standards for interventions to address problematic drug ... standards_for_substance misuse... ·...
TRANSCRIPT

Standards for Interventions to Address Problematic Drug and Alcohol Use in Medium Security Editors: Dr Tom Clark and Dr Jeremy Sandbrook CCQI: CCQI146 April 2013

2

3
Contents Introduction ..................................................................................... 4 Developing the standards .................................................................. 5 Literature Review ............................................................................. 6 Scoping exercise ............................................................................ 10 The Standards ................................................................................ 12 Appendix 1 - References .................................................................. 14 Appendix 2 – Delegates: Expert Consultation Workshop 2 October 2012 16 Appendix 3 – Delegates: Consultation Workshop 12 March 2013 .......... 17 Appendix 4 - Summary of key recommendations of guidance and policy documents relevant to the development of the standards .................... 18

4
Standards for Interventions to Address Problematic Drug and Alcohol Use in Medium Security
Introduction People with serious mental health problems have higher rates of co-morbid problematic substance misuse compared with the general population, (Regier et al, 1990; Department of Health, 2002). Studies of forensic patients in the UK show that rates of substance misuse are higher still within this population (Scott, Whyte, Burnett, Hawley & Maden, 2004; Derry, 2008). Rates of problematic substance misuse amongst patients admitted to forensic units are typically between 50 and 90% (Derry, 2008; Oddie and Davies, 2009). Ongoing misuse of substances following admission has also been shown to be a common problem within forensic units (Whyte and Harrison, 2004; Durand, Lelliott and Coyle, 2006). There are several reasons why addressing the problem of co-morbid substance misuse should be a priority for secure services. Mental disorder with co-morbid substance misuse is associated with poorer outcomes in many areas and on many measures. These include worsening psychiatric symptoms, poorer physical health, increased use of institutional services, poor medication adherence, homelessness, greater dropout from services, higher overall treatment costs, and increased contact with the criminal justice system (NICE, 2011). Forensic patients who misuse substances have also been found to be at higher risk of violent recidivism (Maden, Scott, Burnett, Lewis & Skapinakis, 2004) and reconviction following discharge (Scott, Whyte, Burnett, Hawley & Maden, 2004). Furthermore, substance misuse is strongly associated with violence in all populations, including amongst psychiatric patients (eg. Scott et al, 1998; Soyka, 2000), and it has now been shown that the higher rates of violence seen in patients with schizophrenia and other psychoses may largely be the result of higher rates of substance misuse within these groups (Fazel, Gulati, Linsell, Geddes & Grann, 2009). This makes clear the need to address substance misuse problems as a component of treatment, rehabilitation and risk management within forensic services. To date there has been no specific guidance on substance misuse interventions in secure settings, and variable consensus agreement on the most appropriate way to address the clinical need. Consequently in the past, interventions to address substance misuse in secure units have been shown to vary both in design and sophistication (Whyte and Harrison, 2004; Durand, Lelliott and Coyle, 2006). These standards have been developed by Dr Tom Clark and Dr Jeremy Sandbrook in collaboration with Sarah Tucker (Programme Manager for the Quality Network for Forensic Mental Health Services), with the aim of establishing consensus on what services should aim to achieve in this important area of service provision and improving the quality of services across MSUs in the Quality Network.

5
Developing the standards The following is a summary of the stages involved in the development of these standards:
1. Literature Review. A bibliography of key guidance and policy documents was compiled as well as reviewing the published literature available.
2. A scoping exercise was undertaken by electronic survey of all member MSUs in June 2012. The survey instrument was designed by the authors and informed by the literature review. The survey consisted of a variety of questions to yield qualitative and quantitative data. The key areas of enquiry were: levels of substance misuse in MSUs, levels of training for clinical staff in areas relevant to addressing substance misuse, the provision and design of substance misuse services within MSUs and the range of interventions to address substance misuse problems available within MSUs.
3. The first draft of the standards was developed based on the findings of the
first and second stages. This draft was presented and discussed at an initial expert consultation meeting.
4. Based on feedback from the first consultation the second draft of standards was edited and re-written. This draft was presented and discussed at a further open consultation meeting.
5. Based on feedback from the second consultation the standards were
edited to produce a third draft which was then sent to all Quality Network members, key stakeholders and commissioners for consultation. On the basis of comments made a final version of the standards was created.
6. The final version of the standards was presented at the Quality Network Medium Secure Services Annual Forum on 3rd May 2013.
6
Literature Review Treatment of substance misuse in patients with severe mental illness Substance misuse problems in the absence of co-morbid psychiatric disorder are conventionally treated using psychosocial interventions. These include Motivational Interviewing, which aims to address motivation to affect change in addictive behaviour, CBT, focussing on adapting behaviours and building coping strategies, social skills training, supportive counselling, and contingency management - the use of positive reinforcement for drug abstinence. However, using these interventions in individuals with substance misuse problems and co-morbid psychiatric conditions (‘dual diagnosis’ patients) is acknowledged as more complex and presents further challenges. Models of service provision Three models are usually described: serial, parallel and integrated care. In serial treatment mental illness and substance misuse are addressed consecutively by differing services, necessitating a judgment as to which is the primary problem, and an assumption that one or other can be resolved within a reasonable timescale. In practice the two conditions are usually interdependent and often chronic, and patients may be shunted from one service to the other without receiving adequate treatment from either. In the parallel model, both problems are treated by specialist teams at the same time, necessitating effective communication between difference agencies. In the integrated model the patient receives concurrent treatment for both mental illness and substance misuse from a single clinical team within a mainstream service setting. National policy guidance (detailed below) indicates that substance misuse treatments should be provided within mental health services using an integrated model, which is also referred to as mainstreaming. Treatment approaches Approaches to treating substance misuse commonly identify 4 stages of treatment. Engagement involves the development and maintenance of a therapeutic relationship between staff and patient, through a non-confrontational, empathic and respectful interactional style. It is enhanced by addressing tha patient’s immediate needs rather than focusing on the solely on reducing substance use. Motivation building draws on the cyclical transtheoretical model of substance misuse behaviour (Prochaska and DiClemente, 1982), and the principals of motivational interviewing (Miller and Rollnick, 1991) to encourage the patient to move between motivational stages. Active treatment is the phase of harm minimisation and reducing drug use. Relapse prevention is the fourth stage and is essential in a chronic relapsing condition. The following elements of treatment are considered to characterise successful treatments for dual diagnosis patients (Ziedonis et al, 2005), and are reflected in current policy and guidance (see below):
• Engagement with a trusted provider • Long-term support

