surgical radiography section 7 - weber state universityradpacs.weber.edu/images/t_rigby/radt...
TRANSCRIPT

Surgical RadiographySection 7
Tiera Rigby MS, RT(R)(MR) Additional slides provided by Weber Faculty

Sterile● A substance or object that is completely free of
living microorganisms and is incapable of producing any form of organism.
http://www.engenderhealth.org/IP/aseptic/atimages/atm-1.gif
Sterile Areas: • A properly gloved and gowned provider's sterile area extends from the chest to the level of the sterile field. Sleeves are sterile from 5 cm above the elbow to the cuff. • Areas below the level of the draped client are considered nonsterile.
Sterile Team Members● Surgeon: doctor
responsible for pre op diagnosis & care, selection & performance of the surgery, & post op management. The surgeon assumes full responsibility for all medical acts of judgment & for management of the surgical patient.
www.hometown.aol.com

Sterile Team Members● Surgical Assistant: 1st
assistant is a qualified surgeon or resident. Capable of assuming responsibility for the primary surgeon. Helps maintain visibility of surgical site, controls bleeding, closes wounds, and applies dressings.
http://www.compasssurgical.com/side.jpg

Sterile Team Members
● Physician Assistant: Non-physician allied health practitioner who is qualified by academic and clinical training to perform designated procedures in the OR
http://img.coxnewsweb.com/B/02/65/77/image_4877652.jpg
Sterile Team Members
● Certified Surgical Technologist (CST): responsible for maintaining the integrity, safety, and efficiency of the sterile field. Prepares and arranges instruments and supplies and assists by providing required sterile instruments and supplies.
http://www.nbstsa.org/images/surgery3.jpg
Non-Sterile Team Members
● Anesthesiologist: administers anesthetics, monitors physiologic functions, maintains fluid and electrolyte balance, and performs blood replacements.
http://www.algebralab.org/careers/Anesthesiologist/fred.gif

Non-Sterile Team Members
● Circulating Nurse: monitors and coordinates all activities within the OR, provides supplies to the CST, and manages the care of the patient.
http://www.livefromtheheart.org/images/common/popups/or/circulating_nurse.jpg

Non-Sterile Team Members
● Radiographers: Provide interoperative imaging with various types of equipment.
● Other Possible Team Members: biomedical technicians, monitoring technologists, individuals specialized in equipment or monitoring devices necessary for the procedure.
http://www.vetmed.lsu.edu/vth&c/Orthopedics/Images/C-Arm%20flouroscopy%20used%20in%20surgery.SOA.jpg

Operating Suite
● Restricted Area: operating rooms, clean core, or sterile storage areas ● Semirestricted Area: area of the peripheral support, such as hallways or
corridors leading to restricted areas ● Unrestricted Areas: Areas in which street clothes are permitted, such as
outer hallways, family waiting areas, locker rooms, and employee lounges
Hallway : NONRESTRICTED
SEMIRESTRICTED
Supplies & Equipment
OR
OR
SCUB SUB- STERILE
Operating Room Attire● Protective Eyewear: OSHA regulations
require eyewear be worn when contamination from blood or body fluids is possible.
● Masks: Worn at all times in the OR, but are not necessary in semirestricted areas.
● Shoe Covers: Should be worn when contamination from blood or body fluids can be reasonable anticipated.
● Caps: Should cover hair at all times in restricted and semirestricted areas of the OR. Hoods are also available to cover facial hair not contained by cap and mask.
● Gloves: Worn when contact with bloody or body substances is anticipated.
● Radiation Badge: Worn at all times.http://library.thinkquest.org/J0111850/images/scrubs.jpg

Sterile Drapes
Only after a sterile drape has been placed over radiographic equipment can a technologist move the radiographic equipment over the sterile field.
The sterile field should be covered with a sterile drape
Aseptic Technique
Radiographers Responsibility: ● Support and sustain sterile
fields, instruments, and persons.
● Do not walk between sterile fields if possible
● Avoid turning your back toward the sterile field in compromised spaces.
● Watch the front of your clothing and lead shield when next to patient
● Be aware of machinery close to the sterile field.
http://www.wvhospital.com/images/photo_gallery/operating_room2.jpg
Principles involved with manipulation of sterile and unsterile items to prevent or minimize microbiologic contamination.

