summer undergraduate research fellowship in nandaime, nicaragua
DESCRIPTION
The goal of this project was to use the Barrier Analysis Tool to identify the determinants that have been preventing 7-14 year olds in Nandaime, Nicaragua from brushing their teeth twice daily in order to increase their dental hygiene and prevent cavities. The Barrier Analysis Tool was used in the local public schools and clinics. My secondary goal was to teach the local “brigidistas” the Barrier Analysis Tool as well the approach of identifying why a given population is not doing/doing a behavior before implementing a health education program. After conducting 98 individual interviews and two focus groups, Perceived Susceptibility seems to be the most important barrier. 95% of students said they brushed their teeth though, so the reason for the high occurrence of cavities could be due to improper technique in brushing, inadequate time spent on brushing or improper care of primary teeth.TRANSCRIPT

Using the Barrier Analysis Tool to identify determinants that influence dental hygiene: A case study of 7-14 year olds in Nandaime, Nicaragua By Raj Sundar
In conjunction with Viva Nicaragua! and The Children’s Wellness Fund

1
Table of Contents
Abstract ........................................................................................................................................................ 2
Introduction .................................................................................................................................................. 2
Methods ........................................................................................................................................................ 3
Results........................................................................................................................................................... 4
Recommendations ....................................................................................................................................... 5
Appendix ....................................................................................................................................................... 6
Appendix A: Basic Questions ..................................................................................................................... 7
Appendix B: Perceived Susceptibility ........................................................................................................ 8
Appendix C: Perceived Severity .............................................................................................................. 10
Appendix D: Action Efficacy .................................................................................................................... 11
Appendix E: Perceived Social Acceptability ............................................................................................ 12
Appendix F: Self-Efficacy ......................................................................................................................... 14
Appendix G: Cues for Action ................................................................................................................... 15
Appendix H: Divine Will........................................................................................................................... 16
Appendix I: Positive Attributes of the Behavior ...................................................................................... 18
Appendix J: Prochaska’s Change Theory ................................................................................................. 19

2
Abstract
The goal of this project was to use the Barrier Analysis Tool to identify the determinants that have been preventing 7-14 year olds in Nandaime, Nicaragua from brushing their teeth twice daily in order to increase their dental hygiene and prevent cavities. The Barrier Analysis Tool was used in the local public schools and clinics. My secondary goal was to teach the local “brigidistas” the Barrier Analysis Tool as well the approach of identifying why a given population is not doing/doing a behavior before implementing a health education program. After conducting 98 individual interviews and two focus groups, Perceived Susceptibility seems to be the most important barrier. 95% of students said they brushed their teeth though, so the reason for the high occurrence of cavities could be due to improper technique in brushing, inadequate time spent on brushing or improper care of primary teeth.
Introduction
In the summer of 2010, I worked with Viva Nicaragua! in a Comparative Healthcare Internship. As I worked in clinics, hospitals and NGOs, I also had the opportunity to attend health education “charlas” in the communities. I was exposed to many different health education talks ranging from HIV/AIDS talks to hand washing talks, but even after countless talks, there seemed to be little behavior change on certain subjects like sexual behavior. Scientific literature has shown though that knowledge is not enough to change behavior because many people know what they should do but still do not do it. The Food for the Hungry suggests four important factors that need to be taken into account when creating health education activities:
1. If a person knows what he/she should do, it does NOT mean that he/she will do it. Other factors influence our decisions. Having knowledge about a behavior is only one factor. People often learn about a behavior long before they are willing to adopt it. 2. If a person wants to do a behavior, it does NOT mean that he/she will do it. Sometimes we are blocked and cannot do what we want to do and know we need to do (e.g., for lack of time, money). In addition, people often do not seek help from others (e.g., friends, health providers, God) to overcome a problem or change a habit. 3. Many times we try to increase the level of FEAR that a person has in order to get him/her to do a preventive action. However, sometimes the problem is too much rather than too little fear of the disease or problem. For example, we speak of the danger of diarrhea to convince a person to use the latrine. However, sometimes too much fear can keep a person from doing something. 4. Many of the actions that people engage in that improve their health are NOT necessarily done for health reasons. It is possible to encourage a person to do something that improves his/her health for reasons that are not directed at improving health (e.g., washing yourself with soap in order to smell good). We need to find reasons that motivate (or would motivate) people to do something that will improve their health (or well-being), even if the reason is not health-related (e.g., brushing your teeth in order to have good breath).
While some behavior change can be done with only knowledge education, there are other behaviors that have “determinants” that prevent someone from performing these behaviors. The Barrier Analysis Tool uses a series of questions in individual interviews and focus groups to identify why a target population is not doing/doing a certain behavior and to help create a health education program that effectively promotes and causes behavior change. The Barrier Analysis Tool attempts to identify eight potential determinants that can block people from taking an action by comparing the responses of people who do a behavior (the Doers) with those who do not (the Non-Doers). It is based on the Health

