streptomycin treatment tuberculous meningitis · july 1948 cathie: streptomycin treatment of...
TRANSCRIPT

351
THE STREPTOMYCIN TREATMENT OFTUBERCULOUS MENINGITIS
By I. A. B. CATHIE, M.D.Clinical Pathologist, The Hospital for Sick Children, Great Ormond Street, London
Streptomycin is the antibiotic principle pre-pared from Streptomyces griseus, and it is activeagainst a wide range of bacteria. Its chief in-terest lies in its activity against M. tuberculosis.The scarcity of streptomycin in this country hasled in the main to its use only in conditions forwhich no other form of treatment 1s available, andof these conditions in children tuberculousmeningitis has received the most attention.The toxicity of streptomycin is well known, and
of the many toxic manifestations vestibulardamage, skin rashes and damage to the kidnevsare the most frequently seen. Of lesser importanceand not calling for reduction of dosage of the drugare headache in the third week or so of treatmentand transient numbness of the lips. It is difficultto assess the subjective effects of streptomycin inchildren, particularly as many of them have beenso young, but with the dosage employed no toxicsigns certainly due to the drug have been observed.
Intramuscular streptomycin is painful, the painprobably being due to the presence of impurities.It can be mitigated by the inclusion of a littlenovocain in the same syringe. With intrathecalinjection of streptomycin some of the biggerpatients have complained of pain in the back andlegs when the lumbar route is used, while alarmingreactions, with collapse and coma, have occasion-ally been seen following intracysternal injection.The amount of drug tolerated by the cysternamagna seems clearly to be less than that by thelumbar route.Of fundamental importance in the streptomycin
treatment of any tuberculous condition is thesensitivity of the particular organism to the drug.From primary isolation the great majority ofstrains of M. tuberculosis have an in vitro in-hibitory level of one-eighth to half a unit ofstreptomycin per ml., a unit being one millionth ofa gramme. The readiness with which the or-ganism from treated pulmonary cases becomesdrug-resistant seems to be rarer in meningitis, andstrains recovered at autopsy after seven or moremonths continuous treatment with streptomycinhave been found to have the same in vitro sen-sitivity as that of the primary isolation. For
testing sensitivity, isolation has to be made byculture or from a guinea pig, after which a stan-dard suspension is prepared for inoculation intoserial dilutions of streptomycin. in Dubos'smedium, where reading is made after ten days.Thus it may be six weeks or longer before thesensitivity of a strain is known.As the earlier the disease is treated the better
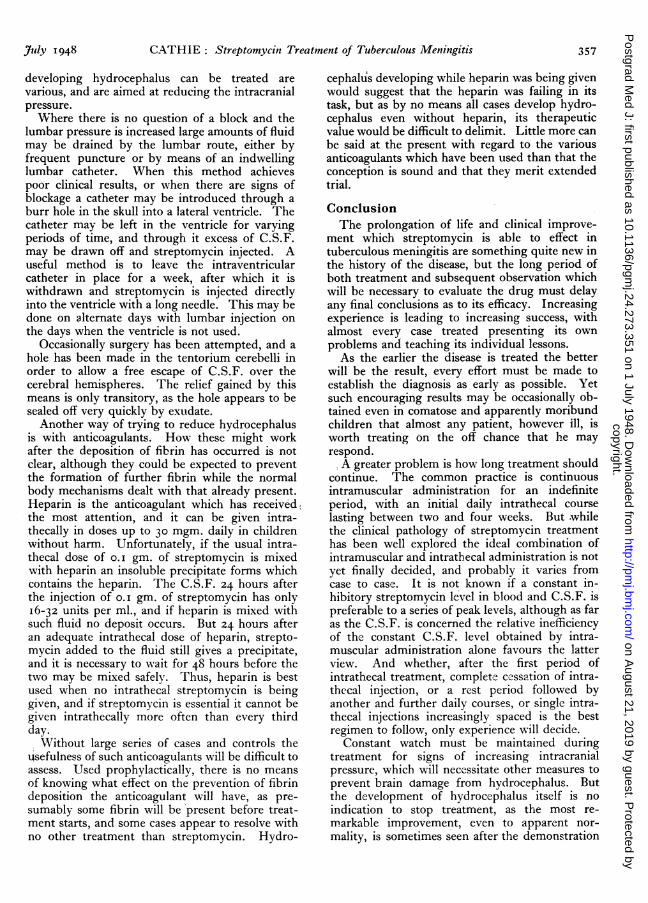
appear to be the results, it would be quite im-possible to wait for sensitivity levels before com-mencing streptomycin therapy, and the dosagechosen is made on the assumption of a usualsensitivity of the organism to the drug. The aimis to maintain a constant inhibitory level in theblood, while the same level in the cerebrospinalfluid is maintained for varying periods according tothe progress of the case.With the dose of 0.02 gm. per lb. of body weight
