strengthening the nursing/midwifery unit manager role ... · pdf filepage 4 nsw health...
TRANSCRIPT

"take the lead"Strengthening the Nursing/Midwifery Unit Manager role across NSW
Report Phase One: August 2008

NSW DEPARTMENT OF HEALTH
73 Miller Street
NORTH SYDNEY NSW 2060
Tel. (02) 9391 9000
Fax. (02) 9391 9101
TTY. (02) 9391 9900
www.health.nsw.gov.au
This work is copyright. It may be reproduced in whole or in part for study
training purposes subject to the inclusion of an acknowledgement of the source.
It may not be reproduced for commercial usage or sale. Reproduction for
purposes other than those indicated above requires written permission from
the NSW Department of Health.
© NSW Department of Health 2009
SHPN (NAMO) 090041
ISBN 978-1-74187-433-4
For further copies of this document please contact:
Better Health Centre – Publications Warehouse
PO Box 672
North Ryde BC, NSW 2113
Tel. (02) 9887 5450
Fax. (02) 9887 5452
Further copies of this document can be downloaded from the
NSW Health website www.health.nsw.gov.au
May 2009
Compiled by:Sue HawesProject Manager Nursing and Midwifery Office
Statistical and thematic analysis by:Dr Donna WatersThe College of Nursing

I would like to acknowledge each and every Nursing and Midwifery Unit Manager that participated in this project.
Your commitment to patient/client care through safe nursing/midwifery practice is inspiring.
Thank you for sharing your experiences with such sincerity and integrity. It is these experiences and other ideas that
create the platform for this report.
I would like to also acknowledge the editorial support given by Helena Harrison, Project Officer and Adjunct Professor
Debra Thoms, Chief Nursing and Midwifery Officer NSW.
Sue Hawes
Registered Nurse
Project Manager "take the lead"
"We must become the change we want to see"Mahatma Ghandi
PAGE 2 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Many people who come into contact with the public
health system are admitted to a ward or unit. It is here
that the professional capabilities of the Nursing or
Midwifery Unit Manager have considerable influence
and contribution to the experiences of these patients,
their families and carers as well as other members of the
health care team.
There are many challenges for Nursing and Midwifery
Unit Managers in today’s health care environment. They
are expected to provide not only clinical leadership within
their units but also deal with an increasing number of
organisational and administrative requirements and at the
same time ensure the maintenance of high standards of
nursing and midwifery care.
These challenges are not unique to New South Wales or
indeed Australia. Throughout the course of this project
we have come into contact with similar work being
undertaken in Queensland, Scotland and Wales.
This Report provides feedback on the first phase of
the "take the lead" project. The work undertaken in
this phase of the project has provided valuable insights
into the challenges faced by Nursing and Midwifery
Unit Managers and has provided a firm basis for the
development of the strategies which make up the next
phase of work in the project.
Three streams of work have been identified as a result of
the information gathered in this first phase, as outlined
in the executive summary.
The leadership provided by Sue Hawes as the Project
Manager and Helena Harrison who has worked with Sue
over the past months has been critical to the success of
the project.
The willingness and enthusiasm with which Nursing and
Midwifery Unit Managers have engaged with the project
has also been an essential element. It is clear from the
interactions with Nursing and Midwifery Unit Managers
during the course of this project that they maintain
a deep commitment to ensuring that nursing and
midwifery practice make a positive contribution to the
outcomes of care for those members of the community
that come into contact with the NSW public health
system. It is a key aim of this project to support and
enable them in achieving that goal.
Adjunct Professor Debra Thoms,
Chief Nursing and Midwifery Officer
NSW Health
Foreword

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 3
Contents
Executive Summary ...........................................4
Background and literature review .....................5
Assessing and determining the issues .............7
1 Methodology ................................................ 8
1.1 N/MUM workshops .....................................8
1.2 One page questionnaire ...............................8
1.3 N/MUM Forum Day .....................................9
1.4 Other stakeholders ......................................9
2 Results ........................................................ 10
2.1 N/MUM workshops ...................................10
2.1.1 The Current N/MUM role ..........................10
2.1.1a General management functions ........ 10
Staff and human resource management .......... 11
Communication ............................................... 11
Budgeting ........................................................ 13
Unit maintenance and equipment .................... 13
2.1.1b Patient Care Activities ...................13
2.1.1c Quality and Safety Management ......14
2.1.1d Leadership ...................................15
2.1.2 Skills and Attributes .................................16
2.1.3 Barriers and Enablers ...............................16
2.1.4 The Ideal N/MUM role ..............................17
2.2 One page questionnaire .............................18
2.3 N/MUM Forum Day ...................................19
2.4 Other stakeholders ....................................19
Conclusion and next steps ............................. 21
References ....................................................... 22
Appendices
1 N/MUM Workshops, Clinical areas ....................24
2 N/MUM Workshops, Hospitals ..........................25
3 Workshop Format ..............................................26
4 N/MUM Questionnaire .......................................27
5 N/MUM Forum Day Agenda ..............................28
6 Key Pad Summary Results ................................29
7 N/MUM Workshop Management Functions ......35

PAGE 4 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Executive Summary
In 2007 a collaborative project between the Nursing
and Midwifery Office (NaMO) and the Health Service
Improvement Branch (HSIB) at NSW Health was
initiated by Adjunct Professor Debra Thoms, Chief
Nursing and Midwifery Officer NSW and Professor
Katherine McGrath, the then Deputy Director General
Health System Performance. This was in response to
patient and carer feedback and anecdotal information
about Nursing/Midwifery Unit Managers (N/MUMs)
experiences.
For many years it has been acknowledged that the
N/MUM is the central and pivotal role in managing
and co-ordinating patient care activities at the unit/
ward level. For the purpose of this report N/MUMs
are defined as the Registered Nurse/Midwife that has
responsibility for leading clinical care and managing the
business aspects of a unit/ward.
The project called “take the lead” aims to facilitate
the role of the N/MUM in order to provide highly
co-ordinated care at the unit level and thereby
improve the patient journey and the patient and carer
experiences. In addition the project aims to identify
strategies to support N/MUMs in achieving this
role, recognising the pivotal part the N/MUM has in
co-ordinating patient care.
Through a range of strategies conducted between
August 2007 and February 2008 the current experiences
of N/MUMs and the expectations of others of the role
were explored.
Data collected identified the current activities
undertaken by N/MUMs, the barriers and enablers
to their role, the skills and attributes required for the
role and what the ideal N/MUM role would be. Other
stakeholders were asked to outline their expectations of
the N/MUM role as well as the behaviours they observe
in a successful N/MUM.
The key findings identified were:
n There is extensive breadth, depth and variability
in the accountability, responsibilities and functions
performed by N/MUMs.
n 60% of N/MUM activities involve general management
tasks and tend to be predominantly transactional
in nature. The remaining 40% of N/MUM activities
include quality and safety, patient care activities and
leadership.
n There are a variety of educational levels among N/MUMs
with over 40% identifying their nursing entry level
qualification as their highest level of education.
n The availability of appropriate professional
development and education that specifically meets the
needs of this role is variable and at times limited.
n Standardised reports and information to support the
N/MUM in fulfilling their role were limited in their
availability.
As a result of the consultation processes and data analysis
three work streams have been identified. These are:
n Defining and seeking agreement on the purpose and
core functions of the N/MUM role across NSW.
n Identifying strategies to address the education and
professional development required to support and
strengthen the N/MUM role.
n Outlining strategies to address the number of
transactional (administrative) tasks N/MUMs currently
undertake that do not align with the purpose and
core functions of the role.
These work streams aim to address the key issues identified
and will be progressed in the next phase of the project.

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 5
Background and Literature Review
In NSW there are three classifications of
Nursing/Midwifery Unit Managers (N/MUMs) as defined
by the NSW Public Health System Nurses’ & Midwives’
(State) Award. They are defined in the Award as N/
MUM Level 1, 2 or 3 and have responsibility for the
co-ordination of patient services, unit management,
and nursing staff management. For the purpose of this
report a N/MUM refers to the “registered nurse in charge
of a ward or unit or group of wards or units in a public
hospital or health service or public health organisation”
(NSW Health, 2008, p.7).
Patient and Carer Experiences
Responsiveness, patient centredness, safety and
effectiveness form the pillars of the NSW State Health
Plan (NSW Health 2007). The role of the N/MUM lies at
the core of these values, and is critical to the delivery of
quality healthcare in line with State objectives.
The N/MUM occupies a frontline management position
and their skills and performance is critically important to
health service outcomes (Duffield et al 2007a; Duffield
et al 2007b).
Over the past 20 years, there has been a steady growth
in research, nationally and internationally, related to
nurses working in frontline management positions.
There is consistent evidence indicating that these
frontline management positions are a key factor in the
delivery of high quality care and are vital links in the
patient and carers experience (Baumann 2007; Casida
2007; Duffield et al 2007b, ICN/FNIF 2006; Read et al
2004; The Scottish Government 2008).
Results from the 2007 NSW Patient Survey revealed
that one of the top priorities for patients is the ability
to access appropriate staff to adequately discuss their
treatment and concerns. Similarly, international studies
identify that patients expect the unit/ward manager to
be easily identified, have a visible presence on the ward/
unit and be approachable (Baumann 2007; Baumann et
al 2001; The Scottish Government 2008). The literature
further highlights the key role nursing leaders play in
determining the context and culture of care, which
influence the quality of care and the patient and carer
experience (Baumann 2007; Casida 2007; Laschinger &
Wong 2007b; McGuire & Kennerly 2006).
The N/MUM role
Results from a review of the N/MUM role in NSW,
as part of the "take the lead” project, identified that
there is considerable disparity in responsibility and
accountability of the N/MUM role. In addition there is
limited agreed understanding of what the purpose and
core functions of the N/MUM role are.
A recent review by Queensland Health of their
comparable role revealed identical issues (Queensland
Health 2008). The literature recognises the N/MUM role
as complex and multifaceted, including its continued
expansion of responsibility over the last 20 years
(Duffield 1991; Duffield et al 2007a; Duffield & Franks
2001). Reviews of similar roles in Scotland, United
Kingdom and Canada found corresponding results
(Laschinger & Wong 2007a; Read et al 2004; The
Scottish Government 2008).
NSW Health is comprised of eight Area Health Services
(AHS) and two public health organisations (The Children’s
Hospital at Westmead and Justice Health). To facilitate
the management and business administration workflows
some corporate service functions are retained locally,
while others have become centralised following the
establishment of Health Support Services. Health
Support Services provide centralised co-ordination of
such activities as information technology support for
AHS, payroll and human resource management support.
N/MUMs participating in workshops as part of the “take
the lead” project identified that a significant proportion
of disparate administrative tasks have been delegated
to their role over many years and following recent
restructuring. The impact of organisational restructures
is well documented in studies conducted in Australia and