3
Belief Model and three other theories. The Health Belief model is a simple design that was created in the 1950s to increase the use of preventive services such as chest x-rays for tuberculosis and immunizations for influenza. Since then, it has also been used in other areas such as HIV/AIDS, cancer screening, and prenatal care in different cultural settings. The Health Belief Model focuses on six determinants: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues for action, and perceived self-efficacy. The Theory of Reasoned Action, Perception of Divine Will and Prochaska’s Change Theory (Appendix J) were integrated into this model to create the Barrier Analysis Tool analysis. Subsequently, the Barrier Tool Analysis has been used by Food for the Hungry in projects in Haiti, Kenya, and Bolivia to discover key barriers to behavior change regarding breastfeeding, other nutritional practices, latrine use, HIV/AIDS behaviors and other intervention areas.
Methods
Over the past 10 weeks, I conducted one-on-one individual interviews in Santa Ana, Casa De Piedra and Manchon and focus groups in Santa Ana and Manchon. Before the interviews were conducted, I received permission from the parents in reunions and, for the parents that did not attend the reunions, I sent permission forms home with children and collected them the following week. The interviews lasted about 15 minutes each and were conducted in a classroom with the help of brigidistas and teachers. Focus groups were conducted in Santa Ana and Manchon in the comedor and clinic, respectively. The focus group in Santa Ana consisted of about seven mothers and one father, and the focus group in Manchon consisted of eight to ten mothers. For both the individual interviews and focus groups, there were pre-formed questions. In the focus group, there was added flexibility, and I was able to get a richer understanding of each question and could diverge from the set of questions when something interesting was said. The eight determinants and the relevant questions used in my project were:
I. Basic Questions* a. Do you brush your teeth twice a day? b. Do you have a brush and toothpaste? 1. Perceived Susceptibility (Can I get the disease or could that problem happen to me?) a. Do you think that you could get cavities/caries? b. Do you think that you will have cavities caused by not brushing your teeth in the next few years? c. What are the diseases or problems that you could have if you do not brush your teeth? 2. Perceived Severity (Is the problem very serious?) a. How bad of a disease/problem is cavities? Would you say it is very bad, somewhat bad, average, or not bad at all? b. Is oral cavity a dangerous disease? c. Ask participants to rank a list of diseases or problems including some innocuous diseases, the disease or problem associated with the behavior you are studying, and some severe/fatal diseases Chronic Hiccups, Cavities, Cancer, AIDS/HIV** 3. Perceived Action Efficacy (Does the preventive action work?) a. When a person brushes his teeth, does that help avoid cavities? b. To what degree does brushing your teeth help prevent cavities? Does it help prevent it a little, somewhat, or a lot?
*Questions were only used in Santa Ana and Manchon **Questions were excluded from analysis because most students did not respond to the question

