stemi management 2007 - marmurstemi management 2007 jonathan d. marmur, md, facc pf fmdiiprofessor...
TRANSCRIPT

STEMI Management 2007STEMI Management 2007
Jonathan D. Marmur, MD, FACCP f f M di iProfessor of Medicine
Director, Cardiac Catheterization and Interventional Cardiology
Health Science Center at BrooklynHealth Science Center at BrooklynState University of New York
917-885-8854
1
917 885 8854

Pathophysiology of ACSPathophysiology of ACS
~ 2.0 MM patients admitted
1 4 MM0 6 MM
admittedto CCU or telemetry annually
1.4 MMNon-ST-segment
elevation ACS
0.6 MMST-segment elevation MI
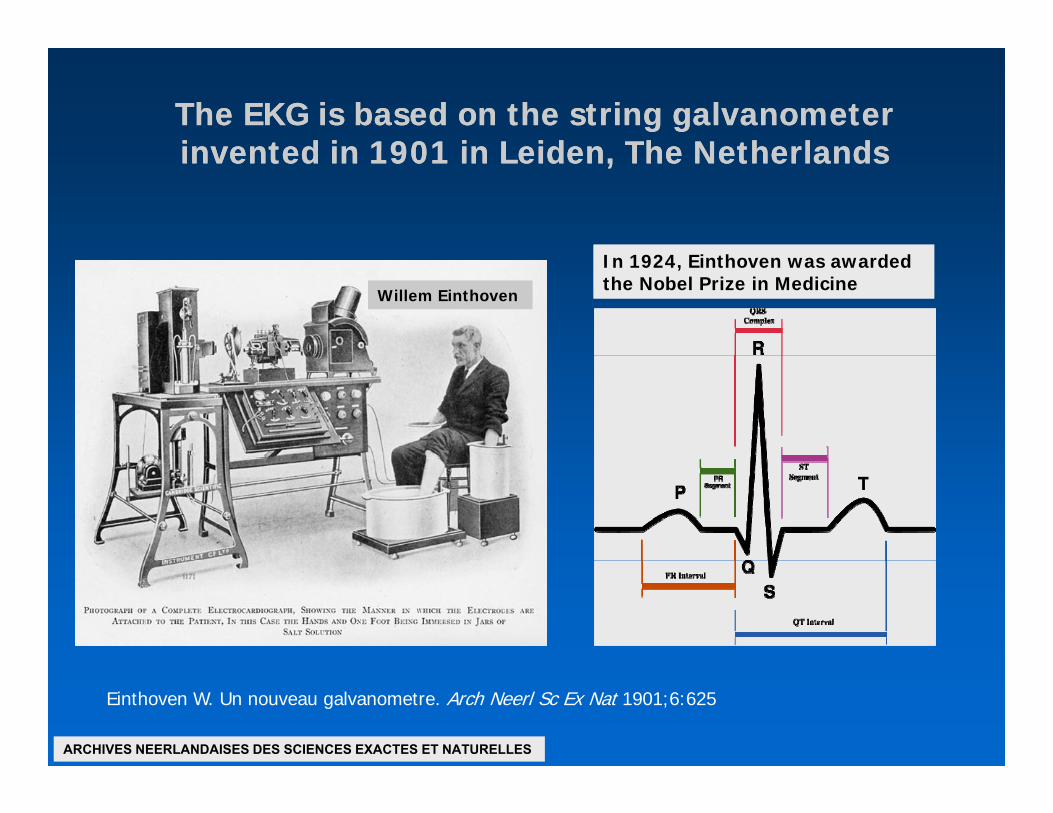
The EKG is based on the string galvanometer The EKG is based on the string galvanometer invented in 1901 in Leiden The Netherlandsinvented in 1901 in Leiden The Netherlandsinvented in 1901 in Leiden, The Netherlandsinvented in 1901 in Leiden, The Netherlands
Willem Einthoven Willem Einthoven
In 1924, Einthoven was awarded the Nobel Prize in Medicine In 1924, Einthoven was awarded the Nobel Prize in Medicine
Einthoven W. Un nouveau galvanometre. Arch Neerl Sc Ex Nat 1901;6:625
ARCHIVES NEERLANDAISES DES SCIENCES EXACTES ET NATURELLES

NSTEMI vs STEMINSTEMI vs STEMI

1980;303:897-902
Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction
MA DeWood J Spores R Notske LT Mouser R Burroughs MS Golden and HT Lang
Prevalence of total coronary occlusion during the early hours of transmural myocardial infarction
MA DeWood J Spores R Notske LT Mouser R Burroughs MS Golden and HT LangMA DeWood, J Spores, R Notske, LT Mouser, R Burroughs, MS Golden, and HT Lang MA DeWood, J Spores, R Notske, LT Mouser, R Burroughs, MS Golden, and HT Lang
To define the prevalence of total coronary occlusion in the hours after transmural myocardial infarction, we used coronary arteriography to study the degree of coronary obstruction in 322 patients admitted within 24 hours of infarction.
Total coronary occlusion is frequent during the early hours of transmural infarction and decreases in frequency during the initial 24 hours, suggesting that coronary spasm or thrombus formation withspasm or thrombus formation with subsequent recanalization or both may be important in the evolution of infarction.

ASA vs Placebo in ISISASA vs Placebo in ISIS--II: Odds of Vascular DeathII: Odds of Vascular Death
Odds ratio and 95% CI
Astrological Gemini/Libra (n=1442)Birthsign All Others (n=7157)
• Play of chance• Unrecognized randomization error • True effectg ( )
Prior MI YesNo
Diabetic YesNo
Sex MaleFemale
Age <6060-6970+
Systolic BP <100Systolic BP <100100-149150-175
Heart Rate <6060-99100+
“When in a trial with a clearly positive result many subgroups are considered, f l ti lt i ti lEKG BBB
IMIAMIST↓
ALL PATIENTS (9 4 11 8% t lit ) 23% ↓
false negative results in some particular subgroups must be expected… It is clear that the best estimate of the real effect is given by the overall results derived from all subgroups combined.”
Modified from: ISIS-2 Lancet 1988 Aug 13;2(8607):349-60
0.5 1 1.5ASA better Placebo better
ALL PATIENTS (9.4 vs 11.8% mortality) 23% ↓g p