C-arm • The RT is responsible for radiation safety and protection in the OR
•Stand as far away from the patient, x-ray tube, and useful beam as possible, and stand at 90 degrees to the primary beam and object to reduce exposure from scatter.
•Most scatter occurs on the tube side of the C-arm. Always place the tube under the patient to reduce exposure. If the tube is placed under the table, the pt shielding must also be placed underneath the patient.
http://www.imaging3.com/images_templ/ig-c-arm.gif

C-arm
• Source to skin distance (SSD) should not be less than 12 inches (30 cm).
• Total filtration of the fluoroscopic C arm x- ray beam = at least 2.5 mm Al eq
• A timer must produce an audible signal when fluoroscopic time has exceeded 5 minutes.

Cholangiography

Cholangiography● Bile is drained and major
intrahepatic and extrahepatic ducts are filled with contrast media.
● Determines patency of bile ducts, functional status of the sphincter of the hepatopancreatic ampulla, demonstrates calculi, small intraluminal neoplasms, and stricture or dilation.
http://www.surgery.wisc.edu/general/images/hbp_ercp.jpg

Cholangiography
● C-arm may need to be tilted 15 degrees toward patient’s right side to prevent superimposition of the spine.
● Pt may be tilted to the left or in the Trendelenburg position to aid in the flow of contrast to the complete biliary system.
http://www.jlrmedicalgroup.com/images/rubeis_c-arm_med.jpg
●Pt is supine ●Center the C-arm in the PA projection over the right side of the abdomen below the rib line.

T-tube Cholangiography● If contrast medium
is injected through an inlaying T-tube, the procedure is called a delayed operative or operative T-tube cholangiography.

Transhepatic Cholangiogram
● a thin needle is inserted through the skin (percutaneous) and through the liver (transhepatic) into a bile duct.
http://www.fleshandbones.com/imagebank/showthumbnail.cfm?ISBN=0702015881&filename=S15881-19-f06.jpg
http://www.e-radiography.net/technique/ptc/ptc2.jpg
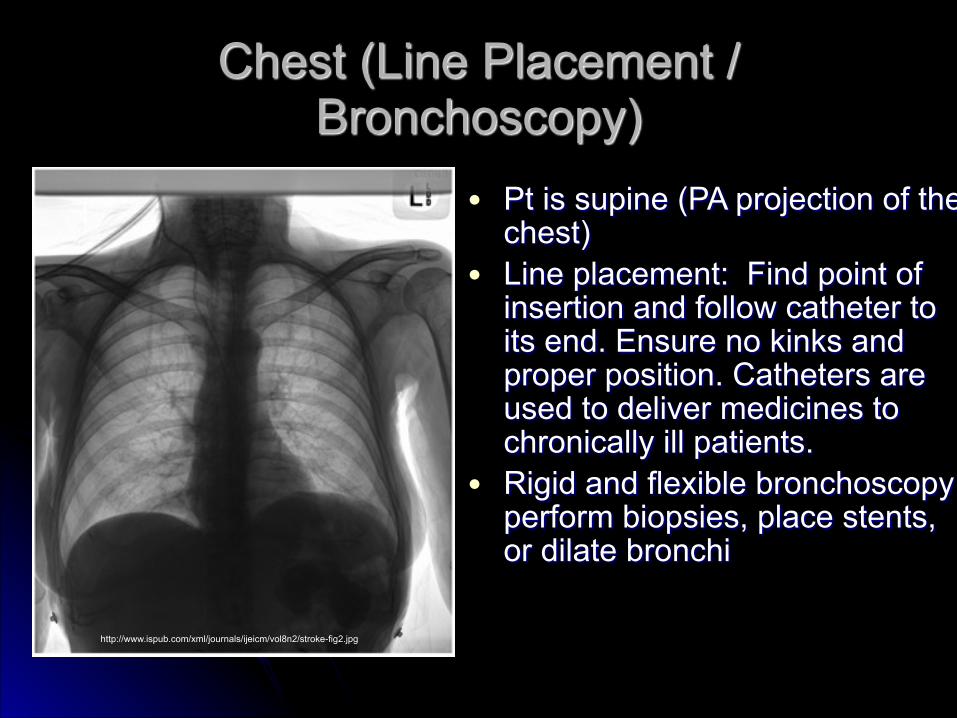
Chest (Line Placement / Bronchoscopy)
● Pt is supine (PA projection of the chest)
● Line placement: Find point of insertion and follow catheter to its end. Ensure no kinks and proper position. Catheters are used to deliver medicines to chronically ill patients.
● Rigid and flexible bronchoscopy: perform biopsies, place stents, or dilate bronchi
http://www.ispub.com/xml/journals/ijeicm/vol8n2/stroke-fig2.jpg

