module.
6) Review and change point of care placement and type
of alcohol hand gel in ambulatory/outpatient care areas
(inpatient areas completed).
All outpatient areas to be
reviewed and changes
implemented.
Outpatient/ambulatory care
areas to be completed by
December 2012.
7) Reward/recognize hand hygiene compliance Develop reward/recognition
program by July 2012
Implement reward/recognition
program by September 2012
Reduce the number of adverse
events affecting patients by
25%, from 229 to 166 by end of
2012/13
Types of Adverse Events Included: Hospital Acquired Infections (MRSA, VRE, CDI, including
colonizations) plus medication incidents (severity level 2, 3, 4), plus Lab specimen labeling
errors/patient identification errors. Baseline is actual number for Jan. - Dec. 2011.
229 166 25% reduction 1
2) Train all housekeeping staff on new
protocol/procedure and perform regular cleaning audits
to measure compliance
100% of housekeeping staff
trained. Regular cleaning audits
performed.
Audits reflect compliance at
≥85%.
3) Increase visibility of IPAC team. Increase staffing by
1FTE
Time rounding on units with staff
reflects increase of 1 FTE.
Hand hygiene results and
reduction in HAI's meeting
target.
4)Implement pre-emptive isolation for MRSA on General
Medicine unit. "Bed" isolation until screen result is
back.
% of patients screened on
admission
% of patients in pre-emptive
isolation for results pending.
5) Implement chlorine based cleaning solutions for
C.Difficile on remainder of patient care areas (3E, 3W,
ICU/CCU/CVICU and outpatient areas).
Implementation complete by
December 2012
100% of inpatient and
outpatient areas with chlorine
based solutions in place for
C.Difficile. By Jan. 2013.
1) Summarize incident reports (2011/12) to determine
points in process that contribute to errors.
Summary to be completed by
April 3 2012.
Determine areas of priority
from incident reports by May 1
2012.2) Reduce errors in transcription of medication errors. Determine areas of opportunity
from incident reports and through
working group by June 1, 2012.
Develop and implement plan
for improvement by November
2012.
3. Lab Specimen labeling and patient identification errors: Q4 2010/11 to Q3 2011/12 48 24 50% reduction 1 Implement bedside positive patient ID and labeling for
lab specimen collection (ED).
Project plan and implementation
team established. Timeline for
completion -July 2012
≤ 1 specimen labelling error per
month (ER) from August 2012-
March 2013.
2. Medication Errors (severity level 2, 3, 4): Jan 2011-Dec. 2011 51
76.8
Reduce rates of deaths and
complications associated with
surgical care
60
1. Hospital Acquired Infections (MRSA, VRE, CDI, including colonizations): Jan.2011-Dec. 2011
0..41
0
Surgical Safety Checklist: number of times all three phases of the surgical safety checklist was
performed (‘briefing’, ‘time out’ and ‘debriefing’) divided by the total number of surgeries
performed, multiplied by 100 - Jan-Dec. 2011, consistent with publicly reportable patient safety data
Improve provider hand hygiene
compliance
1
25% reduction
Hand hygiene compliance before patient contact: The number of times that hand hygiene was
performed before initial patient contact divided by the number of observed hand hygiene
indications for before initial patient contact multiplied by 100 - Jan-Dec. 2011, consistent with
publicly reportable patient safety data
3
1
3
Best performance
Ultimate ideal target
is 100%. Current
target is to reach or
exceed 80%
100%
≥80
99.8%
St. Mary's General Hospital, 911 Queen's Blvd. Kitchener, Ontario N2M 1B2
Rate of central line blood stream infections per 1,000 central line days: total number of newly
diagnosed CLI cases in the ICU after at least 48 hours of being placed on a central line, divided by the
number of central line days in that reporting period, multiplied by 1,000 - Average for Jan-Dec. 2011,
consistent with publicly reportable patient safety data
Reduce clostridium difficile
associated diseases (CDI)
CDI rate per 1,000 patient days: Number of patients newly diagnosed with hospital-acquired CDI,
divided by the number of patient days in that month, multiplied by 1,000 - Average for Jan-Dec.
2011, consistent with publicly reportable patient safety data
0
National Benchmark
(CNISP)
Reduce rate of central line
blood stream infections
See adverse
events
below
≤ .77
See change ideas detailed below identified by type of adverse event.
15% reduction
1) Achieve hand hygiene compliance of ≥80%; see hand hygiene change ideas section above.
