supplementary table 1: clinical characteristics of …€¦ · web viewtemporal bone cavernous...
TRANSCRIPT

Supplementary Table 1: Clinical characteristics of the 41 NPC patients and 21 patients with NPC and unilateral TLN
Characteristic Value for the 41 NPC patients Value for the 21 NPC patients with unilateral TLNNumber 41 21
Gender
Male 31 16
Female 10 5
Age (years)
≤ 40 13 8
> 40 28 13
T stagea
T1 7 1
T2 9 1
T3 17 3
T4 8 16
N stagea
N0 6 4
N1 20 12
N2 11 5
N3 4 0
Overall stagea
I 2 1
II 11 1
III 16 3
IV 12 16
Radiation techniqueb
VMAT 17 0
Static IMRT 24 21
Chemotherapy
No 6 3
Yes 35 18
Involved laterality
Left side 13
Right side 8
Abbreviations: TLN, temporal lobe necrosis; IMRT, intensity modulated radiotherapy; VMAT, volumetric modulated arc therapyaAccording to the 7th AJCC/UICC staging system.bAll the patients were treated with IMRT including 17 with VMAT and 24 with static IMRT.

Supplementary Table 2: Comparison of dosimetric parameters between temporal lobes with and without TLN using the two contouring methods
Dosimetric parameters
Method 1a Method 2b
t Mean difference P-value t Mean difference P-valueD0.1ccc 6.15 10.46 <0.001 6.09 10.40 <0.001D0.5cc 5.08 8.03 <0.001 6.84 11.87 <0.001D1cc 6.98 12.84 <0.001 7.01 12.86 <0.001D5cc 7.12 14.28 <0.001 7.70 14.81 <0.001
D10cc 5.92 12.91 <0.001 6.55 13.45 <0.001D15cc 4.70 10.09 <0.001 5.08 10.49 <0.001D20cc 3.80 7.29 0.001 4.26 7.77 <0.001D25cc 3.52 5.44 0.002 3.96 5.79 0.001D30cc 3.44 3.45 0.004 4.18 4.24 0.001D35cc 2.42 1.97 0.025 4.42 3.03 <0.001D40cc 2.00 1.31 0.049 3.85 2.17 0.001
D1d 7.06 12.54 <0.001 7.14 12.90 <0.001D2 7.23 13.82 <0.001 7.25 14.12 <0.001D5 7.84 14.89 <0.001 8.04 15.05 <0.001D10 7.12 14.66 <0.001 7.01 14.16 <0.001D15 6.17 13.02 <0.001 5.46 11.66 <0.001D20 4.98 11.33 <0.001 4.58 9.12 <0.001D25 4.61 8.91 <0.001 4.20 6.84 0.001D30 4.21 7.05 0.001 4.23 4.96 <0.001D35 4.62 5.75 <0.001 4.81 3.98 <0.001D40 4.51 4.19 <0.001 4.39 3.00 <0.001D45 4.03 3.14 0.001 3.98 2.27 0.001D50 3.63 2.36 0.002 3.74 1.77 0.001D55 3.61 1.76 0.002 3.67 1.51 0.002D60 3.59 1.4 0.002 3.71 1.47 0.001V10e 3.32 4.88 0.003 3.17 5.28 0.005V20 5.13 5.86 <0.001 5.31 6.15 <0.001V25 5.95 7.16 <0.001 6.16 6.79 <0.001V30 6.97 8.72 <0.001 6.95 7.69 <0.001V35 6.77 9.71 <0.001 6.86 8.18 <0.001V40 6.18 10.01 <0.001 6.48 8.26 <0.001V45 5.84 9.89 <0.001 6.10 8.03 <0.001V50 2.72 3.37 0.013 5.81 7.78 <0.001V55 5.19 8.61 <0.001 5.39 7.02 <0.001V60 4.75 7.07 <0.001 4.78 5.75 <0.001V65 3.88 4.93 0.001 3.88 4.01 0.001V70 2.85 2.64 0.01 2.87 2.20 0.009V75 2.06 0.83 0.042 2.19 0.72 0.041
Volume 2.92 3.62 0.009 2.26 3.10 0.035Dmean 5.83 4.98 <0.001 5.83 4.36 <0.001
D1 of PRVf 7.35 11.48 <0.001 7.50 11.80 <0.001D5 of PRV 7.80 14.19 <0.001 8.20 14.73 <0.001D10 of PRV 6.80 14.18 <0.001 7.27 14.73 <0.001D15 of PRV 5.95 13.14 <0.001 5.72 12.45 <0.001

