surrey cardiology conference 2014 - st peter's hospital · surrey cardiology conference 2014...
TRANSCRIPT

1
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Surrey Cardiology Conference 2014Latest Therapies in the Management of Atrial Fibril lation
Royal Holloway University of London
Medication vs. Ablation in AFWhich When
and Why?
A. John CammSt. George’s University of London
and Imperial College, LondonUnited Kingdom
A
Declaration of InterestsChairman: NICE Guidelines on AF, 2006; ESC Guidelines on Atri al Fibrillation ,2010 and Update, 2012; ACC/AHA/ESC Guidelines on VAs and SCD; 2006; NICE Guidelines on ACS and NSTEMI, 2012; NICE Guidelines on heart f ailure, 2008; NICE Guidelines on Atrial Fibrillation, 2006; ESC VA and SCD Guidel ines, 2015
Steering Committees: multiple trials including novel anticoagulants
DSMBs: multiple trials including BEAUTIFUL, SHIFT, SIGNFIG Y, AVERROES, CASTLE-AF, ASTAR II, INOVATE, and others
Events Committees: one trial of novel oral anticoagulants and multiple trials of miscellaneous agents with CV adverse effects
Editorial Role: Editor-in-Chief, EP-Europace and Clinical Cardiolog y; Editor, European Textbook of Cardiology, European Heart Jou rnal, Electrophysiology of the Heart, and Evidence Based Cardiology
Consultant/Advisor/Speaker: Astellas, Astra Zeneca, ChanRX, Gilead, Merck, Menarini, Otsuka, Sanofi, Servier, Xention, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi Sankyo, Pfizer, Boston Scient ific, Biotronik, Medtronic, St. Jude Medical, Actelion, GlaxoSmithKline, InfoBionic , Incarda, Johnson and Johnson, Mitsubishi, Novartis, Takeda

2
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Antiarrhythmic Medical Therapies
Upstream therapies
Antiarrhythmic AgentsNew and Old
Amiodarone
Sotalol
ClassIII
Propafenone
Flecainide
ClassIc
Nexteroneand
Budio-darone
Multi-channel blockers
Class Ia: Disopyramide, Quinidine and ProcainamideClass 1b: mexiletine, tocainide
Modified from Savelieva I and Camm AJ. Europace 2008 :10:647–65
Beta blocker
IKAChBlocker
ConnexinModulator
Late Na blockers
SAC Blockers
IKur Blockers
Na+/Ca2+Inhibitor
Na+/H+ Inhibitor
Ryanodine ReceptorModulator
IK1 Blockers
Novel Drugs
Anti inflammatory
New Class III Agents
Azimilide
Dronedarone
Celivarone
Vernakalant
Tedisamil
Dofetilide
Vanoxerine Abandoned
Abandoned
AbandonedUSA only
Chloroquine Xen 0103
Ranolazine
NTC-801
RotigaptideDangaptide
Colchicine
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
SAFE-T Sotalol Amiodarone AF Efficacy Trial
Singh BN et al. NEJM. 2005;352:1861-1872.
• VA Cooperative Study,
• N=665, 20% AF >1 year:
• Amio 267, Sot 261, Placebo 137
Sotalol
Placebo
Amiodarone
Days
Fre
e fr
om
AF
rec
urr
ence
(O
T /
ITT
)
• Follow-up 1year with TTM,
• 1o EP: time to 1st AF recn after CV
0
20
40
60
80
Spontaneous DCC Failed CV Total
Co
nve
rsio
n to
SR
[%
]
AmiodaroneSotalolPlacebo
300 10009008007006005004002001000

3
N5-319 Cumm Presentation
9/25/2014 3:38 PM
100100
8080
6060
4040
2020
00
Time (days)Time (days)
% sinus rhythm% sinus rhythm
60060050050040040030030020020010010000
Probability of remainingin sinus rhythm (N = 403)CTAF
Sotalol
Propafenone
39%
Amiodarone69%
Open labelFollow-up from Day 21
Amiodarone Prevents AF in SCD-HeFT
Singh BN, et al. Am Heart J 2006;152:e7-11
SCD-HeFT
SR n = 2328
AF n = 173
ICD 757 (33%) 65 (38%)
Amiod-arone
771 (33%) 64 (37%)
Placebo 800 (34%) 44 (25%)
New AF 264 (11%) -
Proportion with new AF
0.20
0.15
0
0.05
0.1
0.15
0.2
0.25
0 1 2 3 4 5Years
ICDPlaceboAmiodarone
0.12
ICD: Placebo 1.33 (0.97 – 1.82) 0.044ICD: Amio 1.96 (1.37 – 2.82) 0.001Amio: Placebo 0.68 (0.47 – 0.98) 0.019

