surgical management of refractory supraventricular tachycardia in infants … · ·...
TRANSCRIPT

124 JACC Vol. 5, No. 1January 1985:124-9
Surgical Management of Refractory Supraventricular Tachycardia inInfants and Children
DAVID A. OTT, MD, FACC, PAUL C. GILLETTE, MD, FACC, ARTHUR (lARSON, JR., MD, FACC,
DENTON A. COOLEY, MD, FACC, GEORGE J. REUL, MD, FACC,
DAN G. McNAMARA, MD, FACC
Houston, Texas
Sixty-seven children underwent attempted surgical correction of refractory supraventricular arrhythmias usinga combination of intraoperative electrophysiologicmapping followed by surgical division or cryoablation of anaberrant conduction pathway or atrial ectopic focus. Thepatients ranged in age from 4 months to 18 years (mean11.4 years).
Fifty-fivepatients (82%) had an abnormal conductionpathway crossing the atrioventricular junction (Kentbundle). Thirty-six (65%) of these 55 patients had classicWolff-Parkinson-White syndrome with a delta wave ofpre-excitation on the surface electrocardiogram. Nineteen (35%), however, demonstrated only retrogradeconduction across the Kent bundle and had a normalsurface electrocardiogram when tachycardia was notpresent. Kent bundles were isolated to the following locations: right anterior or lateral in 19 (34.5%), left posterior or lateral in 22 (40%), posteroseptal in 10 (18%),anteroseptal in 2 (4%) and both right and left in 2 (4%).Follow-up evaluation of as long as 8 years (mean 34.9
The surgical treatment of supraventricular tachycardia queto the presence of an accessory conduction bundle (Kent)has been adequately described in adults and its efficacyaccepted (1-3). The diagnostic evaluation and surgical management of these pre-excitation syndromes in children aswell as those due to an atrial ectopic focus have only recentlybeen documented (4-6). We have described the electrophysiologic evaluation and medical management of supraventricular and ventricular tachycardias in infants and children, and since 1976 we have applied these principles to
From the Divisions of Surgery and Pediatric Cardiology of the TexasHeart Institute and Texas Children's Hospital, Houston, Texas. This studywas presented in part at the 33rd Annual Scientific Session of the AmericanCollege of Cardiology, March [984, Dallas, Texas. Manuscript receivedApril 2, 1984; revised manuscript received July 2, 1984, accepted July18.1984.
Address for reprints: David A. Ott, MD, Texas Heart Institute. P. O.Box 20345, Houston. Texas 77225.
©1985 by the American College of Cardiology
months) has shown seven immediate failures and onelate recurrence of arrhythmia (14.5%). Recent refinements in technique and the use of cryoablation for septalaberrant pathways have improved these results. Therehave been two failures (8%) in the last 25 attempts.Twelve patients underwent surgery for an atrial ectopicfocus by the following techniques: cryoablation in sevenpatients, excision in one patient and both excision andcryoablation in four patients. At a mean follow-up "f16.6 months, there was one late recurrence in the groupwith an atrial ectopic focus.
Children with refractory supraventricular tachycardia, even in the absence of pre-excitation on the electrocardiogram should undergo complete electrophysiologic study to elucidate the mechanism of tachycardia.Surgery for supraventricular tachycardia can be performed safely in infants and children and offers predictable results and the opportunity to cure the tachycardia syndrome.
(J Am Coli Cardiol 1985;5:124-9)
the surgical resolution of the tachycardia in a series of 67patients (7-20). This report documents the evaluation, results and current approach to the surgical treatment of supraventricular tachycardia in children.
MethodsPatients. From March 1976 to September 1983, 67 chil
dren were referred for surgery for incapacitating, refractoryor life-threatening supraventricular tachycardia after complete electrophysiologic evaluation including intracardiaccatheterization. After this evaluation, operative ablation ofthe accessory conduction bundle was attempted, using eithersurgical division, cryoablation or a combination of bothtechniques with or without the use of temporary total cardiopulmonary bypass. Fifty percent of the patients wereoperated on in the most recent 2 years of the study (September 1981 to September 1983).
