survival methods for the equine practitioner in equine ... in small jars (for preserving biopsy...
TRANSCRIPT

Close this window to return to IVIS
www.ivis.org
Proceedings of the 53rd Annual Convention of
the American Association of Equine Practitioners
December 1–5, 2007, Orlando, Florida
Program Chair: Eleanor M. Green, DVM, DACVIM, DABVP
ACKNOWLEDGMENTS Dr. Stephen M. Reed, Educational Programs Committee Chair
Carey M. Ross, Scientific Publications Coordinator
Published by the American Association of Equine Practitioners
www.aaep.org
ISSN 0065–7182 © American Association of Equine Practitioners, 2007

Survival Methods for the Equine Practitioner inEquine Ophthalmology
Dennis E. Brooks, DVM, PhD; Maria E. Kallberg, DVM, PhD;Mary E. Utter, DVM, PhD; Caryn Plummer, DVM; and Ann E. Dwyer, DVM
Authors’ addresses: Department of Ophthalmology, University of Florida, 2015 SW 16th Avenue,Gainesville, FL 32608 (Brooks, Kallberg, Plummer); Department of Ophthalmology, University ofPennsylvania, New Bolton Center, 382 West Street Road, Kennnett Square, PA 19348 (Utter); andGenesee Valley Equine Clinic, 925 Chili Scottsville Road, Scottsville, NY 14546; e-mail;[email protected]. © 2007 AAEP.
1. Introduction
Equine practitioners can develop solid expertise infield ophthalmology with practice and effort. Get-ting known as someone who has a special interest ineyes is a great way to build a client base: eye prob-lems are a serious concern to owners and are nottypical “turf” for non-veterinary caregivers like mas-sage therapists, holistic therapists, lay dentists, andfarriers, although there are equine iridologists outthere! Some problems will always have to be re-ferred to specialists, but the average practitionercan examine, diagnose, and treat 85% of the eyeproblems that are seen in the field.
Items to carry for diagnosis and treatment of eyeproblems:
● direct ophthalmoscopea
● transilluminator,b and/or penlightc
● 14-D magnifying lensd
● digital camera (4.0-megapixel camera orhigher)
● Hand-held slit-lampe (optional)● applanation tonometerf (optional)
● fluorescein and rose bengal dye strips (carryright in scope case)
● Schirmer tear test strips (carry right in scopecase)
● tropicamideg —topical agent to dilate pupils● proparicaine (topical anesthetic); carbocaine
(injectible local anesthetic)● 30-ml bottles of 1 part Betadyne to 50 parts
saline. Small bottles of sterile saline are avail-able through www.floridainfusion.com; the 2%solution can be mixed in house. Larger pourbottle of same for cleaning periorbital region
● sterile cotton swabs bundled six swabs to apack
● sterile individual polyester swabsh
● sterile 4 4 gauze, non-sterile 4 4 gauze,sterile gloves
● scalpel blades, packed in sterile sleeves (anysize as blunt end is used)
● 2-mm biopsy punches (for occasional “scoop-ing” of foreign bodies)
● slide boxes with four microscope slides to a box(for cytology specimens)
374 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
NOTES
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

● formalin in small jars (for preserving biopsyspecimens)
● “write on” plastic bags—4 6 in (to dispensemedications and clarify treatment schedules)
● thioglycollate culture broth tubes or agarplates, Porta-cult transport media
● serum separator tubes (to prepare autologousserum)
● fine suture material: 1-0 through at least 4-0,some use up to 6-0
● sedatives (xylazine, butorphanol tartrate,detomidine)
● subpalpebral lavage systemsi
● adhesive tape (to make butterfly holding wingsfor lavage systems)
● 20-gauge catheters and IV catheter caps (touse with lavage system)
● tongue depressors (to use with lavage systems)● tuberculin and 3-ml syringes as well as larger
sizes● 25- and/or 23-gauge needles● prescription pad● halogen light on tripod or hook, and headlampj
Drugs to carry in your truck or buy locally fortreatment of eye problems.
● antibiotic ointments: triple antibiotic, genta-micin, chloramphenicol—most others need tobe scripted out at pharmacies
● corticosteroid ointments: triple antibioticwith 1% hydrocortisone, triple with 0.1%dexamethasone
● antifungal medications to buy from pharma-cies: OTC Monistat, clotrimazole, silver sul-fadiazine (BE CAREFUL—may be best fortemporary use until compounded products canship; off-label use; may be irritating)
● atropine ointment● injectable antibiotics to make fortified solu-
tions or inject SC: cephazolin 1-g bottles, gen-tamicin 100 mg/ml, amikacin 50 or 250 mg/ml
● 10-ml bottles of saline for mixing fortifiedsolutions
● artificial tears● cyclosporine ointment● timolol maleate 0.5% drops● be ready to prescribe many other drugs such as
5% NaCl, timolol maleate combined with dor-zolamide (0.1% diclofenac, flurbiprofen, 0.3%tobramycin, oxacillen, ciprofloxacin, itracon-azole, or idoxyuridine. Some specializeddrugs may be kept at your clinic and dis-pensed/prepared on an as needed basis, likeEDTA, topical adequan in artificial tears, for-tified antibiotic preparations, etc. Serum willneed to be centrifuged at your clinic. Somedrugs (e.g., 1% liquid miconazole, idoxuridine,itraconazole) are available only through com-pounding pharmacies. University pharma-
cies are often good sources for unusualophthalmic preparations.
● non-steriodal anti-inflammatory drugs (NSAIDs):injectable and oral flunixin meglumine andphenylbutazone
● systemic corticosteroids: injectable and oraldexamethasone
Some tips regarding examination and diagnostictests:
● Owners calling about horses with painful eyesor eye trauma should be told to have a darkexamination area available and to have fourbales of shavings or hay ready to use as headrest for standing surgery/diagnostics. A stoolor other step stand may help if the horse is tallor the vet is short!
● Horses are often most relaxed if examined ini-tially in stalls. Instruct the handler to standon the side opposite to the side being exam-ined. Always examine both eyes fully, even ifthere is an obvious problem in just one. Hav-ing the holder tilt the head one direction oranother by applying pressure on the ear willhelp expose desired site of the eye.
● Chemical restraint is often needed but can beshort lived. Be organized with all diagnosticand treatment supplies at hand before sedat-ing—strive to work quickly! Butorphanol cancause troublesome head tremors.
● Use a small syringe to draw up and administertopical drugs (anesthetics and mydriatics). Ifthe horse is sedated, distribution of topicalswill be facilitated by rolling the head awayfrom the examiner slightly so the target eye ismore vertical. This position will aid in accu-rate “aiming” of medication that is sprayed ordripped on the surface of the globe.
● Get in the habit of performing a systematicevaluation of all regions of the eye, using in-formation discussed below on the anatomy ofeach region. Use a penlight, direct ophthal-moscope, and slit lamp if available. Even ifthe problem is obvious, slow down and look atall regions: orbit, lids, conjunctiva, tear film,cornea, anterior chamber (AC), iris, lens, pos-terior segment, fundus, and optic nerve. As-sess cranial nerve function. Assess visualaxis using dazzle, direct and consensual pupil-lary light response (PLR), menace, and (whenappropriate) blindfold obstacle maze naviga-tion. Use dial settings to change lenses on thedirect ophthalmoscope to focus on deeper lay-ers of the globe. Use (or refer) for tonometryin suspected glaucoma cases.
● Vascularization of the cornea occurs in manydisease processes. Superficial vessels are in-dividual long branching vessels that lie withinthe epithelium or anterior stroma. Deeper,mid-stromal vessels are multiple—they are
AAEP PROCEEDINGS � Vol. 53 � 2007 375
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

short and straight and may form a brush bor-der on the limbus. Very deep vessels that reston the Descemet’s membrane interface are in-dividual long branching vessels.
● Buy at least one atlas or book on equine oph-thalmology (several are listed in the refer-ences). Studying many fundic photos willhone skills in deciding what is “normal” andwhat is “abnormal.” Look at lots of “normal”eyes! At least 20% will have some finding ofrecord!
● Develop a recording system to write down yourobservations. Start taking digital photo-graphs of the eyes. With a little practice, andjudicious cropping, it is easy to get great im-ages using a camera with 4.0 megapixels orhigher resolution. Archiving the images inthe horse’s medical record and rephotograph-ing at later intervals will help determineprogress of your cases.
2. Ocular Examination
Reflex Testing
Making a quick, threatening motion toward the eyeto cause a blink response and/or a movement of thehead tests the menace response. This is a crudetest of vision. Care is taken not to create air cur-rents toward the eye when performing this test.Horses have a very sensitive menace response.
The horse should also quickly squint or “dazzle”when a bright light is abruptly shown close to theeye.
The palpebral reflex is tested by gently touchingthe eyelids and observing the blink response.
Vision could be further assessed with maze testingwith blinkers or a large towel alternatively coveringeach eye. The maze tests should be done under dimand light conditions. Barn aisles that have beencleared of hazards are good stages for maze testing;an obstacle course can be created using overturnedbuckets or other smooth, solid objects that are easilyrearranged. Blindfolded horses that are visual inthe uncovered eye can be coaxed to navigate themaze to reach food. Maze testing is best done withthe horse loose; paths that exit the maze area shouldbe blocked for safety concerns!
The PLR (direct and indirect) evaluates the integ-rity of the retina, optic nerve, midbrain, oculomotornerve, and iris sphincter muscle. The normalequine pupil responds somewhat sluggishly and in-completely unless the stimulating light is particu-larly bright. The reflex is strongest if the lightsource is focused slightly temporal to the centralvisual axis where it shines on the visual “streak.”Stimulation of one eye results in the constriction ofboth pupils. The PLR is valuable in testing poten-tial retinal function in eyes with severe cornealopacity.
Diagnostic Testing
It is important to approach each eye problem in thehorse in an ordered and systematic manner. Themajority of cases can be diagnosed by using stan-dard ophthalmic clinical examination techniques.
Intravenous sedation, a nose or ear twitch, andsupraorbital sensory and auriculopalpebral motornerve blocks may be necessary to facilitate theexamination.
The auriculopalpebral nerve (motor nerve to theorbicularis oculi muscle) can be palpated under theskin and blocked with 2–3 ml of lidocaine just lateralto the highest point of the zygomatic arch.
The frontal or supraorbital nerve (sensory to themedial two thirds of the upper lid) can be blocked atthe supraorbital foramen. This foramen can be pal-pated medially at the superior orbital rim where thesupraorbital process begins to widen. Line blockscan be used near the orbital rim to desensitize otherregions.
Schirmer tear testing is a method to measure re-flex tearing and should be used for chronic ulcersand eyes in which the cornea appears dry. TheSchirmer tear test must be done before instillationof any medications into the eye. The test strip isfolded at the notch and the notched end insertedover the temporal lower lid margin. The strip isremoved after 1 min, and the length of the moist endis measured. Strips are frequently saturated inhorses after 1 min, with values ranging from 14 to34 mm wetting/min considered normal. Values�10 mm wetting/min are diagnostic for a tear defi-ciency state.
Corneal cultures using microbiologic cultureswabs should be obtained before placing any topicalmedications in the eye. The swabs should be gentlytouched to the corneal ulcer and plated directly on abiplate or submitted for culture in transport media.Dacron swabs come packaged in sterile packs of two.These tightly woven synthetic swabs are superior tocotton swabs for culture because they do not leavefiber remnants that may confuse subsequent cytol-ogy analysis.
As an alternative method, one author (A.E.D.)uses a double-wrapped sterile scalpel blade for cor-neal cultures in ambulatory settings. The blade isapplied to the target surface and dropped into athioglycollate broth tube. The broth is carried inthe truck and placed in an incubator at days end andobserved overnight for turbidity. Samples withbroth growth are plated out for microscopic analysisand in house sensitivity testing. A special sensitiv-ity wheel stocked with discs that elute common an-tibiotics used against eye infections (cephazolin,chloramphenicol, gentamicin, amikacin, ciprofloxa-cin, oxacillen, and tobramycin among others) is keptat the clinic and used just for ocular sensitivityanalysis. Useful results are often available in aslittle as 48 h when cultures are done in house; thisapproach is a practical solution to the challenge that
376 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

practitioners face with the long lead time needed toship out culture samples and wait for results fromreference laboratories.
Corneal scrapings to obtain cytology specimens todetect bacteria and deep fungal hyphal elements canbe obtained at the edge and base of a corneal lesionwith topical anesthesia and the handle end of asterile scalpel blade. Superficial swabbing cannotbe expected to yield the organisms in a high percent-age of cases so removing the superficial debris can behelpful before collecting the sample. Cytology ofeyelid and conjunctival masses can also be diagnos-tic. The foil wrapping that covers the blade can befolded around the blunt end of the blade and used asa handle for the scraping so that the sharp endremains cased. The sample is transferred to two orthree glass slides by direct smear. Persistence willpay off—it takes patience to “chase” exfoliated cor-neal tissue around the corneal lesion and actuallyget it to adhere to the blade edge. Once the speci-men is on the slide, it should air dry—fixative is notneeded. The slides are best transported in plasticslotted boxesl instead of cardboard slide carriers.It is not difficult to develop expertise in basic ocularcytology; with practice, slides can be read in-houseso that treatment decisions can be made ASAP.The core concept of ocular cytology is to look forinfectious elements (bacteria and/or filamentousfungi), “visiting cells” (neutrophils, eosinophils, lym-phocytes and monocytes), and foreign material suchas plant parts. All these elements are identifiablewith Romanowskikm stain and gram stain, and pa-tient examination using the oil immersion lens ofthe microscope. Slides will typically show a combi-nation of large rafts of intact blocks of dense epithe-lial cells and smaller thinner sheets of individualcells. The smaller sheets, as well as areas thatshow individual “visiting” cells will provide the mostuseful information. Practitioners often forego cy-tology because of the expense and long turnaroundtime involved in using a reference laboratory. Thischallenge is eliminated if the cytology is performedby a technician or veterinarian right at the practice.
The cornea should be clear, smooth, and shiny.Placing fluorescein dye (use it nondiluted) in the eyeto identify corneal ulcers should be routine in everyeye examination of the horse. Small corneal ulcerswill stain that might otherwise be undetected.
Seidel’s TestFluorescein can be used to detect perforated corneasor leaking corneal sutures.
Tear Film Break-Up TimeNormal tear film is continuous. Blinking main-tains the tear film continuity. The tear film breaksup if blinking does not occur often enough. Darkdry spots will appear under cobalt blue–filtered lightas part of normal evaporation and diffusion of tears.Fluorescein dye is placed on the cornea and notflushed off. The lid is manually blinked three times
and held open to expose the tear film to evaporation.The time needed for a dry spot to appear on thecorneal surface after blinking is referred to as thetear film break-up time (TFBUT). In a normalhealthy eye, dry spots start occurring betweenblinks at �10–12 s. A TFBUT of �10 s is abnormaland probably associated with instability of the mu-cin layer of the tear film.
Rose bengal dye should be used in selected casesafter installation of fluorescein to identify the integ-rity of the tear film. Rose bengal dye strips areavailable at http://www.akorn.com.n
To determine the patency of the nasolacrimal sys-tem, it is best to use irrigation from the nasal orificewith a nasolacrimal cannula or curved multipurposesyringe, although fluorescein dye penetrationthrough the nasolacrimal system may also indicatepatency.
The AC is best examined with a handheld or tran-silluminator mounted slit-lamp. The AC containsoptically clear aqueous humor. Increased proteinlevels in the AC can be noted clinically as aqueousflare. White cells in the AC are called hypopyon,and red cells in the AC are called hyphema. Aque-ous flare, hypopyon, and hyphema indicate uveitis.
The intraocular pressure (IOP) of horses is 16–30mm Hg with applanation tonometer applanationtonometer.f
A mydriatic should be applied to the eye once thepupillary light response has been evaluated. Theagent of choice is topical 1% tropicamide, whichtakes �15–20 min to produce mydriasis in normalhorses and has an action that persists for �8–12 h.Atropine is used for therapeutic mydriasis becauseit can dilate the normal horse pupil for �2 wk.
The lens should be checked for position and anyopacities or cataract. There are a number of lensopacities which may be regarded as normal varia-tions: prominent lens sutures, the point of attach-ment of the hyaloid vessel, refractive concentricrings, fine “dustlike” opacities, and sparse “vacuoles”within the lens substance.
Cataracts are lens opacities and are associatedwith varying degrees of blindness. They can becongenital, secondary to previous uveitis, and beprogressive or nonprogressive. In some horsebreeds they may be hereditary.
Normal aging of the horse lens will result in cloud-iness of the lens nucleus (nuclear sclerosis) begin-ning at 7–8 yr of age, but this is not a true cataract.The suture lines and the lens capsule may also be-come slightly opaque as a normal feature of aging.
The adult vitreous should be free of obvious opac-ities. Vitreal floaters can develop with age or besequelae to equine recurrent uveitis (ERU). Theyare generally benign in nature.
The retina and optic nerve are examined with adirect,m or indirect ophthalmoscopes. The rotarylens setting of the direct ophthalmoscope should beset to 0 to examine the retina and optic nerve and toa “green” number 20 to focus on the lids and cornea.
AAEP PROCEEDINGS � Vol. 53 � 2007 377
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