4
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Museum of Modern Art
Cornedbeef®200200 mg Amiodarone Hydrochloride Fr. P.
28 TabletsDamienDamienDamienDamien
Hirst H
'I can't understand why some people believe completely in medicine and not in art, without questioning either' (quoted in Damien Hirst). The Last Supper refers to the way in which medicinal drugs are becoming a regular part of everyday life, as common as the food.
Class IA < 0.001Class IC < 0.001Metoprolol
Class III < 0.001Amiodarone < 0.001Dofetilide < 0.001Sotalol < 0.001
Quinidine vs. class IQuinidine vs. sotalolAmiodarone vs. class I < 0.001Amiodarone vs. sotalol < 0.001Sotalol vs. class I
0 0.5 1 1.5 2
AF Recurrence
Odds ratio (95% CI)
Lafuente-Lafuente C, et al. Cochrane Database Syst Rev. 2007;(4):CD005049.
AADs for Prevention of AF After DCCSystematic Review of RCTs
RCTs included in analysis
Total 44
No. of patients 11,322
Placebo controlled
25
Active comparator
14
Persistent AF 38 (60% pts)
PAF/recent onset 6
EF > 50% 41
Lone AF 1
Follow-up 1 year
5
N5-319 Cumm Presentation
9/25/2014 3:38 PM
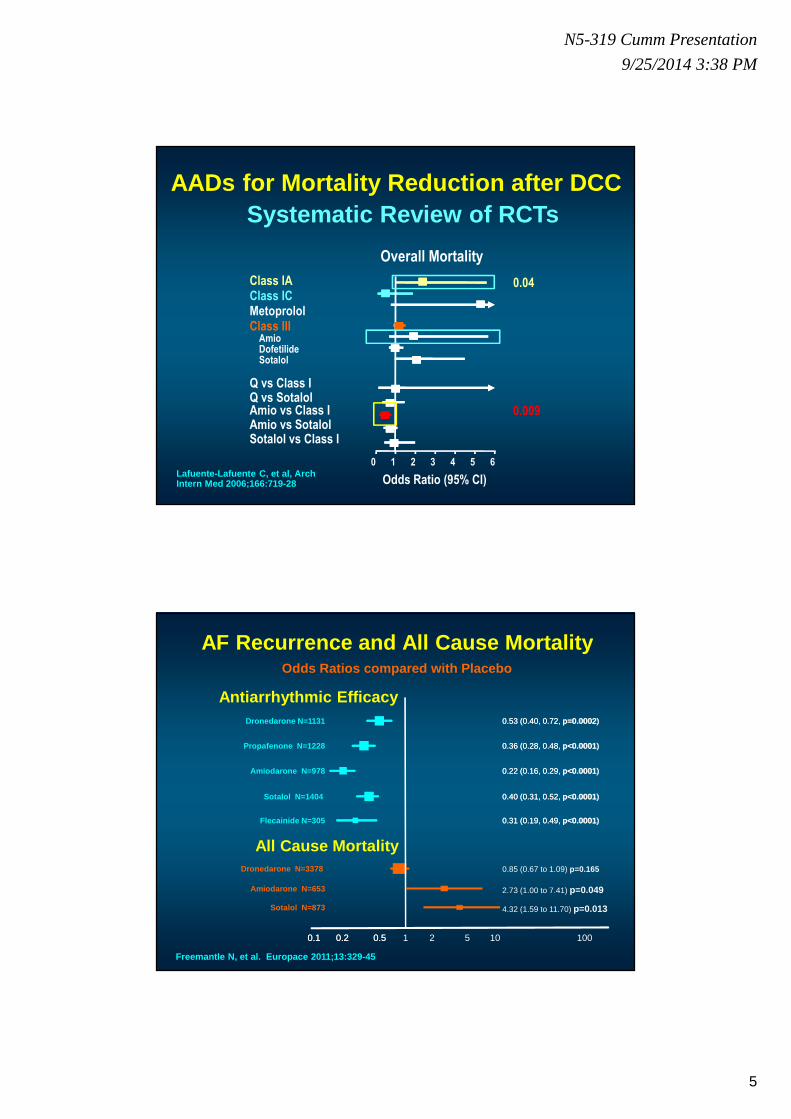
Lafuente-Lafuente C, et al, Arch Intern Med 2006;166:719-28 Odds Ratio (95% CI)
Class IAClass ICMetoprololClass III
AmioDofetilideSotalol
Q vs Class IQ vs SotalolAmio vs Class IAmio vs SotalolSotalol vs Class I
0 1 2 3 4 5 6
0.04
0.009
Overall Mortality
Systematic Review of RCTsAADs for Mortality Reduction after DCC
AF Recurrence and All Cause MortalityOdds Ratios compared with Placebo
0.1 0.2 0.50.1 0.2 0.50.1 0.2 0.5 1 2 5 10 100
Dronedarone N=3378 0.85 (0.67 to 1.09) p=0.165
Amiodarone N=653 2.73 (1.00 to 7.41) p=0.049
Sotalol N=873 4.32 (1.59 to 11.70) p=0.013
0.53 (0.40, 0.72, p=0.0002)Dronedarone N=1131 0.53 (0.40, 0.72, p=0.0002)
0.36 (0.28, 0.48, p<0.0001)Propafenone N=1228 0.36 (0.28, 0.48, p<0.0001)
0.22 (0.16, 0.29, p<0.0001)Amiodarone N=978 0.22 (0.16, 0.29, p<0.0001)
0.40 (0.31, 0.52, p<0.0001)Sotalol N=1404 0.40 (0.31, 0.52, p<0.0001)
0.31 (0.19, 0.49, p<0.0001)Flecainide N=305 0.31 (0.19, 0.49, p<0.0001)
Antiarrhythmic Efficacy
All Cause Mortality
Freemantle N, et al. Europace 2011;13:329-45

6
N5-319 Cumm Presentation
9/25/2014 3:38 PM
ESC Recommendation Class Level
The following antiarrhythmic drugs are recommended for rhythm control in patients with AF, depending on underlying heart disease: • amiodarone• dronedarone• flecainide• propafenone• d.l-sotalol
IIIII
AAAAA
ESC AF GuidelinesAntiarrhythmic Medication for Rhythm Control
Camm J et al. Eur Heart J 2010;31:2369–429
Choice of Oral Antiarrhythmic Drug
Treatment of underlying condition and prevention of remodelling – ACE-I / ARB / statin
HFCHD
Significant structural heart diseaseMinimal or no structural heart disease
HHD
amiodarone
LVHNo LVH
amiodarone
dronedarone / flecainide / propafenone / sotalol
dronedarone
amiodarone
dronedarone
sotalol
European Heart Journal 2012 - doi:10.1093/eurheartj/ ehs253

7
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Improving AAD Safety: Flec-SL Study
Kirchhof P, et al. Lancet 2012;DOI:10.1016/S0140-67 36(12)60570-4
ESC Recommendation
Class Level
Short-term (4 weeks) antiarrhythmic therapy after cardioversion may be considered in selected patients
IIb B
• N = 635, mean age 64 years, 67% hypertension • Flecainide 4 weeks vs long-term• 1o EP: time to persistent AF (telemetry) or death
0
0.2
0.4
0.6
0.8
1
0 50 100 150 200
Months
Pro
baab
ility
eve
nt-f
ree
ControlLong-term RxShort-term Rx
Observational Trials of AF AblationObservational Trials of AF Ablation
59 59.564
69 70 72 7378 80
83 85
77
0
20
40
60
80
100
Free from recurrent AF, %
N= ~2000 Follow-up 6 - 30 months
Pappone C, et al, JACC 2003;42:185-197
0 180 360 540 720 900 10800
20
40
60
80
100
Free from atrial fibrillation, %
Follow-up, days
Hazard ratio 0.30 (95% CI 0.24-0.37)p < 0.001
AAD
Ablation
• Non-randomised• 1171 consecutive pts
(ablation 589)