D20 of PRV 4.93 11.02 <0.001 4.71 9.59 <0.001D25 of PRV 4.30 8.60 <0.001 4.29 7.15 <0.001D30 of PRV 4.01 6.77 0.001 4.20 5.25 <0.001D35 of PRV 3.94 5.07 0.001 4.26 3.92 <0.001D40 of PRV 4.16 3.88 <0.001 4.38 3.06 <0.001D45 of PRV 3.89 2.93 0.001 4.13 2.35 0.001D50 of PRV 3.70 2.23 0.001 3.91 1.88 0.001D55 of PRV 3.72 1.66 0.001 3.76 1.59 0.001D60 of PRV 3.44 1.25 0.003 3.57 1.40 0.002V20 of PRV 5.31 5.66 <0.001 5.21 5.72 <0.001V25 of PRV 5.73 6.88 <0.001 6.01 6.70 <0.001V30 of PRV 6.94 8.77 <0.001 6.70 7.73 <0.001V35 of PRV 6.59 9.40 <0.001 6.82 8.28 <0.001V40 of PRV 6.22 9.61 <0.001 6.52 8.31 <0.001V45 of PRV 5.96 9.92 <0.001 6.31 8.06 <0.001V50 of PRV 5.74 9.17 <0.001 6.04 7.78 <0.001V55 of PRV 5.53 8.47 <0.001 5.76 7.18 <0.001V60 of PRV 5.05 7.16 <0.001 5.17 6.08 <0.001V65 of PRV 4.33 5,.30 <0.001 4.38 4.51 <0.001V70 of PRV 3.18 2.99 0.005 3.42 2.66 0.003V75 of PRV 2.45 1.10 0.024 2.55 0.98 0.019
Abbreviations: PRV=planning organ at risk volume; D mean= mean dose; TLN=temporal lobe necrosis;aTemporal lobe including the basal ganglia and insula, excluding parahippocampal gyrus and hippocampusbTemporal lobe including parahippocampal gyrus and hippocampus, excluding basal ganglia and insula.cD0.1cc is the minimum dose received by the ‘‘hottest’’ 0.1ml of the organ, the other D with suffixes
expresses the same meaning, but the suffix numbers represent the absolute volume.dD1 is the minimum dose received by the ‘‘hottest’’ 1% of the organ, the other D with suffixes express the same meaning, but the suffix numbers represent the percentage of volume.eV10 is the percentage of volume of temporal lobe that receives more than 10 Gy, the other V with suffixes express the same meaning, but the suffix numbers represent the doses received.f D1of PRV is the minimum dose received by the ‘‘hottest’’ 1% of the planning organ at risk volume of temporal lobe volume, the other Dx of PRV, Vx of PRV express the same meaning, but the prefix parameter represent the percentage of volume or the dose received.

Supplementary Table 3: Anatomic boundaries of the organs at risk in NPC.
Organ Standard TPS name [20]
Cranial Caudal Anterior Posterior Lateral Medial
TMJ TMjointa Disappearance of articular cavity
Appearance of the head of mandible or one slice superior to the sigmoid notch of the neck of mandible
Articular condyle of the temporal bone, ant. edge of mandibular condyle
Surface of fossa glenoid
Lat. edge of mandibular condyle or surface of fossa glenoid
Brainstem BrainStem Optic tract or the disappearance of posterior cerebral artery
Foramen magnum Post. edge of prepon- tine cistern or basilar artery
Ant. edge of forth ventricle or mesencephalic aqueduct
Posterior cerebral artery, anterior inferior cerebellar artery, cerebellar peduncle
Optic chiasm Chiasm One or two slices superiorly
Pituitary or suprasellar cistern
Optic canal Infundibulum Internal carotid arteries, middle cerebral arteries
Tongue(oral cavity)b
Tongue Post. edge of the hard palate or soft palate
Disappearance of anterior belly of digastric muscle
Post. edge of mandible or is free
Palate, oropharynx, the palatine tonsil, hyoid bone
Med. edge of the mandible or inferior alveoli socket
Larynx(larynx and laryngopharynx)
Larynx Cranial edge of epiglottis
Caudal edge of cricoid cartilage
Ant. edge of thyroid cartilage or cricoid cartilage
Including arytenoid cartilage, the superior and inferior horns of thyroid cartilage and post. edge of pharyngeal constrictor
Med. edge of hyoid bone, lat. edge of thyroid cartilage and cricoid cartilage, cervical vessels, nerves, and lateral thyroid
Upper Pharyngeal- Caudal edge of Cranial edge of hyoid Nasopharynx, Longus capitis m., Carotid sheath

