staghorn calculi
TRANSCRIPT
STAGHORN CALCULIGUIDE: DR. NITIN JOSHI
PRESENTED BY: DR. PARTH NATHWANIMGM MEDICAL COLLEGE , MUMBAI
INTRODUCTION Staghorn calculi are large , branched
stones that fill all or part of the renal pelvis & extend into majority of the calices.
Staghorn describes configuration rather than composition
Most staghorn consists of pure magnesium ammonium phosphate (struvite) or a mixture of calcium carbonate apatite.

Also referred as infection stones because of their strong association with UTI caused by urea splitting organisms.
If left untreated they may lead to renal failure, end stage renal disease & life threatening uro-sepsis.
PATHOGENESIS Infection stones are composed primarily of
magnesium ammonium phosphate hexahydrate (MgNH4PO4 • 6H2O) but may in addition contain calcium phosphate in the form of carbonate apatite (Ca10[PO4]6 • CO3).
A Swedish geologist discovered magnesium ammonium phosphate in guano and named it “struvite” after his mentor, naturalist H. C. G. von Struve
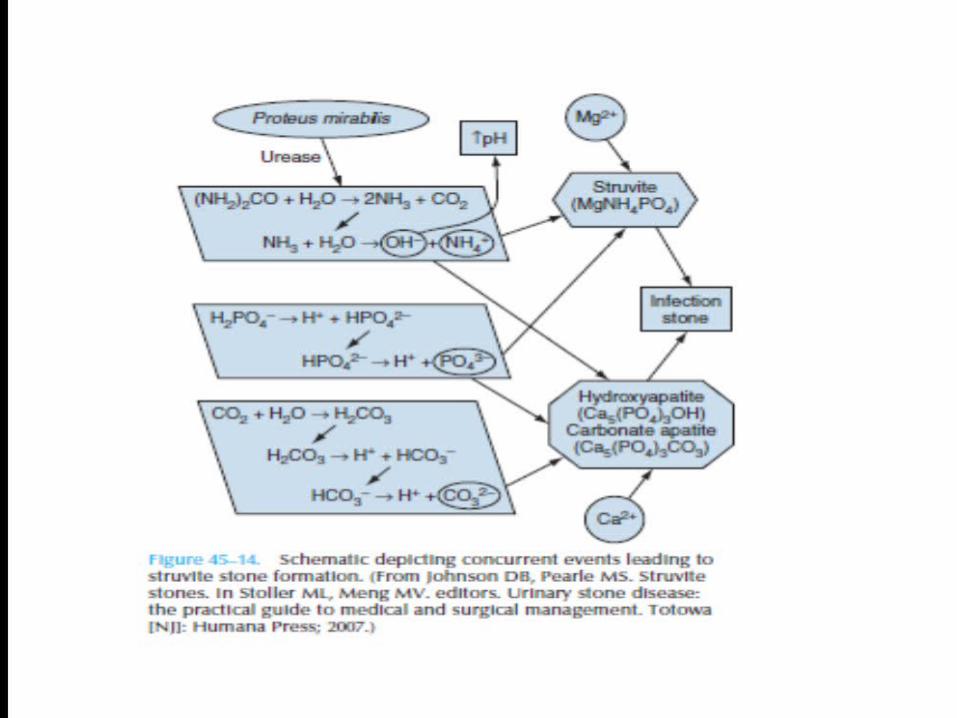
The process of urealysis provides an alkaline urinary environment and sufficient concentrations of carbonate and ammonia to induce the formation of infection stones.
Because urease is not present in sterile human urine, infection with urease-producing bacteria is a prerequisite for the formation of infection stones.
A cascade of chemical reactions generates the conditions conducive to the formation of infection stones.
Urinary urea, a constituent of normal urine, is first hydrolyzed to ammonia and carbon dioxide in the presence of bacterial urease:
(NH2)2CO + H2O 2NH➙ 3 + CO2
The alkaline urine that results from this reaction (pH 7.2 to 8.0) favors the formation of ammonium:
NH3 + H2O NH➙ 4+ + OH-
Under physiologic conditions, the alkaline urine would prevent further generation of further ammonium.
However, in the presence of urease, ammonia continues to be produced despite alkaline urine, further increasing urinary pH.
