subject essential medications in emergency medicine · post intubation management (hemodynamics,...
TRANSCRIPT

RREESSIIDDEENNCCYY DDIIDDAACCTTIICCSS SSCCHHEEDDUULLEESS DDIIRREECCTTOORRYY OOPPEERRAATTIIOONNSS RREESSEEAARRCCHH SSIIMM MMEEDD SSTTUUDD UULLTTRRAASSOOUUNNDDAdvocate Christ Medical Center, Oak Lawn, Illinois
Essential Medications
InEmergency Medicine:
An Introductory Guide
Created by: Dr. Sudip Bose Edited by: Dr. Rolla Sweis
Formatted for the web by: Dr. Rohit Gupta
Last Updated: August 2008 This guide is intended for use in the Advocate Christ Medical Center Emergency Department. It is designed as a reference tool and not intended to be all-inclusive andnot meant to define the standard of care for the clinical practice of EM. Also, this guide should not replace clinical judgment. This guide is independent from and has no affiliation with pharmaceutical companies.
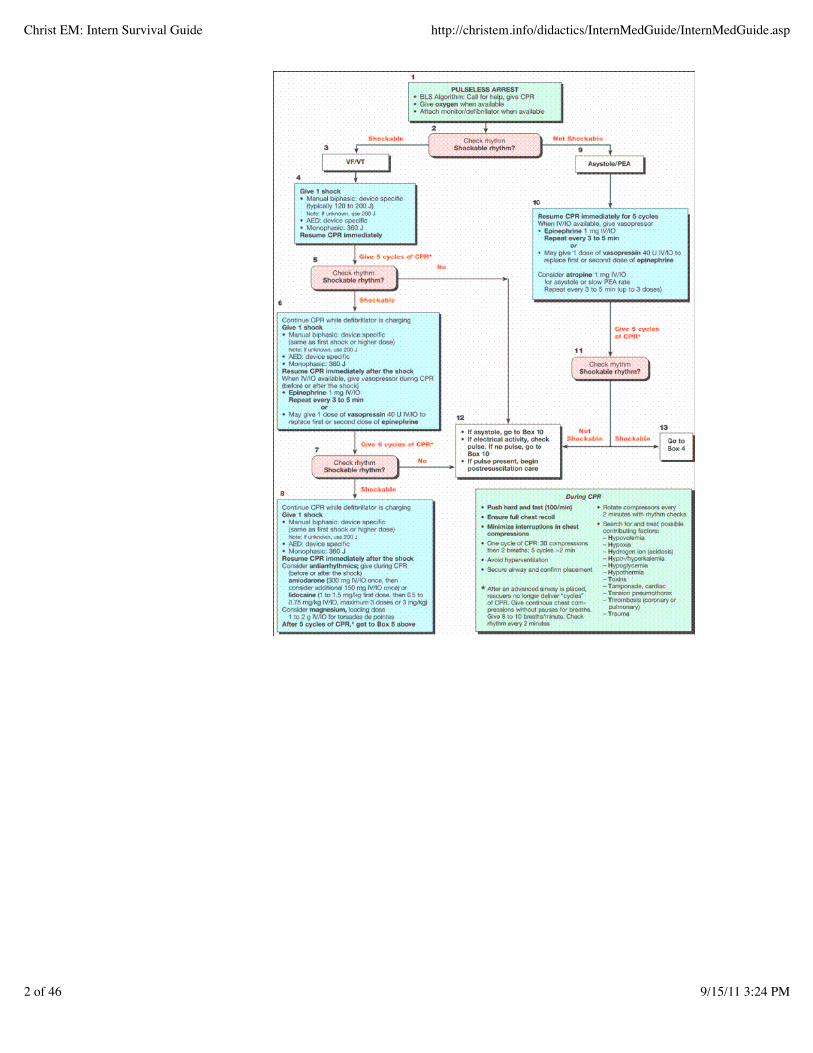
ACLS (Advanced Cardiac Life Support) Algorithms
CHRIST EM HOMEDIDACTICS HOME
SubjectACLS AlgorithmsAirwayAminoglycoside DosingAnaphylaxisAnalgesiaAntibioticsAntiemeticsAsthmaAtrial fibrillationCardiac arrestChest pain/ ACSCongestive Heart FailureContrast Load in RenalInsufficiencyCroupDiabetic KetoacidosisDONTElectrolyte ReplacementEndocarditisINR ElevationInsulin Sliding ScaleLocal anesthesiaMigraine TreatmentMRSA TreatmentPediatric Common MedsPEP: Non-OccupationalPEP: OccupationalPost LP HeadachesPreeclampsia/eclampsiaProcedural SedationRabiesRSV BronchiolitisSeizure – adultSepsisSTD’s and Genital InfectionsToxicologyToxicology – AntidotesNotes
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
1 of 46 9/15/11 3:24 PM
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
2 of 46 9/15/11 3:24 PM

Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
3 of 46 9/15/11 3:24 PM

Airway Preparation (monitors, laryngoscope/BVM, ETT/stylet/syringe, all medications, suction,
-IV, LEMON for difficult airway, rescue devices) -Look; Evaluate 3-3-2 rule; Mallampati; Obstruction evidence; Neck mobility Preoxygenation with 100% oxygen (NO positive pressure ventilation unless desat < 90%) -100% O2 for 5 minutes OR 2 to 6 Full Vital Capacity breaths of 100% O2 -Denitrogenizes alveoli and allows much longer time before desaturation occurs. Pretreatment (LOAD) -Lidocaine- for RAD or increased ICP -Opioid (fentanyl)- blunts sympathetic responses (ICP/CAD/ruptured aneurysm) -Atropine- 10 years old and under -Defasciculation- increased ICP, penetrating eye injuries Paralysis (and induction, which should be done first) Protection with Sellick’s Position for laryngoscopy Placement with Proof (capnography the gold standard)
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
4 of 46 9/15/11 3:24 PM

Post intubation management (hemodynamics, sedation and paralysis, vent settings)
Pretreatment-Lidocaine 1.5mg/kg-Opioid (fentanyl) 3mcg/kg-Atropine 0.02mg/kg-Defasciculating (pan/vec) 0.01mg/kg (10% of paralytic dose)
Induction-Etomidate 0.3mg/kg-Midazolam 0.3mg/kg-Ketamine 1-2mg/kg-Thiopental 3mg/kg
Paralytics-Succinylcholine 1.5-2.0mg/kg-Rocuronium 1mg/kg (0.6-1.2mg/kg)-Pancuronium/Vecuronium 0.15mg/kg
Sample sequences for 70kg adult:
GenericZero – 5 min: 100% oxygenZero: Etomidate 20-30mg Succinylcholine 100mg
Increased ICPZero – 5min 100% oxygenZero – 3min Lidocaine 100mg Vecuronium 1mg Fentanyl 200mcgZero Etomidate 20-30mg Succinylcholine 100mg
RAD/COPDZero – 5min 100% oxygenZero – 3min Lidocaine 100mgZero Ketamine 100mg Succinylcholine 100mg Post Intubation – Sedation Propofol
-Max dose 75mcg/kg/minute-Adverse effect – hypotension
Lorazepam
-2mg IVP q 30 minutes and start infusion at 1mg/hr. Increase infusion by 1mg/hr every 30 minutes. Consideralternate agent if > 20mg/hr is needed due to risk of metabolic acidosis.Consider if patient hypotensive on propofol.
Midazolam
-Loading Dose: 5mg IVP. Drip can be started at 2mg/hr. Increase infusion by 1mg/hr every 15 minutes and rebolusif needed. Max 25mg/hr-Avoid midazolam in renal failure-Consider if patient hypotensive on propofol
Fentanyl
-Loading Dose: 0.5-2mcg/kg (start low). Infusion: 25-100mcg/hr. Increase infusion by 25mcg/hr at 30 minuteintervals to a max of 150mcg/hr-Option for patients still hypotensive on benzodiazepines
Aminoglycoside Dosing this is FYI, you can also write “PharmD to dose” on the orders…)
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
5 of 46 9/15/11 3:24 PM

Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
6 of 46 9/15/11 3:24 PM

Anaphylaxis Benadryl 50mg IV (up to 100mg for severe reactions) (peds 1mg/kg) is H1 blocker Pepcid 20mg IV (peds 0.5 mg/kg) is H2 blocker Epinephrine 1:1000 0.01ml/kg to max 0.5ml (0.3ml peds) IM (normotensive) -Usual initial dose is 0.3ml IM
-Give 0.1 to 0.2ml of total dose at site of antigenic exposure-Recall that 1cc of 1:1000 epinephrine is 1mg
Epinephrine IV if hypotensive or respiratory failure - 0.3mg & if no improvementà -Continuous drip at 1mcg/min to 4mcg/min (peds 0.1mcg/kg/min to 1.5mcg/kg/min) Racemic epinephrine neb 0.5cc in 2.5ml NS to temporize airway management Albuterol and atrovent (continuous neb may be necessary) if pt wheezing Solu-medrol 125mg to 250mg (peds 1-2mg/kg IV) or Prednisone 60mg PO (peds 1mg/kg) -IV corticosteroids confer no greater benefit than PO
-Often ordered incorrectly: Solu-medrol is IM/IV. Prednisone is PO tablets. Prednisilone (Orapred,Pediapred, Prelone) is PO syrup for pediatric dosing
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
7 of 46 9/15/11 3:24 PM

Glucagon 1mg adults and 0.5mg peds w/ prn infusion 1 to 5 mg/hr -useful in refractory cases, especially in patients on beta-blockers
Analgesia (systemic) Acetaminophen (Tylenol) 650-1000mg PO q4h (peds: 15mg/kg q4h) -Mild to moderate pain, not an anti-inflammatory, few CI’s (liver disease) -Works best combined with an NSAID, opioid-sparing agent Ibuprofen (Motrin) 400-800mg PO q6-8h (peds: 10mg/kg q6-8h) -Mild to moderate pain, anti-inflammatory, opioid-sparing agent -More problems than Tylenol (GI upset, bleeding, renal damage) -Avoid in known renal disease, PUD, elderly Ketorolac (Toradol) 30mg IM or IV q6h (peds: 0.5mg/kg q6h) -The only FDA approved parenteral NSAID -More expensive and no more effective than PO NSAIDs -Avoid in elderly, renal disease and dehydration or loop diuretics (pre-renal) -No more than 5 days -Acute pain: 60mg IM unless < 65 years of age 30mg IV (max dose 120mg/24hrs) Morphine 0.1mg/kg IV or IM (may start with 4mg and titrate to effect) lasts 2-4hrs -May cause hypotension Fentanyl 0.5-2mcg/kg (may start with 50-100mcg and titrate to effect) lasts 30-45min -Beware chest wall rigidity -Avoid in children less than 4 months old -Short acting so good for abdominal pain of unknown etiology Hydromorphone (Dilaudid) 1-4 mg IM/SC/IV -There may be a particular role in sickle cell disease PO narcotic-analgesic combinations -Norco (hydrocodone/APAP 5-10/325) 1-2 tabs q4-6h prn -Percocet (oxycodone 5mg/APAP 325mg) 1-2 tabs q6h prn -Tylenol w/codeine (APAP 300mg/codeine 15mg #2, 30mg #3, 60mg #4) 1-2 tabs q4h -Elixir for peds has 12mg codeine and 120mg APAP per tsp
-T#3 shown in studies to be no more effective than APAP alone -Darvon 65mg PO q4h prn
-Used by some for liver disease pts (contains no APAP) ALL narcotics may cause N/V. May give prophylactic antiemetics.
Antibiotics Must know Christ Medical Center Protocols well (ie sepsis protocol antibiotic regimen; pneumonia protocol) Write for standing orders (ie. repeat doses q 6 hrs, etc) if patient will be signed out or be in the emergency roomfor several hours or make sure PharmD is aware to repeat further dosing. Do NOT use in pregnancy:
Erythromycin estolate, lindane (Kwell), Flagyl (safe for use in 2nd and 3rd trimesters), Macrodantin(contraindicated in 3rd trimester), quinolones, sulfonamides (safe in 1st and 2nd trimesters, avoid in 3rd
trimester due to possible kernicterus), tetracycline, doxycycline, Bactrim/Septra (kernicterus in 3rd
trimester, category C in 1st and 2nd trimester due to interference with folic acid metabolism)
TYPE OF INFECTION FIRST LINE ALTERNATIVE NOTESAppendicitis Unasyn 1.5GM-3GM IV q6h or
Zosyn 3.375GM IV q6HCipro 400mg IV q12H +Flagyl 500mg IV q8HPEDS: Cefoxitin:25mg/kg/dose q 6 hours(give in consultation withsurgeon)
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
8 of 46 9/15/11 3:24 PM