pharyngeal constrictor [22]
Const_Upper pterygoid plates bone oropharynx, laryngopharynx, base of tongue
longus colli m., body of cervical vertebra
Middle pharyngeal constrictor [22]
Pharyngeal- Const_Middle
Cranial edge of hyoid bone
Caudal edge of hyoid bone
Laryngopharynx Longus capitis m., longus colli m., body of cervical vertebra
Hyoid bone
Inferior pharyngeal constrictor [22]
Pharyngeal- Const_Lower
Caudal edge of hyoid bone
Caudal edge of cricoid cartilage
Laryngopharynx or cricoids cartilage
Longus capitis m., longus colli m., body of cervical vertebra
Thyroid cartilage or thyroid gland
Trachea Trachea Caudal edge of cricoid cartilage
Two centimeters below the caudal edge of the clavicular head
Post. edge of isthmus of thyroid gland
Ant. edge of esophagus
Lateral thyroid gland One-two millimeters expanded from the lumen of trachea
Subman-dibular gland
Submandibulara Inferior edge of medial pterygoid or the level of C3
Appearance of fat space of submandibular triangle
Lat. surface of mylohyoid m. or hyoglossus m.
Parapharyngeal space, cervical vessels and post. belly of digastric m., sternocleidomastoid m.
Ramus of the mandible, subcutaneous fat or platysma
Cervical vessels, superior and middle pharyngeal constrictor m., hyoid bone, post. belly of the digastric m., mylohyoid m. or hyoglossus m.
Esophagus [22] Esophagus Caudal edge of cricoid cartilage
Two centimeters below the caudal edge of the clavicular head
Trachea Vertebral body or longus colli m.
Fat space or thyroid gland
Optic nerve [23] OpticNervea Below the superior rectus
Superior the inferior rectus
Posterior edge of the center of globe
Optic canal
Temporal lobe TemporalLobea Cranial edge of the Base of middle cranial Temporal bone and Petrous part of Temporal bone Cavernous sinus,

sylvian fissure fossa sylvian fissure, greater wing of sphenoid
temporal lobe, tentorium of cerebellum, incisura preoccipitalis
sphenoid sinus, sella turcica, and sylvian fissure(including parahippocampal gyrus and hippocampus
Parotid gland [21]
Parotida External auditory canal, mastoid process
Appearance post. part submandibular space
Masseter m. post. border mandibular bone, medial pterygoid m.
Ant. belly sternocleidomastoid m., lat. side post. belly of the digastric m. (posterior medial), mastoid process
Submandibular fat, platysma
Post. belly of the digastric m., styloid process, parapharyngeal space, sternocleidomastoid
Spinal cord SpinalCord Disappearance of cerebellum
Two centimeters below the inferior edge of the clavicular head
Exclude the subarachnoid space
Brachial plexus [24]
BrachialPlexusa Caudal edge of C4 Caudal edge of T1 at neural foramina and one to two CT slices below the clavicular head as the posterior aspect of the neurovascularbundle
Anterior scalene muscle Middle scalene muscle
Fat space Spinal cord
Thyroid gland Thyroid Caudal edge of pyriform sinus or midpoint of thyroid
Body of fifth to seventh cervical vertebra
Sternohyoid or sternocleidomastoid
Cervical vessels or longus colli m.
Cervical vessels or sternocleidomastoid
Thyroid cartilage or cricoids cartilage or esophagus or