The alkaline environment also promotes the hydration of carbon dioxide to carbonic acid, which then dissociates into HCO-
3 and H+. Further dissociation of HCO3
- yields carbonate and two hydrogen ions:
CO2 + H2O H➙ 2CO3 H2CO3 H➙ + + HCO3
-
HCO3- H➙ + + CO3
2-
The dissociation of hydrogen phosphate under alkaline conditions provides phosphate, thereby completing the generating of constituent ions for infection stone formation:
H2PO4- H➙ + + HPO4
2- HPO4
2- H➙ + + PO43-
This chemical cascade, along with physiologic concentrations of magnesium, provides the constituents necessary for precipitation of struvite.
In addition, the concentrations of calcium, phosphate, and carbonate allow precipitation of carbonate apatite and hydroxyapatite, thereby comprising the components of infection stones.
Although infection stones are a direct result of persistent or recurrent infection with urease-producing bacteria, they may also be associated with or exacerbated by urinary obstruction or stasis.
As such, growth of infection stones can progress at a very rapid rate.
BACTERIOLOGY Although the family Enterobacteriaceae comprise the
majority of urease-producing pathogens, a variety of gram-positive and gram-negative bacteria and some yeasts and Mycoplasma species have the capacity to synthesize urease .
The most common urease-producing pathogens are Proteus, Klebsiella, Pseudomonas, and Staphylococcus species, with Proteus mirabilis the most common organism associated with infection stones.
Although Escherichia coli is a common cause of urinary tract infections, rare species of E. coli produce urease.
Bacteria may be involved in stone formation by damaging the mucosal layer of the urinary tract, resulting in both increased bacterial colonization and crystal adherence .
It has been proposed that ammonium, generated as a result of urealysis, may alter the glycosaminoglycan layer present on the surface of the transitional cell layer and significantly increase bacterial adherence to normal bladder mucosa, further exacerbating infection risk.
Another potential mechanism for increased stone formation in the presence of bacteria is the finding that particular bacteria, such as E. coli and Proteus, may alter the activity of urokinase and sialidase, whereas organisms not typically associated with infection stones do not .
This altered enzymatic activity may explain the frequent association of E. coli with stone formation despite lacking urease activity.

EPIDEMIOLOGY Infection stones comprise 5 to 15% of all stones . However, struvite/carbonate apatite was the most common
stone composition among a population of African American stone formers in Ohio, accounting for a third of stones in males and nearly half the females in this population.
Because infection stones occur most commonly in those prone to frequent urinary tract infections, struvite stones occur more often in women than men by a ratio of 2:1.
Other populations at risk of recurrent infection include the elderly , premature infants or infants born with congenital urinary tract malformation, diabetics, and those with urinary stasis as a result of urinary tract obstruction, urinary diversion, or neurologic disorders.
Spinal cord—injured patients are at particular risk for both infection and metabolic stones owing to neurogenic urinary tract dysfunction and hypercalciuria related to immobility.
Patients with a functionally complete cord transection are at highest risk of developing a staghorn calculus.
CLINICAL MANIFESTATIONS Asymptomatic Recurrent UTI Haematuria Vague abdominal pain or flank pain Dysuria Fever & urosepsis Pyonephrosis Renal failure Xanthogranulomatous pyelonephritis
INVESTIGATIONS CBC – chronic anaemia Urine analysis – alkaline ph >7 & frequently
magnesium ammonium phosphate crystals. Urine culture – specific organism Serum electrolytes & RFT – Renal failure Additional aspects of the metabolic evaluation of
urinary stones should be pursued because up to 50% of patients with infection-related stones have concomitant metabolic abnormalities.
Thus, a 24-hour urinary collection (for calcium, oxalate, uric acid, citrate, phosphate, uric acid, magnesium, sodium, total volume, and pH) can be done.
Indications for a Metabolic Stone Evaluation
Recurrent stone formers Strong family history of stones Intestinal disease (particularly chronic diarrhea) Pathologic skeletal fractures Osteoporosis History of urinary tract infection with calculi Personal history of gout Infirm health (unable to tolerate repeated stone
episodes) Solitary kidney Anatomic abnormalities Renal insufficiency Stones composed of cystine, uric acid, or struvite
X ray kub - The vast majority of staghorn calculi are radiopaque and appear as branching calcific densities overlying the renal outline and may mimic an excretory phase IVP. Lamination within the stone is common
Ultrasound kub - The collecting system is filled with a densely calcified mass, producing marked posterior acoustic shadowing.