PAGE 6 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
overseas. They include such things as role ineffectiveness
due to broadened responsibilities and functions; greater
complexity, time and financial constraints; lack of clarity
of role accountability; and the distortion of escalation
procedures (Duffield et al 2007a; Duffield et al 2007b;
ICN/FNIF 2006; Laschinger & Wong 2007b; Read et al
2004; The Scottish Government 2008).
Nursing shortages, increasing patient volumes and
financial pressures also contribute to the complexity and
ability of N/MUMs to effectively manage their changing
environments (Duffield et al 2007b). In the past five
years, the flow of patients between wards has increased
in NSW. Patients will on average move at least twice
during their inpatient stay, and the average number
of patients moving through a ward is 1.25% greater
than the number of beds open. This “churn” (Duffield
et al 2007b) has created an increasingly complex ward
environment, particularly when recognising that the
casemix split of patients on wards has increased year
on year since 2001 – as many as 250 DRG groups may
pass through a ward, each with different care/treatment
plans and pharmacology requirements (Duffield et al
2007b). The need for a co-ordinated approach to patient
care at a ward/unit level is critical.
Leadership capacity and capability
National and international research identifies leadership
development for front line nursing and midwifery
managers as critical to ensure they are able to manage
the complex challenges within a constantly changing
health care system and enact positive sustainable change
(Duffield et al 2007b; ICN/FNIF 2006; Laschinger &
Wong 2007a, Read et al 2004; The Scottish Government
2008). Transformational leadership has been linked to
better overall organisational outcomes and is essential
in achieving and maintaining the organisational
effectiveness of acute care hospitals (Casida 2007;
McGuire & Kennerly 2006; RNAO 2006).
Notably, evidence also suggests that the higher the
educational qualifications and professional status
amongst nurses providing care, the better the patient
outcomes (Aitken et al 2007). Therefore the capacity
and capability of those in the N/MUM role is crucial if
they are to influence organisational culture, clinical and
financial outcomes, retention and sustainability of the
health care team.
Australian studies have highlighted the lack of
experience, educational preparation and support
mechanisms for N/MUMs (Duffield 1989, 1994, 1995;
Duffield et al 2001; Duffield et al 1996; Duffield &
Franks 2001; Paliadelis 2005). Further to this, succession
planning is generally absent and support structures such
as mentoring and supervision are not well accessed
or designed (Buchan & Calman 2005; ICN/FNIF 2006;
Moran et al 2002; NSW Health 2006). Together these
impact on the ability of organisations to recruit and
retain nurses in the N/MUM role and result in adverse
patient events, poor business management practices,
and significant financial liabilities (Buchan & Calman
2005; ICN/FNIF 2006; Laschinger & Wong 2007a; Moran
et al 2002).
The International Council of Nurses (ICN) (2006) believes
that leadership development is a critical aspect for
positive and sustainable change. Nurses in key leadership
and management positions need to be prepared to
manage rapid change in a globalised and technologically
driven world with limited financial and human resources
(ICN 2006).

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 7
Assessing and Determining the Issues
Four key activities were undertaken over 12 months to
determine and assess the issues that prevail across NSW
relating to the N/MUM role.
These were as follows:
1. Workshops: attended by N/MUMs where data was collected in
response to a series of questions.
2. Completion of a questionnaire: N/MUMs who attended the workshops were invited
to complete a one page demographic questionnaire.
3. N/MUM Forum Day: data collected at the workshops was validated and
further exploration of issues were conducted through
workshops.
4. Engagement of other stakeholders: workshops, focus groups and one-on-one interviews
were conducted.
Approximately 70 workshops, small focus groups and
one-on-one interviews were conducted between August
2007 and February 2008. The N/MUMs Forum Day held
in March 2008, involved 170 N/MUMs – 44% (n = 75)
of those attending had not been to a workshop prior to
coming to the Forum.
A total of 870 health staff (Table 1) from metropolitan,
rural and remote health facilities located across NSW
participated in workshops and interviews. Health staff
worked in all eight NSW Area Health Services (AHS);
Northern Sydney Central Coast (NSCCAHS), Sydney
South West (SSWAHS), Hunter New England (HNEAHS),
South Eastern Sydney Illawarra (SESIAHS), Sydney West
(SWAHS), Greater Western (GWAHS), North Coast
(NCAHS), and Greater Southern (GSAHS).
Staff from The Children's Hospital at Westmead (CHW)
and Justice Health (JH) were also represented. Those
participants identified as ‘other’ represent sessions held
with health staff at state wide meetings at NSW Health.
Table 2 (below) identifies N/MUMs, both in permanent
positions and in acting roles, which made up 71%
(n = 619) of the total sample of workshop and interview
participants. Stakeholders other than N/MUMs made up
the remaining 29% (n = 251) of workshop and interview
participants.
Table 1: Number of Participants by Area Health Service
NSCC AHS
SESI AHS
SSW AHS
SW AHS
GS AHS
GW AHS
HNE AHS
NC AHS
JH CHW OTHER TOTAL
No. of workshops 4 7 4 6 5 11 10 9 2 2 10 70
Metro 35 136 67 135 – – – – – – – 373
Rural/Remote – – – – 64 66 86 152 – – – 368
Other – – – – – – – – 24 12 93 129
TOTAL 35 136 67 135 64 66 86 152 24 12 93 870
Table 2: Nursing and Midwifery Unit Managers by Area Health Service
NSCC AHS
SESI AHS
SSW AHS
SW AHS
GS AHS
GW AHS
HNE AHS
NC AHS
JH CHW OTHER TOTAL
N/MUM 28 77 60 121 25 41 53 85 24 12 35 561
N/MUM (Acting) 4 16 7 12 6 12 1 – – – 58
TOTAL – – – – – – – – – – – 619
Appendix One lists the clinical areas of the N/MUMs that attended the workshop, Appendix Two lists the hospitals that N/MUMs came from.