Oral AntiOral Anti--platelet Agents platelet Agents –– Sites of ActionSites of Actionp gp g
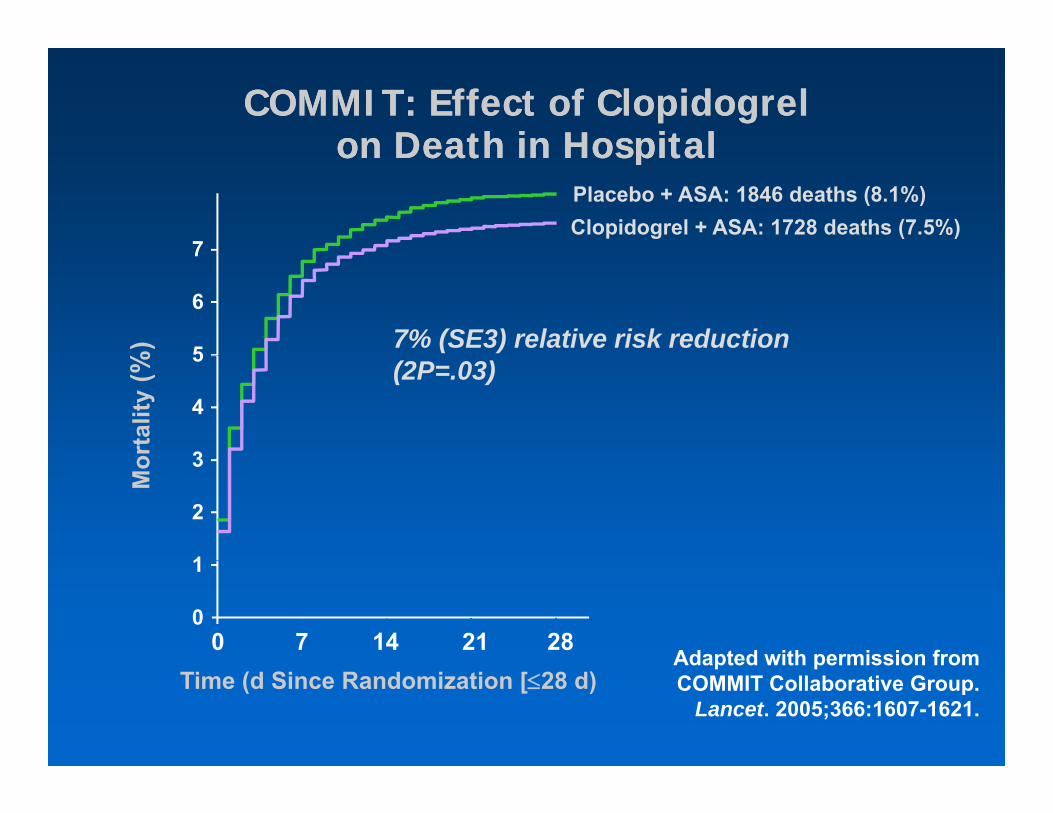
COMMIT: Effect of Clopidogrel COMMIT: Effect of Clopidogrel on Death in Hospitalon Death in Hospitalon Death in Hospitalon Death in Hospital
Placebo + ASA: 1846 deaths (8.1%)Clopidogrel + ASA: 1728 deaths (7.5%)
7
7% (SE3) relative risk reduction
%)
7
6
5 (2P=.03)
orta
lity
(%
5
4
3
Mo 3
2
1
0 7 14 21 28
1
0
Adapted with permission fromTime (d Since Randomization [≤28 d)
Adapted with permission from COMMIT Collaborative Group.
Lancet. 2005;366:1607-1621.

CLARITYCLARITY––TIMI 28: Primary EndpointTIMI 28: Primary EndpointOccluded Artery (or Death/MI Through Angio/HD)Occluded Artery (or Death/MI Through Angio/HD)Occluded Artery (or Death/MI Through Angio/HD)Occluded Artery (or Death/MI Through Angio/HD)
36% 21.7%) 25
P= 001
Odds Ratio: 0.64(95% CI, 0.53-0.76)
Odds Reduction
15.0Dea
th/M
I (%
20
P=.00115.0
rter
y or
D
10
15
cclu
ded
A
5
PlaceboClopidogrel1.00.4 0.6 0.8 1.2 1.6
ClopidogrelBetter
PlaceboBetter
n=1752 n=1739
Oc
0
Better Better
Sabatine MS et al N Engl J Med 2005;352:1179-1189

ST Elevation Myocardial Infarction (STEMI)ST Elevation Myocardial Infarction (STEMI)
8Relationship Between Time to ReperfusionRelationship Between Time to Reperfusion
and Mortality: GUSTOand Mortality: GUSTO--IIbIIb6.4
6
yy
p=0.001
3.7 44
30-daymortality
(%)
12
0< 60 61 – 75 76 – 90 > 91
N: 104 109 76 140
Berger et al. Circulation 1999;100:14
N: 104 109 76 140Time to PTCA (minutes)

Wavefront Theory of Myocardial Lossy y
80
100
80
100
40
60
80
40
60
20
40
20
40
0 040 min 3h 6h 24h 96h 0 3h 6h 24h
Duration of occlusion Time post-occlusion
Reimer et al Circulation 1977;56:786-94
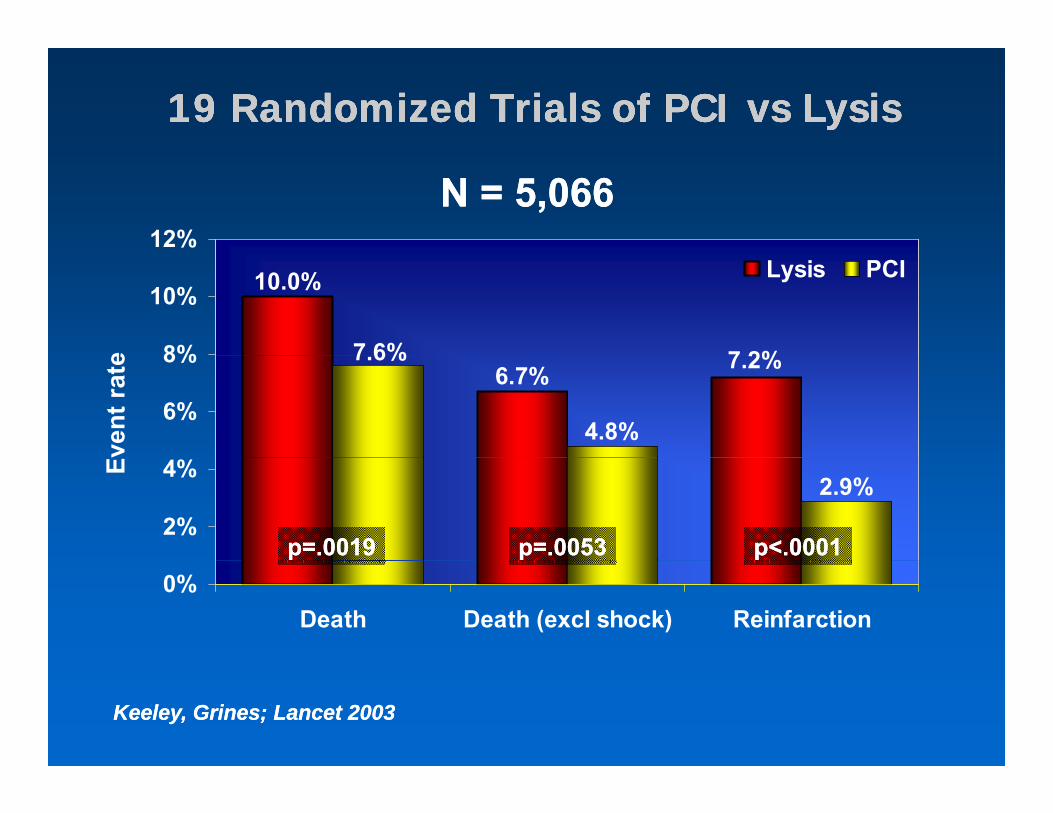
19 Randomized Trials of PCI vs Lysis19 Randomized Trials of PCI vs Lysis19 Randomized Trials of PCI vs Lysis19 Randomized Trials of PCI vs Lysis
12%N = 5,066N = 5,066
10.0%
7 2%7 6%8%
10%
e
Lysis PCI
6.7% 7.2%7.6%
4.8%6%
8%
vent
rate
2.9%2%
4%E
p=.0019p=.0019 p=.0053p=.0053 p<.0001p<.00010%
Death Death (excl shock) Reinfarction
Keeley, Grines; Lancet 2003Keeley, Grines; Lancet 2003