cartilage pharyngeal constrictor
Mandible Mandible The mandible be contoured as whole organ but not be divided into the left and the right. Contouring of the mandible should include alveolar bone and exclude the teeth.
Inner ear Ear_Innera Cochlea and IAC should be individually delineated and named.
Middle ear Ear_Middlea Tympanic cavity, bony part of ET should be individually delineated and named.
Eyes Eyesa Ensure the retina to be contoured completely.
Lens Lensa The boundary between the lens and the vitreum is obvious
Pituitary Pituitary The pituitary is located in the hypophysial fossa. Insure the organ be contoured completely but not beyond the surrounding bone. The pituitary is ovoid and can be visualized on 1-2 slices on CT scans of 3 mm thickness
Abbreviations: TMJ, temporomandibular joint; ET, Eustachian tube; IAC, internal auditory canal; m., muscle.a The organs should be divided into left and right, and the standard TPS name of laterality is indicated by appending an underscore character ( _ ), followed by L or R, respectively. For example, the left parotid is named Parotid_L; the right parotid is named Parotid_R.b include the base of the tongue, body of tongue and mouth floor.

Supplementary table 4: Abbreviations mentioned in the manuscript.
Abbreviations Full name
OAR organ at risk
TMJ temporomandibular joint
NPC nasopharyngeal carcinoma
PC pharyngeal constrictor
ET Eustachian tube
ROC receiver operating characteristic
TLN temporal lobe necrosis
IAC internal auditory canal
RT radiotherapy
GTV gross target volume
CTV clinical target volume
PTV planning target volume
PRV planning organ at risk volume
Dmean mean dose
Dmax maximum dose
S.E. standard error
SNHL sensorineural hearing loss
OME otitis media with effusion
IMRT intensity modulated radiotherapy
VMAT volumetric modulated arc therapy
AUC Area under the curve
Dx(xcc) minimum dose received by the ‘‘hottest’’ x% (or x ml) of the organ
Vx volume percentage of the organ receiving ≥ X Gy

Supplementary Figure 1. Receiver operating characteristic (ROC) curve analysis for the D1 of
the PRV using two different temporal lobe contouring methods in 21 NPC patients with
unilateral TLN.