8
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Treatment of AF: AADs and RFA Systematic Review
Calkins H, et al. Circ Arrhythmia Electrophysiol 20 09;2:349-61
• Studies between 1990 – 2007• Size of the studies ≥ 40 pts• Follow-up ≥ 30 days for AADs and ≥ 7 days
for RFA
Baseline characteristics RFA AAD
# studies (pts) 63 (8789) 34 (6589)
Age, years 55.5 61.6
AF duration, yrs 6.0 3.1
PAF, % 69.8 56.4
PersAF, % 14.9 35.1
AAD failure 2.6 1.7
LVEF, % 57.7 49.0
LA size, mm 41.6 43.7
SHD, % 30.6 49.5
IHD, % 10.0 18.2
CHF, % 15.7 24.6
Prior CABG, % 0 41.6%
Diabetes, % 4.8 12.1
HTN, % 30.3 38.420.0 40.0 60.0 80.0
Efficacy (95% CI), %
Placebo in AAD trials
AAD trials
Single RFA off AAF
Multiple RFA off AAD
Single RFA on AAD
Multiple RFA on AAD
Study # Pts Type of AF Pre AAD
AF free at 1 year
Ablation AAD
Krittayaphong, et al. 2003 30 Paroxysmal,
persistent ≥≥≥≥1 79% 40%
Wazni, et al. 2005, (RAAFT) 70 Mainly
paroxysmal No 87% 37%
Stabile, et al. 2005 (CACAF) 137 Paroxysmal,
persistent ≥≥≥≥2 56% 9%
Oral, et al. 2006 146 Persistent ≥≥≥≥1 74% 4%
Pappone, et al. 2006 (APAF) 198 Paroxysmal ≥≥≥≥2 86% 22%
Jais, et al. 2008, (A4 study) 112 Paroxysmal ≥≥≥≥1 89% 23%
Forleo, et al. 2008 70† Paroxysmal, persistent ≥≥≥≥1 80% 43%
Wilber, et al. 2009 (Thermocool) 167 Paroxysmal ≥≥≥≥1 66% 16%
Packer, et al.2010, (STOP-AF) 245 Paroxysmal ≥≥≥≥1 69.9% 7.3%
Modified from Camm J, et al. Nat Rev Cardiol 2009;6: 332-4
Fre
edo
m f
rom
AF
rec
urr
ence
[%
]
p<0.00166
16
0
20
40
60
80
100
PVI AAD
ThermocoolN = 167
AF Ablation or Antiarrhythmic Drugs?

9
N5-319 Cumm Presentation
9/25/2014 3:38 PM
RCTs of Ablation Versus AADs in AFRCTs of Ablation Versus AADs in AF
Nair GM, et all. JCE 2008
Thai study 0.333 0.112 0.995 0.049
RAAFT 0.204 0.078 0.531 0.001
CACAF 0.483 0.366 0.638 0.000
APAF 0.187 0.113 0.307 0.000
A4 0.258 0.151 0.415 0.000
Morady 0.618 0.387 0.987 0.044
Total 0.331 0.217 0.505 0.000
0.1 0.2 0.5 1.0 2.0
“Inclusion of case series can increase the evidence base and strengthen the credibility of a review of an emerging health technology”
Chambers D, et al. J Clin Epidemiol 2009
ThermoCool AF Trial
Catheter ablation –– Antiarrhythmic drug
HR, 0.3095% CI, 0.19 – 0.47Log-rank P < 0 .001
Follow-up (months)1 2 3 4 5 6 7 8 90
Symptomaticatrial arrhythmia
1.00
0.80
0.60
0.40
0.20
0
Fre
edo
m fr
om
sym
pto
mat
ic a
tria
l arr
hyt
hm
ia
Follow-up (months)1 2 3 4 5 6 7 8 90
Protocol-definedtreatment failure
0
1.00
0.80
0.60
0.40
0.20
Fre
edo
m fr
om
pro
toco
l-d
efin
ed tr
eatm
ent f
ailu
re
HR, 0.2495% CI, 0.15 – 0.39Log-rank P < 0 .001
Follow-up (months)1 2 3 4 5 6 7 8 90
Any atrial arrhythmia1.00
0.80
0.60
0.40
0.20
0
Fre
edo
m fr
om
any
atri
al a
rrh
yth
mia
HR, 0.2995% CI, 0.18 – 0.45Log-rank P < 0 .001
Wilber DJ, et al. JAMA. 2010;303:333-340.
10
N5-319 Cumm Presentation
9/25/2014 3:38 PM
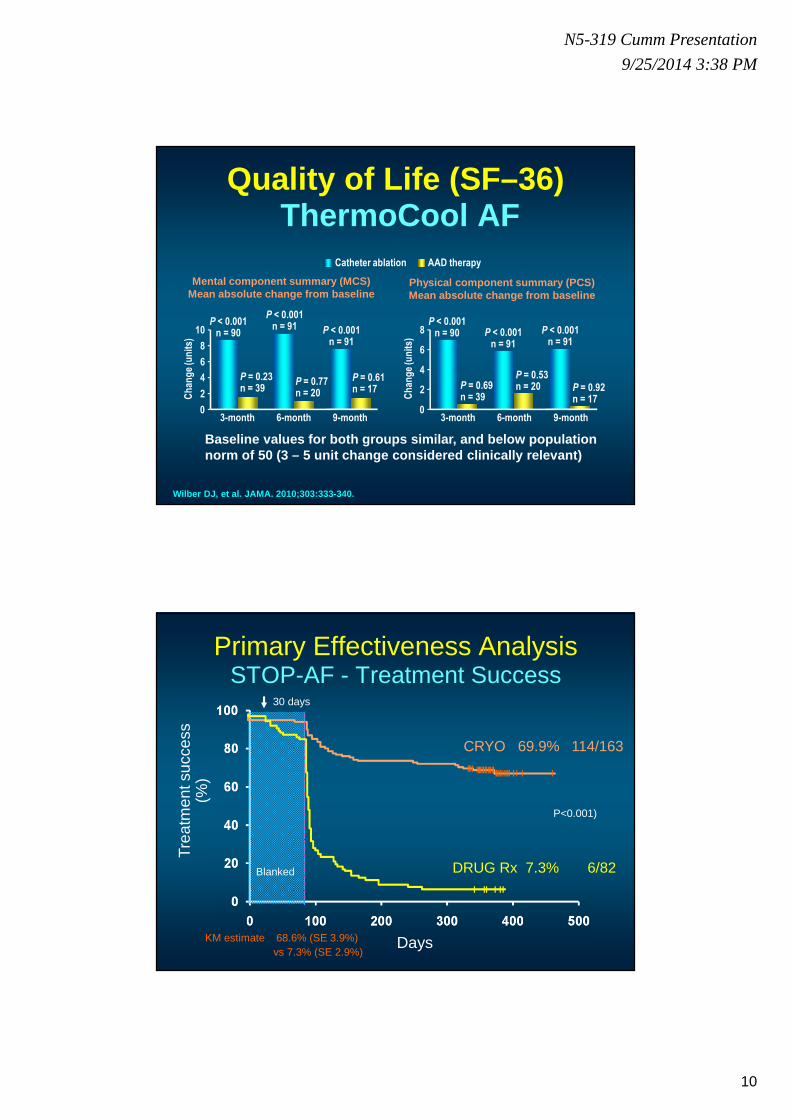
Quality of Life (SF–36)ThermoCool AF
Catheter ablation AAD therapy
3-month 9-month6-month
Mental component summary (MCS)Mean absolute change from baseline
6
8
4
2
0
10
Ch
ang
e (u
nit
s)
6
4
2
0
8
3-month 9-month6-month
Physical component summary (PCS)Mean absolute change from baseline
Ch
ang
e (u
nit
s)
P < 0.001n = 90
P < 0.001n = 91
P < 0.001n = 91
P = 0.23n = 39
P = 0.77n = 20
P = 0.61n = 17
P < 0.001n = 90 P < 0.001
n = 91
P < 0.001n = 91
P = 0.69n = 39
P = 0.53n = 20 P = 0.92
n = 17
Baseline values for both groups similar, and below population norm of 50 (3 – 5 unit change considered clinically relevant)
Wilber DJ, et al. JAMA . 2010;303:333-340.
Primary Effectiveness Analysis STOP-AF - Treatment Success
Tre
atm
ent s
ucce
ss
(%)
Days
P<0.001)
vs 7.3% (SE 2.9%)
CRYO 69.9% 114/163
Blanked DRUG Rx 7.3% 6/82
30 days
KM estimate 68.6% (SE 3.9%)

