steps of the shoemaker protocol for treating chronic
TRANSCRIPT

Steps of the Shoemaker Protocolfor treating
Chronic Inflammatory Response Syndrome acquired following exposure to Water Damaged Buildings [CIRS-WDB]
Werner Vosloo ND
Restorative Health Clinic 503.747.2021
http://restorativehealthclinic.com/
What is CIRS:
The 2009 “WHO guidelines for indoor air quality: dampness and mould” states that based on studies done in the United States, the prevalence of dampness or mold in houses to be approximately 50%. Inthe United Kingdom, 52% of owner occupied homes had dampness and 24% had mold, while 58% of lower income or rented homes were damp and 56% were moldy. Water damage or humidity high enough to initiate or maintain indoor microbial growth is very common.
Chronic Inflammatory Response Syndrome acquired following exposure to Water Damaged Buildings [CIRS-WDB] is a multi-system, multi-symptom illness mediated by a persistent innate immune inflammatory response to toxins, antigens, and inflammagens present in the interior environment of WDBs. These contaminants include but are not limited to fungi, bacteria, actinomycetes, mycobacteriaand their toxins; as well as inflammagens from fragments of fungal structures. [beta glucans, mannans, hemolysins, proteinases, spirocyclic drimanes and microbial volatile organic compounds (VOCs)].
Many patients acquire CIRS following exposure to a WDB after water intrusion followed by presence of either:
1) visible microbial growth;2) speciation of molds as demonstrated by ERMI or HERTSMI [QPCR DNA] testing; or3) musty smells.
Other biological sources of biotoxins and neurotoxins that are recognized as causes of CIRS include tick borne illnesses including Lyme disease, dinoflagellates like Pfiesteria, blue green algae like Cylindrospermopsis and Microcystis and also Ciguatera.1, 2, 3, 10, 11, 12, 13
The inflammatory domino cascade:
The innate and adaptive immune systems normally function together to remove biotoxins from the body: immune pattern recognition by the innate immune system lead to antibody formation through a complex multi-step process. Antibodies bind to offending substances, leading to their clearance from the body. Clearance of offending biotoxins lead to cessation of innate immune system driven inflammation and not getting sick from biotoxins, like mold particulates and mycotoxins.
Genetically susceptible people have a problem with the production of protective antibodies. Offending material left in the body will be detected by the innate immune system in a continuous manner, resulting in a chronic inflammatory response. This ongoing inflammation leads to recruitment of additional immune inflammatory pathways. The same is true for when there is ongoing exposure.
1

Hypothalamic regulation is significantly affected: cytokines damage leptin receptors which leads to reduced MSH, VIP and ADH production. Hypothalamic dysregulation is linked to many of the problematic symptoms in numerous body system.2,11,16
Symptoms of CIRS:
Differential inflammatory responses dependent on individual genetic susceptibility drives the symptomatic presentation of CIRS. Dr. Shoemaker's research revealed that CIRS patients can have 13 different clusters of symptoms. Dr. Shoemaker recommends that if a patient has symptoms present in 6 or more of the symptom clusters, biotoxin illness is possible and further testing and evaluation must be done. Symptoms in 8 ormore clusters is consistent with biotoxin illness.