4
4. Perceived Social Acceptability (Is the preventive action socially acceptable?) a. Who do you think would object or disapprove if you brushed your teeth twice a day? b. Who (individual or groups) do you think would approve if you brushed your teeth twice a day? c. Which of these individuals or groups in either of the two questions above is most important to you? 5. Perceived Self-Efficacy (Is it easy to do, especially in terms of skills, access, time and money?) a. Would it be easy for you to brush your teeth twice a day? b. What makes it difficult or impossible for you to brush your teeth twice a day?** c. What makes it easier for you to brush your teeth twice a day?** 6. Cues for Action (Can I remember to do it?) a. Is it easy to remember to brush your teeth every time that you need to do it? b. Is it easy to remember the steps in brushing your teeth twice a day every time that you need to do it 7. Perception of Divine Will (Is it God’s will (or the gods’ will) that I (a) should not have the problem, or (b) that I overcome the problem?) a. Is it sometimes God’s (or the gods’) will that people/children get cavities? b. Why do some people get cavities and some people do not? c. Do people sometimes get cavities because of curses or other spiritual or supernatural causes? 8. Positive Attributes/Negative Attributes of the Behavior (What are the advantages and disadvantages of the behavior?) a. What do you see as the advantages or good things that would happen if you brushed your teeth twice a day? b. What are the things you like about brushing your teeth twice a day? c. What do you see as the disadvantages or bad things that would happen if you brushed your teeth twice a day?**
Results
I conducted 98 individual interviews in schools with 25 students in Santa Ana, 26 students in Casa de Piedra and 47 students in Manchon. The original Barrier Analysis Tool was designed to compare the behaviors of the Doer (children who brush their teeth) and the Non-Doer (children who do not brush their teeth). Unfortunately, as seen in Appendix A, 95% of the children interviewed said they brushed their teeth twice daily (unfortunate for my research but good for the community!). My goal was stymied by the fact that almost everybody said they brushed their teeth, so I was not able to arrive at statistically significant data to identify the determinants by comparing two sample populations. Whether they were lying or were in fact telling the truth cannot be verified. In both focus groups in Santa Ana and Manchon, the participants also said their children brushed their teeth, so there is evidence to believe they do in fact brush their teeth.
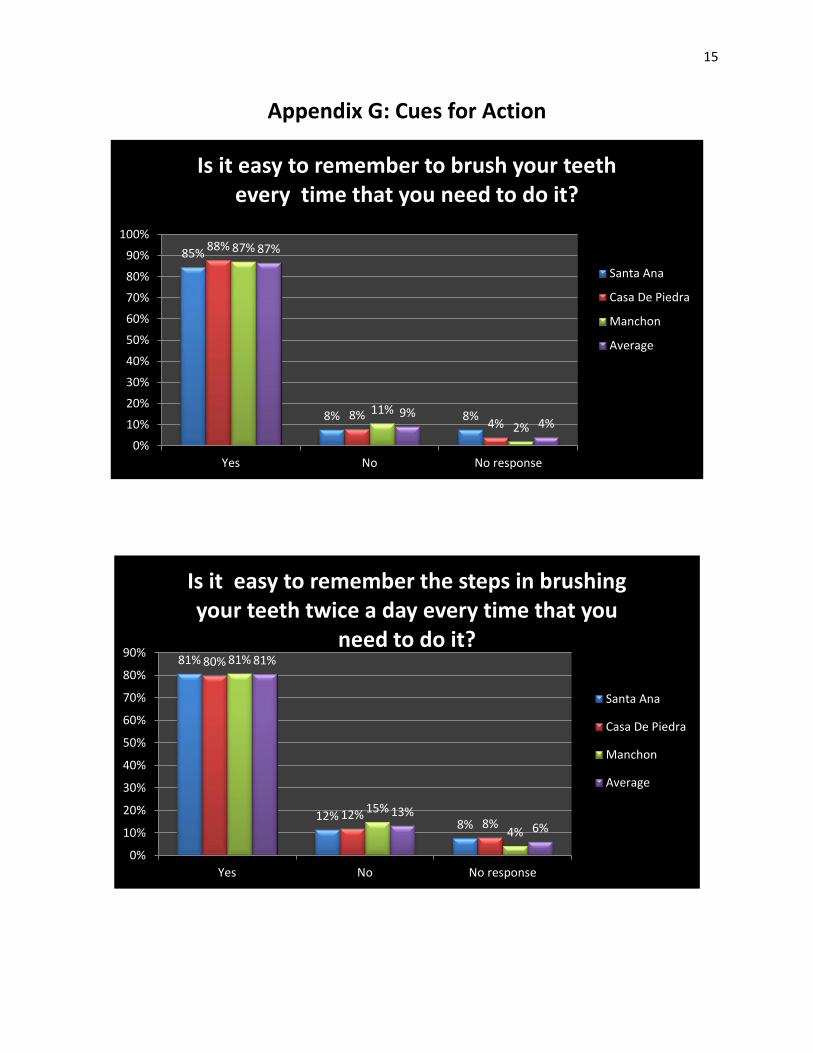
However, I can use the data as a survey of the population to determine what to focus on and emphasize in any future health education programs on dental hygiene, and it can also help identify why people are acquiring cavities even if they are brushing their teeth. Setting an arbitrary significance percentage at 70% for the data collected in individual interviews, we can identify the most important barriers. Subsequently, we can say Perceived Severity (Appendix C), Action Efficacy (Appendix D), Self-Efficacy (Appendix F), Cues for action (Appendix G) and Divine Will (Appendix H) were not the most important barriers. In other words, the children believe cavities is a serious disease, brushing prevents *Questions were only used in Santa Ana and Manchon **Questions were excluded from analysis because most students did not respond to the question