11
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Summary of All Adverse Events (Intention-to-Treat)
Type of Adverse Event CRYO(n = 163)
DRUG(n = 82)
Stroke 4 2.5% 1 1.2%
TIA 3 1.8% 1 1.2%
Tamponade 1 0.6% 1 1.2%
Myocardial infarction 2 1.2% 0 0.0%Hemorrhage requiring transfusion 3 1.8% 1 1.2%
New atrial flutter 6 3.7% 13 15.9%Atrial esophageal fistula 0 0.0% 0 0.0%
Death 1 0.6% 0 0.0%
New or worsened AV fistula 2 1.2% 0 0.0%Pseudoaneurysm 1 0.6% 1 1.2%
Phrenic nerve palsy 22 13.5% 6 7.3%
Persistent phrenic nerve palsy 4 2.5% 0 0.0%PV stenosis 5 3.1% 2 2.4%
Author Study typePts
total (n)Ablation strategy
FU (months, mean + SD)
Arrhythmia free survival (%)
Comp-lications (%)
Gaita2008
randomised 1:1
PVI vs. PVI + LL 204 PVI / PVI+LL41.4±6.2 / 39.7±5.5 41 2%
Fiala2008
randomised 1:1
seg. PVI vs. circumfer. PVI
110 PVI 48±8 56 1%
Bertaglia2009
observational 177 PVI / PVI+LL 49.7±13.3 58 n.r.
Bhargava2009
observational 1404 PVI / PVI+LL 59±16 73 3%
Tsou2010*
observational 123 PVI 71±18 71 n.r.
Wokhlu2010
observational 774 PVI / PVI+LL 36±22.8 64 n.r.
Ouyang2010
observational 161 PVI 57.6 47 2%
Weerasooriya2011
observational 100 PVI / PVI+LL 60 32 6%
Longterm Outcome after PVI
PVI: Pulmonary vein isolation; LL: left lines; n.r.: not reported; seg.: segmental; circumfer.: circumferential *only patients free from AF one year after ablation were included! Regarding to a total of 239 patients who underwent AF ablation: success rate after 71±18 months was only 36.4%!

12
N5-319 Cumm Presentation
9/25/2014 3:38 PM
In-hospital Complications Associated with Catheter Ablation of AF in USA
Complication Overall
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 P value
Any procedural complications
6.29 5.33 5.53 6.01 7.17 6.32 5.10 6.17 6.66 5.93 6.49 7.48 0.108
In hospital death
0.42 0.44 0.55 0.63 0.30 0.61 0.15 0.45 0.53 0.27 0.52 0.47 0.492
Neurological (PostopStroke/TIA)
1.02 0.89 1.11 1.79 1.57 1.13 0.68 1.39 0.53 0.78 0.93 1.20 0.013
Postop-hemorrhage
3.38 1.78 2.54 2.53 2.39 3.38 2.77 3.13 3.52 3.75 3.46 4.90 <0.001
Postop-hemorrhage requiring transfusion
0.58 0.30 0.22 0.32 0.30 0.61 0.34 0.45 0.87 0.65 0.44 1.03 0.020
Deshmukh A, et al. Circulation. published online Se ptember 23, 2013;
93,801 AF ablations from 2000 to 2010 . Overall frequency of complications 6.29% with combined cardiac complications (2.54%) and neurological complications (1.02%).
In-hospital mortality was 0.46%. Annual operator (<25 procedures) and hospital volume (<50 procedures) were significantly associat ed with adverse outcomes .
Atrial Fibrillation Ablation Pilot StudyEURObservational Research Programme
1300 pts 12 months FU
4 deaths19 unknown status
90 lost to FU
333 patients with at least 1 recurrence
(26.1%)
944 patients with no recurrence
(73.7%)
AADS: 43.4%No AADs: 56.6%
Adverse Events
In Hosp
12 months
CV 3.3% 2.02%
Brady+PM 0.2% 1.02%
P Vascular 1.3% 0.71%
AV fistula 0.43% 0.47%
Misc
PVsten - 0.08%
PNI 0.14% 0.16%
Eso Ulcer 0.07% -
Death 0.07% 0.31%
Overall 7.7% 2.6%
Brugada J, et al. ESC 2012