The summary diagram below, by Dr. Yvonne Berry MD, represents the 13 symptom clusters identified by Dr Shoemaker through his research.2,4,11
2
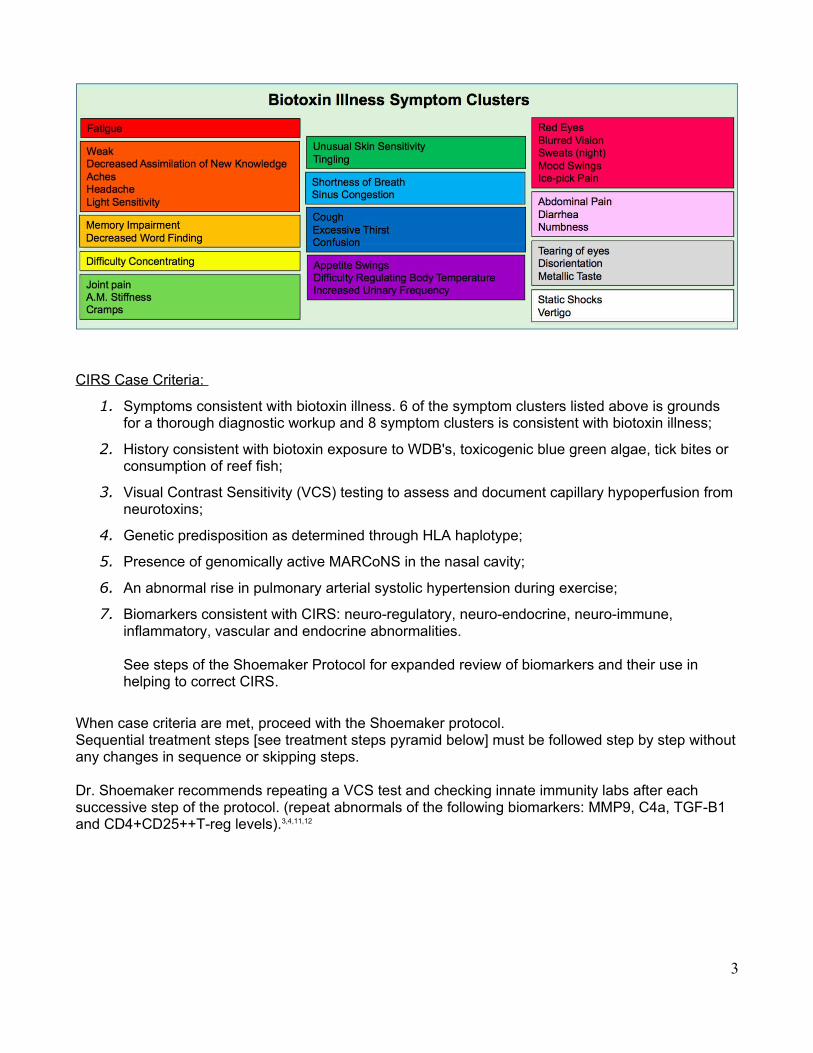
CIRS Case Criteria:
1. Symptoms consistent with biotoxin illness. 6 of the symptom clusters listed above is grounds for a thorough diagnostic workup and 8 symptom clusters is consistent with biotoxin illness;
2. History consistent with biotoxin exposure to WDB's, toxicogenic blue green algae, tick bites or consumption of reef fish;
3. Visual Contrast Sensitivity (VCS) testing to assess and document capillary hypoperfusion from neurotoxins;
4. Genetic predisposition as determined through HLA haplotype;
5. Presence of genomically active MARCoNS in the nasal cavity;
6. An abnormal rise in pulmonary arterial systolic hypertension during exercise;
7. Biomarkers consistent with CIRS: neuro-regulatory, neuro-endocrine, neuro-immune, inflammatory, vascular and endocrine abnormalities.
See steps of the Shoemaker Protocol for expanded review of biomarkers and their use in helping to correct CIRS.
When case criteria are met, proceed with the Shoemaker protocol. Sequential treatment steps [see treatment steps pyramid below] must be followed step by step withoutany changes in sequence or skipping steps.
Dr. Shoemaker recommends repeating a VCS test and checking innate immunity labs after each successive step of the protocol. (repeat abnormals of the following biomarkers: MMP9, C4a, TGF-B1 and CD4+CD25++T-reg levels).3,4,11,12
3

Step 1
Remove from exposure and decrease ERMI below 2.
Normal range: ERMI <2 or HERTSMI 2 <10
Objective – remove from source of inflammagen exposure
Removal from the perceived major eliciting and maintaining cause of chronic inflammatory illness is the single most important and first step in treating CIRS-WDB and other biotoxin illness.
Testing for exposure is most accurately and economically done with the Environmental Relative Mold Index ERMI test through http://mycometrics.com/. Four to six weeks after the completion of mold remediation work, Dr. Shoemaker advises either repeating an ERMI or doing a HERTSMI-2 test.
ERMI or HERTSMI-2 documents fungal DNA in patients environment through quantitative surface dustPCR analysis. Fungal DNA in surface dust is used as an indicator of what was present in the air at an earlier time. The EPA released the ERMI test in 2006. Fungal fragments and spores that were in the air and then settled in dust are relevant in the causation of CIRS, establishing that CIRS is more than a mold or biotoxin illness.