per day given in distilled water intramuscularlysix-hourly, the blood levels have been consistentlysatisfactory. In bccasional cases a transitory levelof 64 units per ml. at the end of the first hour maybe seen, and at six hours a level of i6 units isexceptionally found, but in the main the figuresfall within the lined area in Fig. I. It will be seenthat six hours after the injection, levels of 2 to8 units per ml. are present, an amount well inexcess of the inhibitory I unit.An intramuscular injection every six hours for
periods of six months or more can be a great trialboth to patient and nursing staff, and the samedaily amount of streptomycin given I2-hourly pro-duces nearly as satisfactory blood levels. Fig. 2shows the type of curve with this method ofspacing, and even at 12 hours levels of 4 unitsmay be seen. In one child of i years the cal-culated dose was 2 gm. per day, and as this upsetthe patient considerably the dose was halved,being given as o.oI gm. per lb. of body weight perday 12-hourly: Fig 3 shows that there was stilla therapeutic level at 12 hours, the 2 units perml. in this case being eight times the in vitroinhibitory level for the particular organism.- In cases without meningitis, streptomycinpenetrates only slightly into the cerebrospinalfluid after intramuscular injection, and levels of
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from
copyright.
on August 21, 2019 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.24.273.351 on 1 July 1948. Dow
nloaded from
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

352 POST GRADUATE MEDICAL JOURNAL July 1948
40 units per ml.
30 N
20
10
1 2 3 4 5 Hours
Fig. 1. Blood levels obtained with 0.2 gm. per lb. of bodyweight per day given 6-hourly.
0.5 units per ml. of C.S.F. or less are found. Butwhen meningitis is present higher levels, up to 2and 4 and rarely 8 units, are seen. Fig. 4 shows theC.S.F. findings in a case of miliary tuberculosiswhich developed tuberculous meningitis while onintramuscular streptomycin, and demonstrates thegreater facility with which the drug can cross aninflamed barrier. This higher streptomycin levelis an almost constant finding, and is a reliableindication of meningeal inflammation. Suchlevels are above the average inhibitory amount forM. tuberculosis, and were the rationale for at-tempting to treat some cases of tuberculousmeningitis by the intramuscular toute alone.Above the age of two years, a dose of o.i gm. of
streptomycin diluted in saline is well toleratedwhen given intrathecally by the lumbar route,while under two half this amount should be given.Intracysternally and intraventricularly the irritanteffects of streptomycin are more readily observed,and the amount injected should not exceed o.05gm. One hour after the injection of such amounts,the streptomycin level in the C.S.F., as might beexpected, is very high and after 24 hours thelevels are usually found within the range of 8 toI6 units per ml. of C.S.F.The irritant effect of streptomycin on the theca
is well illustrated when o.I gm. is injected into anormal thecal space. The results of such an in-jection by the lumbar route are shown in Fig. 5,when physiological saline was the diluting fluid.As it has been suggested that the cellular increasemay be due to the saline and not the streptomycin,the lower half of Fig. 5 shows the result whenstreptomycin dissolved in normal cerebrospinalfluid is injected. In each case the considerablepleiocytosis was polymorphonuclear, and the cellcount had returned to normal within a week. Theprotein in each case was rather higher than before
the streptomycin was given. The cellular rise isnot seen to anything like the same extent inmeningitis.