Best Performance
1121 ≤91
St. Mary’s General Hospital 9 911 Queen’s Blvd. Kitchener, ON N2M 1B2
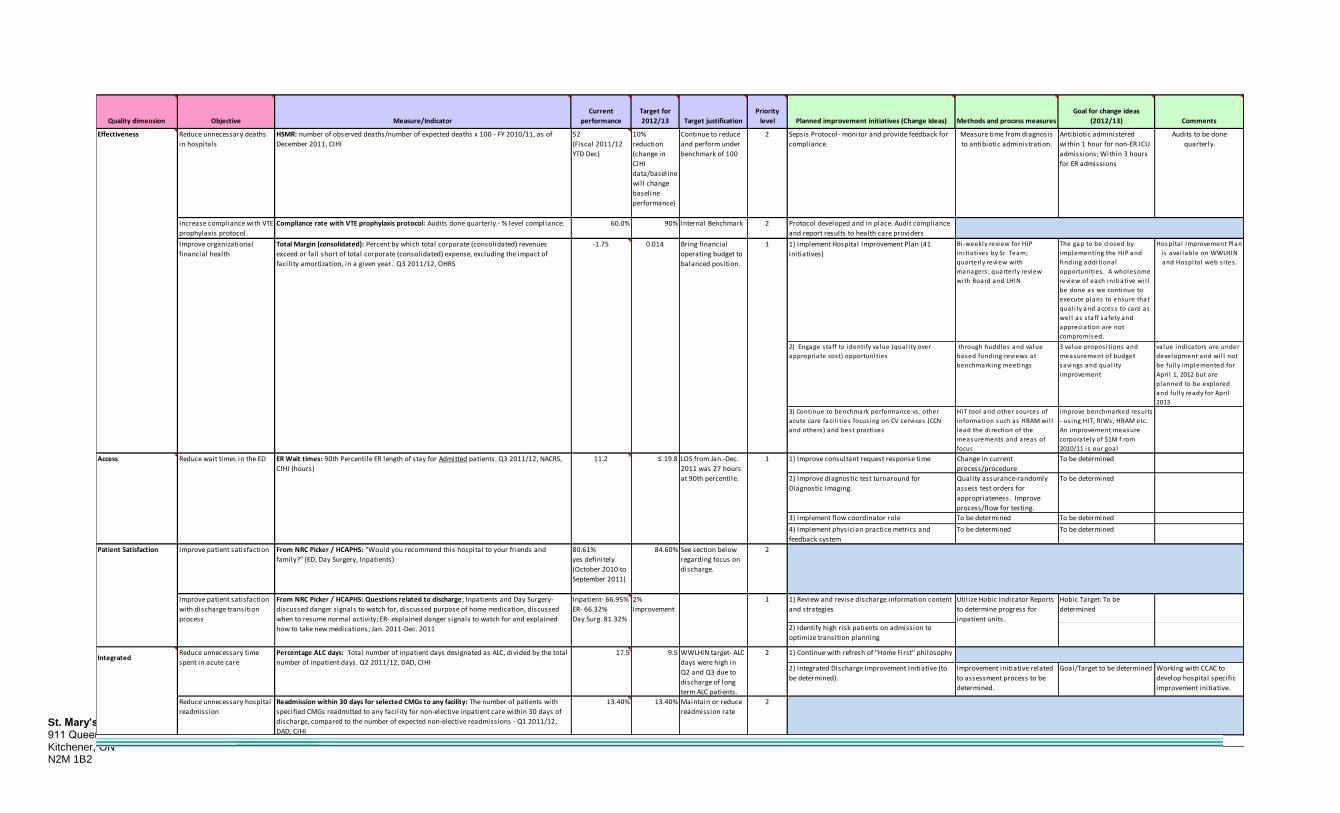
Quality dimension Objective Measure/Indicator
Current
performance
Target for
2012/13 Target justification
Priority
level Planned improvement initiatives (Change Ideas) Methods and process measures
Goal for change ideas
(2012/13) Comments
Effectiveness
Increase compliance with VTE
prophylaxis protocol.
Compliance rate with VTE prophylaxis protocol: Audits done quarterly.- % level compliance. 60.0% 90% Internal Benchmark 2 Protocol developed and in place. Audit compliance
and report results to health care providers
quarterly.1) Implement Hospital Improvement Plan (41
initiatives)
Bi-weekly review for HIP
ini tiatives by Sr. Team;
quarterly review with
managers ; quarterly review
with Board and LHIN
The gap to be closed by
implementing the HIP and
finding additional
opportunities . A wholesome
review of each ini tiative wi l l
be done as we continue to
execute plans to ensure that
qual i ty and access to care as
wel l as s taff safety and
appreciation are not
compromised.