Magnification of the fundic image with the directophthalmoscope is 7.9 laterally and 84 axially inhorses. Magnification with the indirect ophthalmo-scope and a 20-D lens is 0.79 laterally and 8.4axially. The Panopticm ophthalmoscope has an in-termediate level of magnification between the directand indirect ophthalmoscopes. The fundus shouldbe examined for any signs of ERU, such as peripap-illary depigmentation. The nontapetal region ven-tral to the optic disc should be carefully examinedwith a direct ophthalmoscope, because this is thearea where focal retinal scars are seen. Retinaldetachments may be congenital, traumatic, or sec-ondary to ERU and are serious faults because oftheir association with complete or partial vision loss.
B-scan ultrasound, computerized tomography(CT), and magnetic resonance (MR) imaging are im-portant for evaluating intraocular and orbital le-sions in the horse. CT and MR are usuallyperformed at referral institutions. High-resolutionultrasound is a referral procedure, but B mode ul-trasound using a 7.5- to 10-MHz tendon probe andconventional field units can often produce diagnosticimaging of large problems such as detached retina,lens luxation, or abnormal globe dimensions.
3. Common Eye Conditions Seen in the Field
Ocular Problems in the Foal
A newborn foal may exhibit lagophthalmos, low tearsecretion, a round pupil, reduced corneal sensitivity,lack of a menace reflex for up to 2 wk, hyaloid arteryremnants containing blood for several days afterbirth, prominent lens Y sutures, and a round opticdisc with smooth margins.
Tapetal color is related to coat color and is usuallyblue-green but may be partially red, orange, or blue.Color dilute foals have a red fundic reflection from alack of a tapetum and consequential exposure ofchoroidal vessels.
Dermoids (choristomas) are aggregates of skin tis-sue aberrantly located in the conjunctiva, cornea, oreyelid. Treatment would be a keratectomy for cor-neal dermoids and blepharoplasty for eyelid lesions.
Entropion is an inward rolling of the eyelid mar-gin. This causes the eyelid hairs to rub on thecornea. It can be a primary problem in foals orsecondary to dehydration or emaciation as in“downer foals.” It may be repaired to prevent cor-neal ulceration in the neonate by placing sutures atthe lid margin in a vertical mattress pattern to evertthe offending eyelid margin.
Lacrimal puncta agenesis or duct atresia may beunilateral or bilateral. Clinical signs are a chronicmucoid and eventually mucopurulent discharge (of-ten copious) in a young horse. Presumptive diag-nosis of duct agenesis may be made by noting a lackof a distal opening of the nasolacrimal duct orpuncta at the mucocutaneous junction within thenares.
Persistent pupillary membranes (PPMs) seldomcause any visual impairment although focal lens orcorneal opacities may be present. There is notherapy.
Congenital cataracts in foals are common congen-ital eye defects. Surgery is recommended.
Microphthalmos is a common ophthalmic congen-ital defect in the foal. A range of lesions may bepresent. The microphthalmic eye may be visual orassociated with other eye problems that causeblindness.
Strabismus is deviation of the globe from its nor-mal orientation and may be noted alone or withother congenital ocular deformities.
Congenital lens luxation is a severe eye problemthat needs surgery for resolution.
Subconjunctival hemorrhage may be found infoals after dystocias.
Persistent superficial corneal erosions in the neo-natal foal may be associated with decreased cornealsensation.
Iridocyclitis in the foal is generally secondary tosepticemia and may be unilateral or bilateral. Fi-brin, hyphema, and/or hypopyon may be present.Infectious and toxic etiologies are reported in foals.Severe unilateral, blinding, fibrinous uveitis second-ary to plant toxins has been noted in primarily Thor-oughbred foals and yearlings in the southern UnitedStates.
Congenital glaucoma and congenital retinal de-tachment are found periodically in foals and repre-sent severe blinding eye problems.
Ocular Problems in Mature Horses Listed by AnatomicalRegion
OrbitThe orbit is composed of several bones forming a seriesof canals, fissures, and foramina that contain theglobe, orbital fascia, the optic nerve and other nerves,blood vessels, muscle, fat, and glands. Prominence ofthe orbital rim renders it prone to injury, especially insituations where horses are kicked or trapped in nar-row places like starting gates. Radiography may out-line fractures of orbital bones, but image anglingrestrictions may make diagnostic views difficult.Ultrasonography sometimes can identify bone frag-ments. Severe sinus disease may invade the orbitalspace, and abscesses of the caudal upper molar rootsmay threaten orbital health. Common conditions in-clude the following.
Exophthalmos, or anterior displacement of theglobe, is associated with nictitans protrusion andlagophthalmos. It can result in corneal ulceration.Exophthalmos can be confused with buphthalmos,which is a marked increase in globe diameter asso-ciated with advanced glaucoma. Infectious, trau-matic, inflammatory, or neoplastic disease processesinvolving the eyelids, the frontal, maxillary, andsphenopalatine sinuses, tooth roots, the gutturalpouch, and nasal cavity may extend into the orbit to
378 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

cause exophthalmos and/or strabismus. Retrobul-bar hemorrhage and cellulitis associated with or-bital trauma can cause exophthalmos.
Enophthalmos, or posterior displacement of theglobe, is caused by dehydration, atrophy of orbitalfat, orbital fractures, and phthisis.
Strabismus is deviation of the visual axis of one orboth globes and can be found with neurologic defi-cits, visual difficulties, and abnormal head posture.In the neonatal foal, the horizontal axis of the pupiland globe is deviated slightly medially and ventrallywith the eye reaching the normal adult position by 1mo of age. Orbital asymmetry can develop second-ary to orbital rim fractures, orbital cellulitis andabscesses, orbital tumors, and orbital emphysema.Congenital strabismus (hyperopia) and dorsomedialstrabismus are reported in Appaloosa foals and maybe associated with equine congenital stationarynight blindness. Esotropia (crossed eyes) is re-ported in mules. Strabismus may also result fromspace occupying lesions of the orbit or be caused bymuscle avulsion from a traumatic proptosis.
Orbital fat prolapse can occur from trauma oridiopathic means.
Orbital Trauma, Orbital Foreign Bodies, Con-tusions, and Periorbital FracturesHorses may injure the orbital region on the racetrack, in trailers or pastures, by rearing and hittingstall ceilings or starting gates, from gunshots, kicksfrom other horses, or when being disciplined.1-5
These should be taken seriously and treated aggres-sively, because infection secondary to trauma canlead to orbital cellulitis, which can be vision threat-ening or even fatal. Field diagnostics may be in-conclusive for fracture or foreign body, so monitorclosely and use common sense—if the periorbitalregion remains hot, painful, and swollen in the faceof therapy, there may be a sequestra, abscess, orforeign body present even if you cannot image it.Monitor the globe and treat as necessary for second-ary uveitis. Consider location of nasolacrimal ductand extraocular muscles when forming treatmentplan. Broad-spectrum antibiotics and heavyNSAIDs are generally prudent. Ultrasound withsimple equipment may reveal abscess pockets.Orbital TumorsReported neoplasms include lymphoma, neuroendo-crine tumor, lipoma, meningioma, melanoma, sar-coid, squamous cell carcinoma, hemangiosarcoma,osteoma, medulloepithelioma, schwannoma, andneurofibroma.1-5 The horse will present with anappearance of an enlarged bulging eye, but the globemay be normal sized and just proptosed. Ultra-sound with simple equipment (7.5-mHz probethrough the lids) will reveal a disparity in densityand size of orbital contents from the normal eye.A few universities offer orbitotomy (globe sparing)surgery, but most orbital tumors are treated by ex-enteration. Advanced tumors may recur. Surgi-
cal removal of orbital tumors may be accompaniedby extensive hemorrhage!Suture Line PeriostitisThis is an idiopathic condition where the suturelines between the nasal and frontal bones of theskull are inflamed. This condition is noted in theUnited Kingdom. Horses present with hard en-largements of the suture line areas. Occasionallycan cause periocular swelling and/or nasolacrimalitduct obstruction. There is no treatment at present;the condition may resolve spontaneously. Radio-graphs will confirm diagnosis.
Orbital fractures can be identified by palpation,facial deformity, and radiography. Blepharedema,epistaxis, orbital emphysema, corneal ulcers, uve-itis, and limitations of global motility caused byentrapment by bone fragments may accompany or-bital fractures. Orbital fractures can result in dis-placement of globe and have the potential for globe-penetrating bone fragments. Minor orbital rimfractures may not need surgical correction unlessfracture fragments are impinging on the globe orperfect cosmesis is required. Serious periorbitalfractures should be surgically repaired quickly, be-cause fibrous union of the fractured pieces beginswithin 1 wk after the injury to make elevation andrealignment very difficult. Interosseous wiringwith stainless steel suture, bone plating, and can-cellous bone grafts may be necessary to immobilizeand repair extensive orbital fractures.Foreign Bodies Can Lead to Orbital AbscessesOlder horses tend to develop neoplasia, whereasfoals and yearlings may be prone to acute orbitaltrauma and cellulitis. Cellulitis may be associatedwith fever, blepharedema, swelling of the supraor-bital fossa, nictitans protrusion, chemosis, and cor-neal edema.
Head trauma can cause globe proptosis. Propto-sis is forward displacement of the eye from the orbit.It is seen commonly with retrobulbar hemorrhageand edema after penetrating orbital trauma. Incases of traumatic globe proptosis, careful ophthal-mic exam will dictate viability of the eye. Lack ofan indirect pupillary reflex to the normal eye andmiosis with severe hypotony and hyphema indicatesevere trauma and poor visual prognosis. Tempo-rary tarsorrhaphy is recommended for proptosis.
EyelidsThin and highly vascularized, the eyelids containmuscles, connective tissue, cilia, glands that pro-duce components of the tear film, and a tarsal platethat gives the free edge of the lid support. They arelined with conjunctiva. The major issues that arisewith eyelids are trauma and neoplasia. Occasion-ally lids can be malformed. Prompt, definitivetherapy is needed when any condition threatens theanatomy or function of the lids. Eyelids can healvery well if the surgery is done with carefultechniques.
AAEP PROCEEDINGS � Vol. 53 � 2007 379
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