0735-1097/85/$3.30

JACC Vol. 5. No.1January 1985:124-9
OTT ET AL.SURGERY FOR REFRACTORY SUPRAVENTRICULAR TACHYCARDIA
125
Table 1. Congenital Cardiac Defects Associated WithSupraventricular Tachyarrhythmias
Surgical Management
Intraoperative mapping. Patients considered to be candidates for surgical ablation were operated on through amedian sternotomy incision. Care was taken to maintainnormothermic conditions during electrophysiologic mappingbecause we have found that arrhythmias in children are
The study was limited to patients J8 years of age oryounger (mean JJ) at the time of surgery. The diagnosis ofabnormal tachycardia was made in utero in the youngestpatient, who required surgical treatment at 4 months of age.All patients had refractory, incessant or recurrent tachycardia, and three children (all with Wolff-Parkinson-White syndrome) had had documented episodes of ventricular fibrillation from which they were successfully resuscitated beforeevaluation. Various associated congenital cardiac defectswere noted (Table 1) (21).
The patients were managed medically initially unless theirarrhythmia wds considered life-threatening. The latter groupincluded those patients with a documented history of cardiovascular collapse or ventricular fibrillation, as well asthose who had an anterograde effective refractory period ofthe Kent bundle of less than 230 ms (22). This group ofpatients at high risk of sudden death was referred for surgicaltreatment initially whether or not the arrhythmia wasincapacitating.
Medical attempts to control the tachycardia consisted ofadministration of the usual medications for supraventriculartachycardia, including digitalis, propranolol, quinidine andverapamil. Amiodarone was used in two cases without success. Failure of drug treatment was considered an indicationfor surgical intervention. In the later period of the study,confidence in the success and predictability of surgical management resulted in more frequent consideration of the surgical approach as the initial method of management in patients with refractory arrhythmias.
Electrophysiologic evaluation. All patients in whomthe diagnosis of refractory tachycardia was made or stronglysuspected underwent complete electrophysiologic, hemodynamic and angiographic evaluation. The methods for electrophysiologic investigation of supraventricular tachycardiahave been detailed elsewhere (8,9,16,17).
especially sensitive to body temperature changes. Chronotropic anesthetic agents were avoided for similar reasons.Wires for ventricular pacing were placed on the right ventricular wall, and a removable clip-on lead was used toestablish atrial pacing or to act as a bipolar atrial referenceelectrogram (3-5). Various types of sensing probes wereused in searching for the point of earliest retrograde conduction to the atrium during ventricular pacing or sustainedsupraventricular tachycardia using a simplified map of theepicardial surface of the heart. In patients with anterogradeconduction across the accessory bundle, the earliest pointof activation on the ventricular side of the anulus was mappedas needed. In patients with atrial ectopic tachycardia, mapping was done to localize the point of earliest activation ina similar fashion. ,
Methods for division or cryoablation of accessorypathways. The surgical approach to left-sided accessoryconnections was similar to that previously described by Sealyand Gallagher (23). The left atrium was opened as for amitral valve procedure from the right lateral approach duringa period of induced cold cardioplegic arrest. A suture wasplaced through the atrial wall above the coronary sinus fromthe epicardial surface at the site of earliest activation. Withthis point as the center, a wide endocardial incision wasmade just above the mitral valve anulus, dissecting deeplyand caudally until ventricular myocardium was clearly exposed, but without breaking the epicardial surface (Fig. I).In two patients operated on for recurrence of a left-sidedconnection after this technique, we added an epicardial in-
Figure 1. Surgeon's view of endocardial dissection for divisionof a left-sided Kent bundle. The posterior mitral leaflet and chordaeare elevated by the clamp.