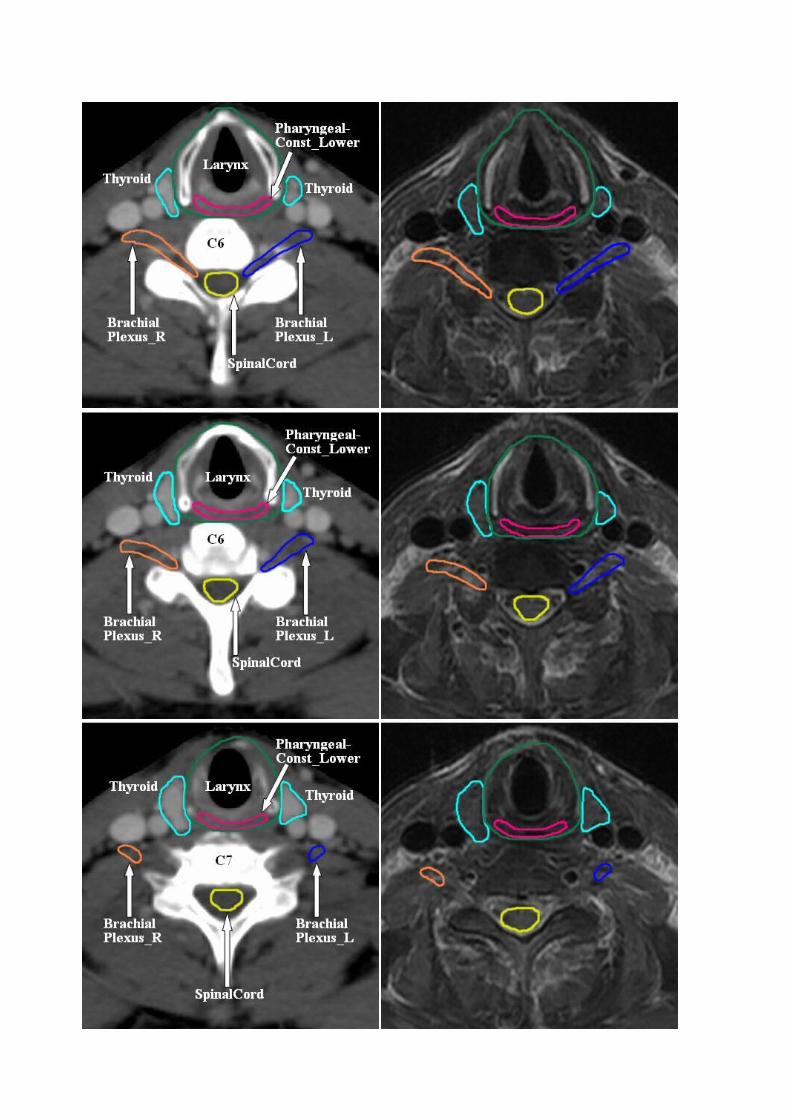



Supplementary Figure 2. Recommended atlas of the tympanic cavity, Eustachian tube (ET), cochlea, IAC,
TMJ, temporal lobe, brainstem, parotid gland, spinal cord, optic nerve, chiasm, submandibular gland,
pituitary, mandible, eyes, lens, brachial plexus, tongue(oral cavity), larynx, pharyngeal constrictors and
trachea as OARs based on CT-MRI fusion in NPC patients.

Supplementary References 1: The list of literatures relative to OARs contouring
1. Baxi S, Park E, Chong V, Chung HT. Temporal changes in IMRT contouring of organs at
risk for nasopharyngeal carcinoma - the learning curve blues and a tool that could help.
Technol Cancer Res Treat 2009; 8:131-140.
2. Gondi V, Tome WA, Rowley HA, Mehta MP. Hippocampal Contouring: A Contouring
Atlas for RTOG 0933. 2011.
3. Penumetcha N, Kabadi S, Jedynak B, et al. Feasibility of geometric-intensity-based semi-
automated delineation of the tentorium cerebelli from MRI scans. J Neuroimaging 2011;
21:e148-55.
4. Chau RM, Leung SF, Kam MK, et al. A split-organ delineation approach for dose
optimisation for intensity-modulated radiotherapy for advanced T-stage nasopharyngeal
carcinoma. Clin Oncol (R Coll Radiol) 2008; 20:134-41.
5. Bonilha L, Kobayashi E, Cendes F, Li LM. The importance of accurate anatomic
assessment for the volumetric analysis of the amygdala. Braz J Med Biol Res 2005; 38:409-
18.
6. Wang SZ, Yan XJ, Guo M, et al. Clinical analysis of otitis media with effuse after 3D
planning system based radiotherapy of nasopharyngeal carcinoma. China Oncol 2006;
16:503–7.
7. Walker GV, Ahmed S, Allen P, et al. Radiation-induced middle ear and mastoid
opacification in skull base tumors treated with radiotherapy. Int J Radiat Oncol Biol Phys
2011; 81:e819-e823.
8. Wang SZ, Wang WF, Guo M, et al. Analysis of anatomic factors controlling the morbidity

