stakeholder scoping 05 nov 14 insight version
TRANSCRIPT
LONG TERM CONDITIONS ACROSS THE LIFECOURSE
Stakeholder Scoping Workshop5th November 2014

Welcome
Agenda for this afternoon
1.30 pm Welcome & Background2.00 pm Topic 1: Key Conditions2.45 pm Topic 2: Cross cutting themes3.20 pm Refreshments break 3.30 pm Topic 3: Understanding local needs4.15 pm Wrap up4.30 pm Finish
Key note address
Dr Arnold Fertig CCG Clinical Lead Older People Services
Cambridgeshire & Peterborough Clinical Commissioning Group
Long Term Conditions JSNA Workshop
• Disease and Demographic Challenges in 1948 completely different from 2014
• Yet has the Health & Care System kept up?• People’s Expectations – enormous change• Whose problem is it?• The end of ageism & unintended
consequences• Workforce needs
Long Term Conditions (LTC) Overview
• Conditions for which there is no cure• 30% Population• 58% for those aged 60 or over• 4% pop. - care needs, in 15 yrs – 6%• 50% GP appts, 64% OP appts, 70% IP bed• 70% of expenditure Health & Care Budget
Major Inequalities
• Frequency (60% differential) and severity (30%)
• Age of onset – 10-15 year differential• Affects housing, education, relationships, work• Over 1% pop. - dementia, expected to double
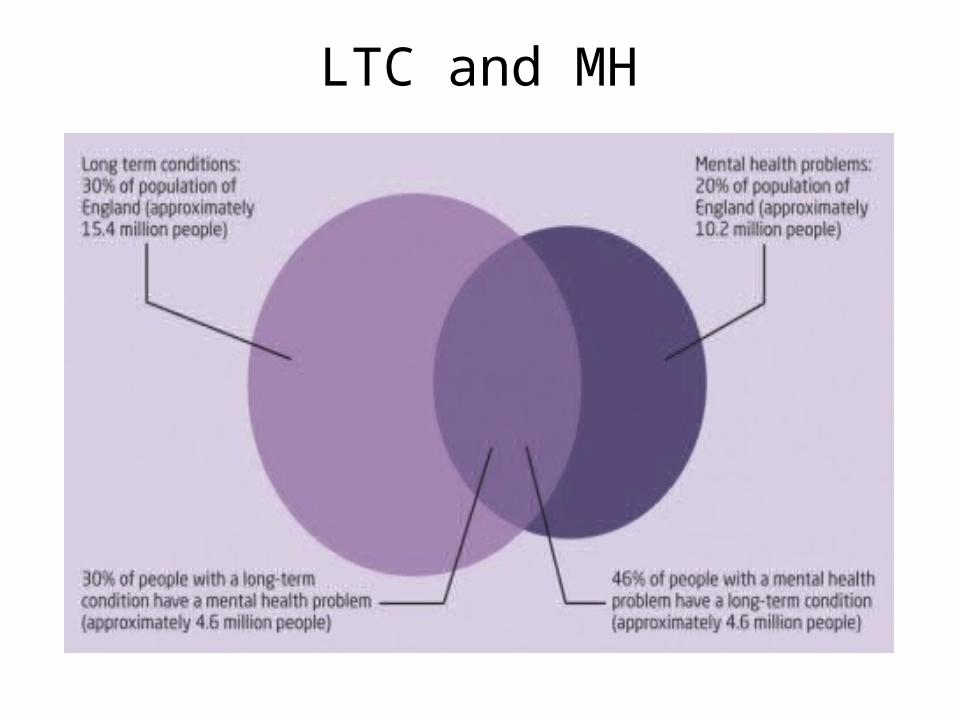
in 15 yrs – most increase cost will be care• 30% people with LTC have MH problems
Prevalence
• 3% pop. disabled by neurological condition• Up to 10% of admissions neurological• 13% of people with an LTC have a
musculoskeletal (msk) condition• Chronic msk to double by 2030• COPD 2% pop, but 2% undiagnosed• Heart failure 2%• Diabetes 5%
OPACS Outcomes Framework mapped against Domain 2 of National Outcomes Framework
1.Better experience of care - Ensuring people feel supported to manage their LTC
2.Safe care
3.Well organised care
4.Keeping healthy - Enhancing the quality of life for people with LTC and carers , mental illness & dementia, Improving functional ability in people with LTC
5.Treatment during acute illness or injury - Reducing time spent in hospital by people with LTC
6.Recovering from illness or injury
7.End of life care
The Future – The Enablers
• People need to be helped to develop the skills to manage their own condition
• They need ownership of their care plan• Care needs to be much better coordinated and
integrated• Technology enabled care services• One record• Primary, secondary & tertiary prevention• Care much closer to patients
Background & Context
Dr Angelique Mavrodaris Consultant in Public Health Medicine
Older People’s Lead
Cambridgeshire County Council
Scene setting
• The management and care of people with long term conditions - one of the most fundamental health and social care challenges
• Health and Wellbeing Strategy 2012-2017• Priority 2 - Support older people to be independent,
safe and well:Promote preventative interventions which reduce unnecessary hospital admissions for people with LTCs, enable them to live independently at home or in a community setting where appropriate and improve their health and wellbeing outcomes, e.g. through falls prevention, stroke and cardiac rehabilitation, supporting voluntary agencies and informal carers.