7
• Staged treatment appropriate for the patient’s stage of motivation and readiness to change
• Establishing a trusting and collaborative relationship • Building hope in the patient through motivational interventions • Substance awareness work • Comprehensive attention to other needs such as physical health, housing,
finances etc • Relapse prevention work and social skills training, including managing
high risk situations Clearly many of the above are qualities to which psychiatric services would aspire in the management of severe mental illness. Hence effective treatment of substance misuse and of mental illness are linked not only through co-morbidity, but also through the interventions used. This tends to support integrated treatment over any other approach. Empirical research The literature regarding the treatment of co-morbid substance misuse in patients with severe mental illness suggests the most effective interventions should constitute an integrated, long-term treatment approach adopting principals of motivational interviewing (MI) combined with cognitive behavioural therapy (CBT), social and coping skills training, and contingency management (eg. Cleary, Hunt, Matheson & Walter, 2009). However the evidence base is not extensive, and is still evolving. A recent Cochrane Review examining 25 RCTs comparing psychosocial interventions to care as usual in patients with severe mental illness and co-morbid substance misuse found ‘no compelling evidence to support any one psychosocial treatment over another to reduce substance use or improve mental state’ (Cleary et al 2010). Treatment of dual diagnosis in secure settings There is a very limited empirical research base examining the effectiveness of treatment interventions for substance misuse in forensic settings. A small number of studies have been published evaluating the use of individual psychological treatment programmes in secure units (eg. Miles at al, 2007; Derry and Batson, 2008; Oddie and Davies, 2009, Weldon and Ritchie, 2011). However these have been based on small samples, using differing programmes, with limited follow-up periods and heterogeneous outcome measures. A number of authors have described experiences of setting up and evaluating substance misuse programmes within secure settings (eg. Piek, 2009; Swain, Boulter and Piek, 2010; Wood et al, 2009, Edwards et al, 2011) and these papers were useful in informing the initial development of these standards. Previous research into substance misuse treatment in MSUs In September 2005 The Royal College of Psychiatrists Research Unit reported on a survey of the availability of interventions to address substance misuse in 28 NHS MSUs (Durand, Lelliott and Coyle, 2006). The main findings reported were: Drug and alcohol use was endemic in MSUs

8
All units reported that substance misuse had occurred within the unit in the past year, and 78% in the last month. Cannabis and alcohol were considered to pose the greatest problem. Most units had written policies regarding substance misuse The majority were orientated towards abstinence, however a number of units had policies orientated towards harm minimisation regarding use of alcohol. MSU staff teams were ill-equipped to manage substance misuse problems The report noted ‘The overall picture is of a lack of capacity, in terms of staff
skills to treat people with co-morbid drug and alcohol misuse problems’. Although most MSUs had at least one identified staff member with some specialist skills, only 4 of 27 service managers were satisfied that the staff group was adequately trained in substance misuse. Many in-house treatment programmes were neither comprehensive nor integrated The majority of units reported offering key interventions to address substance misuse, however such work was generally being undertaken by individual staff members or small groups rather than in the context of an integrated programme. Guidance and policy documents A number of relevant national guidance and policy documents exist in this area which, although not specific to the provision of psychiatric care in secure settings, are relevant to addressing problematic drug and alcohol use in individuals with mental disorder, including in inpatient settings. We noted the following key guidance and policy documents in the preparation of these standards:
• Dual Diagnosis Good Practice Guide, DH 2002 • Dual diagnosis in mental health inpatient and day hospital settings, DH
2006 • Standards for Medium Secure Units, CCQI 2006 • Closing the gap – a Capability Framework for working effectively with
people with combined mental health and substance use problems Hughes/DH 2006.
• Drug misuse: psychosocial interventions (CG100), NICE 2007 • Drug misuse and dependence – UK Guidelines on clinical management
NTA/DH2007 • Best Practice Guidance Specification for adult medium-secure services, DH
2007 • A Guide for the management of Dual Diagnosis in Prisons DH 2009 • Psychosis with coexisting substance misuse (CG120), NICE 2011 • Alcohol Use Disorders (CG115), NICE 2011
A summary of the key recommendations of each document relevant to the development of the standards is given in Appendix 4.