NictitansThis is the “third eyelid” consisting of a conjunctivacovered membrane, a T-shaped cartilage, and a se-romucoid gland at the base. It functions to protectthe cornea and distribute tear film.Eyelid LacerationsThis is very common, especially when horses areirritated by insects and seek objects to rub their eyeson. the most common cause is entrapment of thelid in a bucket handle! Counsel owners to tape upbucket handles before injuries occur. Intralesionalanesthetics will make the horses positive for drugtesting. Great care should be taken with the re-pair, including minimal debridement, careful appo-sition of the torn pedicle, use of 4-0 suture, andclosure of the tarsal plate using a figure of eightsuture pattern that keeps suture tags from abradingthe cornea. Standing surgery is helped by restingthe chin of the sedated horse on bales and using avery short (5.5 in) Olsen Hegar needle holder andforceps. Be careful if you decide to use a two-layerclosure—the inner layer must not abrade the cor-nea. In the field, single-layer closures with metic-ulous deep bites are often the safestrepairs. Temporary tarsorrhaphies may stabilizethe tarsal plate in severe tears. Check the globecarefully for concurrent injury or uveitis. UseNSAIDs and topical and/or systemic antibiotics for afew days,SarcoidsSarcoids are common benign tumors that affect theadnexal region and threaten the eyes by expansionand compromise of lid function. Definitive diagno-sis is by biopsy, but biopsy can stimulate tumorexpansion. “On the farm” treatment includes topicalapplication of a bloodroot-based paste—appropriateif the lesion is located away from the palpebral mar-gin and is not compromising lid function. Shrink-ing the sarcoid lesion with antipsoriasis skinointments and/or topical 5-fluorouracil (5-FU) for 2wk may be beneficial before using BacillusCalmette-Guérin (BCG). Surgical resection of ne-crotic tissue is controversial with some experts sug-gesting it will exacerbate the sarcoid.ImmunotherapyInjecting attenuated Mycobacterium cell wall frac-tion (BCG) often is effective in promoting remission.Referral or “in clinic” treatments include cryother-apy, intralesional chemotherapy with cisplatin, hy-perthermia, CO2 laser ablation, and intralesionalradiotherapy. The bovine papilloma virus (BPV)induces sarcoids, and intralesional treatment withthe BPV vaccine can be helpful. Transmission isthought to be linked to stable flies, but a geneticsusceptibility probably also has a role.
Squamous Cell CarcinomaSquamous cell carcinoma (SCC) is a common tumorthat can affect the lids, nictitans, and globe. Appa-loosas, draft breeds, and Paint horses are at in-
creased risk. Solar radiation promotes neoplastictransformation, especially if the lids lack pigment.SCC is locally invasive and often accompanied bylocal necrosis and functional compromise of the af-fected tissue. Excision with wide margins may becurative, but submission of the mass for marginanalysis is wise. The author has had good lucksupplementing surgery with intralesional cisplatinchemotherapy if the mass cannot be completely ex-cised. Masses located in the nictitans may betreated by excision of the entire nictitans. This is asimple surgery that can be done in the field withgood results—horses do not often suffer tear filmproblems afterward. Adjunctive therapy at refer-ral hospitals includes excision with eyelid recon-struction, hyperthermia, cryosurgery (double freezethaw cycle to 4 to 40°F), beta irradiation withstrontium 90, brachytherapy using interstitial radi-ation with a variety of radioisotopes, and intrale-sional chemotherapy. Other tumors that can affectthe lids include melanoma, fibroma, fibrosarcoma,lymphoma, mast cell tumor, hemangioma, angiosar-coma, and osteoma. Fungal granulomas or myce-tomas resemble neoplastic lesions—differentiate byhistopathology.
Eyelid EdemaThis often occurs unilaterally in summer months; itis thought to reflect an allergic reaction to insectbites. It may be quite dramatic but usually notpainful. It responds promptly to topical and sys-temic corticosteroids. It is important to check globecarefully—uncomplicated cases will show normalpupil size and intact corneal epithelium.
MeibomianitisThese are cheesy abscesses of the meibomiumglands of the tarsal plate. It may affect all four lidmargins, and is idiopathic in origin. Treatment in-volves incision of the gland conjunctiva with a no. 15scalpel blade and curettage of the debris with asmall curette. Inspissated material may be gritty.Post-operative therapy includes topical and/or sys-temic antibiotics and corticosteroids. Recurrence iscommon.
Solar BlepharitisThis is common in Appaloosas and other horses withlight pigmentation of the eyelid margins. It oftenaccompanies chronic insidious uveitis. Palliativetherapy includes the use of a UV light blocking flymask and intermittent, judicious use of topical ste-roids. Topical cyclosporine A helps some horses.
Prolapse of the NictitansBilateral prolapse can accompany systemic tetanusor an acute attack of Hyperkalemic periodic paraly-sis. Unilateral prolapse should prompt a thoroughexamination. After sedation and topical anesthe-sia, the nictitans should be pulled out and evertedout to inspect for neoplasia, foreign body, or other
380 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

abnormality. Horner’s syndrome can cause unilat-eral prolapse with ptosis and sweating on the ipsi-lateral neck.
ConjunctivaConjunctiva is the mucous membrane that lines thelids (palpebral conjunctiva) and covers the sclera(bulbar conjunctiva). The membrane is filled withfine blood vessels and thus is a barometer of sys-temic or vascular abnormalities, including anemiaor jaundice. Almost any ocular inflammationcauses the “red eye” appearance of conjunctivitis.This term is not a diagnosis but a secondary symp-tom of ocular or systemic disease! Look for allergic,infectious, immune, neoplastic, parasitic disease, orforeign bodies as the primary cause of any observedconjunctivitis.ChemosisThis is edema of the conjunctiva, usually associatedwith allergy. It is rapidly responsive to topicalsteroids.DermoidCongenital abnormal growths that may affect theconjunctiva near the limbus. May have hair, glan-dular, or mineralized tissue elements. May be sur-gically removed under general anesthesia.Scleral HemorrhageReddish streaks under the conjunctiva around thelimbus, commonly seen in neonatal foals as a resultof birth trauma. Will resolve in about a week withno therapy.NeoplasiasInclude squamous cell carcinoma, melanoma, lym-phoma, papilloma, and hemangioma/hemangiosar-coma. See notes under eyelids for therapies.HabronemiasisThis is a parasite that can cause ocular granulomasinvolving the conjunctiva and limbus. Onchocer-ciasis can also cause conjunctivitis and keratitis anduveitis. Treatment involves administration of sys-temic ivermectin and topical steroids. Granulomasmay require debridement under sedation and topicalanesthesia.
Nasolacrimal SystemThe nasolacrimal system has both drainage and se-cretory functions.1-5 Drainage begins at the twopuncta in the upper and lower medial canthus ofeach eye, continues through the nasolacrimal canal-iculi, into the nasolacrimal sac, and down the naso-lacrimal duct, which runs through the lacrimal boneof the maxilla. Drainage exits at the nasal punc-tum. The tear film is a byproduct of secretions ofthe lacrimal and nictitans glands, the meibomianglands, and the conjunctival goblet cells. Much re-search is currently being done on the inflammatorymediators that reside in the precorneal tear film,because these have an important role in cornealulcer progression and healing.
Dacryocystitis is inflammation of the lacrimal sacand nasolacrimal duct and is common. It can besecondary to obstruction of the drainage system thatis congenital or acquired. It is seen frequently insummer months accompanying insect irritation orsolar blepharitis. It is characterized by mucopuru-lent discharge at the medial canthus and mild con-junctivitis/hyperemia. Mild unobstructed cases arerapidly responsive to topical antibotics or antibiotic/steroid combinations. Obstructed cases can some-times be cleared by simple retrograde flushing(using a curved tip syringe, jugular catheter, orother small tubing attached to a syringe) of a salinesolution that has been mixed with a small amount ofsteroid and/or antibiotic. Further diagnostics arewarranted on cases where the duct is not patent.This occasionally can be secondary to dental disease.Contrast radiography can determine boundaries ofduct system and location of obstruction, and referralfor surgery (conjunctivorhinostomy) is optimaltherapy.
Keratoconjunctivitis sicca (KCS) or “dry eye” inhorses is a group of clinical signs related to a lack oftears. Corneal ulcers, corneal pigmentation, con-junctivitis, and blepharospasm may be seen. TheSchirmer tear test values (normal is 14–34 mm wet-ting/min) are �10 mm wetting/min in horses withquantitative KCS. This condition is uncommon inhorses. Qualitatitve KCS, where the Schirmers arenormal to elevated and yet the cornea appears dry,is common in the horse.
KCS can be caused by nerve damage that affectsparasympathetic system that innervates lacrimalgland. It is often accompanied by cranial nerve VIIfacial paralysis and an inability to close the lid.It is also seen with some cases of vestibular disease,eosinophilic keratitis, and with locoweed poisoning.Other cases are idiopathic. It may be very difficultto manage because of associated chronic corneal dis-ease, exposure, and discomfort. Lubrication of eyeusing artificial tears in gel format is helpful. Topi-cal cyclosporine A may alleviate signs; some idio-pathic cases resolve spontaneously.
Cornea
Corneal AnatomyThe outer corneal layer is a relatively impermeableepithelium that is richly innervated and very thin(0.14 mm and six to eight cell layers thick), with anunderlying basement membrane. Healing of de-fects in this layer is rapid and occurs by “slidingleapfrog” motion of adjacent cells without mitosis.The next layer is the stroma, which is the thickestlayer. Stroma is composed of type I collagen fibrilsthat are arranged in a parallel lamellar lattice pat-tern. Disruption of the lattice causes opacity.Healing of stromal defects involves a balance of re-sorptive remodeling (facilitated by the proteinasesthat are released from bacteria, corneal cells, andinfiltrating polymorphonuclear leukocytes [PMNs])
AAEP PROCEEDINGS � Vol. 53 � 2007 381
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

and restorative repair where fibroblasts lay downcollagen to fill in the defect. Successful healing ofdefects is followed by several months of collagenremodeling that may return the tissue to a degree ofits original transparency. In deep lesions, or le-sions where healing is delayed, the collagen is laiddown in a thick, random fashion, making an opaquescar. In severe cases, remodeling by proteinases isexcessive, and keratomalacia (melting) or perfora-tion results. The third layer of tissue is a thin (45�m) basement membrane called Descemet’s mem-brane. The final layer of the cornea is a very thinmonolayer of cells, the endothelium. The endothe-lium is no thicker than a single red blood cell (7 �m).This layer of cells has an Na-K–activated ATPase-dependent electrolyte pump that constantly worksto keep the corneal stroma relatively dehydrated.Disruption of the normal pump activity results inedema of the endothelium and overlying stroma thatcan be permanent.1-5
Equine Corneal UlcerationEquine corneal ulceration is very common in horsesand is a sight-threatening disease needing earlyclinical diagnosis, laboratory confirmation, and ap-propriate medical and surgical therapy.1-5
Ulcers can range from simple, superficial breaksor abrasions in the corneal epithelium to full-thick-ness corneal perforations with iris prolapse. Theprominent eye of the horse may predispose to trau-matic corneal injury.
Both bacterial and fungal keratitis in horses maypresent with a mild, early clinical course but needprompt therapy if serious ocular complications areto be avoided. Corneal ulcers in horses should beaggressively treated no matter how small or super-ficial they may be. Corneal infection and iridocy-clitis are always major concerns for even theslightest corneal ulcerations. Iridocyclitis or uve-itis is present in all types of corneal ulcers and mustbe treated to preserve vision. Globe rupture, phthi-sis bulbi, and blindness are possible sequelae tocorneal ulceration in horses.
Proteinases in the Tear FilmTear film proteinases normally provide a surveil-lance and repair function to detect and remove dam-aged cells or collagen caused by regular wear andtear of the cornea. These enzymes exist in a bal-ance with inhibitory factors to prevent excessivedegradation of normal tissue. Two major familiesof proteinases that may affect the cornea include thematrix metalloproteinases (MMPs) and the serineproteinases. MMPs predominate in the horse.1-5
Bacterial and fungal pathogens induce corneal ep-ithelial cells, corneal stromal fibroblasts, and leuko-cytes (PMN) in the tear film to upregulate cytokines(interleukin [IL]-1, IL-6, and IL-8) that induce MMPproduction and elicit inflammatory and degradativeprocesses. Proteinases that may contribute to cor-neal ulceration in the early stages of infection could
be of bacterial or corneal cell origin. In the laterstages as PMNs accumulate, PMN-derived protein-ases predominate as the main factor in corneal tis-sue destruction. In pathologic processes such asulcerative keratitis, excessive levels of these pro-teinases can lead to rapid degeneration of collagenand other components of the stroma, potentially in-ducing keratomalacia or corneal “melting.”
Corneal Sensitivity in Foals and Adult HorsesCorneal sensation is important for corneal healing.The cornea of the adult horse is very sensitive com-pared with other animals. Corneal touch thresholdanalysis revealed the corneas of sick or hospitalizedfoals were significantly less sensitive than those ofadult horses or normal foals. The incidence of cor-neal disease is also much higher in sick neonatesthan in healthy foals of similar age. Ulcerative ker-atitis in the equine neonate often differs from adulthorses in clinical signs and disease course. Foalsmay not show characteristic epiphora, blepharo-spasm, or conjunctivitis, and the ulcers may bemissed without daily fluorescein staining. This de-creased sensitivity may partially explain the lack ofclinical signs often seen in sick neonates with cor-neal ulcers.
Corneal Healing in the HorseThe thickness of the equine cornea is 1.0–1.5 mm inthe center and 0.8 mm at the periphery.1-5
The normal equine corneal epithelium is 8–10 celllayers thick but increases to 10–15 cell layers thickwith hypertrophy of the basal epithelial cells aftercorneal injury. The epithelial basement membraneis not completely formed 6 wk after corneal injury inthe horse, despite the epithelium completely cover-ing the ulcer site.
Healing of large-diameter, superficial, nonin-fected corneal ulcers is generally rapid and linear for5–7 days and then slows. Healing of ulcers in thesecond eye may be slower than in the first and isrelated to increased tear proteinase activity. Heal-ing time of a 7-mm-diameter, midstromal depth,noninfected corneal trephine wound was nearly 12days in horses (0.6 mm/day).
Equine Corneal MicroenvironmentThe environment of the horse is such that the con-junctiva and cornea are constantly exposed to bac-teria and fungi. The corneal epithelium of thehorse is a formidable barrier to the colonization andinvasion of potentially pathogenic bacteria or funginormally present on the surface of the horse corneaand conjunctiva.1-5
A defect in the corneal epithelium allows bacteriaor fungi to adhere to the cornea and to initiate in-fection. Staphylococcus, Streptococcus, Pseudomo-nas, Aspergillus, and Fusarium spp. are commoncauses of corneal ulceration in the horse.
Infection should be considered likely in every cor-neal ulcer in the horse. Fungal involvement should
382 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

