stone disease evaluation in pathology laboratory: current prospective
DESCRIPTION
Urinary Stone disease is painful and destructive disease. It has a bad habit of recurrence. Patients need to be thoroughly investigated and now due to advancements in laboratory, it is possible to know exact cause of stone formation in about 90% cases. This helps in focal prophylactic treatment to effectively stop recurrence.TRANSCRIPT
Dr. Sanjeev Mehta Dr. Sanjeev Mehta MDMD
Metabolic and Renal Stone Analysis : Current prospective
Uro Lab. 1
Stone disease evaluation in Laboratory
• Series of tests to identify underlying causes.
1.Identify treatable metabolic abnormality
2.Identify underlying medical disease that predisposes to stone formation.
3.Outline a treatment plan ; focal
Uro Lab. 2
Why Do Kidney Stones Form?
• Reasons: Gnetic/dietary/Environmental• Urine is supersaturated• 2009: Supersaturation can be “fix” • Therefore, our job is to figure out what is
causing the urinary Supersaturation and
How best to fix it!
Uro Lab. 3
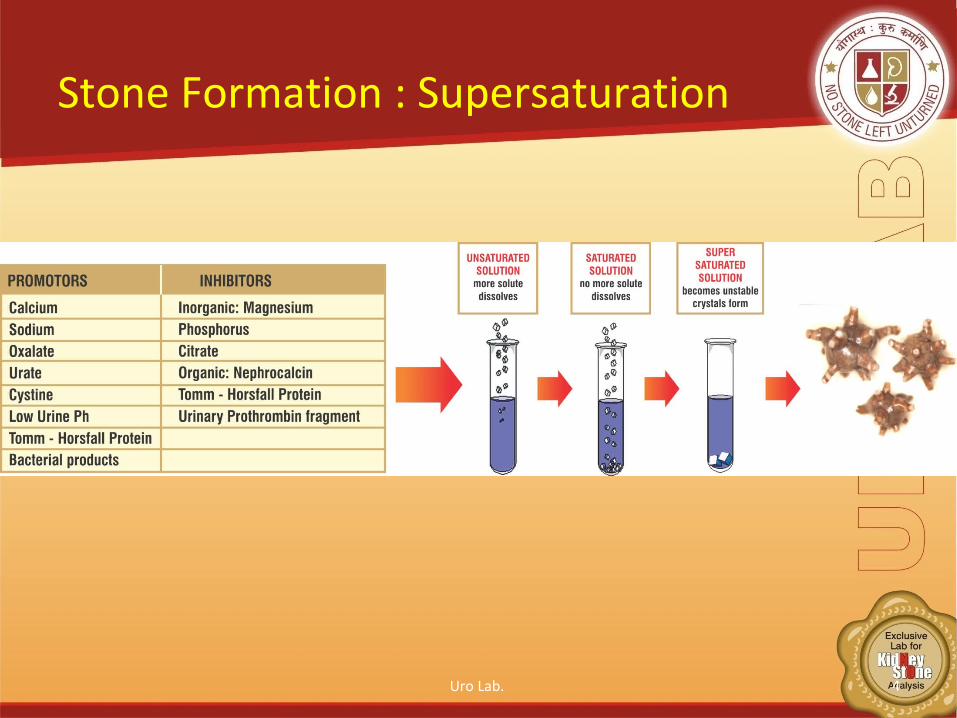
Stone Formation : Supersaturation
• k
Uro Lab. 4
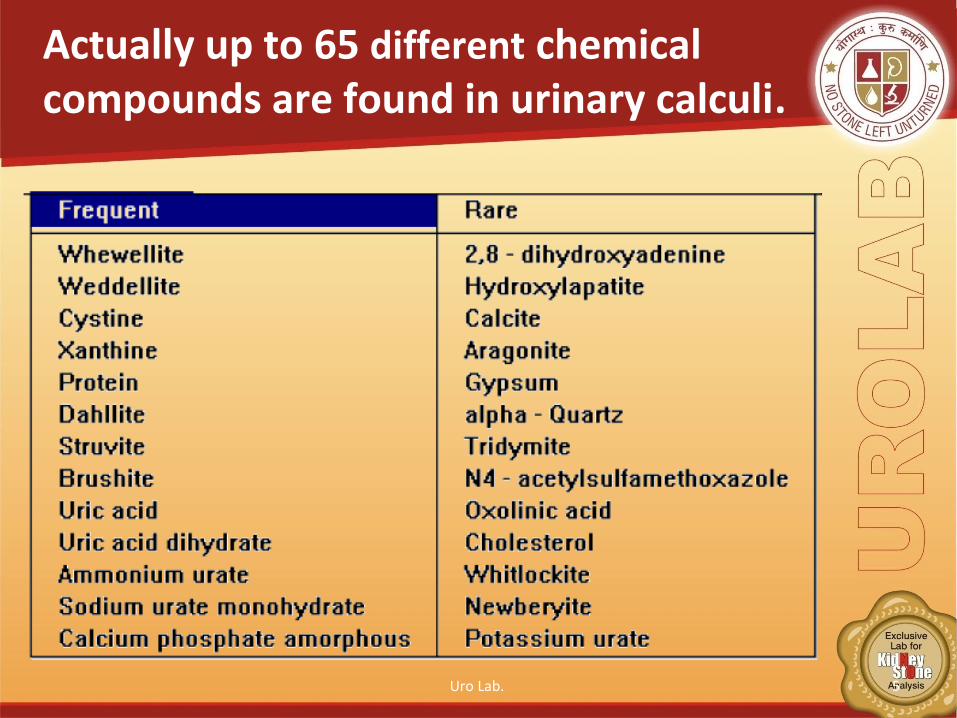
Actually up to 65 different chemical compounds are found in urinary calculi.