In many cases of established tuberculousmeningitis under streptomycin therapy the cellsand biochemistry have been followed daily as aroutine, in the hope that some prognostic changemight be observable. The daily variations in thecells and protein which may be seen in almost anycase are depicted in Fig. 6. All that can be saidis that these elements appear roughly to vary inthe same direction; the day to day oscillation isso wide as to give little information of value forprognosis. The same may be said of daily sugarand chloride estimations. A general rise or fall inthe protein and cells gives a rough indication ofdeterioration or improvement in the condition, andhas proved to be more reliable than apparentclinical change. The cell differential count hasshown a greatly predominant lymphocytosis, andpossibly some of the polymorphs present are dueto the streptomycin irritation already referred to.No alteration in the differential count, as distinctfrom the total count, has proved useful inprognosis.A rising C.S.F. protein as a sign of impending
block is well recognized. A prognostic point inthis connection is a rising protein with fallingcells when clinical improvement is occurring.Many cases which have done outstandingly wellwith streptomycin treatment have shown thisdivergence. Fig. 7 shows the C.S.F. in such acase, the patient having been treated for twomonths before the chart begins. At a pointcoinciding with clinical improvement the protein
80 units per ml.
70
60
50
40
20
10
Hours 12
Fig. 2. Blood levels obtained with 0.2 gm. per lb.of body weight given 12-hourly.
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

July 1948 CATHIE : Streptomycin Treatment of Tuberculous Meningitis 353
continued to rise while the cells fell. During aslight clinical relapse the two converged, but drewapart again as the patient improved. The child isnow clinically cured, and has a C.S.F. chemicallynormal and with four lymphocytes per cu. mm.In a similar case while the cells were falling theprotein rose to a peak of 7,000 mgm. beforestarting to fall.There is no doubt that streptomycin itself may
be the cause of some of the variation in protein.In a baby with coliform meningitis treated withintrathecal streptomycin for one week (Fig. 8), inspite of immediate sterilization of the fluid andclinical cure the protein remained raised, and 17weeks after the streptomycin was given the C.S.F.protein level was still 75 mgm. This prolongedhigh level is almost certainly a streptomycin effect,as it is not seen in cases of purulent meningitiscured without streptomycin. Support for thisview is lent by the findings after streptomycin isinjected into a normal theca (Fig. 5), where anincrease in protein is seen.
Streptomycin is excreted in the urine, and itsconcentration depends upon the system of dosageand the amount of urine passed. Therapeuticlevels are found constantly even when the drug isgiven once daily, and figures of 500 and I,ooounits per ml. of urine are frequently seen.The blood sedimentation rate nearly always falls
in the initial stages of streptomycin treatment andrises again if the case fails to respond and deathapproaches. This is in interesting contrast tomost untreated cases of tuberculous meningitis,
10 units per ml.
9-
8
7
6
5
4
3
2 -
1
Hours 12
Fig. 3. Blood levels obtained with 0.1 gm. per lb.of body wieght given 12-hourly.
Cells
300 cells Streptomycin3 units
200- /2 / /
//-/ /X //
100 /1 /
-- --- - ---/
1 2 3 Weeks
Fig. 4. Developing meningitis, showing concomitantincrease in C.S.F. streptomycin.
where the sedimentation rate rises as the diseaseprogresses and falls terminally.
Although we now know enough about strepto-mycin to be able to use it rationally there is somuch individual variation from case to case oftuberculous meningitis that no stereotyped schemeof therapy can be expected to produce the sameresults. The following two cases illustrate someof the problems which are constantly being seen.The first child, aged two, with miliary tubercu-
losis and meningitis, was treated for two monthscontinuously with intramuscular streptomycin andfor one month daily with the drug intrathecallyfollowed by a rest of a week and then a furtherweek's intrathecal course. In spite of a transientclinical improvement the cells and protein in theC.S.F. rose, and the child died two months afterthe commencement of treatment. Fig. 9 showsthe radiological appearance of the lungs onadmission. At autopsy the lungs felt soft andnodules were not palpable. Fig. io is an X-raypicture of the lungs postmortem, and althoughhistological sections of the lungs showed miliarytubercles the sections of the enlarged paratrachealnodes showed only fibrosis. The meningitisappeared in no way to have been affected by thestreptomycin therapy, and both macroscopicallyand histologically it was typical of the condition.The original strain of M. tuberculosis was sen-sitive to 0.5 unit of streptomycin, while thatisolated at autopsy was resistant to I,ooo unitsper ml. This is one of the unusual instanceswhere streptomycin resistance developed duringthe treatment of meningitis.The most surprising postmortem finding in this
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

354 POST GRADUATE MEDICAL JOURNAL July 1948
PROTEIN CELLS
IN SALINE
Before 16 3
24 hours after 32 1080
7 days after 40 3
IN C.S.F.