PAGE 8 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
One of the objectives of this project was to identify and
describe the depth and breadth of the current N/MUM
role in NSW. All the data was statistically and thematically
analysed by an independent research consultant. The
analysis aimed to offer a full description of the range of
the N/MUM functions identified through workshops and
interviews.
1.1 N/MUM workshops
Each AHS was invited to host as many workshops as
they thought necessary for as long as they thought
appropriate for N/MUMs.
A total of 63 workshops were held for N/MUMs across
NSW. Workshops varied from two to five hours in
length depending on the time allocated by the AHS.
Participants were N/MUMs permanently appointed or
acting in the role.
The workshop format (Appendix 3) included an
introduction and overview of the project. Picture
postcards were used as a tool to introduce participants
and share “why they liked being a N/MUM”. The larger
group was divided into four smaller groups to explore a
particular topic.
The topics and the related questions were:
n Current N/MUM role – identify all the things that
you currently do as a N/MUM.
n Skills and attributes – identify the skills and
attributes you need to have as a N/MUM. This can be
what you currently have or what you think you need.
n Barriers and enablers – identify the barriers and
enablers to your role. What allows you to get on and
do your job and what stops or blocks you from doing
your job?
n The ideal N/MUM role – If you could stop what
you are doing tomorrow and work in your ideal world,
what would that look like and feel like?
Each smaller group explored only one of these topics.
Participants were given blank ‘post-it’ notes where
they could record their individual responses and then
place them onto a large sheet of butcher’s paper. A
representative from the group fed back to the larger
group where the information was validated, clarified and
added to if needed.
To conclude the workshops, an evaluation was done
where each participant was asked to identify the one
thing “they liked least about the workshop” and “they
liked the most about the workshop”. Their responses
were recorded by the facilitator.
Following the workshops, the ‘post-it’ notes from
each session were grouped into common themes and
transcribed verbatim onto excel spreadsheets. The final
dataset comprised the typed verbatim comments from
each workshop participant organised under themes of
response to each of the broad questions.
Further analysis consisted mainly of identifying the
frequency of responses within each of the themes to
highlight areas of commonality or consensus among the
workshop and interview participants.
Frequency counts presented in figures and graphs in
the findings represent the number of times the same or
similar comments were expressed by the sample. Direct
quotes (noted by italics and quotation marks) are also
used to illustrate some major points.
1.2 One page questionnaire
All the N/MUMs that attended workshops were invited
to complete a one page questionnaire (Appendix 4) at
the end of the workshops. The questionnaire aimed
to collect some demographic data about N/MUM
participants.
The demographic data collected from workshop
attendees were analysed using standard descriptive
techniques by an independent research consultant.
Methodology
NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 9
1.3 N/MUM Forum Day
A Forum Day (Appendix 5) for N/MUMs across the
state was hosted on the 27th March 2008 at Australian
Technology Park in Sydney.
N/MUMs were invited to attend through their AHS, Area
Directors of Nursing and Midwifery. AHS were invited
to send 20 participants from metropolitan AHS and 10
from rural AHS, as well as 10 each from The Children’s
Hospital at Westmead and Justice Health.
It was requested that as a minimum, half of the AHS
participants be those who had previously attended a
workshop in their AHS for the “take the lead” project.
The aim of the day was to validate the thematic analysis
that had been undertaken of the workshop data
collected. Each participant at the forum was issued with
a 'keypad' to use to answer questions posed throughout
a presentation given by the Project Manager. Using the
key pad to answer questions was not compulsory, so
results do not add to 100% of the participants. “Turning
Point” software counted the responses and graphed the
results (Appendix 6).
Role plays were also used to present a visual
representation of the findings on current and ideal
N/MUM role analysis. After viewing the role plays,
participants confirmed that these represented a true
reflection of their current and ideal role, further
validating the findings.
1.4 Other stakeholders
Workshops, small group discussions, one-on-one meetings
and phone interviews were conducted with other
stakeholders to explore and discover their expectations
of the N/MUM role. Other stakeholders included nursing
staff at all levels, other health professionals, consumers,
industrial organisations, professional organisations and
non clinical staff. Other stakeholders were also asked
to describe the behaviours they saw of a N/MUM who
worked effectively in their role and the behaviours where a
N/MUM had limited capability in fulfilling the role.
All responses were recorded on ‘post-it’ notes by participants
in workshops, otherwise the information was recorded in
notes taken by the interviewer. This data/ information was
transcribed into an excel spreadsheet for analysis.
All the data was statistically and thematically analysed by
an independent research consultant.
PAGE 10 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
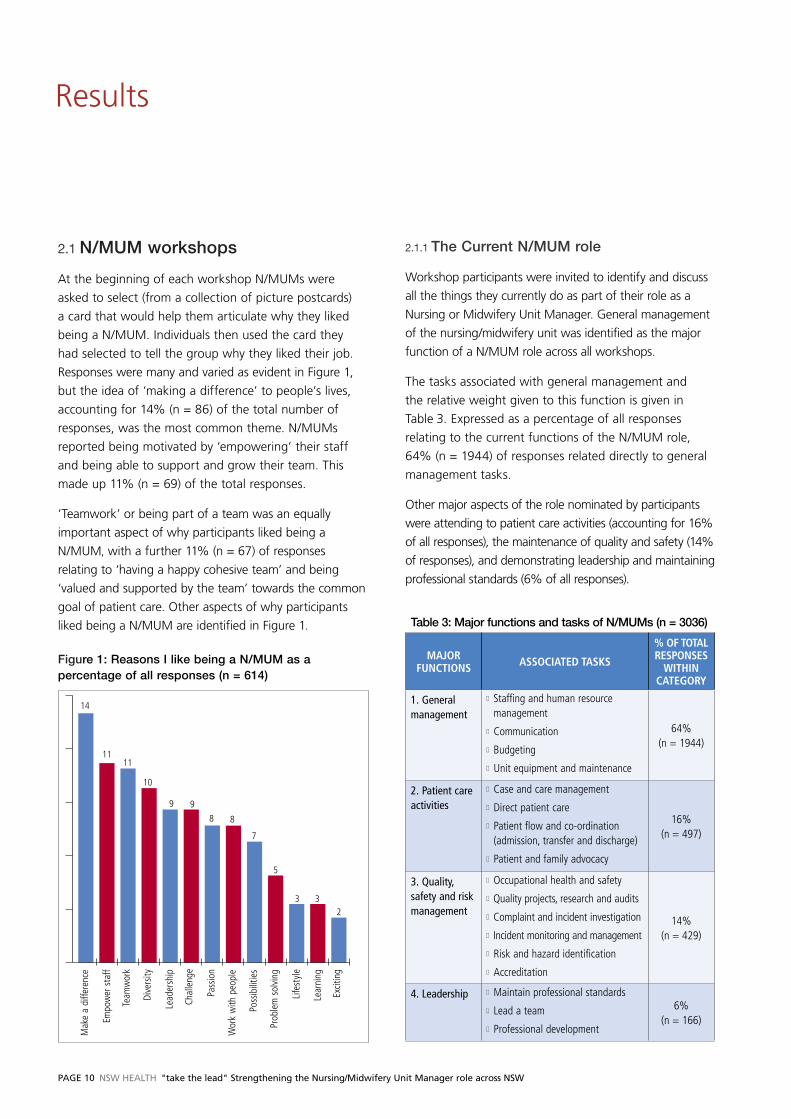
2.1 N/MUM workshops
At the beginning of each workshop N/MUMs were
asked to select (from a collection of picture postcards)
a card that would help them articulate why they liked
being a N/MUM. Individuals then used the card they
had selected to tell the group why they liked their job.
Responses were many and varied as evident in Figure 1,
but the idea of ‘making a difference’ to people’s lives,
accounting for 14% (n = 86) of the total number of
responses, was the most common theme. N/MUMs
reported being motivated by ‘empowering’ their staff
and being able to support and grow their team. This
made up 11% (n = 69) of the total responses.
‘Teamwork’ or being part of a team was an equally
important aspect of why participants liked being a
N/MUM, with a further 11% (n = 67) of responses
relating to ‘having a happy cohesive team’ and being
‘valued and supported by the team’ towards the common
goal of patient care. Other aspects of why participants
liked being a N/MUM are identified in Figure 1.
Figure 1: Reasons I like being a N/MUM as a percentage of all responses (n = 614)
14
1111
10
9 9
8 8
7
5
3 32
Mak
e a
diffe
renc
e
Team
wor
k
Dive
rsity
Lead
ersh
ip
Chal
leng
e
Pass
ion
Wor
k w
ith p
eopl
e
Poss
ibili
ties
Prob
lem
sol
ving
Life
styl
e
Lear
ning
Excit
ing
Empo
wer
sta
ff
2.1.1 The Current N/MUM role
Workshop participants were invited to identify and discuss
all the things they currently do as part of their role as a
Nursing or Midwifery Unit Manager. General management
of the nursing/midwifery unit was identified as the major
function of a N/MUM role across all workshops.
The tasks associated with general management and
the relative weight given to this function is given in
Table 3. Expressed as a percentage of all responses
relating to the current functions of the N/MUM role,
64% (n = 1944) of responses related directly to general
management tasks.
Other major aspects of the role nominated by participants
were attending to patient care activities (accounting for 16%
of all responses), the maintenance of quality and safety (14%
of responses), and demonstrating leadership and maintaining
professional standards (6% of all responses).
Table 3: Major functions and tasks of N/MUMs (n = 3036)
MAJOR FUNCTIONS ASSOCIATED TASKS
% OF TOTAL RESPONSES
WITHIN CATEGORY
1. General management
n Staffing and human resource management
n Communication
n Budgeting
n Unit equipment and maintenance
64% (n = 1944)
2. Patient care activities
n Case and care management
n Direct patient care
n Patient flow and co-ordination (admission, transfer and discharge)
n Patient and family advocacy
16% (n = 497)
3. Quality, safety and risk management
n Occupational health and safety
n Quality projects, research and audits
n Complaint and incident investigation
n Incident monitoring and management
n Risk and hazard identification
n Accreditation
14% (n = 429)
4. Leadership n Maintain professional standards
n Lead a team
n Professional development
6% (n = 166)
Results

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 11
2.1.1a General management functions
N/MUMs acknowledge that an important part of their
role includes management responsibilities and activities;
however it is to what extent they are required to do
such tasks, which inevitably takes them away from
directing and co-ordinating patient care.
The general management functions identified by N/MUMs
were many and varied. While some of this variance can
be explained by the size, location and clinical focus of
the various facilities in which the N/MUMs work, it is
difficult to reconcile an ‘official’ N/MUM role description
with some of the roles actually identified by workshop
participants (listed in Appendix 7) such as events
management, fundraising, student careers advisor,
cleaner, caterer, clerk, travel agent, fleet manager and
community liaison.
General management functions can be further
categorised into specific tasks as identified by the
workshop participants. This includes staff and human
resource management, budgeting, unit maintenance and
equipment and, communicating with others (Table 3).
Staff and human resource management
Staffing and human resource (HR) functions form a major
part of the NSW N/MUM role. Staffing and HR functions
can be further divided into four main categories (Table 4).
The management of leave (annual and sick leave) including
the organisation of staff return to work under Work Cover
agreements is nominated as a major part of staff and HR
management functions. In addition to annual performance
reviews, performance management, and dealing with staff
and family conflict, the N/MUM also frequently acts as a
personal counsellor (staff bereavements and relationship
problems), often describing themselves as ‘staff social
workers’ during the workshops.
Ensuring the unit is adequately staffed is an important
part of the N/MUM role. This function includes completing
and managing rosters and dealing with payroll systems
Table 4: Staffing and human resource management related N/MUM functions
STAFFING AND HUMAN RESOURCE MANAGEMENT INCLUDES AS A % OF RESPONSES
WITHIN CATEGORY
AS A % OF ALL NOMINATED STAFFING AND HR
FUNCTIONS
Managing staff
Leave & injury (Work Cover, annual, sick) 19% (51) –
Counselling (personal) 13% (35) –
Performance management 13% (34) –
Performance appraisals 12% (31) –
Supervision & support 11% (30) –
Conflict management 9% (24) –
Allied health & support staff 6% (17) –
Other (grievance, debrief, discipline) 17% (47) –
Total responses 100% (269) 36%
Staffing the unit
Rosters & rostering systems 42% (74) –
Finding staff (new and leave replacement) 24% (43) –
Staff allocation 15% (28) –
Skill mix & workload 10% (17) –
Audit & report 9% (16) –
Total responses 100% (178) 24%
Staff education and development
Plan, organise & conduct staff education 50% (79) –
Orientation new staff (nursing and other) 26% (41) –
Mandatory training 8% (13) –
Other (supervise, mentor, succession plan) 16% (25) –
Total responses 100% (158) 21%
Human resource administration
Recruitment & selection 65% (91) –
Managing workforce (staffing, succession) 18% (26) –
Payroll & timesheets 13% (18) –
Staff health (immunisation) 4% (6) –
Total responses 100% (141) 19%

PAGE 12 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
such as Proact™ and Kronos™. The actual ‘finding’
of new staff and staff for coverage (for meal breaks,
leave, overtime and ‘on call’) was frequently raised
by workshop participants and clearly constitutes a
major part of the work associated with staffing the
unit. This has significant implications for the N/MUM
role in maintaining a safe workload for staff, and an
appropriate skill mix.
The organisation of staff education and professional
development was identified as another important aspect
of staff and HR management functions (Table 4). The
selection and training of facilitators, mentors, preceptors
and educators was also identified as a significant part of
managing new graduates, trainees and students.
As human resource managers (Table 4), N/MUMs spend
much time in recruitment and selection processes.
Their HR role can include everything from sending
letters to applicants, getting selection panels together
and organising rooms and times, through to reference
checking and other processes required to maintain
compliance with HR policy and procedures. Many
participants commented on the amount of time involved
in this process, not only in completing necessary
recruitment and selection functions, but also in ‘chasing
up’ people and paperwork. In general, a lag time of
around three months was given for the commencement
of new staff.
In addition to common staffing and HR functions
identified by workshop participants in Table 4, there
were a range of other activities that can occur around
managing staff. Many of these are listed in Appendix
7, but include tasks such as coordinating hospital
volunteers, being the staff social director, organising
team building events, monitoring staff security and
being either officially (rostered) or unofficially on call for
staff at any time.
Communication
As a central point of contact within the ward or unit,
the N/MUM’s ability to liaise and network with others
is clearly an important aspect of their role. N/MUMs
identified themselves as the interface between their
staff, patients and families, other health professions, the
executive and management, other departments, police
and ambulance, emergency services, visiting medical
officers, general practitioners and the community.
Answering telephones, mobiles and pagers, returning
calls, teleconferencing and faxing make up much of
the activities that N/MUMs participate in. Sending and
replying to emails was also identified as a significant
part of communicating with others, as was dealing with
general enquires from the public.
The ‘paperwork’ described by workshop participants
ranged from the simple to the complex and
encompassed:
n The dissemination of information to staff, patients
and others
n The writing of memos, briefs and reports to senior
management
n Writing proposals for funding equipment or services
n Briefs to ministers (in three of the AHS)
n Preparing media releases (one AHS)
n Writing a story for the local newspaper (one AHS)
n Preparing submissions for the Health Care Complaints
Commission (one AHS).
A further analysis of the kind of ‘paperwork’ N/MUMs
are dealing with shows that the majority can be more
accurately described as ‘data entry’ and ‘report’ writing
(Figure 2). N/MUMs also identified the need to be
proficient in accessing and using a number of databases
such as DOHRS, CHIME, PIMS, IIMS, MHOAT, ANZICS,
NAOPPPS, CAPS, EDRS, Supero and OST
Audits and reports, such as monthly activity statistics
and the measurement of performance against Key
Performance Indicators, form a large part of the
N/MUMs paperwork load.
Data analysis was identified by 12% (n = 14) of
workshop participants as part of the background
preparation for these reports. N/MUMs identified that
they sometimes become the IT resource for others
(denoted by IT systems 3%, n = 4, in Figure 2).
Attendance at meetings is another major component of
the N/MUM general management role. In addition to
the more than 30 meetings identified and attended by
workshop participants, many N/MUMs have additional
responsibilities such as arranging the meeting schedules
and booking rooms, sending agendas and recording
minutes. Travel is also a significant component of
meeting attendance for many N/MUMs working
in satellite facilities or remote locations with some
spending a whole day travelling for compulsory meeting
attendance.

