structuring value-based contracts: key considerations and
TRANSCRIPT

Structuring Value-Based Contracts: Key
Considerations and Provisions, Risk Mitigation,
and Implementation
Today’s faculty features:
1pm Eastern | 12pm Central | 11am Mountain | 10am Pacific
The audio portion of the conference may be accessed via the telephone or by using your computer's
speakers. Please refer to the instructions emailed to registrants for additional information. If you
have any questions, please contact Customer Service at 1-800-926-7926 ext. 1.
WEDNESDAY, MAY 19, 2021
Presenting a live 90-minute webinar with interactive Q&A
Julian D. Bobbitt, Jr., Attorney, Smith Anderson Blount Dorsett Mitchell & Jernigan, LLP,
Raleigh, N.C.
Lori A. Oliver, Shareholder, Polsinelli, LLP, Seattle
Tips for Optimal Quality
Sound Quality
If you are listening via your computer speakers, please note that the quality
of your sound will vary depending on the speed and quality of your internet
connection.
If the sound quality is not satisfactory, you may listen via the phone: dial
1-877-447-0294 and enter your Conference ID and PIN when prompted.
Otherwise, please send us a chat or e-mail [email protected] immediately
so we can address the problem.
If you dialed in and have any difficulties during the call, press *0 for assistance.
Viewing Quality
To maximize your screen, press the ‘Full Screen’ symbol located on the bottom
right of the slides. To exit full screen, press the Esc button.
FOR LIVE EVENT ONLY

Continuing Education Credits
In order for us to process your continuing education credit, you must confirm your
participation in this webinar by completing and submitting the Attendance
Affirmation/Evaluation after the webinar.
A link to the Attendance Affirmation/Evaluation will be in the thank you email
that you will receive immediately following the program.
For additional information about continuing education, call us at 1-800-926-7926
ext. 2.
FOR LIVE EVENT ONLY
Program Materials
If you have not printed the conference materials for this program, please
complete the following steps:
• Click on the link to the PDF of the slides for today’s program, which is located
to the right of the slides, just above the Q&A box.
• The PDF will open a separate tab/window. Print the slides by clicking on the
printer icon.
FOR LIVE EVENT ONLY
Julian D. “Bo” Bobbitt, Jr.Smith Anderson Blount Dorsett Mitchell & Jernigan, LLP
Lori OliverShareholderPolsinelli, PC
May 19th, 2021
Value-Based Care Contracting

What we’ll discuss today
Key considerations on whether to enter
VBC contracts
Setting the stage for value-based
care (VBC)
Risk mitigation and key provisions
Best practices
2

Setting the Stage for VBC
I. The Triple Aim: a framework for Value-Based Care (VBC)
2007 | Framework developed by researchers at the Institute for Healthcare Improvement
- Better care for individuals
- Better health for populations
- Lower per capital costs
2010 | Adopted as part of the national healthcare strategy and through the Patient Protection and Affordable Care Act (“ACA”)
Ongoing | Evolution to “Quadruple Aim” to include the work life of clinicians/staff and addressing the widespread prevalence of burnout and work-related stress
4
Why?
The state of healthcare in the United States is . . .
- National health spending is projected to grow at an average annual rate of 5.4% for 2019-28 and to reach $6.2 trillion by 2028.
- Failing to deliver on healthcare equity
- Continued growth in cost of care
- Decreased access to core healthcare services
- Social determinants of health
The competence needed to succeed in VBC models served providers well during the public health emergency
5

Trends: ongoing acceleration of adoption of value-based payment models
Proven cost savings in Medicare
- The Medicare Shared Savings Program served 11.2 million seniors in 2019 and saved $2.6 billion last year for Medicare [National Association of ACOs]
- See CMS Innovation Center for examples of Medicare Advance Payment Models at https://innovation.cms.gov/
Medicaid
- Adoption of various models (e.g., patient-centered medical home, health home, shared savings, capitation, procurement changes)
- https://www.medicaid.gov/resources-for-states/innovation-accelerator-program/functional-areas/value-based-payment-financial-simulations/index.html
6