Bites (outpatient tx)
Cat: Augmentin 875mg bid Dog: Augmentin 875mg bid Human: Augmentin 875mg bid
Ceftin 500mg q12h ORDoxy 100mg bid Clinda 300mg qid (peds10mg/kg q 6h) PLUS[(adults) Cipro 500mg POqd /(peds) Bactrim 5mlsusp/10kg (up to 20ml)/dose PO bid] Clinda 300mg qid (peds10mg/kg q 6h) PLUS[(adults) Cipro 500mg POqd /(peds) Bactrim 5mlsusp/10kg (up to 20ml)/dose PO bid]
-Duration: 3-5days prophylaxis(not needed if noinfection 48 hoursafter bite). 10-14days if infected-RememberRATS [Rabies,Antibiotics,Tetanusprophylaxis, Soap(irrigation)]-Give first dose inED
Bites (inpatient tx-- includescat/dog/human)
Unasyn 1.5g IV q6h OR Zosyn3.375g IV q 6h
Clinda 900mg IV q8hPLUS Cipro 400mg q12hOR Bactrim 5mg/kg IV q8h
Bowel perforation/Peritonitis
Unasyn 1.5g IV (3g if >80kg) q6hOR Zosyn 3.375g IV q6h
Cipro 400mg IV q12hPLUS Flagyl 500mg IVq6h
Breast Abscess Keflex OR Dicloxacillin 500mg qidx 10-14d for mild casesAncef 1g IV OR Nafcillin 2g IV ORVanco 15mg/kg IV (max 1g)
If MRSA Possible:TMP/SMX 2 DS PO bidor Vanco 1gm IV (ifMRSA)
I and D (probablyshould be done bysurgery)
Bronchitis (smoker or chronicbronchitis/COPD exacerbation)
(outpt)
Bactrim DS 1 tab bid OR Doxy100mg bid OR Biaxin 500mg BIDor Cefdinir (Omnicef)300mg BID
Bronchitis (acute episode innonsmoker or young smokerwithout chronic bronchitis:
No antibiotics. Usually viral. Treat symptomswith Albuterolinhaler.
Cellulitis
Keflex 500mg qid+/- Bactrim DS 2 tabs po BID (community MRSA)
Clinda 300-450mg PO tid Duration: until 3days afterinflammationdisappearsNote: increasedresistance seen withclinda forcommunity MRSA
Diabetic foot
Unasyn 1.5g IV (3g if >80kg) q 6hor Zosyn 3.375gm IV q6h if latestage
Clinda 600mg IV q 8hPLUS Cipro 400mg q12h
Cholecystitis/Cholangitis
Unasyn 3g IV q 6h OR Zosyn3.375g IV q 6h (give in consultationw/surgeon)
Cipro 400mg IV q 12hPLUS Flagyl 500mg IVq6h
Clostridium Difficile
MILD/MODERATE (WBC < 15, CR<1.5) Flagyl 500mg PO tid x10-14d SEVERE (WBC > 15, Cr>1.5):Vancomycin 125mg po QID X10-14 DAYS Complicated (perforation,megacolon): Vancomycin 500mgPO qid + Flagyl 500-750mg IVQ8H
-Contact isolation-D/c offendingantibiotic-Note POpreferred over IVfor flagyl. Vancoonly effective PO
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
9 of 46 9/15/11 3:24 PM

Conjunctivitis
Emycin/sulfacetamide/ophthalmicbacitracin (gtts q2hrs, ointment qid)x 7d
-Cipro 2 gtts q2h whileawake x 2d then q4h x 5d-Covers pseudomonas**Use forabrasions/conjunctivitisfrom contacts and organicmaterials
-Most cases areviral, but treat allin the ED as ifbacterial-Bacterial willresolve withoutabx, but resolvesquicker with abx-Avoid neomycinbecause causesallergic reactionsfrequently-Avoid gent/tobraas toxic to the eyeand add little tothe treatmentcoverage
Cystitis (<10yo)
-Amoxicillin 10mg/kg/dose tid x 10d-Augmentin 10mg/kg/dose tid x 10d
-Omnicef 14mg/kg/dayup to 600mg/day POdivided qd or bid for 10days
-In < 1yo there is noliterature to supportinitial parenteraldose of abx iftolerating PO-Some docs admitall febrile UTIs if <6mos old, others if< 3mos old (even ifnontoxic)
Cystitis (adult)
3 days of: Bactrim DS bid Levaquin 250mg qd ORCipro XR 500mg PO qdfor non-complicatedcystitis OR Cipro 250mgpo bid (some insuranceplans and Medicaid donot cover cipro XR)OR Nitrofurantoin 100mgBID x 5-7 daysOR Amoxicillin 500mgTID x 7 days
*FQ probablybest choice nowdue to highresistance toBactrim-10 days of:Bactrim DS,Levaquin,Ciprofloxacin,Augmentin, Keflexfor complicatedcystitis
Dental infections and intraorallacs
PCN 500mg qid x 10d Clindamycin 300mg qid
Diverticulitis
OutpatientAugmentin 875mg BID Inpatient:-Unasyn 1.5g IV (3g if >80kg) q6hOR Zosyn 3.375g IV q6h
Levaquin 750mg qd ORCipro 750mg PO bid]PLUS Flagyl 500mg qidx 7-10d - Cipro 400mg IV q12hPLUS Flagyl 500mg IVq6h
-May treat as anoutpatient ifnontoxic and cantolerate PO and noperf/abscess onCT
Epidydimitis/Orchitis/Prostatitis
- <35 yo (tx as GC/C): Should nowtreat the same as PID in a femaleRocephin 250mg IM PLUSDoxycycline 100mg PO bid x 10d - >35yo (coliforms): Bactrim DS 1tab bid
Levaquin 250mg qd x10-14d
Must treatprostatitis forlonger (14-28d)
Gastroenteritis (suspectedbacterial in adults)
Cipro 500mg bid x 3-5 days
Bactrim DS 1 tab bid x 5d Dysenterysymptoms, recenttravel to 3rd world(o/w probablyviral and no abxneeded)
Mastitis
Keflex 500mg qid OR Dicloxacillin500mg qid OR Clinda 300mg qid x10-14d
MRSA Possible: TMP-SMX DS 2 PO bidor Vanco 1gm IV q12h (if
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
10 of 46 9/15/11 3:24 PM

MRSA)
Meningitis
< 8 weeks: Claforan IV (100mg/kgq 8h) PLUS Ampicillin IV(50-100mg/kg q 6h +/- Vanc15mg/kg IV– pharmacy to doseafter first dose)-8wks to 18yrs: Rocephin IV(100mg/kg max 2g q12h) PLUSVancomycin IV (15mg/kg to max1.5g – pharmacy to dose after firstdose)-18yrs to 50yrs: Rocephin IV (2g q12h) PLUS Vanc IV (15mg/kg max1.5 g - pharmacy to dose after firstdose)- > 50yrs: Rocephin IV (2g q12h)PLUS Ampicillin IV (2g q4-6h)PLUS Vanc IV (15mg/kg max 1.5g- pharmacy to dose after first dose)
Rocephin IV (2g q12h) PLUS Vanc IV (15mg/kgmax 1.5g- pharmacy todose after first dose)
Dexamethasone0.15mg/kg q 6h(10 mg max) for2-4 days – giveprior to or at timeof initial abx toprevent bacteriallysis. Give forsuspectedpneumococcalmeningitis andcontinue only inproven cases
Neutropenic Fever with SepticShock
Imipenem/Cilastin IV (500mg q 8h -need creatinine clearance calculatedafter first dose) OR Cefipime IV (2gq8h) PLUS Vancomycin IV (15mg/kg IV max 1g - pharmacy todose after first dose)
Amikacin IV (20mg/kgmax 1.5g q 24h -pharmacy to dosesubsequent doses) PLUSAztreonam IV (2g q 8hPLUS Vancomycin IV(15mg/kg max 1g q 12h -pharmacy to dosesubsequent doses)
-If no shock or orno risk factors forGram + infectiondo not addVancomycin-Indwelling line =vanco
Open Frx
-Ancef (1-2g q 6-8h) -If severe: PLUS Gent 2mg/kg(pharmacy to dose subsequentdoses)
Vanc (15mg/kg max 1g –pharmacy to dosesubsequent doses) ORClinda (600mg q8h)
Osteomyelitis
Vancomycin (15mg/kg - max 1g IV– pharmacy to dose after first dose)PLUS Rocephin (50mg/kg - max 1gIV q24h)
Otitis externa Cortisporin Otic 4gtt qid OR Floxin5-10gtt bid x 10d-If refractory: Cipro HC 3gtt bid x7d OR Dicloxacillin 500mg PO qidx 7d
*Use suspension(not solution) ifTM perforation
Otitis media
Amoxicillin is first-line tx-Low-risk (> 2yrs old/no daycare/noabx for 2 months) gets 40mg/kg/dayx 5d-High-risk (<2 yrs old/daycare/abxin past 2 months) gets80-90mg/kg/day x 10d
Zithromax 10mg/kg onfirst day then 5mg/kg for4 days is first-line tx forPCN allergic Bactrim 1mL/kg/daydivided bid x 10dRocephin 50mg/kg IM x 1dose
Do NOT use foramoxicillinfailures
Otitis media (refractory)
Augmentin 80-90mg/kg/day dividedbid or tid x 10d is first-line tx
Ceftin 10mg/kg/dose bidx 10dRocephin 50mg/kg IM orIV qd for 3 days
One-time dose ofRocephin ONLYgood forNON-treatmentfailures
Pharyngitis
PCN 500mg bid x 10d for adults(15mg/kg/dose tid for children)
Z pack (Azithromycin)-Erythromycin 500mg bidx 10d (10mg/kg/doseqid)
Pharyngitis (refractory cases)
Augmentin 875mg bid x 10d(10mg/kg/dose tid)
Clindamycin 300mg qid x10d (5mg/kg/dose qid)
Pneumonia
- <6 months: Ampicillin 50mg/kg IVPLUS [Gent 2mg/kg ORCefotaxime 50mg/kg IV]-Patients < 6 months of age shouldbe admitted-6 months to 5yrs: Amoxicillin ORAugmentin 80-90mg/kg/day
-Pediazole 50mg/kg/daydivided tid-5 to 18yrs: Azithromycinx 5d OR E-mycin x10-14d
Use doxycyclineinstead oferythromycin if apatient has aprolonged QT.E-mycin not welltolerated.
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
11 of 46 9/15/11 3:24 PM

Pneumonia
Adult:-Outpatient: Z-pack OR E-mycin500mg OR Clarithromycin 500mgPO bid OR Levo 500mg OR Doxy100mg x 10d
Floor: Ceftriaxone IV (1 gm q 24h)+ Biaxin po (500 mg q 12h)OR: Ceftriaxone IV (1 gm q 24h) +Erythromycin IV (500 mg q6h [ifNPO] ICU: Ceftriaxone IV (1 gm q 24h) +Erythro IV (500 mg q 6h) NURSING HOME: Zosyn(piperacillin/tazobactam) IV (3.375gm q 6h) + Erythromycin IV (500mg q 6h)
- Avelox (moxifloxacin)IV (400 mg q 24h) [single antibiotic]-Macrolide allergy:Doxycyline IV/PO (100mg q 12 h) [for Biaxin orerythro]
Avelox (moxifloxacin)IV (400 mg q 24h) Clindamycin IV (600 mgq 8h) + Cipro (400 mg q12h)
If pt isadmitted to theICU giveAztreonam 1gIV X 1 inaddition toAvelox
Pyelonephritis
Outpatient: Ciprofloxacin XR(extended release) 1000mg PO qdOR Cipro 500mg PO bid ORLevaquin 250mg qd OR Augmentin875mg bid x 14d -Pediatric Outpatient (FQcontraindicated): Omnicef 14mg/kgPO qd x 10 days (refer <2yo toPMD for imaging) -Inpatient: Same as Urosepsis -Urosepsis: Zosyn 3.375g IV q6hOR Gentamycin 7mg/kg IV x 1 (ifnot on dialysis), then pharmacy todose
Do NOT useBactrim forpyelonephritis(high resistance)
Sexual assault prophylaxis -STD (GC/C): Azithromycin 2g POalone-Trichomonas: Flagyl 2g PO-Pregnancy: Ovral 2 tabs now then2 in 12h OR Lo/Ovral 4 tabs nowthen 4 in 12h OR Plan B
1GM Azithromycin +Rocephin 125mg IM x 1
-Must have negativeurine hcg first (nopre-existingpregnancy)Phenergan 25mg POfor home (high-dosebirth control will causenausea) -Plan B available inomnicell
Sinusitis
-Sudafed 60mg PO q 4-6h-Afrin 2-3 drops/sprays/nostril BIDfor 3 days (>3 days use results inrebound symptoms)-No prior antibiotics in the priormonth: -Amoxicillin 500 mg PO tid for 10days (peds 90mg/kg/day divided bidfor 10 days)- Antibiotics in the prior month: -Augmentin 500-875mg PO bid for10 days (peds 90mg amoxicillincomponent/kg/day divided bid)
-TMP/SMX (Bactrim) 1double strength tablet PObid for 10 days (peds 8-10mg/kg/d divided bid). -Doxycycline 100mg PObid for 10 days-Clarithromycin 500mgPO bid for 10 days
-Antibioticsindicated if:->7 dayssymptoms withmaxillary/facialpain and purulentnasal discharge-<7 days if severeillness(pain/fever) One study shows3 days treatmentequal to 10 days
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
12 of 46 9/15/11 3:24 PM

Antiemetics
Phenothiazines: block dopamine D2 receptor in CTZ-Compazine 5-10mg IV/IM/PO or 25mg PR-Phenergan 12.5-25mg PO/PR
IV/IM no longer on ACMC formulary - adverse patient outcomes reported (documented cases of loss oflimb if pushed arterially)
Blackboxed <2yo: apnea Watch for dystonic reactions and restlessness
Prokinetic agents (have dopamine antagonist activity at CTZ) and antichol/antiserotonin
-Reglan 10mg IV/IM/PO -Good all-purpose agent and great for gastroparesis -Watch for drowsiness/restlessness/diarrhea
Serotonin receptor antagonists (5HT-3) work in area postrema and intestinal sites -Zofran (ondansetron)
-Good for peds 0.15mg/kg IV or ODT-Studied in chemotherapy patients, but very effective in other forms N/V-Good side effect profile (HA and constipation, does NOT lower sz threshold)
Antihistamines good for N/V secondary to motion sickness and vertigo -Meclizine 25mg PO qid
Asthma
Oxygen to maintain sats >90% (>95% pregnant and peds)Albuterol (racemic R and S isomers beta-2 agonist) with dosages that vary by institution
-No evidence that higher dosages produce better outcomes -Usual dose is 2.5mg to 5mg neb q20min x 3 prn -For severe asthma may use 5mg neb q20 min x 3 or a 1 hr 15mg continuous neb
-No incremental benefit of giving more than 15mg Albuterol for acute asthma.-Should make admission or discharge decision after this first hour’s treatment.
-May also use MDI W/SPACER 6-12 puffs q 20min to deliver 90mcg/puff -Cheap and just as effective as nebs, may do in waiting room or at home
Levalbuterol (Xopenex, R-isomer) available in 0.63mg and 1.25mg neb solutions -Some trials indicate better for chronic asthma, but expensive, so use sparingly -Less tachycardia than racemic albuterol (of questionable significance)
Atrovent (ipratropium bromide, anticholinergic) 0.5mg nebs x 3 mixed w/albuterol nebs -Albuterol combined with atrovent better than either alone -Affects large, central airways
Epinephrine 0.2 to 0.5cc 1:1000 SQ q20-30 min -Severe side effects, almost never used as have terbutaline (causes MI if acidotic)
Terbutaline 0.25mg SQ q 20min x 3 prn if pt can’t inhale neb treatments -IV dose is 10mcg/kg load then 4mcg/kg/min infusion (for severe exacerbation)
Corticosteroids induce great debate over who gets them, when, and what route New literature weekly Give to mod/severe exacerbation
-Clinically: incomplete response to one neb or PEFR<70% pred after ED tx-Give to pts on inhaled/oral corticosteroids, recent exacerbation or prolonged sx’s
-Works late on inflammation, but also may have an early (1-2 hrs) effect Solu-medrol 125mg IV no better than Prednisone 60mg PO
-IV corticosteroids confer no greater benefit than PO -ONLY give IV if pt very ill and can’t tolerate PO -Increased blood sugars in diabetics (check sugars more freq at home) Discharge with Prednisone 40-60mg qd for 3-10 days (burst, no taper needed) Often ordered incorrectly:
-Solu-medrol is IM/IV -Prednisone is PO tablets-Prednisilone (Orapred, Pediapred, Prelone) is PO syrup for pediatric dosing (give 2mg/kg max of60mg PO in ED and discharge on 1mg/kg for 5 days). Orapred is best tasting according to somestudies.Orapred ODT (oral dissolving tablets) in omnicell (10, 15mg)
-Inhaled corticosteroids now recommended at ED discharge (especially >2 days asthma per weekor >2 nights/month –this is highlighted in red in IBEX as a reminder)
§ Asmanex (mometasone) 220mcg bid or 440mcg qd one single puff daily [mnemonic
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
13 of 46 9/15/11 3:24 PM