Purpose of this work
• Describe patterns of long term conditions (LTCs) across lifecourse
• Raise awareness of health needs & inequalities • Understand complexity of LTCs • Understand impact & interaction of mental health across
LTCs• Review suitability & accessibility of current services • Recommendations to improve health, independence &
access to care with a focus on cost-effective solutions• Engage & empower people with LTCs
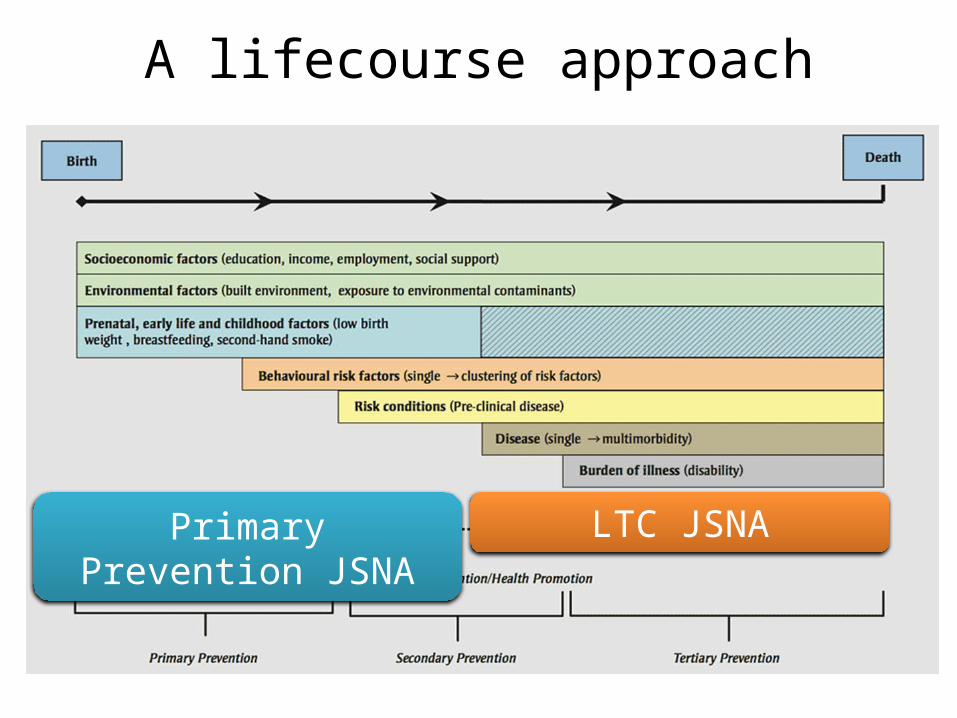
A lifecourse approach
Primary Prevention JSNA LTC JSNA
Vision
• Provide a clearer idea of what is needed• Evidence decisions to enable stakeholders to buy-in
to change• Enable more effective & economic configuration of
services• Deliver what people want & improve the personal experience of health & care• Identify best interventions & services
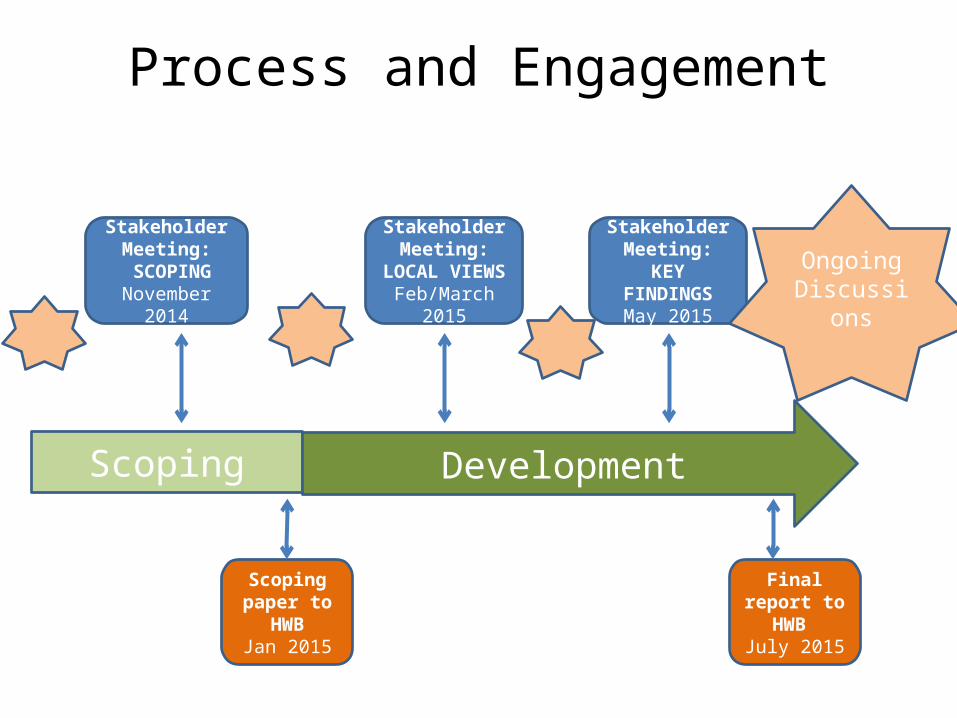
Process and Engagement
Scoping paper to
HWBJan 2015
Stakeholder Meeting: SCOPING
November 2014
Scoping
Final report to HWB July 2015
Development
Stakeholder Meeting:
LOCAL VIEWSFeb/March 2015
Stakeholder Meeting:
KEY FINDINGSMay 2015
Ongoing Discussions
Aims of today’s scoping workshop
Define the scope and shape of this work, by:• Gaining some consensus around key diseases and
conditions of interest– Having a joint rationale for which ones are selected
• Ensuring that we focus on cross cutting themes that are pertinent locally– Informative for service development– Aligning with health/social care priorities– Recognising that data are more limited
• Exploring ways of producing this work together
Gathering your views on scoping
• Understanding your perspectives & priorities
• Group discussions & activities• Flipcharts & notes• Evaluation forms – additional
comments• Hearing from your colleagues
TOPIC 1 – WHAT IS A LONG TERM CONDITION?