of radiation-induced otitis media with effusion. Radiotherapy and Oncology 2007; 85: 463–
468.
9. Wang SZ, Li J, Miyamoto CT, et al. A study of middle ear function in the treatment of
nasopharyngeal carcinoma with IMRT technique. Radiotherapy and Oncology 2009;
93:530-3.
10. Hsin CH, Chen TH, Young YH, Liu WS. Comparison of otologic complications between
intensity-modulated and two-dimensional radiotherapies in nasopharyngeal carcinoma
patients. Otolaryngology-Head and Neck Surgery 2010; 143: 662-8.
11. Bhandare N, Antonelli PJ, Morris CG, Malayapa RS, Mendenhall WM.
Ototoxicity after radiotherapy for head and neck tumors. Int J Radiat Oncol Biol
Phys 2007; 67:469-79.
12. Petsuksiri J, Sermsree A, Thephamongkhol K, et al. Sensorineural hearing loss after
concurrent chemoradiotherapy in nasopharyngeal cancer patients. Radiat Oncol 2011; 6:19.
13. Pacholke HD, Amdur RJ, Schmalfuss IM, Louis D, Mendenhall WM. Contouring the
middle and inner ear on radiotherapy planning scans. Am J Clin Oncol 2005; 28:143-147.
14. Pan CC, Eisbruch A, Lee JS, Snorrason RM, Ten Haken RK, Kileny PR. Prospective study
of inner ear radiation dose and hearing loss in head-and-neck cancer patients. Int J Radiat
Oncol Biol Phys 2005; 61:1393-1402.
15. Low WK, Burgess R, Fong KW, Wang DY. Effect of radiotherapy on retro-cochlear
auditory pathways. Laryngoscope 2005; 115:1823-1826.
16. Chen WC, Jackson A, Budnick AS, et al. Sensorineural hearing loss in combined modality
treatment of nasopharyngeal carcinoma. Cancer 2006; 106 (Suppl. 4):820-829.
17. Bhandare N, Jackson A, Eisbruch A, Radiation therapy and hearing loss. Int J Radia Oncol

Biol Phy 2010; 76:S50-7.
18. Zuur CL, Simis YJ, Lamers EA, et al. Risk factors for hearing loss in patients treated with
intensity-modulated radiotherapy for head-and-neck tumors. Int J Radiat Oncol Biol Phys
2009; 74:490-6.
19. Parashar B, Kuo C, Kutler D, et al. Importance of contouring the cervical spine levels in
initial intensity-modulated radiation therapy radiation for head and neck cancers:
implications for re-irradiation. J Cancer Res Ther 2009; 5:36-40.
20. Kong FM, Ritter T, Quint DJ, et al. Consideration of dose limits for organs at risk of
thoracic radiotherapy: atlas for lung, proximal bronchial tree, esophagus, spinal cord, ribs,
and brachial plexus. Int J Radiat Oncol Biol Phys 2011; 81:1442-1457.
21. Leung WM, Tsang NM, Chang FT, Lo CJ. Lhermitte's sign among nasopharyngeal cancer
patients after radiotherapy. Head Neck 2005; 27:187-194.
22. Harari PM, Song S, Tome WA. Emphasizing Conformal Avoidance vs. Target Definition
for IMRT Treatment Planning in Head and Neck Cancer. Int J Radiat Oncol Biol Phys
2010; 77: 950–958.
23. Ezhi M, Starkschall G, Mohan R, Cox J, Komski R. Validation of a model-based
segmentation approach to propagating normal anatomic regions of interest through the 10
phases of respiration. Int J Radiat Oncol Biol Phys 2008; 71: 900-6.
24. Weiss W, Wijesooriya K, Ramakrishnan V, Keall P. Comparison of intensity-modulated
radiotherapy planning based on manual and automatically generated contours using
deformable image registration in four-dimensional computed tomography of lung cancer
patients. Int J Radiat Oncol Biol Phys 2008; 70: 572–581.

25. Qatarneh SM, Noz ME, Hyodymaa S, Maguire GQ, Kramer EL, Crafoord J. Evaluation of
a segmentation procedure to delineate organs for use in construction of a radiation therapy
planning atlas. Int J Med Inform 2003; 69: 39-55.
26. Pak D, Vineberg K, Feng F, Ten Haken RK, Eisbruch A. Lhermitte sign after chemo-IMRT
of head-and-neck cancer: incidence, doses, and potential mechanisms. Int J Radiat Oncol
Biol Phys 2012; 83(5):1528-33.
27. Uhl M, Sterzing F, Habl G, et al. CT-myelography for high-dose irradiation of spinal cord
and paraspinal tumors with helical tomotherapy: revival of an old tool. Strahlenther Onkol
2011; 187:416-20.
28. Brouwer CL, Steenbakkers RJ, Van den Heuvel E, et al. 3D Variation in delineation of
head and neck organs at risk. Radiat Oncol 2012; 7:32.
29. Schreibmann E, Fox T. Towards automated planning for unsealed source therapy. J Appl
Clin Med Phys 2012; 13:3789.
30. Urbano TG, Clark CH, Hansen VN, et al. Intensity Modulated Radiotherapy (IMRT) in
locally advanced thyroid cancer: Acute toxicity results of a phase I study. Radiother
Oncol 2007; 85:58-63.
31. Zwicker F, Roeder F, Hauswald H, et al. Reirradiation with intensity-modulated
radiotherapy in recurrent head and neck cancer.Head Neck 2011; 33:1695-702.
32. Park SH, Park HC, Park SW, et al. Multi-institutional Comparison of Intensity Modulated
Radiation Therapy (IMRT) Planning Strategies and Planning Results for Nasopharyngeal
Cancer. J Korean Med Sci 2009; 24:248-55.
33. Eisbruch A, Marsh LH, Dawson LA, et al. Recurrences near base of skull after IMRT for