Measurements: When C4a is below 20,000 and MSH is less than 35 the building ERMI score must be below 2.
When C4a exceeds 20,000 and MSH is below 35 the ERMI needs to be -1 to improve the response to treatment due to lower exogenous exposure.
4
Step 2
Binders: CSM / Welchol
Normal range: VCS passed
Objective: Reduce circulating biotoxin burden
Cholestyramine is a cholesterol lowering medicine that binds an ammonium side chain to anion ring formations of biotoxin molecules in the small intestine and decreases the amount of bile plus biotoxins reabsorbed back into the bloodstream from the small intestine. Approximately 95% of bile [in which many biotoxins are released] is reabsorbed in the lower small intestine, making our bodies VERY ineffective at eliminating small molecular size biotoxins. Only 5% of bile and thus likely biotoxins exit the body through stool with each go-around. This means that in the 24% of CIRS susceptible people, the reabsorption and recirculation of bile plus biotoxins will be cause for a sustained inflammatory illness.
The safety and simplicity of Step 2 is genius – sequester and remove inflammagens with a resin or glue like substance and reduce inflammatory recruitment.
Interruption of bile reabsorption 4 times per day yields better results in active treatment phases, thus 4doses of bile binders per day is mandatory for satisfactory results.
Cholestyramine is a very effective bile binder. It must be taken on an empty stomach esp away from prescription medicines. Four doses on an empty stomach may be a challenge if someone is already on a demanding dosing schedule. Alternatively taking only 2 doses of CSM on an empty stomach and 2 doses of Welchol 2 tablets per dose with two meals enables 4 opportunities to bind biotoxins in a more manageable manner.
Cholestyramine doses should ideally be 4 grams per dose, Welchol 625mg tablets. For sensitive patients, compounded CSM is available from compounding pharmacies in both powder and capsule form.
Side effects include heartburn / reflux and constipation which can be counteracted with salts of magnesium without compromising the binding capacity of CSM. It is essential to manage GI transit to avoid constipation. Starting with smaller doses and increasing dose size and frequency as your body demonstrates tolerance is advised in certain circumstances.
In select patients [Lyme disease with elevated MMP9 and patients with ongoing mold and biotoxin exposure] biotoxin binding may cause a systemic inflammatory flare with exacerbation of symptoms. This can be attenuated with pre-treatment for 5 or more days with the low amylose diet and high dose fish oil [enteric coated by preference] consisting of 2.4 grams EPA and 1.8 grams EPA per day, with meals. Actos is more effective, but used only if fish oil is not effective enough. Due to the leptin lowering effectof Actos, high dose Omega-3 fatty acids are preferred over Actos in patients with leptin < 7. Actos has a bladder cancer black box warning. Monitoring guidelines includes baseline and follow up liver function testing.
Objective measurement: The VCS test is an objective measurement to track the effect of binders – doses of binders may be decreased once the VCS is passed and patient is in a safe environment.
5

Step 3
Eradicating MARCoNS with BEG nasal spray
Normal range: no MARCoNS present
Objective: Remove biofilm dwelling resistant staphylococci that keep MSH low
When MSH is low, MARCoNS are present in more than 80% of cases. Less than 2% of patients with normal MSH has MARCoNS present. Diagnostic screening API Staph nasal swab is indicated in all cases with low MSH. In patients under 15 yo this can be done at clinicians judgement, due to there being a lesser MARCoNS incidence.
Low MSH, with resultant decrease in mucosal immune function appears to be correlated with the presence of MARCoNS. When present, MARCoNS secrete exotoxins A and B from biofilm communities which shelters microbes against body defenses and antibiotics.
One month after starting bile binding therapy, one can start with BEG nasal spray [Bactroban (Mupirocin) 0.2%, Edetate Disodium (EDTA) 1%,Gentamicin 0.5%] 2 sprays per nostril three times perday. Lidocaine nasal spray may be used prior to BEG spray doses to reduce treatment discomfort. Discomfort from the spray, nosebleeds, swelling and congestion resembling sinusitis may be experienced during MARCoNS eradication treatment with BEG nasal spray.