Before 24 3
24 hours after 16 1316
7 days after 32 2
Fig. 5. Effect of 0.1 gm. of streptomycin on cellsand protein when injected into a normal theca.
case was an early pyelonephritis. A full urineexamination had been carried out weekly, and oneweek before death there was no albumin or pus inthe specimen and the cultures were sterile. Therewere more than ,000o units of streptomycin perml. in the patient's urine, and the Bact. coliresponsible for the condition was sensitive to I unitof streptomycin per ml. Thus we have an in-fection developing when the urine contains athousand times the inhibitory dose of streptomycinto the organism.The second case was a girl, aged six, with
miliary tuberculosis but without meningitis eitherclinically or on the C.S.F. findings. Treatmentby six-hourly intramuscular streptomycin wasstarted. Routine lumbar puncture was performedweekly, and at the end of the second week thefluid was normal in all its constituents with astreptomycin content of o.125 units per ml. Atthe end of the third week the cells and proteinhad risen and so had the level of streptomycin,and tubercle bacilli were present in the deposit.One week later the protein in the C.S.F. was280 mgm. and there were 2 units of streptomycinper ml. Apart from slight irritability for a fewdays at the end cf the second week there were noclinical signs to suggest the presence of meningealinflammation.As this level of streptomycin is sufficient to
inhibit the growth of most strains of M. tubercu-losis it was decided to treat the patient withintramuscular streptomycin alone. Tubercle bacilliwere present for only a week, and for the nextseven months weekly examination of the C.S.F.showed protein fluctuating around 2oo mgm. andcells up to 250, while the streptomycin level wasnever less than 4 units per ml. Clinical meningitiswas never manifest.
After seven months continuous intramuscularstreptomycin six-hourly, the drug was withdrawnto see what would happen. Within four daystubercle bacilli had reappeared in the C.S.F.This isolation had the same streptomycin in-hibitory level as the original strain grown, whichwas 0.25 units per ml. The patient was put on tointrathecal streptomycin as well as intramuscular,and for eight weeks has shown no change.The points of particular interest in this case are
that meningitis developed after intramuscularstreptomycin was started, that there has neverbeen any evidence of meningitis apart from theC.S.F. findings, and that in seven months ofcontinuous treatment the streptomycin sensitivityof the infecting organism had not altered. Figs.ii and I2 show the radiological improvement inthe miliary process in the lungs during the periodof treatment, with disappearance of mottling andresolution to within normal limits.
Points meriting some discussion are thediagnosis of tuberculous meningitis and thetreatment of hydrocephalus during streptomycintreatment.
DiagnosisAll results indicate that the earlier streptomycin
treatment is started the better the prognosis, so thatthe establishment of the diagnosis of tuberculousmeningitis is of prime importance. The clinicaldiagnosis may be extremely difficult, particularlyas some cases present with such slight signs of
400 protein- ---- cells
300
200 /\i \'
100 ys
Days
Fig. 6. Tuberculous meningitis on intrathecalstreptomycin treatment. Daily variationof cells and protein.
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

July 1948 CATHIE: Streptomycin Treatment of Tuberculous Meningitis 355
meningeal involvement. A contact history is therule, and the Mantoux test is nearly alwayspositive. There is occasionally an unfortunatetendency to discount the diagnostic value of anegative Mantoux reaction, although it appears tobe a very rare finding in established cases. Apoint of clinical interest is the frequency ofobstinate constipation. In one case, indeed, somuch liquid paraffin was given for the constipationthat a dermatitis developed, thought to be due tostreptomycin. Withdrawal of the paraffin, how-ever, and administration of vitamin A cleared thecondition and exonerated the streptomycin.