9
Guidance and policy documents – summary and key themes Integrated treatment is consistently identified as best practice for treatment of mental disorder with coexisting substance misuse. All mental health staff should have competencies in the recognition and treatment of substance misuse problems and this should be reflected in the provision of training for all staff. Mental health service users should have their drug and alcohol use assessed as part of the Care Programme Approach (CPA) and managed through a single care plan. Interventions to address substance misuse should be staged according to engagement and motivational stage and be matched to level of need. Mental health inpatient units should have clear policies relating to substance misuse to promote a therapeutic environment free from drugs and alcohol.

10
Scoping exercise A survey was sent to all MSUs affiliated with the Quality Network. 62 MSUs were contacted, both within the NHS and the private sector. The survey was sent to the QN lead contact within each MSU, who was requested to pass it to ‘the clinician within the MSU with best knowledge of therapeutic interventions currently available for substance misuse’ on the MSU. The design of the survey instrument was informed by the literature review and included open and closed questions to yield qualitative and quantitative data. The key areas of enquiry were:
• levels of substance misuse in MSUs • levels of training for clinical staff relevant to substance misuse • the provision and design of substance misuse services within MSUs • the range of substance misuse interventions available in MSUs
41 of the 62 units contacted responded to the survey (66%). 28 were NHS providers and 11 private sector (2 units responded anonymously). Key findings The majority of MSUs are undertaking a variety of specific interventions to address substance misuse. In many cases substance misuse interventions are being undertaken within programmes that appear well resourced and of a high level of sophistication. However the data suggest that on some units interventions may be undertaken in the absence of a coherent treatment strategy, and without taking into account individual patient need. Additionally, whilst the results suggested that there has been an overall increase in resources available nationwide, the provision of services was observed to vary significantly between units, and some units have very limited provision of substance misuse interventions. There has been an increase in the use of group interventions to address substance misuse on MSUs In 2006 Durand et al found that 67% of NHS MSUs surveyed ran such groups (Durand et al, 2006). In the scoping exercise the figure was 90%. Low numbers of units run ‘open’ groups for substance misuse problems or use contingency management These figures are low in the context of national guidance for addressing substance misuse within inpatient settings (NICE 2007, 2011; DH 2006). Substance misuse teams have become more commonplace, and the majority of units are mindful of a need for dedicated provision for substance misuse interventions within their staff
11
40% of units had a dedicated substance misuse team and two-thirds reported either having staff with protected time or staff whose primary role is to work with substance misuse. We consider that this can be broadly interpreted as the proportion of units making substance misuse a genuine treatment priority. Substance misuse in MSUs may have reduced In 2006 Durand et al found that substance misuse had occurred on all units they surveyed within the last year, and in 74% of units within the last 30 days (Durand et al, 2006). Our data suggest this figure may have fallen, to 66% and 29% respectively. It may be that this finding is related to the increase observed in the provision of treatments. Structured assessment tools seem to be used commonly in MSUs, but tend not to be valued highly. This might be because the tools are not appropriate for the setting. Many MSU staff are not receiving adequate training in substance misuse Only half of the units surveyed reported that clinical staff ‘routinely’ received training related to substance misuse problems. This is low in the context of current national guidance (DH, 2006). The great majority of MSUs are internally resourced with regards to substance misuse interventions This suggests that this is seen as core work within units, in tune with national policy with regard to ‘mainstreaming’ and integration of treatment for substance misuse within mental health services. Summary Based on the literature review and scoping exercise, we developed standards relating to the following areas:
Policies and procedures Staff training Assessment Treatment
A note on terminology – Substance misuse is a broad term, widely used within the guidance, policy documents and literature on the subject. It is generally considered to encompass the harmful use of any psychotropic substance, including alcohol and either legal or illicit drugs. However, the consensus view amongst the consultation groups was that the term ‘problematic drug and alcohol use’ was a preferred term to use within the standards, on the basis that this -
• Acknowledges that not all alcohol (or drug) use is necessarily problematic • Allows discrimination between use of alcohol and other drugs • Does not discriminate between legal and illegal drugs • Avoids the term ‘misuse’ which can be considered as value-laden and
subjective.