13
N5-319 Cumm Presentation
9/25/2014 3:38 PM
294 Patients Randomized
146 Assigned to RFA
140 Underwent RFA (96%)
After 24 months
N=140; 223 RFA procedures (1.6±0.7)
On AAD: N=13/138 (9%) (IC: 10, III: 3)
Withdrawn N=5
Died N=3
665 7D Holter
recordings69 underwent
repeated RFA
148 Assigned to AAD
146 Started AAD (99%)
After 24 months
N=54; 87 RFA procedures (1.6±0.7)
On AAD: N=100 /137 (73%) (IC: 86, III:14)
Withdrawn N=7
Died N=4
666 7D Holter
recordingsTreatment with
1.24±0.48 AAD’s
MANTRA-PAFFirst Treatment for PAF
Nielsen JC et al AHA 2010
MANTRA-PAF
No significant difference between ablation and drug -therapy groups in the cumulative burden of AF (90th percentile of arrhyth mia burden, 13% and 19%, respectively; P = 0.10) or the burden at 3, 6, 12, or 18 months
Primary end point : cumulative burden of AF (i.e., percentage of time in AF on Holter-monitor recordings)
Nielsen JC et al. NEJM 2012;367:1587-95
● 294 pts randomized; 1.6 RFAs/pt● 194 pts followed for 24 months;
7D Holter

14
N5-319 Cumm Presentation
9/25/2014 3:38 PM
MANTRA-PAFFirst Treatment for PAF - Results after 24 Months
Nu
mb
er
of
pa
tie
nts
P=0.012
P=0.004140
120
100
80
60
40
20
0
RFA AAD
SAEs RFA AAD
Death 3 4
Stroke 1 0
TIA 1 1
PV stenosis 1 0
Tamponade 3 0
Pericardial
effusion0 1
?perforation 1 0
Atrial flutter, 1:1 0 2
Afl/AT 3 3
CHF 0 2
Total 25 22
No AFSymptomatic Any AFNielsen JC et al AHA 2010
294 pts randomized; 1.6 RFAs/pt194 pts followed for 24 months; 7D Holter
RAAFT-2Radiofrequency Ablation versus AADs for
paroxysmal AF first-line Therapy
• 127 treatment-naïvepatients
• Follow-up for up to 24 months
• Recurrence of AF was less frequent in patients treated with radiofrequency ablation compared with AADs
Morillo CA, et al. JAMA 2014;311(7):692–700
Time to first recurrence of symptomatic atrial tach yarrhythmias
15
N5-319 Cumm Presentation
9/25/2014 3:38 PM
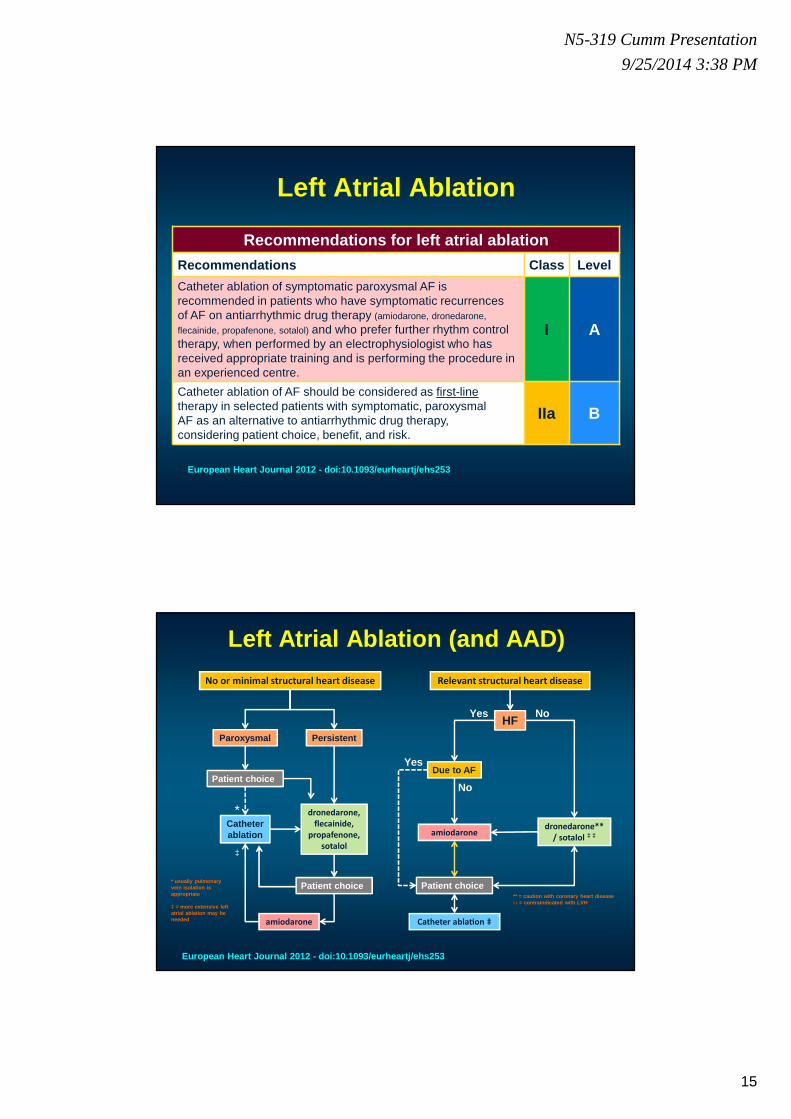
Recommendations for left atrial ablation
Recommendations Class Level
Catheter ablation of symptomatic paroxysmal AF is recommended in patients who have symptomatic recurrencesof AF on antiarrhythmic drug therapy (amiodarone, dronedarone,
flecainide, propafenone, sotalol) and who prefer further rhythm control therapy, when performed by an electrophysiologist who has received appropriate training and is performing the procedure in an experienced centre.
I A
Catheter ablation of AF should be considered as first-linetherapy in selected patients with symptomatic, paroxysmalAF as an alternative to antiarrhythmic drug therapy,considering patient choice, benefit, and risk.
IIa B
Left Atrial Ablation
European Heart Journal 2012 - doi:10.1093/eurheartj/ ehs253
Left Atrial Ablation (and AAD)
No or minimal structural heart disease
Paroxysmal Persistent
amiodarone
dronedarone,
flecainide,
propafenone,
sotalol
Catheter ablation
Patient choice
‡
*
Patient choice
Relevant structural heart disease
HF
dronedarone**
/ sotalol ‡ ‡amiodarone
Catheter abla-on ‡
NoYes
Due to AFYes
No
Patient choice* usually pulmonary vein isolation is appropriate
‡ = more extensive left atrial ablation may be needed
** = caution with coronary heart disease ‡ ‡ = contraindicated with LVH
European Heart Journal 2012 - doi:10.1093/eurheartj/ ehs253