Size of stone , involvement of calycies , hydronephrosis, parenchymal thickness & c-m differentiation , chronic pyelonephritis, pyonephrosis

IVP – pelvicalyceal anatomy , stone location & size and excretion of the dye.
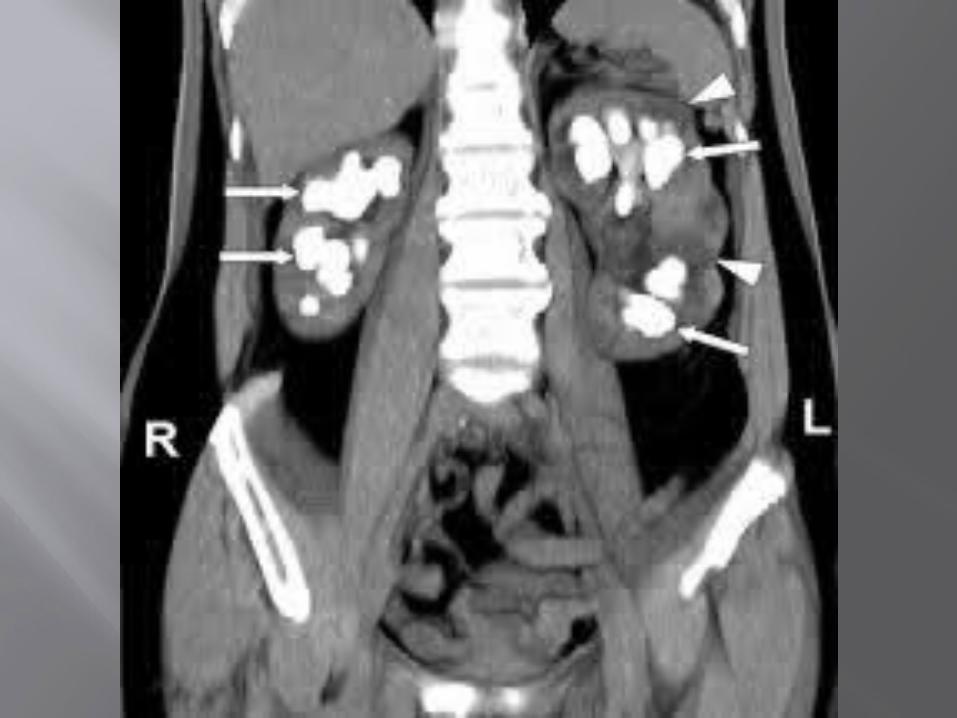
Ct scan – imaging study of choice. noncontrast CT scanning followed by
intravenous contrast CT scanning is obtained most often in the evaluation of urinary stones.
CT scans also display the adjacent structures and may aid in selecting the safest percutaneous tract to access the renal collecting system
Delineates better renal & p-c system anatomy , renal excretion of dye , surrounding structure, parenchymal thickness , hydronephrosis , HU value
Narrow, scarred infundibula indicate the need for percutaneous nephrolithotomy (PCN), while wide, large renal infundibula suggest that extracorporeal shockwave lithotripsy (SWL) might be adequate.
If the passageway between the calyces and renal pelvis is open and unrestricted, stone fragments produced during SWL are much more likely to pass.
Traditionally, staghorn calculi were defined as partial if the renal pelvic stone extended into at least 2 calyceal groups or complete if at least 80% of the collecting system was filled.
CT scanning with 3-dimensional reconstruction offers accurate stone volumes, but the added radiographic analysis is costly, time consuming, and is nor readily available.
Renal scintgraphy – to assess differential renal function
To be done in patients with chronic pyelonephritis & obstruction .
Chemical analysis of stone & stone culture.
TREATMENT Primarily managed surgically by complete
stone clearance as the goal of treatment. Patients who are poor surgical candidates
dissolution therapy may be useful Several treatment options exist for this
patients like PCNL , ESWL , ureteroscopy , open surgery and combination therapy.
PCNL is usually the first line treatment for most patients with staghorn calculi
DISSOLUTION THERAPY Chemolysis or dissolution therapy has been
around for 70 years Suby & albright developed suby’s solution G
which consists of citric acid , magnesium oxide & sodium carbonate.