12
The Standards Number Standard
1
There are policies and procedures for promoting a therapeutic environment free from drugs and alcohol, and these are made widely available.
1.1 There is a policy for search procedures which includes reference to suspected drugs and alcohol.
1.2 There is a policy on visiting arrangements which includes reference to suspected supply or use of drugs and alcohol.
1.3 There is a policy on drug and alcohol testing procedures.
1.4 There is a policy on procedures for containment and disposal of suspected drugs and alcohol.
1.5 There is a policy on patients’ use of drugs and alcohol within the unit and on leave.
1.6 There is a policy on managing intoxication and withdrawal from drugs and alcohol.
1.7 Rules relating to drug and alcohol use are displayed clearly and made available to all service users and their visitors.
1.8 Information about drugs and alcohol use is made available to families and carers.
2 Training relating to drug and alcohol use is provided for all clinical staff.
2.1 Basic training relating to drug and alcohol use is provided to all clinical staff and is tailored for working in secure settings.
2.2 Basic training relating to drug and alcohol use includes knowledge and awareness of the main groups of substances of abuse.
2.3 Basic training relating to drug and alcohol use includes knowledge and awareness of intoxication, withdrawal and overdose with drugs or alcohol.
2.4 Basic training relating to drug and alcohol use includes physical and mental health risks associated with drug and alcohol use.
2.5 Basic training relating to drug and alcohol use includes the principles of assessment, treatment planning, harm minimisation and relapse prevention.
2.6 Basic training relating to drug and alcohol use includes the use of simple interventions to enhance motivation and encourage behaviour change.
2.7 Basic training relating to drug and alcohol use includes the relationship between substance use and offending risk.
2.8 Basic training relating to drug and alcohol use includes relational security and the problems associated with a drug using subculture in secure settings.
2.9 Clinical staff with specific responsibilities for working with problematic drug and alcohol use should undertake further training or experience.
2.10 Clinical staff with specific responsibilities for working with problematic drug and alcohol use are provided with ongoing supervision.
13
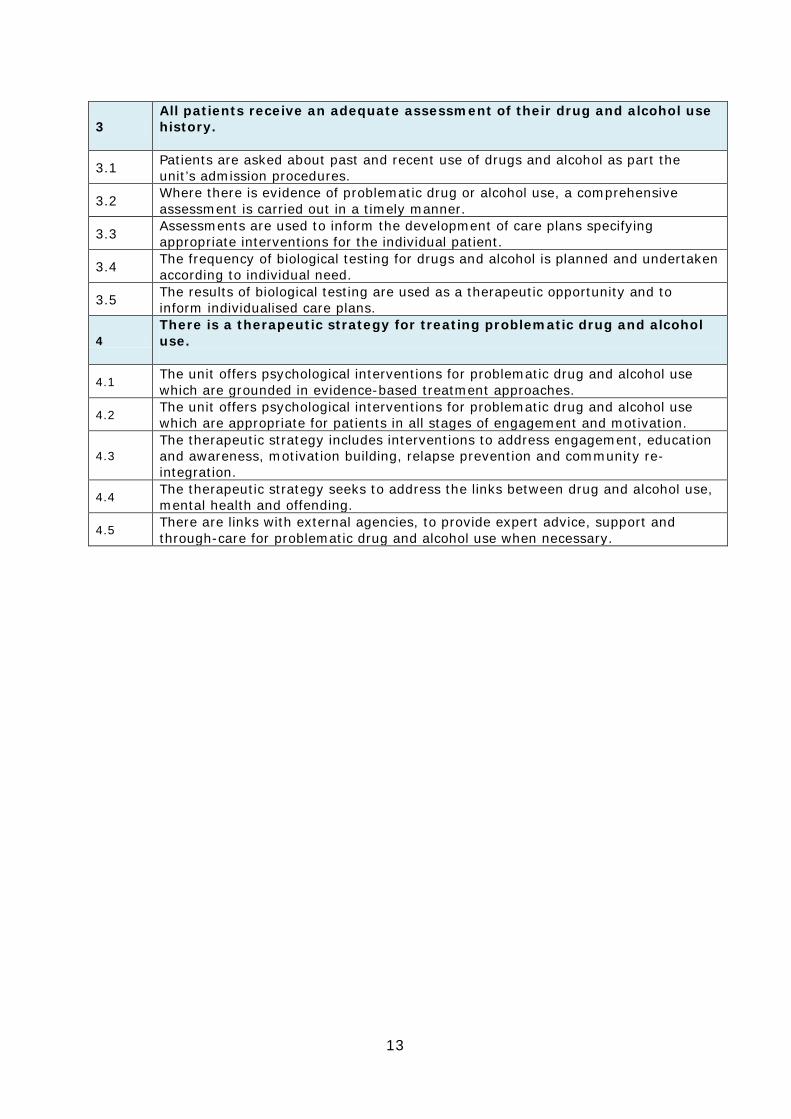
3 All patients receive an adequate assessment of their drug and alcohol use history.
3.1 Patients are asked about past and recent use of drugs and alcohol as part the unit’s admission procedures.
3.2 Where there is evidence of problematic drug or alcohol use, a comprehensive assessment is carried out in a timely manner.
3.3 Assessments are used to inform the development of care plans specifying appropriate interventions for the individual patient.
3.4 The frequency of biological testing for drugs and alcohol is planned and undertaken according to individual need.
3.5 The results of biological testing are used as a therapeutic opportunity and to inform individualised care plans.
4 There is a therapeutic strategy for treating problematic drug and alcohol use.
4.1 The unit offers psychological interventions for problematic drug and alcohol use which are grounded in evidence-based treatment approaches.
4.2 The unit offers psychological interventions for problematic drug and alcohol use which are appropriate for patients in all stages of engagement and motivation.
4.3 The therapeutic strategy includes interventions to address engagement, education and awareness, motivation building, relapse prevention and community re-integration.
4.4 The therapeutic strategy seeks to address the links between drug and alcohol use, mental health and offending.
4.5 There are links with external agencies, to provide expert advice, support and through-care for problematic drug and alcohol use when necessary.