head-and-neck cancer: implications for target delineation in high neck and for parotid gland
sparing. Int J Radiat Oncol Biol Phys 2004; 59:28-42.
34. Claus F, Duthoy W, Boterberg T, et al. Intensity modulated radiation therapy for
oropharyngeal and oral cavity tumors: clinical use and experience. Oral Oncol 2002;
38:597-604.
35. Chen AM, Li BQ, Farwell DG, Marsano J, Vijayakumar S, Purdy JA. Improved dosimetric
and clinical outcomes with intensity-modulated radiotherapy for head-and-neck cancer of
unknown primary origin. Int J Radiat Oncol Biol Phys 2011; 79:756-62.
36. Dirix P, Nuyts S. Evidence-based organ-sparing radiotherapy in head and neck cancer.
Lancet Oncol 2010; 11:85-91.
37. Strigari L, Benassi M, Arcangeli G, Bruzzaniti V, Giovinazzo G, Marucci L. A novel dose
constraint to reduce xerostomia in head-and-neck cancer patients treated with intensity-
modulated radiotherapy. Int J Radiat Oncol Biol Phys 2010; 77:269-76.
38. Zhang Y, Lin J, Zhou W, Tang J, Liao Y. Dosimetric verification and clinical efficacy
of intensity modulated radiotherapy in nasopharyngeal carcinoma. Zhong Nan Da Xue Xue
Bao Yi Xue Ban 2009;34: 879-85
39. van Rij CM, Oughlane-Heemsbergen WD, Ackerstaff AH, Lamers EA, Balm AJ, Rasch
CR. Parotid gland sparing IMRT for head and neck cancer improves xerostomia related
quality of life. Radiat Oncol 2008; 3:41.
40. Huang K, Xia P, Chuang C, Weinberg V, et al. Intensity-modulated chemoradiation for
treatment of stage III and IV oropharyngeal carcinoma: the University of California-San
Francisco experience. Cancer 2008; 113:497-507.

41. Seung S, Bae J, Solhjem M, et al. Intensity-modulated radiotherapy for head-and-neck
cancer in the community setting. Int J Radiat Oncol Biol Phys 2008; 72:1075-81.
42. Bhide S, Clark C, Harrington K, Nutting CM. Intensity Modulated Radiotherapy Improves
Target Coverage and Parotid Gland Sparing When Delivering Total Mucosal Irradiation in
Patients With Squamous Cell Carcinoma of Head and Neck of Unknown Primary Site Med
Dosim 2007; 32:188-95.
43. Guerrero Urbano MT, Clark CH, et al. Target volume definition for head and neck intensity
modulated radiotherapy: pre-clinical evaluation of PARSPORT trial guidelines. Clin Oncol
(R Coll Radiol) 2007; 19:604-13.
44. Lee NY, de Arruda FF, Puri DR, et al. A comparison of intensity-modulated radiation
therapy and concomitant boost radiotherapy in the setting of concurrent chemotherapy for
locally advanced oropharyngeal carcinoma. Int J Radiat Oncol Biol Phys 2006; 66:966-74.
45. Braam PM, Terhaard CH, Roesink JM, Raaijmakers CP. Intensity-modulated
radiotherapy significantly reduces xerostomia compared with conventional radiotherapy.
Int J Radiat Oncol Biol Phys 2006; 66:975-80.
46. de Arruda FF, Puri DR, Zhung J, et al. Intensity-modulated radiation therapy for the
treatment of oropharyngeal carcinoma: the Memorial Sloan-Kettering Cancer Center
experience. Int J Radiat Oncol Biol Phys 2006; 64:363-73.
47. Kwong DL, Pow EH, Sham JS, et al. Intensity-modulated radiotherapy for early-stage
nasopharyngeal carcinoma: a prospective study on disease control and preservation of
salivary function. Cancer 2004; 101:1584-93.
48. Chao KS, Ozyigit G, Blanco AI, et al. Intensity-modulated radiation therapy for