Magnesium decreased mucosal irritablity & enhanced stone dissolution by undergoing ion exchange with calcium.
Using a nephrostomy tube or ureteric cathater this solution is instilled to dissolve struvite stone
Hemiacidrin a chemolytic agent is similar in composition to suby’s solution G but it also contains D-gluconic acid.
Acids provide hydrogen ions & citrate to form soluble complexes with calcium & phosphate components of stone.
But there is risk of sepsis , electrolyte abnormality and even death with these therapy so FDA withdrew approval for the use of these agent
Initially it was also combined with ESWL with success rate of upto 60% for stone clearance but with increased cost, hospital stay & risk of complications it has a very limited role
It is ineffective as a monotherapy to treat staghorn calculus but can be useful in treating residual stones.
ESWL Most commonly used Not used usually as monotherapy as
stone free rate is is low (18-67 %) Eswl for staghorn calculi can cause
potential morbidity including steinstrasse, renal colic , sepsis & perinephric hematoma.
Usually used in combination with PCNL or as “sandwich” therapy.
ESWL monotherapy for staghorn calculus is more suited for paediatric population which may be due to relatively small stone burden , better shock wave transmission & more compliant ureter for transmission of stone
Complications of ESWL include fever , renal obstruction caused by steinstrasse , multiple procedure & painfull haematuria.
URETEROSCOPY Flexible ureteroscopy has not traditionally
been used in treatment of staghorn stone However with development in technology
and introduction of holmium:YAG lasers & nitinol baskets , this approach has gained popularity in selected patients as primary or adjuvant treatment.
Multiple tracts may be required sometimes in PCNL for complete stone clearance which increases the operative morbidity & post operative pain & discomfort.
However flexible ureteroscope can be used to prevent multiple puncture during PCNL
To date there are no published data for flexible ureteroscopy as a monotherapy for staghorn calculus
But it is a good modality if used as a combination therapy with PCNL.
ANATROPHIC NEPHROLITHOTOMY(AN)
Indications for AN have continuously narrowed over past decade with emergence of PCNL & ESWL
AN is done for complete or near complete staghorn calculus & where PCNL & ESWL are difficult & complex
Stone free rate was of 89 to 100 % Avearge hospital stay is of 6-7 days but
less costly than minimal invasive procedures
Classically, the boundary of segmental renal blood supply was identified by clamping the posterior arterial branch & injecting methylene blue.
The kidney is than incised along the demarcated avascular plane between anterior and posterior blood supply
Following stone removal , infundibular reconstruction & formal closure of the entire collecting system is performed.
Smith & boyce modified this technique in which parenchymal incision was made 1 to 2 cm posterior to the lateral kidney surface without segmental vascular dissection , the collecting system was not reconstructed , & closure was accomplished only with a posterior renal capsular flap.
Open surgery (AN) is an appropriate treatment alternative in unusual situations when a struvite staghorn calculus is not expected to be removed by a reasonable number of PCNL or ESWL procedure.
Treatment with PCNL with or without ESWL is shown to be less successful when stone surface area is >2500mm2 , anatomical abnormalities , infundibular stenosis & morbid obesity.
PCNL Based on its superior efficacy & low
morbidity , PCNL have now emerged as the treatment of choice
PCNL is less expensive , decreased need for blood transfusion , requires shorter hospital stay & allows a more rapid return to work.
Stone free rates are 70 to 93 % when used as a monotherapy
This variation is because of different stone burden and different technique.
To further improve outcomes of PCNL several technical refinements have been advocated like multiple percutaneous access & use of flexible nephroscopy.
Flexible nephroscope facilitate stone clearance because the sharp angles of p-c system are difficult to maneuver with rigid nephroscopy
Multiple tracts are also made to achieve complete stone free clearance rates but it is associated with complications like blood transfusion , fever , septic shock , pseudoaneurysm , hydrothorax, post operative discomfort, increased morbidity & hospital stay.
Residual stones following PCNL are cleared by second look or two stage PCNL as their clearance is necessary to prevent recurrent UTI.
In summary , PCNL is safe , effective & minimal invasive approach for management of staghorn calculi.
Procedure of choice due to higher stone free rates and less complication rates.