14
Appendix 1 - References Cleary, M., Hunt, G.E., Matheson, S., Walter, G. (2009). Psychosocial treatments for people with co-occurring severe mental illness and substance misuse: systematic review. Journal of Advanced Nursing 65(2), 238–258. Cleary, M., Hunt, G.E., Matheson, S., Siegfried, N., Walter, G. (2010) Psychosocial interventions for people with both severe mental illness and substance misuse. Cochrane database of systematic reviews, 2010, Issue 3. Department of Health (2007). Best Practice Guidance Specification for adult medium-secure services. London: Department of Health. Department of Health (2009) A Guide for the management of Dual Diagnosis in Prisons. London: Department of Health. Department of Health (2006). Dual diagnosis in mental health inpatient and day hospital settings. London: Department of Health Department of Health (2002). Mental Health policy implementation guide: Dual Diagnosis good practice guide. London: Department of Health. Derry, A. (2008). The clinical response to substance use problems in forensic mental health services. The British Journal of Forensic Practice, 10(3), 20-23. Durand, MA., Lelliott, P., Coyle, N. (2006). Availability of treatment for substance misuse in medium secure psychiatric care in England: a national survey. Journal of Forensic Psychiatry & Psychology, 17, 611-625. Edwards, R., Guy, R., Bartholomew, M., Buckland, R. (2011). Reflecting on the delivery of a structured alcohol and drug group in a medium-secure forensic unit. Advances in Dual Diagnosis 4(4) 180-186. Fazel, S., Gulati, G., Linsell, L., Geddes, J.R., Grann, M., (2009). Schizophrenia and violence: systematic review and meta-analysis. PLoS Med, 6(8). Hughes, L. (2006). Closing the Gap – A Capability Framework for working effectively with people with combined mental health and substance use problems London: Department of Health. Maden, A., Scott, F., Burnett, R., Lewis, GH., Skapinakis, P. (2004). Offending in psychiatric patients after discharge from medium secure units: prospective national cohort study. BMJ,328,1534. Miller, WR., Rollnick, S. (1991). Motivational Interviewing: preparing people to change addictive behaviour. New York: Guildford Press. National Treatment Agency for Substance Misuse (2007). Drug misuse and dependence – UK Guidelines on clinical management. NTA/DH, London. NICE (2011). Alcohol Use Disorders: Clinical Guideline 115. NICE, London.

15
NICE (2007). Drug misuse – psychosocial interventions; Clinical Guideline 51. NICE, London. NICE (2011). Psychosis with coexisting substance misuse; Clinical Guideline 120. NICE, London. Oddie, S., Davies, J. (2009). A multi-method evaluation of a substance misuse program in a medium secure forensic mental health unit. Journal of Addictions Nursing, 20, 132–141. Piek, N. (2009) Developing a therapeutic group programme to address dual diagnosis needs in a medium secure unit. Advances in Dual Diagnosis 2(2)19-23 Prochaska, JO., DiClemente, CC. (1982). Transtheoretical Therapy: towards a more integrative model of change. Psycotherapy: theory, research and practice, 20, 161-73. Regier, DA., Farmer, ME., Rae, DS., Locke, BZ., Keith, SJ., Judd, LL., et al. Comorbidity of mental disorders with alcohol and other drug abuse: results from the Epidemiologic Catchment Area (ECA) Study. JAMA, 264, 2511-8. Royal College of Psychiatrists Centre for Quality Improvement (2006). Standards for Medium Secure Units, CCQI, London. Scott, F., Whyte, S., Burnett, R.,Hawley, C., Maden, A. (2004). A national survey of substance misuse and treatment outcome in psychiatric patients in medium security. Journal of Forensic Psychiatry & Psychology, 15, 595–605. Scott, H., Johnson, S., Menezes, P., Thornicroft, G., Marshall, J., Bindman, J., Bebbington, P., and Kuipers, E. (1998). Substance misuse and risk of aggression and offending among the severely mentally ill. British Journal of Psychiatry, 172, 345-350. Soyka, M. (2000). Substance misuse, psychiatric disorder and violent and disturbed behaviour. British Journal of Psychiatry, 176, 345-350. Swain, E., Boulter, S., Piek, N. (2010). Overcoming the challenges of evaluating dual diagnosis interventions in medium secure units. British Journal of Forensic Practice, 12(1) 33- 37. Weldon, S., Ritchie, G. (2010). Treatment of dual diagnosis in mentally disordered offenders: application of evidence from the mainstream. Advances in Dual Diagnosis, 3, 18-23. Whyte, S., Harrison, C. (2004). Substance misuse services in secure psychiatric units. Medicine, Science and the Law, 44, 71-74. Wood, N., Patel, K., Skinner, J., Thomson, K. (2009). Setting up a dual diagnosis service within a forensic inpatient setting: reflections one year on. Advances in Dual Diagnosis, 2(3) 20-24. Ziedonis, DM., Smelson, D., Rosenthal, RN., Batki, SL., Green, AI., Henry, RJ. et al (2005). Improving the Care of Individuals with Schizophrenia and Substance Use Disorders: Consensus Recommendations. Journal of psychiatric practice, 11, 315-39.