4II1III
No.
Ebstein's anomalyEndocardial cushion defectMultiple atrial septal defectsVentricular inversionTransposition of great vesselsMitral stenosisMitral regurgitation
126 orr ET AL.SURGERY FOR REFRACTORY SUPRAVENTRICULAR TACHYCARDIA
JACC Vol. 5. No. IJanuary 1985:124--9
cision beginning at the left atrial appendage and extendingto the inferior vena cava immediately above the coronarysinus (Fig. 2). This incision was carried deep behind thecoronary sinus by retracting it and the left circumflex coronary artery toward the apex of the heart. We now routinelymake both an endocardial and epicardial dissection at theinitial procedure in an effort to preclude recurrence. Cryoablation was not used on left-sided accessory pathways forfear of injury to the circumflex artery.
Right-sided and septal accessory pathways were approached through a right atriotomy incision with the heartbeating. After closure of a septal defect or patent foramenovale, endocardial mapping was performed to confirm theepicardial map and localize the His bundle spike. Anteriorand lateral accessory bundles were divided using a deependocardial incision extending to the epicardial surface ofthe heart near the right coronary artery. Localization of theKent bundle was more difficult in patients with Ebstein'sanomaly because of the difficulty in determining the exactjuncture between the atrium and ventricle and we found thecryoprobe to be especially useful in these cases.
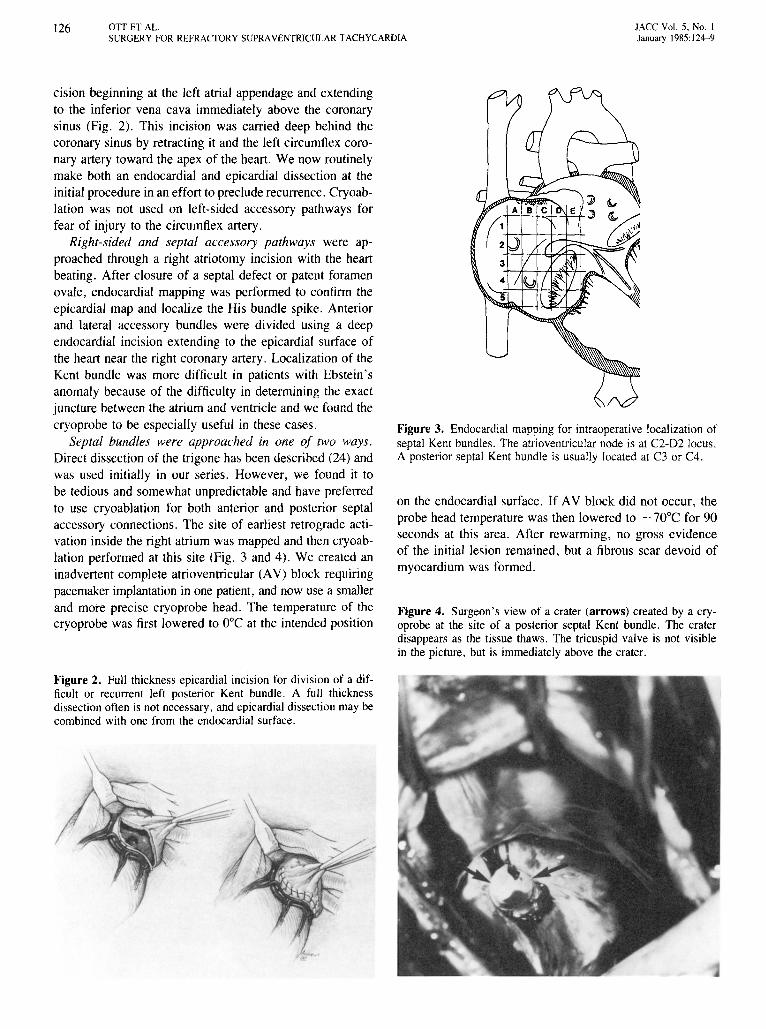
Septal bundles were approached in one of two ways.Direct dissection of the trigone has been described (24) andwas used initially in our series. However, we found it tobe tedious and somewhat unpredictable and have preferredto use cryoablation for both anterior and posterior septalaccessory connections. The site of earliest retrograde activation inside the right atrium was mapped and then cryoablation performed at this site (Fig. 3 and 4). We created aninadvertent complete atrioventricular (AV) block requiringpacemaker implantation in one patient, and now use a smallerand more precise cryoprobe head. The temperature of thecryoprobe was first lowered to O°C at the intended position
Figure 2. Full thickness epicardial incision for division of a difficult or recurrent left posterior Kent bundle. A full thicknessdissection often is not necessary, and epicardial dissection may becombined with one from the endocardial surface.