16
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Consensus Indications for Catheter Ablation for Atrial Fibrillation
RecommendationsSymptomatic AF refractory or intolerant to at least one Class 1 or 3 antiarrhythmic medication
Class Level
Paroxysmal: Catheter ablation is recommended*
I A
Persistent: Catheter ablation is reasonable IIa BLongstanding Persistent:
Catheter ablation may be considered
IIb B
Symptomatic AF prior to initiation of antiarrhythmic drug therapy with a Class 1 or 3 antiarrhythmic agent
Class LevelParoxysmal: Catheter ablation is reasonable IIa B
Persistent: Catheter ablation may be considered
IIb C
Longstanding Persistent:
Catheter ablation may be considered
IIB C
HRS/EHRA/ECAS Consensus Document 2012 Europace, He art Rhythm and JICE
Calkins H,… Camm AJ…
2014 AHA/ACC/HRSGuideline for the Management of Patients With AF
5.6. AF Catheter Ablation to Maintain Sinus Rhythm: Recommendations
Class IAF catheter ablation is useful for symptomatic paro xysmal AF refractory or intolerant to at least 1 class I or III antiarrhyth mic medication when a rhythm control strategy is desired (155-161). (Level of Evidence: A)
Class IIaIn patients with recurrent symptomatic paroxysmal AF , catheter ablation is a reasonable initial rhythm control strategy prior to therapeuti c trials of antiarrhythmic drug therapy , after weighing risks and outcomes of drug and ablation therapy. (Level of Evidence: B)
Class III: HarmAF catheter ablation should not be performed in pat ients who cannot be treated with anticoagulant therapy during and following the procedure. (Level of Evidence: C)
AF catheter ablation to restore sinus rhythm should not be performed with the sole intent of obviating the need for anticoagulation . (Level of Evidence: C)

17
N5-319 Cumm Presentation
9/25/2014 3:38 PM
On-going AF Ablation TrialsMajor CV Outcomes
Acronym Study Title PI N Endpoint
CASTLE-AF
Catheter Ablation versus Standard conventional Treatment in patients with LEft ventricular dysfunction and Atrial Fibrillation
Brachmann 400All-cause death + heart failure hospitalisations
CABANA
Catheter ABlation versus ANtiarrhythmic drug therapy for Atrial fibrillation
Packer 2000
Composite of total mortality, disabling stroke, serious bleeding, or cardiac arrest
EAST Early Atrial fibrillation Stroke Prevention Trial Kirchhof 3000
All cause mortality + cardiovascular hospitalisations
1° ablation• PVI• WACA• CFEGM• GP
Drug Rx• Rate• Rhythm• w/ antico-
agulation
R
2000 patients: ≥≥≥≥65 yr of age<65 yr w/ ≥≥≥≥1 CVA risk factor2000 patients: ≥≥≥≥65 yr of age<65 yr w/ ≥≥≥≥1 CVA risk factor
Secondary analyses1) NSR vs AF2) ± underlying
heart disease3) AF type
(parox, pers, perm)4) D/C anticoagulation
Recent onset AFEligible for ablation
and drug Rx
Recent onset AFEligible for ablation
and drug Rx
Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation
CABANA Trial Design
10 Endpoint: total mortality and CV hospitalisations
After Douglas Packer