Topic 1 – What is a long term condition?
• How are LTCs defined?• Are the definitions appropriate?• What are the key conditions/diseases that
should be addressed within this work?
The definition of LTC varies
• “A health problem that can’t be cured but can be controlled by medication or other therapies” expanded to “the life of a person with a LTC is forever altered – there is no return to ‘normal’.” – Other definitions can include references to duration, quality of life, impact and
alternative terms such as chronic disease or long-standing illness
• Issues identified by House of Commons Health Committee (2014)– Represents a single disease model– Confusing and uncoordinated care for those with multiple conditions– Cancer not specifically included– Does not cover conditions which significantly impact quality of life
• Recommendation that the Department of Health revise its working definition of long-term condition to emphasise: – treating the person, not the condition – treating the person with multiple conditions as a whole
Source of data impacts LTC prevalence estimates
Variable prevalence estimates
Survey data• Used for prevalence estimates for
LTC• Self-reported LTC• Self-reported limiting LTC• Self-reported disease
prevalence• Some questions in national
surveys harmonised (ONS)• 2011 Census combines LTC and
limitation question
Medical record data• Used for information on individual
conditions or multimorbidity• Not often used to give an estimate
of overall LTC prevalence• Diagnosis-based• Definitions vary between studies
affecting prevalence estimates• Have to select specific conditions
to be included
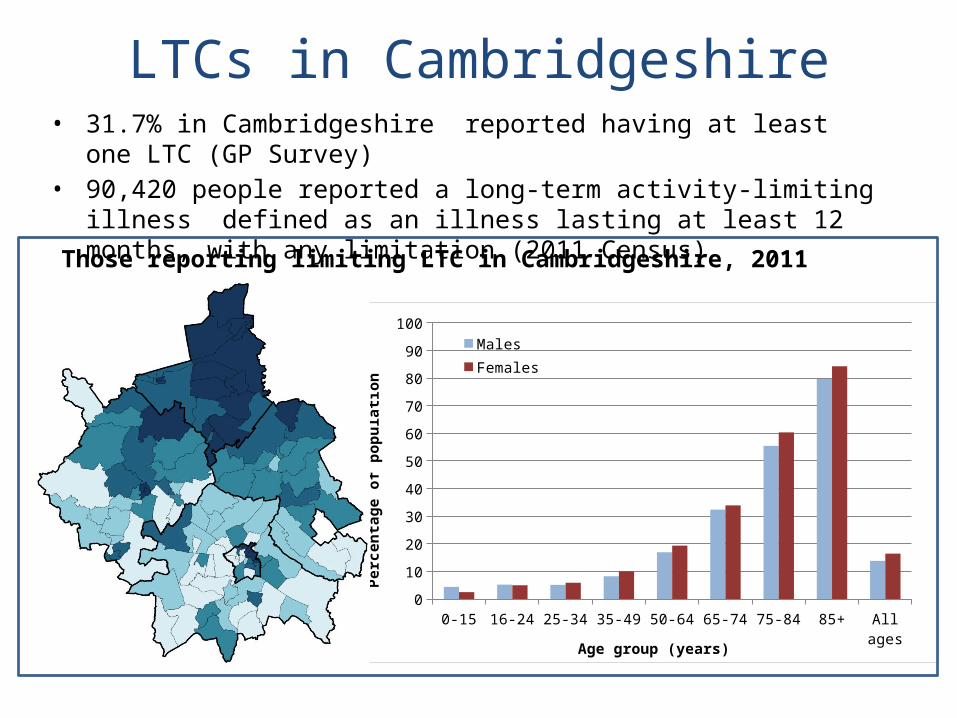
LTCs in Cambridgeshire• 31.7% in Cambridgeshire reported having at least one LTC (GP Survey)• 90,420 people reported a long-term activity-limiting illness defined as an
illness lasting at least 12 months, with any limitation (2011 Census)
0-15 16-24 25-34 35-49 50-64 65-74 75-84 85+ All ages0
10
20
30
40
50
60
70
80
90
100MalesFemales
Age group (years)
Perc
enta
ge o
f pop
ulati
on
Those reporting limiting LTC in Cambridgeshire, 2011 Census
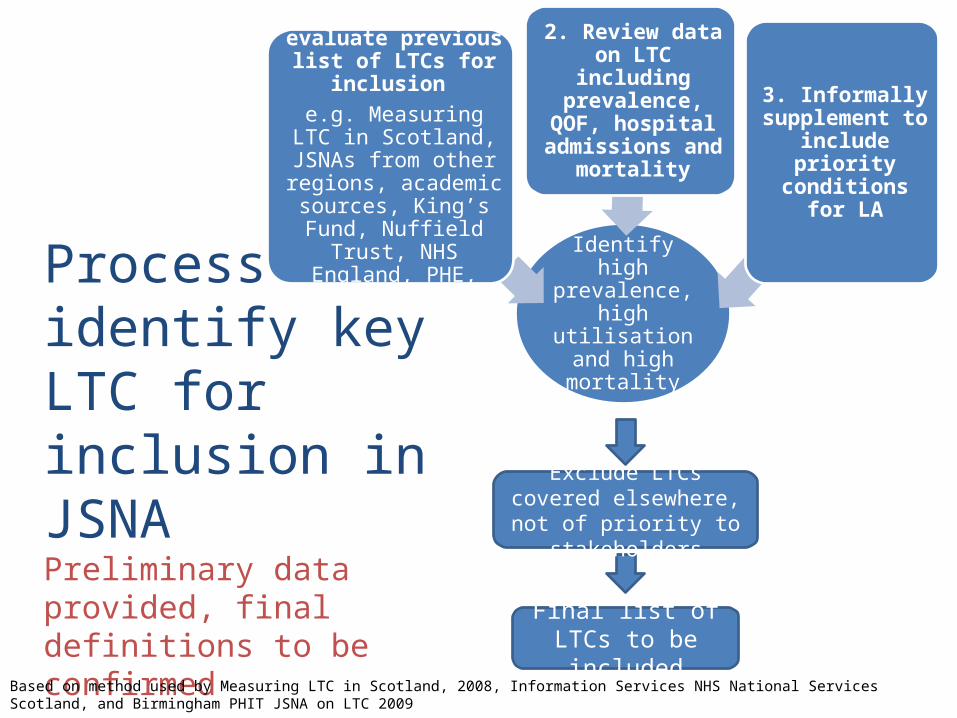
Process to identify key LTC for inclusion in JSNAPreliminary data provided, final definitions to be confirmed
Identify high prevalence, high
utilisation and high mortality
1. Search and evaluate previous list of LTCs for
inclusion e.g. Measuring LTC in Scotland, JSNAs from
other regions, academic sources, King’s Fund, Nuffield Trust, NHS England, PHE, NICE