Figure 3. Endocardial mapping for intraoperative localization ofseptal Kent bundles. The atrioventricular node is at C2-D2 locus.A posterior septal Kent bundle is usually located at C3 or C4.
on the endocardial surface. If AV block did not occur, theprobe head temperature was then lowered to - 70°C for 90seconds at this area. After rewarming, no gross evidenceof the initial lesion remained, but a fibrous scar devoid ofmyocardium was formed.
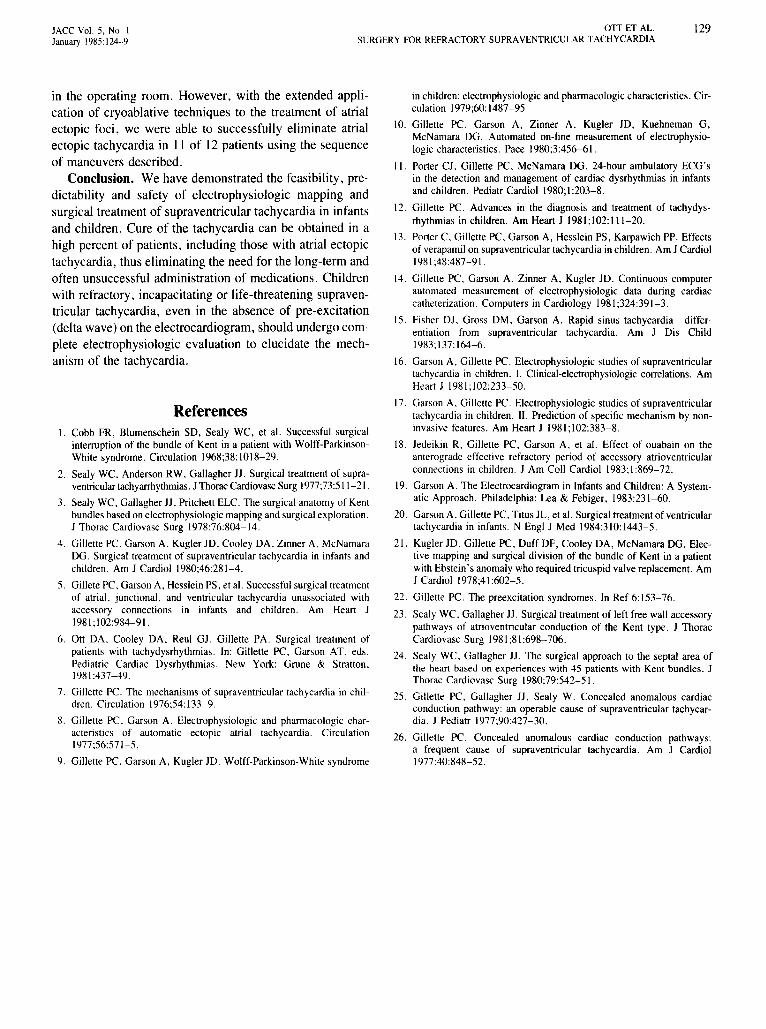
Figure 4. Surgeon's view of a crater (arrows) created by a cryoprobe at the site of a posterior septal Kent bundle. The craterdisappears as the tissue thaws. The tricuspid valve is not visiblein the picture, but is immediately above the crater.