16
Appendix 2 Delegates: Expert Consultation Workshop – 2 October 2012
First Name Surname Role Organisation
Mark Bartholomew Dual Diagnosis Lead, Occupational Therapist
Avon & Wiltshire Mental Health NHS Partnership Trust
Sara Boutler Consultant Clinical Psychologist North London Forensic Service Hanora Byrne Clinical Nurse Specialist in Addictions Health Service Executive Ireland Angela Charles Dual Diagnosis Nurse Mersey Care NHS Trust
Helen Clotherier Principal Clinical Psychologist, ASRO-S Programme Manager
Northumberland Tyne and Wear NHS Foundation Trust
Alison Crozier Dual Diagnosis Nurse Mersey Care NHS Trust Alan Cunningham Psychologist Nottingham Healthcare NHS Trust
Lois Dugmore Nurse Consultant Dual Diagnosis Lancashire Partnership NHS Trust
Richard Edwards Dual Diagnosis Nurse Consultant Avon & Wiltshire Mental Health NHS Partnership Trust
Elaine Fehrman Advanced Practitioner Rampton Hospital Geraldine Hamilton Lead Occupational Therapist Belfast Health & Social Care Trust Peter King Dual Diagnosis Nurse Mersey Care NHS Trust
Cheryl Kippling Consultant Nurse Dual Diagnosis South London & Maudsely NHS Foundation Trust
Steve Lilley Psychologist Partnerships in Care
Clive Long Associate Director of Psychology/Psychological Therapies St Andrews
Coyne Lumley Forensic Psychologist Partnerships in Care
Tawonezwi Manyumbu Social Worker South London & Maudsely NHS Foundation Trust
Jayne Moore Dual Diagnosis Lead, Specialist Services Division.
Oxford Health NHS Foundation Trust
Rob O'Brian Clinical Nurse Specialist Birmingham and Solihull Mental Health Foundation Trust
Julia O'Connor Psychologist West London Mental Health NHS Trust
Aideen O'Kane Consultant Forensic Psychiatrist
Kajal Patel Consultant Psychiatrist Priory
Nicola Piek Psychologist Barnet Enfield & Haringey Mental Health Trust
Gordon Ritchie Clinical Nurse Specialist Carstairs
Rebecca Stevens Lead SM Nurse Southern Health NHS Foundation Trust
Phil Walsh Care Pathway Advisor Midlands and East Specialised Commissioning Team
Pamela Walters Forensic Psychiatrist South West London and St Georges NHS Foundation Trust
Alex Whale Forensic Psychiatric Nurse West London Mental Health NHS Trust
Anna Womersely Senior Nurse Greater Manchester West Mental Health NHS Foundation Trust
Nikki Wood Head of the Forensic Dual Diagnosis Service East London NHS Foundation Trust
17
Appendix 3 Delegates: Consultation Workshop 12 March 2013 First Name Surname Role Organisation Mark Bartholomew Dual Diagnosis Lead, West of England
Forensic Service West of England Forensic Service
Vaughan Bater Ward manager Caswell Clinic
Sara Boulter Consultant Clinical Psychologist North London Forensic Service
Angela Charles Dual Diagnosis Practitioner Scott Clinic
Kitty Clark-McGhee Forensic Dual Diagnosis Practitioner John Howard Centre
Helen Clothier Principal Clinical Psychologist Forensic Services - Bamburgh Clinic
Ian Compson Substance Misuse Counsellor Alpha Hospitals NW Limited Alan Cunningham Clinical Psychologist Arnold Lodge
Paul Delaney Senior Forensic Social Work Practitioner Brockfield House
Lois Dugmore Nurse Consultant Dual Diagnosis Herschel Prins Centre
Elaine Fehrman Advanced Practitioner Rampton Hospital
Phil Garnham Consultant Nurse Bracton Centre
Chris Hall Substance Misuse Lead Bracton Centre
Abdi Hussein Service User Expert QNFMHS
Olajide Jegede SMSS Nurse Champion South West London and St George’s MH NHS Trust
Nusrat Khan Kingsley Green Hospital
Andrea Livesey Clinical Manager / Advanced Practitioner Substance Misuse Team, Edenfield Centre Clive Long Associate Director of Psychology &
Psychological Therapies St Andrew's Healthcare
Lilly Magolo Clinical Nurse Specialist Partnerships in Care Stockton Hall
Tawona Manyumbu Social Worker River House Medium Secure Unit
Davy Martin Deputy Charge Nurse Shannon Clinic MSU
Nick McAndrew Therapeutic group coordinator Caswell Clinic
Sharon Meek Clinical Nurse Specialist Partnerships in care
Jayne Moore Dual Diagnosis Lead Oxford Health NHS Foundation Trust
Pandria Morgan Nurse in substance misuse service Shaftesbury Clinic
Rob O’Brien Clinical Nurse Specialist Reaside Clinic
Julia O'Connor Head of Psychological Therapies West London Mental Health Trust
Zoe Otter Forensic Psychologist in Training Calverton Hill
Vittoria Pezzoni Consultant Psychiatrist Eric Sheppard Forensic Service
Nicola Piek Dual Diagnosis Specialist The North London Forensic Service
Aileen Rainsbury Substance Misuse Deputy Bracton Centre
Ruth Rushton Clinical and Forensic Psychologist Southview, The Drive
Nikki Stefani Service User Expert RCPsych Becky Stevens Substance Misuse Practitioner Ravenswood House
Amanda Tidman Senior Assistant Psychologist - substance use treatment programme manager
Farmfield (Priory Group)
Oliver Tooze Clinical Psychologist Fromeside
Gerard Waldron Consultant Forensic Psychiatrist John Howard Centre
Simon Wels Forensic psychologist South West London and St George’s MH NHS trust.
Anna Womersley Senior Nurse Substance Misuse Team Edenfield Centre Nikki Wood Chartered and Principal Clinical
Psychologist John Howard Centre
18
Appendix 4 - Summary of key recommendations of guidance and policy documents relevant to the development of the standards Dual Diagnosis Good Practice Guide, DH 2002 This document was the policy foundation for the introduction of integrated treatment for dual diagnosis patients in the UK, to be delivered by existing mental health services, in liaison and with support from substance misuse services as necessary. This policy was referred to as ‘mainstreaming’. The key recommendations relevant to the development of these standards were:
• Integrated care delivers better outcomes than serial treatment • Individuals with dual diagnosis deserve high quality, patient focused and
integrated care which should be delivered within mental health services. • Adequate numbers of staff in inpatient services must be suitably trained
to deliver this. • A two tier training strategy delivering basic training across all staff in
relevant services and advanced training and supervision to particular staff must be formulated and implemented by services
• Treatments should be staged according to an individual’s readiness for change and engagement with services