Trends: ongoing acceleration of adoption of value-based payment models
Medicare Advantage
- 42% of eligible Medicare beneficiaries
Broad commercial payer adoption
- United Health Care tripled over 3 years - $75B of spend in CY 2020 or 1 in 3 enrollees
- Aetna – 74% spend in VBC models
- Innovative provider-payer partnerships
Self-insured employers increasingly engaged
- Centers of excellence or single service lines
- Complete provider network
- With or without a TPA
- Customized health benefit plans
- Fee for service + incentives
- Early intervention programs for chronic disease7
Market strategy
Informs collaboration model:
- Individual organizations
o Primary care or specialty groups
o Hospitals or post-acute care
- Networks of providers
o Accountable Care Organizations
o Clinically Integrated Networks
o Independent Physician Associations (IPA)
o Physician-Hospital Organization (PHO)
Depends on provider type
o Multi-specialty provider
o Primary care
o Hospital
o Post-Acute Care
o Behavioral Health8
Readiness
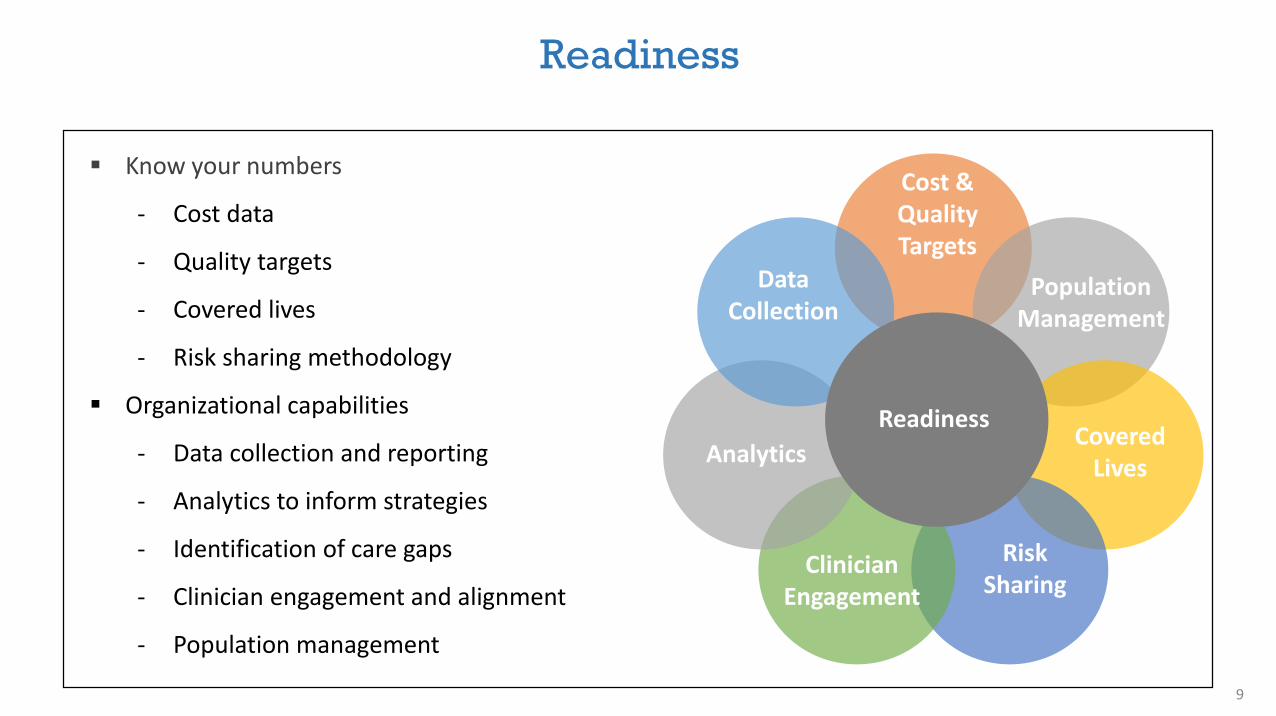
Cost & Quality Targets
Data Collection