2. Review data on LTC including prevalence,
QOF, hospital admissions and
mortality3. Informally
supplement to include priority
conditions for LA
Based on method used by Measuring LTC in Scotland, 2008, Information Services NHS National Services Scotland, and Birmingham PHIT JSNA on LTC 2009
Final list of LTCs to be included
Exclude LTCs covered elsewhere, not of priority
to stakeholders
Identifying key conditions
• What are the key conditions/diseases that should be addressed within this work?
• Information pack (1 per group) includes lists of LTCs, preliminary ranked data on prevalence, QOF, mortality and admissions
High
Low
• In your groups please identify long term conditions of interest
• Write on post it notes• Group with related conditions• Arrange on flipcharts in order
of priority
Comparing lists of ‘key conditions’
• How does your group’s list compare with other groups’ lists?– What are the reasons for this?
• How does your group’s list compare with the JSNA working group’s draft list…
?
Draft list of key conditions
• Arthritis• Cancer• Cardiovascular disease (CVD)• Chronic Obstructive Pulmonary Disease (COPD) • Diabetes• Frailty • Hypertension• Specific chronic kidney and digestive system
conditions
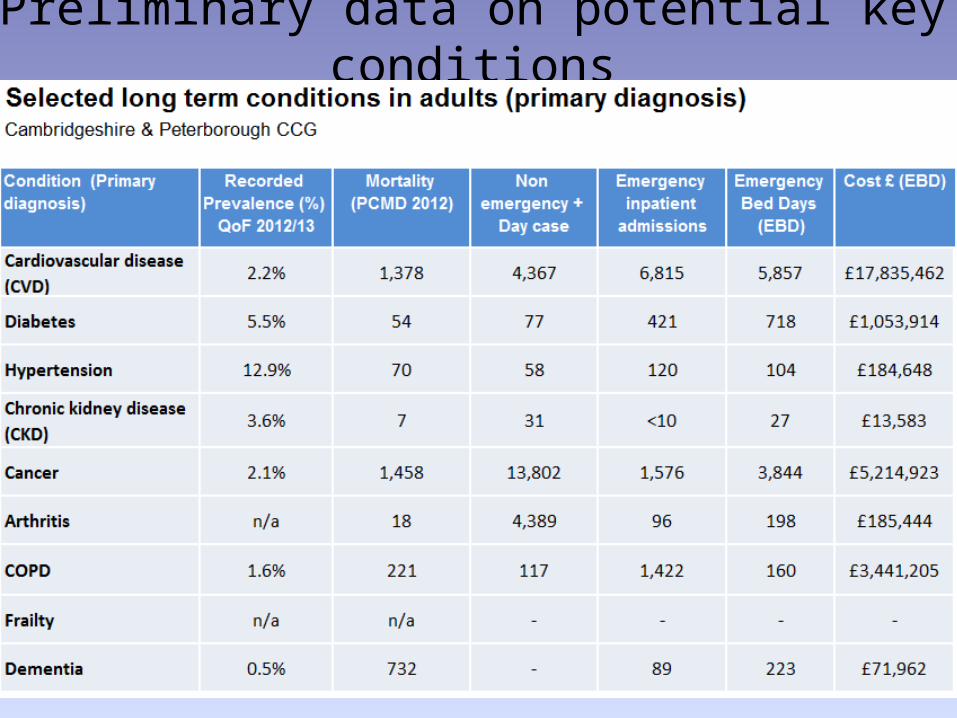
Preliminary data on potential key conditions
TOPIC 2 – CROSS CUTTING THEMES
Multimorbidity becoming more of a national priority
• “We have hospitals that are designed to cure specific conditions and they are full of old people with multimorbidity on polypharmacy” House of Commons Health Committee July 2014
• NICE: at present guidance only available on individual conditions. However multimorbidity guidance in development (due 2016). Scoping suggested indicators for a tailored approach– Taking a specified number of drugs – Limited life expectancy– Unplanned hospital admissions– Having falls– Needing social care– Being housebound
Multimorbidity definitions very variable
• Multimorbidity a relatively recent term and sometimes used interchangeably with comorbidity. Definitions vary.– Multimorbidity can be defined as the simultaneous presence of
multiple health conditions where no one condition is identified as an index condition
– Comorbidity, there is a specific index condition of interest
• Methodological issues– Varies as to which conditions are included and how are conditions
defined e.g. ICD, specified list, patient report– How many conditions are included e.g. some studies use >=2, some
>=3, or counts.