19 Randomized Trials of PCI vs Lysis19 Randomized Trials of PCI vs Lysis
3%N = 5,066N = 5,066
2.2%2%e
Lysis PCI
1.3%
2%
vent
rate P<0.0001P<0.0001 p=0.0002p=0.0002
0 08%
0.8%1%E
0.08%0%
Hemorrhagic stroke Total stroke
Keeley, Grines; in pressKeeley, Grines; in press

DANAMIDANAMI--2: Patient Flow2: Patient Flow
STST-- elevation MIelevation MI(n=1,900)(n=1,900)
RandomizeRandomize
PCI (+ stent)PCI (+ stent)100 mg accelerated t100 mg accelerated t--PAPA PCI ( stent)PCI ( stent)100 mg accelerated t100 mg accelerated t PAPA

DANAMIDANAMI--22
DENMARKDENMARK
5 4 ill i h bit t5 4 ill i h bit t5.4 mill. inhabitants5.4 mill. inhabitants
5 PCI centers5 PCI centers
24 referral hospitals24 referral hospitals
62% of the Danish 62% of the Danish populationpopulation
100 US miles
Transport distanceTransport distanceup to 95 US miles up to 95 US miles (mean 35 miles)(mean 35 miles) 100 US miles(mean 35 miles)(mean 35 miles)

DANAMIDANAMI--2: Primary Results2: Primary Results
16%P=0.0003 P=0.002
Combined Transfer SitesP=0.048
Non-Transfer Sites
16% 16%14%
12%
16%
(%) RRR
45%
14%
12%
16%
12%12%
16%RRR 40%
RRR
8%8%
12%
MI /
Str
oke
9%8%
12%
7%8%
12% 45%
4%Dea
th /
M
4%
7%
4%
0%Lytic Primary PCI Lytic Primary PCI L ti P i PCI
0% 0%Lytic Primary PCI Lytic Primary PCI Lytic Primary PCI
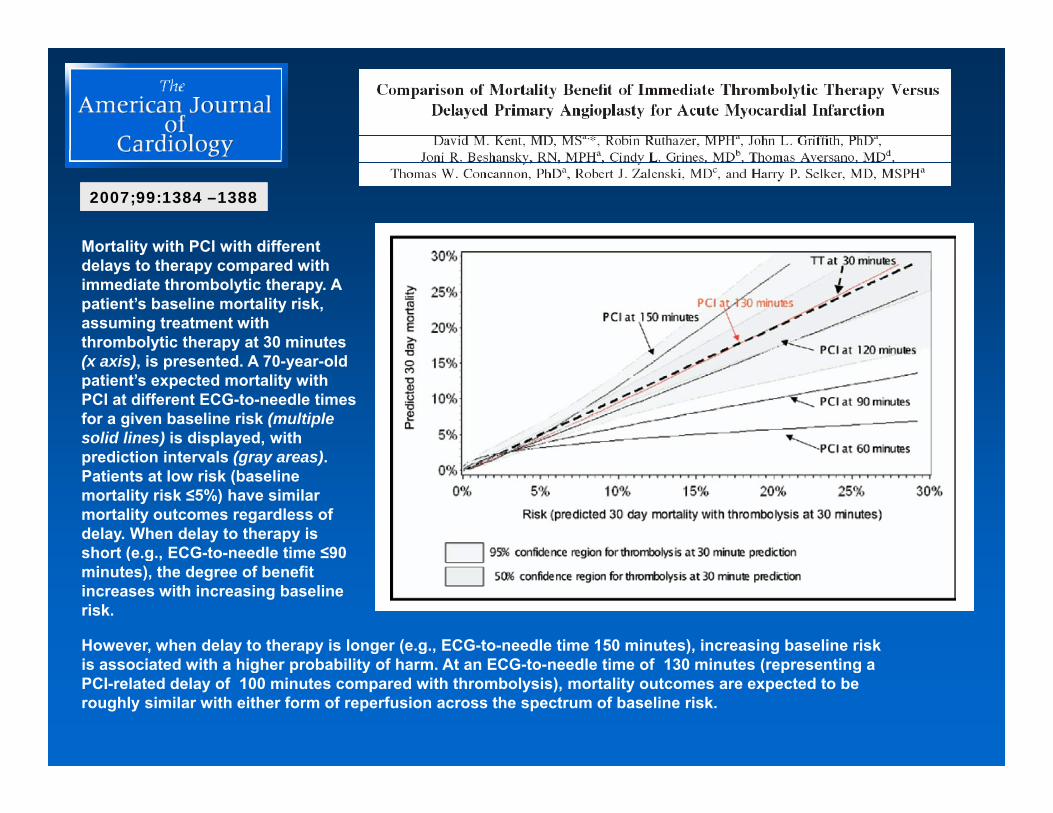
Mortality with PCI with different
2007;99:1384 –13882007;99:1384 –1388
ydelays to therapy compared with immediate thrombolytic therapy. A patient’s baseline mortality risk, assuming treatment with thrombolytic therapy at 30 minutes ( i ) i t d A 70 ld(x axis), is presented. A 70-year-old patient’s expected mortality with PCI at different ECG-to-needle times for a given baseline risk (multiple solid lines) is displayed, with prediction intervals (gray areas)prediction intervals (gray areas). Patients at low risk (baseline mortality risk ≤5%) have similar mortality outcomes regardless of delay. When delay to therapy is short (e.g., ECG-to-needle time ≤90 ( g ,minutes), the degree of benefit increases with increasing baseline risk.
However, when delay to therapy is longer (e.g., ECG-to-needle time 150 minutes), increasing baseline risk is associated with a higher probability of harm At an ECG to needle time of 130 minutes (representing ais associated with a higher probability of harm. At an ECG-to-needle time of 130 minutes (representing a PCI-related delay of 100 minutes compared with thrombolysis), mortality outcomes are expected to be roughly similar with either form of reperfusion across the spectrum of baseline risk.