Covered Lives
Population Management
Risk Sharing
Clinician Engagement
Analytics
Readiness
Know your numbers
- Cost data
- Quality targets
- Covered lives
- Risk sharing methodology
Organizational capabilities
- Data collection and reporting
- Analytics to inform strategies
- Identification of care gaps
- Clinician engagement and alignment
- Population management
9
Key Considerations for Whether to Engage In VBC Contracts
II. Considerations when determining whether to enter in VBC contracts: Introduction
A. INTRODUCTION
“Accountable” in “Accountable Care Organization” really means something.
A Word about Words – “CIN” vs. “ACO”
Value-Based Care (“VBC”) contracts we will (and won’t) cover.
11
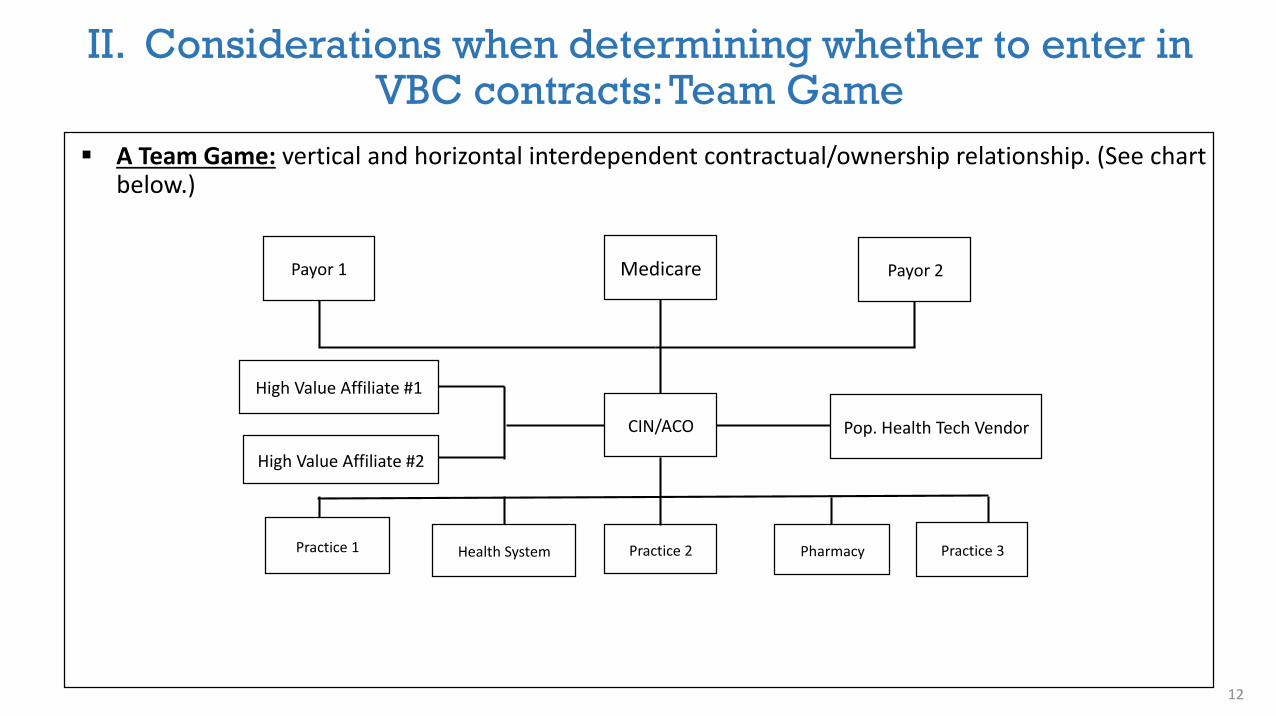
A Team Game: vertical and horizontal interdependent contractual/ownership relationship. (See chart below.)
MedicarePayor 1 Payor 2
CIN/ACO
High Value Affiliate #1
High Value Affiliate #2
Pop. Health Tech Vendor
Practice 2 PharmacyHealth SystemPractice 1 Practice 3
II. Considerations when determining whether to enter in VBC contracts: Team Game
12