be suspected if there is a history of corneal injurywith vegetative material, or if a corneal ulcer hasreceived prolonged antibiotic and/or corticosteroidtherapy with slight or no improvement.
Tear film neutrophils and some bacteria and fungiare associated with highly destructive proteinaseand collagenase enzymes that can result in rapidcorneal stromal thinning, descemetocele formation,and perforation. Excessive proteinase activity istermed “melting” and results in a liquefied, grayish-gelatinous appearance to the stroma near the mar-gin of the ulcer.
Total corneal ulceration ultimately requires thedegradation of collagen that forms the framework ofthe corneal stroma. Horse corneas show a pro-nounced fibrovascular healing response. Theunique corneal healing properties of the horse inregards to excessive corneal vascularization and fi-brosis seem to be strongly species specific.
Many early cases of equine ulcerative keratitispresent, initially, as minor corneal epithelial ulcersor infiltrates, with slight pain, blepharospasm, epi-phora, and photophobia. At first, anterior uveitisand corneal vascularization may not be clinicallypronounced. Slight droopiness of the eyelashes ofthe upper eyelid may be an early, yet subtle, sign ofcorneal ulceration.
A vicious cycle may be initiated after the firstinjury to the cornea, with “second injury to the cor-nea” occurring because of the action of inflammatorycytokines. Ulcers, uveitis, blepharitis, conjunctivi-tis, glaucoma, and dacryocystitis must be consideredin the differential for the horse with a painful eye.Corneal edema may surround the ulcer or involvethe entire cornea. Signs of anterior uveitis arefound with every corneal ulcer in the horse, andinclude miosis, fibrin, hyphema, or hypopyon. Per-sistent superficial ulcers may become indolent be-cause of hyaline membrane formation on the ulcerbed.
Fluorescein dye retention is diagnostic of a full-thickness epithelial defect or corneal ulcer. Faintfluorescein retention may indicate a microerosion orpartial epithelial cell layer defect because of infiltra-tion of fluorescein dye between inflamed epithelialcell junctions. All corneal injuries should be fluo-rescein stained to detect corneal ulcers. Rose ben-gal retention indicates a defect in the mucin layer ofthe tear film.
Horses with painful eyes need to have their cor-neas stained with both fluorescein dye and rose ben-gal dye, because fungal ulcers in the earliest stagewill be negative to the fluorescein but positive forthe rose bengal.
Fungi may induce changes in the tear film mucinlayer before attachment to the cornea. Early fun-gal lesions that retain rose bengal are multifocal inappearance and may be mistaken for viral keratitis.
Microbiologic culture and sensitivity for bacteriaand fungi are recommended for horses with rapidlyprogressive, and deep corneal ulcers. Corneal cul-
tures should be obtained first and followed by cor-neal scrapings for cytology. Mixed bacterial andfungal infections can be present.
Vigorous corneal scraping at the edge and base ofa corneal ulcer is used to detect bacteria and fungalhyphae. Samples can be obtained with the handleend of a sterile scalpel blade and topical anesthesia.Superficial scraping with a cotton swab cannot beexpected to yield organisms in a high percentage ofcases.
A “crater-like” defect that retains fluorescein dyeat its periphery and is clear in the center is a de-scemetocele and indicates the globe is at high risk ofrupture. Descemet’s membrane does not retain flu-orescein dye, whereas deep ulcers that continue tohave stroma anterior to Descemet’s membrane willretain fluorescein. Deep penetration of the stromato Descemet’s membrane with perforation of the cor-nea is a possible sequelae to all corneal ulcers inhorses.
Common Problems of the CorneaSuperficial Corneal ErosionsErosions are defects that do not break into the stroma.If these do not get infected, they heal quickly withoutvisible scars. Topical mydriasis and antibiotic ther-apy is indicated. In some older animals, the erosionsbecome chronic, non-healing indolent ulcers becausethe epithelium does not generate a normal basementmembrane for secure adherence. These cases may behelped by debridement or temporary tarsorrhaphy.If they do not heal in 2 wk, consider performing asuperficial linear keratotomy. Using sedation and lo-cal anesthesia, carefully drag the point of a 22-gaugeneedle clamped very close to the jaws of a hemostatover the surface of the lesion to create a grid incisioninto the superficial stroma and thus provide a latticefor adherence of new epithelial cells. Refer to textsfor exact description of technique. Grid keratotomiescan seed pre-existing infection deeper into the stroma.Do not perform this procedure if infection with bacte-ria or fungus is suspected.Superficial KeratitisThis may present as punctate areas of stain uptake,as focal vascularization, as pigment deposition, asfocal superficial opacities, or as bullous keratopathywhere the epithelium takes on a faintly blisteredappearance. Punctate keratitis may have a viral(herpes?) or an idiopathic etiology. May be painfulor comfortable. Epithelium shows fluorescein stainuptake in a dot like pattern that is scattered overthe surface. A trial of topical idoxyuridine mayimprove the condition. Topical NSAIDs, especially0.1% diclofenac, may be very helpful. Other formsof keratitis may also respond well to topical NSAIDsor antivirals, whereas others respond to topical an-tibiotics. Caution is advised when considering theuse of topical steroids in these cases—horses onsteroid trial therapy should be monitored closely.Horses with unusual epithelial appearance or unex-
AAEP PROCEEDINGS � Vol. 53 � 2007 383
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

plained opacity should be checked for glaucoma bytonometryUlcerative KeratitisUlcers are defects that extend into the stroma (ero-sions are defects limited to the epithelium).1-5
Healing of these defects is a balancing act: ideally,tear film proteinases remodel the stromal defect andnative fibroblasts restore stromal integrity. Bacte-rial or fungal infections and various host factorsmay tip the balance toward excessive resorption,resulting in melting of stromal collagen or even per-foration of the globe. Ulcers are very painful andare accompanied by secondary uveitis, so the syn-drome is complicated by patient objection to topicaltherapy. Refer to the texts in the references for afull discussion of the subject. Adjunctive surgicaltherapy may involve debridement or keratectomywhich can be done in the field. Complex cases mayneed keratotomy, conjunctival grafts, amnioticmembrane grafts, or tarsorrhaphy and thus are re-ferral cases. Very serious cases may need cornealtransplantation by penetrating keratoplasty (PK) orpenetrating lamellar keratoplasty (PLK).
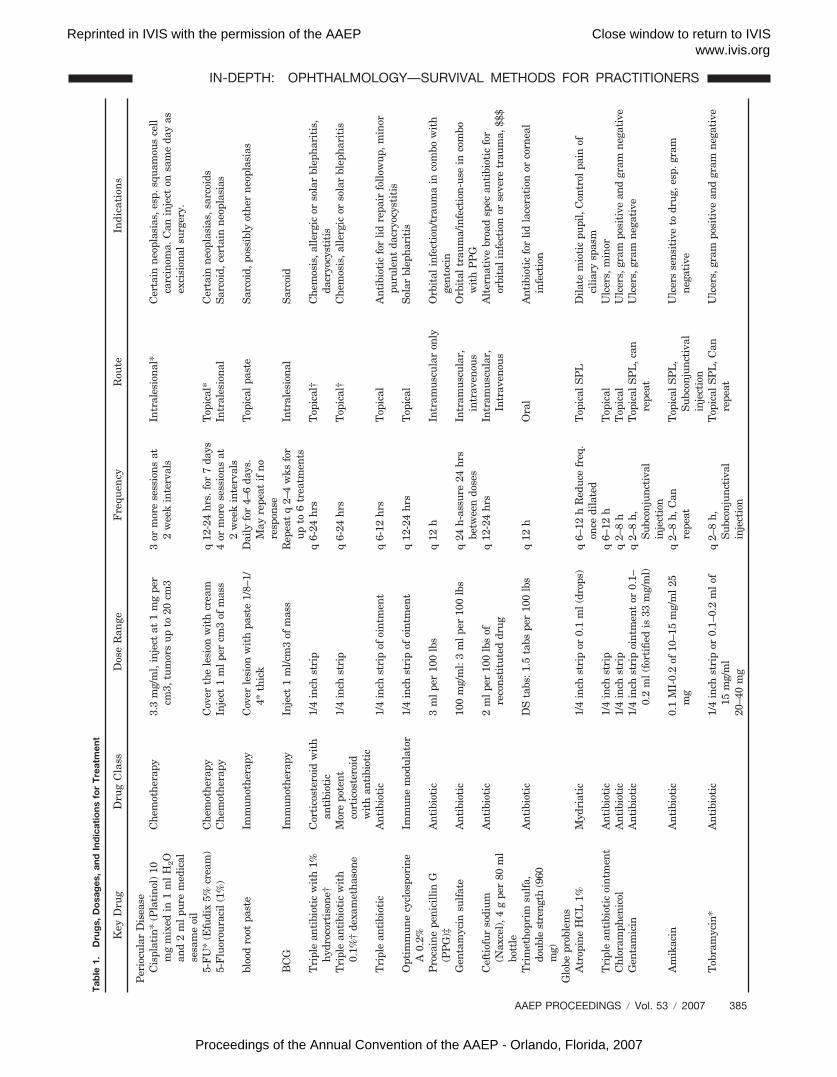
Ulcers with bacterial infection can be diagnosedby cytology. Therapy choices are dictated by thetype of bacteria seen on slides, and later may beadjusted according to clinical response and results oflesion culture/sensitivity. Initial therapy is in-tense, usually four to six times per day. Antibioticsare combined with mydriatics and topical antipro-teinases. Systemic NSAIDs help control pain.Subconjunctival injection may be used to supple-ment topical therapy. Treatment of cooperative pa-tients without obvious keratomalacia may bethrough ointments administered at home, and reso-lution may be straightforward. Treatment of frac-tious patients, or patients with very deep defectsmay be through liquids administered through ansubpalpebral lavage (SPL) tube at home or at areferral hospital. Frequent monitoring will be nec-essary until it is clear that healing is occurring.The most common antibiotic drugs used on bacterialkeratitis are chloramphenicol, cephazolin, tobramy-cin, gentamicin, ciprofloxacin, and amikacin (Table1). Atropine application should be to effect. Topi-cal antiproteinase therapy using serum applicationis routine and may include a combination of MMPinhibitors. Debridement should be judicious.Melting or Very Aggressive UlcersThe most serious, eye-threatening bacterial infec-tions are those caused by beta hemolytic Streptococ-cus spp. and Pseudomonas aeroginosa—theprognosis is guarded if collagenolysis is extensive,and these infections will be expensive and time con-suming to treat.1-5 Treatment must be immediateand aggressive—in referral hospitals, antibioticsand antiproteinases are administered every 1–2 haround the clock. Cephazolin is most effectiveagainst beta hemolytic Streptococcus spp. Amika-cin, tobramycin, and gentamicin are most effective
against Pseudomonas. Topical antiproteinasetherapy usually involves a combination of agents(serum, acetylcysteine, EDTA, ilomastat) adminis-tered every 1–2 h initially. See Table 1 for moreinformation on drug therapy and recommendedstrengths of fortified solutions. Fortified solutionsof amikacin and gentamicin can easily be preparedfrom stock product used in general practice pharma-cies for systemic or orthopedic therapy. Cephazolinis very inexpensive and readily available in 1-g bot-tles through veterinary distributors or local smallanimal hospitals. It may be reconstituted to a 50-mg/ml fortified solution.Ulcers with Fungal Infection (Keratomycosis)Fungi are normal inhabitants of the equine environ-ment and conjunctival microflora, but can becomepathogenic after corneal injury. Aspergillus,Fusarium, Cylindrocarpon, Curvularia, yeasts, andmolds are known causes of fungal ulceration inhorses.1-5
Ulcerative keratomycosis is a serious, sight-threatening disease in the horse. Blindness canoccur. The most often proposed pathogenesis of ul-cerative fungal keratitis in horses begins with slightto severe corneal trauma resulting in an epithelialdefect, colonization of the defect by fungi normallypresent on the cornea, and subsequent stromal in-vasion. Seeding of fungi from a foreign body ofplant origin is also possible. Some fungi may havethe ability to invade the corneal epithelium afterdisruption of the tear film. Stromal destruction re-sults from the release of proteinases and other en-zymes from the fungi, tear film leukocytes, andkeratocytes. Fungi may produce antiangiogeniccompounds that inhibit vascularization.
Fungi seem to have an affinity for Descemet’smembrane, with hyphae frequently found deep inthe equine cornea. Deeper corneal invasion canlead to sterile or infectious endophthalmitis. Sad-dlebreds seem to be prone to severe keratomycosis,whereas Standardbreds are resistant.1-5
Diagnostic tests should include fluorescein androse bengal staining, corneal cytology, corneal cul-ture with attempted growth on both fungal and aer-obic plates, and biopsy if surgery is performed.
Prompt diagnosis and aggressive medical therapywith topically administered antifungals, antibiotics,atropine, and systemically administered NSAIDswill positively influence visual outcome and maynegate the need for surgical treatment. Treatmentmust be directed against the fungi and against theiridocyclitis that occurs after fungal replication andfungal death. Therapy is quite prolonged and scar-ring of the cornea may be prominent. The fungi areoverall more susceptible to antifungal drugs in thisorder: natamycin � miconazole � itraconazole �ketoconazole � fluconazole.
“Ulcer cocktails” are equal parts of equine serum,tobramycin, natamycin, and cefazolin that, whencombined, are very effective against Staphylococcus,
384 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007
Tab
le1.
Dru
gs,
Do
sag
es,
and
Ind
icat
ions
for
Tre
atm
ent
Key
Dru
gD
rug
Cla
ssD
ose
Ran
geF
requ
ency
Rou
teIn
dica
tion
s
Per
iocu
lar
Dis
ease
Cis
plat
in*
(Pla
tino
l)10
mg
mix
edin
1m
lH
2O
and
2m
lpu
rem
edic
alse
sam
eoi
l
Che
mot
hera
py3.
3m
g/m
l,in
ject
at1
mg
per
cm3,
tum
ors
upto
20cm
33
orm
ore
sess
ions
at2
wee
kin
terv
als
Intr
ales
iona
l*C
erta
inne
opla
sias
,esp
.squ
amou
sce
llca
rcin
oma.
Can
inje
cton
sam
eda
yas
exci
sion
alsu
rger
y.
5-F
U*
(Efu
dix
5%cr
eam
)C
hem
othe
rapy
Cov
erth
ele
sion
wit
hcr
eam
q12
-24
hrs.
for
7da
ysT
opic
al*
Cer
tain
neop
lasi
as,s
arco
ids
5-F
luor
oura
cil
(1%
)C
hem
othe
rapy
Inje
ct1
ml
per
cm3
ofm
ass
4or
mor
ese
ssio
nsat
2w
eek
inte
rval
sIn
tral
esio
nal
Sar
coid
,cer
tain
neop
lasi
as
bloo
dro
otpa
ste
Imm
unot
hera
pyC
over
lesi
onw
ith
past
e1/
8–1/
4*th
ick
Dai
lyfo
r4–
6da
ys.
May
repe
atif
nore
spon
se
Top
ical
past
eS
arco
id,p
ossi
bly
othe
rne
opla
sias
BC
GIm
mun
othe
rapy
Inje
ct1
ml/c
m3
ofm
ass
Rep
eat
q2–
4w
ksfo
rup
to6
trea
tmen
tsIn
tral
esio
nal
Sar
coid
Tri
ple
anti
biot
icw
ith
1%hy
droc
orti
sone
†C
orti
cost
eroi
dw
ith
anti
biot
ic1/
4in
chst
rip
q6-
24hr
sT
opic
al†
Che
mos
is,a
llerg
icor
sola
rbl
epha
riti
s,da
cryo
cyst
itis
Tri
ple
anti
biot
icw
ith
0.1%
†de
xam
etha
sone
Mor
epo
tent
cort
icos
tero
idw
ith
anti
biot
ic
1/4
inch
stri
pq
6-24
hrs
Top
ical
†C
hem
osis
,alle
rgic
orso
lar
blep
hari
tis
Tri
ple
anti
biot
icA
ntib
ioti
c1/
4in
chst
rip
ofoi
ntm
ent
q6-
12hr
sT
opic
alA
ntib
ioti
cfo
rlid
repa
irfo
llow
up,m
inor
puru
lent
dacr
yocy
stit
isO
ptim
mun
ecy
clos
pori
neA
0.2%
Imm
une
mod
ulat
or1/
4in
chst
rip
ofoi
ntm
ent
q12
-24
hrs
Top
ical
Sol
arbl
epha
riti
s
Pro
cain
epe
nici
llin
G(P
PG
)‡A
ntib
ioti
c3
ml
per
100
lbs
q12
hIn
tram
uscu
lar
only
Orb
ital
infe
ctio
n/tr
aum
ain
com
bow
ith
gent
ocin
Gen
tam
ycin
sulf
ate
Ant
ibio
tic
100
mg/
ml:
3m
lpe
r10
0lb
sq
24h-
assu
re24
hrs
betw
een
dose
sIn
tram
uscu
lar,
intr
aven
ous
Orb
ital
trau
ma/
infe
ctio
n-us
ein
com
bow
ith
PP
GC
efti
ofur
sodi
um(N
axce
l),4
gpe
r80
ml
bott
le
Ant
ibio
tic
2m
lpe
r10
0lb
sof
reco
nsti
tute
ddr
ugq
12-2
4hr
sIn
tram
uscu
lar,
Intr
aven
ous
Alt
erna
tive
broa
dsp
ecan
tibi
otic
for
orbi
tal
infe
ctio
nor
seve
retr
aum
a,$$
$
Tri
met
hopr
imsu
lfa,
doub
lest
reng
th(9
60m
g)
Ant
ibio
tic
DS
tabs
:1.5
tabs
per
100
lbs
q12
hO
ral
Ant
ibio
tic
for
lidla
cera
tion
orco
rnea
lin
fect
ion
Glo
bepr
oble
ms
Atr
opin
eH
CL
1%M
ydri
atic
1/4
inch
stri
por
0.1
ml
(dro
ps)
q6–
12h
Red
uce
freq
.on
cedi
late
dT
opic
alS
PL
Dila
tem
ioti
cpu
pil,
Con
trol
pain
ofci
liary
spas
mT
ripl
ean
tibi
otic
oint
men
tA
ntib
ioti
c1/
4in
chst
rip
q6–
12h
Top
ical
Ulc
ers,
min
orC
hlor
amph
enic
olA
ntib
ioti
c1/
4in
chst
rip
q2–
8h
Top
ical
Ulc
ers,
gram
posi
tive
and
gram
nega
tive
Gen
tam
icin
Ant
ibio
tic
1/4
inch
stri
poi
ntm
ent
or0.
1–0.
2m
l(f
orti
fied
is33
mg/
ml)
q2–
8h,
Sub
conj
unct
ival
inje
ctio
n
Top
ical
SP
L,c
anre
peat
Ulc
ers,
gram
nega
tive
Am
ikac
inA
ntib
ioti
c0.
1M
I-0.
2of
10–1
5m
g/m
l25
mg
q2–
8h,
Can
repe
atT
opic
alS
PL
,S
ubco
njun
ctiv
alin
ject
ion
Ulc
ers
sens
itiv
eto
drug
,esp
.gra
mne
gati
ve
Tob
ram
ycin
*A
ntib
ioti
c1/
4in
chst
rip
or0.
1–0.
2m
lof
15m
g/m
l20
–40
mg
q2–
8h,
Sub
conj
unct
ival
inje
ctio
n
Top
ical
SP
L,C
anre
peat
Ulc
ers,
gram
posi
tive
and
gram
nega
tive
AAEP PROCEEDINGS � Vol. 53 � 2007 385
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