Monday, November 13, 2006, 12:01 a.m. CT Monday, November 13, 2006, 12:01 a.m. CT
The American College of Cardiology and Partners Launch National AllianceTo Reduce Door-to-Balloon (D2B) Times
D2B alliance aims to save time and lives
The American College of Cardiology and Partners Launch National AllianceTo Reduce Door-to-Balloon (D2B) Times
D2B alliance aims to save time and lives
CHICAGO - The American College of Cardiology (ACC), together with the American Heart Association (AHA) and other key national healthcare organizations, announces the launch of its latest quality campaign, “Door to Balloon (D2B): An Alliance for Quality.” A
CHICAGO - The American College of Cardiology (ACC), together with the American Heart Association (AHA) and other key national healthcare organizations, announces the launch of its latest quality campaign, “Door to Balloon (D2B): An Alliance for Quality.” A q y p g ( ) yGuidelines Applied in Practice (GAP) Program, the D2B campaign is aimed at improving the timeliness of lifesaving therapy for patients with heart attacks at the nation’s hospitals that perform emergency angioplasty.
q y p g ( ) yGuidelines Applied in Practice (GAP) Program, the D2B campaign is aimed at improving the timeliness of lifesaving therapy for patients with heart attacks at the nation’s hospitals that perform emergency angioplasty.
Previously published guidelines developed by the ACC and the AHA recommend that hospitals treating STEMI patients with percutaneous coronary intervention (PCI) should reliably achieve a door-to-balloon time of 90 minutes or less. However, accomplishing this level of performance is an organizational challenge and many patients
Previously published guidelines developed by the ACC and the AHA recommend that hospitals treating STEMI patients with percutaneous coronary intervention (PCI) should reliably achieve a door-to-balloon time of 90 minutes or less. However, accomplishing this level of performance is an organizational challenge and many patients are not treated within the guideline recommendationare not treated within the guideline recommendation
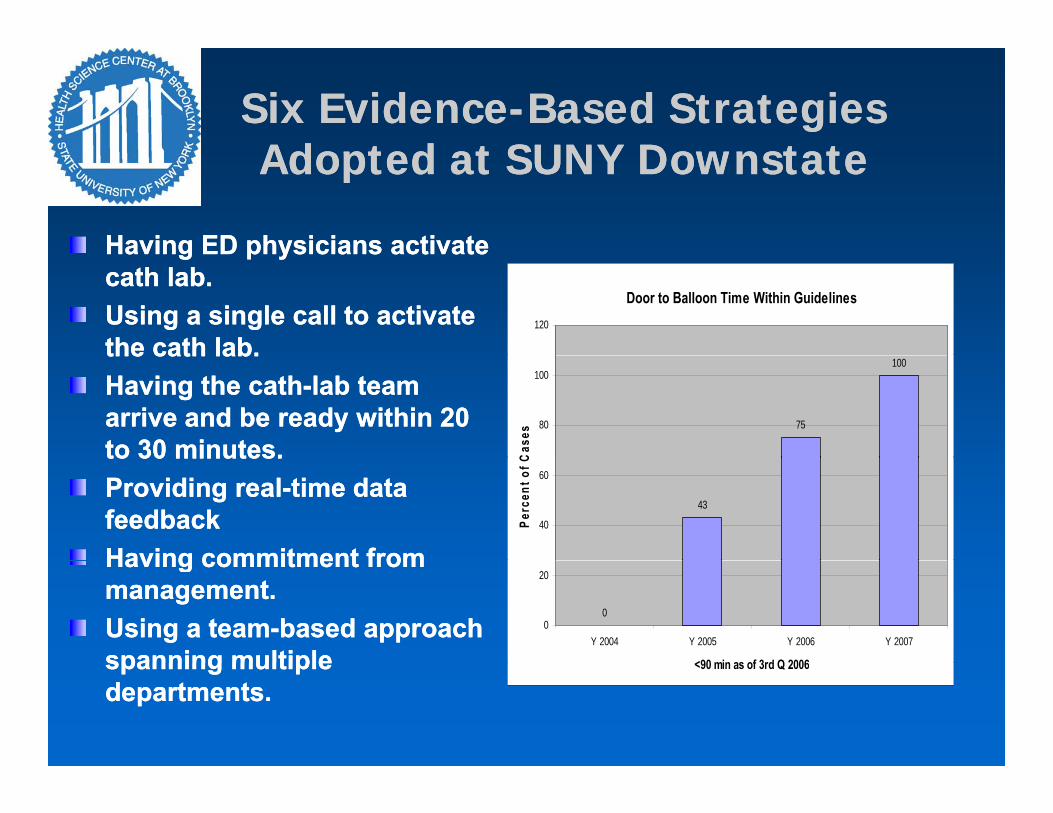
Six EvidenceSix Evidence--Based Strategies Based Strategies Adopted at SUNY Do nstateAdopted at SUNY Do nstateAdopted at SUNY DownstateAdopted at SUNY Downstate
Having ED physicians activateHaving ED physicians activateHaving ED physicians activate Having ED physicians activate cath lab. cath lab. Using a single call to activate Using a single call to activate the cath lab.the cath lab.
Door to Balloon Time Within Guidelines120
the cath lab. the cath lab. Having the cathHaving the cath--lab team lab team arrive and be ready within 20 arrive and be ready within 20 to 30 minutes.to 30 minutes.
75
100
80
100
Cas
es
to 30 minutes. to 30 minutes. Providing realProviding real--time data time data feedbackfeedbackHaving commitment fromHaving commitment from
43
40
60
Perc
ent o
f C
Having commitment from Having commitment from management. management. Using a teamUsing a team--based approach based approach spanning multiplespanning multiple
00
20
Y 2004 Y 2005 Y 2006 Y 2007
<90 min as of 3rd Q 2006spanning multiple spanning multiple departments. departments.
<90 min as of 3rd Q 2006
Treatment DelaysTreatment Delaysyy
Prehospital assessmentPrehospital assessment ED careED care
TransportTransport
Those associated with the cath labThose associated with the cath lab
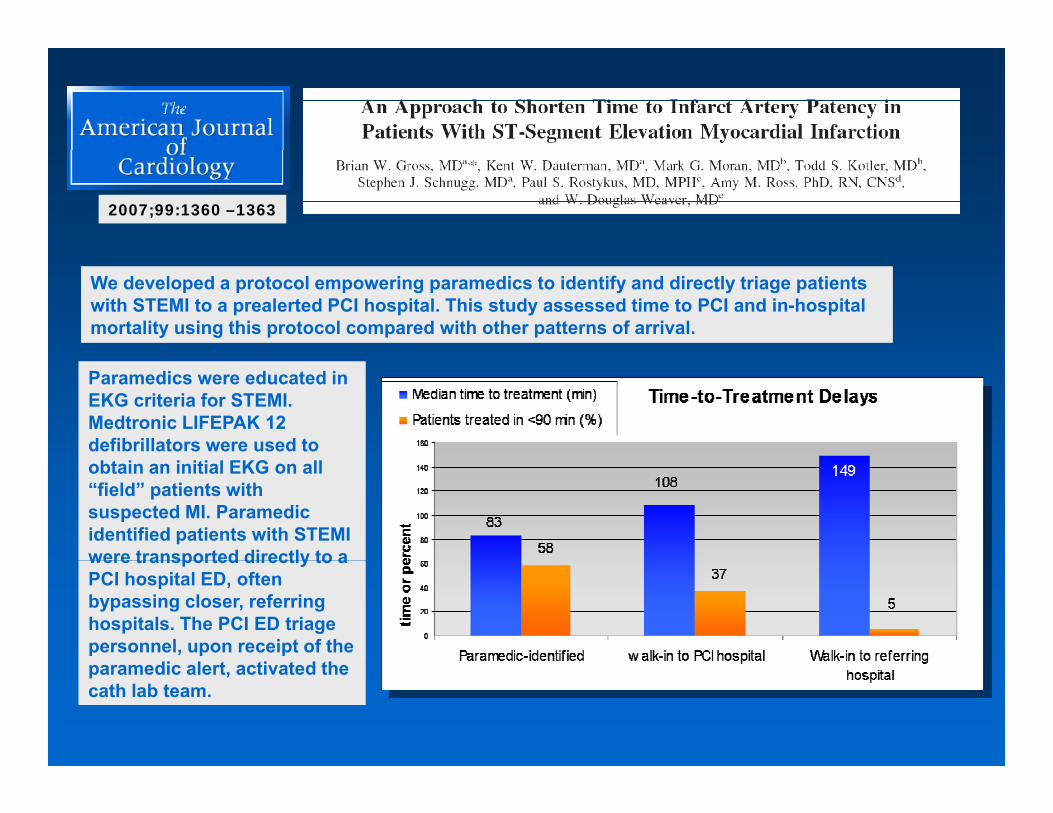
2007;99:1360 –13632007;99:1360 –1363
We developed a protocol empowering paramedics to identify and directly triage patients with STEMI to a prealerted PCI hospital. This study assessed time to PCI and in-hospital mortality using this protocol compared with other patterns of arrival.
We developed a protocol empowering paramedics to identify and directly triage patients with STEMI to a prealerted PCI hospital. This study assessed time to PCI and in-hospital mortality using this protocol compared with other patterns of arrival.
Paramedics were educated in EKG criteria for STEMI. Medtronic LIFEPAK 12 defibrillators were used to
Paramedics were educated in EKG criteria for STEMI. Medtronic LIFEPAK 12 defibrillators were used to obtain an initial EKG on all “field” patients with suspected MI. Paramedic identified patients with STEMI were transported directly to a
obtain an initial EKG on all “field” patients with suspected MI. Paramedic identified patients with STEMI were transported directly to awere transported directly to a PCI hospital ED, often bypassing closer, referring hospitals. The PCI ED triage personnel, upon receipt of the
di l t ti t d th
were transported directly to a PCI hospital ED, often bypassing closer, referring hospitals. The PCI ED triage personnel, upon receipt of the
di l t ti t d thparamedic alert, activated the cath lab team.paramedic alert, activated the cath lab team.