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 13
Figure 2: The ‘paperwork’ of N/MUMs
23 23
18
1312
54
20
5
10
15
20
25
30
Dat
a En
try
Aud
its
Pay
syst
ems
Dat
a A
naly
sis
Wor
kloa
d to
ol
IT s
yste
ms
Not
ifica
tions
Repo
rts
Budgeting
Budgeting is another major management function
of N/MUM (Table 3). Apart from building an annual
budget and managing and reporting against this
budget, workshop participants identified a number of
other associated finance functions. These commonly
included the monitoring of revenue targets, eg private
bed utilization, revenue collecting, eg salary packaging
targets, and fundraising to support and promote the
needs of their unit (also see Appendix 7).
While the need to manage relevant financial aspects
of the role is recognised many workshop participants
identified that they are held to account for things they
feel that they have no control over, such as pathology
and medication utilisation and costs.
Unit maintenance and equipment
The general management function of the N/MUM
includes responsibility for the stores and equipment
within their ward or unit and the maintenance of same.
The degree to which N/MUMs are involved in this
process varies with the size and type of unit, as well
as the geographic location and access to resources for
maintaining and purchasing. A wide range of functions
are apparent with N/MUMs commenting particularly on
the many levels of ‘sign-off’ required for apparently basic
items such as garbage bags.
Workshop participants detailed steps in the process of
ordering non-stock or replacement equipment for which
they are responsible:
n Finding a supplier
n Getting product information and quotes
n Making the submission for funding
n Dealing with company representatives
n Ensuring product complies with occupational health
and safety and infection control guidelines
n Equipment risk assessment
n Gaining approval for purchase
n Monitoring and variation adjustments after delivery
n Tracking and maintenance.
Maintenance of unit equipment can involve a similar
complex process with N/MUMs highlighting the individual
time-consuming tasks contributing to this function. For
example they need to find repairers, get quotes, replace
equipment while it is being repaired, track equipment
location and ensure its timely return to unit.
As illustrated in Appendix 7, the N/MUM role can
also include the maintenance of car fleets with the
management of service logs, safety checks and car
washes all part of the mix. Some N/MUMs have
responsibility for up to 30 cars as part of the fleet.
In some areas, N/MUMs are directly responsible for
the refurbishment of their units, undertaking direct
negotiation with local councils and contractors as part
of their role.
2.1.1b Patient Care Activities
The nursing knowledge and clinical experience that
N/MUMs bring to their role is vitally important to ensure
safe nursing and midwifery practice and high quality
patient care.
Patient care activities were identified by workshop
participants as one of the four major functions of the
N/MUM role (refer Table 3). Almost half of N/MUMs
returning their questionnaire indicated that they are
responsible for a clinical or patient load, in addition to
their unit management and coordination responsibilities.
Figure 3 (page 14) details the major functions identified
during the workshops as part of the N/MUM patient

PAGE 14 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
care activities. Particularly in rural AHS, N/MUMs’
rostered hours to perform clinical work often outnumber
the administration hours available to them. In these
situations, options for completing management tasks
identified by N/MUMs include working paid overtime,
working for unpaid time-in-lieu or working for ‘love’
(unpaid and unrecognised).
Workshop feedback also indicates that N/MUM
are frequently covering staff absences (during meal
breaks, sick leave and night duty), filling Clinical Nurse
Consultant (CNC) roles and working double shifts,
on-call and overtime to cover short falls in their staffing.
Figure 3: N/MUM role and patient care activities (n = 497)
39% patient care activities
26 % Direct patient care
21 % Patient �ow
8 % Advocacy
6 % Other
When not undertaking the broader task of case
and patient care coordination, other service gaps
filled by N/MUM included scrubbing and scouting in
operating theatre, doing medication rounds, giving out
and collecting bedpans, answering patient buzzers,
‘specialling’ patients (one-on-one care), escorting
patients during transport or transfer, showering patients,
making and cleaning beds, assisting with meal service
and feeding, emptying linen and rubbish bins and
mopping the floors.
As N/MUMs are often experienced clinical nurses, they
are also frequently consulted as a ‘clinical expert’ in their
specialty area and act as a resource person for other
units or wards.
NUMs in aged care settings indicated that they were
shopping, banking and running errands for residents.
In smaller communities, the N/MUM role also includes
community outreach and the performance of activities
such as delivering medications from the hospital to the
patient or following patients’ progress on discharge.
Other tasks identified as part of the patient care and
coordination role of N/MUM were weapon screening
and dealing with mental health emergencies and sieges.
2.1.1c Quality and Safety Management
The third major function of the N/MUM (Table 3) is overall
responsibility for unit quality and safety. Again, workshop
participants identified a broad range of tasks within this
category which are grouped in Figure 4. The conduct of
quality audits and projects (16%, n = 53); conducting
investigations such as Root Cause Analyses and case
reviews (15%, n = 50); writing, updating and ensuring
compliance with policies and procedures (14%, n = 44)
and; monitoring and managing incidents (12%, n = 40)
assume approximately equal weight among the N/MUMs
activities within this category.
Staff occupational health and safety (OH&S) is an
associated component of unit quality and safety but is
considered as a separate item in this analysis. For OH&S,
specific audits and staff training are required (such as
manual handling, hazard, fire training and safe work
practices) and most training is mandatory. When added
to the overall functions of the N/MUM role (in Table 3),
OH&S accounts for 20% (n = 63) of quality and safety
monitoring.
Figure 4: N/MUMs role in monitoring quality and safety
(n = 328)
8% Accredition
5% Reporting
2% Infection control
20% OH&S
17% Audits & projects
15% Investigations
14% Policies & procedures
12% Incident monitor/manage
8% Indentify risks
The monitoring of quality and safety is clearly a
continuous process for all N/MUMs, however, there are
also specific tasks associated with accreditation such
as documentation and visits from quality assessors
(8%, n = 27, of responses in Figure 4). Risk and hazard
identification (8%, n = 27) and monthly or annual
reporting against quality benchmarks and performance
indicators (5%, n = 16) is also part of the N/MUM role in
monitoring quality and safety within the unit.
2.1.1d Leadership
A final but equally important major function identified
as part of the N/MUM role (from Table 3) is related to
leadership of the ward or unit team. N/MUMs across
NSW have high expectations for their own personal and
professional development in terms of career progression,

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 15
maintaining currency and undertaking further education
to develop their leadership potential and to manage a
competent and professional service.
While monitoring compliance with policy and
procedure can be regarded as part of quality and safety
management, there is also a requirement to monitor
and maintain the professional standards of the staff and
unit. In identifying all the things N/MUMs do as part of
their role, workshop participants identified the following
common leadership skills:
1. People-skills: listening, communicating, empowering
2. Mediation
3. Problem-solving
4. Delegation
5. Mentoring
Other leadership and management skills identified at the
workshops included having a positive attitude and being
flexible, being a role model, having clear boundaries,
being accountable and able to manage conflict.
2.1.2 Skills and Attributes
Workshop participants were asked to identify the skills
and attributes they believe are necessary for the
N/MUM role. These could be either the skills or attributes
participants believed they already possessed or what they
believe is necessary for the role. While the distinction
between a skill and an attribute is somewhat arbitrary,
for this report a skill has been defined as an ability that
can be acquired by training, whereas an attribute is a
characteristic or quality that is demonstrated by a person.
In Figure 5 eight different skill sets or themes identified
by workshop participants are grouped and presented as
a percentage of the total number of responses. It can be
seen from Figure 5 that workshop participants believe
that skills in ‘management’ are most important. In this
context, management skills included functions such as
budgeting, performance managing, delegation, policy
and procedure development and ‘knowledge’. This
‘knowledge’ related to understanding how things work
– understanding the system, understanding the staff,
understanding the organisation.
‘People skills’ incorporates the advocacy and support
functions of the N/MUM as well as conflict resolution,
mediation and facilitation. Leadership was also rated
as important. While leadership can be both a skill
(learnt) and an attribute (personal quality), workshop
participants named role modelling and mentorship
among the necessary leadership skills.
Figure 5: Necessary skills for N/MUMs (n = 739)
Lead
er
IT &
dat
a
Peop
le s
kills
Reso
urce
Com
mun
icato
r
Inno
vato
r
Man
agem
ent s
kills
Clin
ical s
kill
5%
10%
15%
20%
25%
30%
35%
Being a good ‘communicator’ was also identified as
an important skill for N/MUMs. Across all areas, it
was deemed necessary that a N/MUM has the ability
to listen, to think critically, to interpret and to share
information and knowledge with their staff.
As an ‘innovator’, the N/MUM should possess skills in
motivation, particularly with respect to initiating and
managing change. The N/MUM should also have relevant
‘clinical skills’ for the area in which they work and be a
‘resource’ person, educator and guide to their staff.
Skills in information technology and data (‘IT & data’)
relate to the N/MUM’s ability to use and manage data
for audits and reports.
In Figure 6 (page 16), eight attributes or themes
identified by workshop participants are grouped and
presented as a percentage of the total number of
attribute responses. Across all AHS there is a clear
and distinct expectation that a N/MUM should be ‘fair
and balanced’. This category includes the attributes
of empathy, acceptance, respect, patience and being
approachable.
Being ‘flexible’ or amenable to change, reliable and
‘committed’ to the role as well as having ‘integrity’