5
cavities, brushing is easy to do, can remember to do it and do not believe it’s God’s will that they obtain cavities.
With regards to Perceived Social Acceptability (Appendix E), I was surprised to find that many people like neighbors, grandparents and fathers told their children that they shouldn’t brush their teeth. Even though this is troubling, when asked which group of people is more important to them, the people who tell them not to brush their teeth or the people who tell them to brush their teeth, the children only chose the 1st group 5% of the time and decided not to brush their teeth. With regards to Positive Attributes of brushing teeth, there were a variety of answers from maintaining a fresh and clean breath to teeth not falling out (Appendix I). There were not enough answers to suggest that these reasons were a greater motivation to brush teeth than preventing cavities.
The most important barrier from the individual interviews seemed to be the Perceived Susceptibility (Appendix B). With their current brushing habits and oral hygiene, only 45% of the participants interviewed said they could get cavities. Many are under the impression that they cannot acquire cavities because they are brushing their teeth. If the promoted behavior of brushing teeth at least twice daily is performed, it raises the fundamental question of why children are still acquiring activities. The obvious hypothesis is that children are not brushing their teeth properly. In focus groups, I was able to discern that it does in fact stem from brushing improperly and for an inadequate amount of time. In the two focus groups conducted, the participants showed completely different techniques on brushing their teeth, and some of these techniques seemed to be ineffective at cleaning their teeth. Mothers in Manchon also admitted that children often brushed hurriedly. The problem is exacerbated by the use of water and salt rather than toothpaste for brushing. Although water and salt is seen as a viable alternative to toothpaste, the use of this alternative leads to a lack of fluoride in the diet. In studies, fluoride has shown to prevent plaque from dissolving tooth enamel and helps repair and re-mineralize teeth. Without fluoride, it is imperative that children and community members not only brush their teeth but brush their teeth properly. Another hypothesis is the improper care of primary teeth leads to cavities in permanent teeth. In both focus groups, participants said that they did not believe a cavity in primary teeth was serious and does not affect permanent teeth. Untreated tooth decay or gum disease can lead to infection that may affect the permanent teeth though. From the analysis of the results and the preceding explanation, these are the recommendations derived from the project:
Recommendations 1. Emphasize that brushing properly prevents cavities not just brushing. Currently, many children do not think they can get cavities believing their current habits are adequate (Perceived Susceptibility). 2. Teach proper techniques for brushing to all children and adults in the community. 3. Educate community members on the importance of brushing teeth for at least two minutes in order to adequately clean teeth and remove plaque. 4. Explain the importance of taking care of primary teeth because tooth decay and infection in primary teeth may affect permanent teeth. 5. Replace toothbrushes every 3 months (or at the very least every 6 months.) 6. Arrange for a professional cleaning by dentists or hygienists every 6 months. Although I’m aware there is a lack of resources to employ a regular dentist or a hygienist, a brigade twice a year can be instrumental in good dental health by removing plaque and tartar that cannot be done at home.

6
Appendix***
***For all graphs, y-axis is in percentage of respondents and x-axis is responses given by the participants. Santa
Ana, Casa De Piedra, and Manchon have 26, 25, and 47 participants respectively. Average is calculated with all 98
participants included.

7
Appendix A: Basic Questions
95%
5% 0%
98%
2% 0%
88%
12%
0% 0%
20%
40%
60%
80%
100%
120%
Yes No No response
Do You Brush Your Teeth Twice a Day?
Average
Manchon
Santa Ana
81%
19%
0%
87%
13%
0%
85%
15%
0% 0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Yes No No response
Do You Have a Brush And Toothpaste?
Santa Ana
Manchon
Average

8
Appendix B: Perceived Susceptibility:
54%
42%
4%
40%
60%
0%
28%
62%
11%
38%
56%
6%
0%
10%
20%
30%
40%
50%
60%
70%
Yes No No response
Do you think that you could get cavities/caries?
Santa Ana
Casa De Piedra
Manchon
Average
73%
23%
4%
76%
20%
4%
53%
43%
4%
64%
32%
4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Yes No No response
Do you think that you will have cavities caused by not brushing your teeth in the
next few years?
Santa Ana
Casa De Piedra
Manchon
Average

9
19
11
7
0
5
3
15
10
6
10
7
4
10
0
6 7
23
14
0
5
10
15
20
25
Caries Gusanillo Picadura Mal Aliento Other NoResponse
What are the diseases or problems that you could have if you do not brush your teeth?
Santa Ana
Casa De Piedra
Manchon