Uro Lab. 5
Metabolic evaluation
• Blood and Urinary Tests ; routine• Stone Analysis• 24 hrs Urinary Metabolic Profile with
SUPERSATURTION.
New advances in Stone analysis, Blood and Urinary Chemical analysis can find out 90-95% cause.*
* Preminger G.M., “Guidelines for medical management of urolithiasis”, bussin. meet us kid and urol dis,2005
Uro Lab. 6
Evaluation : First time stone with low risk• Blood screen;
Low K and HCO3, High Chloride - RTA
High Uric acid - gouty diathesis
High Calcium - Pri. Hyperparathyroidism
Low Phosphorus – Renal phosphate leak.
• Stone analysis ; all cases
Uro Lab. 7
Evaluation: First time stone
• Urine
Urinalysis : Routine
pH > 7.5 - infection lithiasis
pH < 5.5 - Uric acid lithiasis
Sediments for crystalluria
Urine culture :
Urea-splitting organisms – infection lithiasis.
Screening / quantitative CystineUro Lab. 8
24 hrs Urine metabolic profile ; Extensive
Uro Lab. 9
24 hrs extensive Metabolic evaluation: indications
• Stone recurrence• Motivated patients wants to investigate.• Select one-time formers:
- Solitary Kidney
- Renal insufficiency.- Residual stone burden.• All children
Uro Lab. 10
Extensive Metabolic Evaluation
24 hrs Urine collections.
Stone risk factors :
Volume
Calcium , Calcium to creatinine index.
Oxalate . ?Primary hyperoxaluria
Citrate
Uric acid.
Uro Lab. 11
Extensive Metabolic Evaluation
• Dietary risk factors:
Sodium,
Potassium
Magnesium
Urinary analytes : phosporus, sulfate, Urea
Marker for accuracy : Creatinine.
Repeat 24 hrs Urine collection 4-6 weeks post intervantion.
Uro Lab. 12
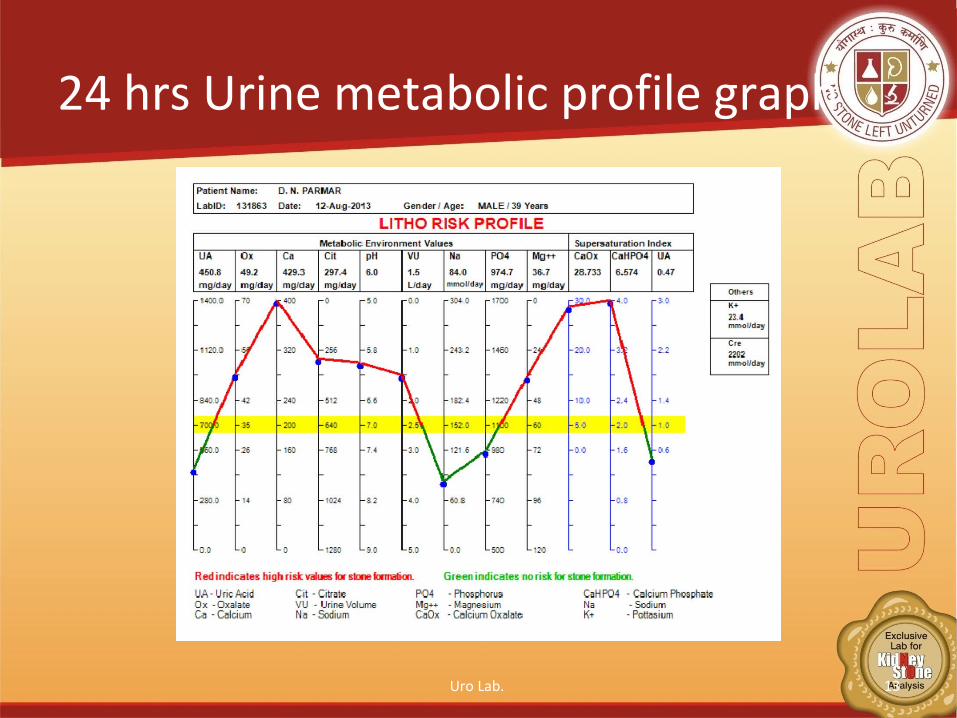
24 hrs Urine metabolic profile graph
Uro Lab. 13
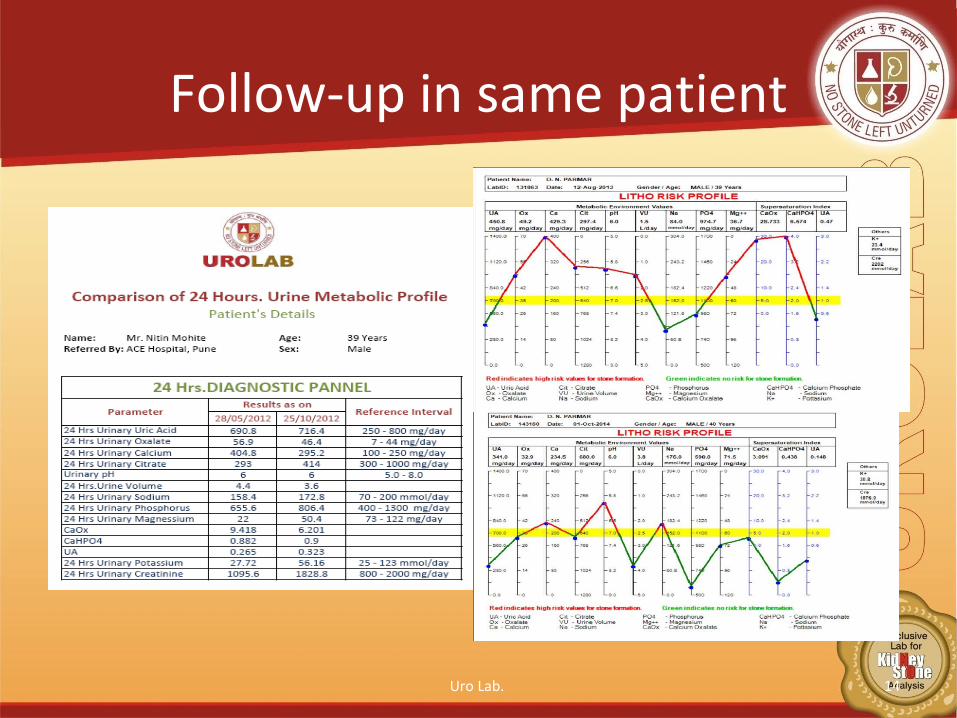
Follow-up in same patient
Uro Lab. 14
Stone analysis
Uro Lab. 15

• Essential step in the examination and initial treatment of Urolithiasis.
• Composition yields fundamental information of pathogenesis of disease like ;- Metabolic abnormality.- Presence of infection.- Possible artifacts.- Drug metabolism.
Renal Calculus Analysis
Uro Lab. 16
Integrated analysis: Techniques
• Optical Crystallogrphy• Chemical Microscopy.• Polarizing Microscopy.• Infrared spectroscopy.• X-ray diffraction.• Electron Microscopy• Fluorescence and chromatography.• Final , semi quantitative, modified estimate from
above results.
* herringlab.comUro Lab. 17
Significance of Stone analysis
• Exact composition gives important clue as to how Stone formed.
• Information may not available from any other type of work-up.
• Identify factors leading to clinical events.• Identify Risk factors.
Uro Lab. 18
Significance of Stone analysis
Three categories :
1.Composition and hardness of Renal Stones.
2.Composition and its predictive value.
3.Composition and related metabolic abnormalities.