A-smanex = A single puff daily in Adults (not approved <12yo)]§ If on oral steroids start 440mcg bid§ Make sure pt gets asthma education and IHCS education by PharmD or RT§ For <12 yo, use Flovent (Asmanex not yet approved for peds). 88-220 mcg twice daily§ Budenoside (pulmicort) is only inhaled steroid in nebulized form
Magnesium 1-2gm IV over 30min for severe exacerbations -Never been proven efficacious, but probably can’t hurt pt about to be intubated
Theophylline hardly ever given in ED, but check a level on any pt who takes this at homeHeliox may also be used as last resort before intubationKetamine (1-2mg/kg IV) may be used for intubation
Atrial fibrillation Diltiazem 0.25mg/kg IV (20mg) followed in 15 minutes by 0.35mg/kg IV (25mg) if no response -Used for rate control -Preferred over Verapamil as may have less inotropic depression with less hypotension -Administer over 5 minutes (not push) to decrease chance of hypotension -Treat hypotension with calcium gluconate 5mL IV -May pretreat with calcium gluconate 5mL IV to prevent hypotension
-If effective, follow by a drip at 5-15mg/hour-Start dosing lower if elderly/in CHF/hypotensive-Concurrent use of diltiazem with erythromycin (ex. Pneumonia patient) prolongs QT – use doxycyclineinstead
Verapamil 2.5-5mg IV followed in 30min by 5-10mg IV if no response -Used for rate control -May cause more hypotension than diltiazem
-Drip at 5mg/hour for maintenance-Start dosing lower if elderly/in CHF/hypotensive-Not used very commonly
Esmolol 500mcg/kg IV bolus over 1min then 50-200 mcg/kg/min IV drip -Used for rate control -Especially useful for pts with AMI or thyrotoxicosis
-Repeat bolus and increase drip as needed-Caution in pts with severe RAD or active wheezing-Half-life is approximately 9 minutes
Metoprolol (Lopressor) 5mg IV q5 min until rate control achieved - Used for rate control -Especially useful for pts with AMI or thyrotoxicosis -Caution in pts with severe RAD or active wheezing Digoxin not used in the acute setting. -Check a level if pt already on this medication Amiodarone 150mg IV over 10min -Not FDA-approved for rate control of supraventricular tachycardias -Wide range of reported efficacies
-Less efficacious than diltiazem and magnesium for rate control and conversion-Very little predisposition to hypotension as even less negative inotropy than diltiazem
Magnesium 2-4gm IV over 30 minutes
-Preliminary investigations suggest better rate control and conversion than dilt and amio Heparin IV or Lovenox SQ administration in the ED is controversial. ED conversion to NSR is VERY controversial. -Only do in consultation with Cardiology or Internal Medicine
Cardiac arrest MUST know PALS and ACLS well…know all drug dosages and algorithms (see above) Review ACC handbook monthly and while in ICUs Epinephrine 1mg IV OR Vasopressin 40IU IV one time only -Repeat epinephrine q3-5min
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
14 of 46 9/15/11 3:24 PM

-May give epinephrine standard dose if Vasopressin fails (Vasopressin lasts 10 minutes-so no need to giveepi for 10 minutes)-Peds: 0.1mL/kg 1:10,000 epinephrine (max 1mg)
Amiodarone
-300mg IVP for pulseless VT and Vfib (peds: 5mg/kg bolus IV) -150mg IV over 10min for all other indications
-Studies have suggested that Amiodarone increases pt survival to hospital admission but does NOTimprove pt survival to hospital discharge
Atropine - 1mg IV q3-5 min to max of 0.04mg/kg
Lidocaine 1.5mg/kg IV (may repeat x 1) with usual dose of 100mg IV Magnesium - 1-2 grams IV Procainamide 17mg/kg (administer at 20-30mg/min) – max dose 1gram -Stop if hypotension, QRS prolongs more than 50% or prolonged QT
Chest pain/Acute Coronary Syndromes IV, O2, monitor and EKG within 5 minutes of arrival Note: Hospital is graded on administration of ASA/Beta Blockers- document reason for withholding (vitals;allergy; taken at home prior to arrival; other contraindications) ASA 81mg x 4 baby aspirins PO (chewed) or 300mg rectally -Plavix 600mg PO if severely allergic to ASA Plavix 600mg PO
-Since plavix should be avoided in patients who will need a CABG and we cannot predict who thesepatients will be prior to cath lab, ask the admitting cardiologist if they desire plavix in addition to ASA
NTG 0.4mg (one tab) SL q5min prn x 3-4
-If now pain free can usually place on Nitropaste 1 inch for continued preload reduction after SLNTG NTG IV—start at 10-20mcg/min and slowly increase -IV is best for unstable pts who may not tolerate large SL dose OR -For patients that are not pain free after SL NTG
-Remember than SL NTG is 400mcg over 5min so it delivers approx 80mcg/min of NTG-Note Christ Medical Center Code 60 criteria (STEMI) requires IV NTG (not sublingual)-Note Christ Medical Center CHF protocol requires IV NTG (not sublingual) since it is easily titratableand desired 20% decrease in mean arterial pressure can be more easily achieved
Lopressor (Metoprolol) 5mg IV x 3 q 5min prn HR > 60 and SBP >100 or 25 PO x 1
-Note Christ Medical Center Protocol requires beta blockers within 24 hours (hospital is graded on this)-STEMI
-IV beta blocker use is controversial based on COMMIT trial (increased cardiogenic shock); maywant to discuss with cardiologist before administering (usually no longer recommended)-Oral beta blocker per AHA Guidelines in 24 hrs if: no signs of heart failure, low output state,increased risk of cardiogenic shock (>70 yo, SBP <120, HR > 110, HR < 60, increase time ofonset since symptoms), other relative contraindications to beta blockers (PR > 0.24, 2nd/3rd
degree heart block, active asthma or reactive airway disease)-NSTEMI/UA
-PO beta blocker within 24hrs in the absence of contraindications Lovenox 1mg/kg SQ after normal CXR and no blood on rectal exam -Lovenox and lopressor only for suspected UA/NSTEMI (not atypical CP)
-Preferred over Heparin. Heparin preferred if creatinine >1.6 or in STEMI protocol Heparin 60units/kg bolus (max 4,000 units) followed by 12units/kg/hr (max 1,000 units/hr) -Note PE/DVT dose is larger (80 units/kg followed by 18 units/kg/hr)
-Heparin preferred over lovenox if there is a relative contraindication (ie. slightly guaic positive) becausethe drip can be turned off
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
15 of 46 9/15/11 3:24 PM

Eptifibatide (Integrilin) (GPIIb/IIIa receptor blocker) -Evidence for use constantly changing, use in consultation w/cardiologist -Probably beneficial if pt will be going to the cath lab
-Contraindication (Creatinine >4.0); recent surgery; BP >180/110; low platelets; bleeding diathesis
Congestive Heart Failure Must know Christ Medical Center CHF Protocol. Mnemonic: LMNOPQ. Q=Quinton Catheter (ie. in the dialysis pt with CHF they need dialysis) Lasix
-1mg/kg.-1-2 x home daily dose (usually 60mg or 80mg IV)-If urine output <200ml after 1hour, repeat same dose
-Second line to NTG for preload reduction-Stated reduction in preload is extrapolated from studies evaluating effects on forearm and wristveins, however, Swan-Ganz catheter studies found no immediate benefit in preload-Lungs can be thought of as buckets partially filled with fluid when patient is in pulmonary edema,however the patient may not be total-body hypervolemic thus diuretic often leads to hypotensionthe next day
Morphine-2mg IV-Not on CHF standing orders-Limited data supporting efficacy in decreasing preload (based on study evaluating venous tone in wristand forearm veins but numerous Swan-Ganz catheter studies show no benefit in preload reduction)-Due to multiple side effects benzodiazepine preferred for anxiolysis-Current literature “no role for morphine”
NTG-IV NTG 20mcg/min and TTE by increasing gtt 10-20mcg q5min or doubling rate q5min
-Titrate to MAP decrease of 20% as per CHF protocol
-Recall SL tab is 400mcg/5min or 80mcg/min (20mcg IV is low dose) so be aggressive with drip or givesublingual initially
-First line for preload reduction
-Avoid in hypotension, valvular problems (acute mitral regurgitation, aortic stenosis, pulmonaryhypertension), Viagra or other erectile dysfunction medication use in the last 24 hours
Nesiritide (Natrecor)
-2 mcg/kg bolus IVP, then start drip at 0.01mcg/kg/min. Hold if SBP < 90.
-Usually ordered after consultation with a cardiologist
-40 times more expensive and not necessarily better than NTG
-VMAC study drug reps refer to criticized for using suboptimal doses of NTG and beingmanufacturer sponsored. VMAC study proved that Nesiritide better than placebo but not that it isbetter than NTG
-Other studies trend towards worsening renal function and increased mortality
Oxygen (titrate to O2 sat > 92% by nasal cannula, ventimask or nonrebreather) Position patient upright Positive pressure ventilation prn
-Either BiPAP, CPAP or intubation with PEEP -Start BIPAP I 10/ E 4 to maintain sat >92%-Positive pressure in only currently available treatment demonstrated to decrease mortality
Pressors/Drips if needed -NTG IV if SBP >90
-Preload reducer, will also reduce afterload at high doses-Excellent single agent for preload and afterload reduction
-Nipride IV if SBP > 100 -Outstanding afterload reducer but not used often
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
16 of 46 9/15/11 3:24 PM

-More afterload reduction than NTG, coronary stealàischemia. -Nurses not as familiar with use -Need to wrap in foil
-Dopamine IV 2-20mcg/kg/min if SBP <100 -Dobutamine IV 2-20mcg/kg/min if SBP >100 -May drop BP due to beta-receptor mediated vasodilation ACE Inhibitor:
-Note that hospital is graded on ACE-I administration so document reason for withholding ACE or ARB(renal insufficiency; allergy; hx of severe cough with ACE; potassium elevated; hypotension; pregnant,severe aortic stenosis)-Lisinopril (Prinvil/Zestril) 10 mg PO
-Enalapril (Vasotec) 1.25mg IV-First dose okay without creatinine or potassium, subsequent doses require creatinine andpotassium level-Contraindications: hypotension, dehydration, poor perfusion, allergy, angioedema, pregnancy,renal insufficiency (cr >3), renal artery stenosis, hyperkalemia- Hold if patient already took ACE in dosing cycle
Angiotensin Receptor Blocker (ARB) Losartan (Cozaar) 25mg PO -Use in ACE allergy
-First dose okay without creatinine, subsequent doses require creatinine -Same contraindications as ACE Inhibitor. -Hold if already taken in dosing cycle -Not much literature exists yet
Contrast Load in Renal InsufficiencyContrast-induced nephropathy remains a common complication of radiographic procedures.Prophylaxis of contrast induced renal failure: 1L 5% Dextrose (D5W) with 3 amps of Sodium Bicarbonate (150 mEq)Infuse 3mL/kg/hr for one hour prior to contrast followed by 1ml/kg/hr for 6 hours post procedure
Or Mucomyst (N-acetylcysteine) 600mg po bid x 4 doses
Or Mucomyst (N-acetylcysteine) 1200mg po bid x 4 doses (one study showed higher doses was more protective forpatients undergoing angioplasty) Nursing Implication: Acetylcysteine is available in two concentrations. Recommend using the 10% solution(100mg/ml). Once appropriate volume is drawn up (6ml for 600mg dose) dilute in 4-6 ounces of juice.
Croup Humidified oxygen Decadron 0.6 mg/kg (max 10mg) IV/IM. PO Decadron dose is the same.
-PO Decadron is available in the omincell-If no PO Decadron available the IV solution may be given PO at the same dose (some report that the IVDecadron tastes better than the PO Decadron!). IV and PO are bioequivalent. Mix IV solution with juiceto dilute it.
Nebulized Epinephrine (0.5 mL of racemic epi OR 5mL of 1:1000 epi)
-Epi not necessary in all croup patients. STRIDOR AT REST usually requires epi because just decadronalone will result in inadequate resolution. However in stridor only with crying humidified oxygen anddecadron alone may suffice. -Standard of care is to observe for 3 hours after epi neb because some patients have recurrence (debatable)-Racemic epi is more expensive and 1:1000 epi works just as well-Dosing recommendations as above- bur remember any excess just goes out to the environment anyways.-Closely monitor patients with severe left ventricular outflow obstruction (IHSS, AS, etc). Nebulized epiis relatively contraindicated in these patients.
Heliox -Consider in patients about to be intubated
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
17 of 46 9/15/11 3:24 PM