10
Appendix C: Perceived Severity
65%
15%
0%
15%
0% 4%
20%
44%
8%
24%
4% 0%
49%
13% 11%
17%
4% 6%
46%
21%
7%
18%
3% 4%
0%
10%
20%
30%
40%
50%
60%
70%
muy malo malo medio malo poco malo no es malo no response
How bad of a disease/problem is cavities? Would you say it is very bad, somewhat bad,
average, or not bad at all? ?
Santa Ana
Casa De Piedra
Manchon
Average
85%
8% 8%
76%
16%
8%
62%
32%
6%
62%
32%
6%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Yes No No response
Is oral cavity a dangerous disease?
Santa Ana
Casa De Piedra
Manchon
Average

11
Appendix D: Action Efficacy
77%
12% 12%
96%
4% 0%
87%
13%
0%
87%
10% 3%
0%
20%
40%
60%
80%
100%
120%
Yes No No response
When a person brushes his teeth, does that help avoid cavities?
Santa Ana
Casa De Piedra
Manchon
Average
38%
4%
35%
4%
19%
68%
8%
16%
0%
8%
77%
6%
15%
0% 2%
64%
6%
20%
1%
8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
mucho algo poco no si
To what degree does brushing your teeth help prevent cavities? Does it help prevent it a
little, somewhat, or a lot?
Santa Ana
Casa De Piedra
Manchon
Average

12
Appendix E: Perceived Social Acceptability
35%
62%
4%
24%
48%
28% 26%
72%
2%
28%
63%
9%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Yes No No response
Is There Anybody in the Community Who Says You Should Not Brush Your Teeth?
Santa Ana
Casa De Piedra
Mancho
Average
85%
8% 8%
76%
8%
16%
85%
4% 11%
83%
6% 11%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Yes No No response
Is There Anybody in the Commmunity Who Says You Should Brush Your Teeth?
Santa Ana
Casa De Piedra
Manchon
Average

13
8%
42% 38%
12% 12%
60%
28%
0%
62%
38%
5%
56%
36%
3%
0%
10%
20%
30%
40%
50%
60%
70%
1st group 2nd group no response other
Which of these individuals or groups in either of the two questions above is most important to
you?
Santa Ana
Casa De Piedra
Manchon
Average

14
Appendix F: Self Efficacy
88%
12%
0%
92%
8%
0%
83%
13%
4%
87%
11%
2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Yes No No response
Would it be easy for you to brush your teeth twice a day?
Santa Ana
Casa De Piedra
Manchon
Average
15
Appendix G: Cues for Action
85%
8% 8%
88%
8% 4%
87%
11%
2%
87%
9% 4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Yes No No response
Is it easy to remember to brush your teeth every time that you need to do it?
Santa Ana
Casa De Piedra
Manchon
Average
81%
12% 8%
80%
12% 8%
81%
15%
4%
81%
13% 6%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Yes No No response
Is it easy to remember the steps in brushing your teeth twice a day every time that you
need to do it?
Santa Ana
Casa De Piedra
Manchon
Average

16
Appendix H: Divine Will
27%
65%
8%
36%
52%
12%
26%
68%
6%
29%
63%
8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Yes No No response
Is it sometimes God’s (or the gods’) will that people/children get cavities
Santa Ana
Casa De Piedra
Manchon
Average
77%
8%
15%
76%
8%
16%
77%
9% 15%
77%
8% 15%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Cepillarse Other No Response
Why do some people get cavities and some people do not?
Santa Ana
Casa De Piedra
Manchon
Average

17
58%
31%
12%
24%
60%
16%
26%
60%
15%
26%
60%
15%
0%
10%
20%
30%
40%
50%
60%
70%
Yes No No response
Do people sometimes get cavities because of curses or other spiritual or supernatural
causes?
Santa Ana
Casa De Piedra
Manchon
Average

18
Appendix I: Positive Attributes Of The Behavior
8
3 4
10
3
7
3 3
7 5
6
0
11
25
5
0
5
10
15
20
25
30
Evitar Caries No LlevaEnfermedad
Buenas Dientes Other No Response
What do you see as the advantages or good things that would happen if you brushed your teeth twice a
day?
Santa Ana
Casa De Piedra
Manchon
9
2 5
10
5 2
11
7
0 2
16
29
0
5
10
15
20
25
30
35
Mantener Limpia ySana
Enfermedad oCaries
No Response Other
What are the things you like (or would like) about brushing your teeth twice a day?
Santa Ana
Casa De Piedra
Manchon

19
Appendix J: Prochaska’s change Theory