Hospita l Improvement Plan
i s ava i lable on WWLHIN
and Hospita l web s i tes .
2) Engage s taff to identi fy va lue (qual i ty over
appropriate cost) opportunities
through huddles and va lue
based funding reviews at
benchmarking meetings
3 va lue propos i tions and
measurement of budget
savings and qual i ty
improvement
value indicators are under
development and wi l l not
be ful ly implemented for
Apri l 1, 2012 but are
planned to be explored
and ful ly ready for Apri l
2013
3) Continue to benchmark performance vs . other
acute care faci l i ties focus ing on CV services (CCN
and others ) and best practices
HIT tool and other sources of
information such as HBAM wi l l
lead the direction of the
measurements and areas of
focus
improve benchmarked results
- us ing HIT, RIWs, HBAM etc.
An improvement measure
corporately of $1M f rom
2010/11 is our goal
Access 1) Improve consultant request response time Change in current
process/procedure
To be determined
2) Improve diagnostic test turnaround for
Diagnostic Imaging.
Quality assurance-randomly
assess test orders for
appropriateness. Improve
process/flow for testing.
To be determined
3) Implement flow coordinator role To be determined To be determined
4) Implement physician practice metrics and
feedback system
To be determined To be determined
Improve patient satisfaction From NRC Picker / HCAPHS: "Would you recommend this hospital to your friends and
family?" (ED, Day Surgery, Inpatients)
80.61%
yes definitely
(October 2010 to
September 2011)
84.60% See section below
regarding focus on
discharge.
2
1) Review and revise discharge information content
and strategies
Hobic Target: To be
determined
2) Identify high risk patients on admission to
optimize transition planning
Integrated1) Continue with refresh of "Home First" philosophy
2) Integrated Discharge Improvement Initiative (to
be determined).
Improvement initiative related
to assessment process to be
determined.
Goal/Target to be determined Working with CCAC to
develop hospital specific
improvement initiative.
Patient Satisfaction
Improve patient satisfaction
with discharge transition
process
Inpatient- 66.95%
ER- 66.32%
Day Surg. 81.32%
2%
Improvement
2
0.014
2
9.517.5 WWLHIN target- ALC
days were high in
Q2 and Q3 due to
discharge of long
term ALC patients.
Maintain or reduce
readmission rate
13.40%
2
From NRC Picker / HCAPHS: Questions related to discharge; Inpatients and Day Surgery-
discussed danger signals to watch for, discussed purpose of home medication, discussed
when to resume normal activity; ER- explained danger signals to watch for and explained
how to take new medications; Jan. 2011-Dec. 2011
Utilize Hobic Indicator Reports
to determine progress for
inpatient units.
1
≤ 19.8 LOS from Jan.-Dec.
2011 was 27 hours
at 90th percentile.
1
13.40%
Continue to reduce
and perform under
benchmark of 100
10%
reduction
(change in
CIHI
data/baseline
will change
baseline
performance)
1
HSMR: number of observed deaths/number of expected deaths x 100 - FY 2010/11, as of
December 2011, CIHI
Bring financial
operating budget to
balanced position.
Reduce wait times in the ED ER Wait times: 90th Percentile ER length of stay for Admitted patients. Q3 2011/12, NACRS,
CIHI (hours)
Reduce unnecessary deaths
in hospitals
-1.75Total Margin (consolidated): Percent by which total corporate (consolidated) revenues
exceed or fall short of total corporate (consolidated) expense, excluding the impact of
facil ity amortization, in a given year. Q3 2011/12, OHRS
Improve organizational
financial health
Reduce unnecessary hospital
readmission
Readmission within 30 days for selected CMGs to any facility: The number of patients with
specified CMGs readmitted to any facil ity for non-elective inpatient care within 30 days of
discharge, compared to the number of expected non-elective readmissions - Q1 2011/12,
DAD, CIHI
Reduce unnecessary time
spent in acute care
Percentage ALC days: Total number of inpatient days designated as ALC, divided by the total
number of inpatient days. Q2 2011/12, DAD, CIHI
11.2
52
(Fiscal 2011/12
YTD Dec)
Audits to be done
quarterly.
Sepsis Protocol- monitor and provide feedback for
compliance.
Measure time from diagnosis
to antibiotic administration.