-Decreases turbulent airflow in airway
DKA (adult) Be familiar with Christ Medical Center DKA protocol Remember the entity is the definition
-Diabetic (hyperglycemic usually >250mg/dL) (Note may have DKA with glucose<250 if AG >16,ketones in urine)
-Ketotic (acetoacetic acid and beta-hydroxybutyric acid in blood and urine) -Acidotic (bicarb usually < 15 and pH usually < 7.3)
-pH may be near normal if concurrent contraction alkalosis from dehydration-Glucose may not be tremendously elevate-Ketones: only acetoacetate (ACAC) not betahydroxybutyrate (BHBA) is measured so ketonesmay be negative if predominantly BHBA (rare). Mnemonic: Acetoacetate is Assayed.-Despite pH, glucose, and ketones not always being reliable a patient cannot have a normal aniongap and be in DKA. A normal AG rules out DKA.
-A VBG is as useful as an ABG and is less painful and easier to obtain Check EKG FIRST (to r/o hyperkalemia) Labs:
dexi/CBC/PA7/CMP/VBG/UA/serum ketones. New onset <45yo: Endocrine consultants at ACMC want serum insulin level, ICA 512 (Islet cellantibody), AntiGAD 65, insulin AB, C-peptide: all prior to initiating insulin therapyDexi, K+, pH (venous)- q 1 hourLytes/BUN/Cr– q 2 hoursCa++, PO4, Mg++- q 4hours
Goals are to replace fluid and electrolyte deficits, identify precipitating cause and supply insulin Remember FICKU:
-Fluids-Insulin-Check urine output-K+-Underlying cause (AMI, infection, noncompliance…)
Fluids
Place two IV’sInitially IV#1 has 0.9NS in as bolus (0.45 NS if Na > 140meq/L), IV#2 is at TKOFirst two liters in IV#1 over first 1-2hrs (pts usually have 100ml/kg water deficit)Then change IV#1 to 0.9NS at 250cc/hrWhen dexi < 250 change IV#2 to D5 1/2NS + (__)KCl
Insulin
IV Regular insulin is started at 0.1u/kg/hr with NO bolus dose neededIncrease drip if glucose not decreasing (q 1 hr dexis)Continued until AG resolves (occurs AFTER glucose normalizes). Residual ketones my persist due toconversion of BHBA to ACACTypically takes 12-18hours
Check urine output (before administering potassium!). Foley for strict I and Os. K+
-If initial K+ > 5.5 begin insulin drip at 0.1u/kg/hr and repeat K+-If initial K+ from 3.5 to 5.5 begin IV#2 with 1/2NS + 40meq KCl at 250cc/hr and insulin -gtt at
0.1u/kg/hr
-If initial K+ < 3.5 hold insulin for 30min and begin IV#2 with 1/2NS + 60meq KCl at 250cc/hr (thrucentral line)
**When d-stick < 250 change IV#2 to D5 1/2NS + (__)KCl Replace phosphate only if level < 1.0mg/dLReplace magnesium if level < 1.2mg/dL or symptoms (tetany) develop
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
18 of 46 9/15/11 3:24 PM

MUST RECHECK lytes q1-2hrs in the initial treatment phaseBicarbonate is controversial since some literature associates it with increased cerebral edema: Per ACMCprotocol give 1meq/kg HCO3 if pH <7.1 or HCO3 below 10. Give over 0.5-2 hours-do not push!
Underlying cause (the “I” ‘s ) Infection, Infarction, Ischemia, Infarct, Imbibing (alcohol), Infant (pregnancy) DKA (pediatric)Only bolus 10cc/kg 0.9NS to start to prevent possible cerebral edema -Literature varies on importance of this entity and its cause, but be cautious with IVF
DONT protocol D50 one amp IV (or just check d-stick and give D50 only if <60 or 70) Oxygen (check pulse ox) Narcan 2mg IV/IM/ETT
-Full 2mg dose if apneic; 0.4 mg IV in known opioid addict who is not apneic-May repeat up to 10mg total dose if no response to initial 2mg dose
Thiamine 100mg IV
Electrolyte Replacement (these guidelines do not apply to patients with a Cr > 2 or dialysis patients) Calcium replacement:
Ionized calcium (mmol/L) Replacement1.1-1.16 2 grams calcium gluconate in
100 ml NS over 2 hours1 or less 4 grams calcium gluconate in
250 ml NS over 4 hours Magnesium replacement:
Magnesium level (mg/dL) Replacement1.3-1.7 Magnesium Oxide 800mg po1.3-1.7 (symptomatic) 2 grams IV< 1.3 4 grams IV< 1.5 and symptomatic 2 grams over 30 minutes, then as above after
level rechecked after 1 hour Phosphorus replacement:
Phosphorus level (mg/dL) Replacement2-2.5 2 packet Na/K Phos (NeutraPhos) q12h x 2 doses
PO/NG/GT1.3-1.9 20 mmol NaPhos IV over 4 hours< 1.3 40 mmol NaPhos IV over 6 hours
Potassium replacement
Potassium level (mmol/L) PO/NG/GT replacement Peripheral IV replacement
3.6-3.8 40 mEq KCL liquid or tab x 1dose
20 mEq over 2 hours
3.1-3.5 40 mEq KCL liquid or tab q4h x2 doses
40 mEq over 4 hours
3 or less 40 mEq KCL liquid or tab q4h x3 doses
60 mEq over 6 hours
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
19 of 46 9/15/11 3:24 PM

Absolute risk rates for IE from a dental procedure in patients with underlying cardiac disease.*Mitral valve prolapse (MVP) 1/1,100,000 proceduresCongenital heart disease (CHD) 1/475,000 proceduresRheumatic heart disease (RHD) 1/142,000 proceduresPatient with prosthetic cardiac valve 1/114,000 proceduresPrevious IE 1/95,000 procedures
Endocarditis Prevention of Infective EndocarditisAmerican Heart Association 2007 Guidelines Revisions to the 1997 guidelines were made based on published evidence over the last 20 years. Theseguidelines have been approved by the ADA, IDSA, and PIDS. Infective Endocarditis (IE)Turbulent blood flow through the heart can cause damage to some of the endothelium of cardiac valves. Plateletsand fibrin can then build up at these damaged sites. Certain invasive procedures, (e.g. dental extractions, GI orGU tract surgery) can release bacteria into the bloodstream which then has the potential to colonize the damagedendothelium in the heart. Colonization and proliferation of bacteria at these sites result in infective endocarditis. Reasons for antibiotic prophylaxis
Viridans group streptococci (part of normal oral, skin, GI, respiratory flora), which is responsible for mostcommunity-acquired IE in non-IVDU, can be released into bloodstream as part of invasive procedureThe normal flora that may cause bacteremia respond well to antibioticsIn animal studies, antibiotic prophylaxis works to prevent IERisks and cost of antibiotic prophylaxis is lower than morbidity and mortality associated with IE
Reasons against antibiotic prophylaxis
Most data is on risk of IE from dental procedures; very little is available on risk or prevention of IE fromGI or GU tract proceduresThe risk of bacteremia is much higher from daily activities (chewing food, brushing teeth, flossing) andpoor oral hygiene than from dental extraction, which is the procedure thought to be most likely to causetransient bacteremia. Brushing twice daily for a year results in 154,000 times more risk for bacteremiathan one tooth extraction.Some studies find amoxicillin prophylaxis to reduce bacteremia after a dental procedure, but others find itdoes not. No data shows that reduction in bacteremia from amoxicillin reduces risk of IE. The same is trueof other antibiotics used for prophylaxis, as well as chlorhexadine or povidone iodine rinses.Several studies are finding that there is no statistical benefit to antibiotic prophylaxis in high-risk groupsundergoing dental procedures, even if the antibiotics are 100% effective. According to these studiesprophylaxis does not prevent IE in very many cases.Risk of adverse events from the antibiotic exceeds the benefit from prophylaxis.General oral hygiene recommendations could be more beneficial to high-risk patients than antibioticprophylaxis before procedures.
*in general population risk is 1/14,000,000 procedures Current RecommendationsAntibiotic prophylaxis during a dental procedure with manipulation of gingival tissue or periapical region of teethor perforation of oral mucosa is recommended in patients with:
· Prosthetic heart valve· Previous IE· Unrepaired cyanotic CHD, including palliative shunts and conduits· Completely repaired congenital heart defect with prosthetic material or device during the first 6 months
after the procedure· Repaired CHD with residual defects at or adjacent to the site of a prosthetic patch or device (which
inhibit endothelialization)· Cardiac transplantation recipients who develop cardiac valvulopathy
Prophylaxis may also be considered in these patients if undergoing a respiratory procedure that involves incisionor biopsy of the respiratory mucosa. If these patients have an established respiratory infection, include an agentthat will work against viridans group streptococci. Prophylaxis is NOT recommended for patients undergoing aninvasive GI or GU tract procedure. However, if an active infection is present in the GI or GU tract in thesepatients, an agent may be chosen that is effective against enterococci (the bacteria most likely to cause bacteremia
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
20 of 46 9/15/11 3:24 PM

in the GI and GU tract). When these patients are undergoing surgery on infected skin, skin structure, ormusculoskeletal tissue, include an agent effective against staphylococci and b-hemolytic streptococci in theantibiotic regimen against the infection.
Antibiotic regimen 30-60 minutes prior to an invasive dental procedure. Antibiotic Adults ChildrenPO Amoxicillin 2g 50mg/kg
NPO Ampicillin ORCefazolin or Ceftriaxone
2g IM or IV 1g IM or IV
50mg/kg IM or IV 50mg/kg IM or IV
PCN allergy – PO Cephalexin*^ORClindamycinORAzithromycin or Clarithromycin
2g 600mg 500mg
50mg/kg 20mg/kg 15mg/kg
PCN allergy – NPO Cefazolin^ or Ceftriaxone^ORClindamycin
1g IM or IV 600mg IM or IV
50mg/kg IM or IV 20mg/kg IM or IV
*or any other 1st or 2nd generation cephalosporin in equivalent dosing^cephalosporins should be avoided if allergic reaction to PCN was severe
INR Elevation INR above therapeutic range but less than 5 with no significant bleeding:
-Lower warfarin dose or omit dose-Monitor more frequently-Resume at lower dose when INR therapeutic
INR equal to or greater than 5 but less than 9 with no significant bleeding:
-Omit next 1 or 2 warfarin doses .Monitor more frequently and resume at lower dose when INR intherapeutic range or-Alternatively, omit dose and give vitamin K (5 mg or less ORALLY), particularly if at increased risk ofbleeding.-If more rapid reversal is required because the patient requires urgent surgery, vitamin K (2 to 4 mgORALLY) can be given with the expectation that a reduction of the INR will occur in 24 hours.-If the INR is still high, additional vitamin K (1 to 2 mg ORALLY) can be given.
INR 9 or greater with no significant bleeding:
-Hold warfarin therapy and give higher dose of vitamin K (5 to 10 mg ORALLY) with the expectationthat the INR will be reduced substantially in 24-48 hrs.-Monitor more frequently and use additional vitamin K if necessary.-Resume therapy at lower dose when INR therapeutic.-Note that INR 5-9 does not necessarily mandate vitamin K but INR >9 does due to markedly increasedrisk of bleeding
INR greater than 20 with no significant bleeding:
-Hold warfarin therapy and give vitamin K (10 mg by slow intravenous (IV) infusion), supplemented withfresh frozen plasma, depending on the urgency of the situation-Recombinant factor VIIa may be considered-Vitamin K can be repeated every 12 hrs.
Life-threatening bleeding:
-Hold warfarin therapy and give vitamin K (10 mg by slow IV infusion)-Fresh frozen plasma-Recombinant factor VIIa may be considered -Repeat if necessary, depending on INR.
-When vitamin K is administered to lower INRs, it should be administered at a dose that will lower the INR into asafe range quickly, without it being subtherapeutic, causing warfarin resistance, or exposing the patient toanaphylaxis risk. -Low doses and slow infusion rates of vitamin K are recommended. If continuing warfarin therapy is indicatedafter high doses of vitamin K, then heparin or low molecular weight heparin can be given until the effects ofvitamin K have been reversed and the patient becomes responsive to warfarin therapy. Intravenous Route of Administration:-If the intravenous route of administration is considered unavoidable, the drug should not exceed anadministrative rate of 1 milligram/minute. Preferably the drug should be diluted in 50-100 mL of 5% Dextroseand infused over 30 minutes.
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
21 of 46 9/15/11 3:24 PM