Tab
le1.
(co
ntin
ued
)
Key
Dru
gD
rug
Cla
ssD
ose
Ran
geF
requ
ency
Rou
teIn
dica
tion
s
Cip
roflo
xaci
nA
ntib
ioti
c1/
4in
chst
rip
or0.
1–0.
2m
lhu
man
drop
sq
2–8
hT
opic
alS
PL
Ulc
ers,
gram
posi
tive
Oxa
cille
nA
ntib
ioti
c0.
1m
lof
hum
andr
ops
q2–
8h
Top
ical
SP
LU
lcer
s,se
nsit
ive
todr
ugC
epha
zolin
(mix
1g
vial
wit
har
tific
ial
tear
sor
salin
e)A
ntib
ioti
c0.
1m
l,�
0.2
mix
to50
mg/
ml
fort
ified
solu
tion
100
mg
q2–
8h,
Sub
conj
unct
ival
inje
ctio
n
Top
ical
SP
L,C
anre
peat
Ulc
ers,
gram
posi
tive
2%po
vido
neio
dine
solu
tion
Ant
i-in
fect
ive
0.1–
0.2
ml
q6
hT
opic
alS
uspe
cted
fung
alul
cers
Silv
ersu
lfad
iazi
neA
nti-
infe
ctiv
ebu
rncr
eam
1/4
inch
stri
pcr
eam
q12
hT
opic
alO
ffla
bel
use,
has
anti
bact
eria
lan
dan
tifu
ngal
acti
vity
1%It
raco
nazo
le/3
0%D
MS
Oin
petr
oleu
m†
Ant
i-fu
ngal
1/4
inch
stri
poi
ntm
ent
q6
hT
opic
alF
unga
lul
cers
.Mus
tbe
com
poun
ded
Nat
amyc
inA
nti–
fung
al0.
1%0.
1–0.
2m
lq
6h
Top
ical
SP
L,
Fun
gal
ulce
rs50
00un
its
One
tim
eS
ubco
nj.i
nj.
1%m
icon
azol
eA
nti–
fung
al1/
4in
chst
rip
crea
mq
6h
Top
ical
Fun
gal
ulce
rs.O
ffla
bel
Clo
trim
azol
eA
nti–
yeas
t1/
4in
chst
rip
crea
mq
6h
Top
ical
Ulc
ers
wit
hye
ast
infe
ctio
n.O
ffla
bel
Itra
cona
zole
†A
nti–
fung
al3
mg/
kgq
10h
Ora
lF
unga
lul
cers
(com
poun
ded
inK
Y)
5%N
aCL
(hyp
erto
nic
salin
e)O
smot
icag
ent
1/4
inch
stri
poi
ntm
ent
q10
hT
opic
alC
lear
corn
eal
edem
aF
lubi
prof
enN
SA
ID0.
1m
lq
6–12
hT
opic
alK
erat
itis
,idi
opat
hic
Dic
lofe
nac
NS
AID
0.1
ml
q6–
12h
Top
ical
Ker
atit
is,p
ainf
ulke
rato
path
y,$$
but
ofte
nve
ryef
fect
ive
Ade
quan
(dilu
tew
ith
art.
tear
s)T
opic
alan
ti-i
nflam
mat
ory
Mix
to50
mg/
ml
q6–
12h
Top
ical
Ker
atit
isno
n-he
alin
gul
cers
Ser
um,a
utol
ogou
sor
hom
olog
ous
MM
Pin
hibi
tor
seri
nepr
otea
sein
hibi
tor
Und
ilute
d,0.
1–0.
2m
lpe
rtr
eatm
ent
q1–
6h
(rep
lace
ever
y5–
7da
ys)
Top
ical
Mel
ting
ulce
rP
reve
ntco
llage
noly
sis
Non
-hea
ling
ulce
rD
oxyc
yclin
eM
MP
inhi
bito
ran
tibi
otic
1m
g/kg
q12
hP
OM
elti
ngco
rnea
lul
cer
Dis
odiu
mE
DT
A(c
anbe
mad
eby
addi
ng1–
5m
lw
ater
toE
DT
Abl
ood
tube
)
MM
Pin
hibi
tor
chel
atin
gag
ent
(Ca
and
Zn)
0.17
%to
1.0%
solu
tion
0.1–
0.2
ml
q1–
6h
Top
ical
Mel
ting
ulce
rT
opic
alch
elat
ion
ofca
lcifi
cke
rato
path
y
N-a
cety
lcys
tein
eM
MP
inhi
bito
rch
elat
ing
agen
t(C
aan
dZn
)5–
10%
,0.1
–0.2
ml
q1–
6h
Top
ical
Mel
ting
ulce
r-pr
even
tco
llage
noly
sis
Ilom
asta
tM
MP
inhi
bito
rch
elat
ing
agen
t9C
aan
dZn
0.1%
,0.1
–0.2
ml
q1–
6h
Top
ical
Mel
ting
ulce
r—pr
even
tco
llage
noly
sis
Tet
anus
anti
–tox
inIm
mun
egl
obul
inre
duce
sco
llage
noly
sis
1m
lO
neti
me
Sub
conj
unct
ival
inje
ctio
nM
elti
ngul
cer
Tis
sue
plas
min
ogen
acti
vato
r(T
PA
)F
ibri
ndi
ssol
utio
n50
–150
mg
(kep
tfr
ozen
atre
ferr
alce
nter
s)O
neti
me
Inje
ctin
ante
rior
cham
ber
unde
rge
nera
lan
esth
esia
Ext
ensi
vefib
rin
inA
nter
ior
cham
ber.
Ref
erra
lpr
oced
ure,
cont
rain
dica
ted
ifhe
mor
rhag
eis
pres
ent
Idox
urid
ine
Ant
ivir
al1/
4*st
rip
or0.
1–0.
2m
lq
4–6
hT
opic
alP
unct
ate
kera
titi
sS
ome
supe
rfici
alke
rati
tis
Cro
mol
ynso
dium
1%M
ast
cell
stab
ilize
r0.
1m
lq
6–12
hq†
6–12
hT
opic
aldr
opE
osin
ophi
licke
rato
conj
unct
ivit
isN
SA
IDs
See
abov
eT
opic
alS
yste
mic
Var
ious
infla
mm
ator
yco
ndit
ions
Cor
tico
ster
oids
See
abov
eT
opic
alsy
stem
icsu
bcon
junc
tiva
lV
ario
usin
flam
mat
ory
cond
itio
nsw
here
the
corn
eal
epit
heliu
mis
inta
ctL
avag
etu
beki
tsT
reat
men
tde
vice
“Flo
rida
tube
s”ar
eth
elo
nges
tan
dbe
stT
reat
men
tca
nbe
give
nas
ofte
nas
need
ed
Top
ical
SP
LD
eep
ulce
rth
erap
yT
opic
alth
erap
yfo
rfr
acti
ous
hors
es
386 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

Tab
le1.
(co
ntin
ued
)
Key
Dru
gD
rug
Cla
ssD
ose
Ran
geF
requ
ency
Rou
teIn
dica
tion
s
Uve
itis
Atr
opin
eH
CL
1%M
ydri
atic
1/4-
inch
stri
por
drop
s,0.
1m
lq
6–48
hT
opic
alD
ilate
pupi
lan
dde
crea
sepa
infr
omci
liary
spas
mP
heny
lep
hrin
e10
%(p
heno
ptic
,neo
-sy
neph
rine
)
Myd
riat
icD
rops
q6–
8h
Top
ical
Can
beep
ithe
lioto
xic-
use
only
ifat
ropi
nefa
ilsto
dila
tepu
pil.
Pre
dnis
olon
eac
etat
e1%
Cor
tico
ster
oid
Dro
ps,0
.1m
lq
1–6
hT
opic
alA
nti-
infla
mm
ator
y,go
odpe
netr
atio
nD
exam
etha
sone
HC
L0.
5%–1
%C
orti
cost
eroi
dD
rops
oroi
ntm
ent
q4–
6h
Top
ical
Ant
i-in
flam
mat
ory,
good
pene
trat
ion
Flu
rbip
rofe
n0.
03%
Top
ical
NS
AID
Dro
ps,0
.1m
lq
1–6
hT
opic
alN
on-s
tero
idal
anti
-infl
amm
ator
yD
iclo
fena
c0.
1%T
opic
alN
SA
IDD
rops
,0.1
ml
q6–
12h
Top
ical
Non
-ste
roid
alan
ti-i
nflam
mat
ory.
$$bu
tpo
tent
Cyc
losp
orin
eA
(0.2
%)
Imm
unos
uppr
essa
nt(P
oor
ocul
arpe
netr
atio
n)O
intm
ent
1/4-
inch
stri
pq
6–12
hT
opic
alS
uppr
esse
sin
flam
mat
ion,
can
beus
edon
ulce
rate
dey
e,m
ayhe
lpin
sidi
ous
case
sw
ith
sola
rbl
epha
riti
s,K
CS
,NK
UT
imol
olm
alea
te0.
5%B
eta
bloc
ker
tode
crea
seaq
ueou
sD
rops
orge
lq
12h
Top
ical
Gla
ucom
ase
cond
ary
touv
eiti
s
Dor
zola
mid
e2%
(Tru
sopt
)Car
boni
can
hydr
ase
inhi
bito
rto
decr
ease
aque
ous
Dro
ps,0
.1m
lq
12h
Top
ical
Gla
ucom
ase
cond
ary
touv
eiti
s
Tim
olol
/Dor
zola
mid
eC
ombo
drug
for
glau
com
aD
rops
,0.1
ml
q12
hT
opic
alG
lauc
oma
unre
spon
sive
toei
ther
drug
alon
e.F
luni
xin
meg
lum
ine
NS
AID
0.5
mg/
kgP
O,I
V,o
rIM
q12
hfo
r5
days
,the
nP
O,I
V,I
MU
veit
is,p
ain,
swel
ling
0.25
mg/
kgP
Oq
12h
asne
eded
Phe
nylb
utaz
one
NS
AID
2.2–
4.4
mg/
kgq
12or
24h
PO
orIV
Uve
itis
,pai
n,sw
ellin
gD
exam
etha
sone
Cor
tico
ster
oid
5–10
mg
per
hors
eq
24h
PO
Uve
itis
—be
caut
ious
ofla
min
itis
risk
2.5–
5m
gpe
rho
rse
q24
hIM
Uve
itis
Tri
amci
nolo
neC
orti
cost
eroi
d2–
6m
g1x
,can
repe
atin
7–21
days
Sub
conj
unct
ival
inje
ctio
nU
veit
isD
oxyc
yclin
eA
ntib
ioti
c10
mg/
kgq
12h
for
4w
kP
OA
nti-
lept
ospi
ral
infe
ctio
nth
erap
yG
enta
mic
inA
ntib
ioti
c4-
mg
inje
ctio
nO
nce
SP
EC
IAL
IST
ON
LY
Intr
avit
real
inje
ctio
nun
der
gene
ral
anes
thes
ia
May
decr
ease
sign
sin
lept
ospi
ral
asso
ciat
edca
ses,
but
ther
ear
esa
fety
conc
erns
.C
yclo
spor
ine
Asu
prac
horo
idal
impl
ant
(und
erde
velo
pmen
t-aw
aiti
ngF
DA
appr
oval
)
Imm
une
supp
ress
ion
inth
epo
ster
ior
segm
ent
Impl
ant
yiel
dssl
owre
leas
eof
drug
Sur
gica
lim
plan
tun
der
scle
raN
CS
tate
,UF
la,a
ndO
hio
Sta
tew
ere
doin
gth
ese
surg
erie
s
Uve
itis
,bes
tpa
tien
tsar
eth
ose
wit
hea
rly,
unco
mpl
icat
eddi
seas
eth
atis
quie
scen
tat
surg
ery
tim
e.D
evic
ecu
rren
tly
unav
aila
ble
Tac
rolim
us,s
irili
mus
,ra
pam
ycin
Imm
une
supp
ress
ion
Res
earc
hdr
ugs
unde
rde
velo
pmen
tA
wai
ting
resu
lts
ofcl
inic
altr
ials
Und
erin
vest
igat
ion
for
topi
cal
and
intr
aocu
lar
use
Uve
itis
–som
ere
ferr
alce
nter
sha
veac
cess
toth
ese
drug
s.
*N
otav
aila
ble
thro
ugh
vete
rin
ary
dist
ribu
tors
,ge
ner
ally
mu
stw
rite
pres
crip
tion
for
hu
man
phar
mac
y.†
Har
dto
fin
dat
all,
gen
eral
lym
ust
com
pou
nd.
‡A
vail
able
over
the
cou
nte
rat
hu
man
phar
mac
ies.
§M
ayon
lybe
avai
labl
eat
refe
rral
inst
itu
tes.
AAEP PROCEEDINGS � Vol. 53 � 2007 387
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