Rifampin 300 mg bid for 1 month may be used in resistant cases, though care should be taken as Rifampin is not intended for routine use and has a higher incidence of side effects as compared to the commonly used antibiotics. EDTA in BEG spray chelates structural minerals out of biofilm structures to enable better antibiotic penetration.
After 4 weeks of treatment, the API Staph culture needs to be repeated to demonstrate eradication.
Step 4
Correct elevated serum anti-gliadin antibodies through avoidance of gluten
Normal Range: 0-19 AGA IgA / IgG
Objective: eliminate further inflammation in an already upregulated immune system by avoiding gluten
Loss of immune tolerance through decreased MSH, elevated TGF-B1 and decreased T-regulatory cells lead to antibody formation to gluten and gliadin. This means more inflammation.
Laboratory test confirmation is helpful - serum IgA and IgG anti-gliadin antibodies should be checked. If the anti-gliadin antibodies are positive, there is immune loss of tolerance with resultant inflammatory dysfunction to gluten exposure. If positive anti-gliadin antibodies are present, check a tTG-IgA / IgG (tissue transglutaminase IgA / IgG) to rule out true celiac disease.
Treatment is a 100% gluten free diet for at least 3 months with retest to confirm antibodies are negative.
6
Step 5
Correct Androgen levels
DHEA/Testosterone – varied reference ranges for age/gender
Objective: endocrine support, especially adrenal and gonadal
Increased cytokines and leptin levels causes hypothalamic dysfunction with resultant neuro-endocrine dysfunction.
Pregnenolone [often below detection threshold to lower normal range in biotoxin patients] and DHEA are the precursors for cortisol and testosterone. CIRS patients increase estrogen production from testosterone through higher aromatase activity, with resultant higher estrogens and lower androgens.
Baseline testing should include androstenedione, DHEA, testosterone and estradiol.When supplementing with DHEA, repeat testing should be performed at 4-8 week intervals until serumlevels are in the normal range.
Due to increased aromatase activity observed in CIRS, estradiol levels must be measured as well.
Refrain from administering exogenous testosterone if possible.
Retesting at 3 month or more frequent intervals is important in the initial stages of treatment to ensure intended effects and identify faulty conversion.
VIP nasal spray corrects aromatase overactivity.
Step 6
Correct ADH/osmolality
Normal Range: ADH - 1.0-13.3 pg/ml; Osmolality [280-300 mOsm Quest] [275−295 mOsm LabCorp]
Objective: correct blood osmolality
Neurotoxicity in CIRS and Lyme-complex illness patients often have low to below detection threshold AVP/ADH levels with resultant increased serum osmolality [too concentrated and “thick”]. Patients typically complain of increased thirst, dry mouth and frequent urination of typically clear urine. Salt levels in blood rises as you loose free water due to lack of ADH mediated reabsorption in the kidneys. Sweat will have increased sodium/chloride [exceeding cystic fibrosis] with resultant generation of staticelectricity and static shocks.
Serum hyperosmolality with resultant cellular osmotic dehydration coupled with inadequate perfusion can cause headache/migraines, cramps in especially the legs and feet.
Lab testing and findings may include low normal to below detection threshold ADH/AVP, high normal to high serum osmolality.
In order to enable better hydration, the pharmaceutical analogue of ADH, desmopressin may be used with caution. Desmopression / DDAVP 0.2mg every other night for two weeks.
Retesting every two weeks: ADH and osmolality and serum sodium - over-treating or over-hydration will cause both to be low. Weigh every few days to detect any weight gain, check hands and feet for edema from water retention.
7

Step 7
Correct MMP-9 [Matrix Metalloproteinase 9]
Normal Range: 85-332 ng/mL
Objective: decrease enzyme levels associated with inflammation
Cytokines activate receptors that cause release of MMP-9 from white blood cells and endothelial cells into the blood-stream. It represents a summation of inflammatory responses and pathways in the bodyespecially in the brain, nerves, muscles, lungs, and joints.
Treatment consists of the low amylose diet in conjunction with high dose fish oil [2.4 grams of EPA and 1.8 grams of DHA per day] to decrease inflammation, pain and dysfunction.
Step 8
Correct low VEGF [Vascular Endothelial Growth Factor]
Normal Range: 31-86 pg/mL
Objective: improve oxygen delivery to cells
Low VEGF contributes to oxygen deprivation at the core of CIRS-WDB. VEGF improves capillary blood flow and supports new blood vessel formation. When VEGF is low, tissue oxygenation may be low, which compromises aerobic energy production.