• All mental health provider agencies must designate a lead clinician for dual diagnosis issues
Dual diagnosis in mental health inpatient and day hospital settings, DH 2006 The focus of this document was that ‘the assessment and management of drug and alcohol use are core competences required by clinical staff in mental health services’. The key recommendations relevant to the development of these standards were:
• Mental health staff should be competent in intervening in drug and alcohol use as an integral part of providing treatment and care.
• Training should be provided, to qualified and unqualified clinical staff, and encompass the development of knowledge and skills in assessment and care/treatment planning for dual diagnosis patients
• A substantial number of cases may respond to simple motivational interventions provided by mental health staff as part of the overall care plan rather than a need for more specialist addiction skills.
• Specialist substance misuse services will usually only be needed to provide care for treatment of severe dependence (generally crack cocaine and opiates) or for more severe or complex cases of cannabis or khat use.
• Mental health service users should have their drug and alcohol use assessed as part of the Care Programme Approach (CPA) through a single care plan
• Action should be aimed at making wards drug and alcohol free rather than accepting that their presence is inevitable. Mental health inpatient units need to have clear policies about searching visitors, patients, staff and premises.
19
Standards for Medium Secure Units, CCQI 2006 These represent the current standards in use within the Quality Network.
1.29. The unit has access to a substance misuse specialist or dual diagnosis specialist either working as part of an integrated or parallel model 2.12 There is a policy on the control of illicit substances covering (a) treatment of substance misuse; (b) education on the dangers of substance abuse; (c) advice to visitors on the dangers of passing illicit/unauthorised substances; (d) a protocol with police for when drugs are discovered; (e) a policy on "searching with cause" for drugs 4.7 The in-patient team has good access to a range of services, as Ippropriate to the needs of the patients. These include… substance and alcohol misuse services
Closing the Gap – A Capability Framework for working effectively with people with combined mental health and substance use problems This Policy document highlighted the roles and responsibilities of various agencies in providing care for people with dual diagnosis. It details the training and service developments that are required to implement the introduction of integrated treatment of substance misuse problems within mental health services. It aims to establish core competencies for all staff that encounter dual diagnosis patients in a range of settings. The key guidance and recommendations relevant to the development of these standards were:
• In order for mainstreaming to be effective, mental health workers will be required to deliver effective integrated interventions which are a combination of approaches from substance use and mental health including screening and detection, comprehensive assessment, motivational interventions, and relapse prevention
• A tier-based description is given of what capability training should be
available across all mental health staff Drug misuse: psychosocial interventions (CG100) NICE 2007 This guideline covers psychosocial interventions for adults and young people who misuse opioids, cannabis or stimulants. The guideline does not specifically cover people with dual diagnoses or people who misuse alcohol. It identifies key priorities as provision of brief interventions, self-help and contingency management.
20
The key guidance and recommendations relevant to the development of these standards were:
• A range of psychosocial interventions are effective in the treatment of drug misuse; these include contingency management and behavioural couples therapy for drug-specific problems.
• Cognitive behavioural therapy and psychodynamic therapy focused on the treatment of drug misuse should not be offered routinely to people presenting for treatment of cannabis or stimulant misuse or those receiving opioid maintenance treatment.
• Residential, prison and inpatient care - the same range of psychosocial interventions should be available in inpatient and residential settings as in community settings. These should normally include contingency management, behavioural couples therapy and cognitive behavioural therapy [for co-morbid psychiatric disorders]. Services should encourage and facilitate participation in self-help groups.
Drug misuse and dependence – UK Guidelines on clinical management NTA/DH2007 This document provides guidance on the treatment of drug misuse in the UK, however this is more focussed on mainstream addiction services than mental health settings or dual diagnosis populations. The key recommendations relevant to the development of these standards were:
• Psychosocial interventions - o Treatment for drug misuse should always involve a psychosocial
component o Treatment should include - provision of drug misuse related advice
and information, interventions to reduce drug-related harm, psychosocial interventions to increase motivation, psychosocial interventions to prevent relapse and help to address social problems.
o A good therapeutic alliance is crucial to the delivery of any treatment intervention, especially a psychosocial one.
o Self-help and mutual aid approaches, especially 12-Step, have been found to be highly effective for some individuals and patients seeking abstinence should be signposted to them.
o There is a strong evidence base for contingency management and family and couples interventions.
• Treatment of dual diagnosis and in inpatient settings -
o The guiding principle should be to match the needs of the patient to the clinical team and its competencies, minimise multiple referrals and movements within multiple teams, and prevent exclusion from services.
o Service models need to be geared to delivery of integrated psychosocial interventions and integrated pharmacotherapies, and to access wraparound services