Streptococcus, and fungi. Natamycin, miconazole,itraconazole/DMSO, fluconazole, amphotericin B,2% betadine solution, chlorhexidine gluconate,posaconazole, voriconazole, and silver sulfadiazinecan be used topically against equine keratomycosis.Although the use is off label, OTC 2% miconazolevaginal cream can be used topically in the eye, it canbe irritating. It is best to order 1% miconazole so-lution through a compounding pharmacy. OTC 1%silver sulfadiazine cream can also be used topically onthe cornea. Call university pharmacies to order otherantifungal topical or systemic pharmaceuticals.
Uveitis may be worse the day after initiation ofantifungal therapy because of fungal death.
Systemically administered itraconazole or flucon-azole may be useful in recalcitrant cases.Stromal AbscessesFocal trauma to the cornea can inject microbes anddebris into the corneal stroma through small epithe-lial ulcerative micropunctures. Some stromal ab-scesses may be secondary to systemic disease.
A corneal abscess may develop after epithelialcells adjacent to the epithelial micropuncture divideand migrate over the small traumatic ulcer to en-capsulate infectious agents or foreign bodies in thestroma. Epithelial cells are more likely to cover afungal than a bacterial infection. Re-epithelializa-tion forms a barrier that protects the bacteria orfungi from topically administered antimicrobialmedications. Re-epithelialization of stromal ab-scesses interferes with both routine diagnostics andtreatment.
Corneal stromal abscesses can be a vision-threat-ening sequelae to apparently minor corneal ulcer-ation in the horse. A painful, blinding chroniciridocyclitis may result.
Most stromal abscesses involving Descemet’smembrane are fungal infections. The fungi seem“attracted” to the type IV collagen of Descemet’smembrane.
Both superficial and deep stromal abscesses donot heal until they become vascularized. The pat-terns of corneal vascularization are often unique,suggesting that vasoactive factors are being re-leased from the abscess that influences the vascularresponse.
Medical therapy consists of aggressive use of top-ical and systemic antibiotics, topical atropine, andtopical and systemic NSAIDs.
Superficial stromal abscesses may initially re-spond positively to medical therapy. If reduced in-flammation of the cornea and uvea are not foundafter 2–3 days of medical treatment, surgical re-moval of the abscess should be considered.
Deep lamellar and PKs are used in abscesses nearDescemet’s membrane and eyes with rupture of theabscess into the AC. PK eliminates sequesteredmicrobial antigens and removes necrotic debris, cyo-tokines, and toxins from degenerating leukocytes inthe abscess.
PK for Deep Corneal Stromal AbscessesCorneal transplantation is performed to restore
vision, to control medically refractory corneal dis-ease, and to re-establish the structural integrity ofthe eye. It is a referral procedure.
PK is considered high risk for rejection in infected,vascularized corneal tissue. Nearly all PKs inhorses are in high-risk corneas.
Fresh corneal grafts are preferred in horse PKs,but frozen tissue can be used.
Vascularization of the grafts, indicating rejection,begins at 5–10 days post-operatively.
Few equine PK grafts remain clear after theirvascularization. They form a therapeutic and tec-tonic function.Corneal Foreign BodiesSuperficial foreign bodies can often be coaxed outwith a sterile cotton swab, flushed out with lavage,or “scooped out” by careful undermining with a nee-dle or small biopsy punch. The remaining ulcershould be swabbed and lavaged with 2% povidoneiodine/saline solution and treated medically. Verydeep or penetrating ulcers must be referred for sur-gery and supportive care.Burdock Pappus Bristle KeratopathyThis is commonly seen in the northeast in the fall,when many pastures have tall burdock weeds.Burdock balls are commonly found in the tail andmane. Affected horses present with signs of cor-neal ulceration or erosion, particularly in the medialcanthus under the nictitans. The tiny burdockbristles are not visible in field conditions, but theremay be vessel patterns in the conjunctiva of thenictitans or on the cornea that “point” to their prob-able location. All suspect areas should be debrided.Nictitans debridement is facilitated by everting thewhole membrane with a small towel clamp or hemo-stat and gently scraping the conjunctiva with theserrated edge of a sterile hemostat until it bleeds.Resolution is prompt if the bristles have been com-pletely removed. Treatment involves topical atro-pine and antibiotics and systemic NSAIDs.Calcific Band KeratopathyThis is a troublesome, painful condition that compli-cates some cases of chronic uveitis and may be re-lated to topical steroid application. Gritty plaquesof Ca2� are deposited in the corneal epithelium andupper stroma. May require superficial keratec-tomy and/or chelation with topical EDTA. Recur-rence is common.
Eosinophilic keratoconjunctivitis (EK) has an un-known etiology, but may be an immune-mediateddisease.
All ages and breeds of horses can be affected, withmany cases reported in the spring. Clinical signsinclude corneal granulation tissue, blepharospasm,chemosis, conjunctival hyperemia, mucoid dis-charge, and corneal ulcers covered by raised, white,necrotic plaques. EK resembles a corneal tumor inappearance.
388 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

KCS may develop in affected horses because oflacrimal gland inflammation. The lacrimal glandshould be palpated to detect swelling.
Corneal cytology typically contains numerous eo-sinophils and a few mast cells to rule out similarappearing infectious and neoplastic causes.
Superficial lamellar keratectomy removes plaquesand speeds corneal healing.
Topical corticosteroids (1% prednisolone acetateor 0.1% dexamethasone) four to six times a day inearly stages (despite corneal ulcerations), antibiotics(e.g., bacitracin-neomycin-polymyxin or chloram-phenicol), 1% atropine, and 0.03% phospholine io-dide (q 12 h) in combination with systemicnonsteroidal antiinflammatory drugs are indicated.Topical cromolyn sodium (4.0%, q 8 h) or lodoxamide(0.1%, q 8 h), mast cell stabilizers, can also aidhealing. Systemic corticosteroids may be neces-sary. Horses with EK should be dewormed twicewith ivermectin 10 days apart. These lesions aretypically slow to heal. Scarring of the corneaoccurs.Herpes KeratitisMultiple, superficial, white, punctate or linear opac-ities of the cornea, with or without fluorescein dyeretention, are found associated with equine herpesvirus 2. The focal punctate corneal opacities may befound at the end of superficial corneal vessels, andmay retain rose bengal stain. Varying amounts ofocular pain, conjunctivitis, and iridocyclitis arepresent. Multiple foals in a herd may be affected.Topically administered idoxuridine and trifluorothy-midine (q 8 h) have been used with topical NSAIDsfor treatment of equine herpes ulcers, but recur-rence is common. Lysine administered 20–30g/day, PO, may be helpful.
Lens
The lens is a biconvex transparent body that is sus-pended in the front third of the eye by the zonularfibers that attach to the ciliary body. The anteriorcapsule rests against the rear or the iris, and theposterior capsule abuts against the vitreous body.The outer edge of the lens is called the equator; thisbounds the outer cortex region of the lens. Thecentral axis of the lens pierces the nucleus or centralregion. Suture lines that reflect the embryologicaldevelopment of the lens are apparent on both theanterior and posterior poles in the nuclear region.Normal lenses may show faint concentric rings to-wards the equator or the nuclear sclerosis of advanc-ing age. Small clear vacuoles may be visible as tinybubbles in the lens substrate—these are of no clini-cal significance.
Cataract is, by definition, any opacity of the lensor lens capsule. Cataracts form when there is adecrease in soluble lens protein, a failure of the lensepithelial cell sodium pump that keeps the innerlens dehydrated, lens fiber swelling, or membranerupture. Cataracts are described according to loca-
tion: anterior polar, anterior subcapsular, perinu-clear, nuclear, equatorial, or complete. They arealso described by extent: dense, diffuse, or focal.Focal cataracts are often described by appearance:floriform, stellate, vermiform, crystalline, orelliptical.
Congenital cataracts have been reported in Mor-gans and a few other breeds. A complete densecongenital cataract in an otherwise normal eye is acandidate for surgical removal. Surgery should bedone before 6 mo of age by phacoemulsification.Horses appear to see adequately when aphakic.
Acquired cataracts are the most common type ofcataract. Most often they are a sequelae of repeatattacks of uveitis. Dense cataracts that are second-ary to uveitis are often accompanied by extensiveposterior synechia and sometimes phthisis bulbi.They also can form after severe blunt trauma orpenetrating injury as release of lens protein to thesystemic circulation causes an autoimmune reac-tion. Aging brings cataract changes to manyhorses, similar to humans and dogs. Surgery onacquired cataracts is rarely performed because thecomplication rate with accompanying intraocular in-flammation is high.Lens Luxation/SubluxationLoss of lens position is a common sequelae of chronicuveitis, especially in Appaloosa horses. If the lensis subluxated, an “aphakic crescent” will be obviouson focal illumination. If the lens is completely lux-ated, an opaque mounded body will be apparent onthe ventral fourth of the globe in the posterior seg-ment. Occasionally, the lens will be luxated ante-riorly into the anterior chamber and be visible as alarge white or yellow elliptoid object. Syneresis orliquefaction of the vitreous accompanies lens luxa-tion. Treatment is complicated for lens luxation.
Uveal TractHeterochromia IridisHeterochromia iridis, or dual coloration of the iris(usually blue and brown), is common to the Appal-oosa, palomino, chestnut, gray, spotted, and whitehorses, and is not considered a true pathologiccondition.Aniridia/Iris Hypoplasia/Enlarged CorporaNigra/Iris ColobomasAniridia, or the complete absence of the iris, is re-ported in Quarter Horses and Belgians and is alsoseen with congenital cataracts in Thoroughbreds.Congenital thinning of the iris (hypoplasia) to a full-thickness hole in the iris (coloboma) may be noted inheterochromic eyes. Enlargement of the corporanigra can obstruct the pupil to cause visionproblems.Iris and Ciliary Body CystsUveal cysts are a hallmark of the hereditary ante-rior segment abnormalities of the Rocky MountainHorse and the Connemara pony. Iris cysts may befound sporadically in other breeds. The cysts con-
AAEP PROCEEDINGS � Vol. 53 � 2007 389
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

tain a thick vitreous gel-like material. Cysts at theventral pupil margin appear to cause more visionproblems.Equine Uveitis: the Leading Cause of Blind-ness in HorsesBy definition, uveitis is inflammation of the uvea ofthe eye (iris, ciliary body, and choroid).1-5 The com-plex of diseases known as ERU refers to intraocularinflammation that recurs or persists causing variousdegrees of inflammation, scarring, degeneration,and dysfunction of multiple components of the eye.Several classification schemes are used to differen-tiate subsets of clinically observed disease.Classification by Observed Inflammation Over TimeIn classic uveitis, horses show repeated bouts ofsevere inflammation and pain in one or both eyes.In between bouts, the eye(s) appear comfortable.Horses who are experiencing their first bout of clas-sic uveitis are called primary cases. Because notall uveitis is recurrent, a case is not termed “recur-rent” until two or more classic episodes haveoccurred.
In insidious uveitis, the horse seems normal to theowner, and the animals do not exhibit overt ocularpain, although astute observers may notice subtleabnormalities such as “dull” appearance to theglobe, intermittent tearing or conjunctivitis, smallpupils, and asymmetric appearance to the eyes.This is most often seen in Appaloosas, draft horses,or European warmbloods. Examination of theglobe with a direct ophthalmoscope or slit lampshows deterioration of numerous ocular structuresthat is progressive over time. Pupils may beslightly miotic. Subtle signs include corneal haze,slight aqueous flare, muddy iris color, slight miosis,iris rim atrophy, corpora nigrans atrophy, cataract,low grade vitreous haze, and retinal scarring.Classification by Stage of Disease at Time of Exam-inationAcute cases are horses who are suffering from a flareup of classic uveitis. Signs of an acute bout includepain, lacrimation, photophobia, chemosis, conjuncti-val hyperemia, corneal edema, corneal vasculariza-tion, dot-like keratic precipitates on the cornealendothelium, aqueous flare, hyphema or hypopyon,miosis, vitritis, and ocular hypotension (pressure of10–12 mm Hg).
Quiescent cases are horses in a “calm” time oftheir cycle of repeat inflammation. Slit-lamp ex-amination will show subtle flare in the anteriorchamber, indicating low-grade persistent inflamma-tion. Ocular examination may reveal scarring or“footprints” of previous disease including chroniccorneal edema, iris atrophy, iris color change, syn-echiae (adherence of the iris to the lens or cornea),pigment rests on the lens, cataract, densities or hazein the vitreous, or scarring around the optic disc.Optic disc scarring is seen as either a focal “bullethole” pattern of numerous tiny scars, or a “butterfly”
pattern where wing-shaped islands of depigmenta-tion flank either side of the optic disc.
End-stage uveitis cases have eyes that have un-dergone severe degeneration and chronic scarring.They may show extensive corneal scarring, circum-ferential synechiae, dense cataract, lens luxation orsubluxation, secondary glaucoma, retinal detach-ment, or phthisis bulbi. End-stage uveitis is asso-ciated with vision loss.
Diagnosis of uveitis is simplified by understand-ing that a horse may present anywhere along thespectrum from acute to end stage and as either aclassic or insidious case. If three of more of theabove signs are found in a horse, and the history issuggestive of either recurrent disease or breed asso-ciated insidious disease, a presumptive diagnosis ofuveitis may be made. Note that some of the signsare related to acute inflammation, and some repre-sent chronic ocular changes that are permanentscars.
Some experts prefer to refer to the syndrome as“equine persistent uveitis” because inflammation isdetectable on a cellular basis in all of these conditions,including quiescent and insidious cases. Miosis is ahallmark of most acute forms of recurrent or persis-tent uveitis.
Aqueous flare may be the first sign to appear andthe last clinical sign to disappear.Classification by Primary Observable Region of Oc-ular InvolvementAnterior uveitis: The observable inflammation is re-stricted to the anterior segment (cornea, AC, iris).
Posterior uveitis: Inflammation is predominantlyobservable in the posterior segment (vitreous, ret-ina, and optic nerve). Most often seen in warm-bloods and Appaloosas.
Panuveitis: Cases where the entire eye is in-flamed. Anterior or posterior disease may progressto panuveitis over time.
Care must be taken to assure that there is notanother primary problem in the eye that is causinginternal inflammation. The cornea must be exam-ined closely for signs of corneal ulcer, stromal ab-scess, foreign body, neoplasia, and immune-mediated or idiopathic keratitis. The globe shouldbe examined for neoplasia. Ruling out concurrentocular disease that incites ocular inflammation iscritical, because corticosteroid therapy is contrain-dicated in many of these conditions.PathophysiologyUveitis begins with compromise of the blood–ocularbarrier. This barrier normally functions to keepthe aqueous and vitreous clear as tight fenestrationsbetween the cells of ocular capillary walls preventcells and large molecules from passing through theblood vessels of the iris and the choroid. The blood–ocular barrier also serves to isolate intraocularstructures from the normal traffic of immune sur-veillance, making the tissue of the inside of the eyean immune privileged site.
390 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