Treatment consists of the low amylose diet in conjunction with high dose fish oil [2.4 grams of EPA and 1.8 grams of DHA per day].
Step 9
Correct elevated C3a
Normal Range 55-486 ng/mL
Objective: improve oxygen delivery to cells and decrease inflammation
C3a is a product of split complement present in only some biotoxin illness patients. When C3a is present, revisit other potential differential diagnoses, which must include acute Lyme disease22 or SLE 23. C3a is one of the more potent factors of the complement system. C3a attracts andactivates neutrophils to release their granules, which causes capillary under perfusion, vasoconstriction, increased vascular permeability.24 The bottom line is that C3a promotes pathological inflammation.24 There is significant overlap symptomatically between Lyme-complex illness and CIRS-WDB.
High dose statins decrease T-cell activation, macrophage activation and vascular wall inflammation in addition to the perceived effects on cholesterol.
Statins can cause side effects. Reduce the chances of statin induced side effects with pre-treatment for at least 10 days with ubiquinone, also known as CoQ10 150mg or more per day and monitoring of CK.
8

Step 10
Correct elevated C4a
Normal Range 0-2830 ng/mL
Objective: improve oxygen delivery to cells and decrease inflammation
C4a is a very important and frequently encountered marker of CIRS-WDB that is a useful indicator of the degree of inflammation and also treatment response. When high, C4a causes cognitive dysfunction, increased smooth muscle contraction, vascular permeability, release of chemotactic factors followed by capillary hypoperfusion and low tissue oxygen.
Without adequate oxygen and nutrients in the cells, energy production is compromised with a decrease in ATP yield from 38 ATP down to 2 ATP per glucose molecule. This is an 18 fold decrease, literally requiring 18 glucose molecules during low oxygen conditions to generate 38 ATP. Post exertional fatigue is a characteristic observation of CFS/ME – 2-3 days of fatigue [glycogen depletion] following exertion. In other words, the cell burns through its glucose stores [glycogen] and it takes a few days to replace. Lactic acid production increases, causing post exertional myalgia.
C4a responds well to VIP nasal spray. Before the use of VIP, erythropoietin (Procrit) injections were used with good results. Procrit has a black box warning, avoid use if any of the contraindicated conditions are present.
Step 11
Correct elevated TGF-B1 (Transforming Growth Factor Beta 1)
Normal range Normal Range: <2380 pg/ml
Objective: restore immune regulation and balance
TGF-B1 is an important and frequently encountered marker of biotoxin illness. It has regulatory functions in many immune pathways and tissues. It is involved in development, proliferation, angiogenesis, regulation of inflammation, extracellular matrix production, protease activity and apoptosis.
TGF-B1 has a bipolar action in that it both suppresses ongoing immune responses and also drives an over active innate response. It depresses the function of innate cells like NK cells.
TGF-B1 impairs normal T-regulatory cell function. T-reg cells help to prevent auto-immunity, therefore elevated TGF-B1 suppresses protective immune mechanisms. TGF-B1's lowering of CD4+CD25++ Treg cells lead to the formation of pathogenic effector T-cells which induces release of more TGF-B1. This enhances the Th 17 response by differentiating naive T cells into IL 17 secreting Th 17 cells. The Th 17 response leads to loss of recognition of self and increased development of autoantibodies, it is strongly associated with inflammatory disorders.
TGF-B1 affects DNA replication; epithelial to mesenchymal transformation (fibrosis in the lung mostly, also in kidney and liver); and is associated with alopecia.
TGF- B1 stimulates production of types I and IV collagen and fibronectin, stimulates calcium ion influx into cells and also fibrosis where tissue cells differentiate into fibroblasts. TGF-B1 is implicated in connective tissue disorders like Marfan's syndrome and Ehlers Danlos type III.
9
A study of vasogenic brain edema and blood brain permeability linked TGF-B1 to increased MMP-9 in a dose dependent manner. Reducing TGF-B1 reduced blood brain permeability.8
In pulmonary arterial hypertension and pulmonary fibrosis, TGF-B1 mediates both the vascular and fibrotic changes. It is associated with disease progression in chronic conditions.