Diagnosis on the C.S.F. findings may be difficultif M. tuberculosis is not seen, and raised proteinand lymphocytes with a lowered sugar andchloride content are the usual but not invariablefindings. A moderate lymphocytosis and slightlyraised protein are constant findings of littlediagnostic value alone as they occur in so manyother conditions, notably poliomyelitis. Chloridesmay be misleading. In one case of establishedtuberculous meningitis under treatment for sixmonths the chloride level has never fallen below700 mgm., while the low levels produced byvomiting, particularly in children, accompany somany other diseases. A reduced and falling sugarin the C.S.F. is possibly the most suggestivefinding, while a normal level is evidence againsttuberculosis.. M. tuberculosis may be found in thespider's web clot which forms on standing, butmay often be more readily seen in smears fromthe centrifuged deposit.
In a case illustrating how misleading the C.S.F.
protein
....-. cells
300
200
100
We,
Week IWeeks
Fig. 7. Divergence of cells and protein in C.S.F.during improvement of tuberculous meningitiswith streptomycin.
600- Streptomycin given
500 \ Protein
400
300
200 \
1 - -
W100
Weeks
Fig. 8. Persistence of high C.S.F. protein after1 week's successful streptomycin treatmentof coliform meningitis.
may be there was no contact history, the 1/1,oooMantoux test was doubtful, and at all times theC.S.F. showed a high polymorph count. Clinicallythe child was more like an encephalitis thantuberculous meningitis, and after a month's treat-ment with streptomycin the drug was stoppedunder the impression that the diagnosis was wrong,particularly as tubercle bacilli had never beenfound in the C.S.F. A fortnight later a guineapig inoculated with the fluid died with dis-seminated tuberculosis. In another case, a baby ofsix months, there was a family history of opentuberculosis, the Mantoux test was positive, andclinically there was a typical onset of tuberculousmeningitis. The C.S.F. findings supported thediagnosis in that there were much loweredchlorides with raised protein and lymphocytes, butthe sugar content was normal. After five days ofstreptomycin treatment the baby died, and atautopsy was found to have a cerebellar tumour,with no evidence of meningeal tuberculosis
In neither of these cases was the tubercle bacillusfound in the C.S.F. on direct examination. Onreviewing them in the light of subsequentknowledge it was realized that in the first case thecontinued polymorph rather than lymphocyteresponse in the C.S.F. was probably a strepto-mycin reaction, while in the second case in-sufficient importance had been attached to thenormal sugar level. These cases are not cited asevidence to contraindicate the early commence-ment of streptomycin therapy when the diagnosisis only presumptive, but to show how difficult maybe the diagnosis when all the clinical and patho-logical data have been assembled.
Ci
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

356 POST GRADUATE MEDICAL JOURNAL July I948\e
I.i:.I ··· ·:'·i··:· iii·:-·:·
:""
.·;··;· lan.s.i. ..g.gqlr
i·i··
·i·
':'···
:''':
···.·:::id.i.LPsF.pr.ns.x.i.·..::.:::::
:':
·: ·8··::''·
·:···· -·
FJG. 9.-X-ray of chest of child dying with pyelo-nephritis, before treatment.
i·a ........
·..:.:...
::· , . ·':':'';:'.i:.::::lili 'i i':iI
-e.::..:: .:..
...:'-
: ..
FIG. Io.-Postmortem X-ray of lungs of same childas in Fig. 9, two months after streptomycin treat-ment.
":~
*.-i
*s- ~ Ira I
FIG. ii.-Miliary mottling of lungs of child whodeveloped meningitis while on streptomycintreatment.
