stromal overgrowth in a brenner tumor or ovarian fibroma ... · 368 cancer control july 2015, vol....
TRANSCRIPT

366 Cancer Control July 2015, Vol. 22, No. 3
Summary: Computed tomography obtained as part of a urinary tract assessment in a 68-year-old woman incidentally detected a solid adnexal mass. Bilateral salpingo-oophorectomy revealed a unilateral, 4-cm, white to tan-yellow colored, focally calcified, left ovarian mass. Microscopically, the tumor was com-posed of bland fibroblasts, abundant collagen, and areas of calcification with a minor component com-posed of nests of epithelial cells with nuclear clefts focally evident, some of which contained central lu-mens with eosinophilic secretions. The major consid-erations were fibromatous overgrowth in a Brenner tumor or ovarian fibroma with minor sex cord ele-ments. Immunostains for cytokeratin 7 showed dif-fuse positivity in the epithelial nests, whereas cy-tokeratin 20 and inhibin were negative, further supporting the diagnosis of a Brenner tumor.
BackgroundMost ovarian neoplasms are surface epithelial tumors, 2% to 3% of which represent Brenner tumors.1 Inci-dental Brenner tumors are not uncommon in oopho-rectomy specimens, and the true incidence of these lesions may be higher than estimated. The clinical significance, if any, of incidental Brenner tumor is unknown. Because of the common presence of mu-cinous epithelium lining the central space in Brenner nests, a variety of mucinous tumors may arise with-in a Brenner tumor. Brenner tumors also commonly occur in association with other ovarian tumors, in-cluding serous adenofibroma and mature cystic tera-tomas.2 Sex cord–stromal tumors represent approxi-mately 6% to 8% of ovarian neoplasms, with fibromas accounting for the majority.3 A small portion of fibro-mas have minor sex cord elements.
Case ReportA 68-year-old white, gravida 4, para 4, postmeno-
pausal woman was referred for computed tomogra-phy as part of a urinary tract assessment. The imaging study incidentally revealed an adnexal mass with calci-fications. Ultrasonography was obtained and showed a 3.3 × 2.4 cm left adnexal mass with no blood flow, which was suspicious for a possible dermoid cyst. Sub-sequently, magnetic resonance imaging demonstrated a 3 × 2.6 × 2.2 cm mass in the left ovary with a homo-geneous, low T2 signal and very minimal enhance-ment following the administration of gadolinium, a finding suspicious for ovarian fibroma (Fig 1A). Her level of cancer antigen 125 was normal (3.1; nor-mal < 35 U/mL). Given the suspected benign nature of the ovarian mass, surgery limited to bilateral salpin-go-oophorectomy was performed.
Grossly, the left ovary was firm with a smooth and glistening external surface. The ovary was sec-tioned to reveal a 4-cm solid mass with a tan-yel-low to white-colored, focally calcified, cut surface (Fig 1B). The lesion replaced nearly the entire left ovary measuring 4.5 × 2.8 × 2.2 cm. Microscopical-ly, the lesion had well-circumscribed borders. It was predominantly composed of fibrous stroma with bland spindle cells and collagen with large areas of calcification distributed in the abundant stromal collagen (Fig 2A and B). Admixed with the fibrous stroma and calcifications were multiple small epi-thelial nests comprising 10% to 15% of the entire le-sion, some of which had central lumens filled with eosinophilic secretions (Fig 2C). Although the epithe-lial nests made up a minor component of the lesion, they were scattered throughout multiple sections and were found in close proximity of the calcifications under high-power examination. The epithelial cells were relatively uniform in size with scant cytoplasm and nuclei with occasional longitudinal grooves. No related mucinous epithelium was identified.
The epithelial nests showed strong and diffuse im-munoreactivity with cytokeratin (CK) 7 (Fig 2D) but were negative for CK20 and inhibin. The contralateral ovary measuring 2.8 × 2.4 × 1.8 cm revealed cortical in-clusion cysts. The fallopian tubes demonstrated para-tubal cysts with no additional pathological findings.
DiscussionThe pathological findings in this case supported the
Case Report
Stromal Overgrowth in a Brenner Tumor or Ovarian Fibroma With Minor Sex Cord Elements? Julia A. Ross, MD, PhD, and Ozlen Saglam, MD
From the Department of Pathology, Yale University School of Medi-cine (JAR), New Haven, Connecticut, and H. Lee Moffitt Cancer Center & Research Institute (OS), Tampa, Florida.
Address correspondence to Ozlen Saglam, MD, Department of Pa-thology, Moffitt Cancer Center, 12902 Magnolia Drive, Tampa, FL 33612. E-mail: [email protected].
No significant relationships exist between the authors and the companies/organizations whose products or services may be ref-erenced in this article.