Uro Lab. 19
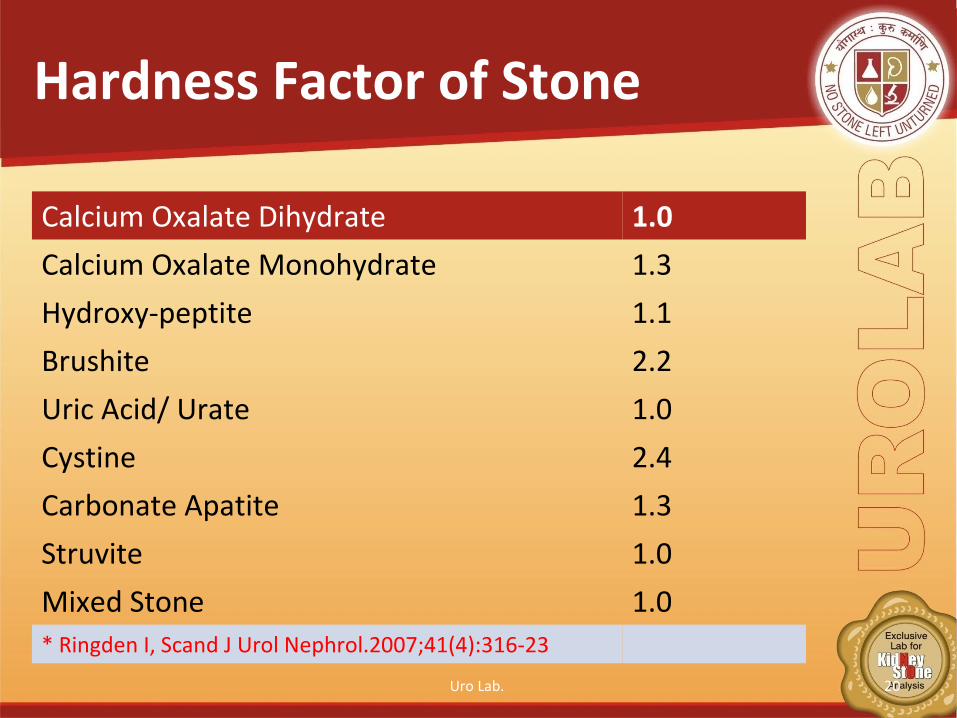
Hardness Factor of Stone
Calcium Oxalate Dihydrate 1.0
Calcium Oxalate Monohydrate 1.3
Hydroxy-peptite 1.1
Brushite 2.2
Uric Acid/ Urate 1.0
Cystine 2.4
Carbonate Apatite 1.3
Struvite 1.0
Mixed Stone 1.0* Ringden I, Scand J Urol Nephrol.2007;41(4):316-23
Uro Lab. 20
Clinical Significance: Hardness pattern in Stone.
• Useful in describing consistency in individual.• Formulation of treatment strategies.
- Number of re-treatments.
- Number of Shock waves. • Energy index (KV x number of shock waves).
• PMID:17763224( PubMed-indexed for MEDLINE)
Uro Lab. 21
Calcium stone….
• Pure Calcium oxalate: More Acid urine, Low urine volume, high oxalate excretion.
• Mixed Stone formers ;
High Calcium, pH and Stone formation rate.
High Calcium excretion.
* Schroeppel j Smith et all ; J Am Soc Nephrol 1997;8:568AUro Lab. 22
Calcium…..
• Calcium Oxalate Monohydrate :
Hypomagnesuria, acid urine, low volume
More hard then dihydrate.• Calcium Oxalate Dihydrate :
- hypercalciuria. High Urine pH and hypocitraturia.
Uro Lab. 23
Calcium Stone with …
Carbonate apatite : may indicate Renal Tubular Acidosis (RTA).
- Increases with amount of apatite.
( 5 – 39%).
Brushite Stones : Consider Renal tubular Acidosis (RTA).
Uro Lab. 24
Struvite Stones• Mixed Stone, infection. Mostly Proteus
Ammonium Urate • Elders : associated with infection.• Children : May also form as result of
hyperuricosuria, but NO urinary tract infection.
• Rare in pure form (0.03%)Uro Lab. 25
Uric Acid
• Hyperuricemia, hyperuricosuria.• Low Urine Ph. < 6.2• Causes:
- Gout.
- Myeloproliferative processes associated with pathological increased purine metabolism.
- Chemotherapy and Radiotherapy.Uro Lab. 26
Rare
Cystine : • Cysteinuria. Acidic• Autosomal recessive disorder.
Xenthene: • Xanthinuria.• Absence of Xanthinooxidase.• Genetic autosomal hereditary recessive
enzyme disorder.
Uro Lab. 27
Conclusion.
• Combined with Optical Crystallography, appropriate Blood & 24 Urine metabolic work-up with super-saturation, it can find out the cause of stone formation in nearly all cases
• Supersaturation Index is GOLD Standard to know exactly patho-physiological basis of Stone formation to guide proper treatment.
Uro Lab. 28

Thank You !Uro Lab. 29