B. BEFORE YOU START NEGOTIATING TERMS, SHOULD YOUR CLIENT EVEN ENTER INTO A PARTICULAR VBC CONTRACT?
II. Considerations when determining whether to enter in VBC contracts: why should you?
13
1. Why your client should enter into a VBC contract.
Existential Necessity – Documented value, Biden Administration, telehealth proven during pandemic—all hastening trend for VBC to dominate delivery and payment.
Grow Market Share – Referrals, narrow networks.
Access Technology
Empowerment – Deliver health care the right way; design care protocols for your patients.
2. Why your client should not enter into a VBC contract.
Fate dependent on other providers
Fate dependent on patient engagement
Uncertainty of future of VBC
Start-up costs
Risk of medical loss
Legal compliance complexities
“I just want to see patients” – Big cultural shift

C. CIN AND ACO AGREEMENTS
Due Diligence Crucial – Joining a CIN or ACO is commonly through “Participation Agreements.” They address many essential terms, but often the real “deal killers” are not in the contract.
The Top 10 Key Due Diligence Questions to Ask:
II. Considerations when determining whether to enter in VBC contracts: CIN / ACO agreements
14
1. What is your shared savings (or other performance payment formula)? What is your track record?
2. What is your budget? Is it an adequate but lean budget? Does paying those expenses come before provider incentive payments?
3. Who owns the CIN? Are they committed to value?
4. Do you have a common, interoperable population health technology chassis?
5. Do you have clinically valid protocols that match the network’s capabilities, patient risks, and payor targets?

C. CIN AND ACO AGREEMENTS
Due Diligence Crucial – Joining a CIN or ACO is commonly through “Participation Agreements.” They address many essential terms, but often the real “deal killers” are not in the contract.
The Top 10 Key Due Diligence Questions to Ask:
15
1. What is your shared savings (or other performance payment formula)? What is your track record?
2. What is your budget? Is it an adequate but lean budget? Does paying those expenses come before provider incentive payments?
3. Who owns the CIN? Are they committed to value?
4. Do you have a common, interoperable population health technology chassis?
5. Do you have clinically valid protocols that match the network’s capabilities, patient risks, and payor targets?
6. Is the culture there? (Look for meaningful physician input on value initiatives, budget, and merit-based performance distribution policies that incentivize with performance.)
7. What are your social determinants of health and community health resources strategies?
8. Do you have a viable mix of providers? (At least 1/3 primary care.)
9. Do you have mechanisms to assure active adherence to protocols?
10. What is your telehealth strategy?
II. Considerations when determining whether to enter in VBC contracts: CIN / ACO agreements
Key CIN/ACO Contract Provisions:
1. Culture Related – MD roles in clinical performance payment distribution and governance. NOTE: Beware of incorporation by reference traps, especially to CIN/ACO LLC Operating Agreement.
2. Take-All-Payors Clauses – Is this de facto exclusive way too contract with payors? Fee-for-service too?
3. Absence of performance payment distribution policy.
4. Referrals and choice of site guided by value criteria, not ownership of CIN/ACO.
5. How are decisions regarding contract protocols and compensation communicated? Opportunity for Board or key committee roles?
6. Legal compliance safeguards.16
II. Considerations when determining whether to enter in VBC contracts: CIN / ACO agreements
Key CIN/ACO Contract Provisions (continued):
7. Meaningful expectations of providers and facilities.
8. Performance monitoring and corrective action plan.
9. Early termination “poison pill?”
II. Considerations when determining whether to enter in VBC contracts: CIN / ACO agreements
17