TGF-B1 is cleared from circulation by the liver.
The HLA haplotypes 4-3-53 and especially 11-3-52B typically has high levels of TGF-B1.2, 4,6,7,8,15,16,17
The two treatment options for elevated TGF-B1 is oral losartan [with minimal blood pressure lowering effects in most cases at 25mg twice per day] or the use of VIP nasal spray.
Losartan is started at 12.5mg per day, and increased to 25mg twice per day per day if tolerated well. Ametabolite of losartan called EXP 3179 lowers TGF-B1.
In an animal model of exercise induced myocardial injury leading to fibrosis, Losartan reduced mRNA expression for TGF-B1 to control levels and prevented coronary arteriole medial thickening, perivascular and myocardial fibrosis.5
Step 12
Correct low VIP [Vasoactive Intestinal Polypeptide]
Normal Range 23-63 pg/mL
Objective: restore neuro-regulation to re-establish normal systems function
Vasoactive intestinal polypeptide is a neuro-immune modulator that restores immune regulation. VIP nasal spray is the final restorative measure of the 12 step Shoemaker recovery program once patientsare properly prepared by the previous 11 steps of the protocol.
VIP reduces inflammatory markers including TGF-B1, regulates dendritic cells (APC's that mediates between the innate and adaptive immune systems) and enhances IL-10 production. Most importantly, VIP restores T-reg numbers and therefore restores regulation of the Th 17 autoimmune response. VIPrestores hormone levels including Vit D, corrects overactivity of aromatase and thereby improves estrogen and testosterone levels and ratio's, raises cAMP levels which improves cell signaling, lowers pulmonary artery systolic pressure to exercise, blocks peripheral innate immune system activation, raises VEGF, corrects ADH/osmolality, restores circadian rhythm.
Abnormal genomic transcription associated with CIRS-WDB is normalized by VIP.
Pulmonary artery hypertension, as measured by echocardiography of tricuspid valve regurgitation, is associated with lower levels of serum VIP. Treatment with VIP leads to relaxation of pulmonary vascular smooth muscle cells with improved and normalized pulmonary arterial hypertension. Shortness of breath and exercise intolerance improves after correction of PASP.
VIP deficiency occurs in 98% of CIRS-WDB patients and in less than 10% of normal controls, making it a very reliable biometric.3,11,18,19
Dr Shoemaker published a study in 2013 from research done on CIRS-WDB patients. This study demonstrates that the use of VIP nasal spray:
1) safely reduced refractory symptoms to control levels
2) corrected inflammatory parameters C4a, TGF beta-1, VEGF and MMP9 to be similar to controls;
10
3) raised levels of VIP and MSH;
4) returned PASP during exercise to normal;
5) corrected estradiol, testosterone and 25-OH Vitamin D levels;
6) corrected T-reg levels;
7) enhanced quality of life in 100% of patients in this study.
Important requirements for starting VIP:
1. VCS passed
2. No further exposure with ERMI <2 or HERTSMI 2 <10
3. MARCoNS negative on API Staph nasal culture
4. Normal serum Lipase levels
VIP first dose administration: has to be in office with pre and 15min post administration blood testing toensure safety and also to measure the magnitude of positive response.
Pre-VIP administration labs: (VIP, MSH, C4a. TGF beta-1, MMP-9, VEGF and lipase).
15 min Post-VIP 50mcg x1 intra nasal administration labs: (TGFB-1, Lipase). Observe any hyper acute changes in symptoms and understand contraindications for continuing VIP: if patient develops abdominal pain and lipase level elevates above range, stop VIP treatment.
30 days Post-VIP commencement labs: stress echo for PASP, lipase, C4a, TGF beta-1, VCS, change in symptoms, hydration, BP.
When symptoms improve, TGF-B1 levels are stable, VCS is normal and lipase is stable, decrease VIPspray to 50mcg twice per day x 30d;
Recheck for abdominal pain and lipase levels, VCS normal, then decrease Rx VIP 50 mcg per spray daily X 30 days, then discontinue.
6 months re-evaluation: re-check stress echo for any changes in PASP, lipase, VCS.
Repeat VCS annually.