2007;99:1360 –13632007;99:1360 –1363

Inclusion Exclusion
ST-segment elevation• Myocardial infarction (MI), with anymention of location or combinations of
ST-segment elevation• Non Q wave MI (NQWMI)• Non ST-elevation MI (NSTEMI)mention of location or combinations of
locations (e.g., anterior, apical, basal,inferior, lateral, posterior, orcombination), IF DESCRIBED ASACUTE/EVOLVING (e.g., “posteriorAMI”)• Q wave AMI
Non ST elevation MI (NSTEMI)• ST ↑ clearly described as confined to ONE lead• ST ↑ described as minimal, < .10mV, <1 mm, non-diagnostic, or non-specific inALL leads noted to have ST-elevation• ST-elevation clearly described as confined to ONE lead• ST-elevation described as minimal, <.10mV, < 1 mm, non-Q
• Q wave MI, IF DESCRIBED AS ACUTE/EVOLVING• ST ↑• ST abnormality consistent with injury,infarct, or acute/evolving MI ST h i t t ith i j
diagnostic, or nonspecific in ALL leads noted to have STelevation• ST-elevation due to early repolarization• ST-elevation due to left ventricular hypertrophy (LVH)• ST-elevation due to normal variant• ST-elevation with mention of pericarditis ST l ti ith ti f P i t t l/P i t t l' i t• ST changes consistent with injury,
infarct, or acute/evolving MI• ST consistent with injury, infarct, oracute/evolving MI• ST-elevation (STE)• ST-elevation myocardial infarction
• ST-elevation with mention of Printzmetal/Printzmetal's variant• ST-segment elevation, or any of the other ST-segment elevation inclusion terms, described using one of the negative modifiers or qualifiers listed in Appendix H, Table 2.6, Qualifiers and Modifiers Table• ST-elevation or any of the other STsegment elevation inclusion ST elevation myocardial infarction
(STEMI)• ST-segment noted as ≥ .10mV• ST-segment noted as ≥ 1 mm• Transmural AMI• Transmural MI, IF DESCRIBED AS
ST elevation, or any of the other STsegment elevation inclusion terms, with mention of pacemaker/pacing (unless atrial only)Left bundle branch block (LBBB)• Incomplete left bundle branch block (LBBB)• Intraventricular conduction block• Intraventricular conduction delay(IVCD)
ACUTE/EVOLVINGLeft bundle branch block (LBBB)• Intraventricular conduction delay ofLBBB type• Variable LBBB
y• Left bundle branch block (LBBB), or any of the other left bundle branch block inclusion terms, described using one of the negative modifiers or qualifiers listed in Appendix H, Table 2.6,Qualifiers and Modifiers Table• Left bundle branch block (LBBB), or any of the other left bundle branch block inclusion terms with mention of bundle branch block inclusion terms, with mention of pacemaker/pacing (unless atrial only)
DefinitionsDefinitions
Definition: A percutaneous coronary intervention (PCI) is considered non-primary when it is used for reasons that are not Definition: A percutaneous coronary intervention (PCI) is considered non-primary when it is used for reasons that are not emergent in nature.
Non-primary PCIs include elective, rescue, and salvage PCIs. In contrast, a primary PCI is the use of a percutaneous
f d h h f T
emergent in nature.
Non-primary PCIs include elective, rescue, and salvage PCIs. In contrast, a primary PCI is the use of a percutaneous
f d h h f T reperfusion procedure in the acute phase of ST-segment elevation MI (usually within 12 hours or less from the onset of ischemic symptoms) with the goal of restoring blood flow to the affected myocardium, thereby improving outcomes including
reperfusion procedure in the acute phase of ST-segment elevation MI (usually within 12 hours or less from the onset of ischemic symptoms) with the goal of restoring blood flow to the affected myocardium, thereby improving outcomes including affected myocardium, thereby improving outcomes including reduced mortality rates.affected myocardium, thereby improving outcomes including reduced mortality rates.