Sample CIN/ACO Agreement Terms with Negotiation Strategies
Made possible by a grant from the Physician’s Foundation and by one of the conditions of the grant, is freely downloadable at https://www.ncmedsoc.org/wp-content/uploads/2019/02/ACO-and-CIN-contracting-guide_2018.pdf.
II. Considerations when determining whether to enter in VBC contracts: extra resources
18

II. VBC Agreements with payors: initial assessment
D. VBC PAYOR AGREEMENTS
19
Is the Payor Ready?
1. Many still have clunky one-size-fits-all programs, poor and untimely data analytics and feedback, and metrics not matched to care and savings goals of the VBC contract.
2. Does it have vestigial us vs. them thinking and negotiation habits as opposed to win/win alignment of incentives? [TIP: Medicare Advantage is exception and thus worthy of prioritized attention.]
3. Do you have enough of their lives in client’s system?
4. Does this VBC approach align with client’s mission?
Is the Provider Organization Ready?
1. Does it have requisite infrastructure, culture, bandwidth, and leadership?
2. Do the payor’s VBC performance requirements, metrics, territory, and patient population fit your strengths?

Negotiation Questions to Ask Before Parsing Contract Language.
1. Who is in the payor’s network if contract includes others than client’s own network?
2. What is the expected patient census? How will they be attributed? Proactive or retroactive?
3. What is history of control, accuracy, timeliness, and transparency of data? In contrast to fee-for-service arrangements, access to such data is critical.
4. Will this be episode-based (i.e., bundled payment) or population based (i.e., shared savings)? Many VBC considerations apply to both, but important contract distinctions regarding carve-outs, scope, metrics, payments, etc.
II. VBC Agreements with payors: negotiation questions
20

BASIC EHR ACO IT INFRASTRUCTUREHIE
Scope of Information Sharing
Functional Complexity
Patient health information available at point of care
Reporting capabilities to state and federal agencies
Data mining capabilities to contribute to financial impact modeling, value reporting, and payor negotiations
Decision support capabilities at point of care
Expanded access to patient records across the continuum
Comparative data collection to determine gaps in care delivery processes and outcomes vs. peers
21
II. VBC Agreements with payors: information infrastructure needs
Reporting capabilities to state and federal agencies
Patient health information available at point of care
Patient health information available at point of care

II. VBC Agreements with payors: MA considerations
22
Medicare Advantage Agreement Considerations
1. Fastest growing VBC area, with strong payor/provider incentive alignment and program design flexibility-giving improved prospects of collaborative, innovative, and tailored VBC contracts. Managed care organization will assess and try to improve provider readiness, which is a logical prerequisite for either to consider more advanced value-based payment alternatives.
2. Match risk profile to patient gap analysis-utilization, costs when setting total cost of care targets or per-member/per-month payments.
3. Accurate coding and documentation is crucial. Include social determinant of health and contributing factors beyond medical conditions. Payor payment amounts affected by this coding and passed on to you.
4. Optimize Star Ratings. Four or five stars will result in significant bonuses for payor and providers. Lower ratings may limit ability to obtain MA contracts in the future.