Managing re-exposure:
Avoiding re-exposure is essential to remain well and to prevent getting sick again. Re-exposure of previously affected patients will bring about immunological host responses that are enhanced in their rapidity of onset and magnitude. These patients are “sicker, quicker.”
Upon re-exposure, follow the following steps to prevent complete relapse and decrease recovery time.
Step 1 – Treat with CSM/Welchol to return patient to control lab values.
Step 2 – Stop all binders and biotoxin medicines and ensure patient is in a safe environment. 3 days after stopping, retest VCS and C4a, leptin, MMP9, TGF-B1, VEGF, von Willebrand's profile.
Step 3 – Stay off binders and Shoemaker protocol medicines if stable.
11

Re-Exposure Trial:
The re-exposure protocol is used for patients identified as cases for whom proof of causation of illnessis needed in a specific building.
A re-exposure trial can be done as outlined by instructions below:
1. At an endpoint of the initial therapy with CSM, called “after CSM first time” (AC-1) draw labs including C4a (not LabCorp), TGF beta-1, MMP9, leptin, VEGF and CD4+CD25+ (not LabCorp). Using von Willebrand’s profile is great too as long as LabCorp isn’t doing the assay.
2. Stop all treatment medications, (cholestyramine/Welchol), and remain away from the suspected moldy building for 3 days. At the end of this 3 day period, document your symptoms, do a Visual Contrast Sensitivity (VCS) test, and obtain the same labs as in AC-1. This step is called “home, off CSM” (HOC). This step looks at the “ubiquitous fungi of the world.” Record your different exposures.
3. Stay off meds. The next steps test the effect of returning to the suspect building without use of any medications for 8 hours. The morning after your first day in building, document symptoms and obtain laboratory studies. (BOC-1)
4. Return to the building for the 2nd 8-hour day. Have the same blood tests done again the following morning before returning to the building for the 3rd day. Record your symptoms. This is (BOC-2).
5. The morning after the 3rd day’s exposure, document symptoms and obtain laboratory studies (BOC-3).
6. Restart all medications. Call us to tell us the re-exposure trial is completed. Send your symptoms roster and VCS scores to the office. We will score your lab results and forward those to you.
7. A second treatment will follow, with more labs to be done to confirm return to AC-1 health. Theresults of the second round of CSM are called AC-2 (after 2nd course CSM). The same labs, symptoms and VCS will be repeated.
8. You will need to set up a phone call to go over the results of your re-exposure trial.14
Summary of WDB exposure response sequence biometrics:
If the suspected building is a cause of CIRS-WDB, the following biometric response sequence is observed. See the table below, put together by Dr. Yvonne Berry MD, for a more complete list of response details:
Day 1: C4a elevation, TGF-B1 increases, Factor VIII clotting protein decreases
Day 2: Leptin elevation, MMP-9 elevation, VCS abnormal, VEGF decreases
Day 3: MMP-9 elevation, VCS abnormal, VEGF returns to nadir, Factor VIII normalizes
Day 4: decreased von Willebrand's factor with bleeding often on Days 3 and 4, VCS abnormal. 2,4,11,21
12

References:
1. Berndtson K, McMahon SW, Ackerley M, Rapaport S, Gupta S, Shoemaker RC. Medically sound investigation and remediation of water-damaged buildings in cases of chronic inflammatory response syndrome. Jan 2016
2. Shoemaker RC. Surviving Mold: Life in the Era of Dangerous Buildings. Otter Bay Books: Baltimore, 2010
3. Shoemaker RC, House D, Ryan J. Vasoactive intestinal polypeptide (VIP) corrects chronic inflammatory response syndrome (CIRS) acquired following exposure to water-damaged buildings. Health, 2013; 5(3): 396-401
4. Berry Y. A Physician’s Guide to Understanding & Treating Biotoxin Illness. April 3, 2014 Based on the work of Ritchie Shoemaker, M.D. Reviewed by Ritchie Shoemaker, M.D.