PAGE 16 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
or being honest and trustworthy (Figure 6), are all
attributes identified as important to a N/MUM. The
notion of having insight into oneself and others,
maintaining a holistic approach and generally keeping
a commonsense perspective were grouped under the
‘reflective’ attribute. Pragmatism is also valued, with
many workshop participants identifying being ‘calm
and confident’ as an attribute, and noting the need for
resilience to withstand daily pressures.
Having a ‘positive’, optimistic attitude and maintaining
a ‘sense of humour’ and fun were also identified as
important and necessary attributes for a N/MUM.
Figure 6: Necessary attributes of N/MUMs (n = 352)
Fair/
bala
nced
Refle
ctiv
e
Posit
ive
Sens
e of
hum
our
Calm
& c
onfid
ent
Com
mitt
ed
Inte
grity
Flex
ible
5%
10%
15%
20%
25%
30%
35%
2.1.3 Barriers and Enablers
During each workshop, participants were asked to
identify the people (roles), resources or systems that
enable or facilitate their role, as well as those that create
barriers to the performance of their role as a N/MUM.
A large range of enablers and barriers were identified
and these are clearly impacted upon by environmental
factors such as staff availability and geographic location.
1. Enablers
Despite small differences the majority of workshop
participants in both metropolitan and rural locations
identified the following as the most important enablers
of the N/MUM role:
a) Support
Support from unit staff, peers and colleagues as well as
from senior management. Clinical Nurse Consultants,
Clinical Nurse Educators and Nurse Educators were
specifically identified as part of the N/MUM's own
support network.
b) Adequate staffing
Adequate staffing levels and appropriate skill mix.
Adequate staffing extended to clerical, allied health
and other administrative and human resource roles that
support the current functions of the N/MUM.
c) Resources
Adequate resourcing of the unit including office space,
an appropriate budget allocation, and functioning
equipment. Access and training in information
technology (computers) was one of the most frequently
cited enablers of the N/MUM role.
d) Education and development
Access and opportunities for professional development
and education to ensure the ability to undertake the role
effectively and efficiently.
e) Effective communication
Adequate and timely access to information necessary to
perform the N/MUM role effectively and appropriately.
Other common enablers of the N/MUM role identified
were the capacity of staff and management to be
receptive and adaptive to change, the support of allied
health and medical staff, autonomy, flexibility, and the
ability to contribute to decisions about the ward or unit.
Guidance from organisational systems and processes
such as policies and procedures was also seen as a major
enabler to the role. There were minimal differences
between the metropolitan and rural areas, although
N/MUMs from rural AHS were more likely to choose
education and development among their role enablers.
Many workshop participants commented on the
importance of a happy workplace with enthusiastic,
motivated staff. Self-care, mentoring, clinical supervision
and the support of family were also identified as
significant role enablers, as was feeling valued and
respected by staff, patients and their families.
‘Time-out’ enabled the more indirect aspects of the role
such as organising staff development or succession planning.

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 17
2. Barriers
There was a clear identification of barriers to the
N/MUM role and a larger number of overall responses
within this category. Almost without exception, lack of
appropriate resources to fulfil the N/MUM role ranked
among the three most common responses of workshop
participants across metropolitan and rural AHS. The most
common shortfall in resources was access to information
technology and to the kind of IT support services required
to use computers and programs effectively.
The non-replacement of broken equipment and
shortages of stock and stores was also raised frequently
within this category. Across NSW, the following were
identified as important barriers to the N/MUM role:
a) Lack of resources and equipment
Responses ranged from a lack of basic equipment
such as faxes and photocopiers, limited access to IT
equipment and expertise, through to issues with the
physical work environment.
b) Lack of staff
Barriers included the long lag-time between recruitment
and commencement, inadequate or inappropriately trained
staff, and shortage within clinical specialties. Vacant, acting
and non-permanent positions in executive and management
were also seen as a barrier to the N/MUM role.
c) Poor understanding of the N/MUM role by others
N/MUMs are aware that inconsistencies, lack of role
clarity and position descriptions impact upon how others
communicate and interact with them. There is also a
perceived lack of insight into how the role of N/MUM can
be further developed within specific specialties or locations.
d) Unrealistic expectations
The N/MUM role is made more difficult by expectations
to provide what many believe is an unrealistically high
level of service. They feel this comes at the same time
as demands for increased performance, efficiency and
reporting within an existing resource base.
e) Prevailing workplace culture
N/MUMs perceive the current workplace culture as one
that is not always supportive of them in their role.
2.1.4 The Ideal N/MUM role
During the workshops, participants were invited to offer
their vision of the ideal N/MUM role – both how it might
look and how it might work.
The following six top features of the ideal N/MUM role
emerged (Table 5). The prioritisation of these responses
was reasonably consistent across all AHS with ‘adequate
support’ appearing among the top five most frequent
responses of all areas.
Table 5: Top six features of the ideal N/MUM role
THE IDEAL ROLE OF THE UNIT MANAGER IS ONE THAT:
Has adequate support Appropriate resources, equipment and staff.
Has autonomy To make decisions about their ward or unit.
Coordinates patient care By focussing the team on the patient.
Has management training
To prepare for the role and improve management skill.
Develops staff Through leadership, mentorship and role modelling.
Has appropriate staffing Appropriate allocation and skill mix for the care setting.
N/MUMs expressed that there was a lack of clarity
around expectations of the management versus the
clinical or nursing aspects of their role. They felt that this
has contributed to the perception of N/MUMs as ‘the
jack of all trades and master of none’ and has cemented
their post as one which offers the promise of ‘all things
to all people’. This is presumably what has led many
N/MUMs attending the workshops to identify the need
for specific management training for the role (Table 5),
a large component of which is the management of
conflicting roles and interests.
N/MUMs described the "ideal" role for a N/MUM as one
where:
n The N/MUM is prepared through succession planning
and mentoring into the role,
n There is autonomy and authority with accountability
and responsibility,
n There is clarity of what the purpose and core functions
of the N/MUM role is and executive, management and
colleagues understand and respect this,
n Meeting and other forms of communication are
efficient and effective,

PAGE 18 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
n There is support for the N/MUM especially for the
large number of transactional tasks that N/MUMs
undertake,
n The N/MUM is involved in decisions that effect the
service they lead and manage,
n The N/MUM has physical space and time to participate
in transformational activities such as service planning,
improvement projects and staff development plans,
n The N/MUM works in collaboration with business
managers to monitor and manage the financial aspects
of the ward/unit,
n The N/MUM coordinates and manages patient care
with a focus on the patient/family, best practice and
appropriate models of care,
n N/MUMs have time to talk to patients,
n N/MUMs work an eight hour day with a lunch break,
n N/MUMs have the opportunity to participate in
education and professional development,
n N/MUMs lead, mentor and develop staff to provide
patient centred care.
2.2 One page questionnaire
Workshop participants who identified themselves as
Nursing or Midwifery Unit Managers (n = 619 in Table 2)
were invited to complete a more detailed demographic
questionnaire following their workshop session
(Appendix 4).
91% (n = 564) participants returned their questionnaires.
Of these, 72% (n = 409) were female and 11% (n = 62)
were male. The gender of a further 93 participants who
elected to anonymously return a survey is unknown.
An average of 66 N/MUMs from each AHS returned a
questionnaire (Table 6).
94% (n = 531) of respondents were in full time
employment with 6% (n = 33) working part-time.
Table 6 outlines the demographic profile of current
N/MUMs working in NSW who responded to the
questionnaire. Not all respondents answered every
question, therefore, some rows do not add to 100%.
While the majority of respondents were being paid
at the award rate of N/MUM Level 2, 39% (n = 15)
respondents were working under other professional
awards. 27% (n = 154) had been working in a N/MUM
role for between three and five years, although there
were equal proportions who were both new to the role
(19%, n = 105, had worked as N/MUM less than 12
months) and who were more experienced (18%, n = 104,
had worked as N/MUM for more than 10 years).
Approximately equal proportions of NSW N/MUMs
nominated their highest educational qualification as a
bachelor degree in nursing (25%, n = 143), a hospital
certificate (21%, n = 121) and a graduate certificate
(21%, n = 116). 13% (n = 74) of N/MUMs had a Masters
level qualification.
All but one survey respondent had access to a computer
in their workplace and 81% (n = 457) of those with
computer access also had an internet connection.
While the majority of N/MUMs (80%, n = 453) worked
to a known position description, a further 14% (n = 78)
of respondents indicated that they did not have a
position description and a further 3% (n = 16) were
unsure. Almost half of all respondents (46%, n = 253)
had a patient load in addition to their N/MUM duties;
however, as shown in Figure 7, this was more likely to
occur in rural-based AHS and in Justice Health.
Figure 7: Percentage of N/MUMs per Area Health
Service with patient load (n = 553)
11
NSC
CAHS
CHW
HNEA
HS
SESI
AHS
CSW
AHS
NCA
HS
GSA
HS
SSW
AHS
GW
AHS
Just
ice H
ealth
32 33 36 3844
52
60
83 87