21
Best Practice Guidance Specification for adult medium-secure services, Mental Health Policy Implementation Guide, DH 2007
Procedural security- A54. (There will be a) policy on the control of illegal substances A55. (There will be a) policy on substance misuse Public health – G15. Health promotion support to individuals and groups in line with expectations in the general community, including alcohol and addictions, physical activity, diet and nutrition.
A Guide for the management of Dual Diagnosis in Prisons DH 2009 This guidance highlights that most prisons in the UK practise a parallel approach to treatment for dual diagnosis, and recommends that ‘this should be developed
to become as fully integrated as possible’ given the potential problems associated with parallel treatments such as impaired communication between teams and the delivery of ‘fragmented care to the recipient’. This guidance notes that given the ‘relatively small body of evidence for what is effective in the treatment of dual diagnosis’, ‘broader principles of good practice are more appropriate to guide planners and practitioners’. These principles are given as:
• Integrated treatment • Staged interventions • Social support interventions • Long-term perspective • Interventions matched to level of need
Alcohol Use Disorders (Clinical Guideline 115), NICE 2011 This guideline details treatment for adults and young people with harmful alcohol use and dependence as the primary diagnosis. It is noted that the guideline will also be relevant to the work, but will not specifically cover the practice, of those working in other healthcare settings including forensic services. The key recommendations relevant to the development of these standards were:
• Identification and assessment - Staff working in services provided and funded by the NHS who care for people who potentially misuse alcohol should be competent to identify harmful drinking and alcohol dependence.
• All interventions for people who misuse alcohol should be delivered by appropriately trained and competent staff

22
Psychosis with coexisting substance misuse (CG120), NICE 2011 This guideline covers the assessment and management of adults and young people (aged 14 years and older) who have a clinical diagnosis of psychosis with coexisting substance misuse. The key recommendations relevant to the development of these standards were:
• Integrated service models - for most adults with psychosis and coexisting substance misuse, treatment for both conditions should be provided by healthcare professionals in secondary care mental health services
• Policies and procedures - inpatient mental health services should ensure that they have policies and procedures for promoting a therapeutic environment free from drugs and alcohol that have been developed together with service users and their families, carers or significant others. These should include: search procedures, visiting arrangements, planning and reviewing leave, drug and alcohol testing, disposal of legal and illicit substances, and other security measures.
• Training - healthcare professionals working within secondary care mental health services should ensure they are competent in the recognition, treatment and care of adults and young people with psychosis and coexisting substance misuse.
• Treatments – should be based on pre-existing NICE guidance (Alcohol
guidelines CG 100 and CG115 and Drug misuse – psychosocial interventions CG 51 and CG 52).
• Do not exclude adults and young people with psychosis and coexisting substance misuse from contingency management programmes because of their psychosis.

23
24