C-Spine (ACDF)Anterior Cervical Discectomy & Fusion
● PA projection: Tilt C-arm 15 degrees cephalic. ● Lateral projection: Rotate C-arm under the table
with the beam parallel to the floor. ● Demonstrates affected C-spine and hardware.
http://uscneurosurgery.com/infonet/graphics/surgery/procedures/acdf/acdf_two_surgeons.JPG http://www2.kumc.edu/neurosurgery/ACDF-PEAK.jpg
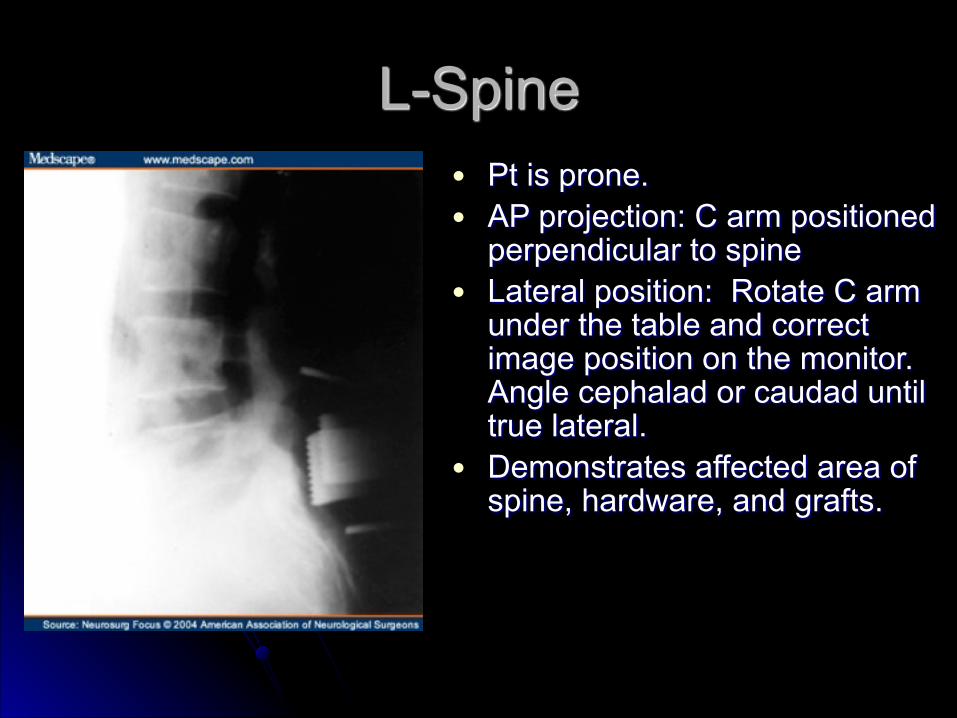
L-Spine● Pt is prone. ● AP projection: C arm positioned
perpendicular to spine ● Lateral position: Rotate C arm
under the table and correct image position on the monitor. Angle cephalad or caudad until true lateral.
● Demonstrates affected area of spine, hardware, and grafts.