In acute uveitis, the uveal blood vessels in the iris,ciliary body and choroid thicken and become con-gested. Soon they become “leaky,” and cells andinflammatory mediators cross the compromisedblood–ocular barrier and enter the inside of the eye.Most of the cells that cross the barrier initially areneutrophils. This is seen grossly as hypopyon,aqueous flare, and vitreous haze. Neutrophils thatenter the eye are soon replaced by large numbers oflymphocytes, some of which infiltrate the connectivetissue of the ciliary body and iris, forming largefollicle-like clusters. Antibodies and inflammatorycytokines are detectable inside the eye and withinocular tissues. These substances probably reactwith host and (in some cases) infective factors tocontribute to ongoing pathologic change. Numer-ous heavy exudates appear on intraocular tissues,most notably on the posterior surface of the iris andciliary body, on the capsule of the lens, and in thelayer between the retinal pigmented epithelium(RPE) and the photoreceptors of the retina. Theexudates interfere with the function of the oculartissue they adhere to. Cytokine activity mediatestissue destruction. With repeated or persistent in-flammation, the various chronic changes occur.Vision loss results when dense cataract and syn-echiae obscure acuity, when the retina detaches ordegenerates and no longer can transmit processedlight signals to the brain, or when glaucoma causesischemic damage and degeneration of the opticnerve.EtiologyDecades of research have substantiated that recur-rent uveitis is an immune-mediated disease.1-5
However, some bacterial, viral, and parasitic infec-tions have been associated as triggering events forthe syndrome. Factors include the following: bac-terial infections (leptospirosis, Borrelia burgdorferi[Lyme disease], brucellosis, Streptococcus, Rhodo-coccus equi [foals], generalized septicemia); viruses(influenza, equine viral arteritis, parainfluenza);parasites (onchocerciasis, strongylus, toxoplasmo-sis); and host conditions (tooth root abscess, severehoof abscess, septicemia, severe trauma).
Of all the possible infectious triggers, leptospirosisis the most significant worldwide. Leptospirosis-associated cases account for at least 60% of the casesof ERU seen in our practice, which is located in atemperate river valley in the northeast UnitedStates.Leptospirosis and UveitisThe most significant serovars associated with dis-ease are L. interrogans serovar Pomona (seen oftenin the United States) and L. interrogans serovarGrippotyphosa (seen often in Germany and centralEurope). Factors that increase the risk of leptospi-rosis in horses include the following: pasture accessto cows, pigs, or deer; close proximity to streams orponds frequented by the same; use of piped pondwater for drinking water; heavy infestation of stable
with rats; and rainy season with persistence ofground water.
Horses become infected when they drink watercontaminated by the urine of a carrier animal (oftena cow, deer, pig, or rat). The spirochete gains ac-cess to the horse’s bloodstream by mechanical pen-etration of mucous membranes. Bacteremiaresults in clinical illness, manifested by anemia,fever, and flu-like symptoms. Clinical disease ismild and self-limiting, and rarely diagnosed as aleptospiral infection when acute. Resolution ofsigns does not mean elimination of the bacteria fromthe body—the spiral organisms often colonize thekidneys of the horse and may persist for a fewmonths, being shed in the urine. Leptospirosis hasalso been associated with numerous cases of abor-tion in mares. Recent research has documentedthat the organisms can persist in the eye and may berecovered from ocular media by culture in somecases.
Ocular signs of classic uveitis associated with lep-tospirosis rarely occur during acute leptospiral in-fection but rather begin months after infection.Initial signs subside with or without therapy butrecur at unpredictable intervals. Subsequent epi-sodes of inflammation may be more or less severethan the initial one. Inflammation associated withsubsequent episodes eventually compounds anddamage of intraocular tissues creates visual deficits.Blindness is a common final outcome.
The pathogenesis of the “lepto link” with equinerecurrent uveitis has been the subject of much re-search and debate. The key findings are as follows:antibodies to pathogenic serovars can be found inthe sera, aqueous, and vitreous of horses with lepto-associated uveitis, and studies have supported thehypothesis that intraocular synthesis of these anti-bodies is occurring; leptospiral organisms have oc-casionally been cultured from the ocular media ofhorses with uveitis; molecular homology has beenshown between the equine cornea and leptospira;pineal inflammation has been shown to accompanylepto-associated uveitis in horses similar to experi-mental models of uveitis in laboratory animals; ma-jor histocompatibility complex (MHC) II reactivityhas been shown on resident and infiltrating cells ofhorses with both natural and experimental lepto-spiral associated uveitis; and seroreactivity toequine retinal proteins has been found in horseswith lepto-associated uveitis.
A unified theory has yet to appear to explain allthe ocular events that accompany leptospiral-asso-ciated uveitis.
● Is it a direct toxicity of an intraocular infectionwith the spirochete?
● Is it an autoimmune disease against “self” thatis triggered by molecular mimicry between lep-tospira and host tissue?
● Are leptospira somehow modulating the im-mune response of the eye?
AAEP PROCEEDINGS � Vol. 53 � 2007 391
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

These questions continue to challenge research-ers. Although systemic infection with pathogenicstrains of leptospirosis is clearly a common triggerfor vision-threatening recurrent uveitis, it is likelythat the genetic makeup, specifically that of theMHC complex, of the individual horse that contractsthe disease plays a role in determining both suscep-tibility to leptospirosis as an inciting trigger andseverity of subsequent inflammatory episodes.Testing Horses for Exposure to LeptospirosisSerum from horses diagnosed with uveitis should besubmitted for modified agglutination test (MAT)analysis against a panel of leptospiral serovars.Many non-uveitic horses will show low titers to thebratislava, autumnalis, hardjo, or canicola serovars.These are judged to be insignificant findings innortheastern practice geography. Positive titers,especially titers �1:400, to L. interrogans serovarPomona or L. interrogans, serovar Grippotyphosa,are judged to be significant and a likely indicator ofleptospiral associated etiology. Seroreactivity to L.interrogans serovar Icterohemorrhagica is oftenpaired with reactivity to L. interrogans serovarPomona.
Research has shown that horses with uveitis canoccasionally be seronegative for antibodies to lepto-spira and still have leptospiral DNA or live organ-isms in the eye. Therefore, a negative titer does notfully rule out leptospirosis as an etiologic factor.A positive titer to serovars Pomona or Grippoty-phosa is, however, strong cause for concern.Breed and UveitisRecent work has also shown that certain breeds areat risk for uveitis, most notably Appaloosas, Euro-pean warmbloods, and draft horses. The Appal-oosa breed is 8.3 times more at risk than otherbreeds for uveitis. Appaloosas that have insidiousdisease often have overall roan or light coat colorsrather than dark coats with a rump blanket. Theskin around the lids of affected Appaloosas is oftenmottled or pink in pigmentation. Mane and tailhair may be sparse. It is theorized that thesehorses have genetic proclivity to uveitis because ofaberrations in the major histocompatibillity com-plex, specifically in their equine lymphocyte antigensubtype. Recent research from Germany has sup-ported this concept in German warmbloods suscep-tible to disease.Unilateral Versus Bilateral DiseaseLittle work has been done to document the incidenceof ocular involvement in horses, but recurrent uve-itis can be a unilateral or bilateral disease. In astudy of 160 cases: 50% of the lepto-associatedhorses had unilateral disease and 50% had bilateraldisease; �80% of the Appaloosas had bilateral dis-ease; and 62% of the cases that were seronegative tolepto, and also non-Appaloosas were unilateral.
Uveitis may begin in one eye and later occur in thefellow eye. However, if a case is unilateral and noattacks are seen in the other eye for 2 yr after the
initial attack, it is uncommon for uveitis to show uplater in the contralateral eye.
Therapy of UveitisMydriasis is essential therapy for all cases of acuteuveitis. Initial application of atropine should befrequent until the pupil is fully dilated. Severecases may show poor response to the action ofmydriatics.
Topical corticosteroids and systemic NSAIDs arethe core elements of anti-inflammatory field therapyfor acute attacks. Therapy should be intense for�2 wk and may be tapered over another 2 wk.Subconjunctival and/or systemic corticosteroids areindicated in severe cases.
Corticosteroid topical therapy may induce calcificband keratopathy, especially in horses with lepto-spiral associated uveitis. Treat with EDTAchelation/keratectomy.
Horses with acute uveitis are very painful andmay suffer secondary corneal ulcers from selftrauma. Corticosteroids are contraindicated inthese cases—use topical NSAIDs instead and treatfor any infection/collagenolysis of the ulcer.
Anecdotal reports indicate that a 1-mo course oforal doxycycline may help cases that are associatedwith leptospiral infection.
Acupuncture therapy may help moderate the fre-quency or severity of episodes.
Therapy does little to alter the progression of dis-ease in horses with insidious uveitis.
Some horses (especially Appaloosas) develop sec-ondary glaucoma late in their disease. Glaucomatherapy is difficult, but timolol, dorzolamide or acombination of these drugs (Cosopt) may be tried.Judicious topical steroids may help as well.
Although horses in central Europe routinely un-dergo pars plana vitrectomy for ERU, results havebeen poor with this procedure in the United States,and the procedure is not often advised here. Dr.Brian Gilger of North Carolina State University hassome success with a surgery where a suprachoroidaldevice that slowly elutes cyclosporine is implantedunder the sclera. Currently, this device is notavailable for private cases, but work is in progress toobtain FDA approval.Prognosis of UveitisVisual prognosis for horses suffering from multipleacute attacks of uveitis or insidious chronic diseaseis always guarded. Data on the incidence of blind-ness in uveitic horses are lacking, but it is clear thatuveitis is the leading cause of blindness in horsesworldwide. The authors have observed ocular in-flammation serious enough to threaten vision in atleast 1–2% of the practice population. Analysis ofthe visual outcome of 160 cases followed over 11 yrrevealed the following trends: 56% of the case se-ries (89/160) lost vision in one or both eyes; 20% ofthe cases (32/160) became completely blind; and 36%(57/160) lost vision in one eye.
392 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007
Breaking the cases down further into those thatwere seropositive or seronegative to L. interrogansserovar Pomona and those that were Appaloosas or“non-Appaloosas,” the following trends were seen:horses that were seropositive to L. pomona and alsoAppaloosas had a very poor visual prognosis: 100%lost vision in at least one eye and 50% went com-pletely blind (n � 14); horses that were Appaloosasand seronegative had substantial occurrence ofblindness: 72% lost vision in at least one eye and29% went completely blind (n � 28); horses thatwere seropositive to L. pomona and non-Appaloosashad a slightly lower rate of blindness: 50% lostvision in at least one eye and 17% went completelyblind (n � 86); horses that were seronegative andnon-Appaloosas had the best visual prognosis: 34%lost vision in at least one eye and just 6% wentcompletely blind (n � 32).
Secondary complications and degeneration of ocu-lar tissues are common sequelae of uveitis. Severalinteresting findings were noted in this series thatare representative of sequelae seen in ERU horses inother geographic regions of the world.CorneaFocal scars, streaks, calcium deposits, and othercorneal opacities were common. The seropositivehorses experienced a high rate of calcific band kera-topathy. Striae and dense corneal streaks werecommon in Appaloosas and were highly correlatedwith blindness.IrisIris atrophy and color change were common, espe-cially in Appaloosas and seropositive horses. Ante-rior synechiae were rare unless phthisis bulbi waspresent, but posterior synechia occurred in nearlyone third of all cases and 40% of Appaloosas.LensDiffuse cataract(s) developed in 41% of all cases, andnearly 75% of the Appaloosas. These were a com-mon cause of blindness. Lens luxation was com-mon in Appaloosas (29%).Posterior SegmentSevere vitritis was observed in nearly one third ofthe cases. Peripapillary scarring was also presentin about one third of the horses. Cataracts andsynechiae often obstructed posterior segment evalu-ation, so inflammatory changes were probablyunderreported.Glaucoma and Phthisis BulbiAppaloosas had the highest rate of glaucoma (21%).Phthisical eyes developed most often in Appaloosasand seropositive horses.
Owners often are concerned that horses with ERUwill need enucleation. In the above series, only 4%(6/160) were enucleated for complications from cor-neal infection or glaucoma. Of more concern is thefact that 43 of the 160 horses (27%) were treated forcorneal ulcers over the observation period. Risk ofcorneal ulcers in ERU horses should be stressed,
because owners often choose to medicate horses withpainful eyes themselves, and they may potentiateserious infections by applying corticosteroids anddelaying proper diagnosis. Ten horses sufferedfrom calcific band keratopathy. This is a trouble-some complication that limits therapeutic optionsfor ERU.
Future understanding of recurrent uveitis in allspecies will revolve around the study of several keyquestions. What genetic makeup predisposes indi-viduals to develop disease? If the disease is auto-immune, which autoantigens participate in theinitiation and perpetuation of inflammation? Whatimmune mechanisms initiate the immune responseand mediate tissue destruction?
Study continues to determine the genetic predis-position for the syndrome in certain horse breeds(i.e., Appaloosas and German warmbloods). If agenetic marker is associated with susceptibility,horses with this genotype could be identified andexcluded from use for reproduction, thus decreasingthe prevalence of the disease. New immunosup-pressive therapies, such as tacrolimus (FK506) mayoffer hope in the medical management. Perfectinga device to deliver such a medication may also befeasible. Studies are also being done to determinethe role of leptospirosis or other microorganisms inthe initiation and pathogenesis of ERU. Effort con-tinues to further quantify the immune events thatcharacterize inflammation and mediate recurrence.Vaccine research is ongoing at several universities.
4. Equine Glaucoma
The glaucomas are a group of diseases resultingfrom alterations of aqueous humor dynamics thatcause an intraocular pressure (IOP) increase abovethat which is compatible with normal function of theretinal ganglion cells and the optic nerve. Horseswith previous or concurrent uveitis, aged horses,and Appaloosas are at increased risk for the devel-opment of glaucoma. Iris and ciliary body neo-plasms can cause secondary glaucoma. Congenitalglaucoma is reported in foals and associated withdevelopmental anomalies of the iridocorneal angle.1-5
The infrequency of diagnosis in the horse may becaused, in part, by the limited availability of tonom-eters in equine practice but also by the fact thatlarge fluctuations in IOP, even in chronic cases, maymake documentation of elevated IOP difficult.
Afferent pupillary light reflex deficits, cornealstriae, decreased vision, lens luxations, mild irido-cyclitis, and optic nerve atrophy/cupping may alsobe found in eyes of horses with glaucoma.
The systemically administered carbonic anhy-drase inhibitors acetazolamide (1–3 mg/kg, PO, q12 h), the topical carbonic anhydrase inhibitor dor-zolamide (2%,q 8 h), and the �-blocker timolol mal-eate (0.5%, q 12 h) have been used to lower IOP inhorses with varying degrees of success. The newerprostaglandin derivatives cause low-grade uveitisand may exacerbate the IOP in horses with glau-
AAEP PROCEEDINGS � Vol. 53 � 2007 393
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