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 19
2.3 N/MUM Forum Day
A total of 173 N/MUMs from across NSW attended
the Forum. Of these, 80% (n = 138) responded to the
question asked about who had attended a "take the
lead" workshop in their AHS. Participants represented
57% (n = 78) who had attended a workshop and 44%
(n = 60) who had not.
A didactic presentation outlining the main themes
and three sub-themes emerging from the data was
delivered to the audience by the Project Manager. The
themes reflected content explored during the N/MUM
workshops and were as follows:
1. Reasons why N/MUMs like their role,
2. Main functions of the current N/MUM role:
a. General management
b. Coordination of patient care
c. Quality and safety
d. Leadership,
3. The skills and attributes required for the role,
4. Enablers to the N/MUM role,
5. Barriers to the N/MUM role,
6. What an ideal N/MUM role looks like.
During the presentation N/MUMs were presented with
a series of questions which were used to validate the
results found within each of the above themes.
An affirmative response rate of between 94% – 100%
was achieved for each theme or sub theme, with an
average rate of agreement of 98% (refer Appendix 6).
Table 6: Demographic profile of N/MUMs (n = 564)
NSW UNIT MANAGERS NUMBER PERCENTAGE
Female: Male 409:62 72:11
Fulltime: Part time 531:33 94:6
Permanent: Acting in Role 445:117 79:21
Award classification Nursing Unit Manager Level 1 164 29
Nursing Unit Manager Level 2 306 54
Nursing Unit Manager Level 3 76 13
Other 15 2
Length of service as a N/MUM Less than 12 months 105 19
1 – 2 years 93 17
3 – 5 years 154 27
6 – 10 years 105 19
More than 10 years 104 18
Highest education qualification Bachelors Degree 143 25
Hospital Certificate 121 21
Diploma/Associate Diploma 43 8
Graduate Certificate 116 21
Graduate Diploma 65 12
Masters Degree 74 13
PAGE 20 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
2.4 Other stakeholders
More than 200 other health service staff across NSW
attended workshops, focus groups, or one on one
interviews. These were Directors of Nursing and
Midwifery; nursing or midwifery managers or educators;
service directors; service managers; human resource and
finance staff; clinical nurses and midwives as well as
allied health staff; doctors; bed managers; network and
clinical practice managers; after-hours managers; union
representatives and members of the N/MUM Society.
These stakeholders (other than N/MUMs) were asked to
comment on their expectations of the N/MUM role and
also whether they could identify attributes that differentiate
between a successful and less successful N/MUM role.
Nurses and Midwives expect N/MUMs to:
n Go on rounds with staff, coordinate patient care and
generally manage the unit and staff and to use Clinical
Nurse Consultants (CNC) and Clinical Nurse Specialists
(CNS) to coordinate clinical care.
n Be a ‘clinical leader’ who is ‘a nurse’ and is an
‘advocate for patients and staff’.
n Have a ‘good work ethic’ and be ‘reliable and punctual’.
n ‘Control their environment’, ‘lead and direct change’
and maintain ‘high standards’ of patient care.
n ‘Direct the traffic’.
n ‘Take on a clinical role when it’s busy’ while others
firmly believe that N/MUM should be letting go
of their ‘clinical and collegial role’ and ‘moving to
management and leadership’.
n Have clinical knowledge but not expertise.
n Be ‘in control’ and know the difference between
leadership and management.
Health service personnel expect N/MUMs to:
n Have skills in ‘small business management’.
n Have knowledge of all aspects of service delivery.
n Have a presence and visibility on the ward.
n Be a role model.
n Undertake human resource functions.
n Successfully instigate and manage change as well as
maintain contact (‘talking’) with patients.
n ‘I need them to do what I ask them to do’.
n Be financially prudent because they are ‘managing part
of a multi-million dollar business’.
n ‘Know what drives the business’.
n ‘We expect them to know who is in bed 6 and why
the budget is over’.
Stakeholders’ perceptions of a successful or less successful N/MUM
Only 24% (n = 29) of the 120 stakeholders other than
N/MUMs attempted to identify the characteristics of a
successful N/MUM, while only five attempted to identify
those attributes that contribute to the N/MUM who is
less successful. This is a small group whose analysis of
the attributes will necessarily be based on their own
experience. This information was therefore not included
in this report.

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 21
Conclusion and Next Steps
It is acknowledged that N/MUMs have a pivotal role in
managing and co-ordinating patient care activities at the
ward/unit level. As a result of the diagnostic phase of
the “take the lead” project, it is clear that the N/MUMs
role and related responsibilities and accountabilities vary
across the state and are often dependant on the context
in which they work and the tasks others expect them to
perform.
It has been identified that more than 60% of activities
N/MUMs participate in are transactional in nature
related to managing the business aspects of the ward/
unit. The remaining 40% of activities relate to quality
and safety, patient care activities and leadership. Other
key stakeholders interviewed agreed that N/MUMs are
loaded with administrative tasks that could be done
by others. Key stakeholders were also clear in their
expectations that N/MUMs should be co-ordinating,
directing and leading care within the ward/unit.
National and international research identifies leadership
development for front line nursing managers as critical to
ensure they are able to manage the complex challenges
within a constantly changing health care system and
enact positive sustainable change (Duffield et al 2007b;
ICN/FNIF 2006; Laschinger & Wong 2007a; Read et al
2004; The Scotland Government 2008).
Information collected from workshops with N/MUMs
identified that they often feel ill equipped to perform
their diverse role, and the availability of appropriate
professional development and education that specifically
meets the needs of this role is variable and at times
limited. From the questionnaire responses of 564
N/MUMs it was also identified that 43% (n=264)
apparently have their entry level nursing qualification as
the highest level of formal education.
As a result of the consultation processes and data
analysis three work streams have been identified.
These are:
n Defining and seeking agreement on the purpose and
core functions of the N/MUM role across NSW,
n Identifying strategies to address the education and
professional development required to support and
strengthen the N/MUM role,
n Outlining strategies to address the number of
transactional (administrative) tasks N/MUMs currently
undertake.

PAGE 22 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Aiken, L., Clarke, S.P., Sloane, D.M., Sochalski, J. & Silber,
J.H. (2002). Hospital nurse staffing and patient mortality,
nurse burnout, and job dissatisfaction. Journal of the
American Medical Association, 288, 1987-1993.
Baumann, A, (2007). Positive Practice Environments:
quality workplaces = Quality patient care. Information
and Action Tool Kit. International Council of Nurses
(ICN), Geneva Switzerland.
Baumann, A., O'Brien-Pallas, L., Armstrong-Stassen, M.,
Blythe, J., Bourbonnais, R., Cameron, Doran, D.I, Kerr,
M., McGillis-Hall, L., Vezina, M., Butt, M., & Ryan, L.
(2001). Commitment and care: The benefits of a healthy
workplace for nurses, their patients and the system.
Canadian Health Services Research Foundation, Ottawa,
Ontario, Canada.
Buchan, J., Calman, L. (2005). The Global Shortage
of Registered Nurses: An Overview of Issues and
Actions. International Council of Nurses (ICN), Geneva
Switzerland.
Casida, J.M. (2007). The relationship of nurse managers
leadership styles and nursing unit organisational culture
in acute care hospitals in New Jersey. PhD thesis, Seaton
Hall, New Jersey, USA.
Duffield, C.M. (1989). The Competencies Expected Of
First-line Nursing Managers - An Australian Context.
Journal of Advanced Nursing, 14(12), 997-1001.
Duffield, C.M. (1991). First-line nurse managers: Issues
in the Literature. Journal of Advanced Nursing, 16(1),
55-62.
Duffield, C.M. (1994). Role Competencies of First-line
Managers. Nursing Management, 23(6), 49-52.
Duffield, C.M. (1995). Future Responsibility and
Requirements for First-Line Nurse Managers in New
South Wales. Journal of Nursing scholarship, 24(1), 9-43.
Duffield, C.M., Donoghue, J.M., Pelletier, D.S. & Adams,
A.F. (1993). First-line nurse managers in NSW: perceived
role competencies (Part II). Contemporary Nurse 2(3),
110-117.
Duffield, C. M. & Franks, H. (2001). The role and
preparation of first-line nurse managers in Australia:
where are we going and how do we get there? Journal
of Nursing Management, 9(0), 87-91.
Duffield, C., Kearin, M., Johnston, J., & Leonard, (2007a).
The impact of hospital structure and restructuring on
the nursing workforce. Australian Journal of Advanced
Nursing, 24(3), 42-46.
Duffield, C.M., Moran, P., Beutel, J., Bunt, S., Thornton,
A., Wills, J., Cahill, P. & Franks, H. (2001). Profile of first-
line managers in NSW, Australia in the 1990's, Journal of
Advanced Nursing, 36, 785-793.
Duffield, C.M., Roche, M.A., O'Brien-Pallas, L., Diers,
D., Aisbett, C., King, M.T., Aisbett, K., Hall, J.P. (2007b).
Glueing it together: nurses, their work environment and
patient safety, Centre for Health Services Management,
UTS, Sydney, 1-243.
Queensland Health. (2008). Review of the Nurse Unit
Manager Role. Office of the Chief Nurse, Queensland
Health. (unpublished at present)
ICN/FNIF, (2006). Global Nursing Shortage: Priority Areas
for Intervention: A Report from International Council
of Nurses (ICN)/ Florence Nightingale International
Foundation (FNIF), Geneva Switzerland.
Laschinger, H. & Wong, C. (2007a). A profile of the
Structure and Impact of Nursing Management in
Canadian Hospitals. Final Report for Canadian Health
Services Research Foundation (CHSRF) Ottawa, Ontario,
Canada.
References

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 23
Laschinger, H. & Wong, C. (2007b). Canadian Nursing
Leadership Study Invitational Symposium: Final Report 26
Canadian Health Services Research Foundation, Ottawa,
Ontario, Canada
McGuire, E. & Kennerly. S. M. (2006) Nurse Managers
as Transformational and Transactional Leaders. Nursing
Economics 24(4), 179-184)
Moran, P. Duffield, C.M. Beutel, J., Bunt, S., Thornton,
A., Wills, J., Cahill, P. & Franks, H. (2002). Nurse
Managers in Australia: Mentoring, leadership and Career
Progression. Canadian Journal of Nursing Leadership,
15(2), 14-20.
NSW Health (2000) A new direction for NSW State
Health Plan-Toward 2010, NSW Health
NSW Health (2006). Profile of the Nursing Workforce in
NSW. An overview of information from the 2006 Labour
Force Survey, Workforce Development and Leadership
Branch, NSW Health.
NSW Health (2007) NSW Health Patient Survey 2007
Statewide Report
NSW Health (2008) The NSW Public Health System
Nurse’ & Midwives’ (State) Award.
Paliadelis, P. 2005. Rural nursing unit managers:
education and support for the role. Rural and Remote
Health 5(325)
Read, S., Ashman, M., Scott, C., Savage, J. (2004).
Evaluation of the modern matron role in a sample of
NHS trusts, Final Report to the Department of Health.
The Royal College of Nursing Institute and the University
of Sheffield School of Nursing and Midwifery.
RNAO Registered Nurses’ Association of Ontario, (2006).
Developing and Sustaining Nursing Leadership. Toronto,
Canada: Registered Nurses’ Association of Ontario.
The Scottish Government (2008). Leading Better Care:
Report of the Senior Charge Nurse Review and Clinical
Quality Indicators Project, The Scottish Government,
Edinburgh, Scotland.