• Therefore there are variable prevalence estimates
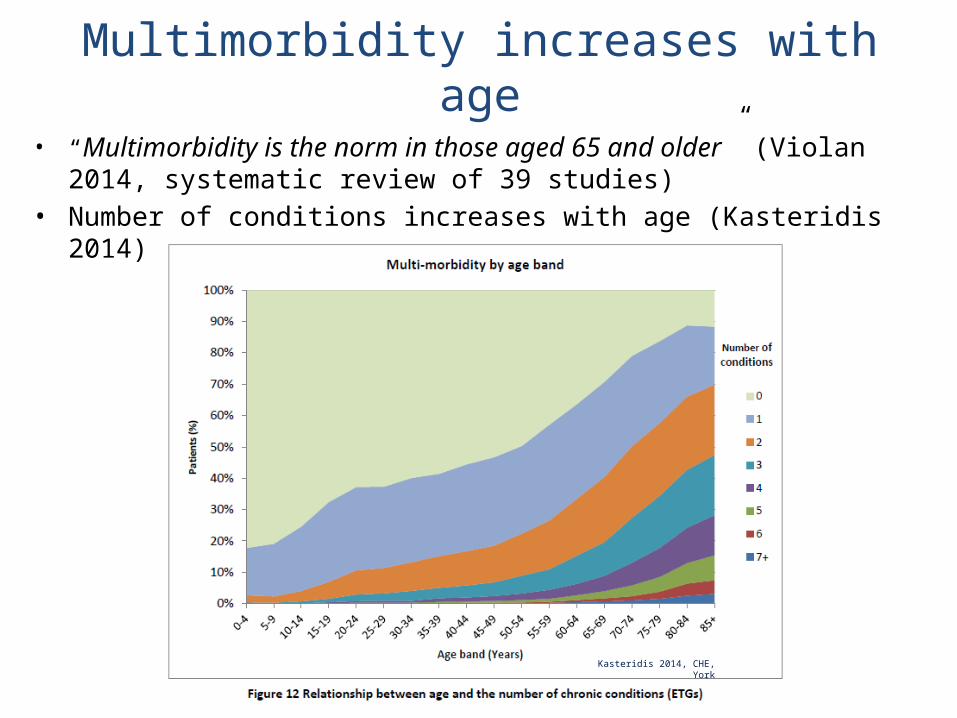
Multimorbidity increases with age• “Multimorbidity is the norm in those aged 65 and older” (Violan 2014,
systematic review of 39 studies)• Number of conditions increases with age (Kasteridis 2014)
Kasteridis 2014, CHE, York
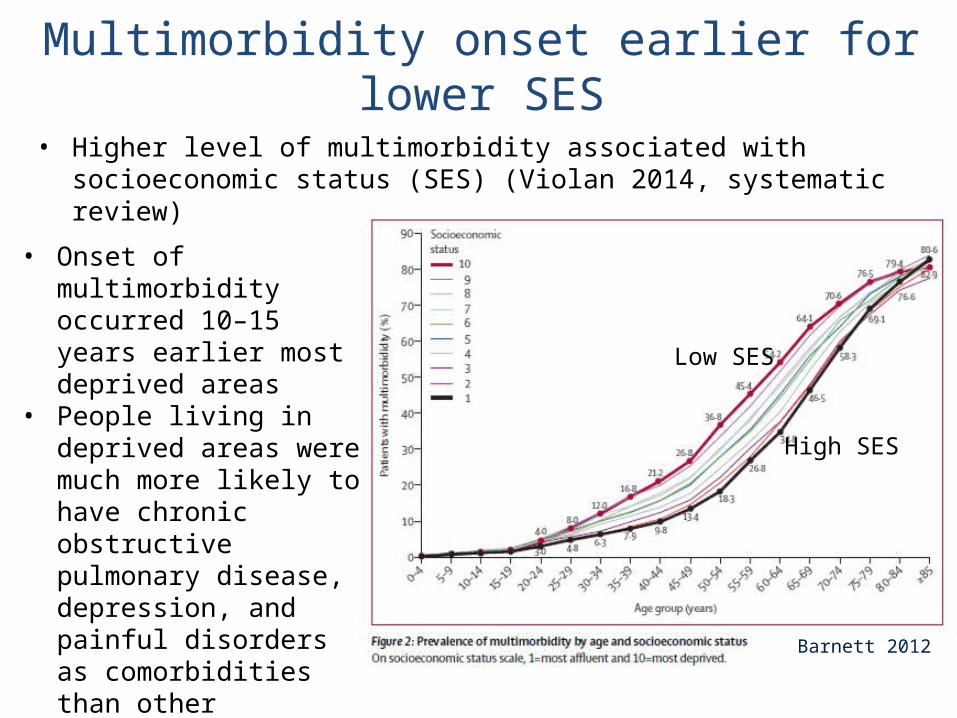
Multimorbidity onset earlier for lower SES• Higher level of multimorbidity associated with socioeconomic status (SES)
(Violan 2014, systematic review)
Barnett 2012
• Onset of multimorbidity occurred 10–15 years earlier most deprived areas
• People living in deprived areas were much more likely to have chronic obstructive pulmonary disease, depression, and painful disorders as comorbidities than other disorders (Barnett 2014)
High SES
Low SES
Disease clusters vary between studies
• Several systematic reviews of how different diseases group together or cluster (Violan 2014, Sinnige 2013, Prados Torres 2014)
• Variable results and hard to synthesise– different data types, classifications, diseases included and analysis methods
• Limited benefit in repeating for Cambridgeshire