JACC Vol. 5, No. IJanuary 1985: 124-9
OTT ET AL.SURGERY FOR REFRACTORY SUPRAVENTRICULAR TACHYCARDIA
127
Methods for resection or ablation of atrial ectopicfoci. Atrial ectopic foci were approached with a progressivesequence of maneuvers after appropriate mapping (8). Excision of the right or left atrial appendage was performedfirst without cardiopulmonary bypass if the focus was thoughtto be so located. If this failed or the lesion was located onthe free wall of the atrium, we created a series of cryoprobelesions at the suspected epicardial site without placing thepatient on cardiopulmonary bypass. For left-sided foci, cardiopulmonary bypass was often required at this point toobtain adequate exposure. If epicardial application of thecryoprobe failed to ablate the focus, the patient was placedon cardiopulmonary bypass and cardioplegic cardiac arrestwas induced and the atrium opened. We found that endocardial cryoablation of left atrial ectopic foci was often moresuccessful than the epicardial approach. This was possiblydue in part to decompression of the heart during cardiopulmonary bypass and cardioplegic arrest, which eliminatedthe warming effect of the blood-filled atrium. A final attemptat elimination of the focus was disconnection and reconnection of the suspected portion of the atrial wall.
Repeat intraoperative epicardial mapping. After theappropriate attempt at ablation of the atrial ectopic focus oraccessory conduction pathway, epicardial mapping was performed again to check for elimination of the delta wave.The absence of retrograde conduction during ventricularpacing confirmed the success of the operation in those patients who had only retrograde bypass tract conduction preoperatively. Failure to eliminate retrograde conduction,however, was not pathognomonic offailure since some normal AV nodes can conduct in a retrograde fashion. Finally,the ability to induce the Wenckebach phenomenon was proofof successful ablation of the accessory connection becausepatients with an accessory connection will not demonstrateWenckebach conduction.
ResultsAccessory pathways (Kent bundle). Of the 55 patients
who underwent surgical division or cryoablation of an accessory conduction bundle (Kent), 36 (65%) had classicWolff-Parkinson-White syndrome had a delta wave on thesurface electrocardiogram; 19 (35%) had only retrogradeconduction across the accessory bundle and, thus, had anormal surface electrocardiogram during sinus rhythm.
The results of surgical management of these patients aresummarized in Table 2 where they are categorized according to location of the accessory connection. Left posterioror posterolateral Kent bundles were the most common inthis series, occurring in 22 patients (40%). The right anterolateral location was the second most frequent location(19 patients, 34.5%), with septal bundles occurring muchless frequently. One patient died (a 9 year old child with
Table 2. Location of Accessory Conduction Pathway (Kentbundle) and Rate of Recurrence of Tachycardia After Surgery
Location ofRecurrence
Accessory Pathway No. % No. %
Right anterior or lateral 19 34.5 3 16Left posterior or lateral 22 40.0 3 14Posterior septal 10 18 I 10Anterior septal 2 4 0 0Both right and left 2 4 I 50Total 55 8 14.5
multiple ventricular septal defects who had a perioperativestroke).
The recurrence rate at 34.9 months mean follow-up (10to 16%) was relatively constant for patients operated onearly in the series and was similar for each location. However, increasing experience and evolution of the electrophysiologic mapping and surgical techniques resulted in ahigher success rate in the later period of the study. In the25 patients most recently operated on, the recurrence ratewas only 8% (two patients), and we believe the prospectfor further improvement is good. Most failures or recurrences are immediate and we have not seen one later than2 months after the initial procedure. The use of the cryoprobe for accessory bundle ablation in the septal locationshas also simplified the surgical approach, and we have nothad a recurrence of a septal pathway conduction since theadvent of the cryoablation technique (Table 3).