July 2015, Vol. 22, No. 3 Cancer Control 367
cystic lesions.5 The cytological features of borderline or low-malignant potential Brenner tumors can be similar to that of benign Brenner tumors; however, their archi-tectural features are more complex, forming papillae or polypoid structures.6
Approximately 50% of Brenner tumors are associ-ated with calcifications and fibromas may show dense calcifications as well.3,7,8 The distinction between a Brenner tumor with fibrous stroma and ovarian fibro-ma may seem to be an academic exercise, particularly because both entities are benign; however, despite the benignity of both lesions, the characterization can be important because multiple reports of tumors metasta-sizing to ovarian lesions such as Brenner tumor — and, to a lesser extent, fibroma — have been described.9-12 These examples include renal cell carcinoma metas-tasizing to mixed Brenner tumor with mucinous cyst-adenoma,9 squamous cell carcinoma of the cervix me-tastasizing to Brenner tumor,10 breast cystosarcoma phyllodes to Brenner tumor,11 and breast adenocarci-noma metastasizing to benign ovarian fibroma.12
ConclusionsImaging, microscopic, and immunohistochemical fea-tures of a Brenner tumor with abundant fibrous stro-mal overgrowth were presented. The rare entity of fibroma with minor sex cord elements was excluded by morphological and immunophenotypical features. Ovarian fibroma with an incidental Brenner tumor component may also be considered in the differential diagnosis. By contrast to the localized nature of the epithelial component in a Brenner tumor with fibrous stroma, the presence of relatively scattered epithelial elements is an atypical finding in this case. Brenner tumors can occur with other ovarian neoplasms; how-ever, a description of Brenner tumor coexisting with ovarian fibroma has, to our knowledge, never been de-
clinical and radiological findings of a benign ovarian neoplasm. The gross examination was characteristic of an ovarian fibroma with a solid, firm, cut surface. The presence of focal microscopic epithelial nests within the fibrous stroma suggested the differential diagno-sis of ovarian fibroma with minor sex cord elements, a rare entity described by Young and Scully in 1983.4 By definition, the sex cord elements represent less than 10% of the lesion and are composed of granulosa cells, Sertoli cells, or indifferent cells of a sex cord–like type. Our case was predominantly a fibrous tumor with a small component of transitional-type epithelial islands (10%–15%) distributed within fibrous stroma. By con-trast to typical sex cord elements, the epithelial nests in this case had cystic lumina with eosinophilic secre-tions. In addition, the presence of nuclear grooves was an indication of a transitional-type epithelium. These entities can be further distinguished with immunohis-tochemistry, because sex cord–stromal elements stain positively with inhibin and Brenner tumors stain with CK7. In our case, the epithelial groups showed CK7 positivity and inhibin negativity, supporting the find-ings on hematoxylin and eosin staining.
Given the patient’s presentation, which included urinary tract complaints, the possibility of metastatic urothelial carcinoma was considered, but the nests of transitional cells lacked significant proliferation, atyp-ia, or mitotic activity. In general, metastatic tumors of the ovary present as multiple bilateral lesions, which is in contrast to the unilateral presentation of this le-sion. Furthermore, urothelial carcinomas coexpress CK7 and CK20. The latter marker was negative in the epithelial nests.
The distinction can be more challenging in a case of borderline or malignant Brenner tumor, or a transi-tional variant of high-grade serous carcinoma, as any and all of these may and, not infrequently, present as
Fig 1A–B. — (A) Magnetic resonance imaging of the left ovarian mass that showed homogeneous, low T2 signal and minimal enhancement after the administration of gadolinium. (B) Gross pathology showing the cut surface of the 4-cm ovarian mass.
A B
22.49 mm
368 Cancer Control July 2015, Vol. 22, No. 3
tailed. Although this may be the scenario in the case presented, the diagnosis of Brenner tumor is favored in the presence of a single gross nodular lesion. Despite the benign nature of both lesions, an awareness of the potential for tumors to metastasize to these lesions should be noted.
The authors would like to thank Fattaneh A. Tavas-soli, MD, for her careful review of the manuscript and helpful comments.
References 1. Longacre TA, Gilks CB. Surface epithelial-stromal tumors of the ovary. In: Nucci MR, Oliva E, Goldbum JR, eds. Gynecologic Pathology. London: Churchill Livingstone Elsevier; 2009:393-444. 2. Waxman M. Pure and mixed Brenner tumors of the ovary: clinico-pathologic and histogenetic observations. Cancer. 1979;43(5):1830-1839. 3. Young RH. In: Ronnett BM, Kurman RJ, Ellenson LH, eds. Blaus-tein’s Pathology of the Female Genital Tract. 6th ed. New York: Springer; 2011:905-966.