5. Gay-Jordi G, Guash E, a Benito B, Brugada J, Natte S, Mont L, Serrano-Mollar A. Losartan Prevents Heart Fibrosis Induced by Long-Term Intensive Exercise in an Animal Model. PLoS One. 2013; 8(2): e55427
6. Schnaper HW, Hayashida T, Hubachak SC, Poncelet AC. TGF- signal transduction and mesangial cell fibrogenesis. Am J Physiol Renal Physiol 2003 Feb;284(2):F243-52
7. Wahl, SM. Transforming growth factor-beta: innately bipolar. Curr. Opin. Immunol. 2007 Feb;19(1):55-62
8. McMillin MA, Frampton GA, Seiwell AP, Patel NS, Jacobs AN, DeMorrow S. TGF-B1 exacerbates blood-brain barrier permeability in a mouse model of hepatic encephalopathy via upregulation of MMP9 and downregulation of claudin-5. Lab Invest. 2015 Aug;95(8):903-13
9. Rusthoven J. Aalderink M, Scotter EL, Oldfield RL, Bergin PS, Mee EW, Graham ES, Faull
RLM, Curtis MA, Thomas I-H. Park T I-H, Dragunow M. TGF-B1 regulates human brain pericyte inflammatory processes involved in neurovasculature function. Journal of Neuroinflammation 2016 13:37
13

10. Hope J. A Review of the Mechanism of Injury and Treatment Approaches for Illness Resulting
from Exposure to Water-Damaged Buildings, Mold, and Mycotoxins. Environmental Medicine February 2013
11. Shoemaker RC, Mark L, McMahon S, Thrasher JD, Grimes C. Research Committee Report on
Diagnosis and Treatment of Chronic Inflammatory Response Syndrome Caused by Exposure to the Interior Environment of Water-Damaged Buildings. July 27, 2010
12. GAO. INDOOR MOLD Better Coordination of Research on Health Effects and More Consistent
Guidance Would Improve Federal Efforts. September 2008
13.WHO. World Health Organization guidelines for indoor air quality: dampness and mould. 2009
14. Shoemaker RC. Repetitive Exposure Protocol: CIRS-WDB Conference 2014. Document
provided as part of physician information packet. CIRS-WDB Conference 2014
15. Hartigan-O'Connor DJ, Hirao LA, McCune JM, Dandekar S. Th17 cells and regulatory T cells in
elite control over HIV and SIV. Curr. Opin. HIV/Aids. 2011 May;6(3):221-7
16. Zambrano-Zaragoza JF, Romo-Martinez EJ, Duran-Avelar MJ, Garcia-Magallanes N, Vibanco-
Perez N. Th17 Cells in Autoimmune and Infectious Diseases. Int J Inflam. 2014; 2014: 651503
17. Chen Z, O’Shea J. Th-17 cells: a new fate for differentiating helper T cells. Immunol. Res.
2008;41(2):87-102
18. Leuchte HH, Prechtl C, Callegari J, Meis T, Haziraj S, Bevec D, Behret J. Augmentation of the
effects of vasoactive intestinal peptide aerosol on pulmonary hypertension via coapplication of a neutral endopeptidase 24.11 inhibitor. Lung Cellular and Molecular Physiology 15 March 2015 Vol. 308 no.6
19. Nauser TD, Stites SW. Diagnosis and treatment of pulmonary hypertension. Am. Fam.
Physician. 2001 May 1;63(9)
20. Lafaytis R. Transforming Growth Factor Beta – at the center of systemic sclerosis. Nat. Rev.
Rheumatol. 2014 Dec;10(12)706-19
21. Shoemaker RC, House DE. Sick building syndrome (SBS) and exposure to water-damaged
buildings: Time series study, clinical trial and mechanisms. Neurotoxicology and Teratology 28 (2006) 573-588
22. Shoemaker RC, Giclas PC, Crowder C, House D, Glovsky MM. Complement split products
C3a and C4a are early markers of acute lyme disease in tick bite patients in the United States. Int Arch Allergy Immunol 2008;146:255–261
23. Stricker RB, Savely VR, Montanya NC, Giclas PC. Complement split products C3a and C4a in
chronic lyme disease. Scandinavian Journal of Immunology. 2009 Jan;69(1):64-9
24. Huether SE, McCanse KL. Understanding Pathophysiology, 5th edition. Elsevier Mosby 2012
25. Peng Q, Li K, Sacks SH, Zhou W. The role of anaphylatoxins C3a and C5a in regulating innate
and adaptive immune responses. Inflamm Allergy Drug Targets. 2009 Jul;8(3):236-46
14