Risk Mitigation and Key Provisions
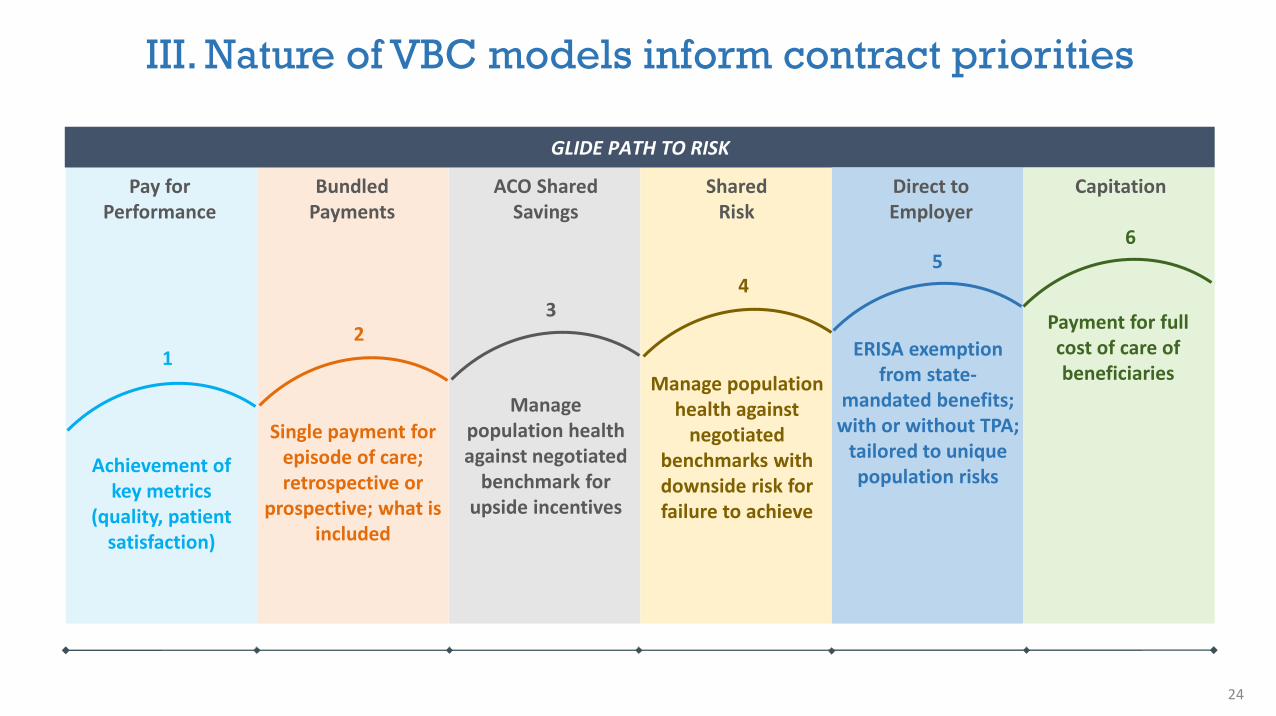
III. Nature of VBC models inform contract priorities
Achievement of key metrics
(quality, patient satisfaction)
Single payment for episode of care; retrospective or
prospective; what is included
Manage population health against negotiated
benchmark for upside incentives
GLIDE PATH TO RISK
Manage population health against
negotiated benchmarks with downside risk for failure to achieve
4
ERISA exemption from state-
mandated benefits; with or without TPA;
tailored to unique population risks
Payment for full cost of care of beneficiaries
12
3
56
Pay for Performance
Bundled Payments
ACO Shared Savings
Shared Risk
Direct to Employer
Capitation
24

III. VBC agreements with payors
Key Payor VBC Contract Terms Considerations
1. Covered Services – Review of definitions key. May include more third-party administrator, fee-for-service, and affiliated payors and products than expected.
2. Data and Reporting – What are the tools? Interoperable? Timely, patient census, gaps, dashboards, metrics, etc. [TIP: Important negotiation area to spell out. Otherwise, successful efforts crippled by poor payor data.]
3. Patient Attribution – Important to pin down.
4. Payment Terms – Are there financial guarantees? Risk? When is payment made?
25