Reasons for DelayReasons for Delayyy
System reasons for delay are not acceptable, regardless of any linkage to the timing of PCI/reperfusion.System reasons for delay are not acceptable, regardless of any linkage to the timing of PCI/reperfusion.
ο Equipment-related (e.g., unavailability, malfunction)
ο Staff-related (e.g., waiting for cath lab staff)
ο Equipment-related (e.g., unavailability, malfunction)
ο Staff-related (e.g., waiting for cath lab staff)
ο Participation in clinical trial (e.g., waiting for trials coordinator)
ο Consultation with other clinician
ο Cath lab unavailability (e g no open cath lab)
ο Participation in clinical trial (e.g., waiting for trials coordinator)
ο Consultation with other clinician
ο Cath lab unavailability (e g no open cath lab)ο Cath lab unavailability (e.g., no open cath lab)
• The linkage between a non-system reason and the timing/delay of PCI/reperfusion/cath/transfer to cath lab must be made clear somewhere in the medical record. Abstractors
ο Cath lab unavailability (e.g., no open cath lab)
• The linkage between a non-system reason and the timing/delay of PCI/reperfusion/cath/transfer to cath lab must be made clear somewhere in the medical record. Abstractors be made clear somewhere in the medical record. Abstractors should NOT make inferences from documentation of a sequence of events alone or otherwise attempt to interpret from documentation.
be made clear somewhere in the medical record. Abstractors should NOT make inferences from documentation of a sequence of events alone or otherwise attempt to interpret from documentation.
Clinical judgment should not be used in abstraction.Clinical judgment should not be used in abstraction.

Reasons for DelayReasons for Delay
Examples of ACCEPTABLE documentation:
“H ld n PCI Will d TEE t / ti diss ti n ”
Examples of ACCEPTABLE documentation:
“H ld n PCI Will d TEE t / ti diss ti n ”− Hold on PCI. Will do TEE to r/o aortic dissection.”
− “Patient waiting for family and clergy to arrive – wishes to consult with them before PCI.”
− Hold on PCI. Will do TEE to r/o aortic dissection.”
− “Patient waiting for family and clergy to arrive – wishes to consult with them before PCI.”
− “Pt. presented to ER in full cardiac arrest. ACLS protocol instituted. Unable to do PCI until patient stable.”
− “He had to be defibrillated several times prior to transfer to cath lab.”
− “Pt. presented to ER in full cardiac arrest. ACLS protocol instituted. Unable to do PCI until patient stable.”
− “He had to be defibrillated several times prior to transfer to cath lab.”p
− “SVG Angiojet cath did not cross lesion. XMI catheter successfully crossed the stenosis. Flow reestablished after 30 min. delay.”
“PCI delayed due to intermittent hypotensive episodes when crossing
p
− “SVG Angiojet cath did not cross lesion. XMI catheter successfully crossed the stenosis. Flow reestablished after 30 min. delay.”
“PCI delayed due to intermittent hypotensive episodes when crossing − PCI delayed due to intermittent hypotensive episodes when crossing lesion.”
o Note: Initial patient/family refusal of PCI/reperfusion/cath/transfer to cath lab is an acceptable reason for delay and does NOT need to be linked
− PCI delayed due to intermittent hypotensive episodes when crossing lesion.”
o Note: Initial patient/family refusal of PCI/reperfusion/cath/transfer to cath lab is an acceptable reason for delay and does NOT need to be linked cath lab is an acceptable reason for delay and does NOT need to be linked to the timing/delay in PCI.cath lab is an acceptable reason for delay and does NOT need to be linked to the timing/delay in PCI.
Reasons for DelayReasons for Delay
Examples of UNACCEPTABLE documentation:
− “Patient is discussing PCI with family.” (Effect on timing/delay of PCI not documented)
Examples of UNACCEPTABLE documentation:
− “Patient is discussing PCI with family.” (Effect on timing/delay of PCI not documented)documented)
− “Patient developed v fib and cardiorespiratory arrest. Defib x 2, intubated. To cath lab for PCI.” (Linkage to timing/delay of PCI not clear – Abstractor should not infer from sequence of events)
documented)
− “Patient developed v fib and cardiorespiratory arrest. Defib x 2, intubated. To cath lab for PCI.” (Linkage to timing/delay of PCI not clear – Abstractor should not infer from sequence of events)
− “ST-elevation on initial ECG resolved. Chest pain now recurring. To cath lab for PCI.” (Linkage to timing/delay of PCI not clear – requires clinical judgment)
− “Cath contraindicated – too high risk.” (Effect on timing/delay of PCI not d d)
− “ST-elevation on initial ECG resolved. Chest pain now recurring. To cath lab for PCI.” (Linkage to timing/delay of PCI not clear – requires clinical judgment)
− “Cath contraindicated – too high risk.” (Effect on timing/delay of PCI not d d)documented)
− “PCI not indicated.” (Effect on timing/delay of PCI not documented)
− “During the Angiojet thrombectomy, the patient had bradycardia which required i ” (Eff t ti i /d l f PCI t d t d)
documented)
− “PCI not indicated.” (Effect on timing/delay of PCI not documented)
− “During the Angiojet thrombectomy, the patient had bradycardia which required i ” (Eff t ti i /d l f PCI t d t d)pacing.” (Effect on timing/delay of PCI not documented)
• If unable to determine whether a documented reason is system in nature, or if physician/APN/PA documentation does not establish a linkage between event(s)/condition(s) and the timing/delay in PCI/reperfusion/cath/transfer to
pacing.” (Effect on timing/delay of PCI not documented)
• If unable to determine whether a documented reason is system in nature, or if physician/APN/PA documentation does not establish a linkage between event(s)/condition(s) and the timing/delay in PCI/reperfusion/cath/transfer to event(s)/condition(s) and the timing/delay in PCI/reperfusion/cath/transfer to cath lab, select “No.”event(s)/condition(s) and the timing/delay in PCI/reperfusion/cath/transfer to cath lab, select “No.”