Antibiotic administered
within 1 hour for non-ER ICU
admissions; Within 3 hours
for ER admissions

St. Mary’s General Hospital 10 911 Queen’s Blvd. Kitchener, ON N2M 1B2
Part C: The Link to Performance-based Compensation of Our Executives
Manner in and extent to which compensation of our executives is tied to achievement of targets
The President, Chief of Staff, Vice Presidents, Director of Communications and Patient and Family Centred Care will have a portion of their compensation held back according to the achievement of the quality improvement plan as outlined below. A portion of the Chief of Staff’s existing bonus (five percent of existing salary) will be tied to achievement of the quality improvement plan as outlined in the chart below. For the President, five percent of existing salary will be held back and awarded according to achievement of quality performance indicators as outlined in the chart below. For the remainder of the executive team (see list of positions below), three percent of existing salary will be held back and awarded according to achievement of quality performance indicators as outlined in the chart below:
• Vice President, Medical Affairs
• Vice President, Quality and Performance Management • Vice President, Patient Services and Chief Nursing Executive • Vice President, Resource and Infrastructure and Chief Financial Officer • Director, Communications and Patient and Family Centred Care
The performance based compensation is linked to the following indicators:
• Quality and Safety:
• Reduction in adverse events (hospital acquired infections, medication incidents, and lab specimen labeling errors)
• Effectiveness: • Our budget will be balanced by the end of 2012/13.
• Access:
• Emergency department length of stay for admitted complex patients (CTAS I, II, III).
• Patient-centred:
• Patient satisfaction with discharge transition. Note: St. Mary’s does not provide additional salary bonuses to its Executives for achieving performance targets. Equal weighting will be given to these indicators. A specific performance allocation plan will be used to determine the magnitude of the performance allocation that will be awarded to each executive.

St. Mary’s General Hospital 11 911 Queen’s Blvd. Kitchener, ON N2M 1B2
The Performance allocation plan below will be used to determine the magnitude of the performance allocation that will be awarded to each executive.
Quality Dimension
Objective Outcome Measure/Indicator
Current Performance
Target for 2011/12
Weighting % of Available Incentive
100% 66% 33% 0% Safety Reduce the number of
adverse events affecting patients by 25%, from 229 to 166 by end of 2012/13
Types of Adverse Events Included: Hospital Acquired Infections (MRSA, VRE, CDI, including colonizations) plus medication incidents (severity level 2, 3, 4), plus Lab specimen labeling errors/patient identification errors. Baseline is actual number for Jan. - Dec. 2011.
229
166
25% ≤166 ≤187
≤208 ≥229
Effectiveness Improve organizational financial health
Total Margin (consolidated): Percent, by which total corporate (consolidated) revenues exceed or fall short of total corporate (consolidated) expense, excluding the impact of facility amortization, in a given year (current performanceQ3 2011/12, OHRS).
-0.175 .014 25% ≥ 0.014
≥ -0.050
≥ -0.113
≤ -0.175
Access Reduce wait times in the Emergency Department for admitted complex patients.
ER Wait times: 90th Percentile ER length of stay for Admitted patients. Q3 2011/12, NACRS, CIHI (hours)
11.2 hours Note: LOS from Jan.-Dec. 2011 was 27 hours at 90th percentile.
≤19.8 hours 25% ≤19.8 hours
≤22.3 hours
≤24.6 hours
≥27 hours
Patient-centred
Improve patient satisfaction with discharge transition process
From NRC Picker / HCAPHS: Questions related to discharge; Inpatients and Day Surgery-discussed danger signals to watch for, discussed purpose of home medication, discussed when to resume normal activity; ER- explained danger signals to watch for and explained how to take new medications; Jan. 2011-Dec. 2011
Inpatient- 66.95% ER- 66.32% Day Surgery. 81.32%
2% Improvement
25% ≥2% ≥1.32% ≥0.66% ≤0%

St. Mary’s General Hospital 12 911 Queen’s Blvd. Kitchener, ON N2M 1B2
Part D: Accountability Sign-off
I have reviewed and approved our hospital's Quality Improvement Plan and attest that our
organization fulfills the requirements of the Excellent Care for All Act. In particular, our
hospital's Quality Improvement Plan:
1. Was developed with consideration of data from the patient relations process, patient and employee/service provider surveys, and aggregated critical incident data
2. Contains annual performance improvement targets, and justification for these targets;
3. Describes the manner in and extent to which, executive compensation is tied to achievement of QIP targets; and
4. Was reviewed as part of the planning submission process and is aligned with the organization's operational planning processes and considers other organizational and provincial priorities.
Tom Hunter Board Chair
Christine Henhoeffer Quality Committee Chair
Don Shilton President