Key Payor VBC Contract Terms Considerations (continued)
5. Compliance – With laws and regulations rapidly changing in VBC, these terms need to anticipate need for adaptation.
6. Performance Measures and Benchmarks – Need to match incentivized behavior, capabilities of provider network, clinically-valid achievable. What phase-in of performance sought? Is there risk adjustment?
7. Term – For unproven relationship, no-cause exit hedge important. Beware of penalties for early termination.
8. Risk Allocation (i.e., Insurance, Indemnification, Force Majeure) – Need to be reasonable and mutual. Sovereign and governmental immunity objective limit ability of health departments and counties to accept such restraints. Cyber insurance and stop-loss policies are often required but may be extraordinarily expensive.
26
III. VBC agreements with payors
5
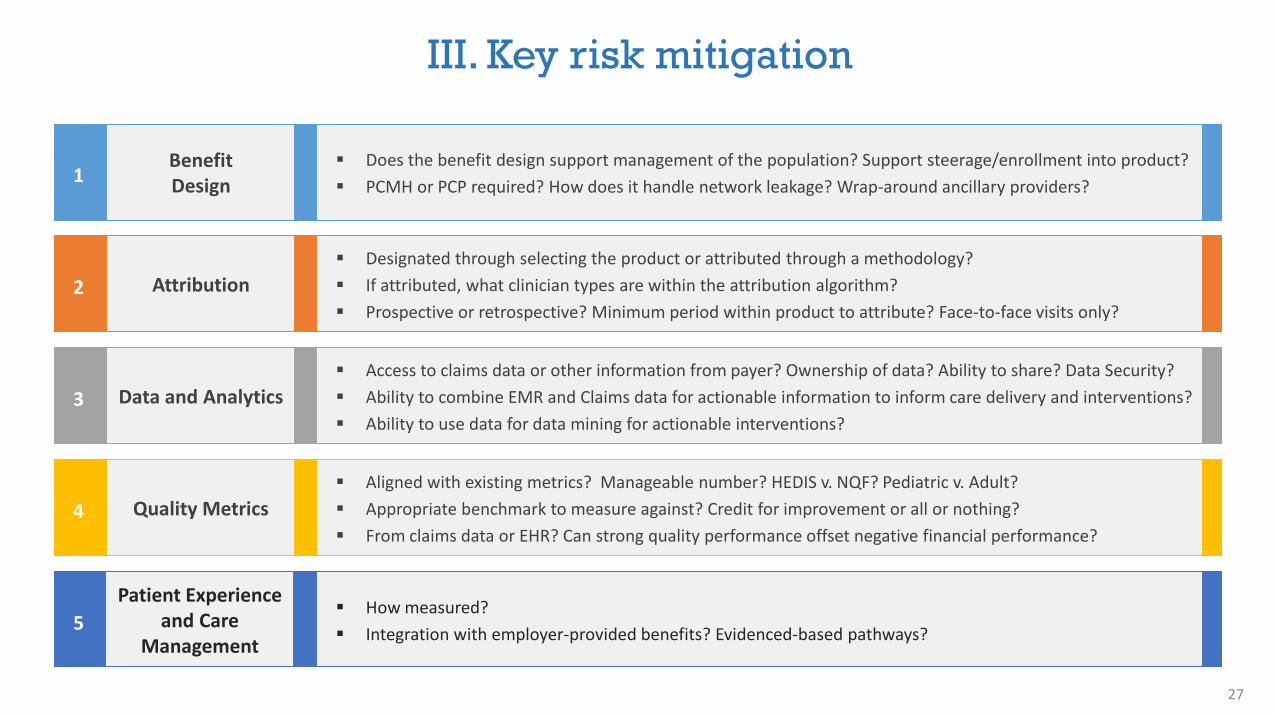
III. Key risk mitigation
1Benefit Design
Does the benefit design support management of the population? Support steerage/enrollment into product?
PCMH or PCP required? How does it handle network leakage? Wrap-around ancillary providers?
2 Attribution
Designated through selecting the product or attributed through a methodology?
If attributed, what clinician types are within the attribution algorithm?
Prospective or retrospective? Minimum period within product to attribute? Face-to-face visits only?
3 Data and Analytics
Access to claims data or other information from payer? Ownership of data? Ability to share? Data Security?
Ability to combine EMR and Claims data for actionable information to inform care delivery and interventions?
Ability to use data for data mining for actionable interventions?
4 Quality Metrics
Aligned with existing metrics? Manageable number? HEDIS v. NQF? Pediatric v. Adult?
Appropriate benchmark to measure against? Credit for improvement or all or nothing?
From claims data or EHR? Can strong quality performance offset negative financial performance?
Patient Experience and Care
Management
How measured?
Integration with employer-provided benefits? Evidenced-based pathways?
27