Parenteral Route of Administration:Severe reactions, including fatalities, have occurred during and immediately after intravenous injection ofvitamin K, even when precautions have been taken to dilute the drug and to avoid rapid infusion. These reactionshave also been reported following intramuscular administration. Typically these severe reactions have resembledhypersensitivity or anaphylaxis, including shock and cardiac and/or respiratory arrest. Some patients exhibitedthese severe reactions when they received vitamin K for the first time. Therefore the intravenous andintramuscular routes should be restricted to those situations where the subcutaneous route is not feasible and theserious risk involved is considered justified (ie serious bleeding or INR >20). Subcutaneous vs. Oral Route of Administration:One mg of oral vitamin K decreases the INR faster than 1mg of subcutaneous vitamin K in asymptomatic patientswith elevated INR values. While subcutaneous vitamin K (1-2mg) reverses warfarin, the response may be lesspredictable and delayed when compared to oral administration. Thus the above protocol recommends PO insteadof SQ vitamin K.
Insulin Sliding Scale Also be familiar with Christ Medical Center “Insulin Infusion Orders-Excluding DKA” which can be usedinstead of a sliding scale for hyperglycemic patients not in DKA Adults: REGULAR INSULIN
LOW DOSE MODERATE DOSE HIGH DOSEIF Blood Sugar… Regular Insulin Regular Insulin Regular Insulin
150-200 2 3 4201-250 3 4 6251-300 4 6 8301-350 5 8 10351-400 6 10 12
> 400 Notify physician Notify physician Notify Physician NOVOLOG INSULIN
LOW DOSE MODERATE DOSE HIGH DOSEIF Blood Sugar… Novolog Insulin Novolog Insulin Novolog Insulin
150-200 2 3 4201-250 3 4 6251-300 4 6 8301-350 5 8 10351-400 6 10 12
> 400 Notify physician Notify physician Notify Physician
Local Anesthesia Lidocaine 1% (onset 2-5min, lasts 30-60min) -Max dose w/o epi is 4.5mg/kg or 0.45ml/kg and w/epi 7mg/kg or 0.7ml/kg - Avoid epi on, pinna of ear, nose, penis and digits Bupivacaine 0.25% (onset 3-7min, lasts 90-360 minutes). Higher cardiac toxicity than lido. -Max dose w/o epiis 2mg/kg or 0.8ml/kg and w/epi is 3mg/kg or 1.2ml/kg LET (lido/epi/tetracaine) for topical use on non-intact skin. -Drip some into wound and place some on gauze taped to wound for 20min Viscous lidocaine for topical use -Used in ED for intraoral lacs -Used for outpatients with intraoral ulcers and genital ulcers
-Remember maximum dose to avoid toxicity in the outpatient setting LMX for topical use on intact skin -30 minutes to effect -Useful for pediatric LPs
-Do not wipe skin with alcohol prior to application since LMX needs oils of skin to get absorbed
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
22 of 46 9/15/11 3:24 PM

Nerve blocks: median/ulnar/radial/digital/inferior alveolar/infraorbital/intercostal
Migraine treatment Compazine (prochlorperazine) 10mg IV Toradol (ketorolac) 30mg IV or IM -No more effective than PO NSAIDs and much more expensive -Be sure pt does not have a SAH before using this Reglan (metoclopramide) 10mg IV Imitrex (Sumatriptan) 6mg SC, may repeat 6mg SC in 1h if not effective -Expensive but quick and easy to give as no IV access needed -CI’d in CAD/uncontrolled HTN/pregnancy (use cautiously if age>50) Decadron 10mg IV (dose debatable in literature) for refractory migraines **Some practitioners give Benadryl 25-50mg IV with Compazine/Reglan -Prophylaxis against side effects of medications -Also makes pt sleep which often helps resolve the headache
MRSA Treatment (soft tissue)
Risk Factors
· Prior history of MRSA infection· History (within the past 12 months) of hospitalization, surgery, long-term care residence, indwelling
catheter or medical device, dialysis, renal failure, or diabetes· Close contact with someone known to be infected with MRSA
Diagnosis
· All MRSA infections should first be classified as hospital acquired vs. community acquired.· MRSA infections may be further broken down into four groups:
A. Superficial colonization of a wound, without signs of infectionB. Superficial soft tissue infection/cellulitisC. Complex skin and skin structure infectionD. Osteomyelitis
Community vs Hospital
· Diagnosis of MRSA was made in the outpatient setting or by a culture positive for MRSA within 48hours after admission to the hospital.
· No medical history of MRSA infection or colonization.· No medical history in the past year of:
HospitalizationAdmission to a nursing home, skilled nursing facility, or hospiceDialysisSurgeryNo permanent indwelling catheters or medical devices that pass through the skin into the body.
Superficial colonization
· May be treated without the use of oral or IV antibiotics.· Regular cleansing of the wound with Hibiclens· Close monitoring of the wound for possible signs of infection
Superficial skin and soft tissue infection/cellulitis
· Local wound cleansing and debridement should be accompanied by antibiotic therapy.· Should be treated with antibiotics for at least ten days but may vary depending on severity of infection
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
23 of 46 9/15/11 3:24 PM

and clinical response.· Antibiotic choice should include one of the following:
Trimethoprim-sulfamethoxazole-2 tablet PO bid. Clindamycin 300mg bid (increasing resistance)Doxycycline-100 mg PO bidRifampin (never use Rifampin as monotherapy due to rapid emergence of resistance.)
Complex skin and skin structure infection
· Community acquired:Treat same as superficial
· Hospital acquired:Vancomycin IVZyvox
Osteomyelitis (Hospital or Community Acquired)
· Aggressive surgical resection of infected bone and soft tissue should be performed as soon as possible.· Peripheral vascular sufficiency should be established immediately and a vascular consult ordered if
there are questions as to peripheral vascular diseases.· Once MRSA has been positively identified, the patient should be placed on a six-week course of
Vancomycin with weekly monitoring of peaks and troughs with BUN and Creatinine.· Zyvox may be used in cases of Vancomycin resistant enterococci.
Pediatric common medications Acetaminophen 15mg/kg PO q4h.
-Mnemonic: Every 10 kg=1 tsp Tylenol (160/tsp) q 4h. 10kg= 1tsp q 4h. 20kg=2 tsp q 4h. 25kg=2.5 tspq4h. Similar mnemonic for ibuprofen
Amoxicillin (low dose) 45mg/kg/d divided tid Amoxicillin (high dose) 80-90mg/kg/d divided bid Ampicillin 50-100mg/kg IV up to 2g -Neonatal fever < 6weeks to cover Listeria -Also used for meningitis in elderly patients and others at risk for Listeria Azithromycin 10mg/kg the first day then 5mg/kg qd for 4 more days Cefotaxime (Claforan) 50-100mg/kg IV -Used mostly in neonates < 4-6wks old when can’t use Rocephin due to biliary sludging Ceftriaxone (Rocephin) 50mg/kg IV up to 1g -100mg/kg up to 2g for meningitis or suspicion of meningitis -Do not use in neonates < 4-6wks old due to possible biliary sludging**Different sources and practitioners utilize varying dosages of Amp/Claf/Ceftriaxone Some use 50mg/kg while others use 100mg/kg Decadron 0.6 mg/kg (max 10mg) IV/IM. PO Decadron dose is the same.
-PO Decadron is available in the omnicell-If no PO Decadron available the IV solution may be given PO at the same dose (some report that the IVDecadron tastes better than the PO Decadron!). IV and PO are bioequivalent
Dextrose 0.5g/kg IV (if unable to tolerate PO glucose) -Neonates get D10 5cc/kg (10 x 5 = 50) -Infants get D25 2cc/kg (25 x 2 = 50) -Children may get D50 1cc/kg (50 x 1 = 50) but preferably get D25 if possible -Higher osmolarity solutions cause tissue necrosis/pain at IV site/rebound -D25 is stocked in the PEC omnicell so have nurses use that concentration Diphenhydramine (Benadryl) 1 mg/kg PO q6h Nebulized Epinephrine (0.5 mL of racemic epi OR 5mL of 1:1000 epi) -Croup, bronchiolitis
-Epi not necessary in all croup patients. STRIDOR AT REST usually requires epi because just decadronalone will result in inadequate resolution. However in stridor only with crying humidified oxygen anddecadron alone may suffice.
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
24 of 46 9/15/11 3:24 PM

-Standard of care is to observe for 3 hours after epi neb because some patients have recurrence (debatable)-Racemic epi is more expensive and 1:1000 epi works just as well-Dosing recommendations as above- bur remember any excess just goes out to the environment anyways.-Closely monitor patients with severe left ventricular outflow obstruction (IHSS, AS, etc). Nebulized epiis relatively contraindicated in these patients.
Ibuprofen 10mg/kg PO q6h
-Every 10 kg=1 tsp Motrin (100/tsp) q 6h. 10kg= 1tsp q 6h. 20kg=2 tsp q 6h. 25kg=2.5 tsp q6h. Similar mnemonic for acetaminophen.
Methylprednisolone (Solu-Medrol) 1-2mg/kg (max 125mg) IV Prednisone/Prednisilone (Oprapred, Pediapred, Prelone) 1-2mg/kg PO (max 60mg) then 1mg/kg PO qd for 5days
Steroids often ordered incorrectly: -Solu-medrol is IM/IV only -Prednisone is PO tablets-Prednisilone (Orapred, Pediapred, Prelone) is PO syrup for pediatric dosing (give 2mg/kg max of60mg PO in ED and discharge on 1mg/kg for 5 days). Orapred best tasting according to somestudies-Orapred ODT (oral dissolving tablets) in omnicell (10, 15mg)-Remember IV is no more effective or quicker acting than PO prednisone
Robitussin (1/2tsp)/10kg PO q4h
Post Exposure Non-Occupational HIV Prophylaxis
The combination and the recommended doses, in the absence of known resistance to zidovudine(ZVD) or lamivudine in the source patient are:
· ZDV 250-300mg twice a day or Combivir twice daily· Lamivudine 150 mg twice a day
PLUS
· Liponavir/Ritonavir (Kaletra) 2 tabs twice a day or Efavirenz (Sustiva) 600 mg once daily (notrecommended for use in pregnant women)
Note: Kaletra is better tolerated than Sustiva
Post Exposure Occupational HIV Prophylaxis · ZDV 250-300mg twice a day or Combivir twice daily· Lamivudine 150 mg twice a day
PLUS
Crixivan (Indinavir) 800 mg TID or Liponavir/Ritonavir (Kaletra) 2 tabs twice a day
Post LP Headache Only proven technique is to use smaller gauge needle and non-cutting needle when performing the procedure. Bedrest, caffeine, IVF have not been proven by evidence based methods Some recommend caffeine 100-200mg PO or 500mg IV over 2 hours (severe). Most cases are severe and requireIV caffeine or epidural patch. For IV Caffeine:Order 1 L NS over 1 hour then caffeine drip (500mg in 1L NS) over 2 hours followed by 1L of NS over 1-2hours. Consult anesthesia to perform epidural patch if not resolved with caffeine.
Preeclampsia/eclampsia
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
25 of 46 9/15/11 3:24 PM

Magnesium 4-6g IV over 15min then 1-2g/h IV -Monitor DTRs and watch for respiratory depression Hydralazine 2.5mg IV then 5-10mg IV repeated up to 40mg max -May take up to 20min to see a response after dose is given
-Is “drug of choice” after Mg for eclamptic HTN Labetolol 20mg IV then 40-80mg IV q10min up to 300mg max -Then start drip at 1-2mg/min and titrate -Less reflex tachycardia and hypotension than hydralazine **Lab studies are: UA, CBC, LFT, PA7, uric acid, PT/PTT/INR
Procedural sedation Agents have various properties: analgesia, sedation, amnesia, dissociation Usually best to start on the lower end of dosing and titrate to effect Etomidate 0.1-0.3mg/kg IV Fentanyl 1-2mcg/kg IV AND Versed 0.02mg/kg IV good for ortho/lacs/adults Ketamine (dissociative agent) 1-2mg/kg IV OR 4mg/kg IM -Agent of choice for peds because patients do not lose airway reflexes. -Increases airway secretions. Some give atropine 0.02mg/kg in same syringe. -May also use glycopyrrolate (Robinul) -Emergence reactions are more common in adults. May decrease with Versed. Methohexital (Brevital) 1mg/kg IV is a great drug. Rapid onset and wears off in 2-10min. Propofol (Diprivan) 1mg/kg over 1-3 minutes followed by 0.1mg/kg/min q 15 seconds -May cause apnea and hypotension
-Rapid onset, short duration (patients awake and responsive within 8 mins of discontinuation)-Nurses can NOT push propofol in this setting, must be done by resident/attending
For reversal: Narcan 0.4mg IV (peds: 0.05mg/kg IV). Lasts 1-2hrs. Flumazenil 0.2mg IV (peds 0.01mg/kg IV). Beware seizures in pts with known d/o.
RABIESRabies Post Exposure Guidelines Wild animals - especially bats - are the most common source of human rabies infectionin the United States. Skunks, raccoons, dogs, and cats can also transmit the disease. Human rabies is rare in the United States. There have been only 39 cases diagnosed since 1990. However,between 16,000 and 39,000 people are treated each year for possible exposure to rabies after animal bites. Also,rabies is far more common in other parts of the world, with about 40,000 - 70,000 rabies-related deaths eachyear. Bites from unvaccinated dogs cause most of these cases. Rabies vaccine can prevent rabies. Rabies vaccine is given to people at high risk of rabies to protect them if they are exposed. It can also prevent thedisease if it is given to a person after they have been exposed. Rabies vaccine is made from killed rabies virus. It cannot cause rabies. Vaccination After an Exposure Anyone who has been bitten by an animal, or who otherwise may have been exposed to rabies, should see adoctor immediately. A person who is exposed and has never been vaccinated against rabies should get 5 doses of rabies vaccine - one
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
26 of 46 9/15/11 3:24 PM

dose right away, and additional doses on the 3rd, 7th, 14th, and 28th days. They should also get a shot of RabiesImmune Globulin at the same time as the first dose. This gives immediate protection. A person who has been previously vaccinated should get 2 doses of rabies vaccine - one right away and anotheron the 3rd day. Rabies Immune Globulin is not needed. Once a physician decides a patient needs to be started on post exposure therapy the following doses arerecommended for both the rabies vaccine and immune globulin. Rabies Vaccine
Adult Dose Rabies, Post-exposure; Prophylaxis: (not previously vaccinated) 1 mL IM x 5 doses, one each on days 0, 3,7, 14 and 28 in conjunction with the administration of Human Rabies Immune Globulin (HRIG) on day 0;begin with the administration of HRIG 20 international units/kg IMRabies, Post-exposure; Prophylaxis: (previously vaccinated) 1 mL IM x 2 doses, one each on day 0 and 3(HRIG should not be given)
Pediatric Dose Rabies, Post-exposure; Prophylaxis: (not previously vaccinated) 1 mL IM x 5 doses, one each on days 0, 3,7, 14 and 28 in conjunction with the administration of Human Rabies Immune Globulin (HRIG) on day 0;begin with the administration of HRIG 20 international units/kg IMRabies, Post-exposure; Prophylaxis: (previously vaccinated) 1 mL IM x 2 doses, one each on day 0 and 3(HRIG should not be given)
Administration GENERAL INFORMATION: (injection) for IM use only; do not inject intravascularly, SUBQ orintradermallyIM: adults and children; administer into the deltoid muscleIM: infants and small children; administer into the anterolateral zone of the thighIM: avoid gluteal area due to reduced antibody formation
Rabies Immune Globulin
Adult Dose Rabies, Post exposure; Prophylaxis: 20 international units/kg IM for 1 dose in combination with Rabiesvaccine
Pediatric Dose Rabies, Post exposure; Prophylaxis: 20 international units/kg IM for 1 dose in combination with Rabiesvaccine
Administration IM: if possible, infiltrate the full dose in the area around and into the wound; give remainder IM distantfrom vaccine administrationIM: do not mix in same syringe as vaccineIM: do not administer in the gluteal area; results in lower antibody titers
RSV BronchiolitisDeep suctioning by respiratory therapist IV 0.9NS 20mL/kg bolus -insensible losses -poor intake due to congestion Nebulized Epinephrine (0.5 mL of racemic epi OR 5mL of 1:1000 epi)
-Standard of care is to observe for 3 hours after epi neb because some patients have recurrence (debatable)-Racemic epi is more expensive and 1:1000 epi works just as well-Dosing recommendations as above- bur remember any excess just goes out to the environment anyways.-Closely monitor patients with severe left ventricular outflow obstruction (IHSS, AS, etc). Nebulized epiis relatively contraindicated in these patients.-Strongly consider admission if repeated doses of epi are required
-Note: Steroids and albuterol not proven to be helpful in RSV bronchiolitis. A trial of albuterol is reasonable incase there is a bronchospastic component and may be discontinued if the child fails to show a response
Seizure-Adult Ativan 0.1mg/kg IV @ 2mg/min IV up to 10mg IV is benzodiazepine of choice -Ativan preferred over Valium, as has longer effect
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
27 of 46 9/15/11 3:24 PM