18
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Composite primary endpoint:CV death, stroke / TIA,
CHF or ACS hospitalization
Early rhythm controlAntiarrhythmic drug therapy; pulmonary vein isolation (PVI)
In case of AF recurrence:Re-PVI, adaptation of antiarrhythmic
drug therapy
Usual careRate control, supplemented by
rhythm control only in symptomatic patients despite optimal rate control therapy, as mandated by the 2010
ESC guidelines for AF
Study procedures
Outpatient follow-up at months 12, 24, 36 (both study groups)
Antithrombotic therapyTherapy of underlying heart disease (both study groups)
Pre-study screening
RPatients without known AF but
positive on ECG screening
Patients with recent-onset AF
(≤ 1 year)
Patients at risk for cardiovascular events
e.g., recruited in cardiology offices, medicine offices,
emergency departments, cardiology departments, neurology
departments, hypertension clinics,
pacemaker clinics, and others
ECG monitoring of therapy
Early treatment of Atrial fibrillation for Stroke and cardiovascular complications prevention Trial
EAST:
Kirchhof P, et al.
Rhythm Control and Mortality in AFLong term benefit
• Population-based administrative databases, Quebec
• 26,130 patients
• 1999 to 2007
• > 65 years
• AF hospitalization
• No AF-related drug prescriptions < 1year < admission (first documented AF)
• AAD < 7 days > discharge
Ionescu-Ittu R, et al. Arch Intern Med. 2012;172:99 7-1004.
HR
for
rhyt
hm v
s ra
te (
95%
CI)
Years since initiation of AF treatment
0.8
1.0
1.2
1.4
0.6
Lower mortality with rate control
Treatmentinitiation
1 2 3 4 5 6 7 8
Lower mortality with rhythm control
No difference
19
N5-319 Cumm Presentation
9/25/2014 3:38 PM
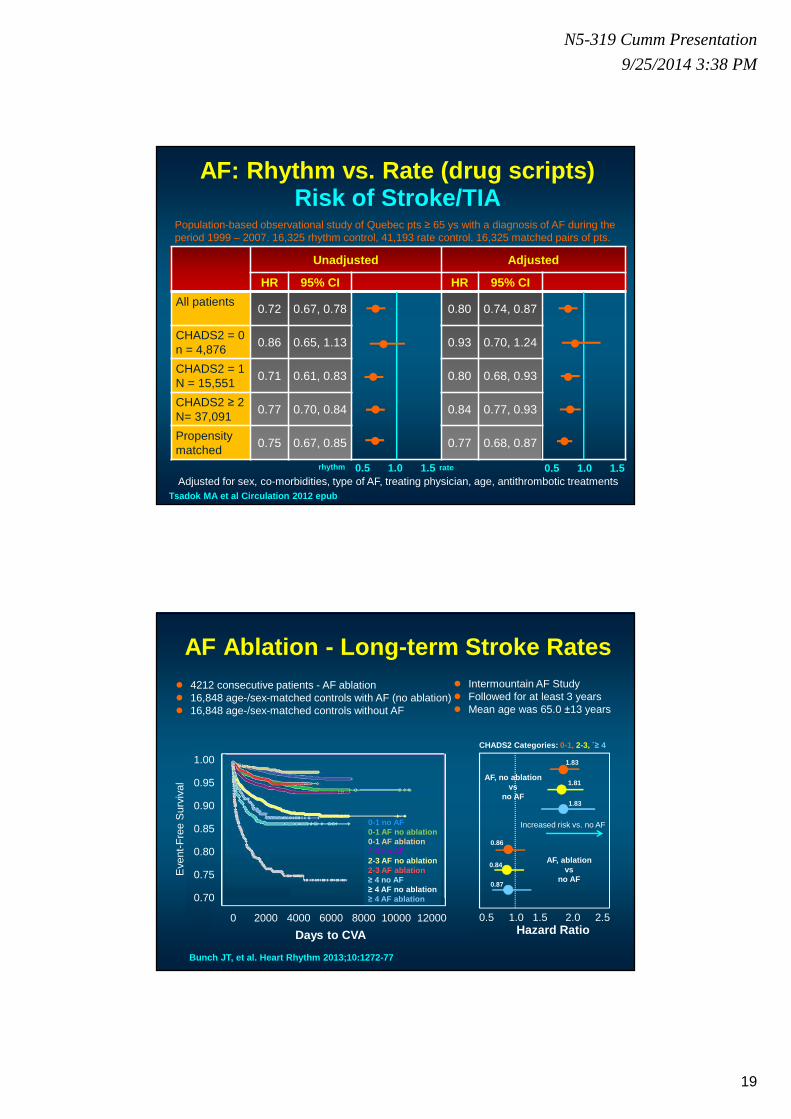
AF: Rhythm vs. Rate (drug scripts)Risk of Stroke/TIA
Unadjusted Adjusted
HR 95% CI HR 95% CI
All patients0.72 0.67, 0.78 0.80 0.74, 0.87
CHADS2 = 0n = 4,876
0.86 0.65, 1.13 0.93 0.70, 1.24
CHADS2 = 1N = 15,551
0.71 0.61, 0.83 0.80 0.68, 0.93
CHADS2 ≥ 2N= 37,091
0.77 0.70, 0.84 0.84 0.77, 0.93
Propensity matched
0.75 0.67, 0.85 0.77 0.68, 0.87
Adjusted for sex, co-morbidities, type of AF, treating physician, age, antithrombotic treatments0.5 1.0 1.5 0.5 1.0 1.5
●
●
●
●
●
●
●
●
●
●
Tsadok MA et al Circulation 2012 epub
Population-based observational study of Quebec pts ≥ 65 ys with a diagnosis of AF during the period 1999 – 2007. 16,325 rhythm control, 41,193 rate control. 16,325 matched pairs of pts.
rhythm rate
AF Ablation - Long-term Stroke Rates
Bunch JT, et al. Heart Rhythm 2013;10:1272-77
● 4212 consecutive patients - AF ablation● 16,848 age-/sex-matched controls with AF (no ablation)● 16,848 age-/sex-matched controls without AF
CHADS2 Categories: 0-1, 2-3, `≥ 4
0.5 1.0 1.5 2.0 2.5Hazard Ratio
AF, no ablationvs
no AF
AF, ablationvs
no AF
1.83
1.81
1.83
0.86
0.84
0.87
Increased risk vs. no AF
● Intermountain AF Study● Followed for at least 3 years● Mean age was 65.0 ±13 years
Eve
nt-F
ree
Sur
viva
l
0 2000 4000 6000 8000 10000 12000
Days to CVA