10
III. Key risk mitigation
6 Bundles
What is within the episode of care?
Allocation of payment to different healthcare participants?
Access to records? Quality reporting? Access to data to audit?
7 Shared Savings
Methodology and risk model; PMPM; trend targets
Understand comparison data
Total cost of care inclusion/exclusion
8 Shared Risk
Symmetrical or asymmetrical sharing of risk? Transition to risk over time?
High-cost beneficiaries caps to shift risk back to payer; outliers
Cap on total financial risk or other method for dealing with material changes, unexpected events
9 Risk Adjustment
What risk score methodology? MARA? DxCG? Other?
How often is risk score calculated?
Examples in the contract very helpful to assuring understanding of methodology.
Financial Matters
Unique dispute resolution clause and right to audit data for financial reconciliation
Key definitions: Allowed amounts, base year, baseline cost PMPM, market benchmarks, attribution, shared
savings, minimum population size, trend guarantees, risk score etc.
28

III. Regulatory considerations: don’t forget
Depending on the VBC arrangement pay attention to regulatory guidance
- Antitrust - when working with those who are otherwise competitors and the role of clinical integration
- New value-based care exceptions within the Stark and Anti-Kickback statutes
- Unique requirements for certain plan types (e.g., HMOs or MA)
- Civil monetary penalties for inappropriate incentives to beneficiaries
- State insurance law and other state law considerations
- Data privacy and security
29

Best Practices

IV. Best practices: roles
Enhanced Role as Counselor
- Value-based contracting exposes your client to a significantly different set of opportunities and traps. Many of the client CFO, practice manager, or CMO’s honed skills at fee-for-service negotiation are actually negatives in VBC contracting. This will evolve in the future, but today, this presents opportunity for legal counsel to help point out the legal and transactional landmines.
31
Some Specific Best Practices
1. Timing is everything.
2. What can the client do best in VBC?
3. Anticipate that though this is existentially important, it is disruptive and not urgent; therefore, the classic recipe for avoidance.
4. Let Medicare pay for client’s VBC infrastructure—monthly payments for codes such as Chronic Care Management, Annual Wellness Visits, Remote Patient Monitoring, Behavioral Health Integration—can fund client’s VBC investments and be an “on ramp” for behavior change.
IV. Best practices: specifics
32

Some Specific Best Practices (continued)
5. You will have better luck negotiating with C-suite people at managed care company. Mid-levels often are not there yet. The exception is the provider rep for the Medicare Advantage agreements.
6. Remember the MACRA 5% bonus on all Medicare payments for some VBC arrangements with Medicare.
7. Single CIN/ACO chassis for all VBC contracts.
8. Remember, client can do great, but if others in network don’t, or patients don’t comply, it is all for naught.
IV. Best practices: specifics
33

THANK YOU!
QUESTIONS?
Julian D. “Bo” Bobbitt, Jr.Smith Anderson Blount Dorsett Mitchell & Jernigan, LLPPost Office Box 2611Raleigh, North Carolina [email protected]
Lori OliverShareholderPolsinelli, PC1000 2nd Avenue, Suite 3500 Seattle WA [email protected]
34