-May give Versed 5mg IM if no IV access -If this is ineffective then: Phenytoin (Dilantin) 10-15mg/kg IV @ 50mg/min (25mg/min in cardiac pt and 1mg/kg/min peds)
-pH of 13 may cause big problems if extravasates, give slowly and must be diluted -Must give while pt on monitors (may prolong QRS) Fosphenytoin (Cerebyx) 15-20 mg PE/kg IV @ 150mg/min -Use when have no IV access to give phenytoin
-Used instead of phenytoin as can be administered more rapidly as no propylene glycol-May give up to 30cc IM as is water soluble-May repeat up to 30mg/kg max dose-If either phenytoin or fosphenytoin ineffective then:
Phenobarbital 20mg/kg @ 100mg/min -May repeat up to 30mg/kg -May cause hypotension and depressed respirations
Sepsis-Be familiar with ACMC Early Goal Directed Therapy (EGDT) Protocol for sepsis -Start central line above the diaphragm (IJ or subclavian) if SBP <90 mmHg (after IVF bolus) or lactate >4mmol/L
-Lactate is a better indicator of global tissue hypoxia than blood pressure -Experts advocate sending more serum lactates (available on blood gas)
-IV fluids à until CVP 8-12mmHg -Norepinephrine or dopamine first (make epinephrine alternative agent) à until MAP > 65. (MAP is inparentheses on the monitor) -Hydrocortisone 100mg IV x 1 -Recommended if not responsive to fluids and pressors
-Some give to all patients receiving IVF with the logic that in the stressed state the adrenals maynot be producing enough steroids-Requires random cortisol draw prior to administration (for stim test). May use 4mg decadroninstead which does not alter the stim test
-Packed Red Blood Cells (PRBC) à if SVO2 <70% AND Hct <30%
-SVO2 is the oxygen saturation from the blood drawn from the central line-Ask respiratory therapist to perform this
-Dobutamine if SVO2 <70% -Ventilator settings: -6cc/kg tidal volume -Respiratory acidosis is okay (permissive hypercapnia) -Peak inspiratory pressures <25-30 cm H2O
STD’s and Genital InfectionsBV: Flagyl 500mg PO bid x 7d OR Clinda cream 2% intravag qhs x 7d
OR Metrogel intravag bid x 5d OR Clindamycin 300mg PO bid x 7d
*If pregnant tx is the same but do not use Clinda cream (teratogenic) *Note: 2gm single dose Flagyl not as effective for BV Candidiasis: Diflucan 150mg PO x 1 (easiest, but can’t use in pregnancy) -May also use various creams and suppositories (treat for 7 days if pregnant) Chlamydia: Azithromycin 1g OR Doxy 100mg BID x 7d -Also treat for gonococcal infection, as these diseases frequently co-exist Gonococcal: Rocephin 125mg IM OR Azithromycin 2grams PO -Also treat for chlamydial infection, as these diseases frequently co-exist HSV (genital, first clinical episode): Valacyclovir (Valtrex) 1000mg PO bid x 10days OR Famciclovir (Famvir)250mg PO tid x 7-10 days OR Acyclovir 400mg PO tid x 7-10d -Note: Valtrex and Famvir not on ACMC formulary; only acyclovir HSV (recurrent infection): Valacyclovir 500mg PO bid x 3 days OR Famciclovir 125mg PO bid x 3 days OR
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
28 of 46 9/15/11 3:24 PM

Acyclovir 400mg PO tid x 5d -Note: Valtrex and Famvir not on ACMC formulary; only acyclovir PID (outpt): Rocephin 250mg IM PLUS [Doxy 100mg bid x 14d +/- Flagyl 500mg bid x14d] PID (inpt): [Cefoxitin] PLUS [Doxy 100mg IV bid OR Azithro 500mg IV] Trichomoniasis: Flagyl 2g PO single dose OR Flagyl 500mg PO bid x 7d
ToxicologyAlmost every pt with known or suspected ingestion needs: EKG/PA7/uhcg/APAP/ASA-EKG to assess QRS and QT intervals and associated ingestions
-uhcg for all females so can provide genetic counseling referral if pregnant -PA7 to rule out an anion gap acidosis and associated ingestions -APAP and ASA to rule out associated deadly and potentially treatable ingestions
-APAP is always obtained, as initially overdose is asymptomatic and treatable-Some argue that normal vitals and exam r/o a clinically significant ASA OD
-UDS is expensive, insensitive for many ingestants and almost never helps ED pt mgmt Remember the ABCDE’s of toxicology:
-Antidotes (e.g. NAC, folate) and Alter Absorption (e.g. Activated Charcoal)-Basics (the real ABCs)-Change metabolism (e.g. fomepizole, ethanol)-Distribute differently (e.g. oxygen)-Enhance Elimination (e.g. diuresis, dialysis, hemoperfusion)
Gastric lavage rarely used, consider for lethal ingestions within 60min of ingestion Activated Charcoal 1g/kg PO OR may give in ratio 10mg AC: 1mg ingested substance -Usual adult dose is 50g PO (combined with sorbitol in pre-mixed bottles) -Administer repeat dosages without sorbitol or may cause electrolyte abnormalities -In practice, given to most awake patients with known ingestion
-No studies have ever proven decreased mortality rate with AC
Acetylcysteine (Acetadote)
Mechanism of Action:
As an acetaminophen antidote, acetylcysteine increases the amount of glutathione in the liver, as well as, act as a glutathionesubstitute. Glutathione binds to and aids in the elimination of acetaminophen metabolites. In an acetaminophen overdose, endogenousglutathione is saturated, allowing hepatotoxic metabolites to accumulate; acetylcysteine increases elimination of these metabolites. Dose:Adult and Pediatric:
- Intravenous (IV)o Loading dose: 150mg/kg in 250mL of D5W over 60 minuteso Maintenance doses:
§ 50mg/kg in 500mL of D5W over 4 hours x 1 dose then§ 100mg/kg in 1000mL of D5W over 16 hours x 1 dose.
- Oralo Loading dose: 140mg/kgo Maintenance dose: 70mg/kg every 4 hours for 17 doses
Adjustments:For patients <40 kg or fluid restricted:
- Loading Dose (IV):o 30 kg: 100 mL D5W + 22.5 mL acetylcysteine; 25 kg: 100 mL D5W + 18.75 mL acetylcysteine; 20 kg: 60 mL
D5W + 15 mL acetylcysteine; 15 kg: 45 mL D5W + 11.25 mL acetylcysteine; 10 kg: 30 mL D5W + 7.5 mLacetylcysteine.
- Second Dose (IV):o 30 kg: 250 mL D5W + 7.5 mL acetylcysteine; 25 kg: 250 mL D5W + 6.25 mL acetylcysteine; 20 kg: 140 mL D5W
+ 5 mL acetylcysteine; 15 kg: 105 mL D5W + 3.75 mL acetylcysteine; 10 kg: 70 mL D5W + 2.5 mL acetylcysteine.- Third Dose (IV):
o 30 kg: 500 mL D5W + 15 mL acetylcysteine; 25 kg: 500 mL D5W + 12.5 mL acetylcysteine; 20 kg: 280 mL D5W +10 mL acetylcysteine; 15 kg: 210 mL D5W + 7.5 mL acetylcysteine; 10 kg: 140 mL D5W + 5 mL acetylcysteine.
How supplied:
- Injection: 200 mg/mL (30 mL)- Inhalation/oral: 100 mg/mL (4 mL, 10 mL, 30mL); 200 mg/mL (4 mL, 10 mL, 30 mL)- Oral: capsule, extended release: 500 mg; tablet: 500 mg
Contraindications:Hypersensitivity to acetylcysteine
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
29 of 46 9/15/11 3:24 PM

Precautions:
- Bronchospasm may occur, use with caution in asthma and history of anaphylaxis.- Use appropriate dose adjustment in patients with fluid restrictions and patients <40 kg.
Monitoring Parameters:
- Acetaminophen levels and overdose (hepatic and renal function, glucose, electrolytes)- Fluid status and anaphylactic reactions
Adverse Effects:
- Anaphylactoid reaction (with IV)- Hypotension- Urticaria/rash- Nausea/Vomiting- Bronchospasm
Drug Interactions: None significantPregnancy Category: B
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
30 of 46 9/15/11 3:24 PM

Atropine Mechanism of Action: Atropine is a muscarinic receptor antagonist. It prevents the binding of acetylcholine at sites such as secretory glands, smoothand cardiac muscle, and the central nervous system. As such, it can be used for an anticholinesterase overdose, which causes anaccumulation of acetylcholine. Dose:Adult
- IV: 2-4 mg, then 2 mg every 5-10 minutes until cholinergic symptoms resolve.
Pediatric- IV/IM: 1 mg, then 0.5-1 mg every 5-10 minutes until cholinergic symptoms resolve.
Adjustments:No adjustments necessary Administration:Administer undiluted IV injection rapidly to prevent paradoxical bradycardia How supplied:Injection: 0.05mg/mL (5 mL), 0.1mg/mL (5 mL, 10 mL), 0.4mg/mL (0.5 mL, 1 mL, 20 mL),0.5 mg/mL (1 mL), 1 mg/mL (1 mL) Contraindications:
- Hypersensitivity to atropine or anticholinergics- Narrow-angle glaucoma- Reflux esophagitis- Obstructive GI disease or uropathy- Ulcerative colitis or toxic megacolon- Unstable cardiovascular status in acute hemorrhage or thyrotoxicosis- Paralytic ileus or intestinal atony- Myasthenia gravis
Precautions:
- Elderly may require lower doses and experience more adverse effects.- Use with caution in hyperthyroidism, coronary heart disease, acute MI, CHF, tachyrhythmia, tachycardia, HTN, or prostatic
hypertrophy- May cause symptoms of heat exhaustion- May cause neuromuscular blockade
Monitoring Parameters:
- Heart rate- Blood pressure- EKG- Resolution of cholinergic symptoms
Adverse Effects:
- Arrhythmia- Tachycardia- Hypotension- Constipation- Urinary retention- Blurry vision
Drug Interactions:- Incompatible with IV administration of norephinephrine or sodium bicarbonate. Pregnancy Category:C
Calcium disodium edetate (Calcium Disodium Versenate) Mechanism of Action:
Calcium disodium edetate binds and chelates to lead in the plasma; the complex is excreted in the urine. This creates aconcentration gradient that draws lead from tissue to the plasma which again can be chelated and excreted. Dose:Adult and Pediatric:
- Intramuscularly (IM)o 1 g/m2/day in divided doses every 8-12 hours x 5 days, hold for 2-4 days then repeat as needed.
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
31 of 46 9/15/11 3:24 PM

- Intravenously (IV)o 1 g/m2/day IV infusion over 8-12 hr x 5 days, hold for 2-4 days then repeat as needed. Maximum dose 75
mg/kg/day.
Adjustments:Dose with impaired renal function:
- SCr 2-3 mg/dL: 500 mg/m2 every 24 h x 5 days.- SCr 3-4 mg/dL: 500 mg/m2 every 48 h x 3 doses- SCr > 4 mg/dL: 500 mg/m2 once weekly
Administration:
- To avoid pain with IM administration, give 1 mL of 1% lidocaine or procaine per mL of calcium disodium edetate.- For IV administration, dilute calcium disodium edetate to a concentration of less than 0.5% in D5W or NS (i.e. 5 mL of
calcium disodium edetate (1 g) in 250-500 mL of D5W or NS)
How supplied:- Injection solution: 200 mg/mL (5 mL)
Contraindications:
- Severe renal failure or anuria- Hepatitis
Precautions:- In patients with lead encephalopathy or cerebral edema, increased intracranial pressure may be experienced with IV
administration; the preferred route for these patients is IM.- Ensure adequate hydration and urine flow during administration- Discontinue therapy if signs of renal dysfunction appear.
Monitoring Parameters:
- Renal function (BUN, SCr, urinalysis)- ECG- Blood and urine lead concentrations.
Adverse Effects:
- Pain at injection site- N/V- Headache- Hypotension- Nephrotoxicity- Thrombophlebitis
Drug Interactions:- IV administration incompatible with LR, amphotericin B, or hydralazine. Pregnancy Category: B
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
32 of 46 9/15/11 3:24 PM