• Some conditions more likely to be associated with multimorbidity (Kasteridis 2014)– 50% of those with asthma had no other condition– Only 10% of those with stroke or COPD have only this condition, 50% have
more than three conditions
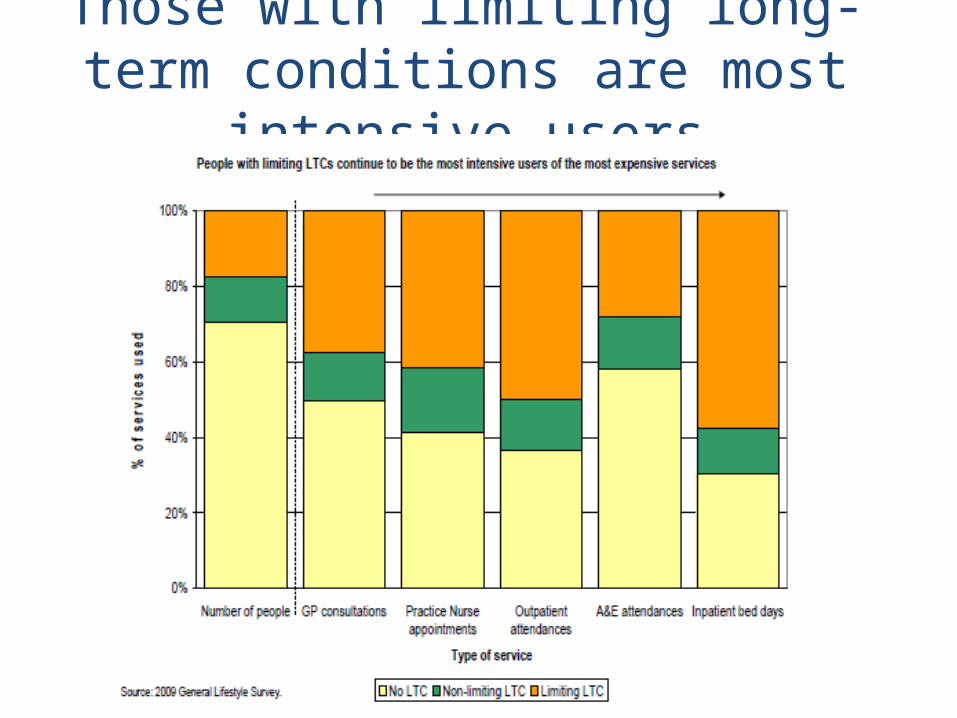
Those with limiting long-term conditions are most intensive users
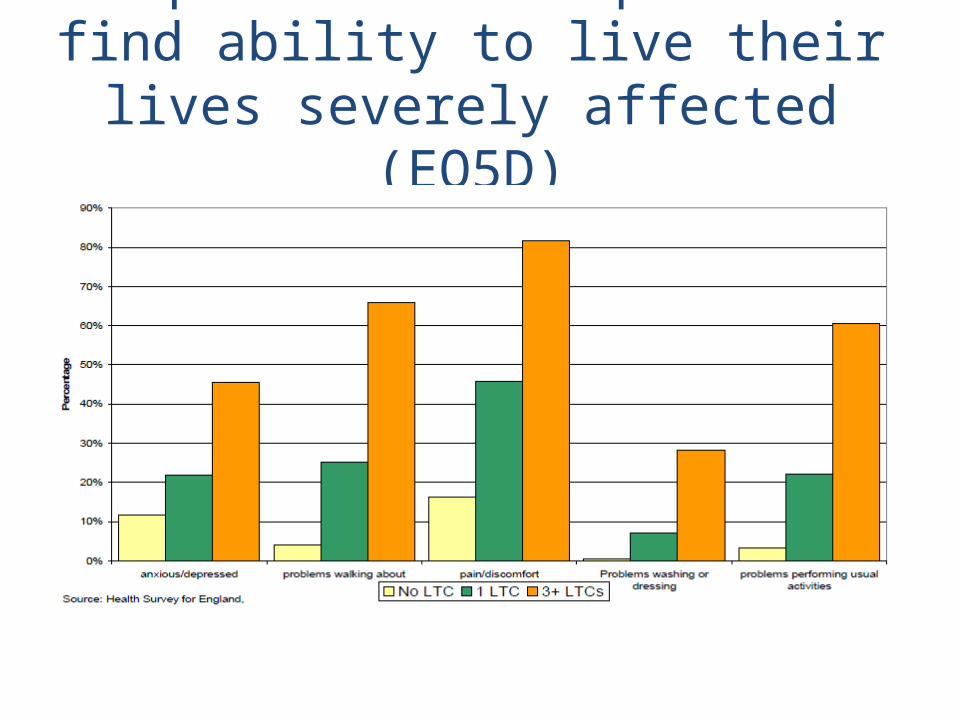
People with multiple LTCs find ability to live their lives severely affected (EQ5D)
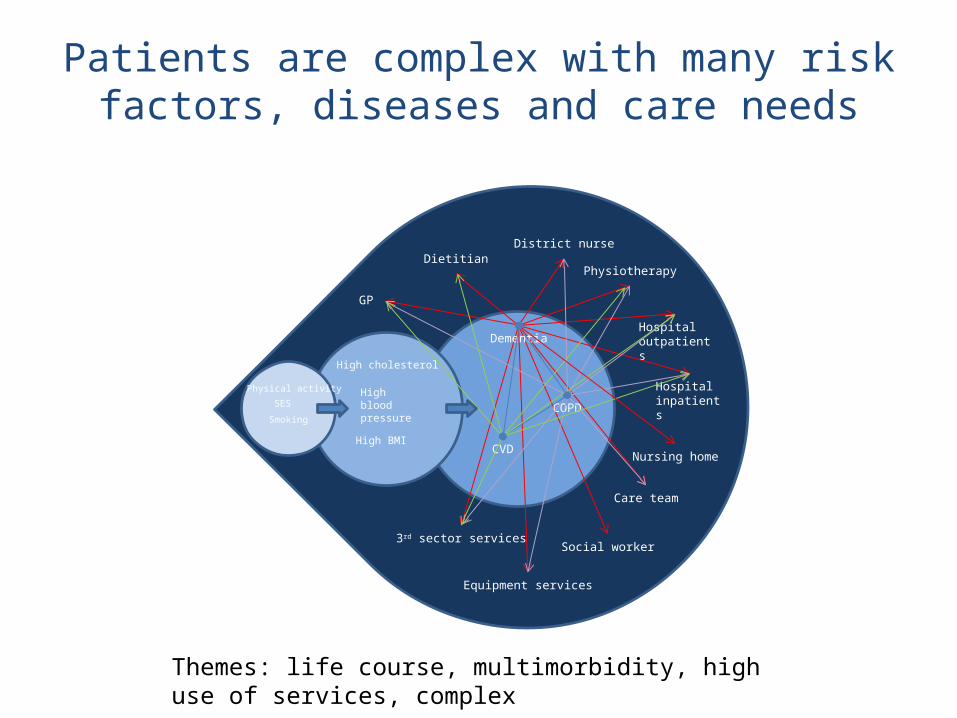
High blood pressure
High cholesterol
High BMI
Physical activity
Smoking
SES
GP
Social worker
Care team
District nurse
Physiotherapy
Hospital outpatients
Hospital inpatients
Nursing home
Equipment services
3rd sector services
Dietitian
Dementia
COPD
CVD
Patients are complex with many risk factors, diseases and care needs
Themes: life course, multimorbidity, high use of services, complex
Identifying cross cutting themes
As a group, list the common issues across long term conditions
Potential cross-cutting themes
Multimorbidity
Limiting
Polypharmacy
Frailty
Unplanned hospital admissionsHousebound
Limited life expectancy
Models of care
Dementia
Inequalities
Life course
Patient/carer satisfactionAdherence
Pain
Mental health
Disability
Prioritisation of cross cutting themes
What common issues across long term conditions should be prioritised for consideration in this work?
Please vote with your sticky spots in terms of which cross cutting themes you feel are most important
You can put all your spots on one piece of information or spread them out
Draft list of cross cutting themes• Multi-morbidity (people with LTCs more frequently have more
than one LTC, therefore at higher risk of adverse outcomes and implications for approaches to care)– Polypharmacy (impact on health and wellbeing)
• Limiting LTCs (to identify greatest need as this group are the most intensive users of expensive services with increased levels of dependence)
• Dementia and mental health (impact on other LTCs)• Inequalities (to ensure equality in access, health and wellbeing)• Risk factors across the life course (to achieve health gains and
reduction of the impact of LTCs)• Models of care (to identify opportunities for integrated and
person-centred approaches to care)
1.30 pm Welcome & Background2.00 pm Topic 1: Key Conditions2.45 pm Topic 2: Cross cutting themes3.20 pm Refreshments break 3.30 pm Topic 3: Understanding local needs4.15 pm Wrap up4.30 pm Finish
Break time…
TOPIC 3 – UNDERSTANDING LOCAL NEEDS
Understanding local needs
What is on your agenda in the months ahead?