Atrial ectopic foci. Twelve patients were operated onfor atrial ectopic tachycardia using the technique described(Table 4). In five patients, the focus was located in the leftatrial wall, most commonly near the oblique vein of Marshall. Seven foci were in the right atrium. Simple excisionof the right atrial appendage was successful in one patient,and cryoablation was successful in six patients with a leftatrial focus and one with a right atrial focus. A combinationof excision and cryoablation was used in four patients witha focus on the right atrial wall near the atrial appendage.Cardiopulmonary bypass was required in four patients with
Table 3. Results of Cryoablation Surgery for Both AccessorySeptal Pathways and Ectopic Foci
No. Recurrence
Accessory conduction pathwaysRight anterior or lateral 2 0Posterior septal 4 0Anterior septal I 0Total 7 0
Atrial ectopic fociRight atrial 7 ILeft atrial 4 0Total II I

128 orr ar AL.SURGERY FOR REFRACTORY SUPRAVENTRICULAR TACIIYCARDIA
JACC Vol. 5. No. IJanuary 1985:124-9
Discussion
Table 4. Surgical Methods and Results in Patients With AtrialEctopic Tachycardia
atrial ectopic tachycardia, three of whom had a left atrialfocus. Immediate surgical ablation was achieved in II patients (92%) with no late recurren ces . In one patient, tachycardia did not occur spontaneously and could not be inducedin the operating room ; therefore, cryoablation of the suspected site previously delineated during catheter electrophysiologic study was attempted , with early recurrence ofthe tachycardia .
A considerable amount of experimental and clinical datahas been published regarding the electrophysiologic diagnostic evaluation' of supraventricular tachycardia due to accessory conduction pathways in adults . Since the pioneeringwork of Sealy and Gallagher (23,24), the surgical treatm entof these syndromes has become relatively routine in institutions actively involved in electrophysiologic mapping. Untilnow, however, experience in the diagnosis , medical evaluation and management and surgical ablation of these tachycardias in infants and children has been relatively limited .In add ition , successful surgical ablation of atrial ectopictachycardia has rarel y been reported (5).
Division or cryoablation of accessory pathways. Wehave encountered a large number of infants and childrenwho were either incapacitated by tachycardia or thought tohave life-threatening forms of tachycardia. Children withsupraventricular tachycardia usually require treatment because of the severity of the episodes or the chronic natureof the tachycardia which can cause cardiomyopathy . However, the administration of medication to children is inconvenient and the possible side effects of long-term treatmentare undocumented in these patients . In addition, no drughas been successful in the control of atrial ectopic tachycardia.
Therefore , in 1976 we began to treat surgically thosechildren whose tachycardia could not be controlled by anadequate medical regimen or who were believed to have amalignant form of arrhythmia. The results presented in this
study demonstrate the feasibility and clinical success ofelectrophysiologic evalu ation and surgical treatment ofsupraventricular tachycard ia due to a Kent bundle in childrenand infants as young as 4 months of age . Achievement ofthe goal of elimination of tachycardia depends on a teamapproach requiring close cooperation between the cardiacelectrophysiologist and surgeon.
One-third of the patients in this series were found to haveonly retrograde condu ction across the accessory bundle andtherefore demonstrated a normal 12 lead electrocardiogram
when they did not have tachycardia. Primary care physiciansand cardiologists need to be aware that absence of a deltawave on the rest electrocardiogram does not preclude thepossibility of an acce ssory pathway. Therefore, only by ahigh index of suspicion was the possibility of an acce ssoryconduction pathway considered and the appropriate diagnostic measures instigated . Thus , there may be a largernumber of children and adults who have supraventriculartachycardia due to an accessory pathway (Kent bundle) , butwho do not have manife st Wolff-Parkinson-White syndrome . These patients can benefit from proper medi cal orsurgical therapy if they are properly evaluated with electrophys iologic studies (25,26). Increasing experience in mapping and the evolution of new surgical techniques, includingthe use of cryoablation techniques for posterior septal Kentbundle s, have resulted in a simplified and safe approach tothe electrophysiologic evaluation and surgical treatment oftachycardias due to accessory pathways.