0-1 no AF0-1 AF no ablation0-1 AF ablation2-3 no AF2-3 AF no ablation2-3 AF ablation≥ 4 no AF≥ 4 AF no ablation≥ 4 AF ablation
1.00
0.95
0.90
0.85
0.80
0.75
0.70
20
N5-319 Cumm Presentation
9/25/2014 3:38 PM
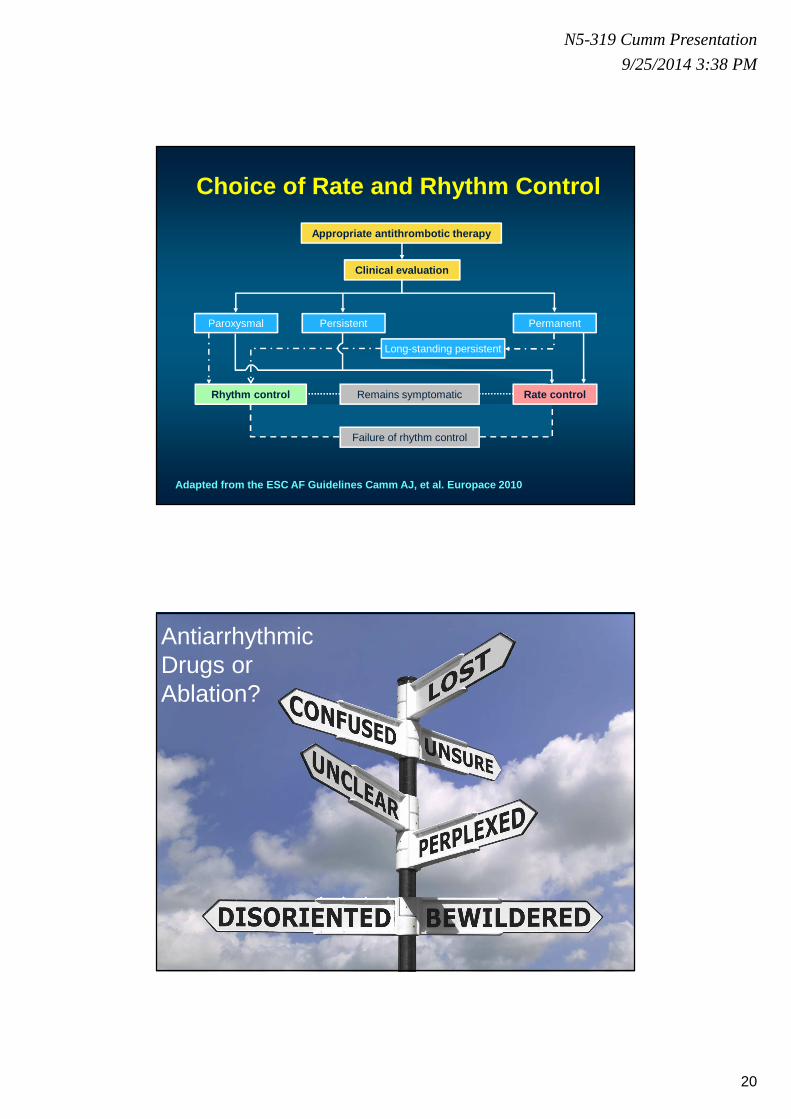
Clinical evaluation
Appropriate antithrombotic therapy
Rhythm control Rate control
Paroxysmal Persistent Permanent
Remains symptomatic
Failure of rhythm control
Choice of Rate and Rhythm Control
Long-standing persistent
Adapted from the ESC AF Guidelines Camm AJ, et al. Europace 2010
Antiarrhythmic Drugs or Ablation?
21
N5-319 Cumm Presentation
9/25/2014 3:38 PM
Thank you for your attention
What’s the premise for AADs?
• Less invasive approach� highly beneficial for younger patients
� this is often preferential for patients compared to ablation
• Lower risk of complications than for ablation
• AF progression can be halted and sinus rhythm achieved
• The Belgian Health Care Knowledge Centre� Retrospective data from 830 AF ablation patients (2007-2008)
� Ablation has high associated costs (€9600) but may be cost-effective
� Real-world effectiveness of ablation, in Belgium, is disappointing
� Raised serious questions about the evidence that underpins current European guidelines
Van Brabandt H, et al. Europace 2013;15:618–19
22
N5-319 Cumm Presentation
9/25/2014 3:38 PM
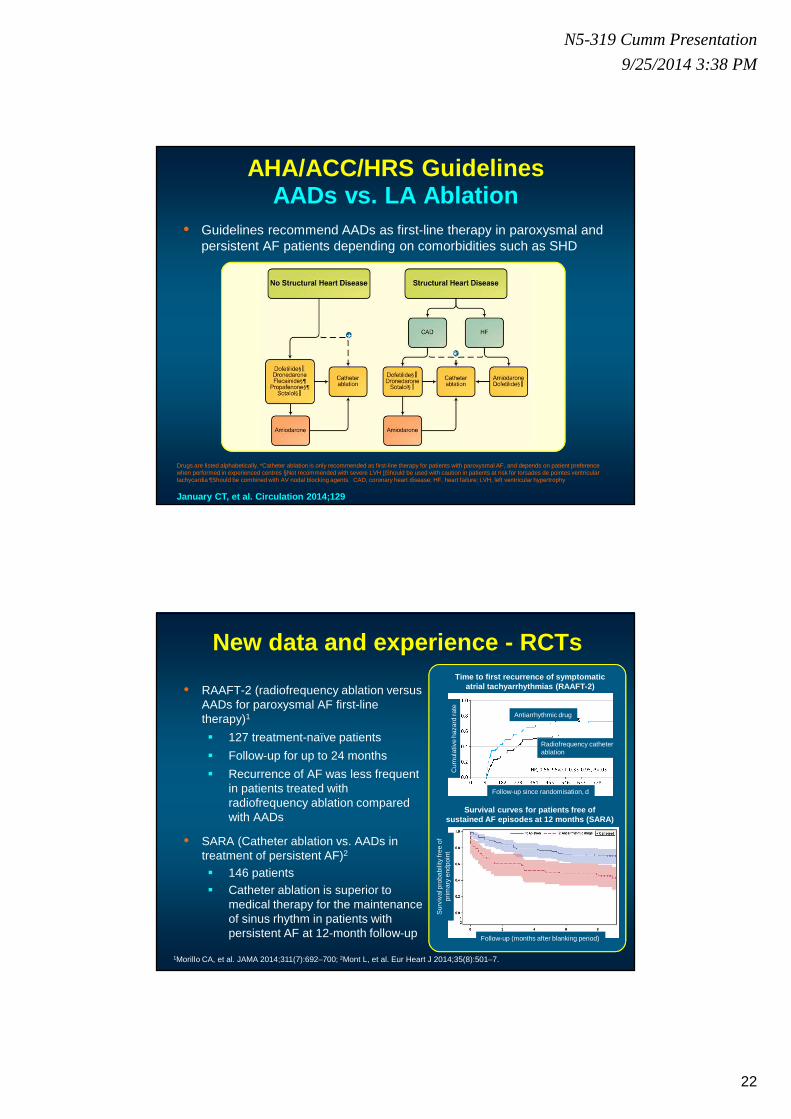
AHA/ACC/HRS Guidelines AADs vs. LA Ablation
• Guidelines recommend AADs as first-line therapy in paroxysmal and persistent AF patients depending on comorbidities such as SHD
Drugs are listed alphabetically. *Catheter ablation is only recommended as first-line therapy for patients with paroxysmal AF, and depends on patient preference when performed in experienced centres §Not recommended with severe LVH ||Should be used with caution in patients at risk for torsades de pointes ventricular tachycardia ¶Should be combined with AV nodal blocking agents. CAD, coronary heart disease; HF, heart failure; LVH, left ventricular hypertrophy
January CT, et al. Circulation 2014;129
**
New data and experience - RCTs
• RAAFT-2 (radiofrequency ablation versus AADs for paroxysmal AF first-line therapy)1
� 127 treatment-naïve patients
� Follow-up for up to 24 months
� Recurrence of AF was less frequent in patients treated with radiofrequency ablation compared with AADs
• SARA (Catheter ablation vs. AADs in treatment of persistent AF)2
� 146 patients� Catheter ablation is superior to
medical therapy for the maintenance of sinus rhythm in patients with persistent AF at 12-month follow-up
1Morillo CA, et al. JAMA 2014;311(7):692–700; 2Mont L, et al. Eur Heart J 2014;35(8):501–7.
Time to first recurrence of symptomatic atrial tachyarrhythmias (RAAFT-2)
Survival curves for patients free of sustained AF episodes at 12 months (SARA)
Cum
ulat
ive
haza
rd r
ate
Follow-up since randomisation, d
Antiarrhythmic drug
Radiofrequency catheter ablation
Sur
viva
l pro
babi
lity
free
of
prim
ary
endp
oint
Follow-up (months after blanking period)