I'. :·.·.··:iallillili.·...i$i.i.i...b.a"a""l.*l':' ·'· ':' ·:··:
31B.......iii.i..i:'i!'i''i:;':Si''"l:I
i.::l:::
.p.tii%iiial·;··: :i'
:···:· .:.::··:···
.··I·· :i.asasep.i.ir
.. ·:·
.iiiii, ':' ·:· ::'''
::ii
··: .·i,iai·i·. ····.. :·: i:·;:·1,1:..:.:.....'tii.
FIG. 12.-Same as Fig. Ii, to show healing after sixmonths on streptomycin.
HydrocephalusIn cases of tuberculous meningitis treated with
streptomycin coming to autopsy the incidence anddegree of hydrocephalus has been striking. Thecause of this complication seems to be the gela-tinous exudate at the base of the brain interferingwith the normal circulation of the C.S.F., andtrue internal hydrocephalus is seldom seen.
Increasing intracranial pressure may be inferredfrom increased C.S.F. pressure on lumbar tap and
sometimes by the onset of papilloedema. At timeshydrocephalus developes so rapidly that in youngerchildren skull measurements are sufficient toassure the diagnosis, and X-rays show greatlywidened sutures.The prolongation of life which streptomycin
causes alters the clinical aspect of tuberculousmeningitis markedly, so that in its chronic form itis almost a new disease, part of which is thistendency to hydrocephalus. The means by wvhich
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from
CATHIE: Streptomycin Treatment of Tuberculous Meningitis
developing hydrocephalus can be treated arevarious, and are aimed at reducing the intracranialpressure.Where there is no question of a block and the
lumbar pressure is increased large amounts of fluidmay be drained by the lumbar route, either byfrequent puncture or by means of an indwellinglumbar catheter. When this method achievespoor clinical results, or when there are signs ofblockage a catheter may be introduced through aburr hole in the skull into a lateral ventricle. Thecatheter may be left in the ventricle for varyingperiods of time, and through it excess of C.S.F.may be drawn off and streptomycin injected. Auseful method is to leave the intraventricularcatheter in place for a week, after which it iswithdrawn and streptomycin is injected directlyinto the ventricle with a long needle. This may bedone on alternate days with lumbar injection onthe days when the ventricle is not used.
Occasionally surgery has been attempted, and ahole has been made in the tentorium cerebelli inorder to allow a free escape of C.S.F. over thecerebral hemispheres. The relief gained by thismeans is only transitory, as the hole appears to besealed off very quickly by exudate.Another way of trying to reduce hydrocephalus
is with anticoagulants. How these might workafter the deposition of fibrin has occurred is notclear, although they could be expected to preventthe formation of further fibrin while the normalbody mechanisms dealt with that already present.Heparin is the anticoagulant which has received4the most attention, and it can be given intra-thecally in doses up to 30 mgm. daily in childrenwithout harm. Unfortunately, if the usual intra-thecal dose of o.I gm. of streptomycin is mixedwith heparin an insoluble precipitate forms whichcontains the heparin. The C.S.F. 24 hours afterthe injection of o.i gm. of streptomycin has onlyI6-32 units per ml., and if heparin is mixed withsuch fluid no deposit occurs. But 24 hours afteran adequate intrathecal dose of heparin, strepto-mycin added to the fluid still gives a precipitate,and it is necessary to wait for 48 hours before thetwo may be mixed safely. Thus, heparin is bestused when no intrathecal streptomycin is beinggiven, and if streptomycin is essential it cannot begiven intrathecally more often than every thirdday.
Without large series of cases and controls theUsefulness of such anticoagulants will be difficult toassess. Used prophylactically, there is no meansof knowing what effect on the prevention of fibrindeposition the anticoagulant will have, as pre-sumably some fibrin will be present before treat-ment starts, and some cases appear to resolve withno other treatment than streptomycin. Hydro-
cephalus developing while heparin was being givenwould suggest that the heparin was failing in itstask, but as by no means all cases develop hydro-cephalus even without heparin, its therapeuticvalue would be difficult to delimit. Little more canbe said at the present with regard to the variousanticoagulants which have been used than that theconception is sound and that they merit extendedtrial.