Arthroscopic Surgery● Procedure used to
visualize, diagnose, and treat problems inside a joint.
● 6 Most Examined Joints: knee, shoulder, elbow, ankle, hip, and wrist.
● The camera attached to the arthroscope displays the image on a screen.
● Small incision decreases recovery time.

Hip (Cannulated Hip Screws or Hip Pinning
● Pt is supine with legs abducted and the affected leg held in traction (i.e. cross table groin lateral hip)
● A isolation drape or “shower curtain” eliminates the need to drape the c-arm, however; a non sterile bag over the tube is recommended to prevent contamination.
● Position the C-arm between the patient’s legs and center over the affected hip. To obtain lateral images, rotate C-arm under the leg and table.
● Demonstrates all parts of proximal femur and hip joint and hardware.

Hip Resurfacing
● An alternative to total hip replacement. Allows femoral head to be preserved and reshaped. The resurfaced bone is then capped with a metal prosthesis and the socket is fitted with a proshtesis.

Femur Nail
!● Antegrade (supine): Affected leg in
traction, unaffected leg flexed at the knee and hip and raised to allow the C-arm room. C-arm positioned between the patient’s legs.
● Antegrade (lateral): affected leg extended forward to clear opposite leg. C-arm rotated under the table for PA projection. The lateral is completed with the C-arm perpendicular and tilting 5-10 degrees cephalad.
●A rod is inserted into the intramedullary canal to reduce the fracture of the shaft of the femur. This rod or nail can be introduced either antegrade through the greater trochanter or retrograde through the popliteal notch.
http://www.uphs.upenn.edu/ortho/oj/1999/html/PICS/p57f3e.jpg

Femur Nail
● Retrograde (Supine): Injured leg is exposed and the knee flexed and supported with a bump. C arm perpendicular to the patient with cephalad tilt. C-arm rotated under the table for lateral position.
!● Screws will be inserted into the femur
through the rod. When lining up screw holes make sure they appear perfectly round and not oblong. Once inserted, check length in PA projection. They should not protrude excessively from the cortical bone.

Joint Replacement
● The most common reason for having hip or knee replacement is osteoarthritis.

Tibia● Pt is supine with affected
leg flexed at the knee. This allows access to the tibial tuberosity without injuring the patella.
● C-arm angle matches that of the leg and laterals are obtained by rotating C-arm under the table. The surgeon will often manipulate the leg during fluoro.

Femoral/Tibial Arteriogram
● Pt is supine and the leg is manipulated medially and laterally to keep the femur or tibia from obscuring any vasculature.
● Use subtraction or road-mapping feature to remove all structures except the contrast injected into the artery
● Demonstrates stenosis or injury

Humerus● Pt supine or in beach chair
position ● C-arm enters parallel to the
field and the arm is manipulated by the surgeon.
● Demonstrated injury, rod placement, and screw placement.
● Be careful not to strike the head of the patient with the image intensifier.

Transsphenoidal Resection of Pituitary Tumor
● Pt is supine. The C-arm will enter perpendicular to the patient in the lateral position. The beam is centered on the temporal pone to place the sella turcica in the middle of the monitor. Orbits, sphenoid wings, and maxillary sinuses are superimposed.
http://drjho.com/399d7a60.jpg

Mobile Radiography and Post OP
● During mobile radiography or post operative imaging, it is a requirement to show areas of interest, have pertinent anatomy in correct alignment, demonstrate joint spaces, and show the entire length of hardware.