Resection or cryoablation of atrial ectopic focus. Wehave also succeeded in accurately mapping and surgicallyablat ing foci causing atrial ectopic tachy cardia, a previ ouslyincurabl e form of suprave ntricular tachycardia. Mapping ofthese lesions is considerably more difficult because of thetwo-dimensional nature of the map. Accessory conductionpathways of the Kent bundle type may be simply localizedby isolating the site at which the pathway crosses the AVgroove and dividing or ablating the lesion at that level. Incontrast, atrial ectopic foci may be located anywhere on thesurface of either the right or the left atrium from where theimpulse may radiate in a variety of directions. In addition ,tachycardias due to an atrial ectopic focus seem to be moresensitive to temperature changes and anesthesia and are notreadily inducible in the operating room . Whereas pat ient swith accessory conduction pathways do not have to be experiencing tachycardia to undergo succe ssful mapping (sinceconduction through the Kent bundle can usually be demonstrated with atrial and ventricular pacing ), atrial ectopictachycard ias cannot be locali zed unless the patient has tachycardia at the time of mapping. The electrophysiologic properties of atrial ectopic tachycardias are such that they cannotbe induced electrically or stimulated pharmacologically . Thus,the one surgical failure in our patients with atrial ectopictachycard ia occurred in a patient who had no tachycardia
57I
7I44
12Atrial ectopic tachycardia
No.Location
LeftRight
RecurrenceTechnique
CryoablationExcisionCombination
Cardiopulmonary bypass required
JACC Vol. 5, No.1January 1985:124-9
OTI ET AL.SURGERY FOR REFRACTORY SUPRAVENTRICULAR TACHYCARDIA
129
in the operating room. However, with the extended application of cryoablative techniques to the treatment of atrialectopic foci, we were able to successfully eliminate atrialectopic tachycardia in 11 of 12 patients using the sequenceof maneuvers described.
Conclusion. We have demonstrated the feasibility, predictability and safety of electrophysiologic mapping andsurgical treatment of supraventricular tachycardia in infantsand children. Cure of the tachycardia can be obtained in ahigh percent of patients, including those with atrial ectopictachycardia, thus eliminating the need for the long-term andoften unsuccessful administration of medications. Childrenwith refractory, incapacitating or life-threatening supraventricular tachycardia, even in the absence of pre-excitation(delta wave) on the electrocardiogram, should undergo complete electrophysiologic evaluation to elucidate the mechanism of the tachycardia.
ReferencesI. Cobb FR, Blumenschein SD, Sealy WC, et at. Successful surgical
interruption of the bundle of Kent in a patient with Wolff-ParkinsonWhite syndrome. Circulation 1968;38:1018-29.
2. Sealy WC. Anderson RW, Gallagher 11. Surgical treatment of supraventriculartachyarrhythmias.J Thorac Cardiovasc Surg 1977;73:511-21.
3. Sealy WC, Gallagher 11, Pritchett ELC. The surgical anatomy of Kentbundles based on electrophysiologic mapping and surgical exploration.J Thorac Cardiovasc Surg 1978:76:804-14.
4. Gillette PC. Garson A. Kugler JD, Cooley DA, Zinner A, McNamaraDG. Surgical treatment of supraventricular tachycardia in infants andchildren. Am J Cardiol 1980;46:281-4.
5. Gillete PC, Garson A, Hesslein PS, et at. Successful surgical treatmentof atrial, junctional, and ventricular tachycardia unassociated withaccessory connections in infants and children. Am Heart J1981;102:984-91.