oropharyngeal carcinoma: impact of tumor volume. Int J Radiat Oncol Biol Phys 2004;
59:43-50.
49. Parliament MB, Scrimger RA, Anderson SG, et al. Preservation of oral health-related
quality of life and salivary flow rates after inverse-planned intensity- modulated
radiotherapy (IMRT) for head-and-neck cancer. Int J Radiat Oncol Biol Phys 2004; 58:663-
73.
50. van Asselen B, Dehnad H, Raaijmakers CP, Roesink JM, Lagendijk JJ, Terhaard CH. The
dose to the parotid glands with IMRT for oropharyngeal tumors: the effect of reduction of
positioning margins. Radiother Oncol 2002; 64:197-204.
51. Lee N, Xia P, Quivey JM, et al. Intensity-modulated radiotherapy in the treatment of
nasopharyngeal carcinoma: an update of the UCSF experience. Int J Radiat Oncol Biol
Phys 2002; 53:12-22.
52. Sultanem K, Shu HK, Xia P, et al. Three-dimensional intensity-modulated radiotherapy in
the treatment of nasopharyngeal carcinoma: the University of California-San Francisco
experience. Int J Radiat Oncol Biol Phys 2000; 48:711-22.
53. Wu Q, Manning M, Schmidt-Ullrich R, Mohan R. The potential for sparing of parotids and
escalation of biologically effective dose with intensity-modulated radiation treatments of
head and neck cancers: a treatment design study. Int J Radiat Oncol Biol Phys 2000;
46:195-205.
54. Butler EB, Teh BS, Grant WH 3rd, et al. Smart (simultaneous modulated accelerated
radiation therapy) boost: a new accelerated fractionation schedule for the treatment of head
and neck cancer with intensity modulated radiotherapy. Int J Radiat Oncol Biol Phys 1999;

45:21-32.
55. Grégoire V, Jeraj R, Lee JA, O'Sullivan B. Radiotherapy for head and neck tumours in
2012 and beyond: conformal, tailored, and adaptive? Lancet Oncol 2012; 13:e292-300.
56. Scrimger R. Salivary gland sparing in the treatment of head and neck cancer. Expert Rev
Anticancer Ther 2011; 11:1437-48.
57. Anand AK, Jain J, Negi PS, et al. Can dose reduction to one parotid gland prevent
xerostomia?--A feasibility study for locally advanced head and neck cancer patients treated
with intensity-modulated radiotherapy. Clin Oncol (R Coll Radiol) 2006; 18:497-504.
58. Faggiano E, Fiorino C, Scalco E, et al. An automatic contour propagation method to follow
parotid gland deformation during head-and-neck cancer tomotherapy. Phys Med Biol 2011;
56:775-91.
59. Feng M, Demiroz C, Karen A, et al. Normal Tissue Anatomy for Oropharyngeal Cancer:
Contouring Variability and Its Impact on Optimization. Int J Radiat Oncol Biol Phys, 2012;
84:e245-9.
60. Mukesh M, Benson R, Jena R, et al. Interobserver variation in clinical target volume and
organs at risk segmentation in post-parotidectomy radiotherapy: can segmentation protocols
help? The British Journal of Radiology 2012; 85: e530–e536.
61. Loo SW, Martin WM, Smith P, Cherian S, Roques TW. Interobserver variation in parotid
gland delineation: a study of its impact on intensity-modulated radiotherapy solutions with
a systematic review of the literature. Br J Radiol 2012; 85:1070-7.