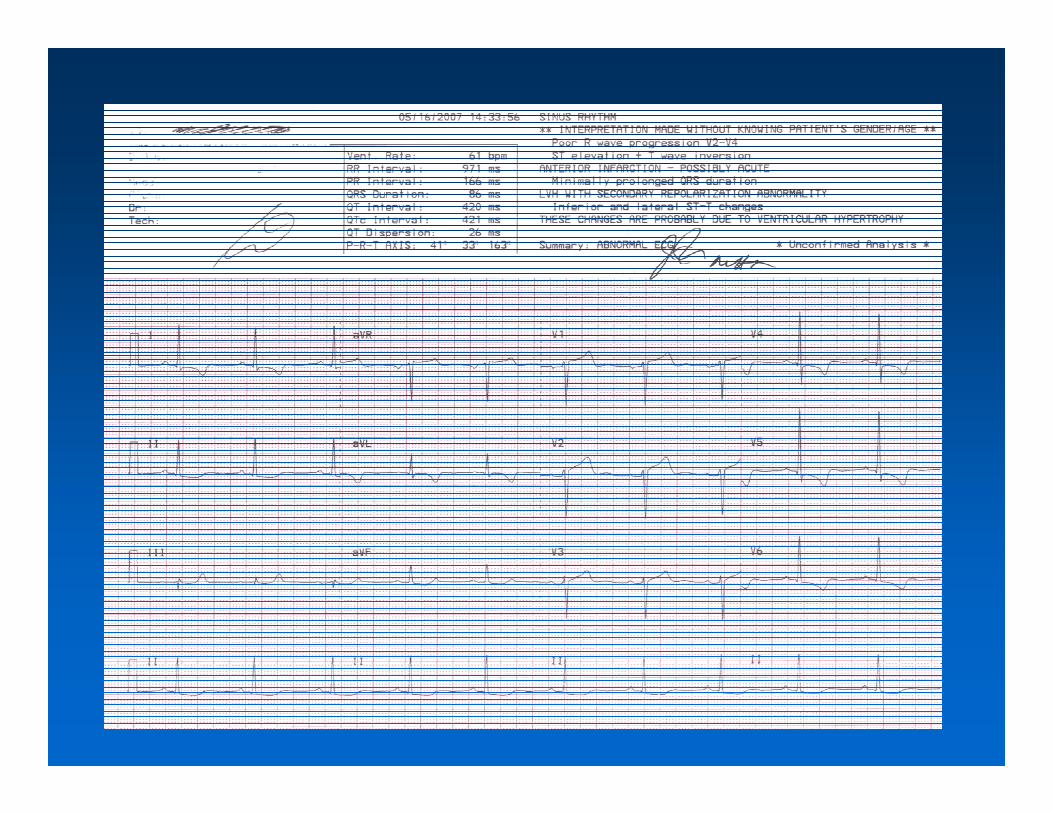
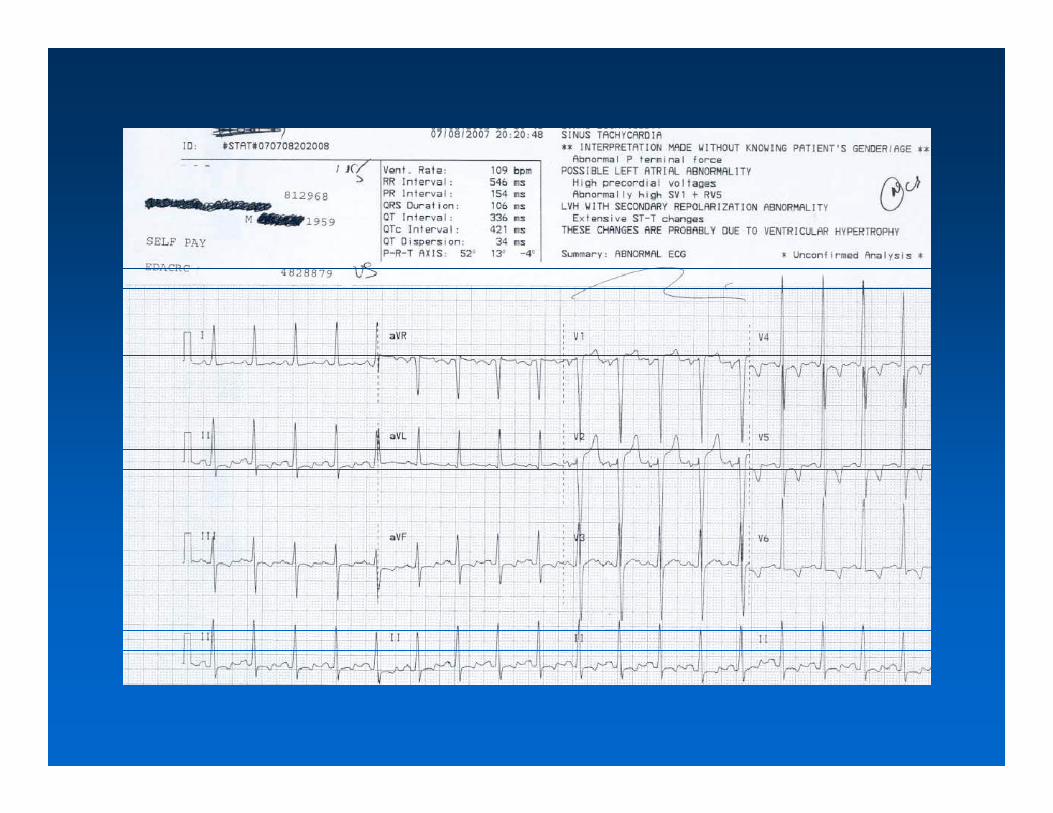
False Positive STEMIFalse Positive STEMI