6. Ott DA, Cooley DA, Reul GJ, Gillette PA. Surgical treatment ofpatients with tachydysrhythmias. In: Gillette PC, Garson AT, eds.Pediatric Cardiac Dysrhythmias. New York: Grone & Stratton,1981:437-49.
7. Gillette Pc. The mechanisms of supraventricular tachycardia in children. Circulation 1976;54:133-9.
8. Gillette PC, Garson A. Electrophysiologic and pharmacologic characteristics of automatic ectopic atrial tachycardia. Circulation1977;56:571-5.
9. Gillette PC, Garson A, Kugler JD. Wolff-Parkinson-White syndrome
in children: electrophysiologic and pharmacologic characteristics. Circulation 1979;60:1487-95.
10. Gillette PC, Garson A, Zinner A, Kugler 10, Kuehneman G,McNamara DG. Automated on-line measurement of electrophysiologic characteristics. Pace 1980;3:456-61.
II. Porter CJ, Gillette PC, McNamara DG. 24-hour ambulatory ECG'sin the detection and management of cardiac dysrhythmias in infantsand children. Pediatr Cardiol 1980;1:203-8.
12. Gillette PC. Advances in the diagnosis and treatment of tachydysrhythmias in children. Am Heart J 1981;102: 111-20.
13. Porter C, Gillette PC, Garson A, Hesslein PS, Karpawich PP. Effectsof verapamil on supraventricular tachycardia in children. Am J Cardiol1981;48:487-91.
14. Gillette PC, Garson A, Zinner A, Kugler JD. Continuous computerautomated measurement of electrophysiologic data during cardiaccatheterization. Computers in Cardiology 1981;324:391-3.
15. Fisher DJ, Gross DM, Garson A. Rapid sinus tachycardia-differentiation from supraventricular tachycardia. Am J Dis Child1983;137:164-6.
16. Garson A, Gillette PC. Electrophysiologic studies of supraventriculartachycardia in children. I. Clinical-electrophysiologic correlations. AmHeart J 1981;102:233-50.
17. Garson A, Gillette PC. Electrophysiologic studies of supraventriculartachycardia in children. II. Prediction of specific mechanism by noninvasive features. Am Heart J 1981;102:383-8.
18. Jedeikin R, Gillette PC, Garson A, et at. Effect of ouabain on theanterograde effective refractory period of accessory atrioventricularconnections in children. J Am Coll Cardiol 1983;1:869-72.
19. Garson A. The Electrocardiogram in Infants and Children: A Systematic Approach. Philadelphia: Lea & Febiger, 1983:231-60.
20. Garson A, Gillette PC, Titus JL, et at. Surgical treatment of ventriculartachycardia in infants. N Engl J Med 1984:310:1443-5.
21. Kugler 10, Gillette PC, Duff DF, Cooley DA, McNamara 00. Elective mapping and surgical division of the bundle of Kent in a patientwith Ebstein's anomaly who required tricuspid valve replacement. AmJ Cardiol 1978;41:602-5.
22. Gillette rc. The preexcitation syndromes. In Ref 6:153-76.
23. Sealy WC, Gallagher 11. Surgical treatment of left free wall accessorypathways of atrioventricular conduction of the Kent type. J ThoracCardiovasc Surg 1981;81:698-706.
24. Sealy WC, Gallagher 11. The surgical approach to the septal area ofthe heart based on experiences with 45 patients with Kent bundles. JThorac Cardiovasc Surg 1980;79:542-51.
25. Gillette PC, Gallagher 11, Sealy W. Concealed anomalous cardiacconduction pathway: an operable cause of supraventricular tachycardia. J Pediatr 1977;90:427-30.
26. Gillette Pc. Concealed anomalous cardiac conduction pathways:a frequent cause of supraventricular tachycardia. Am J Cardiol1977;40:848-52.