Deferoxamine (Desferal)
Mechanism of Action: Deferoxamine is chelates and binds to ferric iron to form ferrioxamine, which is excreted in the urine. Dose:Adult:
- Acute Iron toxicity:o IV/ IM: 1 g loading dose then 500 mg every 4 hours for up to 2 doses. May give additional 500mg every 4-12 hours if
needed. Maximum dose 6 g/day. - Chronic Iron toxicity:
o IV/IM: 500-1000 mg/day IM and 2 g given IV for each unit of blood transfused. Maximum 6 g/dayo SC: 1-2 g infused over 8-12 hours.
Pediatric:
- Acute Iron toxicity:o IM: 90mg/kg/dose every 8 hours. Maximum 6g/dayo IV: 15mg/kg/hour. Maximum 6g/day
- Chronic Iron toxicity:o SC: 20-40mg/kg/day infused over 8-12 hours. Maximum 1-2g/day.
Adjustments:Renal Impairment: for CrCl <10 mL/min give 50% of dose. Administration:
- For IM, reconstitute with sterile water for a concentration of 250 mg/mL- For IV, dilute and administer reconstituted deferoxamine with D5W, LR, or NS.- Infuse IV deferoxamine at a rate of ≤15mg/kg/hour at a maximum rate of 125mg/hour.
How supplied:Injection powder for reconstitution: 500mg, 2 g. Contraindications:
- Hypersensitivity to deferoxamine- Primary hemochromatosis- Anuria
Precautions:
- Increased susceptibility to Yersinia enterocolitica, Yersinia pseudotuberculosis, mucormycosis- Visual and hearing disturbance may occur with prolonged use- High doses may cause acute respiratory distress syndrome (ARDS)
Monitoring Parameters:
- Serum Iron- Respiration with high doses- Reduction in toxicity symptoms
Adverse Effects:
- Flushing- Hypotension- Injection site reaction- N/V- ARDS
Drug Interactions:
- No significant drug interactionsPregnancy Category: CNote: The preferred route of administration is IM, unless the patient is in shock.
Digoxin Immune Fab (Digibind) Mechanism of Action: Digoxin immune antigen-binding fragments (Fab) are antibodies that bind to digoxin in the plasma; the complex is thenexcreted in the urine. The clearance of digoxin from the plasma creates a concentration gradient that draws tissue-bound digoxin into theplasma, which also binds to digoxin immune Fab. Dose:Adult:
- Acute digoxin ingestion toxicity:o Empirically: 20 vials of Digibind in 2 divided doseso If amount of digoxin ingested is known:
§ Number of Digibind vials to use = [(mg of digoxin ingested) x (bioavailability)] / 0.5§ Bioavailability: 0.8 for 0.25mg tablets; 1 for 0.2 mg Lanoxicaps
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
33 of 46 9/15/11 3:24 PM

- Chronic digoxin ingestion toxicity:o Empirically: 6 vials of Digibind.o Based on serum digoxin levels:
§ Number of Digibind vials to use= [(level in ng/mL) x (weight in kg)]/ 100Pediatric:
- Acute digoxin ingestion toxicity:o Refer to adult dose
- Chronic digoxin ingestion toxicity:o Empirically: If weight ≤20 kg then 1 vial of Digibind, if >20 kg refer to adult doseo Based on serum digoxin levels:
§ Refer to adult dose
Administration:- Reconstitute with 4 mL of sterile water- Infuse over 30 minutes with a 0.22 micron filter. Dilute in 50-100ml NS
How supplied:- Injection powder for reconstitution: 38mg, 40mg Contraindications:No known contraindications
Precautions:- Allergy to sheep products or papaya extract- Hypokalemia may be worsened- Renal failure as excretion of Digibind-digoxin complex is decreased- Worsening in heart failure
Monitoring Parameters:
- Potassium- EKG
Adverse Effects:
- CHF exacerbation- Hypotension- Hypokalemia- Fever
Drug Interactions: No known drug interactionsPregnancy Category: CNote: Serum digoxin levels may be falsely elevated; monitoring of levels is not recommended.
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
34 of 46 9/15/11 3:24 PM

Generic Name (Trade Name): Dimercaprol (Bal In Oil) MOA/Description: Heavy Metal Chelator; gold, lead, arsenic Adult Dose: 3 mg/kg IM every 4 hr-6 hr for 2 days, then every 12hr
for 7 - 10 days or recovery Pediatric Dose: Same as adult Dose Adjustment:
Renal: use at a reduced dosage with extreme caution, or discontinue, in patients developing acute renal insufficiency duringtherapyHepatic: contraindicated with hepatic insufficiency
Administration: IM How Supplied: Intramuscular Oil: 10 % Contraindications: Hepatic insufficiency Precautions: Potentially a nephrotoxic drug, keep urine alkaline to protect kidneys, use with caution in patients with oliguria or GPD insufficiency Monitoring Parameters: decreased symptoms of toxicity, reduced concentrations of toxic agents blood pressure, heart rate renalfunction Adverse Reactions: CommonCardiovascular: Tightness sensation, Chest, limbs, jaw, abdomenGastrointestinal: Nausea, VomitingNeurologic: Headache, Paresthesia, TremorOphthalmic: Blepharospasm, Conjunctivitis, Finding of lacrimation SeriousCardiovascular: Hypertension (frequent), Pulse fast (frequent) Drug Interactions: Toxic complexes with iron, cadnium, selenium, or uranium Pregnancy Category: C
Flumazenil (Romazicon®)
Indications: Benzodiazepine toxicity, sedation reversalMechanism of Action: Competitively inhibits the activity at the benzodiazepine (BZD) recognition site on the GABA/BZD receptorcomplex Dosing:- Adult
o BZD Overdose:§ Initial: 0.2 mg IV over 30 s (if desired response not obtained after additional 30 s, give dose of 0.3 mg IV
over 30 s). Further doses of 0.5 mg IV over 30 s may be given at 1-min intervals if needed to MAX totaldose of 3 mg.
· Note: Patients with only partial response to 3 mg may require additional slow titration to a total doseof 5 mg. If no response 5 min after receiving total dose of 5 mg, overdose is unlikely to be BZD andfurther tx with flumazenil will not help
- Pediatric (> 1 year old)o 0.01 mg/kg (up to 0.2 mg) IV over 15 s; (if desired response not obtained after additional 45 s) further injections of
0.01 mg/kg may be repeated at 1-min intervals, as needed up to 4 times). Maximum total dose: 0.05 mg/kg or 1 mg.
Dose Adjustments:- Renal impairment: none necessary- Hepatic impairment: Initial dose for initial reversal is not changed; however, subsequent doses should be reduced in amount or
frequency Administration:- Administer in freely-running IV into large vein. - Administer as a series of small injections and not as a single bolus dose- Compatible with D5W, LR, NS- Stable for 24 hours if drawn into a syringe or mixed with solutions
How Supplied: IV solution: 0.1 mg/mL Contraindications:- Hypersensitivity to flumazenil, BZDs- Patients given BZDs for control of life-threatening conditions (eg, control of intracranial pressure or status epilecticus)- Patients showing signs of serious cyclic-antidepressant overdosage
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
35 of 46 9/15/11 3:24 PM

Precautions:- Drug and alcohol dependent patients- History of long-term BZD abuse- If neuromuscular blocking agents are used, do not use flumazenil until the effects of neuromuscular blockade is fully reversed- Liver disease- May induce panic attacks in patients with a h/o panic disorder- Patients with head injuries- Does not reduce the risks associated with the use of large doses of BZDs- Does not reverse respiratory depression/hypoventilation Monitoring Parameters: monitor pts for return of sedation or respiratory depression Adverse Reactions:
- Common:o Diaphoresiso Injection site paino Dizziness, HAo Blurred visiono Agitation, Anxiety
- Serious:o Cardiac dysrhythmiao Seizure
Drug Interactions: Non-BZD Hypnotics (zaleplon, zolpidem, zopiclone) Pregnancy Category: C
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
36 of 46 9/15/11 3:24 PM

Fomepizole (Antizol®)
Indication: Ethylene glycol poisoningMechanism of Action: Competitive inhibitor of alcohol dehydrogenase, an enzyme which catalyzes the metabolism of ethanol, ethyleneglycol and methanol to their toxic metabolites Dosing:
- Adult:o Loading dose of 15 mg/kg, followed by 10 mg/kg q12h x 4 doses, then 15 mg/kg q12h until ethylene glycol level <
20 mg/dL and patient is asymptomatic with normal pH- Pediatric: Safety and efficacy have not been established in pediatric patients
Dose Adjustments:- Renal Impairment
o Beginning of hemodialysis (HD):§ < 6 hours since last fomepizole dose: Do not administer dose§ ≥ 6 hours since last fomepizole dose: Administer next scheduled dose
o During HD: Dose q4ho Following HD (based on time between last dose and the end of HD):
§ < 1 hour: Do not administer dose at end of hemodialysis§ 1-3 hours: Administer ½ of next scheduled dose§ > 3 hours: Administer next scheduled dose
o Maintenance dose when off HD: Give next scheduled dose 12 hours from last dose administered Administration:
- Do not administer undiluted due to venous irritation. Mix into at least 100 ml of sterile NS or D5W.- All doses should be given as a slow 30-minute IV infusion- Stable for 24 hours after dilution
How Supplied:- IV solution, 1 g/ml
Contraindications:- Hypersensitivity to fomepizole or other pyrazoles
Precautions:- Do not give undiluted or by bolus injection- Liver disease (fomepizole primarily metabolized in liver)- Dosage adjustment required in HD; renal impairment
Monitoring Parameters:
- Plasma/urine ethylene glycol or methanol concentrations- Urinary oxalate crystals- Plasma/urine osmolality- Renal/hepatic function- Serum electrolytes- Arterial blood gases (ABGs)- Anion and osmolar gaps- WBC- ECG/EEG
Adverse Reactions:
- Common:
o Hypotensiono Hypertriglyceridemiao N/Vo HAo Dizzinesso Seizureo Anxiety
- Serious: Disseminated intravascular coagulation (rare), Anuria
Drug Interactions: Ethanol
Pregnancy Category: C
Glucagon (GlucaGen®, Glucagon®)
Indications: β-blocker toxicity and CCB (verapamil) toxicity, severe hypoglycemia Mechanism of Action:
- Stimulates adenylate cyclase to produce increased cAMP, which promotes hepatic glycogenolysis and gluconeogenesis →increases blood glucose levels
- Positive inotropic and chronotropic effect on the heart
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
37 of 46 9/15/11 3:24 PM

Dosing (for β-blocker/CCB toxicity):
- Adult:o 5-10 mg IV infusion over 1 minute followed by an infusion of 1-10 mg/hro Alternative for β-blocker OD: 3-10 mg or initially 0.5-5 mg bolus followed by continuous infusion of 1-5 mg/hr
Dose Adjustments: none Administration:
- Can be given IM, IV, or SubQ- Reconstitute with diluent to max concentration of 1 mg/mL- Use immediately; solution should be clear & water-like- 1 unit = 1 mg- IV: Inject at a rate not exceeding 1 mg/min. May be administered through line running D5W or given at same time as a bolus
of dextrose How Supplied:
- Injection powder for solution: 1 mg, 10 mg Contraindications:
- Hypersensitivity to glucagons- Pheochromocytoma
Precautions:
- Malnutrition- Adrenal insufficiency- Chronic hypoglycemia- History of pheochromocytoma- Insulinoma- Allergic reactions
Monitoring Parameters:
- BP- Heart rate- Blood glucose
Adverse Reactions:
- Rash- N/V- HTN- Tachycardia
Drug Interactions:
- Anticoagulants (warfarin) – may enhance anticoagulant effect Pregnancy Category: B
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
38 of 46 9/15/11 3:24 PM

Methylene Blue (Urolene Blue®)
Indication: Drug-induced methemoglobinemia Mechanism of Action:- Weak germicide in low concentrations- Accelerates the conversion of methemoglobin to hemoglobin- In high concentrations, it converts ferrous iron of reduced hemoglobin to ferric iron to form methemoglobin Dosing:- Adult & Pediatric:
o 1-2 mg/kg or 25-50 mg/m2 IV over several minutes; may be repeated in 1 hr if necessary Dose Adjustments:- Severe renal impairment: adjustment should be considered (specific guidelines not available) Administration:- Administer undiluted by direct IV injection slowly over several minutes.- Do not inject SubQ or intrathecally How Supplied:- IV solution: 10 mg/ml- Oral tablet: 65 mg- Topical solution: 2% Contraindications:
- Hypersensitivity to methylene blue- Intraspinal injection- Methemoglobinemia in cyanide poisoning
Precautions:- Use with caution in young patients and in patients with G6PD deficiency (continued use can cause profound anemia)- Renal impairment Monitoring Parameters:
- Arterial blood gases- Blood pressure- CBC- Methemoglobin levels- Renal function (SCr/BUN)- Serum bilirubin (unconjugated)
Adverse Reactions:- Hypertension/hypotension- Cardiac dysrhythmia- Dizziness- Confusion- N/V/D- Abdominal pain- Hemolytic anemia- Diaphoresis- Skin/urine discoloration Drug Interactions: none clinically significant Pregnancy Category: C
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
39 of 46 9/15/11 3:24 PM