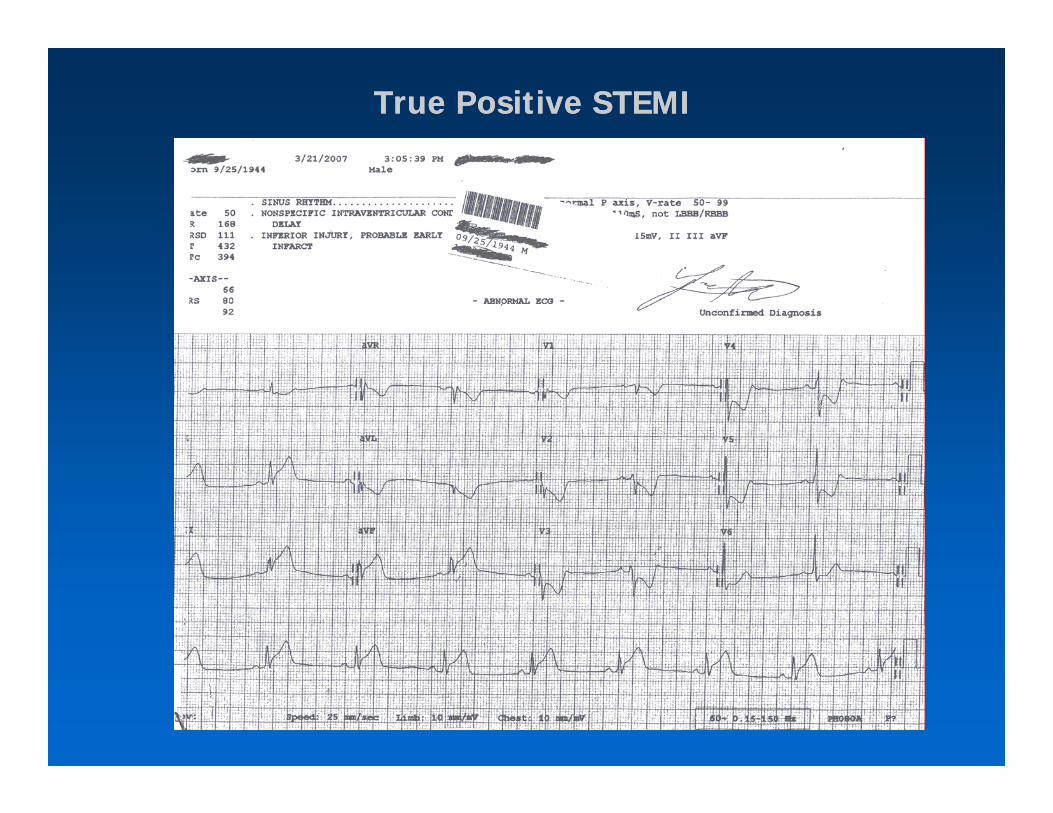
True Positive STEMITrue Positive STEMI



Reciprocal ChangesReciprocal Changes
Wall AffectedLeads Showing ST Segment Elevation
Leads Showing Reciprocal ST Segment Depression
Suspected Culprit ArteryElevation Depression y
Septal V1, V2 None LAD
Anterior V3, V4 None LAD
Anteroseptal V1, V2, V3, V4 None LADe osep a , , 3, o e
Anterolateral V3, V4, V5, V6, I, aVL II, III, aVF LAD, or CIRC
Extensive anterior (Sometimes called V1 V2 V3 V4 V5(Sometimes called Anteroseptal with Lateral extension)
V1,V2,V3, V4, V5, V6, I, aVL II, III, aVF Left Main
Inferior II, III, aVF I, aVL RCA or CIRC
L t l I VL V5 V6 II III VF CIRCLateral I, aVL, V5, V6 II, III, aVF CIRC
Posterior (Usually associated with Inferior or Lateral but can be isolated)
V7, V8, V9 V1,V2,V3, V4 PDA
Right Ventricular (Usually associated with Inferior)
II, III, aVF, V1, V4R I, aVL RCA
http://en.wikipedia.org/wiki/Myocardial_infarction


IMI due to OM1 (old total RCA); patent LADIMI due to OM1 (old total RCA); patent LAD

IMI due to proximal RCA occlusion; patent LADIMI due to proximal RCA occlusion; patent LAD
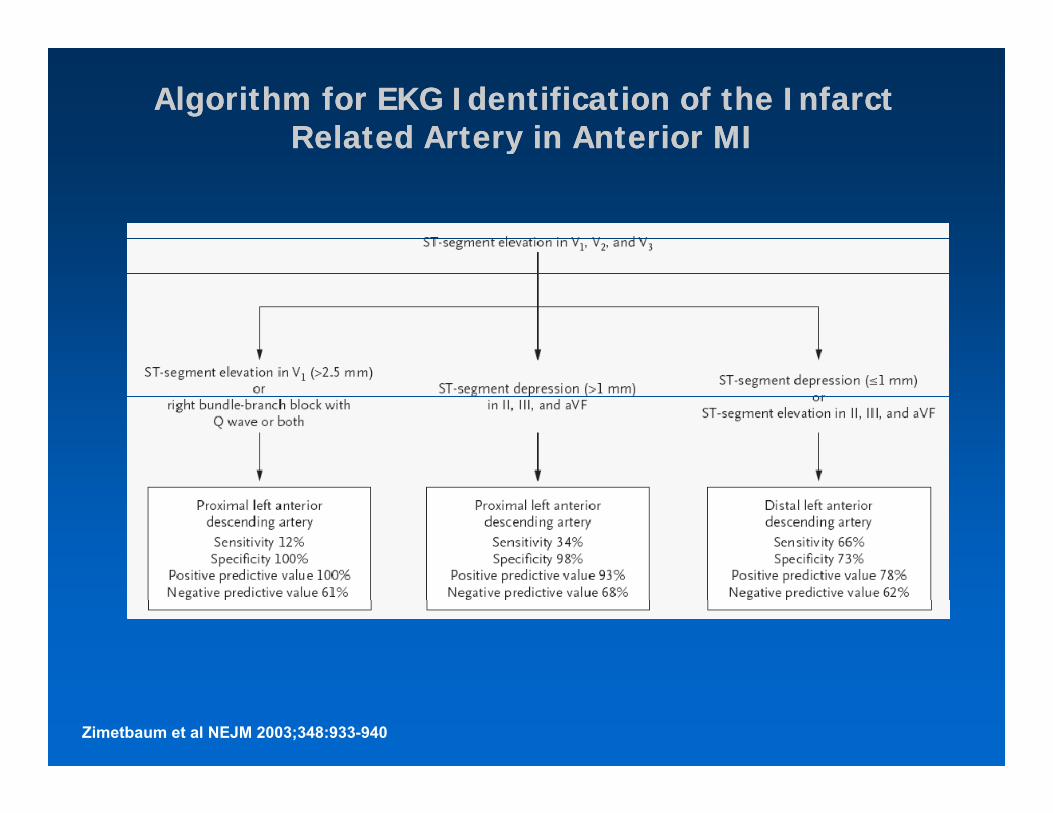
Algorithm for EKG Identification of the Infarct Algorithm for EKG Identification of the Infarct Related Artery in Anterior MIRelated Artery in Anterior MIyy
Zimetbaum et al NEJM 2003;348:933-940

Algorithm for EKG Identification of the Infarct Algorithm for EKG Identification of the Infarct Related Artery in IMIRelated Artery in IMIyy
Zimetbaum et al NEJM 2003;348:933-940


The Evolution of Optimal MyocardialThe Evolution of Optimal MyocardialInfarction Therapy 1955Infarction Therapy 1955--20002000
Eisenhower Cheney1
pypy
Year: 1955 2000
Therapy: Morphine Angioplasty/StentHeparin HeparinHeparin HeparinWarfarin AspirinAtropine Abciximab
Clopidogrelp d gβ-BlockerStatin
B d R t 7 W k 2 DBed Rest: 7 Weeks < 2 Days
Expected Mortality: 30% < 5%