ConclusionThe prolongation of life and clinical improve-
ment which streptomycin is able to effect intuberculous meningitis are something quite new inthe history of the disease, but the long period ofboth treatment and subsequent observation whichwill be necessary to evaluate the drug must delayany final conclusions as to its efficacy. Increasingexperience is leading to increasing success, withalmost every case treated presenting its ownproblems and teaching its individual lessons.As the earlier the disease is treated the better
will be the result, every effort must be made toestablish the diagnosis as early as possible. Yetsuch encouraging results may be occasionally ob-tained even in comatose and apparently moribundchildren that almost any patient, however ill, isworth treating on the off chance that he mayrespond.A greater problem is how long treatment should
continue. The common practice is continuousintramuscular administration for an indefiniteperiod, with an initial daily intrathecal courselasting between two and four weeks. But.whilethe clinical pathology of streptomycin treatmenthas been well explored the ideal combination ofintramuscular and intrathecal administration is notyet finally decided, and probably it varies fromcase to case. It is not known if a constant in-hibitory streptomycin level in blood and C.S.F. ispreferable to a series of peak levels, although as faras the C.S.F. is concerned the relative inefficiencyof the constant C.S.F. level obtained by intra-muscular administration alone favours the latterview. And whether, after the first period ofintrathecal treatment, complete cessation of intra-thecal injection, or a rest period followed byanother and further daily courses, or single intra-thecal injections increasingly spaced is the bestregimen to follow, only experience will decide.
Constant watch must be maintained duringtreatment for signs of increasing intracranialpressure, which will necessitate other measures toprevent brain damage from hydrocephalus. Butthe development of hydrocephalus itself is noindication to stop treatment, as the most re-markable improvement, even to apparent nor-mality, is sometimes seen after the demonstration
July 1948 357
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

358 POST GRADUATE MEDICAL JOURNAL July 1948
of such a degree of hydrocephalus that there seemsto be scarcely aiy brain substance left.
In many cases of tuberculous meningitisstreptomycin seems to maintain the condition ofthe patient when treatment was commenced, butlittle subsequent improvement is seen. Such ex-periences support the case for the inclusion ofsome adjuvant antibacterial agent with thestreptomycin, in the hope that a synergistic actionsuch as is seen with sulphonamide and penicillinmight be found.
Finally, it must be realized that the strepto-mycin treatment of tuberculous meningitis cannotbe lightly undertaken. Apart from full laboratoryfacilities for controlling the clinical pathology of acase much extra nursing is required, continuous
medical supervision is necessary, and from thepatient's point of view there will be a course ofintramuscular injections lasting for six months ormore, apart from intrathecal and general support-ing treatment. Only the fullest and continuingco-operation of everybody concerned can givestreptomycin treatment the fair trial it deserves,and even in the most successful cases with ap-parent cure, prolonged subsequent observation isnecessary owing to the possibility of relapse.ADDENDUMThese observations were made at the Hospital
for Sick Children, which was one of the centrestaking part in the investigation by the MedicalResearch Council of streptomycin in tuberculosis.
NON-TUBERCULOUS MENINGITISBy GEORGE NEWNS, M.D., M.R.C.P.
Physician to the Hospital for Sick Children, Great Ormond Street
(1) PURULENT MENINGITISThe treatment of purulent meningitis has under-
gone a great change in the past ten years. Beforethe introduction of sulphonamide therapy, theprognosis in all but meningococcal meningitis wasvery bad and there were very few recoveries. Aradical transformation has been brought aboutby modern chemotherapy and even cases of in-fluenzal meningitis with early and thoroughtreatment, may now be expected to recover,although hitherto they were almost always fatal.Nevertheless many patients with purulent menin-gitis still die, due largely to failure to diagnose thedisease early enough and to inadequate treatment.
Diagnosis. The diagnosis of acute meningitis isnot difficult although in infants the onset may bemore insidious and typical meningeal signs absent.As a rule the onset is very acute, sudden high feverdeveloping in a previously healthy child; drowsinessis an early symptom. Pain in the neck muscles
especially on flexion soon appears and Kernig'sand Brudzinski's signs become positive.