Naloxone (Narcan®)
Indication: Opiate overdose Mechanism of Action: Pure opioid antagonist that competes and displaces narcotics at opioid receptor sites (mu, kappa, sigma).Greatest affinity for the mu receptor. Dosing:- Adult:
o IV: 0.4-2 mg q2-3 minutes prn; may repeat doses q20-60 minuteso Continuous IV infusion: Loading dose of 0.005 mg/kg, followed by 0.0025 mg/kg/hr
- Pediatric:o Birth to 5 years or < 20 kg: 0.1 mg/kg IV; repeat q2-3 minutes prn; may need to repeat doses Q20-60 minuteso > 5 years or ≥ 20 kg: 2 mg/dose; if no response, repeat q2-3 minutes; may need to repeat doses Q20-60 minutes
Dose Adjustments: none needed. Use with caution in patients with hepatic impairment. Administration:- May be administered IV (preferred), IM, SubQ- IV continuous infusion: dilute with NS or D5W to a concentration of 0.004 mg/mL (2 mg in 500 mL). Rate titrated to patient
effect.- IV push: Administer over 30 seconds as undiluted preparation How Supplied:- Injection solution: 0.02 mg/mL, 0.4 mg/mL, 1 mg/mL Contraindications: hypersensitivity to naloxone Precautions:
- Pre-existing cardiovascular disease- Concurrent cardiotoxic drugs- Known or suspected physical dependence on opioids- Neonates- IM or SubQ injections in patients who are hypotensive or have impaired peripheral circulation
Monitoring Parameters:
- Reduction in opioid drug effects (i.e., respiratory depression)- BP, HR, RR- S/sxs of opioid withdrawal
Adverse Reactions:
- Cardiac dysrhythmia, ventricular fibrillation- Hypertension/hypotension- Hepatotoxicity- Pulmonary edema- Opioid withdrawal
Drug Interactions:
- Opiate agonists- Clonidine (probable)- Yohimbine
Pregnancy Category: C
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
40 of 46 9/15/11 3:24 PM

Octreotide (Sandostatin®) Indication: Oral sulfonylurea overdose Mechanism of Action: Inhibits growth hormone, glucagon, and insulin more effectively than the natural hormone, somatostatin Dosing:- Adult (optimal dosage has not been established):
o 100-450 mcg/day SubQ given in 2-3 divided doseso Continuous SubQ infusion:300-1500 mgc/day
- Pediatric (optimal dosage has not been established):o 1-10 mcg/kg/day SubQ
Dose Adjustments:- Elderly: Dose adjustment may be necessary (elimination t1/2 is increased by 46% and clearance is decreased by 26%)- Renal Impairment: severe renal failure requiring dialysis—clearance is reduced by ~50%; specific dosing guidelines not
available Administration:- IV push: give over 3 minutes- IV infusion: dilute in NS or D5W to volume of 50-200 mL; infuse over 15-30 min How Supplied:- Injection powder for solution: 10 mg, 20 mg, 30 mg- Injection solution: 50 mcg/mL, 100 mcg/mL, 200 mcg/mL, 500 mcg/mL, 1000 mcg/mL Contraindications: Hypersensitivity to octreotide Precautions:
- Altered absorption of dietary fats- Biliary tract abnormalities- Decreased vitamin B12 levels- Thyroid abnormalities- Diabetes mellitus- Renal failure
Monitoring Parameters:
- Symptomatic improvement- Thyroid function- Blood glucose- ECG
Adverse Reactions:
- Common:o Injection site paino Hyper-/hypoglycemiao Hypothyroidismo Abdominal discomforto Cholelithiasiso N/V/Do Dizziness, HA
- Serious:o Cardiac dysrhythmia, CHF, bradycardia, HTN
Drug Interactions:
- Antidiabetic agents- Calcium channel blockers- β-agonists, β-blockers- Class IA, III antiarrhythmics- Diuretics- Local anesthetics- Opiate agaonists- Tricyclic antidepressants
Pregnancy Category: B
Penicillamine (Cuprimine, Depen)
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
41 of 46 9/15/11 3:24 PM

MOA/Description: Heavy Metal Chelator; Copper, Lead Adult Dose: 250mg – 500mg/dose every 8 – 12hr, continue until blood level is <15 ug/dL Pediatric Dose: 25 – 35mg/kg/day in 3 to 4 divided doses; initiating treatment at 25% of dose and gradually increasing tp full dose over
2 – 3 weeks may minimize adverse reactions Dose Adjustment: Hepatic: 250mg/day tgo start, increase by 250mg every 2 weeks up to a maintenance dose of 1g/day, in 4 divided doses Renal: Clcr<50 mL/min: Avoid use Administration: Give on empty stomach, 1 hour before meals and at bedtime How Supplied: Oral Capsule: 125 MG, 250 MG Oral Tablet: 250 MG Contraindications: breastfeeding, pregnancy, hypersensitivity to penicillamine products, patients with history or evidence ofrenal insufficiency Precautions: penicillamine should not be used in patients receiving concurrent gold therapy, antimalarial or cytotoxic drugs,oxyphenbutazone or phenylbutazone, possible cross-sensitivity in patients allergic to penicillin, renal dysfunction; avoid interruption oftherapy - may cause sensitivity reaction after resuming therapy Monitoring Parameters: urinalysis, WBC with differential, hemoglobin, direct platelet count, skin, lymph node, body temperature,liver function Adverse Reactions: CommonDermatologic: RashGastrointestinal: Disorder of taste, Epigastric pain,Nausea, VomitingHematologic: Myelosuppression SeriousDermatologic: PemphigusGastrointestinal: Oral lichenoid reactionHematologic: Agranulocytosis, Aplastic anemia, ThrombocytopeniaMusculoskeletal: Myasthenia gravisNeurologic: Peripheral motor neuropathy, Sensory neuropathyOphthalmic: Optic neuritisOtic: TinnitusRenal: Proteinuria, Renal glomerular disease, Renal vasculitis Drug Interactions:Increased effect of antimalarials, immunosuppresants, and phenylbutazoneDecreased digoxin levels may occur Pregnancy Category: D
Physostigmine MOA/Description: Cholinesterase Inhibitor Adult Dose: Anticholinergic drug overdose: 2 mg IV, no faster than 1 mg/min; dose may be repeated if no reversal has occurred or ifanticholinergic symptoms return Pediatric Dose: Anticholinergic drug overdose: 0.02 mg/kg IV, no faster than 0.5 mg/min; dose may be repeated in 20 minutes if noreversal has occurred or if anticholinergic symptoms return; maximum recommended dose is 2 mg Dose Adjustment: N/AAdministration: IV injection or IM; no faster than 1 mg/min in adults, no faster than 0.5 mg/min in children How Supplied: Injection solution, 1mg/ml in 2ml ampule Contraindications: asthma, cardiovascular disease, concomitant choline ester or depolarizing neuromuscular blocker use,diabetes, gangrene, hypersensitivity to physostigmine, mechanical obstruction of the intestine or urogenital tract Precautions: atropine sulfate injection should be available to reverse toxic effects of physostigmine injection; tricyclic antidepressantoverdose Monitoring Parameters: ECG, reversal of anticholinergic symptoms, symptoms of excessive sweating, salivation, emesis, urination,defecation; signs of cholinergic crisis Adverse Reactions: CommonDermatologic: DiaphoresisGastrointestinal: Diarrhea, Excessive salivation, Hyperperistalsis, Nausea and vomiting
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
42 of 46 9/15/11 3:24 PM

Ophthalmic: Finding of lacrimation, Miosis, Mydriasis SeriousCardiovascular: Bradyarrhythmia, Cardiac arrest, Cardiac dysrhythmia, Increased cardiac outputNeurologic: SeizureRespiratory: Bronchospasm, Dyspnea Drug Interactions: Succinylcholine, bethanecol Pregnancy Category: C
Phytonadione (Mephyton)
MOA/Description: Phytonadione is a vitamin which is necessary for the hepatic synthesis of prothrombin (factor II), proconvertin(factor VII), plasma thromboplastin component (factor IX), and Stuart factor (factor X, Fat soluble vitamin, Vitamin K Adult Dose: Drug action reversal, Anticoagulant: 1 to 10 mg ORAL/IV/SQ depending on degree of INR elevaion; oral ispreferred over SUBQ and IV Pediatric Dose: Hemorrhage of newborn: 1 mg SC or IM (SC route preferred) Hemorrhage of newborn; Prophylaxis: 0.5-1 mg SC/IMwithin 1 hr of birth, SC route is preferred Dose Adjustment: N/A Administration: ORAL: anticoagulant, drug action reversal; ORAL is preferred over SQ (response to SQ is less predictable andsometimes delayed compared to ORAL) and IV. Oral vitamin K is also predictably effective, safe and more convenient How Supplied: Injection Solution: 1 MG/0.5 ML, 10 MG/ML Oral Tablet: 0.1 MG, 5 MG, 100 MCG Contraindications: hypersensitivity to phytonadione products Precautions: liver disease; severe reactions, including fatalities, have occurred with IV and IM administration Monitoring Parameters: reduction in bleeding, PT Adverse Reactions: CommonDermatologic: Skin reaction - finding, IM SeriousImmunologic: Anaphylaxis, IV and IM use Drug Interactions: Anticoagulant effects warfarin are reversed by phytonadione Pregnancy Category: C
Pralidoxime (Protopam) MOA/Description: Nerve Gas Antidote; reactivates cholinesterase (mainly outside CNS) which was inactivated by organophosphatepesticides through phosphorylation Adult Dose: Anticholinesterase overdose: initial, 1-2 g IV, maintenance, 250 mg IV every five minutesOrganophosphate poisoning: initial,1-2 g in 100 mL NS IV infused over 15-30 min, repeat 1-2 g in 1 hour if muscle weakness persists Pediatric Dose: Organophosphate poisoning: 25-50 mg/kg IV; may repeat in 1-2hrs, then at 10-12hr intervals if necessary Dose Adjustment:Renal: dose should be reduced Administration: IV: infuse in 100 mL of NS over 15-30 min maximum rate of administration is 200 mg/min Can give IM or SQ if IV access not available How Supplied: Injection Powder for Solution: 1 GM Contraindications: hypersensitivity to pralidoxime Precautions: myasthenia gravis (may precipitate myasthenic crisis), renal impairment Monitoring Parameters: resolution of muscle weakness and respiratory depression, ECG Adverse Reactions: CommonGastrointestinal: NauseaNeurologic: Dizziness, HeadacheOphthalmic: Blurred visionRespiratory: Hyperventilation, Laryngeal spasm
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
43 of 46 9/15/11 3:24 PM

Drug Interactions: Use with aminophylline, morphine, theophylline, and succinylcholine in containdicated Pregnancy Category: C
Protamine MOA/Description: Heparin Antagonist; combines with strongly acidic heparin to form a stable complex salt neutralizing theanticoagulant activity of both drugs Adult Dose: 1 mg IV for every 100 units of heparin remaining in patient; if 30 minutes have elapsed since the injection of heparinone-half the dose may be sufficient; maximum 50 mg given over 10 minutesThe dose can be given as a loading dose of 25 to 50 mg by slow IV injection, with the rest of the calculated dose over 8 to 16 hours byintravenous infusion Pediatric Dose: safety and effectiveness in children have not been established Dose Adjustment: N/A Administration: administer by very slow intravenous injection over 10 minutes How Supplied: Intravenous Solution: 10 MG/ML Contraindications: hypersensitivity to protamine products Precautions: Rapid administration may cause severe hypotensive and anaphylactoid reactions; heparin rebound or bleeding has beenreported in cardiac surgery patients despite adequate neutralization of heparin with protamine; all of the following have been associatedwith an increased risk of hypersensitivity: hypersensitivity to fish, infertile or vasectomized men, and previous exposure to protamine Monitoring Parameters: coagulation test, aPTT, blood pressure, heart rate Adverse Reactions: CommonDermatologic: FlushingGastrointestinal: Nausea, VomitingRespiratory: Dyspnea SeriousCardiovascular: Bradyarrhythmia, HypotensionImmunologic: Anaphylactoid reaction, Circulatory collapse, capillary leak, noncardiogenic pulmonary edema, Anaphylaxis Drug Interactions: N/A Pregnancy Category: C
Sodium Nitrite, Sodium Thiosulfate, Amyl Nitrite (Cyanide Antidote Package) Mechanism of Action: Thiosulfate provides extra sulfur to increase the rate of activity of rhodanese, an enzyme that inactivates cyanide. Sodiumnitrite and amyl nitrite work by forming methemoglobin, which has a high affinity for cyanide. Cyanmethemoglobin, a nontoxiccompound, is formed and excreted in the urine. Dose:Adult:
- Crush 0.3 mL ampul of amyl nitrite and inhale vapor up to 30 seconds. Repeat every minute until IV sodium nitrite is infused.- Sodium Nitrite: 300mg IV- Sodium thiosulfate: infuse 12.5 g IV over 10 minutes- Repeat infusions of sodium nitrite and sodium thiosulfate at half the initial dose if needed
Pediatric:- Crush 0.3 mL ampul of amyl nitrite and inhale vapor up to 30 seconds. Repeat every minute until IV sodium nitrite is infused.- Sodium Nitrite: 6-8 mL/m2; maximum: 10 mL- Sodium thiosulfate: infuse 7 g/m2 over 10 minutes; maximum 12.5 g- Repeat infusions of sodium nitrite and sodium thiosulfate at half the initial dose if needed
Administration:
- Infuse sodium nitrite at a rate of 2.5-5 mL/min How supplied:Kit includes:
- Sodium nitrite 300 mg/10 mL injection (2)- Sodium thiosulfate 12.5g/50 mL injection (2)- Amyl nitrite 0.3 mL inhalant (12)- Syringes, stomach tube, tourniquet
Contraindications:
- Hypersensitivity to any component
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
44 of 46 9/15/11 3:24 PM
- Pregnancy due to amyl nitrite- Cerebral hemorrhage- Glaucoma- Recent head trauma
Precautions:
- Anemia- Hyperthyroidism- Hypotension- Recent MI
- Volume depletion
Monitoring Parameters:
- Blood pressure- Reduced cyanide poisoning- Pulse
Adverse Effects:
- Skin rash- Hypotension- Nausea/vomiting- Hemolytic anemia- Tachycardia-
Drug Interactions:- No significant drug interactions- Use caution with hypotensive agents
Pregnancy Category: C
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
45 of 46 9/15/11 3:24 PM

For suggested changes/feedback please contact:
Dr. Sudip Bose: [email protected]
Or
For any drug related questions or issues:
Dr. Rolla Sweis: Inhouse Pager: 3867/Long Range Pager: 708-727-2677
Christ EM: Intern Survival Guide http://christem.info/didactics/InternMedGuide/InternMedGuide.asp
46 of 46 9/15/11 3:24 PM