PAGE 24 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Aged Care Assessment Team
Acute Geriatric
Acute Medical
Adolescent Health
Adolescent Mental Health
Adult Correction Centre
Aged Care
Aged Care Psychiatry
Aged Care Rehabilitation
Aged Care/Community Health
Aged Care/Dementia
Aged Day Care Community
Ambulatory Care
Anesthesia/Recovery
Antenatal/Gynecology
Birth Unit
Brain Injury Rehab
Breast Cancer Oncology
Burns Unit
Cancer Services
Cardiology
Cardiothoracic
Child and Family Health
Colorectal
Community Health
Critical Care Unit
Day Surgery
Drug and Alcohol Services
ED/HDU
Emergency
Endoscopy
General Medicine
Geriatric Medicine
Gl Surgery
Gosford ED
GP Casualty
Hematology
HIV Aids Dementia & Psych
ICU
Maternity
Medical
Mental Health
Midwifery
Midwifery Aboriginal Health
Neonatal Intensive Care
Nephrology/Gastro
Neural Trauma High Dependency
Neuroscience
Newborn Care
Oncology
Operating Theatre
Operating Theatre/Recovery
Opioid Treatment Services
Ophthalmology
Orthalmology
Paediatric
Palliative Care
Preoperative Services
Postnatal/Antenatal/Gynecology
Primary Care Health
Psycho Geriatrics
Radiology
Rehabilitation
Renal
Residential Aged Care
Respiratory Medicine
Sexual Health
Spinal Cord Injury
Stroke Unit
Surgical Ward
Transitional Care Unit
Tresillian Child and Family Health
Tuberculosis/Chest
Upper GI and Gastro
Urology
Women's Health
Appendix 1 – N/MUM Workshops, Clinical Areas
Clinical areas represented in N/MUM workshops

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 25
Appendix 2 – N/MUM Workshops, Hospitals
Hospitals/Health Services represented in N/MUM workshops
Albury Base Hospital
Armidale Hospital
Auburn Hospital
Ballina Hospital
Barkala Aged (Acute) TSH
Bathurst Base Hospital
Bathurst Comm Mental Health
Bega Hospital
Bellingen Hospital
Belmont Hospital
Blacktown Hospital
Bloomfield Hospital
Blue Mountains Hospital
Bourke Health Service
Broken Hill Base Hospital
Bulli Hospital
Calvary Hospital
Canterbury Hospital
Casino & Corak Hospital
Cessnock Hospital
The Children's Hospital at Westmead
Coffs Harbour Hospital
Coledale Hospital
Collarenebn Health Service
Concord Hospital
Coonabarabran Health Service
Coonamble Health Service
Cowra Health Service
Croucester Soldiers Memorial Hospital
Dubbo Health Service
Eloura West Shellharbour Hospital
Eurobodalla - Moruya Health Service
Forbes Health Service
Garrawarra Hospital
Gosford Hospital
Grenfell Multi Purpose Service
Hawkesbury Hospital
Hoxton Park Community Health Centre
John Hunter Children's Hospital
John Hunter Hospital
Kaleidoscope Child & Family Nursing
Kempsey District Hospital
Kyogle Memorial Hospital
Lismore Base Hospital
Lithgow Hospital
Liverpool Hospital
Macarthur Health Service
Maclean Hospital
Maitland Hospital
Manning Base Hospital
Merrylands Hospital
Moruya Hospital
Mt Druitt Hospital
Mudgee Health Service
Mullumbimby Hospital
Murwillumbah Hospital
Nepean Hospital
Nowra Community Health Centre
Orange Base Hospital
Parkes Communityy Mental Health
Parramatta Community Hospital
Port Kembla Hospital
Port Macquarie Base Hospital
Prince of Wales Hospital
Riverlands Hospital
Royal North Shore Hospital
Royal Newcastle Centre
Royal Prince Alferd Hospital
Sacred Heart Hospice
Sydney Children's Hospital
Shellharbour Hospital
Shoalhaven Hospital
Singleton Hospital
St George Hospital
St Vincent's Hospital
St Heliers Hospital
St Joseph Hospital
Sydney Hospital
Tamworth Base Hospital
The Tweed Hospital
Trundle Multi Purpose Service
Tullamore Multi Purpose Service
Tweed Byron Community Health
Tweed Byron Mental Health
Urbenville Health Service
Wagga Base Hospital
Walgett Health Service
Wallsend Aged Care Facility
War Memorial Hospital
Warren Multi Purpose Service
Wauchope Hospital
Wingham Hospital
Westmead Hospital
Wollongong Hospital
Wyong Hospital
Yarrabee TSH
Yass Hospital
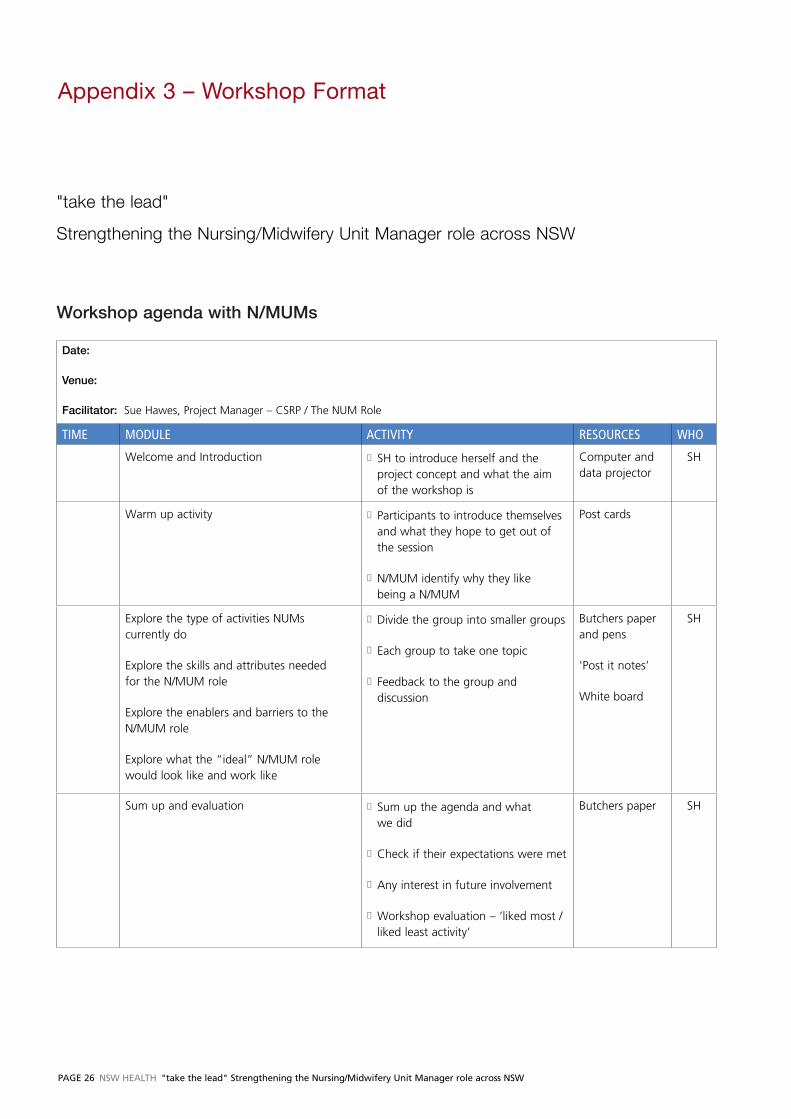
PAGE 26 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Appendix 3 – Workshop Format
Date:
Venue:
Facilitator: Sue Hawes, Project Manager – CSRP / The NUM Role
TIME MODULE ACTIVITY RESOURCES WHO
Welcome and Introduction n SH to introduce herself and the project concept and what the aim of the workshop is
Computer and data projector
SH
Warm up activity n Participants to introduce themselves and what they hope to get out of the session
n N/MUM identify why they like being a N/MUM
Post cards
Explore the type of activities NUMs currently do
Explore the skills and attributes needed for the N/MUM role
Explore the enablers and barriers to the N/MUM role
Explore what the “ideal” N/MUM role would look like and work like
n Divide the group into smaller groups
n Each group to take one topic
n Feedback to the group and discussion
Butchers paper and pens
'Post it notes’
White board
SH
Sum up and evaluation n Sum up the agenda and what we did
n Check if their expectations were met
n Any interest in future involvement
n Workshop evaluation – ‘liked most /liked least activity’
Butchers paper SH
"take the lead"
Strengthening the Nursing/Midwifery Unit Manager role across NSW
Workshop agenda with N/MUMs

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 27
Appendix 4 – N/MUM Questionnaire
"take the lead"
Specialty area currently working in _________________________________________________________________________
What is your position called (e.g. N/MUM, Clinical Co-ordinator etc) _____________________________________________
1. Are you ? (Please √) Full time o Part time o
2. Are you ?
Permanent in the role o Acting in the role o Other o
3. Are you paid as a ?
NUM 1 o NUM 2 o NUM 3 o Other o
4. How long have you been a N/MUM?
< 12 months o 1-2 years o 3-5 years o 6-10 years o >10 years o
5. Do you have a copy of your position description?
Yes o No o Unsure o
6. What is the highest level of education you have attained (Please √ only one box):
Hospital Certificate o Associate Diploma o Diploma o Bachelor's Degree o
Graduate Certificate o Graduate Diploma o Master's Degree o PhD o
7. Do you have access to a computer at work ?
Yes o No o Comment:________________________________________________________________________
8. Do you have access to the Internet at work ?
Yes o No o Comment:________________________________________________________________________
9. Do you have a clinical (patient) load in your day-to-day duties? Yes o No o
If “yes” (Please √):
Part of my Position Description o
OR
Rarely o Sometimes (2-4 shifts per month) o Often (twice per week) o
10. Would you be interested in becoming involved with activities related to this project?
Yes, please contact me with more information o No o
Name:__________________________________________________________________________________________________
Email:__________________________________________________ Telephone Number: ______________________________

PAGE 28 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Appendix 5 – N/MUM Forum Day Agenda
Nursing & Midwifery Unit Manager Forum
0830 Coffee and Registration
0900 Overview and Housekeeping Sue Hawes, Project Manager NaMO NSW Health Department
0920 Keynote Welcome Professor Debora Picone AM, Director General
NSW Health Department
0930 NUM/MUM Data feedback and validation Sue Hawes
1045 Morning Tea
1115 Where are we now? Theatrical Presentation
1145 Where could we go? Theatrical Presentation
1215 Lunch
1300 NUM/MUM Workshops
1530 Regroup and snapshot review Sue Hawes, Project Manager
1545 Closing Remarks Adjunct Professor Debra Thoms,
Chief Nursing and Midwifery Officer
NaMO NSW Health Department