coma. Topical atropine therapy was once thoughtto reduce the incidence of glaucoma in horses withuveitis, but it should be used cautiously in horseswith glaucoma because it may cause IOP spikes.Anti-inflammatory therapy, consisting of topicallyand systemically administered corticosteroids,and/or topically and systemically administered non-steroidal anti-inflammatories also seem to be bene-ficial in the control of IOP.
Laser destruction of the ciliary body (cyclophoto-coagulation) works the best at controlling IOP andpreserving vision in horses.1-5
Contraindications/Possible InteractionsConventional glaucoma treatment with miotics mayprovide varying amounts of IOP reduction in horses.Miotics and prostaglandins can potentiate the clin-ical signs of uveitis and should be used cautiously inhorses with anterior uveitis. The horse eye seemsto tolerate elevations in IOP for many months toyears that would blind a dog; however, blindness isthe end result. Buphthalmia can be associatedwith exposure keratitis. Topical atropine does notseem to have the benefit of lowering IOP in a ma-jority of glaucomatous horse eyes as originallyproposed.
5. Optic Nerve/Peripapillary Region
The optic nerve is formed by the bundling of�750,000 axons of the ganglion cells of the retina.The portion visible on fundic exam is the optic discthat is located below and slightly temporal to theposterior pole of the globe. It is ovoid in shape,with the longer horizontal diameter measuring 5–7mm. When viewed with a direct ophthalmoscope,the optic nerve and other fundic structures are un-der �8 magnification. The vascularization of theoptic disc is paurangiotic, with 40–60 small arteriesand venules that can be seen radiating from the disc.Horses with light coat colors may have a sparselypigmented non tapetum, revealing the underlyingtigroid pattern of the larger choroidal vessels. Theperipapillary region shows great variability in ap-pearance. Equine practitioners should consult at-lases and texts on equine ophthalmology to look atpictures of normal variations of peripapillary pig-ment, vascularization, disc color, and myelindistribution.
The most common pathologic findings observed onfundic examination of the peripapillary region in-clude the following.
Chorioretinitis
Chorioretinitis is inflammation of the choroid andretina. Inactive lesions are more often reportedthan active lesions. The tapetal region is rarelyaffected. It is manifested in equine eyes as focal“bullet-hole” retinal lesions, diffuse chorioretinal de-generative lesions, horizontal band lesions of thenontapetal retina, and chorioretinal degenerationnear the optic nerve head.1-5
Active chorioretinitis appears as focal white spotswith indistinct edges and as large diffuse gelatinousgray regions of retinal edema. Inactive chorioreti-nitis can appear as circular depigmented regionswith hyperpigmented centers or large areas of de-pigmentation that appear in some cases as thewings of a butterfly flanking the nasal and temporalmargins of the optic disc. Consult atlases of equineophthalmology for photographs of chorioretinitisand pictures of benign conditions like coloboma orvariations of pigment in the non-tapetal area thatare commonly confused with pathologic changes.
Lesions can be caused by infectious agents (e.g.,leptospirosis, equine herpes virus-1, Onchocerca cer-vicalis, Rhodococcus, Streptococcus equi, Lyme’s dis-ease, brucellosis, toxoplasmosis, Halicephalobusgingivalis), immune-mediated uveitis of unknownorigin, trauma, or vascular disease. Chorioretinitismay be found with or without the signs of anterioruveitis found with ERU. Serologic testing mayidentify infectious causes of chorioretinitis. Sys-temic NSAID medication is administered for chori-oretinitis. Flunixin meglumine, phenylbutazone,or aspirin are indicated. Topical medication doesnot reach the retina and is only indicated if signs ofanterior uveitis are also present.
Senile Retinopathy
This is commonly seen in aged animals. It presentsas bilateral multifocal islands of hyperreflective tis-sue bounded by darkened irregular linear hyperpig-mentation, most prominent in the peripapillarynontapetal region. Senile retinopathy resemblesthe spiculated microscopic appearance of bonetissue.
Optic Atrophy/Ischemic Retinopathy
Disc shows severe pallor and attenuation of vessels,and it may also show extensive retinal depigmenta-tion and focal pigment hypertrophy. It follows in-farction from head trauma, intracarotid injection,embolism, or optic neuritis.
Proliferative Optic Neuropathies
Typical finding is a focal, lobulated pink or whitemass that extends from the margin of the disc intothe vitreous. It is generally asymptomatic, benign,and non-progressive; lesion may be reactive glialcells. No treatment is needed. Should be moni-tored to check for enlargement because the differen-tial includes optic nerve neoplasia. Astrocytomas,medulloepithelioma, and neuroepithelioma havebeen reported. Documentation of an enlargingmass off the optic disc with blindness is an indica-tion for immediate exenteration.
Retinal Detachments
Retinal detachment is a separation of the nine lay-ers of the sensory retina from the RPE. It is asso-ciated with slowly progressive or acute blindness inhorses. It can be congenital in newborn foals or
394 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

acquired later in life in adults. Retinal detach-ments can occur bilaterally or unilaterally and bepartial or complete. Complete retinal detachmentsare seen clinically as free-floating, undulating,opaque veils in the vitreous overlying the optic disc.The tapetum is hyper-reflective.
Retinal detachments are a complication of ERUand are also associated with microphthalmos, headtrauma, perforating globe wounds, cataract surgery,equine protozoal myeloencephalitis, and may be sec-ondary to tumors or vitreal degenerative processes.Retinal detachments can also be idiopathic. If themedia of the eye are so opaque (e.g., corneal edema,cataract) that the fundus cannot be visualized, b-scan ultrasound can be used to diagnose the classic“seagull sign” of retinal detachment. Laser surgeryand pneumatic retinopexy to reattach the retina arewell described for the dog but have not yet beenreported for the horse.
Congenital Stationary Night Blindness
Congenital stationary night blindness (CSNB) isfound mainly in the Appaloosa and was oncethought to be inherited as a sex-linked recessivetrait. Up to 25% of Appaloosas may be affected.Cases are also noted in Thoroughbreds, Paso Finos,and Standardbreds.
Clinical signs include visual impairment in dimlight with generally normal vision in daylight andbehavioral uneasiness and unpredictability occur-ring at night. CSNB does not generally progress,hence its name, but cases of progression to visiondifficulties in the daytime are noted. Ophthalmo-scopic examination is normal. Diagnosis is by clin-ical signs, breed, and electroretinogram (ERG) withdecreased scotopic b-wave amplitude and a largenegative, monotonic a-wave. CSNB seems to becaused by functional abnormality of neurotransmis-sion in the middle retina. There is no therapy forthis condition, but affected animals should not bebred.
Equine Motor Neuron Retinopathy
Retinal pigment epithelial cell accumulation of cer-oid lipofuscin is found to be associated with theneurodegenerative condition, equine motor neurondisease (EMND). Generalized weakness, musclefasciculations, weight loss, and muscle atrophycharacterize EMND.
Ophthalmic lesions are found in 30% of affectedhorses. A mosaic pattern of dark to yellow brownpigmentation in the tapetum of affected horses isnoticed, associated with a horizontal band of pig-mentation at the tapetal–non-tapetal junction.
Consistent evidence of a plasma vitamin E defi-ciency (1.799 �g/ml) in horses with EMND sug-gests that the RPE, retinal, and spinal lesions are aresult of oxidative injury associated with a pro-longed deficiency of nutritionally derivedantioxidants.
Although visual deficits may not be consistentlyfound, nyctalopia and ERGs with a 50% reduction inb-wave amplitude and normal appearing a-waveshave been noted associated with EMND.
Supplementation with 6000 IU vitamin E per dayin horses with EMND may stabilize the neurologicsigns, but it is not known if this will affect the RPEand retinal changes.
6. Tips on Therapeutics for Equine Eye Problems
If ophthalmic ointments are prescribed, spend timewith the owner showing the best way to apply them.Helpful tips include pointing out the orbital rim andtelling the owners that they can rest the finger thatis holding the lid open against, or slightly under-neath, the rim dorsally. Having the owners touchthe crease of the eyelid to lift it dorsally is anotheruseful tip.
Dispense topical meds in a 4 � 6-in “Write onbag.”u Write out the treatment schedule for thatmedication for the next several days by making cir-cles on the bag label next to days of the week. Thissimple step increases compliance and keeps themedication clean.
Study ophthalmic textbooks for eyelid plastic sur-gery techniques. Practice some procedures on ca-davers to get a feel for tissue handling. Becomecomfortable using fine 4-0 sutures for repairs. Theauthor schedules suture removal of all skin su-tures—whether resorbable or not—at 8–12 days,because the eyelid tissue retains some persistentinflammation if these sutures are left in.
The use of a fly mask or modified racing blinkerhood helps protect the periorbital region after sur-gery. Be sure that there is not a “greenhouse” ef-fect from a closed blinker—perforate the plastic ifneeded.
Decision making on handling tumors in the peri-orbital region is difficult because there are manyoptions for treatment. If the tumor is large, close tothe lid, or approaching the globe, referral may be thebest option. Recurrence or ineffective treatmentmay have a disastrous result.
Nictitans removal is a simple surgical procedurethat can be done at a clinic or in the field. I like todo it within stocks at our clinic.
Train owners to call for same day examination onany lids that show severe swelling.
Debridement of the cornea should be performed insuperficial ulcers only. It can be as simple as swab-bing the lesion with a sterile swab or as involved asactually cutting away some cornea with a no. 15 orno. 63 blade.
Subconjunctival injections are easiest if thehorse’s head is supported by a table made of bales,and the handler, who is standing on the contralat-eral side of the horse, uses the ear of the horse to tiltthe top of the head away from the clinician, therebyexposing the target sclera.
AAEP PROCEEDINGS � Vol. 53 � 2007 395
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007

Application of topical anesthetic using sterile cot-ton swabs will facilitate subconjunctival injectionsand work on the nictitans.
Lavage catheters (SPL tubes) are useful ways todeliver medication to the surface of the eye, espe-cially in fractious horses. Order the longer “Floridacatheters” from Mila. The footplate should be putin the fornix of the upper or lower lid. Tape thetreatment end to one half of a tongue depressor tomake injection of medication easier. The treat-ment end should be made of a 20-gauge catheterinserted in the tubing and plugged by a standardinjection cap. Inject 0.1–0.2 ml of drug at a timeand “chase” with 1.0 ml of air before injection ofadditional medications. Horses that rub shouldwear hoods so they do not dislodge the system.Adhesive tape “butterfly” tabs sewn to the skin workbetter for securing the tube than the guides thatcome with the kits. Weave the long delivery tubethrough braids in the mane to prevent inadvertenttearing of the tubing. Medication loss will be min-imized and horse comfort maximized if injections ofliquid and air are delivered slowly through the in-jection port. See detail in Table 1 for informationon fortified solutions that can be administeredthrough the lavage tube. Most horses with SPLsare on complex medication schedules that include avariety of anti-infective agents, a mydriatic, and oneor more anti-collagenase therapies.
7. Key Prognostic PointsPrognosis of orbital and periorbital disease varieswith the etiology, but prompt assessment, vigoroustherapy, and judicious referral will optimize out-come. Client seminars or handouts discussing eyeproblems should stress that lumps, cuts, and asym-metry of the region around the eye can be veryserious, and they should schedule examination ofthese conditions without delay.
Prognosis of eyelid lacerations or reconstruction ofacquired scars is dependent on meticulous tech-nique. Immediate repair of lacerations is desir-able, but if the clinician is presented with an “old”injury, there may be plastic surgery strategies thatwill effectively reconstruct the eyelid. Prognosis ofthe repair is optimized if the clinician uses carefulplacement of small gauge sutures and takes care inreconstructing the tarsal plate. Some severe lacer-
ations may be stabilized by temporary tarsorrhaphy.Placement of the head of the horse on a “table” madeof bales will facilitate standing surgery.
Corneal ulcers can be simple traumas that resolveuneventfully or complex problems that are amongthe most complicated and expensive that horses ex-perience. Often, prompt assessment and aggres-sive therapy wards off disaster. Practitionersshould commit to seeing painful eyes on the date ofoccurrence.
Many drugs are used to treat corneal problems.Familiarity with the available medications will op-timize success of treating the equine cornea. Manyof these meds are human products that must beprescribed through pharmacies, compounded, or ob-tained at universities. Table 1 summarizes manyof these products.
Cataracts are rarely operated on unless congeni-tal and complete. Lens luxation and cataract arefrequent complications of uveitis.
References and Footnotes1. Barnett KC, Crispin SM, Lavach JD, et al. Color atlas and
text of equine ophthalmology, 2nd ed. London: Mosby-Wolfe,2004.
2. Brooks, DE. Ophthalmology for the equine practitioner.Jackson, WY: Teton NewMedia, 2002.
3. Brooks, DE, Matthews AM. Equine ophthalmology. In:Gelatt KN, ed. Veterinary ophthalmology, 4th ed. Philadel-phia: Williams and Wilkins, 2007;1165–1274.
4. Cutler T, ed. Veterinary clinics of North America equine prac-tice 2004;20 (2):p. 417–428. Updates in Equine Ophthalmol-ogy. Philadelphia, Saunders.
5. Gilger B, ed. Equine ophthalmology. Philadelphia: Elsevier,2005.
6. Brooks DE. Clinical techniques in equine practice. Philadel-phia: Elsevier, 2005.
7. Lavach D. Large animal ophthalmology. St. Louis, MO:Mosby, 1990.
a Heine, Lombart Instruments, Bradenton, FL 34210.b Finoff, Lombart Instruments, Bradenton, FL 34210.c Maglite, Ontario, CA 91761.d Lombart Instruments, Bradenton, FL 34210.e Kowa SL-15, Kowa Optimed, Torrance, CA 90502.f Tonopen Vet, Dan Scott Associates, Westerville, OH 43081.g Mydriacyl, Alcon Labs, FT Worth, TX 76134.h Dacron Medical Packaging, Corp, Camarillo, CA 93017.i MILA International, Erlanger, KY 41018.j OpticsPlanet, Inc., Northbrook, IL 60062.k Diff-Quick Stain, IMEB, San Marcos, CA 92069.l Heine, Lombart Instruments, Bradenton, FL 34210.m Welch Allyn, Skaneateles, NY, 13153.
396 2007 � Vol. 53 � AAEP PROCEEDINGS
IN-DEPTH: OPHTHALMOLOGY—SURVIVAL METHODS FOR PRACTITIONERS
Reprinted in IVIS with the permission of the AAEP Close window to return to IVIS www.ivis.org
Proceedings of the Annual Convention of the AAEP - Orlando, Florida, 2007