COMBINATION THERAPY It refers to the use of multiple endo-
urological techniques for treatment of staghorn calculi
The most commonly used therapy is “sandwich therapy “.
Classically described by streem & colleagues it consists of PCNL- ESWL – PCNL
It is less commonly used now a days because of inferior results as compared to PCNL used as a monotherapy.
PREVENTION Following surgical therapy medical
management may be useful in preventing stone recurrence
Strategies include dietary modifications & oral therapies that acidify urine , inhibit ammonia production & sterilize the urine .
DIETARY MODIFICATIONS In 1945 , shorr proposed a regimen of low
phosphorous , low calcium diet in conjunction to oral estrogen & aluminium hydroxide gel.
Oral estrogen acts to decrease calcium excretion by their effect on bone mineralization
Aluminium hydroxide gel binds phosphate in the gut and is excreted entirely in the stool as aluminium phospahte
The net result of these manipulation is less substrate excretion in urine to bind surrounding lithogenic molecule
Aluminium hydroxide can cause constipation , anorexia , lethargy , bone pain & hypercalciuria.
These regimens are usually not recommended due to these side effects
Avoidance of foods and vitamins supplements high in phosphorus & magnesium is recommended
Our goal is reduction in urinary phosphate , magnesium & ammonia.
URINARY ACIDIFICATION Solubility is highly dependent on urinary pH &
crystallization which occurs only between 7.2 & 8.4
In vitro studies have shown that acidification of struvite stones to pH less than 6.5 increases the solubility of stones and can be used to dissolve stone
Ascorbic acid promotes urinary alkalinization through increase citrate production.
A single dose of L-methionine 1500mg caused a reduction in urinary pH values to 6.0 to 6.2
Oral dose of L-methionine is metabolized to sulphate and H+ ions via L-cysteine
UREASE INHIBITORS These are oral agents that inhibit stone growth
by blocking the cascade of events that lead to supersaturation of struvite precursors
Acetohydroxamic acid is the only inhibitor that is FDA approved
It works synergistically with several antibiotics and thereby helps in sterilization of urine
It has got high renal clearance & ability to penetrate bacterial cell wall
It decreased urine alkalinity & ammonia levels Contraindicated in patients with creatinine > 2.5
ANTIBIOTICS Presence of persistent infection has been
demonstrated to increase the risk of stone recurrence
Thus eradication of infection & elimination of the source of infection is a critical step in stone prevention
Post surgery chances of recurrence rate is 31% and 56% chance of resistant UTI so culture specific antibiotics should be given
Antibiotics may suppress bacteriuria, but in presence of stone fragments their effectiveness in eliminating infection is compromised.
AUA GUIDELINES FOR MANAGEMENT OF
STAGHORN CALCULUS
Standards 1. As a standard, a newly diagnosed struvite
staghorn calculus represents an indication for active treatment intervention.
Although this recommendation was not formally subjected to data abstracting and statistical methods, the panel strongly believes based on expert opinion that a policy of watchful waiting and observation is not in the best interest of the standard patient with struvite staghorn calculi.
2. As a standard, a patient with a newly diagnosed struvite staghorn calculus must be informed about the four accepted active treatment modalities, including the relative benefits and risks associated with each of these treatments.

Guidelines 1. As a guideline, percutaneous stone removal,
followed by shock-wave lithotripsy and/or repeat percutaneous procedures as warranted, should be utilized for most standard patients with struvite staghorn calculi, with percutaneous lithotripsy being the first part of the combination therapy.
2. As a guideline, shock-wave lithotripsy monotherapy should not be used for most standard patients as a first-line treatment choice.
3. As a guideline, open surgery (nephrolithotomy by any method) should not be used for most standard patients as a first-line treatment choice.
Options 1. As options, shock-wave lithotripsy monotherapy
and percutaneous lithotripsy monotherapy are equally effective treatment choices for small-volume struvite staghorn calculi in collecting systems which are of normal or near normal anatomy.
2. As an option, open surgery is an appropriate treatment alternative in unusual situations where a staghorn calculus is not expected to be removable by a reasonable number of percutaneous lithotripsy and/or shock-wave lithotripsy procedures
3. As an option for a patient with a poorly functioning, stone-bearing kidney, nephrectomy is a reasonable treatment alternative.
THANK YOU