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 29
Appendix 6 – Key Pad Summary Results
Turning Graphical Results by Question
Session Name: New Session 3.27.2008 4.27PM.tpz
Created: 3/27/2008 4:29 PM
2) HOW WOULD YOU PREFER TO HEAR ABOUT "TAKE THE LEAD" PROJECT ACTIVITIES ?
RESPONSES
"take the lead" Website 18 14%
Email 74 58%
Regular "take the lead" newsletter 34 26%
From your line manager 3 2%
Don't want to hear anything 0 0%
Totals 129 100%
From your line manager
"take the lead" website
Regular "take the lead" newsletters
PIE 4
"take the lead" newsletter
Email sent by Project Manager
Your line manager
Another N/MUM
Other
1) HOW DID YOU HEAR ABOUT TODAY'S FORUM?
RESPONSES
"take the lead" newsletter 7 5%
Email sent by Project Manager 34 26%
Your line manager 65 50%
Another N/MUM 5 4%
Other 20 15%
Totals 131 100%
3) HOW CONFIDENT ARE YOU THAT ANYTHING WILL CHANGE AS A RESULT OF "TAKE THE LEAD" PROJECT?
RESPONSES
Confident 43 31%
Not confident 42 31%
Unsure 52 38%
Totals 137 100%
Con�dent
Not con�dent
Unsure

PAGE 30 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
4) HOW CONFIDENT ARE YOU THAT "TAKE THE LEAD" WILL MAKE A DIFFERENCE TO ...
RESPONSES
You the N/MUM 10 8%
The team 5 4%
The patients and carers 2 2%
All of the above 46 35%
None of the above 11 8%
Unsure 57 43%
Totals 131 100%
You the N/MUM
The team
The patients and carers
All of the above
None of the above
Unsure
5) ARE YOU ABLE TO HAVE MEANINGFUL CONVERSATIONS WITH YOUR LINE MANAGER ABOUT MAKING CHANGES?
RESPONSES
Yes 90 68%
No 43 32%
Totals 132 100%
Yes
No
6) WHERE DO YOU SEE YOUR BIGGEST OPPORTUNITY FOR CHANGE ? RESPONSES
Recruitment and retention 14 10%
Patient care co-ordination 24 18%
Financial/budget management 6 4%
Developing staff 25 19%
Quality and safety 12 9%
Communication 13 10%
Managing staff 15 11%
Self empowerment 21 16%
Self development 4 3%
Totals 131 100%
Recruitment and retention
Patient care co-ordination
Financial/budget management
Developing sta�
Quality and safety
Communication
Managing sta�
Self empowerment
Self development
7) DID YOU ATTEND A "TAKE THE LEAD" WORKSHOP FACILITATED BY EITHER SUE OR HELENA?
RESPONSES
Yes 78 57%
No 60 43%
Totals 138 100%
Yes
No

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 31
9) ARE YOU CURRENTLY ENROLLED IN A TERTIARY PROGRAM THAT IS RELATED TO MANAGEMENT, LEADERSHIP OR BUSINESS ADMINISTRATION ?
RESPONSES
Yes 23 16%
No 118 84%
Totals 141 100%
10) THE EMERGING THEMES DESCRIBED ABOUT WHY YOU LIKE BEING A N/MUM ARE...
RESPONSES
A true reflection 134 98%
Not reflective 3 2%
Totals 137 100%
11) HAVE YOU CHANGED ANYTHING IN YOUR OWN PRACTICE SINCE ATTENDING A "TAKE THE LEAD" WORKSHOP?
RESPONSES
Yes 28 20%
No 47 34%
Did not attend workshop 63 46%
Totals 138 100%
8) SINCE BECOMING A REGISTERED NURSE/MIDWIFE HAVE YOU COMPLETED ANY OF THE FOLLOWING TERTIARY (UNIVERSITY) QUALIFICATIONS? (SELECT THE HIGHEST DEGREE)
RESPONSES
Bachelor of Health Administration 8 6%
Graduate Certificate in Management, Health Management
17 12%
Graduate Diploma in Management, Health Management
14 10%
Masters in Management, Health Management
14 10%
PHD 1 1%
None of the above 86 61%
Totals 140 100%
Bachelor of Health AdministrationGraduate Certi�cate in Management,Health Management
Graduate Diploma in Management, Health Management
Masters in Management, Health Management
PHDNone of the above
Yes
No
A true re�ection
Not re�ective
Yes
No
Did not attend a workshop

PAGE 32 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
15) THE EMERGING THEMES DESCRIBED ABOUT THE LEADERSHIP ASPECTS OF YOUR ROLE ARE...
RESPONSES
A true reflection of what currently happens
140 99%
Not a true reflection of what currently happens
2 1%
Totals 131 100%
PIE 18
A true re�ection of what currently happens
Not a true re�ection of what currently happens
14) THE EMERGING THEMES DESCRIBED ABOUT THE QUALITY AND SAFETY ASPECTS OF YOUR ROLE ARE...
RESPONSES
A true reflection of what currently happens
142 100%
Not a true reflection of what currently happens
0 0%
Totals 131 100%
13) THE EMERGING THEMES DESCRIBED ABOUT THE CO-ORDINATION OF PATIENT CARE ASPECTS OF YOUR ROLE ARE...
RESPONSES
A true reflection of what currently happens
134 96%
Not a true reflection of what currently happens
5 4%
Totals 139 100%
12) THE EMERGING THEMES DESCRIBED ABOUT THE GENERAL MANAGEMENT ASPECTS OF YOUR ROLE ARE...
RESPONSES
A true reflection of what currently happens
132 96%
Not a true reflection of what currently happens
5 4%
Totals 137 100%
A true re�ection
PIE 21
A true re�ection
Not re�ective
A true re�ection
Not re�ective

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 33
PIE 22
A true re�ection of what you want to happen
Not re�ective of what you want to happen
19) THE EMERGING THEMES DESCRIBING THE IDEAL ROLE ARE... RESPONSES
A true reflection of what you want to happen
142 99%
Not reflective of what you want to happen
74 1%
Totals 129 100%
18) THE EMERGING THEMES DESCRIBED ABOUT THE SKILLS AND ATTRIBUTES TO YOUR ROLE ARE...
RESPONSES
A true reflection 142 100%
Not reflective 0 0%
Totals 142 100%
PIE 21
A true re�ection
17) THE EMERGING THEMES DESCRIBED ABOUT WHAT ENABLES YOU TO DO YOUR ROLE ARE...
RESPONSES
A true reflection of what currently happens
131 95%
Not a true reflection of what currently happens
7 5%
Totals 138 100%
PIE 20
A true re�ection of what currently happens
Not a true re�ection of what currently happens
16) THE EMERGING THEMES DESCRIBED ABOUT THE BARRIERS TO YOUR ROLE ARE...
RESPONSES
A true reflection of what currently happens
136 98%
Not a true reflection of what currently happens
3 2%
Totals 139 100%
PIE 18
A true re�ection of what currently happens
Not a true re�ection of what currently happens

PAGE 34 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
20) HOW CONFIDENT ARE YOU THAT ANYTHING WILL CHANGE AS A RESULT OF "TAKE THE LEAD" PROJECT?
RESPONSES
Confident 81 65%
Not confident 43 35%
Totals 124 100%
Con�dent
Not con�dent
21) HOW CONFIDENT ARE YOU THAT "TAKE THE LEAD" WILL MAKE A DIFFERENCE TO ...
RESPONSES
You the N/MUM 24 18%
The team 5 4%
The patients and carers 6 5%
All of the above 73 56%
None of the above 23 17%
Totals 131 100%
22) ARE YOU WILLING TO BECOME A "TAKE THE LEAD" CHAMPION, LEADING CHANGES IN YOUR LOCAL FACILITY OR COMMUNITY AREA ?
RESPONSES
Yes 63 53%
No 57 47%
Totals 132 100%
PIE 25
You the NUM/MUM
The team
The patients and carers
All of the above
None of the above
Yes
No

NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW PAGE 35
Appendix 7 - N/MUM Workshop General Management Functions
Daily ward administration and management
Photocopy, faxing, filing
Disaster management: plans and audits
Proposals, submissions and reports
Service planning
General ward and theatre cleaning
Car & fleet management and maintenance
Universal problem solving
Project management
Resource person for general and specific health information
Strategic planning
Business cases and plans
Trouble shoot problems
Food service, catering officer
Fundraising in community
Plan social functions, raffle prizes & supplies for fundraising
Security & security management plans
Computer programs & support
Order ward food (tea, coffee), stores and supplies
Monitor and manage change
After hours contact
Change agent
Typing minutes from meetings
Dealing with drug and product reps
Switchboard operation
Mail: collection, sorting, distributing
Building and site manager
Building refurbishment redesign, planning and development
Signing documents
Meeting & monitoring KPI's: medication errors, pressure areas, falls
Events planning, co-ordination and management
Hospital portfolio on top of NUM role
Research
Ward clerking
Manage the barriers
Education and orientation
Feedback
Budget
Be a middle manager as well as a front line manager
Investigate everything before acting
Set the tone of your unit
Keep abreast of technological change and implementation
Crisis management
Arranging agendas for meetings
Keep the notice board up to date
Notification births to Births, Death and Marriages
Update ward brochures
Write and type letters
Creating new ways of doing things
Printing patients labels
Organizing IT access for all staff
Answering the phone
Taking phone enquiries from public patients and health professionals
Public speaking to community groups
Acquisition of health service premises
Access control
Community Liaison
Health promotion
Careers advisor for High School
Clinical redesign
Winter bed strategy
Surge capacity
Bed utilization strategy
Review of other area business plans
General management functions of NSW N/MUMs
The following general functions of the N/MUMs were identified by those attending workshops. The most common general
management functions of a N/MUMs are at the top of the list with less frequent functions towards the bottom of the list.

PAGE 36 NSW HEAltH "take the lead" Strengthening the Nursing/Midwifery Unit Manager role across NSW
Appendix 7 (continued)
Ward cleaning: drug fridge and all other equipment
Pest control
Attending to building alarms
Organize funeral for destitute person
Ethics and law officer
Coordinate emergency response
Public relations
Building works - quotes, resource information on building
Time manager and time manager consultant
Public relations officer
Representative face of service
Provide safe harmonious work environment
Travel agent
Spokesperson for unit
Media officer
Police contact
Community Liaison officer - builders
Wash the dog
Audits and overseeing of same e.g. S4 and S8 and files
Manage bed closures staff redeployment
Open door
Donation responses
Take work home
Downtime "lockdown" management
Aboriginal Unit Liaison Programs
Pandemic Plan
Clinical stream management
Investigate & follow up with parents
Angry parent/staff meeting
Ward closures and mergers
Statewide projects
Unpacking stores
Being the middleman between area ideas and ward staff
Housekeeping issues
Policy changes
Monitor and coordinate clinics for VMO
Planning theatre schedules and lists
Hospital management
Keeping the finger on the pulse
Travel between sites
Answer everyone's questions
Manager community service


SHPN (NAMO) 090041