If the child is untreated he becomes stuporosewith marked neck retraction and in severe casesopisthotonus may develop. Vomiting follows as aresult of rise in the intra-cranial pressure (ininfants under two years the sutures may separateand hydrocephalus may develop).
It is not easy to distinguish one form of puru-lent meningitis from another, but if purpura andsmall haemorrhagic spots appear, the infection isprobably due to the meningococcus. In infants,acute meningitis often does not present the typicalsyndrome outlined above. Neck stiffness may beabsent, and Kernig's sign is often negative.Irritability, drowsiness, photophobia, bulging ofthe fontanelle in a child with unexplained fever arevery suggestive of the onset of meningitis and alumbar puncture should be carried out withoutdelay.
DIFFERENTIAL DIAGNOSIS OF MENINGITIS
Polymorphs Mononuclears Sugar Chlorides Protein
Tuberculous Meningitis. .. + Decreased Very low +
Purulent Meningitis . ... + + + Absent Slightly decreased +
Virus Meningitis .. ... .. + Normal Normal +
Serous Meningitis .. .. + Normal Normal +
copyright. on A
ugust 21, 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.24.273.351 on 1 July 1948. D
ownloaded from

390 POST GRADUATE MEDICAL JOURNAL August I948
The following day was spent in Utrecht, a citywith an old university and an excellent medicalschool. Again we were delighted by the ver-satility of our host who was a general surgeon in itswidest sense, who could teach us much, yet wasever willing to listen. A delightful evening at ourhost's home in a fine old house, with the waterlapping against its walls, ended a memorable day.To conclude our visit we drove out to the greatdyke which makes the Zuyder Zee a fresh watersea by shutting it off from the ocean. The scenery,utterly flat and not even relieved by a windmill,soon lost its novelty and one could well imaginethat in time it would engender agerophobia in thestaunchest. There were depressing signs ofGerman wantonness in the skeletons of woodenhouses made uninhabitable by flooding. Thedykes were destroyed as they retreated in 1945,not long before the surrender. However theDutchman has not earned his reputation forstubbornness without cause and already a mostambitious rebuilding programme is well on theway to completion.The Dutch, even as ourselves, seem to take the
problem of recovery after the war very seriously,and in fact in some ways have been more successfulthan us. We have much in common and it is hopedthat the exchange of medical knowledge and ofdoctors in the future will be even greater than inthe past. e
Aid for the DeafIt is gratifying to learn that a committee has
been set up to consider the three aspects of therapyfor the deaf. Medical, surgical and instrumental.The greatest advances in these three aspects hasbeen made in the surgical treatment of otosclerosisand in the construction of the present-day crystalmicrophone, with miniature valve amplifier,hearing aid.
The surgical approach is, of course, to be under-taken only by those taking the trouble to perfectthe difficult technique, and the operation has nodoubt come to stay, for its place in the treatmentof otosclerosis is now proven without any doubt.
Although advances have been made in thesethree branches of therapy for the deaf, there stillremains to be formed in this country, clinics setapart entirely for the treatment of the deaf, frominfancy to old age. Thus within the one clinicthere should be facilities for speech therapy, lipreading, hearing aid selection and maintenance,surgical treatment for those suitable for the opera-tion, medical treatment for those who require itand finally and perhaps most important of all,facilities for further research in one or all of thesethree branches. Such clinics, I believe, are inexistence in the Western Hemisphere but not inEurope.
E.R.G.P.
Paediatric NumberThe July issue of the Journal was devoted to Paediatrics, but owing to the shortage of paper itwas impossible to print all the articles. This month Dr. J. L. Henderson's paper on ' Infectionin the Newvborn Infant' has therefore been included in addition to the published contents.
CorrectionIn the article by Dr. I. A. B. Cathie on' The Streptomycin Treatment of Tuberculous Meningitis 'appearing in last month's issue of the Journal a typographical error occurs beneath a number ofillustrations. In Figures I and II, 0.2 gm. per lb. of body weight should read: 0.02 gm. per lb. ofbody weight. In Figures III and V, o.i gm. per lb. of body weight should read: o.oi gm. per lb.of body weight. We apologise for this error and hope that it has not proved misleading.