4. Young RH, Scully RE. Ovarian stromal tumors with minor sex cord elements: a report of seven cases. Int J Gynecol Pathol. 1983;2(3): 227-234. 5. Ulbright TM, Roth LM, Stehman FB. Secondary ovarian neoplasia. A clinicopathologic study of 35 cases. Cancer. 1984;53(5):1164-1174. 6. Roth LM, Gersell DJ, Ulbright TM. Ovarian Brenner tumors and transitional cell carcinoma: recent developments. Int J Gynecol Pathol. 1993;12(2):128-133. 7. Green GE, Mortele KJ, Glickman JN, et al. Brenner tumors of the ovary: sonographic and computed tomographic imaging features. J Ultra-sound Med. 2006;25(10):1245-1251. 8. Jung SE, Lee JM, Rha SE, et al. CT and MR imaging of ovar-ian tumors with emphasis on differential diagnosis. Radiographics. 2002;22(6):1305-1325. 9. Ibrahim A, Al-Jafari MS. Metastatic renal cell carcinoma in an ovar-ian benign mixed mucinous cystadenoma and brenner tumour: a case re-port. Case Rep Pathol. 2012;2012:523231. 10. Johnson TL, Keohane ME, Danzey TJ, et al. Squamous cell carci-noma of the cervix metastatic to an ovarian Brenner tumor. Mod Pathol. 1995;8(3):307-311. 11. Hines JR, Gordon RT, Widger C, et al. Cystosarcoma phyllodes metastatic to a brenner tumor of the ovary. Arch Surg. 1976;111I(3): 299-300. 12. Perry LJ, Lewis CJ, Ball RY. Adenocarcinoma of the breast meta-static to benign ovarian fibroma. Gynecol Oncol. 1996;62(3):408-410.
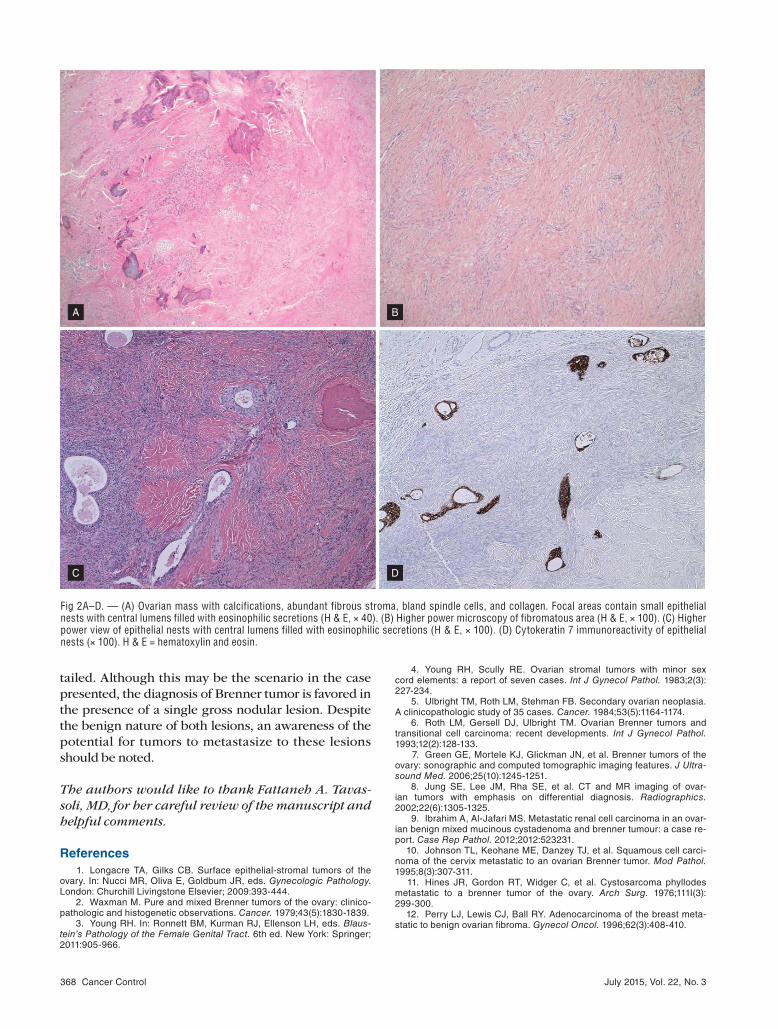
Fig 2A–D. — (A) Ovarian mass with calcifications, abundant fibrous stroma, bland spindle cells, and collagen. Focal areas contain small epithelial nests with central lumens filled with eosinophilic secretions (H & E, × 40). (B) Higher power microscopy of fibromatous area (H & E, × 100). (C) Higher power view of epithelial nests with central lumens filled with eosinophilic secretions (H & E, × 100). (D) Cytokeratin 7 immunoreactivity of epithelial nests (× 100). H & E = hematoxylin and eosin.
A B
C D