April 2015
July 2015
Oct2015
April 2016
Jan2016
July 2016
Oct 2016
Jan 2017
Please plot your• Workstreams• Dates for business planning• Service changes and developments• Commissioning intentions
Understanding local needs: data availability
• What forms of data are available?• What kinds of questions can be answered?• What are the limitations of the data?
• Does the data address the questions you want answered?
• Are there any additional resources/data sets we should be looking at?
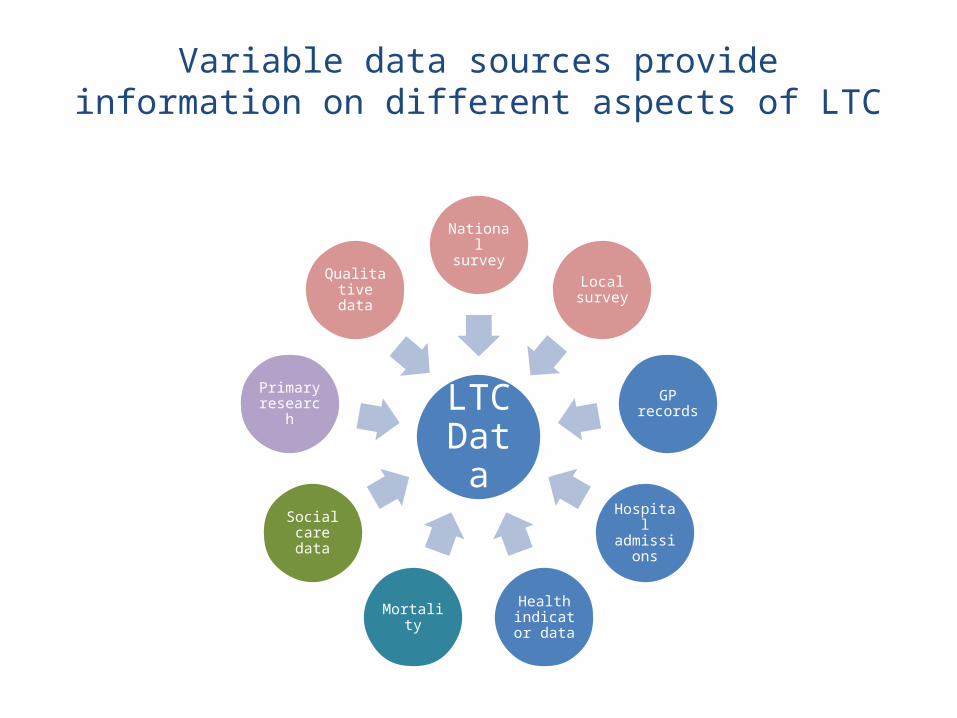
Variable data sources provide information on different aspects of LTC
LTC Data
National survey
Local survey
GP records
Hospital admissions
Health indicator
dataMortality
Social care data
Primary research
Qualitative data
Key conditions/diseases
• Traditional viewpoint• Lots of information on each individual condition• Broad data types available: survey data, GP data,
hospital data, QOF, mortality etc– Provide information on condition-based prevalence,
admissions, costs, quality of life, activity limitation, mortality
• Able to compare nationally• Definitions will vary between types of data leading
to variable estimates
LTC Data
National survey
Local survey
GP records
Hospital admissions
Health indicator
dataMortality
Primary research
Qualitative data
Data about multimorbidity• Data availability mixed
– Prevalence based on self-reported or medical record data of selected conditions
– Definitions and conditions selected will impact estimates• Qualitative data from health care practitioners, patients and carers
provides key information on issues and barriers • Limited national guidance on care pathways and therefore need to
understand local approach• Individual studies informative and can possibly be extrapolated to
Cambridgeshire – South Somerset Symphony Project combined anonymised individual level
data including primary, community, acute, mental health and social care. Data includes activity, cost, clinical condition, age, sex, socioeconomic indicators, ward
– Data analyses assessed impact of clusters of LTCs, multiple LTCs on costs
LTC Data
National survey
Local survey
GP records
Hospital admissions
Health indicator
dataMortality
Primary research
Qualitative data
Data about limiting LTCsLTC
Data
National survey
Local survey
GP records
Hospital admissions
Health indicator
dataMortality
Social care
Primary research
Qualitative data
LTC Data
National survey
Local survey
GP records
Hospital admissions
Health indicator
dataMortality
Social care
Primary research
Qualitative data
• Reliant mainly on survey data as very difficult to define in medical record data– Census data provides information from 1 question– National survey data has been harmonised and
provides self-reported data on type of condition and utilisation of healthcare data
– GP survey provides local detail but there is a poor response rate
• Social care data will provide information on social services used by those with limitations
Discussion: data availability for local needs
What data and intelligence would you like to enable you to achieve service changes?
Can you suggest any solutions for themes where data is limited?
What resources can you offer in producing the JSNA?
Wrapping up – being involved
• Participation?• Contributions?• Resources?• Joining the working group?• Inputting into technical discussions?
Next Steps
• Local demographic and epidemiological data – collation, analysis and interpretation
• Key contributions of commentary and intelligence• Building local picture• Discussing opportunities and key partnership actions • Ongoing consultation
– Local views– Jointly determining key findings
• Translation of findings into practice
Keeping in touch
• Contact:[email protected]@cambridgeshire.gov.uk
Thank you very much for your attendance & participation today